
Abstract
This chapter provides an updated and critical review of the use of indocyanine green (ICG) kinetics as a dynamic assessment of liver function using the new noninvasive bedside monitors now available in clinical practice. The analysis encompasses the most common indications ICG has today in clinical practice [1]: the diagnostic and prognostic role in the perioperative period of major liver surgery and liver transplantation [2] and the role in the critically ill patients in ICU to predict mortality and to assess the impact of intraabdominal hypertension on splanchnic perfusion.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others



Keywords
13.1 Notes on Liver Anatomy and Physiology
The liver is the largest visceral organ, weighing, in healthy adults, between 1,500 and 1,600 g: it has two anatomical lobes (left and right) separated by a reflected surface of peritoneum (falciform ligament) [1]. Instead, from the surgical point of view, the porta hepatis, point of division of the hepatic artery and portal vein into right and left branches, is the reference point for the division. Based on the branches of portal and hepatic veins, the two lobes are divided into eight segments, allowing the definition of the various types of hepatic resection (Couinaud) [1, 2] (Fig. 13.1).

Liver segmental anatomy (From Mulaikal and Edmond [2])
The hepatic lobule is the anatomical and functional unit of the liver. It has the shape of a polygonal (hexagonal) pyramid with an apex trunk of 1 mm in diameter and a height of about 1.5–2 mm, delimited by a layer of connective tissue (reticular connective). Each lobule is formed by numerous cellular laminae consisting of hepatocytes; the plates are perforated and anastomosed with each other and define a system of irregular vascular spaces: the hepatic sinusoids. The cellular edges and capillaries show a radial arrangement converging from the periphery toward the centre of the lobule. The axis of the lobule is occupied by the centrilobular vein, tributary of the hepatic vein, within which the sinusoids open up. The area where three or more adjacent lobules are in contact with each other is called a portal space (‘portal triad’, containing a bile duct, a terminal branch of the hepatic artery and the portal vein). Metabolic zones form the hepatic acinus [2]. Zone 1 is the periportal zone, is centred around the portal triad and, being close to the hepatic artery, is oxygen rich. It is more resilient to hemodynamic stressors, least susceptible to necrosis and first to regenerate. These zones are involved in gluconeogenesis/glycogenolysis. Zone 3 is the pericentral or perivenous zone, very close to the central vein: it has the lowest oxygen tension. This zone is highly susceptible to stressors, hypoxia and is the last to regenerate. Zone 3 is the site of drug detoxification and phase 1 and 2 metabolism [2].
The liver has a dual blood supply, which includes an arterial system (hepatic artery, HA) and a venous system (portal vein, PV). The total liver blood flow is approximately 1,500 ml/min (100 ml/min/100 g). The hepatic artery flow is approximately 300 ml/min (30 % of total hepatic flow, 45–50 % of total oxygen intake), while portal vein is usually estimated between 1,000 and 1,200 ml/min (70 % of total blood flow, 50–55 % of oxygen supply). The O2 hepatic extraction, normally less than 40 % (4–6 ml/100 g/min), is increased in case of increased demand [2].
Both the terminal portal venules and the terminal hepatic arterioles end in the hepatic sinusoids, through which the entire afferent hepatic blood flows before reaching the efferent vascularisation (terminal hepatic venules). Hepatic blood drainage is via the hepatic veins (right, left, middle) which drain into the inferior vena cava.
The portal system is a low-pressure (5–12 mmHg)/low-resistance system: the gradient between portal vein and hepatic vein (HVPG) ranges between 1 and 5 mmHg: portal hypertension is defined as a pressure of >12 mmHg or for a portal vein–inferior vena cava (IVC) gradient >5 mmHg. The arterial system has a high level of resistance and a high flow. Hepatic blood flow and distribution are dependent on hepatic arterial resistance, intrahepatic portal resistance and portal flow. Intrinsic and extrinsic mechanisms regulate the hepatic blood flow. Among the extrinsic factors, sympathetic innervation plays an important role in controlling vascular tone (adjusting the capacitance of the uptake capacity of circulating blood). Within the hepatic arterial bed, both alpha (alpha 1 and 2) and beta (beta 2) receptors are represented, while only alpha receptors are present in the portal vein. Dopaminergic receptors are present in both vessels. Vasopressin, able to increase the hepatic artery resistances, reduces the PV resistances, thus playing a relevant role in the treatment of portal hypertension. Maintaining a constant hepatic inflow is crucial to optimise drug metabolism and synthetic functions. Self-regulating mechanisms, present in the hepatic artery, are not demonstrated in the portal vein. Among the intrinsic factors (working independently of humoral neuroregulation) are self-regulating mechanisms for flow/pressure: in case of critical drop in blood pressure, arterial hepatic blood flow is maintained until systolic arterial pressure falls below 75–80 mmHg, via reduction of resistance mechanism. In case of reduced portal flow, hepatic artery flow increases, buffering the changes in portal flow (hepatic artery buffer response, HABR). In a situation of critical drop in portal flow (flow reduction of 20–30 %), there is an increased vicarious flow in the hepatic artery (increase up to 100 %) in order to maintain the hepatic blood supply. The mechanism is supported by the reduction of adenosine washout (present with normal portal flow, but missed in the presence of low flow) followed by hepatic artery vasodilatation. A portal flow counterbalance in the presence of hepatic artery occlusion does not seem to exist. Instead, there is an increased hepatic arterial resistance with flow reduction in case of elevated hepatic venous pressure [1, 2].
The liver performs many functions such as protein synthesis; uptake, storage and metabolism (biotransformation and degradation) of endogenous and exogenous substances (among them carbohydrates, lipids, proteins, hormones, drugs); bile production; and immune defence with different mechanisms, mainly operated by the Kupffer cells (KC, so-called fixed hepatic macrophages, 80–90 % of the reticular endothelial system, 10 % of the entire liver cell mass), responsible of phagocytosis (bacteria, fungi, viruses, immune complexes, antigens), clearance of endotoxin and secretion of mediators capable of adjusting microcirculatory hepatic protein catabolism. Due to the indeed wide variety of processes the liver is involved, no single parameter or test able to measure all components simultaneously has been available so far [1–4].
13.2 Static and Dynamic Liver Function Tests [1–5]
To assess liver function, static (also called conventional tests) and dynamic tests are available [3–5]. The static tests track the different functions separately, and, in the event of injury, they might describe its size: these tests are, since long, part of scoring systems, able to track chronic (Child–Pugh; MELD) or acute (SOFA) functional impairment of the liver. However, static tests are not able to predict the quality and the extent of the functional recovery of the liver (or of a newly grafted liver), as they essentially show a ‘frozen’ (static) representation of the integrity (or not) of hepatocytes and of metabolic and synthetic pathways (Fig. 13.3). Metabolic function includes enzymes of the cytochromes (phase 1) and the phase of glucuronide conjugation (phase 2). Bilirubin, derived from haemoglobin catabolism, expresses the capacity of uptake, conjugation and excretion in the bile of haeme (breakdown product of haemoglobin; 1 g Hb leading to 36 mg bilirubin). After uptake by the liver cell, the haeme is exposed to glucuroconjugation (metabolic phase 2) for solubilisation, aimed at excretion in the bile: the process can be relatively insensitive to ischaemic insult, at least in the early stages. In general, hyperbilirubinaemia depends on haemolysis (pre-hepatic disease), cell damage or reduced intrahepatic bile excretion (cholestasis). Albumin, vitamin K-dependent coagulation proteins (factors II, VII, IX, X; protein C; protein S; and protein Z), factor V, fibrinogen, antithrombin, alpha 2 plasmin inhibitor, and plasminogen represent the (elevated) share of synthetic activity of the liver. The short half-life of FV (4 h) and FVII (4–6 h) might quantify the liver damage in acute liver failure and is used in the Clichy criteria, together with the presence of hepatic encephalopathy, to indicate LTx for FHF [6].

