
Abstract
This chapter describes how School-Based Family Counseling (SBFC) may be used by mental health practitioners and educators to promote well-being in children, families, and schools. SBFC is defined and its historical roots in the work of Dr. Alfred Adler explained. Research describing the need for the SBFC approach is provided. The chapter explores the significant impact that both families and schools—the two most important social institutions affecting children—have on children’s well-being with specific reference to mental health and academic success. The nine strengths of SBFC are outlined: (1) school and family focus, (2) systems orientation, (3) educational focus, (4) parent partnership, (5) multicultural sensitivity, (6) child advocacy, (7) promotion of school transformation, (8) interdisciplinary focus, and (9) evidence-based support. SBFC theoretical models, such as Bronfenbrenner’s Ecological model, the SBFC metamodel, and the Circumplex Model, are described. Evidence-based support for SBFC, mainly in the form of randomized control group studies, is provided. The chapter provides examples of how SBFC is a global movement. The chapter concludes with a discussion of challenges experienced by SBFC and solutions that can be implemented.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
Introduction
School-Based Family Counseling (SBFC) is an integrated, systems approach designed to help children succeed academically and personally through mental health approaches that link school and family (Gerrard & Soriano, 2019). The fundamental premise behind SBFC is that the family and school are the two most important social systems affecting children and that by working simultaneously with both systems mental health practitioners are better able to enhance the well-being of children.
Origins of School-Based Family Counseling
The earliest large-scale application of SBFC was practiced by the psychiatrist Alfred Adler in Vienna in the 1920s. Adler believed that an especially effective way to help children was through conducting demonstration interviews with them, their teacher, and their parents, in front of an audience of mental health practitioners, parents, and teachers. Adler described his approach as follows:
The purpose of these clinics is to put the knowledge of modern psychology at the service of the educational system. A competent psychologist who understands not only psychology, but the life of the teachers and parents as well, joins with the teachers and holds a consultation clinic on a certain day. On that day the teachers will have a meeting, and each one will bring up his particular cases of problem children. They will be cases of lazy children, children who corrupt the class, children who steal, etc. The teacher describes his particular cases, and then the psychologist will contribute his own experiences. Then the discussion starts. What are the causes? When did the situation develop? What should be done? The family life of the child and his whole psychological development is analyzed. With their combined knowledge, the group comes to a decision as to what should be done with a particular child.
At the next session the child and the mother are both present. The mother will be called in first…Then the mother tells her side of the story, and a discussion starts between the mother and the psychologist…..When, finally, the method of influencing the child is agreed upon, the child enters the room. He sees the teacher and the psychologist, and the psychologist talks to him but not about his mistakes. The psychologist speaks as in a lecture, analyzing objectively - but in a manner that the child can grasp - the problems and the reasons and the ideas that are responsible for the failure to develop properly….
This summary account will give an indication of the possibilities that can be realized from the fusion of psychology and education. Psychology and education are two phases of the same reality and the same problem. (Adler, 1930, pp. 187–189)
The clinics that Adler referred to were 30 child guidance centers that he established throughout Venna. Each was attached to a school. At these clinics children, referred by teachers or parents, were seen by psychologists or psychiatrists trained by Adler. The mental health practitioners would work with the teachers and the parents to help children overcome their problems. These clinics, which Adler called “Advisory Clinics,” provided remedial assistance for children with existing problems. In addition, the clinics provided preventive work through demonstrations in an auditorium before an audience of mental health practitioners, teachers, and parents. This innovative linking of school and family is the essence of a School-Based Family Counseling approach.
During World War II, the Vienna guidance clinics were closed. Dr. Rudolf Dreikurs, a psychiatrist who trained with Adler, came to the USA during the 1940s and carried on Adler’s work. Dreikurs’ books Children the Challenge, written for parents, and Maintaining Sanity in the Classroom, written for teachers, illustrates the Adlerian SBFC approach (Dreikurs, 1958; Dreikurs, 1968). A comprehensive review of the development of SBFC from the 1940s to the present can be found in Gerrard (2008, 2013a). At a time, when Freudian therapists were emphasizing psychoanalysis with a patient on a couch in the analyst’s office, Adler was promoting the well-being of children, families, and schools through an educational and prevention approach. For that time, it was a revolutionary approach to mental health and presaged the school mental health and full-service school movements that developed in the 1990s (Dryfoos, 1994; Foster et al., 2005).
The Need for SBFC
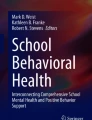
Success at school is widely considered critical for the well-being of children. As can be seen in Fig. 23.1, academic success is strongly correlated with unemployment and wages (US Bureau of Labor Statistics, 2016). Both unemployment and low wages are correlated with poor mental and physical health (McKee-Ryan et al., 2005; Pharr et al., 2012). Thus, when children fail academically, they are at risk for future problems associated with unemployment, low wages, and potential health and mental health problems.

USA unemployment rates and earnings by educational attainment, 2016
The Benefits of Parent Support for Children’s Well-Being and Academic Performance
There are several known factors that interfere with school success. Family problems, such as divorce, marital discord, domestic violence, parental mental illness, incarceration, substance abuse, family illness and death, siblings in gangs, neglect, physical and sexual abuse, are all known to be adverse childhood events (ACEs). All of these can produce negative outcomes in adulthood, including poor physical and mental health, substance abuse, and risky behaviors (e.g., unsafe sex) (Centers for Disease Control & Prevention, 2016).
When families are dysfunctional, for example, when parents are in the process of a divorce, there is often domestic violence, marital conflict, child abuse, and neglect or substance abuse. During marital discord, children often experience a variety of problems. These include behavior problems (Henderson et al., 2003; Jogdand & Naik, 2014; Morris et al., 2002) delinquency (Coll et al., 2004; Loeber & Stouthamer-Loeber, 1986), depression (Cummings, Keller, & Davies, 2005; Elgar et al, 2005), suicidality (DeVille et al, 2020; Zhai et al., 2015) risky peer behavior (Anyanwu et al., 2020; Haghdoost et al., 2014), and substance abuse (Bahr, 2005; Henry et al., 2004).
Not surprisingly, when children experience problems at home, it can have a negative effect on their ability to do well at school. Poor academic performance has been linked to lack of parental support (Lagana, 2004; Lara & Saracostti, 2019; Ponsford & Lapadat, 2001), divorce (Potter, 2010; Jeynes, 1998); mother absence (Ma, Deng & Zhou, 2018); and parental loss (Abdelnoor & Hollins, 2004; Berg et al., 2014). However, when parental support is strong, this has a positive effect on children’s academic performance (Anguiano, 2004; Chen & Gregory, 2009; Castro et al., 2015; Catalano & Catalano, 2014; Cheung & Pomerantz, 2011; Chohan & Khan, 2010; Deslandes & Cloutier, 2002; Eccles & Harold, 1996; Fan & Chen, 2001; Fan & Williams, 2010; Flouri & Buchanan, 2003; Garbacz et al, 2017; Grolnick et al, 2000; Grolnick & Slowiaczek, 1994; Hill et al, 2004; Hill & Tyson, 2009; Jeynes, 2009, 2016; Johnson et al., 2001; Newman et al., 2007; Patall et al., 2008; Ross, 2016; Shumow & Lomax, 2002; Simons-Morton & Crump, 2003; Spera, 2005; Wang et al., 2013; Wang & Eccles, 2012a, 2012b, 2013; Wilder, 2014).
