
Abstract
Tooth loss is a very important phenomenon which affects both oral and systemic health. It may impair the functional stability of the stomatognathic system. The aftereffects of tooth loss show individual differences which depend on local and systemic factors. Number and location of the missing teeth, occlusal relationships, the periodontal status of the remaining teeth, and movement pattern or size of the tongue can be considered as local factors. Neuromuscular control mechanism, age, psychological status, and general resistance can be accepted as systemic factors. Dentists should be aware of the possible consequences or concomitant conditions of tooth loss and inform their patient or refer them to a physician when necessary. It is also vital to know which dentition and/or patient is at a greater risk due to tooth loss and to decide the treatment plan in the light of these facts.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others



Keywords
1 Definitions
- Combination syndrome:
-
The characteristic features that occur when an edentulous maxilla is opposed by natural mandibular anterior teeth, including loss of bone from the anterior portion of the maxillary ridge, overgrowth of the tuberosities, papillary hyperplasia of the hard palate’s mucosa, extrusion of the lower anterior teeth, and loss of alveolar bone and ridge height beneath the mandibular removable dental prosthesis bases—also called anterior hyperfunction syndrome
- Residual ridge:
-
The portion of the residual bone and its soft tissue covering that remains after the removal of teeth
- Residual ridge resorption:
-
A term used for the diminishing quantity and quality of the residual ridge after teeth are removed
- Supraeruption:
-
Movement of a tooth or teeth above the normal occlusal plane
Tooth loss is a very important phenomenon which affects both oral and systemic health. Dentists should be aware of the possible consequences or concomitant conditions of tooth loss and inform their patient or refer them to a physician when necessary. It is also vital to know which dentition and/or patient is at a greater risk due to tooth loss and to decide the treatment plan in the light of these facts.
Dentition is completed by the eruption of the second molars. Thus occlusion is achieved by the existence of 28 teeth. The absence of one or more third molars has been observed in approximately 25 % of the population.
For the most part, posterior tooth loss is observed more than anterior tooth loss and upper teeth are lost before lower teeth. Initially, the first molars are commonly lost. Afterwards, second molars, second premolars, and first premolars may follow. Posterior tooth loss generally occurs bilaterally.
Tooth loss may impair the functional stability of the stomatognathic system. The aftereffects of tooth loss show individual differences, which depend on local and systemic factors. Number and location of the missing teeth, occlusal relationships, the periodontal status of the remaining teeth, and movement pattern or size of the tongue can be considered as local factors. Neuromuscular control mechanism, age, psychological status, and general resistance can be accepted as systemic factors. Thus, it has been concluded that it is not possible to predict the identical consequences of tooth loss for every patient, and it should be noted that every partial edentulism does not have to be treated immediately (see Chap. 5).
2 Consequences of Tooth Loss
In spite of the individual differences, one or more following consequences that might affect the oral and systemic health can be observed after tooth loss:
-
1.
Alveolar residual bone loss is the main result of tooth loss (Fig. 2.1a, b) and occurs rapidly in the first 3–6 months after the extraction; however, it continues throughout the life at a slower rate. Various results from studies have shown that horizontal bone loss (average 3.87 mm) was more than vertical bone loss (average 1.67 mm). Both horizontal and vertical bone loss have mainly been observed at the buccal part of the residual ridge which becomes narrower and shorter after the resorption process. Therefore, the alveolar ridge is relocated in a more posterior position. Relocation of the ridge is more noticeable in the maxilla, necessitating more lip and cheek support in the buccal region.
Fig. 2.1 
(a, b) Tooth loss results in alveolar bone loss showing individual differences. Preserving of teeth is vital to protect the residual bone (a), and severe bone loss (b) can be prevented or slowed down by saving the teeth as long as possible with different prosthodontic treatment alternatives
-
2.
Migration of the teeth in the form of tipping, extrusion, and rotation may occur, especially after the first year of the extraction. It has been demonstrated that supraeruption occurred in most of the unopposed teeth, usually resulting in periodontal attachment reduction, and is mostly observed in the upper arch (Fig. 2.2a, b). Supraeruption can be divided into active eruption (in which the tooth erupts out of its socket while the periodontium remains stable as seen in Fig. 2.2) and growth of the periodontium (growth in an occlusal direction of the periodontal tissues including the alveolar bone, together with the tooth as seen in Fig. 2.3a, b). The teeth adjacent to the extraction site have a tendency to tip towards this side. While rotation of teeth mesial to the edentulous site has been more observed in the mandible, rotation of teeth distal to the edentulous ridge is greater in the maxilla.