Static and dynamic assessment of liver function (From Sakka [3])

ICG indicator dilution curve. ICG indocyanine green, C ICG, ICG blood concentration. A Primary peak, B secondary peak (recirculation phase), C (hepatic) elimination phase (From Vos et al. [9])
13.3 Liver Enzymes, Liver Function and Liver Injury [4, 5]
AST (aspartate aminotransferase) and ALT (alanine aminotransferase), present in various organs, have an important role for the metabolism of amino acids. AST is less specific, being present at cardiac and muscular level. ALT is more liver specific, is highly represented in the cytoplasm and is, for the most part, in the periphery of the liver lobule: moderate increase is reported in case of centrilobular hypoxia. In the presence of acute hepatic injury (acute hepatitis), the serum concentration of ALT, mainly represented in the periportal areas of the liver, increases significantly, as a consequence of increased permeability of the cell membrane or necrosis. Increased AST/ALT is associated with ischaemic injury and its size (liver injury), but does not provide information on functional hepatic impairment and therefore is considered inferior to dynamic tests when assessing hepatic functional reserve [3–5]. Alkaline phosphatase (ALK) and gamma-glutamyl transferase (GGT) are mainly used to quantify cholestasis. Lactate dehydrogenase (LDH, mainly fraction 5) is a rather nonspecific index of ischaemic liver (but not only!).
Dynamic tests [3, 7] are related to the ability of the liver to metabolise or eliminate substances. Unlike conventional tests, dynamic tests are able to assess liver function within a relatively short time span, are repeatable in relatively short time and may confidently provide a reliable and more global prognostic assessment (Fig. 13.2). Among them are ICG clearance, caffeine test, BSF clearance, amino acid clearance, galactose elimination capacity, formation of monoethylglycinexylidide from lignocaine (MEGX test) and aminopyridine test.
-
The aminopyrine breath test measures the microsomal metabolical capacity of the liver cell. The test is based on demethylation and subsequent metabolism of 14C-aminopyrine marked by the microsomal enzyme cytochrome P450 dependent. The extent of demethylation is measured indirectly by the exhaled CO2.
-
Galactose elimination capacity (depending on cytosolic mitochondrial function) studies the function of the liver cell. Metabolisation occurs through phosphorylation by the galactokinase. The test is complex in clinical practice since it requires samples over 20–50 min and presents false positives in relation to fasting and liver regeneration.
-
Monoethylglycinexylidide (MEGX) is a derivative of lidocaine metabolism and is related to the activity of cytochrome P450. It has been used in the past (and still by some) in liver surgery (value >25 ng/ml predicts safe liver resection) and as a prognostic indicator in patients candidate for liver transplantation. The results can be altered by interaction with other drugs that affect the cytochrome P450. The test, performed in the laboratory and whose results are not obtained in real time, has not been used in the field of anaesthesia and ICU.
13.4 The Clearance Principle: Liver Function and Hepatic Perfusion [8]
Most quantitative liver function tests rely on the clearance principle: the hepatic clearance (Cl) is the product of flow (Q) and hepatic extraction (Ex).
According to this principle [8], substances are classified at high or low hepatic extraction rate. In case of drugs at high extraction rate, liver blood flow becomes the limiting factor, and clearance will approach liver blood flow. Instead, low extractable compounds are flow independent: in this case, the hepatic clearance is the measure of the metabolism and/or elimination process, or more precisely, it represents the intrinsic ability of the liver to remove substances without flow limitation, i.e. the intrinsic hepatic clearance. Equation 13.1 can be rewritten as
Then, according to Imamura et al. [8], the measure of clearance of compounds with high extraction rate is an indicator of liver blood flow, while the clearance of low extractable substances represents intrinsic clearance (Clint). In healthy subjects, with very high extraction, indocyanine green (ICG) clearance is considered a surrogate of hepatic blood flow; on the contrary, in cirrhotic patients, due to the reduced hepatic extraction secondary to the disease, ICG clearance represents the intrinsic clearance, characterised by a reduced uptake: steady-state hemodynamic conditions are mandatory to adequately assess liver function.
13.5 Indocyanine Green Clearance: The Tests
Among the dynamic tests, indocyanine green (ICG) clearance remains the most relevant, widely used in clinical practice today both in the surgical and medical critically ill patient [9–12]. ICG is a fluorescent, water-soluble, inert, tricarbocyanine with a very high hepatic extraction (70–80 %) and a very low toxicity (the side effects described are very rare, about 1/40,000): the only known contraindications are allergy (non-immunological histamine release), iodine allergy or thyrotoxicosis, the latter due to the presence of iodine in the molecule. Since 1960, its elimination rate has been largely used to measure liver function and hepatic blood flow [13–15]: in the late 1990s, Lau had shown the superiority of ICG clearance (ICGCl) compared to the aminopyrine breath test and the clearance of amino acids as a predictor of mortality in patients undergoing liver resection [15]. Important applications are now available in liver resection surgery, in liver transplantation and in intensive care [3, 9–11]. The conventional measurement of ICGCl requires serial blood sampling after ICG injection. Ex vivo photometric analysis of consecutive arterial blood samples after intravenous bolus injection is the gold standard; however, being a time-consuming and complex procedure, it has now been abandoned in favour of the more recently developed monitors that allow transcutaneous noninvasive pulse dye densitometry (PDD) tests at the bedside (LiMON, Pulsion, Germany; DDG-2001 Nihon Kohden, Japan) [9–11]. Available monitors express ICG elimination in terms of the ICG plasma disappearance rate (ICGPDR) or retention rate at 15 min (ICGR15), since only relative ICG concentration changes have to be assessed (Fig. 13.3).
The results of ICG elimination measured by the PDD method have been shown to correlate with those obtained by the invasive method used in critically ill patients (whether or not haemodynamically stable) and in patients after liver surgery. Both devices calculate the rate constant (k) of the ICG indicator–dilution curve using backward dynamic extrapolation of the elimination phase [9]. Appropriate calculations using K value allow the determinations of functional parameters able to quantify liver function. The ICG kinetics have been studied since 1960 in animals and humans to measure blood flow, cardiac output and circulating blood volume and, later, to assess liver function [9–11]. Due to high hepatic extraction (70–80 %), ICG clearance has been used as an index (measure) of liver blood flow. The usual ICG dose of 0.5 mg/kg generates in the average subject an initial plasma concentration of 100 mg/ml: according to Sakka, however, reliable results are also available using 0.25 mg/kg [3]. Once injected, ICG shows a very high protein binding (95 % to albumin, alpha1 lipoproteins and beta lipoproteins) and a very short half-life (3–5 min) [9–11]. It distributes uniformly and rapidly (2–3 min) in the blood, with a volume of distribution approximately equal to that of plasma. ICG is almost entirely extracted by the liver (uptake across the sinusoidal plasma membrane) and transported within the liver cells by transporting polypeptides (1 B3 and Na-taurocholate cotransporting polypeptides). It is excreted unchanged almost exclusively into the bile in nonconjugated form with neither metabolism nor enterohepatic recirculation, carried by the ATP-dependent export pump multidrug resistance-associated protein 2 (MDRP2) and multidrug resistance P-glycoprotein (MDR3), reflecting hepatic excretory function and hepatic energy status [9–11]. Then two processes are involved in hepatic ICG clearance: sinusoidal uptake and canalicular excretion, the former playing the most important role in humans. Due to the very high hepatic extraction, ICG clearance is, in normal conditions, hepatic blood flow limited. After the intravenous bolus administration, the ICG dilution curve shows (i) a primary peak (used to calculate cardiac output); (ii) a second elimination peak (recirculation phase), sometimes followed by smaller peaks, used to estimate circulating blood volume; and (iii) an (hepatic) elimination phase, lasting 10–20 min [9].
In the dye dilution time curve, two components are recognised [8]: (a) the distribution phase, representing ICG removal from the plasma, due to the uptake by the liver cells; and (b) the elimination phase in the bile (97 % of the entire elimination process) (Fig. 13.4).

