
Abstract
The impact of the Italian expenditure for the health care on Gross Domestic Product (GDP) and on total public expenditure, is in line with those of the major industrialized countries, and somewhat lower than the European average. The issue of the Italian health sector is not simply related to the contraction of the expenditure: in effect, it should be highlighted that Italy currently does not spend “a lot” and, above all, invests “little” in the mentioned sector. Nevertheless, the health sector can be a very important flywheel for the economic recovery but, in order to make this possible, it is necessary to pay a lot of attention, and to invest the best resources. In this work, the authors intend to develop an analysis of the desirability of investment on Information and Communication Technologies (ICT) in the health sector, and the consequent compatibility with current expenditure, by identifying at the outset the channels multipliers related to the resources at present allocated to the current health expenditure and capital account.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
1 Introduction
At the beginning of the twenty-first century, WHO ranked the Italian health system among the three best in the world. A dozen years later, among the 34 countries surveyed by the EuroHealth Consumer index,Footnote 1 the same system is ranked at 21st place for quality of care. The reasons for this drop can be attributed to several factors, among which we can include the lack of investment and expenditure restraint.Footnote 2
Surely years of crisis and negative expectations about the economic system recovery still make the curbing of public expenditure a priority.Footnote 3 The need to restore public finances and to re-balance the weight of the health sector on government expenditure has often led to consider the health system as a source of potential costs and inefficiencies, rather than as a strategic sector that plays a crucial economic and social importance for the entire country. This has been triggering the sequence of public control operations mainly oriented to the short term, with a logic of linear expenditure cuts, which have tended, however, to fundamentally weaken the areas where public health has more difficulty and to fail to distinguish the virtuous areas from the non-virtuous ones as well as to reward the virtuous.
What is worth highlighting is that the impact of the Italian public health expenditure on GDP and on total public expenditure is in line with those of more industrialized countries and somewhat lower than the European average. The issue of health sector is not simply related to the contraction of the expenditure: you must be well aware, in fact, that Italy currently does not spend “a lot” and, above all, invest “little” in the mentioned sector.
According to the latest available data from Istat (2012), in Italy public health expenditure per capita is well below the average of OECD countries.Footnote 4 Perhaps, then, it is necessary to focus attention on issues related to the redistribution (reallocation) of the expenditure rather than on the simple policy of contraction.
The immediate requirement is therefore to address the issue of “how to spend” (what is important is to spend better and focus on quality of expenditure) and at the same time to prepare the system to support future demand [2]Footnote 5: these are the elements that make up the ratio of the future direction of policy maker who is responsible for the political accountability of health care expenditure. In the absence of these structural interventions you would risk worsening the economic sustainability of the system of cares and to return to an accounting statement out of control. You cannot ignore, for example, that the issue of sustainability of public expenditure is also linked to the development of social and demographic factors. Italy is the European country with the highest percentage of population over 65 and in the coming years, due to the aging of the population, the demand for health services will grow inexorably [3].
Accordingly, it is not just a problem of economic sustainability of public finances, then, but also of competitiveness of the economic system: for instance, with the new rules on cross-border healthcare, the countries with a range of services that do not match the needs of people will be bound to lose competitiveness. In this respect, the demand for health services that will not be satisfied on the Italian territory will impact hard on the balance of payments precisely because of imports of care services [4]. The imported services will trigger a drain of economic resources, both public and private, giving benefit to other health systems with significant consequences for the Italian economy, in particular for the ability to generate income and employment with unfavorable outcomes on the quality of human capital of national health sector.
Indeed, health sector can be a very important flywheel for the economic recovery, but to make this possible it is necessary to pay a lot of attention and invest the best resources.
Tangible experiences along this direction are rapidly growing and show how the production of health services play the role of key productive sector within a local context.