Fig. 2.2 
(a, b) Active eruption in maxillary first molar
Fig. 2.3 
(a, b) In some cases, supraeruption of the teeth occurs accompanied by the growth of the periodontal tissues and alveolar bone
This shift may continue until the tooth encounters an obstacle (such as other teeth or the residual ridge) and a new occlusal balance may develop. After the migration of the teeth, premature contacts and interferences may occur. Thus, pseudoprognathism and retruded contact position interferences (Fig. 2.4a, b) may develop or a pathway may be created by wearing between the opposite teeth (Fig. 2.5a–c). Further changes that could affect oral health may develop, such as traumatic occlusion, root and furcation exposure, soft tissue trauma, plaque retention, and loss of proximal contacts resulting in food impaction.
Fig. 2.4 
(a, b) After tooth loss, migrated teeth may cause premature contacts and interferences
Fig. 2.5 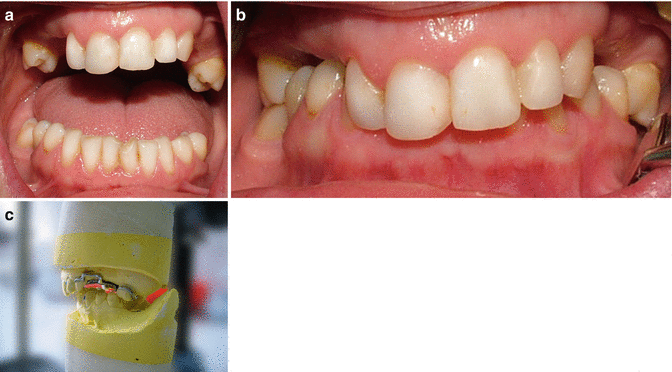
(a–c) After 11 years of the partial edentulism without any prosthetic treatment, patient is closing her mouth on a pathway formed by wearing on the second premolar
There is no consensus regarding the negative effects of occlusal interferences on the stomatognathic system. Furthermore, it should be noted that the relationship between tooth loss or occlusal factors and temporomandibular disorders is controversial (see Chap. 21).
-
3.
Enlargement of the tuberosities may be observed. When mandibular molars are lost, maxillary teeth may extrude together with the alveolar process, and as a consequence, excessive fibrous connective tissue may occur. If this tissue cannot be reduced surgically in the post-extraction phase, it may result in contact with the retromolar pad, inappropriate occlusal plane, and/or lack of space for denture material (Fig. 2.6a, b). Although it is not observed in all cases, overgrowth of the tuberosities can also be observed in cases which have only anterior mandibular teeth and a maxillary complete denture. Additionally, it has been revealed that these patients are at risk of the formation of hypermobile tissue in the anterior maxillary jaw region (Fig. 2.7a, b). These processes were explained by Kelly as two symptoms of the “combination syndrome.”
Fig. 2.6 
(a, b) Overgrown tuberosity may contact with the retromolar pad leaving no space for a prosthetic restoration
Fig. 2.7 
(a, b) In cases having anterior mandibular teeth and maxillary complete denture, hypermobile tissue in the anterior region of the maxilla may be more likely to develop
-
4.
Loss or decrease of occlusal vertical dimension may develop. Alterations of occlusal vertical dimension may occur due to loss of tooth contacts, displacement of the teeth, and uncompensated tooth wear (see Chap. 22).
-
5.
When all posterior occlusal units have been lost, overloading of the anterior tooth region may occur (Fig. 2.8).
Fig. 2.8 
Posterior tooth loss may result in overloading of the anterior tooth. This situation may be further exacerbated by the presence of periodontal problems
-
6.
Masticatory function may be impaired and/or unilateral or anterior chewing may occur, especially in free-end saddle partially edentulous cases. Digestion begins in the mouth, and many nutrients need chewing before swallowing. Patients with impaired dentition may encounter nutritional problems which may lead to systemic disorders and psychosocial difficulties. It has been revealed that the chewing ability is significantly impaired when more than 7 teeth are missing and chewing ability is satisfactory with 20 or more teeth, especially if the teeth are well positioned as in the premolar dental arch. As a result, numbers and types of occluding pairs of teeth are important to evaluate masticatory function (shortened dental arch—see Chap. 5). In cases having large or bilaterally tooth-bound edentulous areas, masticatory function may also be disturbed. Although these cases may be able to chew with most of the remaining occlusal contacts, they may need longer chewing time and swallow larger particles, which may lead to digestive problems, and this may cause them to prefer easy-to-chew food items.
-
7.
Especially in the absence of anterior teeth and maxillary premolars, esthetics, speech, and physiognomy are affected (Fig. 2.9a, b). Psychosocial problems (such as loss of self-esteem and self-confidence) and disorders may develop. It has been shown that adults with depression and anxiety were more likely to have tooth loss. In other words, adults with depression, either in the long term or short term, were significantly more likely to have had at least one tooth removed than those without these disorders.
