
Abstract
Although family-centered interventions are known to be effective at reducing risk behavior and increasing academic success, few schools can deliver these interventions successfully. The Positive Family Support (PFS) program was developed based on multiple research studies on the Family Check-Up that have shown the Family Check-Up to be an efficacious prevention model that reduces the risk of substance use, problem behavior, and achievement difficulties. The PFS program was designed to take the Family Check-Up and associated intervention modules to scale in middle schools. The PFS program was implemented in 41 middle schools randomly assigned to receive the training and support associated with the PFS program or middle school as usual. School staff at each middle school delivered the intervention to youths and families. In this chapter, we summarize the key aspects of the PFS program and our approach to implementation. We discuss challenges we faced in the schools, such as budget cuts, staffing, leadership turnover, school climate issues, and fidelity of implementation. Last, we discuss implications of this work for future research and scale-up of family-centered interventions in schools.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
Students who display problem behaviors at school are at risk for a variety of difficulties, including poor academic achievement, poor school attendance, depression, and substance use (Barry, Lyman, & Grofer Klinger, 2002; Patterson, Reid, & Dishion, 1992), all of which can be challenging for teachers and school administrators to manage (Dishion & Stormshak, 2007; Walker, Colvin, & Ramsey, 1995). Many schools also lack the infrastructure necessary to systematically and effectively support children and adolescents with academic, behavioral, or mental health concerns (Eccles & Harold, 1993; Ringeisen, Henderson, & Hoagwood, 2003). However, schools are an ideal location to implement evidence-based prevention and intervention programs to address problem behaviors because youths spend a considerable amount of time there (Dishion, 2011). The World Health Organization (WHO, 2008) and Centers for Disease Control (CDC, 2013) promote school settings as particularly important for actions that target and improve outcomes for child and adolescent health. Moreover, using schools as service delivery settings may increase opportunities to provide health services to underserved populations, such as rural populations, low-income families, and ethnically diverse youths. As such, local, state, and federal policies have increasingly called for the use of evidence-based practices in school settings.
Although schools have become consistent venues for intervention efforts, research is limited on effective implementation and execution of these programs to high-quality standards. Schools are thus left without effective or efficient plans when they choose to adopt empirically based interventions. Clearly, the unique issues and challenges presented by program scale-up must be addressed.
Implementation of Evidence-Based Practices in School Settings
Little theory or research exists regarding how to implement behavioral and mental health interventions, such as family–school partnership programs, with fidelity (Domitrovich & Greenberg, 2000; Elliott & Mihalic, 2004), yet high-quality implementation is directly linked to strong outcomes and improved effect sizes across intervention models (Durlak & DuPre, 2008). Family-centered treatment models that emphasize parent training and support for families show the largest effects over time in nearly every review of interventions designed to reduce problem behavior and substance use (Kazdin, 2010; Prinz & Dumas, 2004). Despite this overwhelming evidence, a high proportion of children and adolescents never receive treatment for these problems, and a very small percentage of parents participate in parenting or family interventions to address behavior problems (Prinz & Sanders, 2007; Zubrick et al., 1995). Limited access to mental health treatment for children has fueled an increase in the number of school-based mental health programs in the United States. Nevertheless, there are many barriers to implementing the programs effectively (Weist, 2005).
The majority of interventions focus on the individual child or on the school context (e.g., positive behavior support; Horner, Sugai, Todd, & Lewis-Palmer, 2005); few are brief and target known risk factors for substance use, such as family management. They typically consist of a response-to-intervention (RtI) framework that embeds services in a model of universal, selected, and indicated interventions delivered in the school, but they offer little coordination between school and home. This is a serious shortcoming in that the nature of interactions between parents and their child’s school becomes more formalized and less frequent in middle school (Rimm-Kaufman & Pianta, 2000) and leads to less engagement by parents in their child’s overall adjustment, when parenting and family management are critical to school success and healthy adaptation. Data strongly suggest that motivating parents to engage in family management will effect long-term change (Dishion & Kavanagh, 2003; Forgatch, Bullock, & Patterson, 2004; Kazdin, 2002; Stormshak, Fosco, & Dishion, 2010), and research supports the efficacy of interventions for high-risk students in the public school environment that target parenting practices (e.g., Atkins et al., 2008).
Multiple barriers, such as time, money, and competing priorities, limit the ability of schools to implement interventions that involve families (Forman, Olin, Hoagwood, Crowe, & Saka, 2009), making most interventions that target parenting practices unrealistic for schools (Christenson, 2003), despite their proven efficacy. Given the dire economic situation currently facing many school systems, it is imperative to find a cost-effective means of improving student success rates that is efficient and effective, realistic, does not require extensive school staff time to implement with fidelity, and integrates families and family-centered care into school systems.
Literature pertaining to the diffusion, implementation, and sustainability of school-based interventions is sparse and leaves schools with little strategic support regarding the use of evidence-based programs (Feldstein & Glasgow, 2008). Additional research has found that evidence-based programs implemented outside of controlled trials are generally not executed to proficient levels of quality (Dusenbury, Brannigan, Hansen, Walsh, & Falco, 2005; Gottfredson & Gottfredson, 2002). This is unfortunate because program fidelity is strongly linked to positive intervention outcomes (Durlak & DuPre, 2008). A more systematic understanding of how to effectively and accurately implement evidence-based family–school partnership interventions in school settings is needed to ensure successful student outcomes (Greenberg, Domitrovich, Graczyk, & Zins, 2001). Failure to fulfill this need may lead to detrimental effects, such as the inability of schools to develop and sustain systems of intervention that support struggling students (Dishion, 2011).
Translation of research to practice in community settings involves several phases, including a preadoption phase, during which key stakeholders and markets are identified; the adoption phase, during which organizations get ready to implement the program; the implementation phase, during which training and fidelity evaluation occur; and a sustainability phase, during which structures and policies are identified to enable continuation of the intervention (Spoth et al., 2013). Many contextual factors in schools influence their ability to implement family–school partnership practices and sustain them, including teacher training, administrative support, financial resources, and school morale and organization. Few of these factors are taken into consideration when these interventions are developed or disseminated, however (Domitrovich et al., 2008). Protecting program fidelity is a primary goal when evidence-based programs are embedded in existing school frameworks (Spoth, Kavanagh, & Dishion, 2002). Even though few guidelines exist that demonstrate how to integrate programs effectively and realistically (Dishion, 2011) and that identify contextual and program structures that can make or break implementation quality (Payne & Eckert, 2010), researchers and practitioners must understand the conditions that both facilitate and impede high-quality implementation in schools. This is a crucial next step in implementation science because schools connect daily with large numbers of children and thus are valuable venues for dissemination of prevention and intervention programs. In fact, schools are the largest provider of child behavioral health services and the only community setting where many children receive any behavioral health interventions at all (Bums et al., 1995; Hoagwood, Bums, Kiser, Ringeisen, & Schoenwald, 2001).