In this sense, for example, you can highlight the need to create health districts that play the role of very supply chains where the main activity made by healthcare services it is able to trigger the production of goods and services from different sectors (chemical, engineering, transport, etc.) with obvious advantages in terms of employment.Footnote 6
Economic policies in the health sector, moreover, should not only meet the need to find resources in view of the containment of the main indicators related to structural public deficit and debt; rather they should be (and create an occasion to remove structural inefficiencies and prevent the system from being vulnerable in front of protracted crises that could seriously undermine its stability.Footnote 7
Unfortunately, due to the difficulty of decision-making and layering regulations, health sector is now at risk of losing gradually in quality and efficiency [5].
In the latest report of the Court of Auditors, the Chairman reported that “the health care system has confirmed the progress already highlighted in recent years in cost containment and absorption of unjustified deficits in the management.Footnote 8
However, health system is still facing challenging choices, but there are worrying indicators concerning the quality of services provided to citizens.”
The fact that the new “Patto della salute” (an agreement between state and the regions for public expenditure containment and for basic healthcare standards assurance) has not yet been finalized is an evidence of the “difficult phase that still lies ahead for healthcare despite the progress that has been made in recent years”.
Hence “the importance and urgency of strengthening the tools available to local government to accelerate action of re-adjustment of structures and improvement of the appropriateness of the services provided to citizens and to bring up to speed the review of the mechanisms that govern the operation of the sector”.
Despite the size of the overall deficit, there are encouraging signs of reduction thanks to more effective expenditure review.
More concretely, in the shortest possible time the Italian health care system will face, therefore, the issue of sustainability, which remains strongly correlated to population dynamics.
The aging of the population and the natural pressure that it exerts on the progress of expenditure requires that the policy makers to be able to use the innovation to bring out gaps and productive inefficiencies, especially in those systems where the public presence is relevant.
In addition, the investment policy should not only be able to respond to the growing demand for health care that characterizes the elderly population, and generally “the weaker”, but mainly to the change in the type of demand for services, given the new needs that emerge in the last period of people’s life.
These are the critical factors that can create, from the economic point of view, large diseconomies of scale, of variety and location; diseconomies that must be tackled with the introduction of innovations of both process and product.
Just with regard to the benefits that can bring innovations of process and/or product, in this work we intend to develop an analysis of the desirability of investment in ICT in the health sector and the consequent compatibility with current expenditure by identifying at the outset the channels multipliers related to the resources at present allocated to the current health expenditure and capital account. In this way it will be possible to identify the different multiplicative intensity of investment expenditure compared to current expenditure.
This first result is the premise to justify and support the choice of policy makers to redistribute resources from the pockets of inefficiency in current expenditure towards programs for research and innovation in ICT (in other words: it is not beneficial to spend less but you need to spend better).
As a result this not only generate immediate and positive effects on income and employment, but you would have in addition a structural change of the production processes of health care services towards greater efficiency and effectiveness.Footnote 9
2 The Health Care System and the Main Areas of Digital Innovation
The Information and Communication Technologies applied to Italian health sector is a possible innovation but especially needed. In effect, in this sector, the ICT can significantly help to improve the offered care services with savings opportunities for the citizens and for the National Health Service, in terms of time and especially money. Numerous studies have been carried out, and by the introduction of ICT in healthcare, it has been proven to save, at European level, billions of euros. Moreover, the quality and efficiency of health services must be improved, and ICT can help in this process. In this section, we analyze the main, significant and priority areas of ICT with high desirability of investment in the Italian health sector.
Firstly, it is necessary to understand how the limited ICT resources are used on the Italian health care system. About this, it has been identified the main areas of innovation, analyzing not only current investments associated with them, but also the strategic importance attributed to the various areas and their development barriers (e.g., complexity of realization, high required investments, resistance to change, etc.). This analysis [6] reveals three main clusters of ICT innovation:
-
Breakthrough: radical innovation fields with strong strategic benefits that, however, require major changes in the processes and organization. These include Electronic Medical Records (EMRs), document management systems, digital services for the citizen, clinical governance solutions, business intelligence solutions for medication management, business continuity systems, disaster recovery and interoperability solutions integrated with regional and/or national health care digital systems.
-
Must-have: fields with limited benefits and impacts on the key performance of the health structures, but without barriers to development. Some examples are: the administrative management systems, human resources management systems, front-end systems and ward management systems.