Fig. 2.9 
(a, b) Loss of teeth can also cause psychological problems in addition to functional problems
-
8.
Loss of teeth may cause and/or increase risk of several systemic diseases:
-
(a)
As patients with impaired dentition tend to eat soft food and avoid vegetables or fruit which are hard, they have a higher risk of obesity. This may result in increased gastrointestinal disorders, high cholesterol levels, cardiovascular diseases, and noninsulin-dependent diabetes mellitus. A recent study also showed that the number of natural teeth is inversely associated to the presence of metabolic syndrome in adults.
-
(b)
It has been demonstrated that tooth loss increases the risk of electrocardiographic abnormalities, hypertension, heart failure, ischemic heart disease, stroke, and aortic valve sclerosis. It has been revealed that both men and women with 1–10 teeth had a significantly higher risk of coronary heart disease compared to subjects with 25–32 teeth. Furthermore, a similar study has showed that a sevenfold increased risk for mortality from coronary heart disease has been observed in subjects with less than 10 teeth compared to subjects with more than 25 teeth.
-
(c)
It has been shown that tooth loss may increase the proportion of gastrointestinal disorders, such as chronic inflammatory changes of the gastric mucosa, upper gastrointestinal and pancreatic cancer, and peptic or duodenal ulcers.
-
(d)
The results of a study showed a significant positive correlation between tooth loss and orodigestive cancer mortality risk, but a causal relationship has not been determined yet.
-
(e)
It has been shown that periodontal disease may result in tooth loss, and this may increase the risk of chronic kidney disease.
-
(f)
Missing teeth may affect the daily functions, physical activity, and quality of life. It has been shown that the above factors are affected by number, location, and distribution of missing teeth. It has been revealed that the number of occluding pairs is an important factor for oral health quality of life and having less than 20 teeth increases the prevalence of negative impacts. It has also been shown that having nine and fewer teeth had a significant effect on the physical index of general health-related quality of life. Furthermore, it has been found that reduced dentition, if not treated with a removable or fixed denture, reduces the physical index of quality of life to the same level as cancer or renal diseases.
-
(a)









Bibliography
Abnet CC, Qiao YI, Dawsey SM, Dong W, Taylor PR, Mark SD. Tooth loss is associated with increased risk of total death and death from upper gastrointestinal cancer, heart disease, and stroke in Chinese population-based cohort. Int J Epidemiol. 2005;34:367–74.
Abt E, Carr AB, Worthington HV. Interventions for replacing missing teeth: partially absent dentition (Review). Cochrane Database Syst Rev. 2012;2:1–52.
Agerberg G, Carlsson GE. Chewing ability in relation to dental and general health. Acta Odontol Scand. 1981;39:147–53.
Ansai T, Takata Y, Yoshida A, Soh I, Awano S, Hamasaki T, Sogame A, Shimada N. Association between tooth loss and orodigestive cancer mortality in an 80-year-old community-dwelling Japanese population: a 12-year prospective study. BMC Public Health. 2013;13:814.
Badr SE, Unger JW. Some treatment alternatives for dealing with the enlarged maxillary tuberosity. Quintessence Int. 1987;18:465–8.
Cleary TJ, Hutton JE. An assessment of the association between functional edentulism, obesity, and NIDDM. Diabetes Care. 1995;18:1007–9.
Compagnon D, Woda A. Supraeruption of the unopposed maxillary first molar. J Prosthet Dent. 1991;66:29–34.
Craddock HL, Youngson CC, Manogue M, Blance A. Occlusal changes following posterior tooth loss in adults. Part 1: a study of clinical parameters associated with the extend and type of supraeruption in unopposed posterior teeth. J Prosthodont. 2007a;16:485–94.
Craddock HL, Youngson CC, Manogue M, Blance A. Occlusal changes following posterior tooth loss in adults. Part 2. Clinical parameters associated with movement of teeth adjacent to the site of posterior tooth loss. J Prosthodont. 2007b;16:495–501.
Craddock HL. Occlusal changes following posterior tooth loss in adults. Part 3. A study of clinical parameters associated with the presence of occlusal interferences following posterior tooth loss. J Prosthodont. 2008;17:25–30.
Emami E, de Souza RF, Kabawat M, Feine JS. The impact of edentulism on oral and general health. Int J Dent. 2013;2013:498305.
Fisher MA, Taylor GW, Shelton BJ, Jamerson KA, Rahman M, Ojo AO, Sehgal AR. Periodontal disease and other nontraditional risk factors for CKD. Am J Kidney Dis. 2008;51:45–52.