Importance of Family–School Partnerships
Poor parenting practices and family relationships have been linked to the development and maintenance of youths’ problem behaviors (Connell & Dishion, 2008; Spoth et al., 2002; Stormshak, E. A., Bierman, K. L., McMahon, R. J., Lengua, L., & Conduct Problems Prevention Research Group, 2000). On the other hand, healthy parenting practices and relationships have been associated with positive youth outcomes, even in the presence of factors such as poverty and stress (Galambos, Barker, & Almeida, 2003; Ryan, Martin, & Brooks-Gunn, 2006). It makes sense that interventions targeting the development of positive parenting systems are effective for reducing youth problem behaviors (Dishion, Nelson, & Kavanagh, 2003; Dishion & Stormshak, 2007; Forgatch, DeGarmo, & Beldavs, 2005). A particularly salient time for intervening with parents may be during their child’s transition to middle school, in that problem behaviors often amplify during adolescence (Dishion & Patterson, 2006; Patterson, Capaldi, & Bank, 1991). For example, decreased parental monitoring and parent–teacher communication and increased exposure to peers make the middle school years a risk period for the development of adolescent substance use, aggression, and violence (Dishion, Patterson, Stoolmiller, & Skinner, 1991; Eccles, Lord, & Roeser, 1995).
Even though parental involvement in school tends to decline when children enter middle school, research has shown that parent involvement in education is associated with positive child outcomes, including higher grade point averages (Gutman & Midgley, 2000), better self-regulation and social skills (Brody, Flor, & Gibson, 1999; McWayne, Hampton, Fantuzzo, Cohen, & Sekino, 2004), lower dropout rates (Rumberger, 1995), fewer grade retentions and special education placements (Miedel & Reynolds, 1999), and improvements in language and reading skills (Sheridan, Knoche, Kupzyk, Pope Edwards, & Marvin, 2011). When parents are involved in their child’s education, students also more readily adjust to the demands of the classroom and show improved academic performance (Epstein, 1991; Henderson & Berla, 1994; Henderson & Mapp, 2002; Reynolds, 1992). Despite the advantages of involving parents in school settings in terms of primary school outcomes, such as achievement, few schools develop or maintain organized systems for positively intervening with them (Stormshak & Dishion, 2002).
Positive Family Support Program
To support the advancement of positive family–school partnerships, particularly during the middle school years, Dishion and colleagues developed the Positive Family Support (PFS) project. PFS is a tiered intervention designed to increase collaboration between families and school personnel during periods of developmental transition or risk. In this chapter, we provide a brief introduction to the model underlying PFS (Dishion & Stormshak, 2007) and its adaptation to the middle school environment (Fosco, Dishion, & Stormshak, 2012). Scale-up of the PFS model in 41 Oregon middle schools, a project funded by the Department of Education (R324A090111), is described in detail.
PFS evolved from intervention trials of the Family Check-Up in schools. The Family Check-Up (FCU) is a brief, cost-effective intervention that has emerged from a series of intervention trials in public middle schools to prevent escalating problem behaviors among young adolescents (Dishion et al., 2008; Dishion & Kavanagh, 2003; Dishion & Stormshak, 2007; Stormshak et al., 2011; Stormshak, Dishion, Light, & Yasui, 2005). These trials with ethnically and socioeconomically diverse young children and middle school-age youths have demonstrated intervention effects on self-regulation, grade point average, attendance, school engagement, and growth of teacher-rated child problem behavior over time (Fosco et al., 2012; Stormshak et al., 2005, 2010), as well as a variety of nonacademic outcomes, such as rates of depression, substance use, high-risk sexual behavior, and early-adult obesity (Connell, Dishion, & Deater-Deckard, 2006; Stormshak et al., 2010; Van Ryzin & Nowicka, 2013).
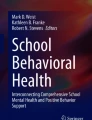
The PFS model is intended to be delivered by school personnel with relatively little support from external consultants. Adaptations to the model for integration into middle schools have included tiered intervention intensity (Myers & Nastasi, 1999), strategies to enhance motivation (Miller & Rollnick, 2002), and a tailored intervention design (Collins, Murphy, & Bierman, 2004). As depicted in Fig. 2.1, the core components of PFS have been matched and dovetailed to components of school-wide positive behavior support systems, such as the Positive Behavior Interventions and Supports (PBIS; Sugai et al., 2000) model, to build bridges between school and home. The dovetailing of PFS with programs such as PBIS was intentional with respect to a public health implementation perspective (Biglan, 1995; Biglan, Sprague, & Moore, 2006; Shaw, 1986). This perspective suggests that by using an effective intervention model that makes pragmatic use of naturally occurring ecological settings and well-established service delivery structures (e.g., PBIS), the rate of engagement will increase while some of the implementation response cost to the setting will be reduced. In the scaling-up process, the ability of PFS to improve family–school partnerships and student academic and social outcomes was tested through dissemination and promotion of family support services by existing school personnel. The program has been implemented in a range of schools and economic conditions in Oregon; Table 2.1 shows the distribution of the participating schools with respect to number of students, ethnic/minority status, and eligibility for free/reduced-cost lunch. The study sample are approximately 30 % ethnically diverse, and 59 % are eligible for free/reduced-cost lunch.

Concatenation of school and family Positive Behavior Interventions and Supports (PBIS)
A number of challenges and obstacles arose throughout the scaling-up process. The remainder of this chapter focuses on the complexities of scaling up evidence-based family–school partnership practices aimed at improving the behavioral and mental health of students. It also describes approaches to successfully managing these complexities.
Contextual Complexities in School-Based Scale-Up of Family–School Partnership Interventions
Designing and implementing school-based interventions that target improvement of family–school partnerships is a challenging task (Spoth et al., 2002). As posited by Stormshak and Dishion (2002), interventions that can be embedded within existing school frameworks and that take into account each school’s unique contextual factors are the most likely to engage large numbers of school personnel and families. It can be challenging for program designers and implementers to develop and disseminate interventions that account for such complexities, however, because little research has specifically addressed them. More work is needed to understand the impact of a variety of contextual factors on successful scale-up and to articulate potential solutions to manage them successfully. The majority of research in this area has focused on similar constructs that predict effective implementation, such as principal support, school climate, and teacher support for the model, and most of these factors have indeed spelled success. The problem is that many schools nationwide do not have these basic structures in place. How can we implement programs in schools with few resources, high principal turnover, and limited support for the models we have developed? Additional research on implementation and dissemination in this area would increase our understanding of successful uptake of these programs in all schools, regardless their immediate resources.
