
Abstract
Ultrasound performed and interpreted by the clinician combines knowledge of the anatomy and disease processes with technical expertise to produce images of superior quality which answer a specific clinical question. An understanding of the physical principles of ultrasound, proper probe selection and machine settings is critical to obtaining high quality diagnostic images. This chapter will describe the physical principles of ultrasound along with an explanation for how to adjust machine settings to correct for common ultrasound artifacts.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
Ultrasound performed and interpreted by the clinician combines knowledge of the anatomy and disease processes with technical expertise to produce images of superior quality which answer a specific clinical question. An understanding of the physical principles of ultrasound, proper probe selection and machine settings is critical to obtaining high quality diagnostic images. This chapter will describe the physical principles of ultrasound along with an explanation for how to adjust machine settings to correct for common ultrasound artifacts.
Physics of Ultrasound
The images generated by ultrasound are created by the interaction between the mechanical ultrasound waves and human tissue. Ultrasound requires a conducting medium (ultrasound gel) and a physical medium such as tissue or fluid. The ultrasound waves are transmitted into the body by the transducer and then reflected back to the transducer at frequent intervals producing a real-time image. The transducer acts as both a sender and a receiver.
The sound waves are generated by electrical impulses which are converted to mechanical sound waves via the piezoelectric effect. The piezoelectric effect [1] occurs when alternating current is applied to a crystal containing dipoles. Areas of charge within a piezoelectric element are distributed in patterns which yield a “net” positive and negative orientation. When alternating charge is applied to both faces of the element, a relative contraction or elongation of the charged areas occurs, resulting in a mechanical expansion and then a contraction of the element (Fig. 1.1). This results in a mechanical wave which is transmitted into the patient. These ultrasound waves are longitudinal waves which produce compression and rarefaction of tissue in the direction of the wave (Fig. 1.2).

Piezoelectric effect. Areas of “net” charge within a crystal expand or contract when current is applied to the surface, creating a mechanical wave. When the returning wave strikes the crystal an electrical current is generated

Longitudinal waves are created by the expansion and contraction of piezoelectric crystals within the transducer. These waves are created when an alternating current is applied to the crystals which create compression and rarefaction of molecules in the body
Reflected mechanical sound waves are received by the transducer and converted back into electrical energy via the piezoelectric effect. The electrical energy is interpreted via software within the ultrasound instrument to generate an image which is displayed upon the monitor.
This compression and rarefaction of molecules can be represented graphically as a sine wave (Fig. 1.3) which alternates between a positive and negative deflection from the baseline. The wavelength is the distance between one peak of the wave and the next peak. A cycle is the complete path of the wave. One cycle per second is known as 1 Hz (Hertz). The maximal excursion of the wave in the positive or negative direction from the baseline is the amplitude of the wave. The time it takes for one complete cycle of the wave is known as the period. The amplitude of the wave is a function of the acoustical power used to generate the mechanical compression wave and the medium through which it is transmitted.

Sine wave: when referring to a sine wave a cycle represents the path of the wave from above the baseline then below the baseline and back to the baseline
For most modes of ultrasound, the transducer emits a limited number of wave cycles (usually two to four) called a pulse. The frequency of the two to four wave cycles, called the pulse repetition frequency, is usually less than 2 KHz. The transducer is then “silent” as it awaits the return of the reflected waves from within the body (Fig. 1.4). The transducer serves as a receiver more than 99 % of the time.

The pulsed-wave ultrasound mode depends on an emitted pulse of 2–4 wave cycles followed by a period of “silence” as the transducer awaits the return of the emitted pulse
The pulse repetition frequency (PRF) is the number of pulses being sent out per unit time. By timing the pulse from transmission to reception it is possible to calculate the distance from the transducer to the object reflecting the wave. This is known as ultrasound ranging (Fig. 1.5). This sequence is known as pulsed-wave ultrasound.