-
Challenge: fields that appear to be less important to the pursuit of the strategic objectives, and which require significant changes for their implementation, such as overcoming high cultural barriers. Among these fields, there are the mobile health, cloud computing, ICT solutions to support medicine and care (including tele-medicine), ICT solutions for social assistance and electronic social record (that is, however, extremely important for the 94 % medical directors).
where, the Breakthrough is the cluster on which the important is strongly perceived. The Must-have cluster is the most consolidated one because referring to available ICT solutions, also coming from other public medicine sectors. Conversely, the Challenge cluster contains areas which currently are identified as most problematic, but which can represent the real challenge for the development of the italian health sector in the near future.
In order to determine the significant and priority fields of ICT with high desirability of investment in the Italian health sector, it is crucial to determine how the limited ICT resources are now allocated. The research study carried out by the “ICT in Health Observatory” [6] shows not only the overall ICT spending on health care, but also the budget allocated to the different ICT fields, that is the ICT budget that the Italian health authorities have allocated in 2013 for each field. These results are resumed in Fig. 1.

Budget (Mln) on different ICT fields of the Italian health system in 2013
From this analysis, it is evident that the Italian investments on ICT are strongly oriented to the development of hospital care solutions, while to the territorial and social developments are devoted only few resources. This is mainly due to the fact that the decision-makers have limited vision on the challenging ICT solutions based on cloud computing, on mobile health and on innovative ICT digital solutions. In the next, we analyze the compatibility with current spending to invest on these challenging and crucial ICT fields, by identifying at the outset the channels multipliers related to the resources at present allocated to the current health expenditure and capital account.
3 Relationship Between ICT and Human Health Services in Economic National Account
The increase in efficiency and quality of producing health is deeply linked with the possibility to introduce ICT in the process of creation of Health services [7]. As for the other services sectors the industry of Health care services is ruled by innovation and it was shown that a proper policy of investment in ICT for health care procedure has the potential to drive economic growth and innovation [8, 9].
The relevance of Health care services and its relation with the ICTs production can be stressed given a proper data showing the production setting by mean it is possible to measure the incidence of ICT expenditure on total public health expenditure. Actually, public health system spent in ICT about 1.3 billion euro for the year 2011 [6]. This value is affected by the cyclical trend of the economic variables that has substantially been reduced. In per capita terms the total expenditure on ICT in public health services is around 22 euro per inhabitant. Comparing this value to those of the main European countries, it is possible to show a clear difference. In Germany, in fact, the per capita expenditure in ICT in health is about 36 euro, in France rises to 40 euro and Britain reaches a value of 60 euro. The countries of northern Europe and especially Sweden and Denmark, are above these prices with a per capita total expenditure on ICT by 63 and 73 euro.
According to the definition of ICT [10, 11], we can quantify the absorption of ICT in the production of health care services using the available data base represented by the Social Accounting Matrix for Italy, 2009 [12]. The quantification of ICT absorption is made considering the entire production of health services (both public and private) and taking into account that some ICT productions are included in activities that are more traditional. The approximation does not affect the results of the analysis.
We include in ICT the following sectors: Computer, electronic and optical products (17), Electrical equipment (18), Wholesale trade services, except of motor vehicles and motorcycles (29), Publishing services (37), Motion picture, video and television program production services, sound recording and music publishing (38), Telecommunications services (39), Computer programming, consultancy and related services; information services.
Using the USE table (the table of intermediate absorption) it is possible to identify the amount of intermediate goods of the ICT typology purchased by health industry according the definition of ICT industry. In the year we are interesting to simulate the investment policy the production of Health care services is around 107,412 million of euro which are divided into 61.53 % in terms of value added and 38.47 % in terms of absorption of intermediate goods. Then the value added is represented by compensation of employees (69.7 %), mixed income (16.3 %), gross operating surplus (9.5 %) and finally other taxes less subsidies on domestic production (4.5 %). Within the intermediate consumption the absorption of ICT goods are stressed in Fig. 2.