Lack of Resources
Lack of resources, money, and staffing is probably the most common reason that researchers fail to successfully disseminate interventions, curricula, and other empirically based models to schools. It is a key underlying factor that predicts poor uptake and implementation, and it is related to staff turnover, lack of training, lack of principal support, and other critical variables that predict implementation success (Gingiss, Roberts-Gray, & Boerm, 2006; Payne & Eckert, 2010). Many schools are serving growing numbers of students and managing increasing rates of mental health and behavioral problems with limited financial resources (Stormshak et al., 2011). A diminished staff-to-student ratio can leave school personnel at all levels feeling overworked and undersupported, with little energy or time left to implement family–school partnership interventions. Assets are being depleted in an effort to comply with existing public policy, such as achievement testing and complex teacher and administrative evaluations. Amid financial cutbacks and reductions in funding, many schools struggle to find the administrative focus, support services, class time, or physical space necessary to support additional programs. Family–school interventions may be seen as a luxury rather than a component of student success and well-being (Stormshak et al., 2005). Principals who must cut key staff members often find it politically challenging to prioritize interventions that are considered superfluous by influential stakeholders (Fosco et al., 2014). The overall lack of resources and the increasing numbers of problematic students present substantial barriers to successful implementation and sustainability of school-based prevention and intervention programs.
Finding a balance between the need to sustain all pertinent intervention components and the need to be brief and cost-effective is a potential difficulty in family–school partnership research. Infusion of a multilevel, family-centered approach, that is, a combination of universal, selected, and indicated levels, contributes to the efficient management of resources, in that only those students who are most in need of intensive intervention receive costly services (Stormshak et al., 2011). A tiered design also dovetails more easily with other multilevel education programs, such as PBIS and/or RtI. Programs can be executed gradually to further reduce burden and support school staff who may be overwhelmed by the implementation of a new intervention. This approach can also prove to be more economical. Similarly, when it is not possible for one school staff member to devote the time needed to put the intervention into action, it may become necessary to shift responsibilities to a range of staff members. When this occurs, it is crucial that intervention components be seamlessly integrated into the existing activities of school personnel, so as not to overload already-pressured individuals (Gottfredson & Gottfredson, 2002). Finally, user-friendly and streamlined implementation materials, such as manuals, brochures, and videos, enable school staff to easily accommodate an intervention without expending excessive amounts of time or energy. Materials should offer detailed guidelines and explicit scripts yet remain flexible enough to match the unique needs of individual schools and staff members (Turner & Sanders, 2006). In sum, it is vital that intervention designers and implementers seriously consider each school’s available resources because attempts to support expensive and time-consuming programs often result in poor uptake, execution, and sustainability. Research that focuses on adapting programs to fit into existing curricula and services in schools is critical to understanding how to improve uptake in schools with few resources.
In our PFS project, schools in the intervention condition have weathered constant budgetary changes during the course of implementation. Forty-eight percent of the schools experienced a loss in overall operating expenditures per student between the 2007–2008 and 2011–2012 school years. In particular, one relatively small rural school lost more than $1,500 of operating expenditures per student during this time period. Expenditure per student for counselor, nurse, and support staff services was reduced in 57 % of PFS intervention schools. A common result has been low teacher and administrator morale brought on by multiple years of job loss, employment insecurity, and turnover. Constant budgetary shortages have also compromised continuity in terms of training, intervention implementation, and staff expectations.
School Staff Training and Experience
While the majority of school staff are involved in education out of genuine concern for children and excel at being student centered, few understand or take into account family contributions to problem behavior (Shirk & Jungbluth, 2008; Stormshak, Connell, & Dishion, 2009). That said, schools are not likely to gather information from parents regarding conditions at home or involve parents in school-based interventions. Furthermore, most school staff are trained according to individual models of development (Stormshak et al., 2005), meaning few individuals working in schools have the knowledge or skills necessary to consistently engage parents in a manner that effectively and positively supports children’s academic and behavioral success. Programs that require schools to enact structural changes to accommodate the proactive involvement of parents in school-based student interventions often necessitate a substantial shift in traditional paradigms (Fosco et al., 2014). Such large-scale changes may impede the successful implementation and scale-up of family–school partnership programs. If these changes can be embedded or dovetailed with other successful structural changes, such as PBIS, these impediments may be diminished.
Positive family–school partnership is a key component in the behavioral, mental health, and academic success of students, yet many school staff do not receive training in how to effectively engage parents (Stormshak et al., 2005, 2011). Not only must scientists who are developing and disseminating family–school interventions be cognizant of the need to empower through efficient multilevel program design, but school administrators and teachers must learn how to proactively and positively interact with parents. To begin, implementers should be ready to provide direction, coaching, scaffolding, corrective feedback, and encouragement to school personnel about their interactions with parents (Gottfredson & Gottfredson, 2002). This support opens an important channel of communication between scientists and schools regarding best practices with respect to using family–school partnerships to enhance student success and well-being. It may also be necessary to contextualize parenting skills in terms of school-relevant tasks, such as homework routines and positive behavior support, to overcome resistance and help staff recognize their own expertise in providing parental support (Fosco et al., 2014). Similarly, materials must be available that are concrete, behavioral, and positive in nature (Fosco et al., 2014). Overall, all these exigencies must be addressed to overcome any resistance to altering existing school paradigms whose focus is on individual student development to the exclusion of family participation.
In light of this potential impasse, efficient training in the use of family–school relationships seems necessary to foster positive student outcomes. Research on the most effective means for preparing teachers and school staff to develop constructive relationships is necessary. Essential to that goal is to focus on concrete, behavioral, and positive strategies that are familiar to school staff and therefore are not intimidating (Fosco et al., 2014). Administrators and teachers can be provided with easily accessible and scripted materials (e.g., scaffolding) that strengthen collaboration with parents. Research that examines training in these approaches prior to implementation of family-centered practices in schools would help us understand the importance of this training and content. Finally, if staff appear resistant or fearful of contacting parents, it may be necessary to encourage school administrators to provide incentives to reward attempts at positive parent interactions until staff become fluid in these skills. All these recommended tactics represent fruitful lines of research on professional development in the area of family–school partnerships.
School Leadership
Support and leadership from school principals is a key element in the successful implementation of evidence-based family–school partnership programs. Without it, fidelity is not maintained long enough to fully integrate the program into school policy and routines (Handler et al., 2007; McDougal, Clonan, & Martens, 2000). When factors that predict successful uptake of interventions are studied, principals’ support often predicts successful implementation and maintenance of models in schools (Payne, 2008; Payne & Eckert, 2010). Closely involving principals in the training, consultation, implementation, and sustainability of these programs can be difficult in the face of time constraints, limited resources, varying interest levels, and individual differences in leadership ability. Yet, principals are crucial to establishing family–school partnerships as an overarching school norm and holding school staff accountable for maintaining positive collaborations with families. When principals do not consistently advocate for family collaboration, uptake and maintenance of the intervention can be seriously constrained. Persistent administrative turnover presents additional challenges, especially during difficult economic times. In the PFS project, high levels of turnover occurred during the 3 years of the study, with 45 % of schools turning over at least one principal and 20 % of schools hiring a new principal every year of the study. In addition, vice principal turnover occurred at 40 % of schools at least once during the project period. To accomplish buy-in and support for the existing model required quick adjustment to working with new school leadership in the middle of the project.
