
Abstract
On the WHO’s ranking of causes of disability, headache disorders is listed among the 10 most disabling conditions for the two genders, and into the five most disabling for women. But despite being the most common neurological symptom, the diagnosis and treatment approaches for headache disorders are not globally established and their burden of disease is underestimated.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others

Keywords
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
2.1 Introduction
On the WHO’s ranking of causes of disability, headache disorders is listed among the 10 most disabling conditions for the two genders, and into the five most disabling for women. But despite being the most common neurological symptom, the diagnosis and treatment approaches for headache disorders are not globally established and their burden of disease is underestimated.
Epidemiology is defined as “the study of distribution and determinants of disease frequency in human populations” [1]. Epidemiological studies in headache disorders are mainly performed for evaluating the prevalence and incidence and determining the burden of disease to raise awareness for this common health problem [2]. “Prevalence” answers the question “how common a disease is?” and is expressed by the proportion of a given population that has a disease over a defined period of time. “Incidence” is a measure of the probability of occurrence of a given medical condition in a population within a specified period of time. “Incidence proportion” is the number of new cases within a specified time period divided by the size of the population initially at risk [3]. The other aims of epidemiological studies are to examine the sociodemographic, familial, and environmental risk factors, which may help to identify high-risk groups for headache and provide a better understanding on the pathogenesis of disease and improve treatment strategies [4].
Due to methodological issues, many papers regarding epidemiological studies show discrepancies. The main challenge in all studies is that the diagnosis depends on subjective experiences rather than standard criteria. To eliminate these differences, International Headache Society (IHS) has published criteria of headache disorders subtypes firstly in 1988, revised in 2004, and recently, preliminary form named as beta was published in 2013 [5–7]. The International Classification of Headache Disorders, 2nd edition (ICHD-II) and The International Classification of Headache Disorders, 3rd edition (beta version) have provided improved definitions to reduce problems in methodological studies. However, personal interview and neurological examination are still the “gold standards” used in headache epidemiology studies. This methodology, which provides an improved clinical headache diagnosis is difficult to carry out, as they should involve large populations, which in turn requires a high cost. Therefore, such studies have been carried out only in a limited number of studies [8]. Another and probably more important issue is the lack of diagnostic biomarkers or other study tools that may provide an accurate diagnosis of primary headaches!
Headache prevalence usually corresponds to the sum of “primary headaches,” mainly of migraine and tension-type headache prevalence. The overall headache prevalence rates in one year vary between 29 and 77 % in adults, which is more frequent in women (40–83 % vs. 19–69 %). Lifetime prevalence was found 35–96 % in European countries. As a summary of six European studies, it showed 50.5 % headache prevalence in one year, which is more common in women (57.6 vs. 41 %) [9].
2.2 Epidemiology of Migraine
2.2.1 Incidence of Migraine
Although there are a large number of migraine prevalence studies, the incidence studies are limited. The high variability of incidence rates among age groups and some migraine definition-related issues have resulted in having only a few reliable, large population-based incidence studies in migraine. In order to obtain exact incidence rates in migraine, large cohorts need to be followed in long periods.
Incidence studies show significant differences, which may be explained by various study populations and methodology. A population-based study using estimated onset age of migraine was conducted by Stewart et al. in 1991. Telephone interviews were done randomly with 10,619 participants between ages 12 and 29. Three hundred and ninety-two men and 1018 women with migraine were evaluated. Onset age for migraine with aura peaked between ages 12 and 13 (adjusted incidence rate: 14.1/1000) and migraine without aura between 14 and 17 years among females. Incidence of migraine with aura peaked in 5 years (6.6/1000) and without aura between 10 and 11 years (adjusted incidence rate: 10/1000) in men. They emphasized that the incidence rate of migraine with aura peaks 3–5 years earlier than migraine without aura. One of the limitation study was the lack of the participants older than 30 [10].
In 1996, Breslau et al. conducted a prospective study in migraine. The cohort comprised 1007 individuals between 21 and 30 ages. Follow-up interviews were carried out at 3.5 and 5.5 years later in 972 patients. At the end of the study, the cumulative incidence of migraine was estimated to be 8.4 % (71/848). The rate of incidence was 6 per 1000 person-years for men, and 24 per 1000 person-years for women. The major limitation of the study was the narrow age group of the study population [11].