Mental health practitioners who use an SBFC approach help children succeed at school by working with families to reduce the family stress that is negatively impacting the children. SBFC practitioners also collaborate with parents to increase their parental support and mobilize family resources and strengths to help improve children’s well-being and academic performance.
The Benefits of School Support on Children’s Well-Being and Academic Performance
Unsupportive school environments, such as the presence of bullying (Monks et al., 2005; Skrzypiec et al., 2011, 2012; Smith et al., 2015; Slee et al., 2003; Slee & Skrzypiec, 2016), low school cohesion (Maxwell et al., 2017; Springer et al, 2006), incompetent or harsh teachers (Banfield et al., 2006; Range et al., 2012; Yariv, 2011), can have a negative impact and directly affect children’s well-being and academic performance.
Extensive research demonstrates that supportive teachers, effective and caring school administrators and positive school climates benefit children’s well-being and promote school involvement and academic success (Aldridge et al., 2016; Chapman et al., 2013; Denman, 1999; Frydenberg et al., 2009; García-Moya et al., 2015; Huang et al., 2013; Jose & Pryor, 2010; Jose et al., 2012; Konishi et al., 2010; Lau & Li, 2011; Maddox & Prinz, 2003; McGraw et al, 2008; McNeely & Falci, 2004; Niehaus et al., 2012; Oberle et al., 2011; Prelow et al., 2007; Resnick et al., 1997; Shute & Slee, 2016; Svavarsdottir & Orlygsdottir, 2006; Thomson et al., 2015; Wang & Degol, 2016). Mental health practitioners who use an SBFC approach help children succeed at school by collaborating with teachers, principals, and other school staff to promote school cohesion and engagement.
The Strengths of SBFC
SBFC has nine strengths: family and school focus; systems orientation; educational focus; parent partnership; multicultural sensitivity; child advocacy; promotion of school transformation; interdisciplinary focus and evidence-based support.
Family and School Focus
The most distinguishing feature of SBFC is its focus on helping children by strengthening family and school relationships. This is in contrast with more traditional mental health approaches that focus solely on school intervention or on family intervention. The SBFC metamodel is a diagram that emphasizes the importance of family and school in prevention and intervention with children (Fig. 23.2).

The SBFC metamodel
The extensive research, previously reviewed, indicates that supportive family and school environments significantly impact children’s well-being and thus improve their academic performance. Therefore, the SBFC practitioner works with children to help strengthen their resilience in dealing with school and family challenges. They also work with the family to reduce family tensions that negatively impact children and mobilize family resources that empower them. Working with the school also improves school cohesion and engagement, reduces bullying, and strengthens school–family relationships. Other systems, such as the peer group and the community, are also the focus of intervention. But the main emphasis in an SBFC approach is the family and the school. These are the two main institutions that affect the lives of young children. During adolescence, the peer group becomes more important and can be more significant than the family in influencing student behavior. However, early intervention and prevention are widely viewed as more important in preventing children from developing more serious problems in adolescence and adulthood.
Systems Orientation
SBFC is a systems approach. The SBFC practitioner is constantly aware, and on the lookout for, how parents, grandparents, siblings, teachers, principals, friends, neighbors, and community organizations such as churches, synagogues, temples, mosques, sporting centers, etc., affect children. Bronfenbrenner’s ecological model (Ecological Systems Theory, 2020; Bronfenbrenner, 1979) is a useful model for SBFC practitioners because it directs attention to the multiple systems that can affect a child (see Fig. 23.3).

Bronfenbrenner’s ecological systems theory
SBFC practitioners typically work most often with a child’s Microsystem, Mesosystem, and Exosystem.
Microsystem: Refers to the institutions and groups that most immediately and directly impact the child’s development including: family, school, religious institutions, neighborhood, and peers.
Mesosystem: Consists of interconnections between the microsystems, for example between the family and teachers or between the child’s peers and the family.
Exosystem: Involves links between social settings that do not involve the child. For example, a child’s experience at home may be influenced by their parent’s experiences at work. A parent might receive a promotion that requires more travel, which in turn increases conflict with the other parent resulting in changes in their patterns of interaction with the child. (Wikipedia, July 13, 2020)
The systems theory most widely used by SBFC practitioners is family systems theory (Bowen, 1978). The central premise in family systems theory is that a family is a social system in which the behavior of every person has an influence on the behaviors of every other family member. Behavior of a child which appears “individual” may be the result of interpersonal influence, or “pressure” exerted by other family members. Family therapists frequently use the term “identified patient” to indicate the family member who demonstrates problem behavior or psychopathology (e.g., the child who throws temper tantrums at school and at home), but whose aberrant behavior is actually caused by dysfunctional behavior in the family (e.g., severe marital conflict in which the child is encouraged to take sides). You cannot treat the identified patient without treating the family.
An important family systems assessment approach is the Circumplex Model (Olson, 2000). In the Circumplex model, families are assessed on two key dimensions: Flexibility and Cohesion. Flexibility refers to the ability of a family to adapt to change. Families that are incapable of changing as situations demand are Rigid (e.g., have authoritarian parenting). Families that are overly reactive to change are Chaotic (e.g., lacking in parental discipline). Families between these opposite poles of Rigid and Chaotic are considered Flexible and are examples of healthy family systems. Cohesion refers to the degree of closeness between family members. Families that are overly close are Enmeshed (e.g., family members are overly dependent on each other, and independent thinking is discouraged). Families that lack closeness are Disengaged (e.g., no warmth between family members). Families that are between these opposite poles of Enmeshed and Disengaged are Connected and are examples of healthy family systems. Olson has developed instruments that can be used to measure Cohesion and Flexibility in order to position a family’s location on the Circumplex Map (see Fig. 23.4). It is important to note that the Circumplex Model does not diagnose individual behavior: it assesses relationships.

Circumplex model
The Circumplex Model can also be used to diagnose school relationships and relationships between schools and families. In Fig. 23.4, a Chaotically Disengaged family is shown in relationship to the school where the child is a student. A Chaotically Disengaged family would typically be one in which there are few family rules enforced. Members act very independently of each other. There is a lack of warmth and closeness between family members, and there is little parental authority exercised. The school as a whole is classified as Somewhat Flexible-Connected. This would be typically a school with very clear leadership by teachers and principal, rules that are enforced (but with some flexibility), and a school where staff and students have positive relationships. A student who might feel unaccepted in a Chaotically-Disengaged family, would likely feel more accepted in a Connected school. This same student might have difficulty conforming to school rules if they come from a Chaotic family where few rules are followed. The Circumplex Model is a systems assessment approach and can also be used to assess family–school relationships. In the example, we are currently considering the family and the school (denoted by the letters F-S) and have a rigidly–disengaged relationship. A typical illustration of this would be where the principal sent a letter to the parents complaining about the student not following rules and hinting that the family needs “therapy.” The parents in return did not respond to the letter which they found insulting. No further communication takes place between the school and the family.