Gaining the support and buy-in of school principals can be a challenging task. Tremendous demands have been placed on them in this age of achievement accountability, instructional leadership, and federal and state requirements for new, time-consuming teacher evaluation methods. As a result, they may not appreciate additional expectations to foster a family-friendly school culture. Implementation strategies can be adapted to enhance the adoption of systemic change by those in leadership positions (Turner & Sanders, 2006). Individual consultation and face-to-face time enables implementers to understand and work with the principal’s unique leadership style and tailor intervention strategies accordingly (Fosco et al., 2014). With research strongly suggesting that principal support predicts successful uptake, it is critical to consider how to work successfully with schools that have a high leadership turnover. Research that focuses on factors that predict successful uptake under these conditions will be important future work. District-wide support and teacher support may be two ways to ensure that continuity exists in the school despite changes in leadership.
School Climate
The overall school climate can significantly affect the staff’s ability to successfully implement evidence-based family–school partnership programs. School climate, defined in the literature in multiple ways, often refers to supportive administration and endorsement of program implementation (Beets et al., 2008). Schools that foster a sense of respect, collaboration, support, and active problem solving at all staffing levels to effectively sustain implementation requirements may be the most successful at long-term uptake of programs (Greenberg, Domitrovich, & Bumbarger, 2001). Constructive and encouraging interpersonal relationships among staff members can promote a sense of community that is critical to promoting positive student outcomes (King & Newmann, 2000). Unfortunately, for a multitude of reasons, such as high turnover rates, poor leadership, staff shortages, and inadequate communication systems, the school climate does not always appear supportive or optimistic. The result may be an absence of collegiality and insufficient motivation to implement the intervention, which can require significant amounts of focus, energy, and openness to change. Poor school climates almost guarantee a lack of buy-in.
Staff members’ readiness and motivation to increase collaborative family involvement with the school can be assessed before a partnership intervention is begun. This evaluation helps pinpoint what additional support may be needed and which strategies may be used to increase buy-in by school personnel and ultimately, to facilitate implementation (Gottfredson & Gottfredson, 2002). Particularly in inadequate school climates, it is helpful if implementers work closely with the school’s key opinion holders and develop working relationships with administrators and teachers that facilitate positive family–school practices (Stormshak et al., 2005). We have found it necessary for implementers to align the key components of an intervention with the school’s current mission (e.g., the family involvement and partnership requirement in federal and state regulations, such as Title 1 and IDEA) and change capacity (Feldstein & Glasgow, 2008). Although it can be quite challenging to implement and sustain family–school interventions in hostile or resistant school climates, implementers may be able to combat some of these difficulties by first prioritizing effective and supportive relationships with staff members at all levels. Research in this area could broaden the definition of school climate to include factors such as teacher support, parent involvement, and community-level support. These factors may buttress successful uptake of programs in schools.
Critical Events
Critical events are serious incidents at a school that may affect training, implementation, or the program itself. These events are disruptive to the school, learning environment, and overall school climate. When these events occur, leadership are compelled to focus almost entirely on them, and the school enters a “crisis mode” that interrupts learning and programming until the school recovers from the incident. During the course of the PFS project, critical incidents were tracked and documented. The number of incidents was surprising: they occurred in nearly 50 % of schools. Following are examples of some of these incidents that led to disruption of the implementation of the model.
-
School A principal was involved in a career-altering motorcycle accident.
-
Teacher at School B committed suicide.
-
Physical fight between parents occurred in the School C family resource center.
-
Several project schools experienced strikes; strikes occurred statewide.
-
204 teachers were laid off in the school district that included two middle schools in the study.
-
School E was restructured from sixth to eighth grades to seventh and eighth grades.
-
Eighth grader in School F lost a parent in a multiple homicide.
-
Teacher at School G died unexpectedly.
-
Sixth grader at School H died in a bus accident.
Although some of these crises were disruptive and divisive and caused a setback to positive program implementation, some schools were able to use these crises as a positive opportunity to increase support and collaboration with parents (e.g., using the universal-level family resource center as a safe room for staff, students, and parents). Implementation research has not addressed the issue of critical events. More research is needed in this area to understand the impact that critical events have on schools, their support of students and families, and their ability to continue implementing programs.
Attitude Toward Parents
School staff seldom receive adequate training regarding the influence of family factors on student outcomes or how to include families in student interventions (Stormshak et al., 2005). For example, one of the staff members in the PFS study completed a school administrator credentialing program that included 10 content areas and 27 modules, yet not one involved families or family factors in education interventions or outcomes. Schools typically attempt to resolve the academic, behavioral, and emotional problems of students with little parent input or communication. As a result, parents tend not to be contacted by school personnel until their child’s behavior has gained significant momentum and becomes severe, leaving little opportunity or emotional space to proactively prevent problem behaviors or focus on student and family strengths (Fosco et al., 2014). The unfortunate result is that school staff concentrate on student deficits and offer few opportunities to collaborate with parents; most of the “solutions” that are generated rely on punitive techniques, such as suspension or detention. These approaches tend to disregard the unique context of the family, which in turn reduces the likelihood that solutions will be helpful or sustainable. Given that few school staff receive extensive training in how to effectively collaborate with families, the chance that family–school partnership programs will be implemented is seriously diminished.
Program Integration
Schools may have access to a number of promising intervention programs, yet few possess a map for how to realistically integrate programs into their daily norms and routines (Dishion, 2011). Consequently, schools often feel burdened by their attempts to implement too many individual interventions and may never uptake any particular program to fidelity. School staff can also be wary of new intervention efforts because other daily requirements are seldom reduced to accommodate them, and most often the workload is increased with no commensurate increase in pay. To make matters worse, because few schools are able to sustain evidence-based programs with a high degree of fidelity, program effectiveness is thereby decreased (Durlak & DuPre, 2008), and school staff may not observe positive changes in their students as a result of intervention efforts. Rarely seeing clear and consistent positive student outcomes may reduce the likelihood that schools continue to devote time to applying new interventions. Successful uptake of family–school partnership programs suffers because developing positive, proactive, and collaborative relationships with families is a potentially difficult endeavor and can seem quite distal to student achievement.