The Danish 12-year follow-up incidence study, which was conducted by Lyngberg in 2005, showed similar results with Breslau et al. The annual incidence rate was 8.1/1000 person-years, with a male-to-female ratio of 1:6. The study population was between 25 and 64 ages and incidence rates were higher in the 25–34 years group and decreased markedly by age in both genders afterward (25–34 years: 13.8/1000; 35–44 years: 7.0/1000; 45–54 years: 6.7/1000; 55–64 years: 2.6/1000). Young age, female gender, no vocational education, familial disposition, a high workload, and having frequent tension-type headaches were found to be risk factors for developing migraine. Forty percent of migraine patients described aura [12].
A follow-up study regarding the incidence of migraine was conducted in 2008 by Stewart et al. Cumulative lifetime migraine incidence in women and men was assessed. Data was obtained from the American Migraine Prevalence and Prevention study, in which a mailed survey was sent to 120,000 US households. Cumulative incidence of 43 % was found in women and 18 % in men by age 85. Median age of onset was 25 years among women and 24 years among men [13].
In a Turkish incidence study using ICHD-II criteria, which was conducted by Ertas et al., 2563 people who did not have migraine in the original Turkish Headache Epidemiology study [14] were reached by a headache specialist through a telephone interview after 5 years. This study has shown a yearly incidence of 2.38 % (females 2.98 %; males 1.93 %) (Ertas et al., poster presentation at the American Headache Association Meeting, San Diego, 2014).
2.2.2 Prevalence of Migraine
Prevalence studies in migraine are numerous. However, different results were found among studies because of variations in case definitions and demographic features of the study groups.
The range of migraine prevalence varies between 3 and 35 % in these studies. Results in European countries and North America show similarities. Most studies in the adult population give rates of 5–9 % for men and 12–25 % for women. Stovner and Andree published a review paper in 2010 as a part of the Eurolight projects, including all headache prevalence studies until 2009. The prevalence of migraine in adults was found to be 14.7 % (8 % in man and 17.6 % in woman) in more than 170,000 participants [15].
The first comprehensive migraine prevalence study in the United States was conducted by The American Migraine Study group in 1989 using a case definition based on the International Headache Society (IHS) criteria [4, 5]. Migraine prevalence was found to be 18 % for women and 6 % for men varying with age (highest in the 35–45 years range), household income (highest in lowest income), and race (highest in whites than in blacks) [16]. Ten years after the first study, The American Migraine Study II was conducted. The one-year prevalence of migraine was found 18.2 % among females and 6.5 % among males, which was similar to the reported results in the first study [4, 16]. The prevalence of migraine in the United States remained constant from the American Migraine Study I to the American Migraine Study II, which were conducted 10 years apart [4, 16]. However, according to the US Centers for Disease Control, the self-reported migraine prevalence in the United States increased by 60 %, from 25.8 per 1000 person-years to 41 per 1000 person-years between 1981 and 1989 [17].
The Turkish primary headache prevalence studies showed similar results with other reported studies. The migraine prevalence rates in 1998, 2008, and 2013, were 16.4 %, 16.4 %, and 16.7 %, respectively [14]. The frequency of migraine in females was almost three times higher than men.
In the Turkish Headache epidemiology 5-year follow-up study, 10.2 % of participants without a primary headache in 2008 were diagnosed as having definite migraine in 2013. Interestingly, 14.7 % of definite TTH, their diagnosis changed to definite migraine 5 years later (Ertas et al., in preparation).
In children within 36,000 participants, the migraine prevalence was 9.2 % (5.2 % for boys, 9.1 % for girls) [15]. Migraine prevalence in children ranges from 3.2 to 14.5 % in other studies. One of the main reasons of difference among studies is the use of various definitions of migraine in pediatric population. Of note, 60–77.5 % of children with migraine report family history, which shows higher frequency than adults and the debate is still going on to put family history in the criteria of pediatric migraine to better distinguish from TTH [18].
A large epidemiological study among 5562 children between ages 8 and 16 was conducted by Ozge et al. in Mersin, a Mediterranean city of Turkey. The migraine prevalence was found to be 10.4 % with a similar distribution in both genders (52.6 % were girls; 47.4 % were boys) and emphasized that “severity of pain” was the most sensitive headache characteristic for migraine [19]. Interestingly, when this population was restudied 6 years later, the prevalence of migraine increased to 18.6 % and episodic-TTH prevalence increased from 22.6 to 57.5 %, respectively [20].