Gerritsen AE, Allen PF, Witter DJ, Bronkhorst EM, Creugers NH. Tooth loss and oral health-related quality of life: a systematic review and meta-analysis. Health Qual Life Outcomes. 2010;8:126.
Holmlund A, Holm G, Lind L. Number of teeth as a predictor of cardiovascular mortality in a cohort of 7,674 subjects followed for 12 years. J Periodontol. 2010;81:870–6.
Hung HC, Joshipura KJ, Colditz G, Manson JE, Rimm EB, Speizer FE, Willett WC. The association between tooth loss and coronary heart disease in men and women. J Public Health Dent. 2004;64:209–15.
Hung HC, Joshipura KJ, Colditz G. The association between tooth loss and the self-reported intake of selected CVD-related nutrients and foods among US women. Community Dent Oral Epidemiol. 2005;33:167–73.
Käyser AF. Teeth, tooth loss and prosthetic appliances. In: Öwall B, Käyser AF, Carlsson GE, editors. Prosthodontics. Barcelona: Mosby; 1996.
Kelly E. Changes caused by a mandibular removable partial denture opposing a maxillary complete denture. J Prosthet Dent. 1972;27:140–50.
Mack F, Schwahn C, Feine JS, Mundt T, Bernhardt O, John U, Kocher PT, Biffar R. The impact of tooth loss on general health related to quality of life among elderly Pomeranians: results from the study of health in Pomerania (SHIP-O). Int J Prosthodont. 2005;18:414–9.
Naka O, Anastassiadou V, Pissiotis A. Association between functional tooth units and chewing ability in older adults: a systematic review. Gerodontology. 2014;31:166–77.
Okoro CA, Balluz LS, Eke PI, Ajani UA, Strine TW, Town M, Mensah GA, Mokdad AH. Tooth loss and heart disease: findings from the Behavioral Risk Factor Surveillance System. Am J Prev Med. 2005;29:50–6.
Okoro CA, Strine TW, Eke PI, Dhingra SS, Balluz LS. The association between depression and anxiety and use of oral health services and tooth loss. Community Dent Oral Epidemiol. 2012;40:134–44.
Österberg T, Dey DK, Sundh V, Carlsson GE, Jansson JO, Mellström D. Edentulism associated with obesity: a study of four national surveys of 16 416 Swedes aged 55–84 years. Acta Odontol Scand. 2010;68:360–7.
Stolzenberg-Solomon RZ, Dodd KW, Blaser MJ, Virtamo J, Taylor PR, Albanes D. Tooth loss, pancreatic cancer, and Helicobacter pylori. Am J Clin Nutr. 2003;78:176–81.
Sülün T, Şakar O, Bilhan H, İspirgil E. The effect of mandibular anterior teeth on the hypermobile tissue in the anterior part of the maxilla. Arch Gerontol Geriatr. 2012;55:12–5.
Takata Y, Ansai T, Matsumura K, Awano S, Hamasaki T, Sonoki K, Kusaba A, Akifusa S, Takehara T. Relationship between tooth loss and electrocardiographic abnormalities in octogenarians. J Dent Res. 2001;80:1648–52.
Tan WL, Wong TLT, Wong MCM, Lang NP. A systematic review of postextractional alveolar hard and soft tissue dimensional changes in humans. Clin Oral Implants Res. 2012;23 suppl 5:1–21.
The glossary of prosthetic terms. J Prosthet Dent. 2005;94:10–92.
Van der Weijden F, Dell’Acqua F, Slot DE. Alveolar bone dimensional changes of post-extraction sockets in humans: a systematic review. J Clin Periodontol. 2009;36:1048–58.
Völzke H, Schwahn C, Hummel A, Wolff B, Kleine V, Robinson DM, Dahm JB, Felix SB, John U, Kocher T. Tooth loss is independently associated with the risk of acquired aortic valve sclerosis. Am Heart J. 2005;150:1198–203.
Zhu Y, Hollis JH. Associations between the number of natural teeth and metabolic syndrome in adults. J Clin Periodontol. 2015;42:113–20.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2016 Springer International Publishing Switzerland
About this chapter
Cite this chapter
Şakar, O. (2016). The Effects of Partial Edentulism on the Stomatognathic System and General Health. In: Şakar, O. (eds) Removable Partial Dentures. Springer, Cham. https://doi.org/10.1007/978-3-319-20556-4_2
Download citation
DOI: https://doi.org/10.1007/978-3-319-20556-4_2
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-20555-7
Online ISBN: 978-3-319-20556-4
eBook Packages: MedicineMedicine (R0)