To reduce the burden of implementation experienced by schools and potentially increase uptake, program developers must design and test interventions that can easily be integrated into other efforts and existing school structures. There are several ways to address the challenge of increasing the ease of integration and usability of these programs. For example, family-centered interventions that offer a range of services, from brief but effective parent contacts to more intensive involvement, often fit well with referral and intervention systems that already exist in schools (Stormshak et al., 2005). Similarly, family–school partnership programs that offer a menu of empirically supported interventions (e.g., brief-focused consultation, two to three sessions about a parenting topic, multisession parenting group) that can be accomplished using diverse delivery methods are often accessible to a greater number of families and school personnel (Stormshak & Dishion, 2009). Offering a range of intervention options and multiple delivery methods enables schools to more easily integrate new interventions into their existing routines, thereby increasing the uptake, penetration of families served, and sustainability of family-centered practices. Using a bottom-up collaborative approach to intervention design that recognizes the expertise of school staff enables developers and implementers to successfully integrate intervention efforts and motivate school personnel toward positive change (Cappella, Jackson, Bilal, Hamre, & Soulé, 2011; Shernoff et al., 2011). For example, building on the skill and experiences that schools already possess regarding parent interactions (e.g., a well-attended parent topic night, assignment completion and attendance records proactively provided to parents via technology) can increase buy-in for integrating new methods of family involvement, as well as encourage innovation and risk taking among administrators and teachers. Finally, future research must continue to investigate how schools both struggle and succeed in managing the educational, social, behavioral, and mental health outcomes of students (Dishion, 2011). Such information is pivotal to increased understanding of how to develop, implement, and sustain family–school partnership programs that are meaningful and successful for students, parents, and school staff alike.
Conclusion and Future Research Directions
Research in the area of implementation has been growing during the past decade, and multiple studies have been examining circumstances such as principal support, resources, teacher training, and school climate as primary factors that predict successful uptake and implementation. The challenge is that with declining financial support for schools, research must find a way for programs to be implemented in spite of few resources and for these models to be sustained over time. Molloy, Moore, Trail, Epps, and Hopfer (2013) examined schools that had implemented PBIS to understand factors related to sustaining the model. They found that full implementation was related to reduced rates of problem behavior, which provides meaningful support for the model. Smaller schools, elementary schools, and those with higher SES parents had the best quality implementation; on the other hand, only 37–49 % of schools implemented the model fully. If we can implement programs effectively only in high-SES, well-resourced schools, a nation-wide improvement in family–school partnership and quality of education will not occur. Measures of school capacity are commonly used to evaluate whether schools are “ready” to implement programs with fidelity (Gingiss et al., 2006). This practice eliminates schools that are the most disadvantaged and would most benefit from implementing family-centered practices. Research that focuses on understanding how to implement family-centered programs in schools with few resources and limited stability will be important for the future of implementation science.
The most effective intervention for enhancing family-centered practices in schools may involve training the next generation of teachers in these practices and studying their ability to integrate them as they get their first jobs across the country. Including research and training that enhances the ability of teachers and educators to work with parents will be important for future generations of teachers. Although parent involvement in school has been linked to a multitude of positive student outcomes (Epstein, 1991; Henderson & Berla, 1994; Henderson & Mapp, 2002; Reynolds, 1992), few schools use effective family–school partnership programs (Stormshak & Dishion, 2002). As a result, students may not receive the behavioral, academic, and mental health support they need to be successful in school. It can be challenging to scale-up family–school partnership interventions with a high degree of fidelity because many contextual factors in schools complicate the uptake and maintenance of evidence-based interventions. In particular, successful scale-up requires that programs be simple and flexible to adapt to school environments. Programs must also fit into a school’s culture, daily routines, other change initiatives, and leadership structure so they are not regarded as overbearing and burdensome. For example, multitiered family–school partnerships are successful when they integrate well with existing multitiered strategies already being used to improve academic and developmental outcomes (e.g., RtI, PBIS, Data-based Decision Making). It is recommended that researchers address factors such as dissemination, uptake, implementation, and sustainability by using theoretical frameworks such as Re-Aim (Glasgow, Vogt, & Boles, 1999) or Diffusion of Innovation (Rogers, 2003) throughout the development process rather than at scale-up. Policy changes at the local and state level may also have to be made to help schools successfully uptake and sustain models of prevention (Biglan & Taylor, 2000).
Without doubt, identifying how to increase schools’ effective use of positive family–school partnership practices is worthy of continued investigation and inquiry. By taking into consideration the unique needs, strengths, and constraints of school systems, intervention implementers can bridge the gap between research and practice in natural settings and those with few resources across the country.
References
Atkins, M. S., Frazier, S. L., Leathers, S. J., Graczyk, P. A., Talbott, E., Jakobsons, L., … Bell, C. C. (2008). Teacher key opinion leaders and mental health consultation in low-income urban schools. Journal of Consulting and Clinical Psychology, 76, 905–908. doi:10.1037/a0013036.
Barry, T. D., Lyman, R. D., & Grofer Klinger, L. (2002). Academic underachievement and attention-deficit/hyperactivity disorder: The negative impact of symptom severity on school performance. Journal of School Psychology, 40, 259–283. doi:10.1016/S0022-4405(02)00100-0.
Beets, M. W., Flay, B. R., Vuchinich, S., Acock, A. C., Li, K.-K., & Allred, C. (2008). School climate and teachers? Beliefs and attitudes associated with implementation of the positive action program: A diffusion of innovations model. Prevention Science, 9(4), 264–275. doi:10.1007/s11121-008-0100-2.
Biglan, A. (1995). Translating what we know about the context of antisocial behavior into a lower prevalence of such behavior. Journal of Applied Behavior Analysis, 28, 479–492. doi:10.1901/jaba.1995.28-479.
Biglan, A., Sprague, J., & Moore, K. J. (2006). A functional contextualist framework for affecting peer influence practices. In K. A. Dodge, T. J. Dishion, & J. E. Lansford (Eds.), Deviant peer influences in programs for youth: Problems and solutions (pp. 342–365). New York, NY: The Guilford Press.
Biglan, A., & Taylor, T. K. (2000). Increasing the use of science to improve child-rearing. The Journal of Primary Prevention, 21, 207–226. doi:10.1023/A:1007083203280.
Brody, G. H., Flor, D. L., & Gibson, N. M. (1999). Linking maternal efficacy beliefs, developmental goals, parenting practices and child competence in rural single-parent African American families. Child Development, 70, 1197–1208. doi:10.1111/1467-8624.00087.
Bums, B. J., Costello, E. J., Angold, A., Tweed, D. L., Stangl, D. K., Farmer, E. M. Z., & Erkanli, A. (1995). Children’s mental health service use across service sectors. Health Affairs, 14, 147–159.
Cappella, E., Jackson, D. R., Bilal, C., Hamre, B. K., & Soulé, C. (2011). Bridging mental health and education in urban elementary schools: Participatory research to inform intervention development. School Psychology Review, 40, 486–508.