ICT intermediate expenditures by human health care services
The absorption of ICT in order to produce Human Health care services is 2,816 million of euro that represents the 2.6 % of the whole health care production. As it can be seen in Fig. 2 ICT goods that play a major role in the production of Human Health care are: Computer programming, consultancy and related services; information services (37.03 %), Computer, electronic and optical products (33.10 %) e Telecommunications services (24.93 %).
4 Dynamic CGE: The Economic Impact on ICT Through Human Health Services Demand
This study develops the recursive dynamic Computable General Equilibrium (CGE) model where the behaviour of agents depends on adaptive expectations. It is calibrated on the basis of SAM structure and the blocks of the SAM determine the blocks of the equations in order to replicate and provide a fast check of macroeconomic aggregates. The model is characterized by nested production function (CES technology to determine VA, LEONTIEF to aggregate the intermediate goods and VA to determine the domestic production), equalization between supply and demand across all the interconnected markets in the economy. The dynamic component in the model is introduced following the logic of the Ramsey model, according to which all the Institutional Sectors maximise the present value of their intertemporal utility function, which depends on final consumption expenditure and gross saving subject to the lifetime budget constraint. According to the market clearing condition for capital, any change in gross fixed capital formation must affect the capital yearly growth given a constant rate of capital depreciation [13].
The time horizon is finite and considers a time period from 2014 to 2020. Given that ICT and related productions show frequent changes, this does not allow to go beyond short-term time horizons.
Given the interaction of Health care services with other production processes and Institutional Sectors, as highlighted in the SAM for Italy (year 2009), we can calibrate a dynamic CGE model in order to assess the impact of an increase in final demand of Health services on ICT sectors. In particular, it is possible to highlight the impact on GDP, Value Added by commodity and Income by Institutional Sectors resulting from an increase of 2 % in Health final demand. To be more specific, we simulate two different scenarios: in the first (SIM1) we assume an increase in Health services demand by Government of 17,962 millions of Euro; in the second scenario (SIM2) we consider an increase in final demand of Health services by Households for 2,752 millions of euro. In both scenarios the fiscal policy is made under budget constraint.
In Fig. 3 we observe the real GDP path from 2014 to 2020 without any policy (benchmark), with the increase of final demand of the Human Health services from the Government (SIM1) and Household (SIM2). When the policy is devoted to increase households final demand in health services, the overall effect on the economy over time is positive in terms of GDP change. Looking at the results showed in Fig. 3, in a quite short time horizon (6 years from 2014 to 2020), it appears that the economic system reacts more when the health services are stimulated by the private demand instead of public demand. In other words, the private health care expenditure is connected more with the other production processes and with the economic system than the health care expenditure sustained by Government.

Gross domestic product from 2014 to 2020 (millions of Euro)
In disaggregate terms we observe the effects of the manoeuvres on Value Added by commodity and look in particular to the impact on ICT commodities. As showed in Table 1, the value added by ICT commodity has a better performance when the policy is implemented using resources from the Government to finance the Households expenditure in health services.
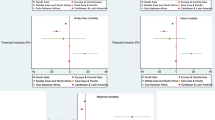
Finally, it is possible to observe the difference between the value added in Benchmark path and the value added resulting from the policies for each of the commodities included in ICT sector. Looking at Figs. 3 and 4 we observe that in both scenarios the effects of the policies runs out in a period of 6 years. Moreover, the results emphasizes a strong impact on Computer, electronic and optical products (17) and none effect on Wholesale trade services (29) because it encompasses a portion not associated with ICT production (Fig. 5).

Simulation 1—Changes in ICT commodities value added from 2014 to 2020 (differences form benchmark—millions of euro)

Simulation 2—Changes in ICT commodities value added from 2014 to 2020 (differences form benchmark—millions of euro)
5 Conclusion
In this work, an analysis of the desirability of investment on Information and Communication Technologies in the health sector has been developed. In order to accomplish this study and to assess the impact of an increase in final demand of health services on ICT sectors, a recursive dynamic Computable General Equilibrium model has been calibrated where the behavior of agents depends on adaptive expectations. Two different scenarios with the fiscal policy made under budget constraint, have been considered: in the first it has been assumed an increase in health services demand by Government of 17,962 millions of Euro; in the second scenario, it has been considered an increase in final demand of health services by Households for 2,752 millions of euro. The result is that, when the policy is devoted to increase households final demand in health services, the overall effect on the economy over time is positive in terms of GDP change. Moreover, it appears that the economic system reacts more when the health services are stimulated by the private demand instead of public demand. In addition, the value added by ICT commodity has a better performance when the policy is implemented using resources from the Government to finance the Households expenditure in health services.