As the SBFC practitioner does this type of systems analysis, the practitioner would also be thinking of ways to repair the family–school relationship by facilitating a more connected, collaborative relationship between principal and parents. Furthermore, the SBFC practitioner would be motivated to help the family become more connected and flexible and the school to be less rigid in dealing with the family. That is, the SBFC focus is on modifying relationship systems. Peer group relationships and relationships between dyads (two person groups, such as mother–child, child–teacher, father–principal, principal–teacher) can also be diagrammed on the Circumplex Model (Gerrard, 2015).
Educational Focus
School mental health professionals, such as school social workers, school counselors, and school psychologists, are trained to work directly with students to assist them with school problems. Because the traditional school mental health practitioner is not trained in family systems intervention, when students present with family problems, school personnel will typically refer the family to a community mental health center that offers family therapy. But frequently the family does not accept the referral and resents the implied message that something is wrong with the parents and that “therapy” is needed. Also, many families regard mental health therapy as a sign they are “crazy.” Many mental health researchers acknowledge that the social stigma concern can be a barrier to seeking professional help (Bathje & Pryor, 2011; Corrigan, 2004). The emphasis in the SBFC approach is not on “therapy,” but on promoting the academic success of children. This explicit educational focus is more appealing to parents who typically are eager to have their child succeed at school. Thus, inviting a parent to meet with the SBFC practitioner to discuss ways to help a son or daughter do better at school is less threatening than being invited to meet with a mental health professional to discuss family problems. During the session when the SBFC practitioner assists parents to help their child do better at school, ways of lowering family stresses are discussed, but always in an educational context. The framing of the work between the family and the SBFC practitioner as educational avoids the use of language that frames the family as deficient.
Parent Partnership
In an SBFC approach, the relationship between the parents (or guardians) and the SBFC practitioner is framed as a collaborative partnership where the two parties meet to identify ways to help the child succeed at school. This is in contrast to the therapist–client frame of mental health which is hierarchical and implies a deficiency on the part of the client. Treating the parents and family as partners is important because in every family there is typically one or more family members who will be a source of strength and empowerment for a child who is struggling academically. The parent partnership approach is respectful of the parents’ roles and defuses parents’ feelings of concern about meeting with a mental health professional. In many situations, the difficulty the child is having at school is precipitated by actual events at the school, for example, incompetent teachers, low school cohesion, bullying, etc. To resolve some of these issues, a school intervention would be appropriate.
Multicultural Sensitivity
Most psychotherapy and mental health approaches were developed in Europe and America and, as such, are Eurocentric or Americentric in nature. That is, they emphasize the importance of the individual and stress concepts like assertiveness and independence. However, many clients come from collectivistic cultural backgrounds where values such as interdependence and being family-oriented are considered more important. These Western individualistic approaches to mental health are culturally inappropriate with Asian, African, Middle Eastern, Latinx, First Nations Peoples (e.g., Native American), and other ethnic groups (Gopalkrishnan, 2018; Sue & Sue, 2008).
Much of the theory and practice of mental health, including psychiatry and mainstream psychology, have emerged from Western cultural traditions and Western understandings of the human condition. Notions of Cartesian dualism of body and mind, positivism, and reductionism have been central to the development of mainstream mental health systems as they are widely implemented today (8, 9). While these relatively monocultural understandings of mental health have provided powerful conceptual tools and frameworks for the alleviation of mental distress in many settings, they have also been very problematic when applied to the context of non-Western cultures without consideration of the complexity that working across cultures brings with it (10, 11). Tribe [(1), p. 8] suggests that Western cultural approaches to health tend to be “predicated on a model that focuses on individual intrapsychic experience or individual pathology, while other traditions may be based more on community or familial processes.” (Gopalkrishnan, 2018, p. 179)
Although SBFC was developed in the West, it is not a typical Eurocentric or Americentric mental health approach. It is a systems approach. Family, as a resource, is a primary focus. This family-centric emphasis makes SBFC culturally congruent with a wide spectrum of families with different cultural backgrounds.
Child Advocacy
Although SBFC practitioners work to strengthen the well-being of families and school personnel, they are first and foremost advocates for children. Clearly, children are more vulnerable and require greater protection. As the child advocate, the SBFC practitioner must establish an effective relationship with families and schools and frequently act as advocates for both families and schools. However, in the advocacy hierarchy, children are the top priority.
Promotion of School Transformation
Schools, like families and individual clients, can be dysfunctional. Research reviewed above demonstrates some of the ways schools can be dysfunctional: for example, bullying may be common, school engagement and cohesion can be minimal, and teachers are sometimes harsh or incompetent. These problems seriously interfere with a student’s well-being and academic performance. Effecting change in the behavior of principals or teachers is challenging for the SBFC practitioner who often is employed by the school and whose immediate supervisor may be the principal. It is therefore imperative that SBFC practitioners develop good working relationships with school personnel and have the courage to “speak truth to power” in a way that does not alienate. The family therapist, Salvador Minuchin, wrote of the central importance of the family therapist being able to “join” with the family as though the therapist were a distant uncle or aunt. This, too, is an important skill for SBFC practitioners in their relationship with school personnel.
Interdisciplinary Focus
Within the mental health professions, SBFC is an interdisciplinary approach. It may be used by any of the mental health disciplines: psychology (school psychology, family psychology), counseling (school counseling, family counseling), social work and school social work, psychiatry, and family therapy. The term SBFC practitioner, or SBFC professional, is used to denote the interdisciplinary nature of SBFC. What is important about SBFC is not the theoretical orientation (e.g., behavioral or humanistic) or the mental health discipline, but the use of a systems focus with an emphasis on how family and school systems influence children. The SBFC metamodel in Fig. 23.5 illustrates some of the categories of intervention and prevention that an SBFC practitioner with any theoretical or discipline orientation could consider in helping their client, the child.

The SBFC metamodel with prevention and intervention categories
Let us use one category as an example: Group Counseling under the School Intervention category. Group counseling is a useful intervention when several students are experiencing the same problem (e.g., death of a family member or dealing with bullies). However, the SBFC practitioner can implement a group counseling program from a behavioral or humanistic perspective, or perhaps a combination of the two. If the mental health practitioner is willing to adopt the SBFC perspective—which is granted as a theoretical perspective—the practitioner can use its flexibility within the general theoretical orientation of the mental health discipline in which they were trained. In this sense, the SBFC approach should be viewed as a value-added element to any mental health practitioner’s training.
Evidence-Based Support
There is modest evidence-based support for SBFC in eight randomized control group studies comparing school and family intervention with school only or family only intervention (see Box 23.1). In all 8 studies, the combined treatment (the SBFC intervention) was superior. In addition to these RCT studies, there is extensive correlational and qualitative research supporting the SBFC approach (Gerrard, 2008, 2013b).