Centers for Disease Control and Prevention. (2013, February 27). Coordinated School Health Program. Retrieved from http://www.cdc.gov/HealthyYouth/CSHP/
Christenson, S. L. (2003). The family–school partnership: An opportunity to promote the learning competence of all students. School Psychology Quarterly, 18, 454–482. doi:10.1521/scpq.18.4.454.26995.
Collins, L., Murphy, S., & Bierman, K. (2004). A conceptual framework for adaptive preventive interventions. Prevention Science, 5, 185–196. doi:10.1023/B:PREV.0000037641.26017.00.
Connell, A. M., & Dishion, T. J. (2008). Reducing depression among at-risk early adolescents: Three-year effects of a family-centered intervention embedded within schools. Journal of Family Psychology, 22, 574–585. doi:10.1037/0893-3200.22.3.574.
Connell, A. M., Dishion, T. J., & Deater-Deckard, K. (2006). Variable- and person-centered approaches to the analysis of early adolescent substance use: Linking peer, family, and intervention effects with developmental trajectories [Special Issue]. Merrill-Palmer Quarterly, 52, 421–438. doi:10.1353/mpq.2006.0025.
Dishion, T. J. (2011). Promoting academic competence and behavioral health in public schools: A strategy of systemic concatenation of empirically based intervention principles. School Psychology Review, 40, 590–597.
Dishion, T. J., & Kavanagh, K. (2003). Intervening with adolescent problem behavior: A family-centered approach. New York, NY: Guilford.
Dishion, T. J., Nelson, S. E., & Kavanagh, K. (2003). The Family Check-Up with high-risk young adolescents: Preventing early-onset substance use by parent monitoring. Behavior Therapy, 34, 553–571. doi:10.1016/S0005-7894(03)80035-7.
Dishion, T. J., & Patterson, G. R. (2006). The development and ecology of antisocial behavior in children and adolescents. In D. Cicchetti & D. J. Cohen (Eds.), Developmental psychopathology: Vol. 3. Risk, disorder, and adaptation (pp. 503–541). New York, NY: Wiley.
Dishion, T. J., Patterson, G. R., Stoolmiller, M., & Skinner, M. (1991). Family, school and behavioral antecedents to early adolescent involvement with antisocial peers. Developmental Psychology, 27, 172–180. doi:10.1037/0012-1649.27.1.172.
Dishion, T. J., Shaw, D. S., Connell, A. M., Gardner, F., Weaver, C. M., & Wilson, M. N. (2008). The Family Check-Up with high-risk indigent families: Preventing problem behavior by increasing parents’ positive behavior support in early childhood. Child Development, 79, 1395–1414. doi:10.1111/j.1467-8624.2008.01195.x.
Dishion, T. J., & Stormshak, E. A. (2007). Intervening in children’s lives: An ecological family-centered approach to mental health care. Washington, DC: American Psychological Association.
Domitrovich, C. E., Bradshaw, C. P., Poduska, J. M., Hoagwood, K., Buckley, J. A., Olin, S., Romanelli, L. H., … Ialongo, N. S. (2008). Maximizing the implementation quality of evidence-based preventive interventions in schools: A conceptual framework. Advances in School Mental Health Promotion, 1, 6–28. doi: 10.1080/1754730X.2008.9715730
Domitrovich, C. E., & Greenberg, M. T. (2000). The study of implementation: Current findings from effective programs for school aged children. Journal of Educational and Psychological Consultation, 11, 193–222. doi:10.1207/S1532768XJEPC1102_04.
Durlak, J. A., & DuPre, E. P. (2008). Implementation matters: A review of research on the influence of implementation on program outcomes and the factors affecting implementation. American Journal of Community Psychology, 41, 327–350. doi:10.1007/s10464-008-9165-0.
Dusenbury, L., Brannigan, R., Hansen, W. B., Walsh, J., & Falco, M. (2005). Quality of implementation: Developing measures crucial to understanding the diffusion of preventive interventions. Health Education Research, 20, 308–313. doi:10.1093/her/cyg134.
Eccles, J. S., & Harold, R. D. (1993). Parent–school involvement during the early adolescent years. Teachers College Record, 94, 568–587.
Eccles, J. S., Lord, S. E., & Roeser, R. W. (1995). Round holes, square pegs, rocky roads, and sore feet: The impact of stage-environment fit on young adolescents’ experiences in schools and families. In D. Cicchetti & S. Toth (Eds.), Rochester Symposium on Developmental Psychopathology: Vol. VII. Adolescence: Opportunities and challenges (pp. 47–92). New York, NY: University of Rochester Press.
Elliott, D. S., & Mihalic, S. (2004). Issues in disseminating and replicating effective prevention programs. Prevention Science, 5, 47–53. doi:10.1023/B:PREV.0000013981.28071.52.
Epstein, J. L. (1991). Effects on student achievement of teachers’ practices of parent involvement. Advances in Reading/Language Research, 5, 261–276.
Feldstein, A. C., & Glasgow, R. E. (2008). A practical, robust implementation and sustainability model (PRISM). Joint Commission Journal on Quality and Patient Safety, 34, 228–243.
Forgatch, M. S., Bullock, B. M., & Patterson, G. R. (2004). From theory to practice: Increasing effective parenting through role play. The Oregon Model of Parent Management Training (PMTO). In H. Steiner, K. Chang, J. Lock, & J. Wilson (Eds.), Handbook of mental health interventions in children and adolescents: An integrated development approach (pp. 782–813). San Francisco, CA: Jossey–Bass.
Forgatch, M. S., DeGarmo, D. S., & Beldavs, Z. G. (2005). An efficacious theory-based intervention for stepfamilies. Behavior Therapy, 36, 357–365. doi:10.1016/S0005-7894(05)80117-0.
Forman, S. G., Olin, S. S., Hoagwood, K. E., Crowe, M., & Saka, N. (2009). Evidence-based interventions in schools: Developers’ views of implementation barriers and facilitators. School Mental Health, 1, 26–36. doi:10.1007/s12310-008-9002-5.
Fosco, G. M., Dishion, T. J., & Stormshak, E. A. (2012). A public health approach to family-centered prevention of alcohol and drug addiction: A middle school strategy. In H. J. Shaffer, D. A. LaPlante, & S. E. Nelson (Eds.), The American Psychological Association addiction syndrome handbook (pp. 225–245). Washington, DC: American Psychological Association.
Fosco, G. M., Seeley, J. R., Dishion, T. J., Smolkowski, K., Stormshak, E. A., Downey-McCarthy, R., … Strycker, L. A. (2014). Lesson learned from scaling-up the Ecological Approach to Family Interventions and Treatment (EcoFIT) program in middle schools. In M. Weist, N. Lever, C. Bradshaw, & J. Owens (Eds.), Handbook of school mental health (2nd ed.) New York, NY: Springer.