Graphic representation of ICG kinetics (From Imamura et al. [8])
The decay is bi-exponential, with linear kinetics up to a dose of 1 mg/kg. The ICG hepatic clearance therefore depends on hepatic blood flow and transporter capacity: signs of liver dysfunction as indicated by impaired clearance of ICG (see below) may depend on reduction of blood flow, on impaired cellular function, or on both (blood flow clearance and transporter capacity). ICG half-life is substantially prolonged in the case of liver disease. Different from the usual two-compartment model, ICG is excreted from the peripheral compartment (the liver) and not from the central compartment (plasma). According to this model, the initial rapid fall in concentration, called the distribution phase, represents the uptake of ICG from the plasma by the liver; the subsequent relatively slow fall, called the elimination phase, represents the elimination of ICG from the liver into the bile. The transition from the distribution phase to the elimination phase of ICG occurs approximately 20–30 min after the administration. ICGK (min−1) is usually determined from the first 15-min component of the ICG disappearance curve.
The ICG transport capacity may be reduced either because of the downregulation of organic anion-transporting polypeptides [4] or by competitive inhibition due to hyperbilirubinaemia [16]. With respect to the former, cytokines such as tumour necrosis factor-α (TNF-α) and interleukin 6 (IL6), released by Kupffer cells in patients with steatosis and/or hepatic injury (hepatitis), are able to affect the expression of organic anion-transporting polypeptide isoforms and sodium taurocholate cotransporting polypeptide, thereby affecting ICG uptake by the liver. Bilirubin and ICG share the same enzyme transport system (ATP export pump MDRP2), making high the chance of altered results (false pathological values) in the presence of hyperbilirubinaemia (vide infra) [9, 16, 17]. Consequently, the ICG test may be of limited value in patients with a condition of global hepatocellular dysfunction and in the case of hyperbilirubinaemia (generation of false poor results) [9, 10]. At the opposite site are high flow states, able to mask an altered excretory function and providing false-reassuring results (better than expected liver function), due to the generation of false ‘normal or near-normal’ results [10]. It has been documented that ICGCl is not adequate to measure hepatic blood flow in specific clinical settings: for example, the fraction of hepatic extraction (70–80 % in healthy subjects) is greatly reduced in cirrhotic patients (20–30 %), making ICGCl a representation of Cint (uptake clearance; see above) [18]. Studying ICG kinetics in patients with cirrhosis, Kawasaki et al. [19] reported significant alterations of uptake and release constants (k) (but the release constant is questioned by other authors). Instead, the constant of elimination of ICG in the bile seems to be normal. In the same study, measuring hepatic blood flow with the galactose clearance test, it was shown that in cirrhotic patients, the reduction of ICGCl, expressed as ICGR15 (the circulatory retention of ICG 15 min after bolus injection, vide infra), does not (only) depend on hepatic blood flow reduction but also on a reduced extraction of the liver cells. In cirrhotic patients, this phenomenon seems to be related to the extent of the sinusoidal capillarisation and to the presence of intrahepatic shunts [9, 19, 20]. In normal conditions, substances (including proteins) diffuse freely between the sinusoids and hepatocytes. As sinusoid capillarisation develops, diffusion of these substances becomes impaired and barrier limited, as is in the capillaries of other districts. Due to its high protein binding, ICG is very sensitive to the sinusoidal capillarisation. Figure 13.6 shows the disappearance of ICG from plasma in normal subjects (full signs) and cirrhotic subjects (empty signs). According to Imamura, in cirrhotic patients, ICGK and ICGR15 might reflect the degree of sinusoidal capillarisation, intrahepatic shunts and, in part, reduced liver blood flow [19].
The logarithmic transformation of the curve in the distribution phase allows the measurement of different parameters that quantitatively assess the removal of ICG by the liver cells [9, 10].
-
1.
Constant K (ICGK) – disappearance rate constant or elimination rate constant
-
2.
Clearance of green indocyanine (ICGCl)
-
3.
Plasma disappearance rate (ICGPDR)
-
4.
Retention rate at 15 min (ICGR15)
In clinical practice, ICGPDR and ICGR15 are the ICG kinetic parameters most frequently used to dynamically assess liver function [9, 10] (Fig. 13.5):

Variables to quantificate ICG kinetics (From Vos et al. [9])
-
1.
ICG PDR – plasma disappearance rate
-
(a)
Reduction of ICG blood concentration expressed as the percentage change over time, starting (time 0) from a concentration of 100 % (normal values >18 %/min). The method, having satisfactory correlation (r 2 = 0.77) with ICGCl, is validated as a surrogate for clearance in the critically ill)
-
(i)
PDR(%/min) = ln 2/t½ × 100 ICGPDR might represent, at variance of ICGR15, ICG uptake by hepatocytes, its excretion into the bile, blood flow-dependent liver metabolism and energy status [21]
-
(i)
-
(a)
-
2.
ICGR15 – retention ratio after 15 min
-
(a)
The relationship between the concentration of ICG at 15 min and initial concentration (normal <10 %)
-
(i)
R15 (%) = C ICG15/C ICG T0 × 100
Assuming an initial plasma concentration of 100 mg/ml (0.5 mg/kg ICG in a subject with a plasma volume of 50 ml/kg BW), ICGR15 can be determined by transforming the ICG concentration curve to a ‘point zero’ (100 %) and then describing the decay (at min 15) as percentage change per time (%/min) in a logarithmic graph, seen as a negative slope. According to Imamura, as the assumption of the initial concentration of ICG is correct, ICGR15 is pharmacologically equivalent to ICG K, and it has been widely used as an alternative to ICGK for its convenience [8]. It might represent the hepatic blood flow.
-
(i)
-
(a)
-
3.
ICG plasma clearance 500–700 ml/min/m2
-
(i)
It depends on hepatic blood flow, liver function and bile flow. It describes the volume of blood completely purified by ICG in the time unit.
-
(i)
ICGPDR and ICGR15 are the two sides of the same phenomenon: ICGPDR reads the disappearance of ICG from plasma (% per min) and ICGR15 the amount of ICG remaining in circulation 15 min after the administration. However, these tests are used in the literature in a different (and potentially confounding) manner. ICGR15 is mainly used in the evaluation of the functional reserve of the liver in case of hepatic resection in cirrhotic patients [8, 11], ICGPDR and ICG R15 in the assessment of liver graft function [22] and PDR and clearance in critically ill patients [3, 21].
As mentioned above, plasma disappearance rate (ICGPDR) and retention rate at 15 min (ICGR15) are calculated using either the conventional invasive method or, more recently and more simply, a noninvasive method (pulse dye densitometry (PDD) and spectrophotometry) [9–11]. The conventional invasive method involves the construction of the dilution curve by measuring the concentration of ICG in plasma by spectrophotometry of various arterial blood samples taken at defined times: it has been used in many studies dealing with functional assessment of the liver even in recent times [19]. However, this method is expensive and difficult to implement in clinical practice. In the 1990s, it was possible to measure PDR through a fibre-optic catheter placed in the femoral artery and connected to a computer (COLD System, Pulsion) which allowed, together with the measurement of PDR, the study of volumetric haemodynamics [23]. As already mentioned, the noninvasive method relies, instead, on the measurement of ICG concentrations using PDD and spectrophotometry via an optical transcutaneous pulse spectrophotometric sensor (DDG-2001 Nihon Kohden; LiMON, Pulsion) [11, 24–26]. Pulse dye densitometry measures the concentration of ICG in blood based on the principle of the difference in absorption of the light wave with two different frequencies: 805 nm (absorption frequency of the peak of ICG) and 905 nm (frequency at which ICG has no absorption); the principle is analogous to the mechanism of absorption of the difference between oxyhaemoglobin and reduced haemoglobin. There is no influence of haemoglobin, whether oxidised or reduced, absorption being very low at the frequency wave used for ICG. The same is true for bilirubin (absorption peak at 470 nm) [9, 10]. This method has been validated both in conditions of haemodynamic stability in critically ill patients as well as in unstable conditions, such as in liver transplantation [22–25]. Both systems have algorithms which calculate the constant K (‘rate constant’) using an equation which deals with the elimination phase (‘backward dynamic extrapolation’) [9]. The ICG kinetic parameters are determined by monoexponential transformation of the original ICG concentration curve, backward extrapolation to the time point ‘zero’ (100 %), and describing the decay as percentage change per time [9]. The algorithm was validated by Purcell et al. determining ICGR15 with LiMON and direct measurement of blood samples [26]. The most recent revisions on this item insist on the need for haemodynamic stability in order to obtain reliable data on liver function [9, 11]. In fact, as already underlined, hepatic blood flow and cellular uptake are variables able to impact on ICG elimination (increasing or decreasing the elimination). The hepatic blood flow can be altered by systemic factors (reduced cardiac output able to impact on the hepatosplanchnic perfusion) or by local factors (thrombosis of the hepatic artery or abdominal hypertension); both tend to reduce ICG elimination. On the contrary, the possibility exists that a splanchnic hyperperfusion results in a rise in the extraction of ICG and therefore in a (false) increased PDR.