Notes
- 1.
EuroHealth Consumer index 2013 in http://www.healthpowerhouse.com/index.php?Itemid=55.
- 2.
It is worth paying attention to the details that are stressed in the report by the OECD Health Division prepared following a request for clarification from the Hygiene and Health Commission of the Italian Senate (the report has come in the first months of 2014 to the attention of parliamentarians) (http://www.quotidianosanita.it/allegati/create_pdf.php?all=1683299.pdf). The report underlines that in the current government, “the data provided in support of health care expenditure reductions proposed in the expenditure review does not allow you to fully appreciate the situation of increasing disadvantage of the National Health Service with respect to the health care systems of other European countries”. It is also highlighted that “Italy has a public health expenditure per capita more than a third lower than the average of other countries in the Eurozone considered in the expenditure review, and the gap has tripled since the early 2000 s”. But this is not enough. According to the OECD, “the level of health services provided in Italy is significantly lower than that observed in almost all other countries in the Euro area considered in the expenditure review”. For this reason “any expenditure reductions aimed not only for the recovery of inefficiencies would affect further on access to healthcare, on the levels and quality of health care, particularly for the most disadvantaged citizens”. Not to mention that the benchmark for the public health expenditure (5.25 % of GDP) suggested by the Working Group on the Review of public expenditure is not compatible with the existing model of the Italian National Health Service.
- 3.
By reading the history of the Italian health since 1978 (the date of creation of Italian national health system) one can easily notice how financial difficulties have been a feature of the system and have also been affecting the organization and the decisions of policy makers [1].
- 4.
According to the latest data presented by ISTAT, the Italian public health expenditure amount to 111 euro billion, that is 7 % of GDP: € 1867 year/inhabitant. But Italy is in the second half of the ranking of European countries in per capita expenditure, below France, England and Germany, that are our reference countries. Essentially, let alone other problems, the funding allocated to public health care is not sufficient. It is therefore unsurprising that a group of citizens, gathered by the Association Giuseppe Dossetti, has decided to promote a class action and to sue the State, because it does not guarantee the LEA, the essential levels of assistance in 12 regions out of 21. According to the data, it will ask for a compensation for not complying with the law and the “Patto sulla salute”. See http://www.sanita.ilsole24ore.com/art/dibattiti-e-idee/2014-02-10/dallassociazione-dossetti-class-action-130644.php?uuid=Ab0MKYMJ.
- 5.
The authors argue that the problem is not the sustainability of the system rather than its survival.
- 6.
An example is the industrial district wellness spa: http://ideario.formez.it/content/distretto-produttivo-del-benessere-termale-siciliano.
- 7.
A serious policy of investments in ICT, in fact, may generate significant improvements both from the point of view of the ability of care and with respect to containment of expenditure. For example, one of the cornerstones to a more effective and efficient health care system is digital innovation: according to the data, if the Italian health system realized completely the potential of digital technologies, it could save 6.8 billion a year—much more than the cuts expected in 2015 and 2016 for financing public health sector. In contrast to the cuts, however, “the digital” innovation would achieve transparency and appropriateness, would reduce many errors (just think of the interpretation of recipes written by doctors) and would improve the quality of services provided to citizens (think of the queues that could be avoided by allowing you to download the reports from home). Even if the investments to be implemented would be limited (we are speaking about millions of euros and not billions in the maneuvers of stability), Italy does not appear to be keen on digital healthcare. There are several ongoing trials but the total expenditure allocated to digitization is estimated to decrease as compared to 2011 and in proportion Italy spends a third in comparison with countries such as France or England. See the case of the Region “Marche”: http://www.ecommunity.marche.it/AgendaDigitale/tabid/174/Default.aspx.