Galambos, N. L., Barker, E. T., & Almeida, D. M. (2003). Parents do matter: Trajectories of change in externalizing and internalizing problems in early adolescence. Child Development, 74, 578–594. doi:10.1111/1467-8624.7402017.
Gingiss, P. M., Roberts-Gray, C., & Boerm, M. (2006). Bridge-It: A system for predicting implementation fidelity for school-based tobacco prevention programs. Prevention Science, 7(2), 197–207. doi:10.1007/s11121-006-0038-1.
Glasgow, R. E., Vogt, T. M., & Boles, S. M. (1999). Evaluating the public health impact of health promotion interventions: the RE-AIM framework. American Journal of Public Health, 89, 1322–1327.
Gottfredson, D. C., & Gottfredson, G. D. (2002). Quality of school-based prevention programs: Results from a nation survey. Journal of Research on Crime and Delinquency, 39, 3–35. doi:10.1177/002242780203900101.
Greenberg, M. T., Domitrovich, C., Graczyk, P., & Zins, J. (2001). The study of implementation in school-based preventive interventions: Theory, research, and practice. Washington, DC: Center for Mental Health Services, Substance Abuse and Mental Health Administration, U.S. Department of Health and Human Services.
Greenberg, M. T., Domitrovich, C., & Bumbarger, B. (2001). The prevention of mental disorders in school-aged children: Current state of the field. Prevention and Treatment, 4, 1–62. doi:10.1037/1522-3736.4.1.41a.
Gutman, L. M., & Midgley, C. (2000). The role of protective factors in supporting the academic achievement of poor African American students during the middle school transition. Journal of Youth and Adolescence, 29, 233–248. doi:10.1023/A:1005108700243.
Handler, M. W., Rey, J., Connell, J., Their, K., Feinberg, A., & Putnam, R. (2007). Practical considerations in creating school-wide positive behavior support in public schools. Psychology in the Schools, 44, 29–39. doi:10.1002/pits.20203.
Henderson, A. T., & Berla, N. (1994). A new generation of evidence: The family is critical to student achievement (p. 174). Washington, DC: National Committee for Citizens in Education.
Henderson, A. T., & Mapp, K. L. (2002). A new wave of evidence: The impact of school, family and community connections on student achievement. Austin, TX: Southwest Educational Laboratory.
Hoagwood, K., Bums, B. J., Kiser, L., Ringeisen, H., & Schoenwald, S. K. (2001). Evidence-based practice in child and adolescent mental health services. Psychiatric Services, 52, 1179–1189. doi:10.1176/appi.ps.52.9.1179.
Horner, R. H., Sugai, G., Todd, A. W., & Lewis-Palmer, T. (2005). School-wide positive behavior support. In L. Bambara & L. Kern (Eds.), Individualized supports for students with problem behaviors: Designing positive behavior plans (pp. 359–390). New York, NY: Guilford Press.
Kazdin, A. E. (2002). Psychosocial treatments for conduct disorder in children and adolescents. In P. E. Nathan & J. M. Gorman (Eds.), A guide to treatments that work (2nd ed., pp. 57–85). London, United Kingdom: Oxford University Press.
Kazdin, A. E. (2010). Problem-solving skills training and parent management training for oppositional defiant disorder and conduct disorder. In J. R. Weisz & A. E. Kazdin (Eds.), Evidence-based psychotherapies for children and adolescents (pp. 211–226). New York, NY: Guilford Press.
King, M. B., & Newmann, F. M. (2000). Will teacher learning advance school goals? Phi Delta Kappan, 81, 576–580.
McDougal, J. L., Clonan, S. M., & Martens, B. K. (2000). Using organizational change procedures to promote the acceptability of prereferral intervention services: The School-Based Intervention Team Project. School Psychology Quarterly, 15, 149–171. doi:10.1037/h0088783.
McWayne, C., Hampton, V., Fantuzzo, J., Cohen, H. L., & Sekino, Y. (2004). A multivariate examination of parent involvement and the social and academic competencies of urban kindergarten children. Psychology in the Schools, 41, 363–377. doi:10.1002/pits.10163.
Miedel, W. T., & Reynolds, A. J. (1999). Parent involvement in early intervention for disadvantaged children: Does it matter? Journal of School Psychology, 37, 379–402. doi:10.1016/S0022-4405(99)00023-0.
Miller, W. R., & Rollnick, S. (2002). Motivational interviewing: Preparing people for change (2nd ed.). New York, NY: Guilford.
Molloy, L. E., Moore, J. E., Trail, J., Epps, J. J., & Hopfer, S. (2013). Understanding real-world implementation quality and “active ingredients” of PBIS. Prevention Science, 14(6), 593–605. doi:10.1007/s11121-012-0343-9.
Myers, J., & Nastasi, B. (1999). Primary prevention in school settings. In C. R. Reynolds & T. B. Gutkin (Eds.), Handbook of school psychology (3rd ed.). New York, NY: Wiley.
Patterson, G. R., Capaldi, D., & Bank, L. (1991). An early starter model for predicting delinquency. In D. J. Pepler & K. H. Rubin (Eds.), The development and treatment of childhood aggression (pp. 139–168). Hillsdale, NJ: Erlbaum.
Patterson, G. R., Reid, J. B., & Dishion, T. J. (1992). A social learning approach: Vol 4. Antisocial boys. Eugene, OR: Castaglia.
Payne, A. A. (2008). A multilevel analysis of the relationships among communal school organization, student bonding, and delinquency. Journal of Research in Crime and Delinquency, 45, 429–455. doi:10.1177/0022427808322621.
Payne, A. A., & Eckert, R. (2010). The relative importance of provider, program, school, and community predictors of the implementation quality of school-based prevention programs. Prevention Science, 11, 126–141. doi:10.1007/s11121-009-0157-6.
Prinz, R. J., & Dumas, J. E. (2004). Prevention of oppositional-defiant disorder and conduct disorder in children and adolescents. In P. Barrett & T. H. Ollendick (Eds.), Handbook of interventions that work with children and adolescents: From prevention to treatment (pp. 475–488). Chichester, UK: Wiley.
Prinz, R. J., & Sanders, M. R. (2007). Adopting a population-level approach to parenting and family support interventions. Clinical Psychology Review, 27, 739–749. doi:10.1016/j.cpr.2007.01.005.
Reynolds, A. J. (1992). Comparing measures of parental involvement and their effects on academic achievement. Early Childhood Research Quarterly, 7, 441–462. doi:10.1016/0885-2006(92)90031-S.
Rimm-Kaufman, S. E., & Pianta, R. C. (2000). Patterns of family–school contact in preschool and kindergarten. School Psychology Review, 28, 426–438.