Box 23.1 Evidence-Based Support for SBFC
Apisitwasana, Perngparn, U., & Cottler, L. (2018). Effectiveness of school- and family-based interventions to prevent gaming addiction among grades 4–5 students in Bangkok, Thailand. Psychology Research and Behavior Management, 11, 103–115. https://doi.org/10.2147/PRBM.S145868
Conduct Problems Prevention Research Group. (2007). Fast track randomized controlled trial to prevent externalizing psychiatric disorders: Findings from grades 3 to 9. Journal of the American Academy of Child and Adolescent Psychiatry, 46(10), 1250–1262. https://doi.org/10.1097/chi.0b013e31813e5d39
Crozier, M., Rokutani, L., Russett, J., Godwin, E., & Banks G. (2010). A multisite program evaluation of families and schools together (FAST): Continued evidence of a successful multifamily community-based prevention program. The School Community Journal, 20 (1), 187–207. ERIC: EJ891838.
Eddy, J., Reid, J., & Fetrow, R. (2000). An Elementary School-Based Prevention Program Targeting Modifiable Antecedents of Youth Delinquency and Violence: Linking the Interests of Families and Teachers (LIFT). Journal of Emotional and Behavioral Disorders, 8(3) 165–176.
Flay, B., Graumlich S., Segawa, E., Burns, J., Amuwo, S., Bell, C., Campbell, R., Cowell, J., Cooksey, J., Dancy, B., Hedeker, D., Jagers, R., Levy, S., Paikoff, R., Punwani, I, &Weisberg, R. (2004). Effects of 2 prevention programs on high-risk behaviors among African American youth: A randomized trial. Archives of Pediatrics and Adolescent Medicine, 158(4), 377–384. https://doi.org/10.1001/archpedi.158.4.377
Kratochwill, T., McDonald, L., Levin, J., Scalia, P., & Coover, G. (2009). Families and schools together: An experimental study of multi-family support groups for children at risk. Journal of School Psychology, 47, 245–265. https://doi.org/10.1016/j.jsp.2009.03.001
Kratochwill, T., McDonald, L., Levin, J., Bear-Tibbetts, H., & Demaray, M. (2004). Families and Schools Together: an experimental analysis of a parent-mediated multi-family group program for American Indian children. Journal of School Psychology, 42(5), 359–383.
Lochman J., & Wells K. (2004). The coping power program for preadolescent aggressive boys and their parents: outcome effects at the 1-year follow-up. Journal of Consulting and Clinical Psychology, 72(4), 571–578.
SBFC is a Global Movement
SBFC, although developed in the West, has evolved into a global movement. The Oxford Symposium in School-Based Family Counseling, an international association, meets annually at Oxford University and other international sites. Its mission is to promote SBFC worldwide. To date, members come from approximately 20 countries. The International Journal for School-Based Family Counseling is an SBFC resource containing articles on SBFC as applied to immigrant families in New Zealand (Everts, 2008); school violence in South Africa (Marchetti-Mercer, 2008); assessing Chinese families in Macao (van Schalkwyk, 2010); school refusal in Hong Kong (King, 2012); using reflecting teams in SBFC in the UK (Agudelo, 2017); Black fathers and autistic children in the USA (Hannon, 2017), and other topics presented at the yearly international conference held at Brasenose College, Oxford; Venice International University; the University of Barcelona; and the University of Hong Kong. During the 2020 coronavirus pandemic, a Special Interest Group of the Oxford Symposium in SBFC, called the Disastershock Global Volunteer Team, translated the book Disastershock: How to Cope with the Emotional Stress of a Major Disaster (Gerrard et al., 2020) into 25 different languages. This practical stress reduction book, written for parents, teachers, and other professionals working with children, was then distributed by the 101 person global team as a free ebook to countries around the world (“Disastershock,” 2020). In winter 2021, members of the Disastershock Educator Collaborative Team developed a book called Disastershock: How Schools Can Cope with the Emotional Stress of a Major Disaster, a Manual for Principals and Teachers (Disastershock Educator Collaboration Team, 2021). This ebook is also available free on the website https://www.disastershock.com.
The largest SBFC program is Place2Be, a UK organization that provides integrated school and family counseling in over 300 schools in England, Scotland, and Wales (Adams-Langley & Everts, 2013). The Sifriyat Pijama program in Israel uses a home and school-based approach to promoting reading literacy in a way that promotes school and family cohesion, fosters cultural identity of children, and empowers disadvantaged families (Hareven, 2019). The Center for Child and Family Development in the San Francisco Bay area is an SBFC university–schools partnership that has served over 20,000 children and families in 70 public, private, and Catholic schools over a 35 year period.
The first masters’ degree program in SBFC was offered at California State University, Los Angeles, in 1992 (Carter & Perluss, 2008). Certificates in SBFC approaches may be earned at Central Connecticut University and at Loyola University, Chicago (which also offers continuing education training in SBFC through the Family and School Partnership Program).
SBFC Challenges and Solutions
There are three common challenges faced by mental health practitioners and educators who want to develop SBFC programs: the “silo” nature of mental health professional training, difficulties in engaging parent and family involvement, and funding SBFC programs.
Challenge: “Silo” Professional Training
Because most mental health professionals are trained in a narrow “silo” approach to mental health that does not emphasize collaboration between the mental health disciplines, it may be difficult for some mental health professionals to adopt the systems approach required to practice SBFC. This tendency for the mental health disciplines to operate in isolation from each other, even to the point of engaging in “turf wars” with each other, is a major barrier to developing SBFC programs (Carter et al., 2017; Soriano, 2017). There are, however, strategies that can be used to minimize inter-professional competition and maximize collaboration with other mental health professions in a school district where one wishes to implement an SBFC program. These include: making a concerted effort to collaborate with other mental health professionals working in schools; becoming familiar with approaches used by other mental health disciplines by reading their literature; emphasizing that SBFC is an additive approach to the other mental health disciplines, not a replacement for them; using neutral, interdisciplinary language, e.g., terms like SBFC practitioner and SBFC professional; being familiar with the evidence-based support for SBFC (Carter et al., 2017; Powers & Swick, 2017). Mental health practitioners who are trained only in school or family mental health approaches, can develop an SBFC perspective by taking continuing education in the approaches they are less familiar with. They can also develop an SBFC team by collaborating with a mental health professional who has the training and skills they currently lack. For example, a traditional school mental health professional could collaborate with a traditional family therapy professional, and thereby learn from each other as they link school and family interventions.
Challenge: Engaging Parent and Family Support
Engaging low-income families in SBFC presents challenges. Parents’ work schedules may make it difficult or impossible to attend counseling during normal workday hours. As an SBFC solution, the flexibility of the practitioner is important. Stepping away from the normal 9–5 workday with staggered hours of, e.g.,12–8 p.m. and availability to meet with parents on Saturday mornings, is helpful. But this requires administrative support and an appreciation of the parents’ dilemma. Asking a low-income parent to miss work to attend a counseling session is simply unreasonable. Although the literature clearly indicates that students’ success in school depends, to a great extent, on the degree of parent engagement, many school districts communicate with low-income families in a manner that marginalizes them (Strickland & Lyutykh, 2020). SBFC addresses this issue by communicating with parents with respect, engaging them as equal partners to promote their children’s success, and frames the purpose of the parent–SBFC practitioner meeting as “educational” rather than “mental health/therapy.”