2.2.3 Age, Gender, Genetics, and Environmental Factors in Migraine
Migraine prevalence rates vary by age and gender. Migraine prevalence is more common in boys than in girls before puberty and the prevalence ratio inverses in favor of girls following puberty. In women, prevalence increases throughout childhood and in early adult life until approximately age of 40, after which it declines [17]. Prevalence is highest between ages 25 and 55, and more specifically between ages 35 and 45, which corresponds to the peak productivity years of men and women. These findings emphasize the magnitude of the burden of migraine in economic productivity [21].
Although genetics in migraine is complex and multifactorial, prevalence studies showed significant increase among the first-degree relatives of migraine patients. Russell et al. reported a 1.9-fold increased risk in first-degree relatives and 1.5 in the spouses of migraineurs without aura, which indicates the importance of both genetic and environmental factors in migraine without aura. In contrast to migraine without aura, the risk was 3.8 in first-degree relatives and no risk for spouses in migraine with aura, which highlights the major role of genetic factors in migraine with aura [22]. Twin studies also support the contribution of genetic factors on migraine [23, 24]. Migraine may also be a part of the clinical symptomatology of some genetic disorders, such as CADASIL (cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy), MELAS (mitochondrial encephalomyopathy, lactic acidosis, stroke-like episodes), RVCL (retinal vasculopathy and cerebral leukodystrophy), COL4A1 (retinal arteriolar tortuosity and leukoencephalopathy), and FASPS (familial anticipated sleep phase syndrome).
In addition to the above genetic disorders with migraine features, autosomal dominant transmission of the ion transportation genes CACNA1A, ATP1A2, and SCN1A can cause the familial hemiplegic migraine (FHM). Overlap of idiopathic migraine and FHM more than a chance may support the common pathway among two disorders [25]. Consequently, after the evaluation of both family and twin studies, approximately 50 % of patients have a first-degree relative affected from migraine. However, whether in these genetic disorders, having a headache with migrainous features should be accepted as this headache being “migraine” and therefore related to a common migraine gene needs to be further evaluated!
Due to limited studies, the effect of race in headache is still controversial. American Migraine Study I-II and the AMPP, which are the largest population-based studies revealed similar migraine prevalence among Blacks and Whites and Baltimore County Study also did not show significant prevalence differences among races (Whites 29 %, Blacks 23.4 %) [4, 15, 26].
ARIC (Atherosclerosis Risk in Communities) study was mainly designed to estimate the lifetime course of atherosclerosis in the US population. However, at the third clinic examination, they intended to determine the lifetime prevalence of migraine and other headaches lasting than 4 h. When we compare the differences among races in this study, the age-adjusted prevalence of migraine without aura was highest in white women (4.5 %), followed by African American women (2.0 %), white man (1.1 %), and African American men (0.5 %). The rate of migraine without aura was also common in white women (9.0 %) than other groups (white men 2.7 %, African American women 2.2 %, African American men 0.5 %) [27].
In the National Health Interview Survey (NHIS), which was conducted by the National Center for Health Statistics, overall prevalence was estimated as 14.3 % in Whites, 14.0 % in Blacks, 9.2 % in Asians, 12.9 % in Hispanics, 11.9 % in Mexican Americans, and 17.7 % in Native Americans [28].
When we evaluate all studies regarding the migraine prevalence among races in the United States, all of the prevalence studies except ARIC showed similar ratios in both races.
Geographic diversity is another controversial issue regarding the headache epidemiology. The prevalence of migraine is higher in European and North American studies and slightly lower in Asia. In Asia, the estimated one-year prevalence of primary headache disorders was 9.1 % for migraine, 16.2 % for TTH, and 2.9 % for CDH [29].
In contrast to other continents reports, African studies show very low frequency, which may support the effect of environmental factors on migraine. In a review of 21 community-based studies, including 137,277 people, migraine prevalence was found to be 5.61 % in the general population [30]. A recent study that was conducted in Enugu, the southeast part of Nigeria the prevalence of migraine and TTH were 6.4 % and 13.8%, respectively [31]. Further well-designed studies must be carried out in Africa to reveal the prevalence and impact of headache.
2.2.4 Chronification of Migraine
Chronification of migraine is one the major issues that affects the quality of life and causes lower productivity in patients. Chronic migraine was not recognized as a distinct entity in ICHD-I and later as an emerging concept, it was subclassified as a complication of migraine in ICHD-II. Finally, in ICHD, 3rd edition (beta version) chronic migraine was added as a distinct disorder to reduce the underestimation of such a disabling disorder and to create awareness for new treatment strategies.
