
Abstract
The present paper is the outcome of instigated thought by several studies on urbanization and prevalence of vector-borne disease in tropical areas. It is envisaged and hypothesised to find if any correlation exists between urbanization process, heat island generated due to urbanization (e.g. higher density of road network, buildings and traffic) in the urban areas and the outbreak of vector-borne diseases like malaria and dengue. The paper primarily looked into the temporal data of all metropolitan cities and found that there is an increased incidence of dengue outbreak in all metropolitan cities. There is a lot of variability in the rainfall in Delhi, but all other metropolitan cities have been experiencing an average rainfall over the past two decades. Review of literature led to the construction of hypothesis that there exists a close association between urbanization and the increased incidence of dengue outbreak. Ordinary least square method is used to find if there is any correlation between the urbanization variables and disease outbreak. Regression result shows that there is high possibility between the urbanization and disease outbreak.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others

Keywords
1 Introduction
Arthropod disease viruses such as yellow fever, malaria, encephalitides, filariasis and dengue fever are changing the health epidemic scenario mainly in developing countries, especially in the tropical countries. These are the most important arboviral diseases in human both in terms of mortality and morbidity. Dengue fever because of its persisting trend in countries can be considered the most common of all arthropod-borne diseases after malaria. Each year an estimated 100 million cases of dengue fever occur worldwide with the greatest risk occurring in Indian subcontinent, Southeast Asia, Southern China, Taiwan, the Pacific Islands, the Caribbean, Africa and Central and Southern America. Though DF is hardly fatal, the disease incapacitates the infected patients in several ways. Over half of WHO member states representing a total of 2000 million are threatened by dengue. It occurs in most of the tropical countries. The dengue infection ranges from asymptomatic through classical dengue to life-threatening dengue hemorrhagic fever with shock (DSS) or without shock (DHF).
2 Indian Context
Dengue is a threat in India, especially in the capital city of Delhi, Kolkata and Chennai where the number of reported dengue cases and deaths is higher and trend shows that it may go even higher in the future (Table 7.1). Epidemiologically, dengue fever/dengue hemorrhagic fever is not only changing in disease pattern but has changed its course of manifestation in the form of severe DHF with increasing number of outbreaks. The table also indirectly proves that the disease is more of an urban disease.
Possible cause which has been hypothesised in this paper is the growth of urban structures (buildings, roads and other urban infrastructures) which has been causing rise in temperature by creating urban heat island effect in the main city leading to increased frequency of rain and humidity causing vectors to reproduce at an alarming rate.
3 Methodology and Data
The paper tries to assess the series of outbreaks and expected causes of persisting phenomena of disease by finding the climatic variables – average rainfall, average maximum temperature, average annual temperature and some select urbanization-related indicators such as urban density, urban population and vehicular load on roads with the disease data in the metropolitan cities. Procuring the disease data on zone level was difficult, and also no direct data to indicate the urban expansion (until interpretation of satellite images at different points of time) and outbreak of the disease could be utilised. With such limitation, the increased burden of population in the city, urban density and traffic on the roads are considered as the best alternative to analyse urbanization in Delhi.
The paper therefore first looks into the morphology of the urban growth considering urban density and population growth and then further analyses this growth in the context of disease pattern, rainfall and temperature oscillation in Delhi. As already mentioned, the paper hypothesises that the prevalence of dengue is closely linked with the heat entrapped by the urban structure accentuating the temperature and humidity, thus helping Aedes mosquitoes to breed faster and in larger number.
Besides plotting the time series data of rainfall, temperature and dengue prevalence from 1996 to 2013 in Delhi, the study also tries to find if there is any changes occurring in some other Indian metropolitan cities. The study tries to statistically estimate the effect of urban growth on disease of dengue by taking the help of ordinary least square method only in the case of Delhi.