True pathological ICGPDR or ICGR15 is present in the case of end-stage liver failure (cirrhosis) or of severe rejection after liver transplantation, both conditions able to reduce ICG liver extracting abilities [9, 10]. Elevated ICGR15 in cirrhotic patients may be due to:
-
1.
Decreased ICG transport from the systemic circulation to the liver
-
2.
Decreased uptake from the sinusoids into hepatocytes
Altered ICGPDR and ICGR15 are present also in case of cholestasis: as mentioned above, ICG and bilirubin, competing for the same carrier in the transport process in hepatocytes (sodium taurocholate cotransporting peptide), can alter ICG elimination parameters (by competition and not by functional defect). This condition, not uncommon in the early postoperative period of liver transplantation, can be associated with falsely pathological results, leading to misinterpretation of the tests. Generally speaking, the pathological results may be wrongly attributed to a condition of liver dys/malfunction (falsely reduced function) which might not be the real condition: falsely altered ICGR15 or ICGPDR is present when serum bilirubin level is >3 mg/dl [9, 10]. Thus, extreme caution must be used interpreting ICG tests in the presence of hyperbilirubinaemia. In the literature, bilirubin level above 3 mg/dl is reported as the cut-off value: in AA’s personal experience in a series of liver-transplanted patients, the cut-off should be at 6 mg/dl [27].
ICGPDR and ICGR15 can be used as a starting point for preoperative screening and evaluation of the functional reserve in the case of liver resection, as proposed by Makuuchi’s group [8]; with sequential assessments during liver transplantation or during the early postoperative period of liver transplant (OLT) (functional recovery of the transplanted liver); after hepatic resection (functional assessment of the remnant liver after hepatic resection, also in case of living-related donation). In both cases, mandatory is caution in interpreting the results in the presence of hyperbilirubinaemia, frequent in post-liver transplantation and able to give false/altered information on ICG results (high R15/low PDR) [27]. Finally, too short intervals between sequential ICG administrations (<30 min) might significantly alter ICG clearance parameters: this phenomenon is correlated with a baseline drift associated with residual circulating ICG, possibly leading to an (incorrectly) increased ICGPDR [9]. Clinical indications for ICG elimination in perioperative liver medicine and ICU are the following [3, 9–11]:
-
1.
Assessment of hepatic functional reserve and prediction of mortality and morbidity in hepatic resection in cirrhotic patients
-
2.
Evaluation of liver function in cadaveric and living donors (not included in this review)
-
3.
Quality assessment of functional recovery of the liver graft in liver transplant (OLT) recipient
-
4.
Prognostic index in critically ill patients with septic shock in the ICU
13.6 ICG Clearance in the Preoperative Assessment of Liver Resection in Cirrhotic Patients
Liver resection and liver transplantation are the surgical procedures able to treat or even cure hepatocellular carcinoma in patients with cirrhosis. Liver resection is reserved to patients with compensated liver function as assessed by static or dynamic tests, scores and imaging [28]. Despite the improvements in surgical techniques and perioperative management, postoperative liver failure still remains an extremely feared complication in cirrhotic patients undergoing liver resection: it ranges, according to the literature, between 5 and 8 % and is associated with a high mortality rate [9, 30–32]. As a matter of fact, while Imamura et al. reported in 2003 0 % mortality out of 1,056 hepatectomies [29], other series still report mortality rate ranging from 2 to 5 % [11, 25–29]. Inadequate functional hepatic reserve, the extent of resection, blood loss/transfusion needs and severe sepsis/septic shock are among the major causes of postoperative liver failure, more frequent in cirrhotic patients [32–38]. Preoperative evaluation of the extent of liver resection is usually based on clinical conditions (the presence or absence of ascites and hepatic encephalopathy), routine liver function tests (AST/ALT, bilirubin, ALK), dedicated MRI/CT volumetric imaging for the estimation/prediction of the volume of the remnant liver and scoring systems [11, 35–38]. For a global assessment, Child–Pugh (CTP) and MELD scores are the most widely used classification systems in clinical practice [32–37]. CTP score was introduced in 1964 by Child and Turcotte and then modified in 1973 by Pugh (CTP) [39, 40] to predict the operative risk in cirrhotic patients undergoing shunt surgery for portal hypertension (Fig. 13.8). Using common biochemical (albumin, bilirubin, prothrombin time) and clinical parameters (the presence of ascites and encephalopathy, classified according to increasing severity), the Child–Pugh classification identifies in chronic liver diseased patients three classes of severity (A, B, C). Different scores for different values of the biochemical and clinical parameters identified subgroups of patients at increasing severity within the three classes (A 5–6, B 7–9; C 10–15) [11]. The classes and the score are able to predict mortality after general surgery in the different classes (CTP A-10 %; CTP B up to 30 %; CTP-C >50 %) [9]. Major flaws of CTP score are global (instead of regional) evaluation of liver function and no indication of the amount of liver parenchyma safely resectable [9, 10] (Fig. 13.6).

Child–Pugh classification (From Mizuguchi et al. [11])
In spite of that, in the Western world, the liver function is still evaluated primarily using CTP [39, 40] and the degree of portal hypertension: hepatic resection in cirrhotic patients is usually reserved for Class A patients and, with limitations, for class B patients (vide infra). In this specific setting, the definition of the extent of the resection is crucial to avoid postoperative hepatic dysfunction [8, 29–32].
The use of MELD score and its derivates (Fig. 13.7, MELD, NaMELD and iMELD) is instead controversial in this specific setting. The MELD score is based on prothrombin time (PT) as INR, bilirubin and creatinine. MELD was first introduced to evaluate the outcome in patients undergoing transjugular intrahepatic portosystemic shunt (TIPS): now MELD score is widely used to assess the severity of chronic liver diseases and its prognosis, as a prognostic indicator of survival in patients awaiting liver transplantation and to prioritise the transplant procedure [41–43]. Its predictive value for mortality in liver resection is debated, due to the narrow range of values in which it is used. In a retrospective study, Cucchetti et al. observed a high frequency of postoperative liver failure in patients with MELD >10 [44]. While uniform agreement exists to exclude for hepatic resection patients in CTP class C or with MELD score >14, subjects in CTP class B or with MELD score ranging from 9 to 14 should undergo a thorough evaluation to determine if and to what extent a liver resection might be feasible [44–46].

MELD and derived scores (From Mizuguchi et al. [11])
On the contrary, the Eastern surgical schools (Japanese, Chinese and Korean) have used, since the 1980s, the quantitative tests, particularly ICG clearance (usually as ICG R15) [8, 34–36] to assess the maximum extent of major hepatic resection associated with good function of the remnant liver. Recently, ICGR15 was added to a score of liver functional evaluation derived from the CTP classification (Liver Damage Grading System) (Fig. 13.8) and recommended by the Liver Cancer Study Group of Japan: according to the proponents, it might become a more accurate tool to assess functional hepatic reserve if compared to the original CTP score [11].