Chronic migraine, which is defined as at least 15 days (more than 4 h/day) of headache each month, including at least eight of these days, the headache having migrainous features in the ICHD 3rd edition (beta version). It was shown that 2.5–3.0 % of people with episodic migraine will transform to chronic migraine every year [32]. High frequency of headaches at baseline, medication overuse, obesity, sleep disorders, excessive caffeine intake, psychiatric comorbidities, female sex, lower socioeconomic status, comorbid pain disorders, history of head or neck injury, and presence of cutaneous allodynia are the risk factors for chronification [32]. However, in 2 years, 26 % of these patients with chronic migraine, also will remit back to episodic migraine [33].
According to 12 reported studies regarding chronic migraine, the overall prevalence of CM ranges from 0 to 5.1 % [34]. The major reason of various results among studies was the usage of different criteria for CM. The largest study, which was conducted by Buse et al. in the US population, the prevalence of CM was found to be 0.91 % (1.29 % of females and 0.48 % of males) and the prevalence increased throughout adolescence, peaked in midlife, and declined after age 50 in both genders. The proportion of CM among all migraine patients was 7.68 % in this study (7.45 % – among females with migraine; 8.47 % – among males with migraine [35].
In The Turkish primary headache prevalence study, the prevalence of chronic migraine was found to be 1.7 %. Three-fourths of CM patients reported medication overuse. CM was seen in 10.7 % of the migraineurs [14].
2.3 Tension-type Headache (TTH)
There are relatively few studies regarding the epidemiology of tension-type headache (TTH) in comparison with migraine. Most of the studies show different results probably due to methodological differences including case definition and demographic factors. The first study with episodic TTH prevalence using IHS criteria was conducted in Denmark. One thousand men and women aged 25–64 years were randomly drawn from the Danish National Central Person Registry and invited for a general health examination, and 740 people participated in the study. The lifetime prevalence of TTH was 69 % in men and 88 % in women. Prevalence of TTH in the previous year was 63 % in man and 86 % in woman. They also reported increased prevalence by age [8].
The second large-scale population study was carried out in the United States by collecting data through a telephone interview. The one-year prevalence rate was found to be 38.3 %, which is lower than the Danish study. The prevalence of episodic TTH peaked in fourth decade and decreased afterward [36].
Stovner et al. evaluated 107 publications consistent with headache epidemiology. In this study, the adult population with tension-type headache (TTH) was found to be 42 %. Headache in general is most prevalent in the youngest age group whereas TTH is most prevalent in adolescents. This is probably due to few studies of TTH among children. TTH appears to be much more common in Europe (80 %) than in Asia or the Americas (20–30 %). The headache-related disability of tension-type headache was larger than migraine because of higher prevalence [37].
According to published 19 reports, Stovner and Andree estimated that the prevalence of TTH was 62.6 % among >66,000 adults. In children and young adolescent group, the estimated prevalence was lower at 15.9 % among 25,000 children [15].
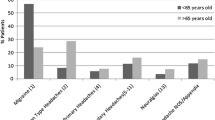
In contrast to other published reports, in Turkish study the rate of TTH was very low (14.5 %; with probable TTH being 9.5 % and definite TTH being 5 %). The significant difference in comparison to other studies may be explained by some probable methodological issues. In the Turkish study, a diagnosis of TTH was made only if participants were not diagnosed with “definite” or “probable” migraine and fulfilled all TTH criteria. This could have been caused by overlapping the groups of probable TTH and probable migraine. One other issue to be considered is that “true” TTH is likely to be less than all cases diagnosed with TTH, as most of them would turn out to be not primary, but having headaches secondary to somatization or other psychogenic causes, or due to head-neck postural changes. Such an approach would be more selective and detect lower rates of TTH [14]. This issue is discussed in more details elsewhere [38] (Table 2.1).
2.4 Chronic Daily Headache (CDH)
The definition of chronic headache still remains controversial. There is no agreement on how many days per month the headache must be present, the obligatory time from initiation of headache and the type of headache. Although a lot of studies have been done, only two of them used the same criteria.
Global prevalence of CDH was found in 3 %. CDH is less prevalent among children and adolescents. It is more common in Central/South America (5 %) than Africa (1.7 %). Medication-overuse headache (MOH), a potentially treatable and preventable headache type, is common among those with CDH. Possible MOH was found to occur in about 1 % [15].