Challenge: Funding of SBFC Programs
Any mental health program in schools requires funding, and this can be a challenge for developing a new SBFC program in a school district. Mental health practitioners and educators who want to develop an SBFC program can provide evidence-based support for administrators who make program decisions. The research evidence supports a combined school and family mental health intervention as being more effective than a school only or a family only approach in helping children succeed at school (see Evidence-Based Support above). Presenting this information to school principals, and school district superintendents, may facilitate SBFC program funding. The Center for Child & Family Development, an SBFC program in San Francisco, utilizes a cost-effective approach by staffing schools with masters-level trainees in Marital and Family Therapy. These trainees are provided with SBFC in-service training to complement their traditional family therapy training and prepare them to work in school environments. The schools are charged a nominal fee which is a fraction of what it would cost to hire a full-time licensed mental health professional. This university–schools partnership program has provided more than 20,000 children and families with SBFC services in over 70 San Francisco Bay area public and private schools over a 35 year period (Gerrard, 2013b). The Place2Be SBFC program which is in over 300 schools in the UK receives funding from multiple sources: schools, corporate donors, and grants (Place2Be: Improving Children’s Mental Health in Schools, 2020).
Ultimately, the maintenance of an effective SBFC program requires visionary leadership, adequate funding, and political skills to negotiate challenges. Persons wishing to implement a SBFC program will find useful guides in the SBFC texts: School-Based Family Counseling: An interdisciplinary guide (Gerrard et al., 2020) and School-Based Family Counseling: Transforming family–school relationships (Gerrard & Soriano, 2013). The bibliography at the end of this chapter contains additional resources helpful for developing and maintaining an SBFC program to benefit the well-being of children, families, and schools.
Bibliography
Boyd-Franklin, L., & Hafer Bry, B. (2000). Reaching out in family therapy. The Guilford Press.
Fine, M. J., & Carlson C. (Eds.). (1992). Family-school intervention: A systems perspective. Allyn and Bacon.
Gerrard, B., & Soriano, M. (Eds.). (2013). School-based family counseling: Transforming family-school relationships. CreateSpace.
Gerrard, B., Carter, M., & Ribera, D. (Eds.). (2019). School-based family counseling: An interdisciplinary practitioner’s guide. Routledge.
Hinckle, J., & Wells, M. (1995). Family counseling in the schools. ERIC/CASS Publications.
Laundy, K. C. (2015). Building school-based collaborative mental health teams: A systems approach to student achievement. TPI Press.
Miller, L. D. (Ed.). (2002). Integrating school and family counseling: Practical solutions. American Counseling Association.
Palmatier, L. L. (1998). Crisis counseling for a quality school community: A family perspective. Taylor & Francis.
Sherman, R., Shumsky, A., & Roundtree, Y. (1994). Enlarging the therapeutic circle. Brunner/Mazel.
Sheridan, S., & Kratochwill, T. (2008). Conjoint behavioral consultation, promoting family-based connections and interventions. Springer.
Shute, R., & Slee, P. (Eds.). (2016). Mental health and wellbeing through schools: The way forward. Routledge.
Steele, W., & Raider, M. (1991). Working with families in crisis: School-based intervention. The Guilford Press.
Walsh, W., & Williams, G. (1997). Schools and family therapy: Using systems theory and family therapy in the resolution of school problems. Charles C. Thomas.
References
Abdelnoor, A., & Hollins, S. (2004). The effect of childhood bereavement on secondary school performance. Educational Psychology in Practice,20(1), 43–54.
Adams-Langley, S., & Everts, H. E. (2013). Place2Be in the inner city: A school-based mental health service in the United Kingdom. International Journal for School-Based Family Counseling, 2013/2014, 1–14.
Adler, A. (1930). The education of children. Gateway.
Agudelo, J. (2017). Using reflecting teams in school-based family counseling. International Journal for School-Based Family Counseling,8, 1–11.
Aldridge, J. M., Fraser, B. J., Fozdar, F., Ala’l K., Earnest, J., & Afari, E. (2016). Students’ perceptions of school climate as determinants of wellbeing, resilience and identity. Improving Schools, 19(1), 5–26.
Anguiano, R. P. (2004). Families and schools: The effect of parental involvement on high school completion. Journal of Family Issues,25, 61–85.
Anyanwu, F., Akinsola, H., Tugli, A., & Obisie-Nmehielle, N. (2020). A qualitative assessment of the influence of family dynamics on adolescents’ sexual risk behaviour in a migration-affected community. International Journal of Qualitative Studies on Health and Well-Being,15, 1. https://doi.org/10.1080/17482631.2020.1717322
Bahr, S., Hoffmann, J., & Yang, X. (2005). Parental and peer influences on the risk of adolescent drug use. Journal of Primary Prevention,26, 529–551.
Banfield, S. R., Richmond, V. P., & McCroskey, J. C. (2006). The effect of teacher misbehaviors on teacher credibility and affect for the teacher. Communication Education,55, 63–71.
Bathje, G., & Pryor, J. (2011). The relationships of public and self-stigma to seeking mental health services. Journal of Mental Health Counseling,33, 161–176.
Berg, L., Rostila, M., Saarela, J., & Hjern, A. (2014). Parental death during childhood and subsequent school performance. Pediatrics, 682–689. https://doi.org/10.1542/peds.2013-2771
Bowen, M. (1978). Family Therapy in Clinical Practice. Jason Aronson.
Bronfenbrenner, U. (1979). The ecology of human development: Experiments by nature and design. Harvard University Press.
Carter, M., Garner, W., Geiger, P., Gerrard, B., & Soriano, M. (2017). Reducing inter-professional barriers affecting school-based family counseling. International Journal for School-Based Family Counseling, Special Topic Issue, 1–25.
Carter, M., & Perluss, E. (2008). Developments in training school-based family counselors: The school-based family counseling (SBFC) graduate program at California State University, Los Angeles. International Journal for School-Based Family Counseling,1, 1–12.
Castro, M., Expósito-Casas, E., López-Martín, E., Lizasoain, L., Navarro-Asencio, E., & Gaviria, J. (2015). Parental involvement on student academic achievement: A meta-analysis. Educational Research and Reviews, 14, 33–46. https://doi.org/10.1016/j.edurev.2015.01.002
Catalano, H., & Catalano, C. (2014). The importance of the school-family relationship in the child’s intellectual and social development. Procedia—Social and Behavioral Sciences,128, 406–414. https://doi.org/10.1016/j.sbspro.2014.03.179
Centers for Disease Control and Prevention. (2016). About the CDC-Kaiser ACE study: Major findings. Retrieved from https://www.cdc.gov/violenceprevention/acestudy/about.html
Chapman, R. L., Buckley, L., Sheehan, M., & Shochet, I. (2013). School-based programs for increasing connectedness and reducing risk behaviour: A systematic review. Educational Psychology Review,25(1), 95–114.