Liver damage grading system (From Mizuguchi et al. [11])
At the beginning of the 1990s, Hemming et al. studied liver function with both conventional and ICG kinetic tests in a group of 22 cirrhotic patients undergoing major liver surgery [46]. While conventional liver function tests were not able to predict mortality, the AAs found ICGcl ≤5.2 ml/kg/min strongly associated with mortality. Lau et al. [15], during the period 1989–1993, preoperatively studied 127 candidates for liver resection with aminopyrine breath test, clearance of amino acids and ICGcl measured as ICG R15 (normal value 0–8 %, range 3.5–10.6). Unlike the other tests, ICGR15 was able to predict in-hospital mortality and specifically to define the ICG R15 values above which the test correctly predicted mortality in major (>14 %) and minor (>23 %) liver resections. According to the literature, resection of three or more Couinaud segments is defined as ‘major’ resection, ‘minor’ being considered the resection of up to two contiguous or isolated segments (see Fig. 13.1) [9–11]. Of the utmost importance was in authors’ view the thorough preoperative liver function assessment and the meticulous and careful surgical technique. In more recent series, which included younger patients with adequate remnant liver volume [35, 47], ICGR15 values associated with mortality after major liver resection were slightly higher (17 % vs. 14 %), thus allowing an extension of the indication of major resections to more compromised patients. In addition to their predictive value, ICG clearance tests may allow a reliable assessment of the extent of the resectable liver parenchyma, keeping in mind in particular that the higher the R15, the smaller the amount of resectable parenchyma should be. In the years 1985–1995, Nonami reported in 318 cirrhotic patients undergoing liver resection a reduction in mortality from 11 to 7 %. The extension of liver resection was mainly guided by an ICGK algorithm: ICGK and the amount of blood loss were predictive of mortality [36]. Major liver resections are usually performed with ICGR15 <15 %; however, in one series, right hepatectomies were performed in patients with ICGR15 >10 % and left hepatectomies with ICGR15 between 10 and 19 % [9–11, 48–50]. In other experiences, in the presence of an estimated ‘sufficient’ remnant liver volume, major hepatic resections were successfully performed with a slightly higher ICGR15 (15–20 %) [47]. ICGR15 became a reference standard after the publication of the results of Makuuchi’s group [8]. The authors reported zero mortality in 1,056 hepatectomies performed in the period 1994–2002; particular attention was given to the following three variables: (i) the presence of ascites, (ii) serum bilirubin values and (iii) ranges of ICG R15 [8, 29].
Main points of the algorithm are:
-
1.
Absolute contraindication to hepatic resection in case of uncontrolled ascites and serum bilirubin >1.9 mg/dl
-
2.
Limited (minor) resections possible in case of bilirubin >1 mg <1.9 mg/dl, depending on serum bilirubin
-
3.
With no ascites and serum bilirubin <1.1 mg/dl, different types of liver resection possible according to the interval of ICG R15 (see original algorithm in [8] and Fig. 13.9)
Fig. 13.9 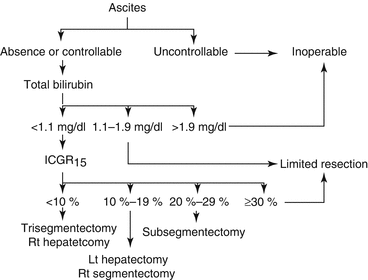
Makuuchi decision tree to select operative procedure in patients with impaired liver function reserve (From Mizuguchi et al. [11])

Very interesting, even if to be definitively implemented so far, is the use of the test in case of liver resection with ICGR15 15–20 % and remnant liver volume deemed ‘not sufficient’. In these cases, preoperative selective portal vein embolisation (PVE) is performed to increase the future ‘remnant’ liver volume by inducing hyperplasia of liver lobules perfused by the contralateral portal vein [9, 10]. The ICGR15 values correlate with volumetric changes of the liver following PVE. ICGR15 after embolisation and immediate before surgery correlates with both volumetric and functional reserve changes [9, 51]. The relationship relies upon the preservation of total hepatic blood flow and the induced hepatic hyperplasia (see original algorithm proposed by Poon and Fan) [35]. In 2009, the Japanese guidelines for the treatment of hepatocellular carcinoma recommended ICGR15 as test for preoperative liver function evaluation (level of evidence B) [48].
Interesting is the use of ICG kinetic tests (R15 or PDR) during or immediately after surgical resection. Recent studies confirm the ability of the ICG tests to predict postoperative morbidity (mainly hepatic dysfunction), but not mortality, due to the absence of a significant number of deaths [49]. Similar results were found at our centre in a series of 100 consecutive cirrhotic patients undergoing liver resection: ICG R15 >40 % was predictive of morbidity but not of mortality [52]. In another smaller study, using intraoperative ICGPDR (normal value >18 %/min), a value of <9 %/min predicted (sensitivity 88 %, specificity 82 %) postoperative liver failure [49]. In another experience, ICGPDR <7 %/min on the first postoperative day was associated, 2–5 days ahead, with the onset of liver failure [50].
As mentioned above, in case of biliary obstruction, a prolonged preoperative ICGR15 value may falsely suggest impaired liver function. Should it be the case, the test must be interpreted with caution and should not be used, as it is, to withhold the intended surgical strategy: in this specific setting, further and multimodal investigations are mandatory [9]. ICG R15 remains a valuable tool to assess functional hepatic reserve together with the liver volume evaluation using tomography or magnetic resonance. In the case of hyperbilirubinaemia, as reported by Ge et al., the Korean and Japanese schools suggest Tc-galactosyl serum albumin scintigraphy (Tc GSAS), to study liver function. GSA is the ideal agent to predict hepatocyte mass and function due to the ability to monitor functional status and distribution of asialoglycoprotein receptor [21].
13.7 Indocyanine Green Kinetics and Liver Transplantation
The conventional static tests of liver function may sometimes leave doubts or uncertainties about the functional recovery of the newly grafted liver, both from cadaveric and living donors [9]. The clearance of ICG expressed as plasma disappearance rate (ICGPDR) or K constant of elimination (the use of ICG R15, is, in fact, much less frequent in liver-transplanted patients) has been used to assess liver function in the cadaveric donor before harvesting and in the liver transplant recipient during and after transplantation, to predict early complications and survival of both the graft and the recipient after the transplant procedure [9].
Organ shortage is one of the major problems in the field of organ transplantation. Marginal or so-called extended criteria donors are now increasingly considered for organ harvesting to expand the donor pool. In this setting, ICGPDR was used in few small single centre studies to assess the quality of the potential graft and to assist the decision about using marginal or extended criteria donors. Unfortunately, the role of ICGPDR to assist in the assessment of graft suitability is weak at best: a value < 15 % min−1 before organ harvesting was associated with primary graft non-function [9]. A combination of ICG kinetics and MELD score (ICG-MELD score) was recently considered to refine the accuracy of survival prediction in candidates awaiting liver transplantation: the ICG-MELD score improved prediction performance in patients with MELD score ranging from 10 to 30 points (intermediate to severely compromised patients) [53].
In liver-transplanted patients, the most feared complications early after the surgical procedure are primary graft non-function (PGNF) and hepatic artery thrombosis (HAT). Both conditions deserve very aggressive treatment: in large part of the cases, urgent/emergent retransplantation is the only solution able to avoid fatality. The studies of Jalan et al. [54], Plevris et al. [55] and Tsubono et al. [56] at the end of the 1990s confirmed the great interest in the use of ICGcl in assessing early liver function and in predicting graft function, graft and patient survival and the final outcome. Essentially, in the early post-transplant period, a ‘low’ ICGPDR (an ill-defined value ranging from 5 to 12 % min−1) was associated with graft malfunction/failure: the major problem in this specific setting is to define a reliable and reproducible cut-off value, not affected by parameters or conditions able to generate falsely altered results (hyperbilirubinaemia, as mentioned above, not uncommon reported early after OLT), which make data unreliable at best and extremely difficult to be interpreted. Jalan et al. [54], invasively studying ICG clearance, observed that ICGcl values greater than 200 ml/min were associated with immediate recovery of liver function and a normal function after 3 months; on the contrary values, <200 ml/min predicted PGNF, retransplantation, long-term care and death. 200 ml/min was found to be the ICGcl value able to predict outcome (100 % sensitivity and 95 % specificity) [55]. Faybik studied the ICGcl in liver-transplanted patients using both invasive (COLD system, Pulsion, Germany) and noninvasive techniques (LiMON, Pulsion, Germany) as ICGPDR [57]. ICGPDR <10 % min was predictive of postoperative complications. In 30 patients who underwent living donor liver transplantation, Hori et al. [58] monitored liver function using ICG test, expressed as ICGK (DDG-2001 Nihon Kohden) for 14 consecutive postoperative days and then at postoperative days (PODs) 21 and 28. According to the outcome, patients were subsequently allocated to two groups. The six patients with unfavourable outcome (increased morbidity and mortality) had ICGK <0.180 24 h after transplantation; this value was able to predict poor outcome at 28 days.