In the Turkish study, chronic daily headache was found to be 3.3 %, of which 1.8 % had a diagnosis of chronic migraine (0.4 % for those without medication overuse and 1.3 % for those with medication overuse) and 0.2 % for chronic TTH.
2.5 Trigeminal Autonomic Cephalalgias
Trigeminal autonomic cephalalgias consists of cluster headache (CH), paroxysmal hemicrania (PH), short-lasting unilateral neuralgiform headache attacks with conjunctival injection and tearing (SUNCT)/short lasting neuralgiform headache attacks with cranial autonomic features (SUNA), and hemicrania continua (HC).
Because of the low frequency of TACs, there are few available data on epidemiology.
In the Vågå study, 1838 people between 18 and 65 years were studied; two were diagnosed as having SUNCT and in 18 individuals (11 females and 7 males), the symptoms were consistent with hemicrania continua. For paroxysmal hemicrania, the one-year prevalence rate was estimated to be 0.5 per 1000 [46].
Epidemiological studies with CH are more common than the other TACs. Vågå study is the most comprehensive study estimating the prevalence of CH [47].
The study was conducted in Norwegian rural community among 1838 participants by face-to-face interviews. Prevalence of CH was found to be 326 per 100,000 in the total population (106 per 100,000 for females, and 558 per 100,000 for males).
In an Italian study similar to the Norwegian study, the prevalence was found to be 279/100,000 among >10,000 patients [48]. D’Alessandro et al. found the prevalence of CH 69/100,000 in Republic of San Marino [49]. Rasmussen et al. and Monteiro et al. showed similar prevalences (100/100,000) [50, 51]. In Germany, the one-year prevalence of CH was estimated to be 119/100,000 [52]. Ekbom et al. reported the lifetime prevalence and concordance risk of cluster headache in the Swedish twin population in 2006. They found the prevalence as 1 per 500 of the general population [53].
However, when considering the clinical practice, the number of cluster patients seems to be lower than these prevalence studies (personal comment: Rigmor Jensen)
2.6 Impact of Headache
Global Burden of Disease (GBD) Study 2010 revealed that TTH and migraine are, respectively, the second and third most common prevalent diseases after dental caries and migraine is ranked as the seventh highest cause of disability in the world. The main disadvantage of GBD 2010 is the lack of data regarding the interictal impairment in migraine and medication overuse headache [54].
The societal impact of headache consists of direct and indirect costs. Direct costs correspond to the sum of diagnostic investigations and treatment costs. Indirect costs, which include loss of productivity due to absenteeism and reduced performance, are the major leading causes of cost when compared with direct costs of headache. The cost of migraine in Europe is estimated at € 27 billion annually. Although there are many epidemiological studies with the prevalence of headache, migraine, TTH, the data on impact of headache is rare. The most comprehensive study evaluating the impact of headache was conducted by Eurolight project. In this study, personal impact of headache was assessed by seven questions to show headache-attributed lost work, housework, and social days in preceding three months. Eurolight project emphasized that the common headache disorders have very high personal impact [55]. However, much more studies with applicable questionnaires have to be done to indicate the impact of headache, which will provide awareness among physicians.