Chen, W., & Gregory, A. (2009). Parental involvement as a protective factor during the transition to high school. Journal of Educational Research,103, 53–62.
Cheung, C. S., & Pomerantz, E. M. (2011). Parents’ involvement in children’s learning in the United States and China: Implications for children’s academic and emotional adjustment. Child Development,82, 932–950.
Chohan, B., & Khan, R. (2010). Impact of parental support on the academic performance and self-concept of the student. Journal of Research and Reflections in Education,4(1), 14–26.
Coll, K., Thobro, P., & Haas, R. (2004). Relational and purpose development in youth offenders. Journal of Humanistic Counseling Education and Development,43(1), 41–46.
Corrigan, P. (2004). How stigma interferes with mental health care. American Psychologist,59, 614–625.
Cummings, E., Keller, P., & Davies, P. (2005). Towards a family process model of maternal and paternal depressive symptoms: Exploring multiple relations with child and family functioning. Journal of Child Psychology and Psychiatry, 46(5), 479–489. https://doi.org/10.1111/j.1469-7610.2004.00368.x
Denman, S. (1999). Health promoting schools in England—A way forward in development. Journal of Public Health Medicine,21(2), 215–220.
Deslandes, R., & Cloutier, R. (2002). Adolescents’ perception of parental involvement in schooling. School Psychology International,23, 220–232.
DeVille, D., Whalen, D., Breslin, F., Morris, A., Khalsa, S., Paulus, M., & Barch, D. (2020). Prevalence and family-related factors associated with suicidal ideation, suicide attempts, and self-injury in children aged 9–10 years. JAMA Network Open, 3(2). https://doi.org/10.1001/jamanetworkopen.2019.20956
Disastershock Educator Collaboration Team. (2021, May 10). Disastershock: How schools can cope with the emotional stress of a major disaster, a manual for principals and teachers. Retrieved from https://www.disastershock.com/educators-disasters
Dreikurs, R. (1958). Children: The challenge. Norton.
Dreikurs, R. (1968). Maintaining sanity in the classroom. Harper & Row.
Dryfoos, J. (1994). Full-service schools: A revolution in health and social services for children, youth, and families. Jossey-Bass.
Eccles, J. S., & Harold, R. D. (1996). Family involvement in children’s and adolescents’ schooling. In A. Booth & J. F. Dunn (Eds.), Family-school links: How do they affect educational outcomes? (pp. 3–34). Erlbaum.
Ecological Systems Theory. (2020). In Wikipedia, Retrieved July 13, 2020 https://en.wikipedia.org/wiki/Ecological_systems_theory
Elgar, F., McGrath, P., Waschbusch, D., Stewart, S., & Curtis, L. (2005). Mutual influences on maternal depression and child adjustment problems. Clinical Psychology Review,24(2004), 441–459.
Everts, H. (2008). Integrating supportive care in schools with the enhancement of family resilience—A New Zealand project for immigrant families. International Journal for School-Based Family Counseling,1, 1–11.
Fan, X., & Chen, M. (2001). Parental involvement and students’ academic achievement: A meta-analysis. Educational Psychology Review,13, 1–22.
Fan, W., & Williams, C. (2010). The effects of parental involvement on students’ academic self-efficacy, engagement and intrinsic motivation. Educational Psychology,30, 53–74.
Flouri, E., & Buchanan, A. (2003). The role of father involvement and mother involvement in adolescents’ psychological well-being. British Journal of Social Work,33, 399–406.
Foster, S., Rollefson, M., Doksum, T., Noonan, D., & Robinson, G. (2005). School mental health services in the United States, 2002–2003. Center for Mental Health Services, Substance Abuse and Mental Health Services Administration.
Frydenberg, E., Care, E., Freeman, E., & Chan, E. (2009). Interrelationships between coping, school connectedness and wellbeing. Australian Journal of Education,53(3), 261–276.
Garbacz, S., Herman, K., Thompson, A., & Reinke, W. (2017). Family engagement in education and intervention: Implementation and evaluation to maximize family, school, and student outcomes. Journal of School Psychology,62, 1–10. https://doi.org/10.1016/j.jsp.2017.04.002
García-Moya, I., Brooks, F., Morgan, A., & Moreno, C. (2015). Subjective well-being in adolescence and teacher connectedness. A health asset analysis. Health Education Journal, 74(6), 641–654.
Gerrard, B. (2008). School-based family counseling: Overview, trends, and recommendations for future research. International Journal for School-Based Family Counseling,1, 1–30.
Gerrard, B., & Soriano, M. (2019). School-based family counselling: The revolutionary paradigm. In B. Gerrard, M. Carter, & D. Ribera (Eds.), School-based family counselling: An interdisciplinary practitioner’s guide (pp. 1–15). Routledge.
Gerrard, B., Girault, E., Appleton, V., Giraudo, S., & Shaffer, S. L. (2020, July 15). Disastershock: How to cope with the emotional stress of a major disaster. Retrieved from https://www.disastershock.com/
Gerrard, B., Girault, E., Appleton, V., Giraudo, S., & Shaffer, S. L. (2020). Disastershock: How to cope with the stress of a major disaster. Oxford Symposium in School-Based family Counseling.
Gerrard, B. (2013a). SBFC: A Re-emerging paradigm. In B. Gerrard & M. Soriano (Eds.), School-based family counseling: Transforming family–school relationships (pp. 16–36). Createspace.
Gerrard, B. (2013b). Mission possible: A 3o year university-schools partnership in school-based family counseling. In B. Gerrard & M. Soriano (Eds.), School-based family counseling: Transforming family–school relationships (pp. 709–725). Createspace.
Gerrard, B. (2015). Trans-system assessment: A strategy for improving school-based family counseling.International Journal for School-Based Family Counseling,5, 1–14.
Gerrard, B. (2020). How to develop an SBFC case conceptualization. In B. Gerrard, M. Carter, & D. Ribera (Eds.), School-based family counseling: An interdisciplinary practitioner’s guide (pp. 16–67). Routledge.
Gopalkrishnan, N. (2018). Cultural diversity and mental health: Considerations for policy and practice. Frontiers of Public Health.,6, 179–193.
Gorman-Smith, D., Tolan, P., Loeber, R., et al. (1998). Relation of family problems to patterns of delinquent involvement among urban youth. Journal of Abnormal Child Psychology,26, 319–333. https://doi.org/10.1023/A:1021995621302
Grolnick, W. S., & Slowiaczek, M. L. (1994). Parents’ involvement in children’s schooling: A multidimensional conceptualization and motivational model. Child Development,65, 237–252.
Grolnick, W. S., Kurowski, C. O., Dunlap, K. G., & Hevey, C. (2000). Parental resources and the transition to junior high. Journal of Research on Adolescence,10, 465–488.
Haghdoost, A., Abazari, F., Abbaszadeh, A., & Rabori, E. (2014). Family and the risky behaviors of high school students. Iranian Red Crescent Medical Journal, 16(10). https://doi.org/10.5812/ircmj.15931
Hannon, M. (2017). Black American fathers, their children with autism, and the utility of school-based family counseling: A narrative inquiry. International Journal for School-Based Family Counseling,8, 1–16.