More recently, Levesque et al. identified two main objectives: (a) to determine if the value of ICGPDR measured by noninvasive technique (LiMON, Pulsion) might predict early postoperative complications and (b) to hypothesise the cause of early graft dysfunction [59, 60]. The test was performed daily from POD 1 to POD 5. ICGPDR of 24.4 ± 6.8 % was recorded in the group of patients with good functional recovery of the graft, regular postoperative course and favourable outcome [59]. Patients who suffered early complications were retrospectively divided into two groups: the first included patients with early postoperative complications (PGNF, HAT, septic shock or haemorrhagic shock) and the second, patients with late complications (mainly rejection). ICGPDR in the first group was low during the first 5 days (8.8 ± 4.5 %); in the second group, on the contrary, the ICGPDR, initially normal, decreased significantly within 3–5 days (10.3 ± 2.5 %). Levesque et al. proposed an ICGPDR <12.85 % min−1 in the very early postoperative days as a marker of almost immediate postoperative complications, mainly associated with hepatocellular dysfunction (PGNF) or perfusion deficit secondary to hepatic artery thrombosis (HAT); late (3–5 days after OLT)-onset low ICGPDR (<12.85 % min−1) was instead associated with acute rejection [60], underlining the importance, in authors’ view, of both time course and absolute values of the ICG kinetics. Recently, Olmedilla et al. [61] reported similar results using ICG elimination at the end of surgery (neohepatic phase) or on POD 1. ICGPDR in patients with severe hepatic dysfunction was <10.8 % min and was associated with increased mortality; on the contrary, ICGPDR >10.8 % min was associated with a good outcome and showed high (99 %) negative predictive value [52]. Very recently, Escorsell et al. [62] were not able to confirm the ability of ICGPDR performed on POD 1 to predict liver dysfunction and survival. In fact, the group of patients with ICGPDR <8.8 % min−1 (group A) did not show an outcome worse than the group with value >.8 (group B): in group A, however, bilirubinaemia was significantly higher, likely determining a false reading of the low ICGPDR value (therefore, a falsely malfunctioning graft). Very similar results were found by our group in a series of 76 consecutive patients who underwent OLT. Mazza et al. were unable to confirm ICGPDR <10 % min−1 as reliable predictor of both early graft dysfunction and poor outcome; in this experience, ICGPDR <8 % min−1 was associated with the presence of serum bilirubin >6 mg/dl (the same was for ICGR15), making the results, as above underlined, unreliable [27]. Essentially, the presence of hyperbilirubinaemia altered the test results, falsely showing an initial hepatic dysfunction that was not confirmed by the subsequent clinical course and outcome of both the graft and the patients. In this study, lactate clearance was strongly correlated with the functional recovery of the grafted livers, showing a high positive predictive value, thus confirming a previous study performed by our group [63]. It has to be underlined that other factors/conditions (different values of total protein or haematocrit) might induce similar interferences with ICG kinetics [64].
The need for caution in the interpretation of low values of ICGPDR in order to indicate malfunction of the graft is having further confirmations in studies using LiMAx test (maximal enzymatic liver function), a test used since 2010 to identify patients at risk for hepatic failure, both after liver surgery or liver transplantation [65, 66, 68]. Intravenously administered 13C-methacetin is metabolised to paracetamol and 13CO2. Continuous and noninvasive breath analysis of 13CO2 production is measured as a surrogate of maximal liver metabolic capacity. Lock et al. reported a better predictive ability of LiMAx than ICGPDR. Patients suffering from initial graft dysfunction (defined as technical complications or primary non-function (n = 8)) had significantly decreased LiMAx results, making the test potentially effective to identify very early life-threatening complications after OLT. These observations emphasise once again the importance of the interference of various parameters on PDR/R15 results and the caution needed in the interpretation of these values [9, 10]. In the most recent experience with LiMAx in 167 chronic ESLD patients evaluated for liver transplantation, taking as primary end point 6 months liver-related death, median LiMAx values were significantly lower in patients who died, at variance of ICGPDR, not different in survivors or non-survivors. LiMAx, if compared to ICGPDR and MELD, showed a slightly higher negative predictive value in predicting risk of death within 6 months [66]. The use of ICG kinetics in acute liver failure as prognostic indicator has been reported in small or preliminary series with interesting results [10, 67]: however, it must be underlined that high bilirubin values (present by definition in patients suffering for acute subacute or hyperacute liver failure) might critically influence the results, likely making unreliable or doubtful the tests in this setting. LiMAx has very recently been considered in patients with acute liver failure. The LiMAx was significantly lower in patients who did not recover, whereas neither biochemical parameters nor MELD score showed difference. According to these data, LiMAx test might be effective in predicting the individual prognosis and the need for OLT in ALF [68].
13.8 ICG Kinetics as a Prognostic Score in Intensive Care
ICG kinetics have been long used even within the ICU, to determine the severity of the disease and/or to predict mortality [1, 3, 9, 10, 68–71]. In this setting, it might be interesting to differentiate, having achieved an acceptable haemodynamic stability, the different contributions given to the ICG elimination by parenchymal liver function and hepatic blood flow [1, 68]. In critically ill patients, very common is the use of scores based on clinical and biochemical variables (APACHE II, SAPS II, SOFA), designed to quantify the severity of the disease or to predict mortality. In a retrospective study of 336 critically ill patients, ICGPDR was able to predict mortality in ICU patients similar to SAPS II and APACHE II [70]. Non-survivors had significantly lower values compared with survivors (6.4 %/min vs. 16.5 %/min). In patients with septic shock, ICG kinetics parameters evaluating liver function and perfusion might be able to give a reliable prognostic evaluation. ICGPDR values <8 %/min predicted mortality in patients with septic shock: again sensitivity and specificity were similar to those determined by APACHE II score [70]. Kimura et al. were able to document a favourable outcome associated with an improvement in ICGPDR, while extremely low levels were predictive of poor outcome [71]. It might be hypothesised that in critically ill septic patients in which splanchnic perfusion is appropriately supported by inotropes/pressors, ICGPDR could be considered an indicator of hepatocellular dysfunction if haemodynamic improvement is not associated with a favourable trend in ICG kinetics. Since long, ICG kinetics have been demonstrated of interest to document, in trauma patients, hepatic dysfunction (ICG clearance results preceding the increase in serum bilirubin)[72]. Pollack et al. were able to demonstrate the superiority of ICG clearance compared to the value of bilirubin in predicting survival in patients with trauma or shock [68]. As already reported, the cytokine increase associated with shock might constitute a factor able to interfere with the ICG transport within the liver cell, making not completely reliable the results [9]. Abdominal hypertension (defined as an intraabdominal pressure exceeding 12 mmHg, with values above 20 mmHg associated with abdominal compartment syndrome) [72] might impact on ICG kinetics. Low values of ICGPDR (unfortunately an univocal cut-off is not available, so far) are associated with reduced splanchnic perfusion, and extremely low values of ICGPDR correlate with mortality [9, 10, 72–77]. According to preliminary reports, it might be speculated that low ICGPDR, even if in the presence of normal or near-normal intraabdominal pressure (<15 mmHg) might unveil a suboptimal splanchnic blood flow, thus making ICGPDR a possible early marker of inadequate splanchnic perfusion [76].