References
Hennekens CH, Buring JE (1987) Epidemiology in medicine. Lippincott, Williams & Wilkins, Philadelphia
Andlin-Sobocki P, Jönsson B, Wittchen HU et al (2005) Cost of disorders of the brain in Europe. Eur J Neurol 12:1–27
Rothman KJ, Lash TL, Greenland S (2008) Modern epidemiology, 3rd edn. Lippincot Williams & Wilkins, Philadelphia, pp 33–48
Stewart WF, Lipton RB, Celentano DD et al (1992) Prevalence of migraine headache in the United States. Relation to age, income, race, and other sociodemographic factors. JAMA 267(1):64–69
Classification and diagnostic criteria for headache disorders, cranial neuralgias and facial pain. Headache Classification Committee of the International Headache Society (1988) Cephalalgia 8(Suppl 7):1–96
Headache Classification Subcommittee of the International Headache Society (2004) The international classification of headache disorders, 2nd edn. Cephalalgia 24(Suppl 1):1–150
Headache Classification Committee of the International Headache Society (IHS) (2013) The International Classification of Headache Disorders, 3rd edition (beta version). Cephalalgia 33(9):629–808
Rasmussen BK, Jensen R, Schroll M et al (1991) Epidemiology of headache in a general population–a prevalence study. J Clin Epidemiol 44(11):1147–1157
Stovner LJ, Zwart JA, Hagen K et al (2006) Epidemiology of headache in Europe. Eur J Neurol 13(4):333–345
Stewart WF, Linet MS, Celentano DD et al (1991) Age- and sex-specific incidence rates of migraine with and without visual aura. Am J Epidemiol 134(10):1111–1120
Breslau N, Chilcoat HD, Andreski P (1996) Further evidence on the link between migraine and neuroticism. Neurology 47(3):663–667
Lyngberg AC, Rasmussen BK, Jorgensen T et al (2005) Incidence of primary headache: a Danish epidemiologic follow-up study. Am J Epidemiol 161(11):1066–1073
Stewart WF, Wood C, Reed ML et al (2008) Cumulative lifetime migraine incidence in women and men. Cephalalgia 28(11):1170–1178
Ertas M, Baykan B, Orhan EK et al (2012) One-year prevalence and the impact of migraine and tension-type headache in Turkey: a nationwide home-based study in adults. J Headache Pain 13(2):147–157
Stovner LJ, Andree C (2010) Prevalence of headache in Europe: a review for the Eurolight project. J Headache Pain 11(4):289–299
Lipton RB, Stewart WF, Diamond S et al (2001) Prevalence and burden of migraine in the United States: data from the American Migraine Study II. Headache 41(7):646–657
Scher AI, Stewart WF, Lipton RB (1999) Migraine and headache: a meta-analytic approach. In: Crombie IK (ed) Epidemiology of pain. IASP Press, Seattle, pp 159–170
Ozge A, Termine C, Antonaci F et al (2011) Overview of diagnosis and management of paediatric headache. Part I: diagnosis. J Headache Pain 12(1):13–23
Ozge A, Bugdayci R, Saşmaz T et al (2003) The sensitivity and specificity of the case definition criteria in diagnosis of headache: a school-based epidemiological study of 5562 children in Mersin. Cephalalgia 23(2):138–145
Ozge A, Sasmaz T, Cakmak SE et al (2010) Epidemiological-based childhood headache natural history study: after an interval of six years. Cephalalgia 30(6):703–712
Bigal ME, Lipton RB (2009) The epidemiology, burden, and comorbidities of migraine. Neurol Clin 27(2):321–334
Russell MB, Iselius L, Olesen J (1996) Migraine without aura and migraine with aura are inherited disorders. Cephalalgia 16(5):305–309
Ulrich V, Gervil M, Kyvik KO et al (1999) The inheritance of migraine with aura estimated by means of structural equation modelling. J Med Genet 36:225–227
Russell MB, Ulrich V, Gervil M et al (2002) Migraine without aura and migraine with aura are distinct disorders. A population-based twin survey. Headache 42:332–336
Persico AM, Verdecchia M, Pinzone V et al (2015) Migraine genetics: current findings and future lines of research. Neurogenetics 16(2):77–95
Stewart WF, Lipton RB, Liberman J (1996) Variation in migraine prevalence by race. Neurology 47:52–59
Perry Carson AL, Rose KM, Sanford CP et al (2004) Lifetime prevalence of migraine and other headaches lasting 4 or more hours: the Atherosclerosis Risk in Communities (ARIC) study. Headache 44:20–28
National Health Interview Survey website. http://www.cdc.gov/nchs/nhis.htm. Accessed 29 July 2014
Peng KP, Wang SJ (2014) Epidemiology of headache disorders in the Asia-pacific region. Headache 54(4):610–618
Woldeamanuel YW, Andreou AP, Cowan RP (2014) Prevalence of migraine headache and its weight on neurological burden in Africa: a 43-year systematic review and meta-analysis of community-based studies. J Neurol Sci 342(1–2):1–15