Hareven, S. (2019). Promoting home reading and ethnic identity through national book programs: The experience of Pajama Library (“Sifriyat Pijama”) and Lantern Library (“Maktabat al-Fanoos”) in Israel. Presentation at the 2019 Oxford Symposium in School-Based Family Counseling. https://www.oxfordsymposium-sbfc.com/2020-presentation-abstracts
Henderson, A., Sager, T., & Horne, A. (2003). Mothers and sons: A look at the relationship between child behavior problems, marital satisfaction, maternal depression, and family cohesion. Family Journal: Counseling and Therapy for Couples and Families,11(1), 33–41.
Henry, C., Robinson, L., & Wilson, S. (2004). Adolescent perceptions of their family system, parents’ behavior, self-esteem, and family life. Journal of Child and Adolescent Substance Abuse,13(2), 29–59.
Hill, N. E., & Tyson, D. F. (2009). Parental involvement in middle school: A meta-analytic assessment of the strategies that promote achievement. Developmental Psychology,45, 740–763.
Hill, N. E., Castellino, D. R., Lansford, J. E., Nowlin, P., Dodge, K. A., Bates, J. E., et al. (2004). Parent academic involvement as related to school behavior, achievement, and aspirations: Demographic variations across adolescence. Child Development,75, 1491–1509.
Huang, K., Cheng, S., & Theise, R. (2013). School contexts as social determinants of child health: Current practices and implications for future public health practice. Public Health Reports,128(S3), 21–28.
Jeynes, W. (1998). Does divorce or remarriage have the greater negative impact on the academic achievement of children? Journal of Divorce & Remarriage,29(1–2), 79–101. https://doi.org/10.1300/J087v29n01_05
Jeynes, W. H. (2009). The relationship between parental involvement and urban secondary school student academic achievement: A meta-analysis. Urban Education,42, 82–92.
Jeynes, W. H. (2016). A meta-analysis: The relationship between parental involvement and Latino student outcomes. Education and Urban Society,49, 4–28. https://doi.org/10.1177/0013124516630596
Jogdand, S., & Naik, J. (2014). Study of family factors in association with behavior problems amongst children of 6–18 years age group. International Journal of Applied and Basic Medical Research,4(2), 86–89. https://doi.org/10.4103/2229-516X.136783
Johnson, M. K., Crosnoe, R., & Elder, G. H., Jr. (2001). Students’ attachment and academic engagement: The role of race and ethnicity. Sociology of Education,74, 318–340.
Jose, P. E., & Pryor, J. (2010). New Zealand youth benefit from being connected to their family, school, peer group and community. Youth Studies Australia,29(4), 30–37.
Jose, P. E., Ryan, N., & Pryor, J. (2012). Does social connectedness promote a greater sense of well-being in adolescence over time? Journal of Research on Adolescence,22(2), 235–251.
King, L. Y. (2012). A multiple-family group with youngsters who refuse to attend school: Learning and implications for school-based family counseling. International Journal for School-Based Family Counseling,2, 1–15.
Konishi, C., Hymel, S., Zumbo, B. D., & Li, Z. (2010). Do school bullying and student teacher relationships matter for academic achievement? A multilevel analysis. Canadian Journal of School Psychology,25(1), 19–39.
Lagana, M. (2004). Protective factors for inner-city adolescents at risk of school dropout: Family factors and social support. Children & Schools,26(4), 211–220.
Lara, L., & Saracostti, M. (2019, June 27). Effect of parental involvement on children’s academic achievement in Chile. Frontiers in Psychology. https://doi.org/10.3389/fpsyg.2019.01464
Lau, M., & Li, W. (2011). The extent of family and school social capital promoting positive subjective well-being among primary school children in Shenzhen, China. Children and Youth Services Review,33(9), 1573–1582.
Loeber, R., & Stouthamer-Loeber, M. (1986). Family factors as correlates and predictors of juvenile conduct problems and delinquency. Crime and Justice,7, 29–149.
Ma, X., Deng, W., & Zhou, A. (2018, September 10). The link between parental absence and poor reading comprehension: Evidence from the left-behind children in rural China. Frontiers of Education. https://doi.org/10.3389/feduc.2018.00071
Maddox, S. J., & Prinz, R. J. (2003). School bonding in children and adolescents: Conceptualization, assessment, and associated variables. Clinical Child and Family Psychology Review,6(1), 31–49.
Marchetti-Mercer, M. (2008). The value of using a school-based family counseling approach following an incident of school violence: A case study. International Journal for School-Based Family Counseling, 1, 1–15.
Maxwell, S., Reynolds, K., Lee, E., Subasic, E., & Bromhead, D. (2017, 05 December). The impact of school climate and school identification on academic achievement: Multilevel modeling with student and teacher data. Frontiers of Psychology, 2017. https://doi.org/10.3389/fpsyg.2017.02069
McGraw, K., Moore, S., Fuller, A., & Bates, G. (2008). Family, peer and school connectedness in final year secondary school students. Australian Psychologist,43(1), 27–37.
McKee-Ryan, F., Song, Z., Wanberg, C., & Kinicki, A. (2005). Psychological and physical well-being during unemployment: A meta-analytic study. Journal of Applied Psychology,90(1), 53–76.
McNeely, C., & Falci, C. (2004). School connectedness and the transition into and out of health-risk behavior among adolescents: A comparison of social belonging and teacher support. Journal of School Health,74(7), 284–292.
Monks, C. P., Smith, P. K., & Swettenham, J. (2005). Psychological correlates of peer victimization in preschool: Social cognitive skills, executive function and attachment profiles. Aggressive Behavior,31(6), 1–18.
Morris, A., Silk, J., Steinberg, L., Sessa, F., Avenevoli, S., & Essex, M. (2002). Temperamental vulnerability and negative parenting as interacting predictors of child adjustment. Journal of Marriage and Family,64(2), 461–471.
Newman, B., Newman, P., Griffen, S., O’Connor, K., & Spas, J. (2007). The relationship of social support to depressive symptoms during the transition to high school. Adolescence,42, 441–459.
Niehaus, K., Rudasill, K. M., & Rakes, C. R. (2012). A longitudinal study of school connectedness and academic outcomes across sixth grade. Journal of School Psychology,50(4), 443–460.
Oberle, E., Schonert-Reichl, K. A., & Zumbo, B. D. (2011). Life satisfaction in early adolescence: Personal, neighborhood, school, family, and peer influences. Journal of Youth and Adolescence,40(7), 899–901.
Olson, D. (2000). Circumplex model of marital and family systems. Journal of Family Therapy,22, 144–167.
Patall, E. A., Cooper, H., & Robinson, J. C. (2008). Parent involvement in homework: A research synthesis. Review of Educational Research,78, 1039–1101.