4 Overview of the Literature: Pragmatic Issues in Urbanization, Urban Heat Island Effect and Health
Literature and studies on climate change and epidemic is fewer but gripping faster to establish climate change and epidemic in tropical countries. Frequent outbreak and consistency in dengue fever attributed to the climate change explored by the researchers at Imperial College London and WHO Kobe Centre in Bangkok in 2008. The report asserts and declares dengue an urban disease (Gubler et al. 2001) because vectors breed mainly in containers such as pots and tyres. There are studies which have reported the climatic change-influencing factors (Napier 2003; Chakravarti and Kumaria 2005; Githeko et al. 2000) such as extreme humidity, extreme temperature, El Niño and human development factors. The current paper envisages that the seasonal or cyclic factors of the disease are combined with the fluctuating humidity and temperature data with the urban density (a proxy variable of urban growth) which creates heat effect in some of the dense area and thus leads to pocketed outbreak of the disease. The “tiger” mosquito Aedes aegypti is quoted to be very sturdy and travels up to 500 m. Aedes aegypti is extremely common in areas lacking piped water systems and depends greatly on water storage containers to lay eggs.
The mosquito which feeds exclusively on human blood is considered well adapted in the urban surrounding. A study in Delhi metropolitan area says that the disease has changed from being benign to becoming a more frequent and severe form of DHF (Gupta et al. 2006). Delhi has faced seven outbreaks of dengue infection as reported by the study, which may have gone up by two digits considering 2010 and 2013 outbreak years. The study found all four dengue serotypes present in the blood samples, yet in 2003 serotype 3 was more prevalent. A time series study done by Chaosuansreecharoen and Ruangdej in Yala Province, Thailand, found that temperature was positively associated with dengue incidences and relative humidity and monthly rainfall were not positively associated with the dengue incidences in this study area in Thailand (Chaosuansreecharoen and Ruangdej 2014). Another study on the climate change and its impact on vector-borne diseases assessing on continental basis says that the global temperature will rise by 1.0–3.5 °C by 2100 increasing the risk of more outbreak and wider spatial spread of vector-borne diseases by stating that the arthropods can regulate their internal temperature by changing their behaviour but cannot do so physiologically and thus are essentially dependent on climate for their continued existence and reproduction. The authors also propose that the effect of climate change on transmission is more likely to be observed in the extremes of the range of temperature (within the range of 14–18 °C at lower bound and 35–40 °C at the upper bound) (http://www.eliminatedengue.com/faqs/index/type/aedes-aegypti).
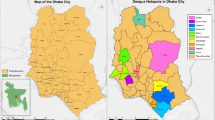
In Asia, the temperature has increased by 0.3–0.8 °C across the continent in the past 100 years and is projected to rise by 0.4–4.5 °C by 2070. The authors appear to be fully convinced by citing the incidences in highland Kenya that along with several other factors like seasonal variations, socio-economic status, vector control programmes, drug resistance, climate change and variability are highly likely to influence current vector-borne disease epidemiology. A study in Dhaka found alternate fluctuations in the outbreak of dengue every second year which was observed in the study conducted in Thailand also. The authors give reason where the outbreak was considered urban, and 70–80 % of the population developed herd immunity to the circulating dengue serotypes to thus prevent another outbreak in the following year. The study found some linear relationship with the climatic factors and the outbreak of the dengue fever (Karim et al. 2012). Another study was primary research based on blood samples of 1550 patients in Delhi. In this study, the result showed the large number of serological positive cases coinciding with post-monsoon period of subnormal rainfall and concludes that high rainfall, temperature and relative humidity can be the important climatic factors responsible for an outbreak (Chakravarti and Kumaria 2005).
Sharma and colleagues assert that Aedes aegypti, the primary vector of dengue fever, has global distribution, and it is invading areas under urbanization, citing several cities all over the world where different types of vectors have been traced in urban areas (Sharma et al. 2002).
5 Discussion
The review of literature and other evidences pinpoints to find the relationship between urbanization and dengue infection prevalence. The first section of the discussion revolves around urbanization, rainfall and temperature variability in Delhi. This section also briefly looks at the temperature and rainfall distribution in other metropolitan areas in India to find out if the cases of dengue have any correspondence with the flux of rainfall or temperature in the cities.