Ezeala-Adikaibe BA, Onyekonwu C, Okudo G et al (2014) Prevalence of primary headaches in an urban slum in Enugu South East Nigeria: a door-to-door survey. Headache 54(10):1601–1610
Bigal ME, Serrano D, Buse D et al (2008) Acute migraine medications and evolution from episodic to chronic migraine: a longitudinal population-based study. Headache 48:1157–1168
Manack A, Buse DC, Serrano D et al (2011) Rates, predictors, and consequences of remission from chronic migraine to episodic migraine. Neurology 76(8):711–718
Natoli JL, Manack A, Dean B et al (2010) Global prevalence of chronic migraine: a systematic review. Cephalalgia 30:599–609
Buse DC, Manack AN, Fanning KM et al (2012) Chronic migraine prevalence, disability, and sociodemographic factors: results from the American Migraine Prevalence and Prevention Study. Headache 52:1456–1470
Schwartz BS, Stewart WF, Simon D et al (1998) Epidemiology of tension-type headache. JAMA 279(5):381–383
Stovner LJ, Hagen K, Jensen R et al (2007) The global burden of headache: a documentation of headache prevalence and disability worldwide. Cephalalgia 27(3):193–210
Uygunoglu U, Siva A (2014) Headache attributed to somatization disorders: is it tension-type headache, is it “somatization headache,” or both? In: Siva A, Lampl C (eds) Case-based diagnosis and management of headache disorders. Springer, Cham, pp 259–265
Steiner TJ, Stovner LJ, Katsarava Z et al (2014) The impact of headache in Europe: principal results of the Eurolight project. J Headache Pain 15:31
Mitsikostas DD, Tsaklakidou D, Athanasiadis N et al (1996) The prevalence of headache in Greece: correlations to latitude and climatological factors. Headache 36(3):168–173
Pfaffenrath V, Fendrich K, Vennemann M et al (2009) Regional variations in the prevalence of migraine and tension-type headache applying the new IHS criteria: the German DMKG Headache Study. Cephalalgia 29(1):48–57
Lampl C, Buzath A, Baumhackl U et al (2003) One-year prevalence of migraine in Austria: a nation-wide survey. Cephalalgia 23(4):280–286
Russell MB, Levi N, Saltyte-Benth J et al (2006) Tension type headache in adolescents and adults: a population based study of 33,764 twins. Eur J Epidemiol 21(2):153–160
Matías-Guiu J, Porta-Etessam J, Mateos V et al (2011) One-year prevalence of migraine in Spain: a nationwide population-based survey. Cephalalgia 31(4):463–470
Ayzenberg I, Katsarava Z, Sborowski A et al (2012) The prevalence of primary headache disorders in Russia: a countrywide survey. Cephalalgia 32(5):373–381
Sjaastad O, Bakketeig LS (2007) The rare, unilateral headaches. Vågå study of headache epidemiology. J Headache Pain 8(1):19–27
Sjaastad O, Bakketeig LS (2003) Cluster headache prevalence. Vågå study of headache epidemiology. Cephalalgia 23(7):528–533
Torelli P, Beghi E, Manzoni GC (2005) Cluster headache prevalence in the Italian general population. Neurology 64(3):469–474
D’Alessandro R, Gamerini G, Benassi G et al (1986) Cluster headache in the Republic of San Marino. Cephalalgia 6:159–162
Rasmussen BK (1994) Epidemiology of headache. Thesis, Köbenhavns Universitet, Copenhagen
Pereira Monteiro JM (1995) Cefaleias. Estudo epidemiologico e clinico de uma população urbana. Thesis, Porto
Katsarava Z, Obermann M, Yoon MS et al (2007) Prevalence of cluster headache in a population-based sample in Germany. Cephalalgia 27(9):1014–1019
Ekbom K, Svensson DA, Pedersen NL et al (2006) Lifetime prevalence and concordance risk of cluster headache in the Swedish twin population. Neurology 67(5):798–803
Vos T, Flaxman AD, Naghavi M et al (2012) Years lived with disability (YLDs) for 1160 sequelae of 289 diseases and injuries 1990–2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet 380(9859):2163–2196
Stovner LJ, Andree C, Eurolight Steering Committee (2008) Impact of headache in Europe: a review for the Eurolight project. J Headache Pain 9(3):139–146
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2016 Springer International Publishing Switzerland
About this chapter
Cite this chapter
Uygunoglu, U., Siva, A. (2016). Epidemiology of Headache. In: Mitsikostas, D., Paemeleire, K. (eds) Pharmacological Management of Headaches. Headache. Springer, Cham. https://doi.org/10.1007/978-3-319-19911-5_2
Download citation
DOI: https://doi.org/10.1007/978-3-319-19911-5_2
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-19910-8
Online ISBN: 978-3-319-19911-5
eBook Packages: MedicineMedicine (R0)