Pharr, J., Moonie, S., & Bungum, T. (2012). The impact of unemployment on mental and physical health, access to health care and health risk behaviors. International Scholarly Research Notes, 2012, 7p., Article ID 483432 https://doi.org/10.5402/2012/483432
Place2Be: Improving Children’s Mental Health in Schools. (2020). Retrieved 7/26/2020 from https://www.place2be.org.uk/
Ponsford, K., & Lapadat, J. (2001). Academically capable students who are failing in high school: Perceptions about achievement. Canadian Journal of Counselling,35(2), 137–156.
Potter, D. (2010). Psychosocial well-being and the relationship between divorce and children’s academic achievement. Journal of Marriage and Family,72(4), 933–946. https://doi.org/10.1111/j.1741-3737.2010.00740.x
Powers, J., & Swick, D. (2017). Establishing and maintaining successful university-school partnerships in school-based research. International Journal for School-Based Family Counseling, Special Topic Issue, 1–7.
Prelow, H. M., Bowman, M. A., & Weaver, S. R. (2007). Predictors of psychosocial wellbeing in Urban African American and European American youth: The role of ecological factors. Journal of Youth and Adolescence,36(4), 543–553.
Range, B., Duncan, H., Scherz, S., & Haines, C. (2012). School leaders’ perceptions about incompetent teachers: Implications for supervision and evaluation. NASSP Bulletin,96(4), 302–322.
Resnick, M. D., Bearman, P. S., Blum, R. W., Bauman, K. E., Harris, K. M., Jones, J., Tabor, J., Beuhring, T., Sieving, R. E., Shew, M., Ireland, M., Bearinger, L. H., & Udry, J. R. (1997). Protecting adolescents from harm: Findings from the national longitudinal study on adolescent health. JAMA, 278(10), 823–832.
Ross, T. (2016). The differential effects of parental involvement on high school completion and postsecondary attendance. Education Policy Analysis Archives,24, 1–38. https://doi.org/10.14507/epaa.v24.2030
Shumow, L., & Lomax, R. (2002). Parental efficacy: Predictor of parenting behavior and adolescent outcomes. Parenting: Science and Practice, 2, 127–150.
Shute, R., & Slee, P. T. (2016). Mental health and wellbeing through schools: The way forward. Routledge.
Simons-Morton, B. G., & Crump, A. D. (2003). Association of parental involvement and social competence with school adjustment and engagement among sixth graders. Journal of School Health,73, 121–126.
Skrzypiec, G., Slee, P. T., Murray-Harvey, R., & Pereira, B. (2011). School bullying in one or more ways: Does it matter and how do students cope? School Psychology International,32, 288–312.
Skrzypiec, G., Slee, P., Askell-Williams, H., & Lawson, M. (2012). Associations between types of involvement in bullying, friendships and mental health status. Emotional and Behavioural Difficulties, 17(3–4), 259–272.
Slee, P. T., & Skrzypiec, G. (2016). Well-being, positive peer relations and bullying in school settings. Springer.
Slee, P.T.; Ma, L, Hee-og, S, Taki, M; Sullivan, K. (2003). School Bullying in five countries in the Asia-Pacific Region. In J. Keeves & R. Watanabe (Eds.), Handbook on educational research in the Asia Pacific Region. Kluwer Academic Publishers.
Soriano, M. (2017). When leadership and vision fail: The dismantling of a school-based family counseling leadership program. International Journal for School-Based Family Counseling, Special Topic Issue, 1–10.
Spera, C. (2005). A review of the relationship among parenting practices, parenting styles, and adolescent school achievement. Educational Psychology Review,17, 125–146.
Springer, A., Parcel, G., Baumler, E., & Ross, M. (2006). Supportive social relationships and adolescent health risk behavior among secondary school students in El Salvador. Social Science & Medicine,62, 1628–1640.
Strickland, M., & Lyutykh, E. (2020). Community, diversity, and marginalization: An ecological construction of immigrant parenting within the U.S. neoliberal home and school contexts. Journal of the American Educational Studies Association, 56(3): 286–305.
Sue, D. W., & Sue, D. (2008). Counselling the culturally diverse: Theory and practice (5th ed.). Wiley.
Svavarsdottir, E. K., & Orlygsdottir, B. (2006). Health-related quality of life in Icelandic school children. Scandinavian Journal of Caring Sciences,20(2), 209–215.
Thomson, K. C., Schonert-Reichl, K. A., & Oberle, E. (2015). Optimism in early adolescence: Relations to individual characteristics and ecological assets in families, schools, and neighborhoods. Journal of Happiness Studies,16(4), 889–913.
U.S. Bureau of Labor Statistics, Current Population Survey. (2016). Retrieved from https://www.bls.gov/careeroutlook/2017/data-on-display/more-education.htm
van Schalkwyk, G. J. (2010). Mapping Chinese family systems and parental involvement in educational settings in Macao. International Journal for School-Based Family Counseling,2, 1–20.
Wang, M.-T., & Degol, J. L. (2016). School climate: A review of the construct, measurement, and impact on student outcomes. Educational Psychology Review,28(2), 315–352.
Wang, M. T., & Eccles, J. S. (2013). School context, achievement motivation, and academic engagement: A longitudinal study of school engagement using a multi-dimensional perspective. Learning and Instruction,28, 12–23.
Wang, M. T., Brinkworth, M. B., & Eccles, J. S. (2013). The moderation effect of teacher-student relationship on the association between adolescents’ self-regulation ability, family conflict, and developmental problems. Developmental Psychology,49, 690–705.
Wang, M. T., & Eccles, J. S. (2012a). Social support matters: Longitudinal effects of social support on three dimensions of school engagement from middle to high school. Child Development, 83, 877–895.
Wang, M. T., & Eccles, J. S. (2012b). Adolescent behavioral, emotional, and cognitive engagement trajectories in school and their differential relations to educational success. Journal of Research on Adolescence, 22, 31–39.
Wilder, S. (2014). Effects of parental involvement on academic achievement: A meta-synthesis. Educação Em Revista,66, 377–397. https://doi.org/10.1080/00131911.2013.780009
Yariv, E. (2011). Deterioration in teachers’ performance: Causes and some remedies. World Journal of Education,1(1), 81–91.
Zhai, H., Bai, B., Chen, L., Han, D., Wang, L., Qiao, Z., Qiu, X., Yang, X., & Yang, Y. (2015). Correlation between family environment and suicidal ideation in university students in China. International Journal of Environmental Research and Public Health,12(2), 1412–1424. https://doi.org/10.3390/ijerph120201412
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2022 The Author(s), under exclusive license to Springer Nature Singapore Pte Ltd.
About this chapter

Cite this chapter
Gerrard, B.A. (2022). Promoting Child, Family, and School Well-Being: A School-Based Family Counseling Approach. In: Deb, S., Gerrard, B.A. (eds) Handbook of Health and Well-Being. Springer, Singapore. https://doi.org/10.1007/978-981-16-8263-6_23
Download citation
DOI: https://doi.org/10.1007/978-981-16-8263-6_23
Published:
Publisher Name: Springer, Singapore
Print ISBN: 978-981-16-8262-9
Online ISBN: 978-981-16-8263-6
eBook Packages: Behavioral Science and PsychologyBehavioral Science and Psychology (R0)