The second section evolves out of statistical analysis of the data on climatic variables and disease prevalence in the city of Delhi. The variables which have been used as indicators of urbanization are urban density, urban population and vehicular population in Delhi, while for climate variables, average annual rainfall, mean maximum temperature and mean annual temperature are considered to find the climatic influence on the disease. It can be argued that the variables selected for urbanization and climate are insufficient to segregate or decide on the heat island effect and climate influence on the disease prevalence; however, the paper heavily depends on the availability of the secondary data. Several limitations are encountered, e.g. unavailability of zone-wise data of the disease, temperature, and rainfall which could have provided a better relationship between disease, urbanization and climate-related change at micro level. The regression model nevertheless and correlation matrix do good justice to the hypothesis of urbanization, urban heat island effect and dengue prevalence.
6 Section I: Urban Expansion of Delhi
Satellite image of Delhi clearly (Fig. 7.1) shows that population expansion in and around the Delhi metropolitan city has increased tremendously. The upper images are a 1974 Landsat MSS (80 m resolution) on the left and a 1999 Landsat Thematic Mapper (28.5 m resolution) on the right. Growth in urban area from 1974 to 1999 is portrayed in the lower maps (areas coloured red). The image clearly shows the growth of the urbanised area has been tremendous in just two decades.

Population expansion in Delhi (1975 and 1999) (Source:http://www.mdafederal.com/environment-gis/national-security-policy-support/land-use/)
Recent release of the census data provides a clear indication that urban expansion has been tremendous as the density in all districts has reduced except Central and New Delhi (Fig. 7.2). However, a look at the density of Delhi reveals that some of the areas which may have geographically expanded could not possibly reduce the aggregate population density of Delhi which is higher than the 2001 census figures.

Population density in the districts of Delhi
7 Rainfall and Temperature in Metropolitan Cities
Temperature rise and temperature extremities have been studied at global scale and noted that even rise of temperature as low as 1° may expand the coverage of vector-borne diseases like malaria and dengue in temperate zone as well. There are incidences of increased frequency of flooding of urban areas. With a look at the average annual temperature in all four major metropolitan cities and the bearable limit within one degree of the temperature, then it can be concluded that the temperature has been shooting up beyond the recorded average temperature in all cities (Fig. 7.3). Delhi in particular has recorded annual average temperature either below the boundary of 1° (i.e. 1997, 2003) and sometimes above (2002, 2006 and 2009). In recent years, even Kolkata and Mumbai also experienced slightly hot years on an average, whereas Chennai has shown a trend of rising temperature consistently.

Average annual maximum temperature in the metropolitan cities
The average annual rainfall shows fluctuation especially in Mumbai, Chennai and Kolkata. Delhi however remained within the 500–1000 mm and recorded very regular rainfall for the past two decades (Fig. 7.4). The data on temperature and rainfall is only indicative to measure the climate change or heat island effect; we have to analyse the geographical variability also of rainfall or temperature to conclude the epidemic outcome. Nonetheless, the data still shows the rising trend of fluctuating rainfall and temperature. Further, we are not looking at the monthly variation of rainfall and temperature which is beyond the scope of this paper. This aspect if attempted may reveal some more intriguing aspects of climate change and disease in the urban areas.

Average annual rainfall in the metropolitan cities (in millimetres)
8 Section II
The cause of heat island effect may be not clearly perceptible but certainly has greatly influenced the span of humidity, longer rain spell thus becoming fertile time for the mosquitoes to breed and increased scope of infecting people also. The studies prove that the longer the duration of humidity and overcast sky leads to increased outbreak of vector-borne diseases especially of different strains. The National Vector-Borne Disease Control Programme and other microbiologists claimed the emergence of strain 2 which is more dangerous than earlier strains. Kolkata has recorded three times more dengue cases than Mumbai and Chennai. In sheer numbers, Delhi is a close second with 2,068 cases of the mosquito-borne diseases in 2012. Kolkata leads among the metros with the highest number of dengue cases (3321). Mumbai and Chennai have recorded 907 and 988 cases of dengue, respectively, in 2012. The number of dengue cases increased in Kolkata which rose from 199 in 2011 to as high as 3,321 in 2012. Mumbai’s dengue cases have increased by 283 %, while Chennai has seen over a 100 % rise in dengue cases in 2012. Delhi, which has recorded a 186 % increase in dengue cases in 2012 as compared to 2011, is confronting an outbreak of the most dangerous and virulent form of dengue virus.