13.9 Conclusions
Used since the 1960s for research purposes, the ICG kinetics have received a major boost in clinical use in the recent years, with the introduction of reliable and simple noninvasive monitoring methods (LiMON, Nihon Kohden). The applications in the field of major liver surgery (resection in cirrhotic patients) underscore the relevant implications in predicting both the resectability of liver cancer in cirrhotic patients and the potentials for postoperative liver failure: relevant in this setting are the studies coming from Japan, China and Korea. The ability to predict mortality, however, is still under debate. Despite initial enthusiasms, post-OLT ICG kinetics for the prediction of mortality and morbidity still raise some concerns. This refers, in particular, to the presence of mixed results and ‘false positives’ in the presence of hyperbilirubinaemia (liver grafts falsely classified, according to ICGPDR, as severely dysfunctioning or at unfavourable outcome). Problems are still encountered with the PDR/R15 cut-off values below which they reliably assess poor graft function. While negative predictive values are indeed relevant in predicting good graft outcome (no complications in the presence of ‘normal’ PDR or R15 values), caution is still needed in case of ‘low’ or pathological values. As appropriately commented by Vos et al., ‘further prospective, randomised controlled trials of the ability of ICG elimination measurement to impact positively on outcome are required before the green light can be given for routine clinical use’ [9].
Bibliography
Hawker F (1993) The liver, chap 1. Saunders Co., London, UK, pp 1–43
Mulaikal TA, Edmond JC (2012) Physiology and anatomy of the liver: chap 1. In: Wagener G (ed) Liver anesthesiology and critical care medicine. Springer, New York, pp 3–20
Sakka SG (2007) Assessing liver function. Curr Opin Crit Care 13:207–214
Hoekstra LT, De Graaf W, Niboug G, Heger M, Bennick JR, Stieger B, Van Gulik TM (2013) Physiological and biochemical basis of clinical liver function tests. Ann Surg 257:1–27
Dufour DR, Qazi N (2012) Evaluation of liver disease: chap 4. In: Wagener G (ed) Liver anesthesiology and critical care medicine. Springer, New York, pp 51–58
Slack A, Ladher N, Wendon J (2012) Acute hepatic failure: chap 2. In: Wagener G (ed) Liver anesthesiology and critical care medicine. Springer, New York, pp 21–41
Wagener G (2013) Assessment of hepatic function, operative candidacy, and medical management after liver resection in the patient with underlying liver disease. Semin Liver Dis 33:204–212
Imamura H, Sano K, Sugawara S, Kukudo N, Makuuchi M et al (2005) Assessment of hepatic reserve for indication of hepatic resection: decision tree incorporating indocyanine green test. J Hepatobiliary Pancreat Surg 12:16–22
Vos JJ, Wietasch JKG, Absalom AR, Hendriks HGD, Scheeren TWL (2014) Green light for liver function monitoring using indocyanine green? An overview of current clinical application. Anesthesia. doi:10.1111/anae.12755
Halle BM, Poulsen TD, Pedersen HP (2014) Indocyanine green plasma disappearance rate as dynamic liver function test in critically ill patients. Acta Anesthesiol Scand 58:1214–1219
Mizuguchi T, Kawamoto M, Meguro M, Hui TT, Hirata K (2014) Preoperative liver function assessments to estimate the prognosis and safety of liver resections. Surg Today 44:1–10
Leevy CM, Mendenhall CL, Lesko W, Howard MM (1962) Estimation of hepatic blood flow with indocyanine green. J Clin Invest 41:1169–1180
Pessayre D, Lebrec D, Descantoire V et al (1978) Mechanism for reduced drug clearance in patients with cirrhosis. Gastroenterology 74:566–571
Paumgartner G, Probst P, Kraines R, Leevy CM (1970) Kinetics of indocyanine green removal from the blood. N Y Acad Sci 170:134–147
Lau H, Man K, Fan ST et al (1997) Evaluation of preoperative hepatic function in patients with hepatocellular carcinoma undergoing hepatectomy. Br J Surg 84:1255–1259
Shinohara H, Tanaka A, Kital T et al (1996) Direct measurement of hepatic indocyanine green clearance with near-infrared spectroscopy: separate evaluation of uptake and removal. Hepatology 23:137–144
Cui Y, Konig J, Leier J et al (2001) Hepatic uptake of bilirubin and its conjugates by the human organic anion transporter SLC21A6. J Biol Chem 276:9626–9636
Keiding S (1987) Hepatic clearance and liver blood flow. J Hepatol 4:393–398
Kawasaki S, Sugiyama Y, Yga T et al (1985) Pharmacokinetic study on the hepatic uptake of indocyanine green in cirrhotic patients. Am J Gastroenterol 80:801–806
Huet PM, Goresky CA, Villeneuve JP et al (1982) Assessment of liver microcirculation in cirrhosis. J Clin Invest 70:1234–1244
Ge PL, Du SD, Mao YL (2014) Advances in preoperative assessment of liver function. Hepatobiliary Pancreat Dis Int 13:361–370
Faybik P, Krenn C-G, Baker A, Lahner D, Berlakovich G, Steltzer H, Hetz H (2004) Comparison of invasive and noninvasive measurement of plasma disappearance rate of indocyanine green in patients undergoing liver transplantation: a prospective investigator-blinded study. Liver Transpl 10:1060–1064
Kisch H, Leucht S, Lichtwarck-Aschoff M et al (1995) Accuracy and reproducibility of the measurement of actively circulating blood volume with an integrated fiberoptic monitoring system. Crit Care Med 23:885–893
Aoyagi T, Fuse M et al (1994) Pulse dye-densitometry. Jpn J Clin Monit 5:371
Sakka SG, Reinhart K, Meier Hellmann A (2000) Comparison of invasive and non invasive measurements of indocyanine green plasma disappearance rate in critically ill patients with mechanical ventilation and stable hemodynamics. Intensive Care Med 26:1553–1556
Purcell R, Kruger P, Jones M (2006) Indocyanine green elimination: a comparison of the Limon and serial blood sampling methods. ANZ J Surg 76:75–77
Mazza E, Prosperi M, DeGasperi A et al (2008) Plasma disappearance rate of indocyanine green after liver transplantation: always a reliable tool to predict graft function and out come? Liver Transpl 14:S201
Manizate F, Hiotis SP, Labow D et al (2010) Liver functional reserve estimation: state of the art and relevance for local treatments. J Hepatobiliary Pancreat Sci 17:385–388
Imamura H, Makuuchi M et al (2003) One thousand fifty-six hepatectomies without mortality in 8 years. Arch Surg 138:1198–1206
Bellavanca EC, Lumpkins KM et al (2008) Surgical management of early – stage hepatocellular carcinoma: resection or transplantation ? J Gastrointest Surg 12:1699–1708
Jarnagin W, Gonen M, Fong Y et al (2002) Improvement in perioperative outcome after hepatic resection: analysis of 1803 consecutives cases over the past decade. Ann Surg 236:397–407
Fan ST (2010) Liver functional estimation: state of art and relevance for local treatments: the eastern perspective. J Hepatobiliary Pancreat Sci 17:380–384
Bruix J, Castells A, Bossch J et al (1996) Surgical resection of hepatocellular carcinoma in cirrhotic patients: prognostic value of preoperative portal pressure. Gastroenterology 111:1018–1022
Lee S, Shin Hwang (2005) How I do it: assessment of hepatic functional reserve for indication of hepatic resection. J Hepatobiliary Pancreat Surg 12:38–43
Poon RT, Fan ST (2005) Assessment of hepatic reserve for indication of hepatic resection: how I do it. J Hepatobiliary Pancreat Surg 12:31–37
Nonami T, Nakao A et al (1999) Blood loss and ICG clearance as best prognostic markers of post-hepatectomy liver failure. Hepatogastroenterology 46:1669–1672
Janssen MW, Druckerey-Fiskaaen KY et al (2010) Indocyanine green R 15 ratio depends directly on liver perfusion flow rate. J Hepatobiliary Pancreat Sci 17:180–185
Capussotti L, Viganò L et al (2009) Liver dysfunction and sepsis determine operative mortality after liver resection. Br J Surg 96:88–94