Ringeisen, H., Henderson, K., & Hoagwood, K. (2003). Context matters: Schools and the “research to practice” gap in children’s mental health. School Psychology Review, 32, 153–168.
Rogers, E. M. (2003). Diffusion of Innovations (5th ed.). New York, NY: Free Press.
Rumberger, R. W. (1995). Dropping out of middle school: A multilevel analysis of students and schools. American Educational Research Journal, 32, 583–625. doi:10.2307/1163325.
Ryan, R. M., Martin, A., & Brooks-Gunn, J. (2006). Is one good parent good enough? Patterns of mother and father parenting and child cognitive outcomes at 24 and 36 months. Parenting: Science and Practice, 6, 211–228. doi:10.1207/s15327922par0602&3_5.
Shaw, M. C. (1986). The prevention of learning and interpersonal problems. Journal of Counseling and Development, 64, 624–627. doi:10.1002/j.1556-6676.1986.tb01024.x.
Sheridan, S. M., Knoche, L. L., Kupzyk, K. A., Pope Edwards, C., & Marvin, C. A. (2011). A randomized trial examining the effects of parent engagement on early language and literacy: The Getting Ready intervention. Journal of School Psychology, 49, 361–383. doi:10.1016/j.jsp.2011.03.001.
Shernoff, E. S., Maríñez-Lora, A., Frazier, S. L., Jakobsons, L., Atkins, M. S., & Bonner, D. (2011). Teachers supporting teachers in urban schools: What iterative research designs can teach us. School Psychology Review, 40, 465–485.
Shirk, S. R., & Jungbluth, N. J. (2008). School-based mental health checkups: Ready for practical action. Clinical Psychology: Science and Practice, 5, 217–223. doi:10.1111/j.1468-2850.2008.00131.x.
Spoth, R. L., Kavanagh, K. A., & Dishion, T. J. (2002). Family-centered preventive intervention science: Toward benefits to larger populations of children, youth, and families. Prevention Science, 3, 145–152. doi:10.1023/A:1019924615322.
Spoth, R., Trudeau, L., Shin, C., Ralston, E., Redmond, C., Greenberg, M., & Feinberg, M. (2013). Longitudinal effects of universal preventive intervention on prescription drug misuse: Three randomized controlled trials with late adolescents and young adults. American Journal of Public Health, 103, 665–672. doi: 10.2105/AJPH.2012.301209.
Stormshak, E. A., Connell, A. M., Véronneau, M-H., Myers, M. W., Dishion, T. J., Kavanagh, K., & Caruthers, A. S. (2011). An ecological approach to promoting early adolescent mental health and social adaptation: Family-centered intervention in public middle schools. Child Development, 82, 209–225. doi: 10.1111/j.1467-8624.2010.01551.x.
Stormshak, E. A., Connell, A. M., & Dishion, T. J. (2009). An adaptive approach to family-centered intervention in schools: Linking intervention engagement to academic outcomes in middle and high school. Prevention Science, 10, 221–235. doi:10.1007/s11121-009-0131-3.
Stormshak, E. A., & Dishion, T. J. (2002). An ecological approach to child and family clinical and counseling psychology. Clinical Child and Family Psychology Review, 5, 197–215. doi:10.1023/A:1019647131949.
Stormshak, E. A., & Dishion, T. J. (2009). A school-based, family-centered intervention to prevent substance use: The Family Check-Up. The American Journal of Drug and Alcohol Abuse, 35, 227–232. doi:10.1080/00952990903005908.
Stormshak, E. A., Dishion, T. J., Light, J., & Yasui, M. (2005). Implementing family-centered interventions within the public middle school: Linking service delivery to change in student problem behavior. Journal of Abnormal Child Psychology, 33, 723–733. doi:10.1007/s10802-005-7650-6.
Stormshak, E. A., Bierman, K. L., McMahon, R. J., Lengua, L., & Conduct Problems Prevention Research Group. (2000). Parenting practices and child disruptive behavior problems in early elementary school. Journal of Clinical Child Psychology, 29, 17–29. doi:10.1207/S15374424jccp2901_3.
Stormshak, E. A., Fosco, G. M., & Dishion, T. J. (2010). Implementing interventions with families in schools to increase youth school engagement: The Family Check-Up model. School Mental Health, 2, 82–92. doi:10.1007/s12310-009-9025-6.
Sugai, G., Horner, R. H., Dunlap, G., Hieneman, M., Lewis, T. J., Nelson, C. M., … Ruef, M. (2000). Applying positive behavioral support and functional assessment in schools. Journal of Positive Behavior Interventions, 2, 135–141. doi: 10.1177/109830070000200302
Turner, K. M., & Sanders, M. R. (2006). Dissemination of evidence-based parenting and family support strategies: Learning from the Triple P-Positive Parenting Program system approach. Aggression and Violent Behavior, 11, 176–193. doi:10.1016/j.avb.2005.07.005.
Van Ryzin, M. J., & Nowicka, P. (2013). Direct and indirect effects of a family-based intervention in early adolescence on parent–youth relationship quality, late adolescent health, and early adult obesity. Journal of Family, 27(1), 106–116. doi:10.1037/a0031428.
Walker, H. M., Colvin, G. R., & Ramsey, E. R. (1995). Antisocial behavior in school settings. Pacific Grove, CA: Brooks/Cole.
Weist, M. D. (2005). Fulfilling the promise of school-based mental health: Moving toward a public mental health promotion approach. Journal of Abnormal Child Psychology, 33, 735–741. doi:10.1007/s10802-005-7651-5.
Zubrick, S. R., Silburn, S. R., Garton, A., Burton, P., Dalby, R., Carlton, J., … Lawrence, D. (1995). Developing health and well-being in the Nineties. Western Australian Child Health Survey. Perth, WA, Australia: Australian Bureau of Statistics and the Institute for Child Health Research.
Acknowledgment
This work was supported by grant R324A09011 from the Institute of Education Sciences to John Seeley (PI) and Thomas Dishion (PI).
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2016 Springer International Publishing Switzerland
About this chapter
Cite this chapter
Stormshak, E.A., Brown, K.L., Moore, K.J., Dishion, T., Seeley, J., Smolkowski, K. (2016). Going to Scale with Family-Centered, School-Based Interventions: Challenges and Future Directions. In: Sheridan, S., Moorman Kim, E. (eds) Family-School Partnerships in Context. Research on Family-School Partnerships, vol 3. Springer, Cham. https://doi.org/10.1007/978-3-319-19228-4_2
Download citation
DOI: https://doi.org/10.1007/978-3-319-19228-4_2
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-19227-7
Online ISBN: 978-3-319-19228-4
eBook Packages: Behavioral Science and PsychologyBehavioral Science and Psychology (R0)