Simple time series data however in itself is insufficient to predict the outbreak of dengue, yet the analysis of the dengue prevalence, monthly rainfall and temperature data does indicate that there exists a relationship in the climatic data, temperature and rainfall. Relative humidity is a better measurement to establish the association (if any) between the disease outbreak and the heat island effect. However, data constraints limit the scope of understanding this aspect of hypothesis. Close examination of Figs. 7.5, 7.6 and 7.7 shows a relationship between the disease prevalence temperature and rainfall. Looking at the rainfall and temperature, it is easier to locate more humid year along with all other years; 1996, 2001, 2004, 2006 and 2009 have experienced higher average temperature from June to August, and as observed in Fig. 7.6, which shows an analysis of average monthly rainfall, we find that the rainfall during the month of monsoon has considerably reduced, but its span has increased. Average monthly rainfall in 1993, 1994, 1995, 2003 and 2011 peaked during the monsoon time, but when we see the epidemic outbreak of dengue we find that when the temperature hovers around the average temperature but experience high and longer spell of rainfall disease is more likely to reach a level of outbreak. The paper as discussed does not reveal positive relationship between heat island effect and epidemic but leads to indicate the correlation and explanatory strength of the model.

Seasonal variation in dengue prevalence: 1996–2012

Average monthly rainfall in Delhi {1991–2013}

Average monthly temperature of Delhi {1996–2010}
The paper interprets the relationship existing among all variables by running Pearson’s correlation. It can definitely be concluded in two things: firstly, the number of cases reported has a significant positive relationship at 0.05 level with rainfall and, secondly, rainfall has no relationship with the urban density or vehicular population. However, the mean maximum temperature and mean annual temperature show significant positive relationship with the urbanization variables – urban population, urban density or vehicular population (Table 7.2).
Table 7.2 does not determine the strength of the variables. Therefore, the regression was done, and the study is able to explain 57 % of the total model which is reasonably acceptable explanation and shows association between disease prevalence, urbanization and climatic factors. Another important feature is the significant p values where values lower than <.05 are for rainfall and vehicular population. This suggests that the man-made factors such as vehicular density on roads leave higher impact on the disease outbreak and prevalence in the city (Table 7.3).
9 Some Points to Ponder on the Rainfall and Temperature Pattern in the Metropolitan Cities
Based on the regression results and the rainfall and temperature pattern in the metropolitan cities including Delhi, it can be easily said that the variability in the minimum temperature has been very low in the past two decades; however, the average maximum temperature is showing an increasing trend in all metropolitan cities for the same duration (Figs. 7.1 and 7.2). Annual average rainfall in the metropolitan cities is also showing a very high variability which could be due to other global influences, e.g. El Niño impact (Fig. 7.3). Delhi which has expanded remarkably over the last two decades is showing a rising trend of dengue prevalence which is though worrisome yet could be better predicted depending on the urban growth and population density in the particular areas. If rainfall for all other years is not considered except the rainfall in the year of outbreak of dengue, the study noted interesting features. For instance, July has recorded higher rainfall in the outbreak years except year 2010 leading to fertile ground for mosquito breeding in the forthcoming months by increased humidity and temperature (Figs. 7.4 and 7.5). Models have been developed on the basis of entomological, parasitological and also GIS-based meteorological variables to predict the outbreak of vector-borne diseases particularly malaria as both mortality and morbidity have been a cause of concern during malaria outbreak. In one such study based on the meteorological explanation, it is derived that when the mean monthly temperature is between 16.0 and 33.60 and relative humidity does not exceed 61 %, the correlation became stronger to predict the malaria outbreak. With all limitations, the paper quite ably put forth the question of urban planning and disease control especially urban diseases like dengue and malaria. Urban heat island greatly influences the relative humidity and may cause disease prevalence at an alarming rate besides causing other problems like uncomfortable living, boils, depression, etc. The paper also attempts to attract the plight of the poor people especially those who are living at the marginal ends of the city both at economic and geographical location. Advertisements, fuming and DDT spray are becoming ineffective at the time of disease outbreak. What is important is to reduce the cause of heating the core of the cities which is caused by traffic load, lack of green areas and emission of hazardous gases through air conditioning. It is all the more a cause of concern as the dengue epidemic is now becoming more visible in other metropolitan cities too. Another conclusion is that the reporting of the dengue cases is primarily by the hospitalisation cases and there is severe underreporting also by the government departments.