TurcotteJ G, Child GG (1964) Surgery and portal hypertension. Major Probl Clin Surg 1:1–85
Pugh RWH, Murray –Lyon IM et al (1983) Transection of the esophagus for bleeding esophageal varices. Br J Surg 60:646–649
Malinchoc M, Kamath PS, Gordon FD, Peine CJ, Rank J, ter Borg PC (2000) A model to predict poor survival in patients undergoing transjugular intrahepatic portosystemic shunts. Hepatology 31:864–871
Dutkowski P, Oberkofler CE, Béchir M, Müllhaupt B, Geier A, Raptis DA et al (2011) The model for end-stage liver disease allocation system for liver transplantation saves lives, but increases morbidity and cost: a prospective outcome analysis. Liver Transpl 17:674–684
Cholongitas E, Marelli L, Shusang V et al (2006) A systematic review of the performance of the model for end-stage liver disease (MELD) in the setting of liver transplantation. Liver Transpl 12:1049–1061
Cucchetti A, Ercolani G, Vivarelli M et al (2006) Impact of model for end-stage liver disease (MELD) score on prognosis after hepatectomy for hepatocellular carcinoma on liver cirrhosis. Liver Transpl 12(6):966–971
Teh SH, Christein J et al (2005) Hepatic resection of hepatocellular carcinoma in patients with cirrhosis: Model of End-Stage Liver Disease (MELD) score predicts perioperative mortality. J Gastrointest Surg 9:1207–1215
Hemming AW, Scudamore CH, Shackleton CR, Pudek M, Erb SR (1992) Indocyanine green clearance as a predictor of successful hepatic resection in cirrhotic patients. Am J Surg 163:515–518
Lam CM, Fan S, lo CM, Wong J (1999) Major hepatectomy for hepatocellular carcinoma in patients with an unsatisfactory indocyanine green clearance test. Br J Surg 86:1012–1017
Kokudo N, Makuuchi M (2009) Evidence–based clinical practice guidelines for hepatocellular carcinoma in Japan: the Japan _HCC guidelines. J Gastroenterol 44:119–121
Ohwada S, Kawate S, Hamada K et al (2006) Perioperative real time monitoring of indocyanine green clearance by pulse spectrophotometry predicts remnant liver functional reserve in resection of hepatocellular carcinoma. Br J Surg 93:339–346
Greco E, Nanji S, Bromberg IL, Shah S, Wei AC, Moulton C-A, Greig PD, Gallinger S, Cleary SP (2011) Predictors of periopertative morbidity and liver dysfunction after hepatic resection in patients with chronic liver disease. HPB (Oxford) 13:559–565
Shindoh JD, Tzeng CW, Vauthey JN (2012) Portal vein embolization for hepatocellular carcinoma. Liver Cancer 1:159–167
Mazza E, Kroeller D, Prosperi M et al (2013) Does ICG clearance (ICGR15) predict morbidity and mortality after hepatic resection for hepatocellular carcinoma in cirrhotic patients? Intensive Care Med Abs. Transpl Inter (Suppl 2) 185–329, S609
Zipprich A, Kuss O, Rogowski S et al (2010) Incorporating indocyanine green clearance into the model for end stage liver disease (MELD-ICG) improves prognostic accuracy in intermediate to advanced cirrhosis. Gut 59:963–968
Jalan R, Plevris JN, Jalan AR, Bzeizi KI, Dollinger MM, Lee A, Garden OJ, Hayes PC (1994) A pilot study of indocyanine green clearance as an early predictor of graft function. Transplantation 58:196–200
Plevris JN, Jalan R et al (1999) Indocyanine green clearance reflects reperfusion injury following liver transplantation and is an early predictor of graft function. J Hepatol 30:142–148
Tsubono T, Todo S, Jabbour N, Mizoe A, Warty V, Demetris AJ, Starzl TE et al (1996) Indocyanine green elimination test in orthotopic liver recipients. Hepatology 24(5):1165–1171
Faybik G, Hetz H (2006) Plasma disappearance rate of indocyanine green in liver dysfunction. Transplant Proc 38:801–802
Hori T, Lida T et al (2006) Kicg value, a reliable real–time estimator of graft function, accurately predicts outcomes in adult living-donor liver transplantation. Liver Transpl 12:605–613
Levesque E, Saliba F, Benhamida S et al (2009) Plasma disappearance rate of indocyanine green: a tool to evaluate early graft outcome after liver transplantation. Liver Transpl 15:1358–1364
Levesque E, Hoti E, Azoulay D, Saliba F et al (2011) Non-invasive ICG-clearance: a useful tool for the management of hepatic artery thrombosis following liver transplantation. Clin Transpl 25:297–301
Olmedilla L, Perez-Pena JM et al (2009) Early noninvasive measurement of the indocyanine green plasma disappearance rate accurately predicts early graft dysfunction and mortality after deceased donor liver transplantation. Liver Transpl 15:1247–1253
Escorsell A, Mas A et al (2012) Limitations of use of the noninvasive clearance of indocyanine green as a prognostic indicator of graft function in liver transplantation. Transplant Proc 44:1539–1541
De Gasperi A, Mazza E, Corti A et al (1997) Lactate blood levels in the perioperative period of orthotopic liver transplantation. Int J Clin Lab Res 27:123–128
Kim GA, Bae KS, Noh GJ et al (2009) Estimation of indocyanine green elimination rate constant k and retention rate at 15 min using patient age, weight, bilirubin and albumin. J Hepatobiliary Pancreat Surg 16:521
Lock JF, Schwabauer E, Martus P et al (2010) Early diagnosis of primary nonfunction and indication for reoperation after liver transplantation. Liver Transpl 16:172–180
Jara M, Malinowski M, Lüttgert K, Schott E, Neuhaus P, Stockmann M (2015) Prognostic value of enzymatic liver function for the estimation of short-term survival of liver transplant candidates: a prospective study with the LiMAx test. Transpl Int 28:52–58
Merle U, Sieg O, Stremmel W, Encke J, Eisenbach C (2009) Sensitivity and specificity of plasma disappearance rate of indocyanine green as a prognostic indicator in acute liver failure. BMC Gastroenterol 9:91
Lock JF, Kotobi AN, Malinowski M, Schulz A, Jara M, Neuhaus P, Stockmann M (2013) Predicting the prognosis in acute liver failure: results from a retrospective pilot study using the LiMAx test. Ann Hepatol 12:556–562
Pollack DS, Sufian S, Matsumoto T (1979) Indocyanine green clearance in critically ill patients. Surg Gynecol Obstet 149:852
Inal MT, Memis D, Kargi M, Sut N (2009) Prognostic value of indocyanine green elimination assessed with LiMON in septic patients. J Crit Care 24:329–334
Sakka SG, Reinhart K, Meier-Hellmann A (2002) Prognostic value of the indocyanine green plasma disappearance rate in critically ill patients. Chest 122:1715–1720
Kimura S, Yoshioka T et al (2001) Indocyanine green elimination rate detects hepatocellular dysfunction early in septic shock and correlates with survival. Crit Care Med 29(6):1159–1163
An G, West MA (2008) Abdominal compartment syndrome: a concise clinical review. Crit Care Med 36:1304–1310
Gottlieb ME, Stratton HH, Newell JC et al (1984) Indocyanine green. Its use as an early indicator of hepatic dysfunction following injury in man. Arch Surg 119:264
Sakka SG (2007) Indocyanine green plasma disappearance rate as an indicator of hepato-splanchnic ischemia during abdominal compartment syndrome. Anesth Anal 104:1003–1004. 109
Thumer O, Huttemann E, Sakka SG (2007) Indocyanine green plasma disappearance rate. Marker of partial hepatosplanchnic ischemia. Anaesthesist 56:339–344
Seibel A, Muller A, Sakka SG (2011) Indocyanine green plasma disappearance rate for monitoring hepatosplanchnic blood flow. Intensive Care Med 37:357–359
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2015 Springer International Publishing Switzerland
About this chapter
Cite this chapter
De Gasperi, A., Mazza, E. (2015). Clinical Use of Indocyanine Green (ICG) Kinetics in Liver Anaesthesia and ICU. In: Chiumello, D. (eds) Practical Issues Updates in Anesthesia and Intensive Care. Springer, Cham. https://doi.org/10.1007/978-3-319-18066-3_13
Download citation
DOI: https://doi.org/10.1007/978-3-319-18066-3_13
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-18065-6
Online ISBN: 978-3-319-18066-3
eBook Packages: MedicineMedicine (R0)