- 8.
The key elements are: “an evaluation network that allows an effective monitoring capable of making the benchmarking technique a tool to control and effectively manage the system; a redesign of accounting rules that gradually helps to strengthen the reasons for a structural adjustment; a central government that, in comparison to the local government, accompanies the pursuit of cost containment interventions with structural adjustment, with improvements in equipment and with investments in human resources training”.
Report 2013 on the Coordination of the Public Finance—28.05.2013 in http://www.regioni.it/it/show-presentazione_del_rapporto_2013_sul_coordinamento_della_finanza_pubblica_-_28052013_/news.php?id=299026.
- 9.
This paragraph has been authored by Monica De Angelis.
References
De Angelis, M.: La complessità del sistema sanitario italiano: profili giuridici (in particular Chapter I) (2012)
Caruso, E., Dirindin, N.: Perché tagliare ancora una sanità già sostenibile? http://www.lavoce.info/perche-tagliare-sanita-gia-sostenibile/ (2014)
Ciaschini, M., De Angelis, M., Pretaroli, R., Severini, F., Socci, C.: The third age in the national health system: a proposal for increasing the spending effectiveness in health care for the elderly. In: Ambient Assisted Living: Italian Forum 2013, vol 9, pp 345–353. Springer-Verlag (2014)
De Angelis, M.: The expansion of patients’ rights in Europe: a new perspective for healthcare abroad. In: Bulletin of the Transilvania University of Brasov. Volume 7 of Series VII: Social Sciences Law (2014)
De Angelis, M.: La complessità dei sistemi sanitari. Problematiche giuridiche del caso italiano. Esculapio, Bologna (2012)
Dipartimento di Ingegneria Gestionale, Politecnico di Milano: Innovazione Digitale in Sanità: l’ICT non basta! Osservatorio ICT in Sanità (May 2014)
Ciaschini, M., Pretaroli, R., Socci, C.: Number 2/09 in Contenimento della spesa corrente e spesa in conto capitale nel sistema sanitario pubblico. In: Tendenze Nuove. Il Mulino pp. 115–132 (2009)
Socci, C., Ciaschini, M., Pretaroli, R., Severini, F.: Health services as a key sector for income and employment change. Bull. Transilvania Univ. Braşov 3, 163–172 (2010)
Ciaschini, M., Pretaroli, R., Socci, C.: Health-care in europe as a driving force for output and gdp. Glob. Forces Local Identity Econ. Cult. Divers. 28, 106–135 (2011)
Ciaschini, M., Pretaroli, R., Socci, C.: A convenient multisectoral policy control for ICT in the US economy. Metroeconomica 60(4), 660–685 (2009)
Ciaschini, M., Pretaroli, R., Socci, C.: Multisectoral structures and policy design. Int. J. Control 83(2), 281–296 (2010)
Ciaschini, M., Socci, C.: Final demand impact on output: a macro multiplier approach. J. Policy Model. 29(1), 115–132 (2007)
Ahmed, I., Ciaschini, M., Pretaroli, R., Severini, F., Socci, C.: Economic policy effects and financial crisis: a dynamic cge model for italy. In: 22nd International Conference of Input-Output, Lisboa, Portugal (14–18 July 2014)
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2015 Springer International Publishing Switzerland
About this chapter
Cite this chapter
Ciaschini, M., De Angelis, M., Monteriù, A., Pretaroli, R., Severini, F., Socci, C. (2015). Investments and Sustainability of Public Expenditure in the Health Sector. In: Andò, B., Siciliano, P., Marletta, V., Monteriù, A. (eds) Ambient Assisted Living. Biosystems & Biorobotics, vol 11. Springer, Cham. https://doi.org/10.1007/978-3-319-18374-9_4
Download citation
DOI: https://doi.org/10.1007/978-3-319-18374-9_4
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-18373-2
Online ISBN: 978-3-319-18374-9
eBook Packages: EngineeringEngineering (R0)