The present paper is a small step to construct the hypothesis of urban influence on dengue which has baffled public health experts and planners to take up preventive measures in the coming years. It is even more important to ascertain the effect of urbanization as the disease has been called an urban epidemic by the WHO and other studies.
References
Chaosuansreecharoen P, Ruangdej K (2014) A time series analysis of dengue incidence and weather factors in Yala Province, Thailand. Int J Health Wellness Soc 4. International conference on health, wellness and society, Vancouver, Canada, 14–15 March 2014
Chakravarti A, Kumaria R (2005) Eco-epidemiological analysis of dengue infection during an outbreak of dengue fever, India. Virol J 2:32
Githeko AK, Lindsay SW, Confalonieri UE, Patz JA (2000) Climate change and vector-borne diseases: a regional analysis. Bull World Health Organ 78(9):1136–1147
Gubler DJ, Reiter P, Ebi KL, Yap W, Nasci R, Patz JA (2001) Climate variability and change in the United States: potential impacts on vector- and rodent-borne diseases. Environ Health Perspect 109(suppl 2):223–233
Gupta E, Dar L, Kapoor G, Broor S (2006) The changing epidemiology of Dengue in Delhi, India. Virol J 3:92, http://www.eliminatedengue.com/faqs/index/type/aedes-aegypti
Karim MN, Munshi SU, Anwar N, Alam MS (2012) Climatic factors influencing dengue cases in Dhaka City: a model for dengue prediction. Indian J Med Res 136(1):32–39
Napier M (2003) Application of GIS and modeling of dengue risk areas in the Hawaiian Islands In: Proceedings of the 30th symposium for remote sensing of environment: information for risk management and sustainable development, International symposium on remote sensing of environment, Tucon, AZ, 260–263
Sharma RC, Sharma A, Mathur AC (2002) Forecasting of malaria: a challenge yet to be met. In: Sharma A (ed) Epidemiology, health and population. B.R. Publishing Corporation, Delhi, 209–211
Acknowledgement
The authors are extremely thankful for helping in procuring the data and their suggestions on the paper to Dr. D. N. Singh (Commissioner, MCD) and Dr. N. K. Yadav (Municipal Health Officer, Municipal Corporation of Delhi).
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2016 Springer International Publishing Switzerland
About this chapter
Cite this chapter
Akhtar, R., Gupta, P.T., Srivastava, A.K. (2016). Urbanization, Urban Heat Island Effects and Dengue Outbreak in Delhi. In: Akhtar, R. (eds) Climate Change and Human Health Scenario in South and Southeast Asia. Advances in Asian Human-Environmental Research. Springer, Cham. https://doi.org/10.1007/978-3-319-23684-1_7
Download citation
DOI: https://doi.org/10.1007/978-3-319-23684-1_7
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-23683-4
Online ISBN: 978-3-319-23684-1
eBook Packages: Earth and Environmental ScienceEarth and Environmental Science (R0)