Demonstrates ultrasound ranging. The elapsed time from the transducer (A) to a bladder tumor (B) is 0.045 ms. The total time it takes to travel back to the transducer (C) is 0.09 ms
Ultrasound ranging depends on assumptions about the average velocity of ultrasound in human tissue to locate reflectors in the ultrasound field. The elapsed time from pulse transmission to reception of the same pulse by the transducer allows for determining the location of a reflector in the ultrasound field.
The amplitude of the returning waves determines the brightness of the pixel assigned to the reflector in an ultrasound image. The greater the amplitude of the returning wave the brighter the pixel assigned. Thus, an ultrasound unit produces an “image” by first causing a transducer to emit a series of ultrasound waves at specific frequencies and intervals and then interpreting the returning echoes for duration of transit and amplitude. This “image” is rapidly refreshed on a monitor to give the impression of continuous motion. Frame refresh rates are typically 12–30/s. The sequence of events depicted in Fig. 1.6 is the basis for all “scanned” modes of ultrasound including the familiar gray-scale ultrasound.

Schematic depiction of the sequence of image production by an ultrasound device
Frequency and wavelength affect the velocity with which sound travels through tissue. The velocity of sound in tissue is constant; therefore, changing the frequency will change the wavelength and influence the depth of penetration.
The velocity with which a sound wave travels through tissue is a product of its frequency and its wavelength. The velocity of sound in a given tissue is constant. Therefore, as the frequency of the sound wave changes the wavelength must also change. The average velocity of sound in human tissues is 1,540 m/s. Wavelength and frequency vary in an inverse relationship. Velocity equals frequency times wavelength. As the frequency diminishes from 10 to 1 MHz the wavelength increases from 0.15 to 1.5 mm. This has important consequences for the choice of transducer depending on the indication for imaging.
Common Ultrasound Interactions with Human Tissue
Ultrasound waves are altered in a variety of ways as they interact with human tissue. There may be loss of energy, change in direction or a change in frequency. In order to maximize image quality and correctly interpret the images the sonographer must understand these interactions.
Attenuation
Sound waves lose energy as they interact with tissue and fluid within the body [2]. This interaction is called attenuation. Attenuation is measured in dB/cm/MHz. The greater is the attenuation, the more energy is lost as the soundwave passes through the tissue. The amount of attenuation that may occur varies by specific tissues. For example, the kidney has an attenuation of 1.0 and muscle an attenuation of 3.3. Therefore, sound waves will lose more energy as they pass through muscle.
The three most important mechanisms of attenuation are absorption, reflection and scattering. Absorption occurs when the mechanical kinetic energy of a sound wave is converted to heat within the tissue. Absorption is dependent on the frequency of the sound wave and the characteristics of the attenuating tissue. Higher frequency waves are more rapidly attenuated by absorption than lower frequency waves.
Correcting for Attenuation
Since sound waves are progressively attenuated with distance traveled, deep structures in the body (for example kidney) are more difficult to image. Compensation for loss of acoustic energy by attenuation can be accomplished by selecting a lower frequency or by increasing the acoustic power. Adjusting the gain settings to increase the sensitivity of the transducer to the returning sound waves and will result in a brighter image, however, it will not increase the effective energy of the reflected ultrasound wave.
Refraction
Refraction occurs when a sound wave encounters an interface between two tissues of differing impedance and at any angle other than 90°. When a wave strikes an interface at an angle a portion of the wave is reflected and a portion is transmitted into the adjacent tissue. The transmitted wave is refracted, which results in a loss of some information because the wave is not completely reflected back to the transducer (Fig. 1.7).

When a wave strikes the interface between two tissues of differing impedance, the wave is usually partially reflected and partially transmitted with refraction. A portion of the wave is reflected (θR) at an angle equal to the angle of insonation (θi), a portion of the wave is transmitted at a refracted (θt) angle into the second tissue
There are also potential errors in registration of object location because of the refraction of the wave.
Correcting for Refraction
Refraction may be minimized by altering the angle of insonation to make it as close to 90° as feasible.
Reflection
Reflection which occurs when a sound wave strikes an object with a large flat surface is called a specular reflection. Specular reflection may occur, for example, when sound waves strike the bladder wall during pelvic ultrasound.
Diffuse reflection occurs when an object is small or irregular resulting in a scattering pattern or “speckle effect”. This type of reflection may often be seen with ultrasound of the uterus or testis (Fig. 1.8).

In this transverse image of the bladder, the rectus abdominis muscle (A) is a diffuse reflector. Note the speculated or finely granular nature of the muscle. The bladder wall (B) serves as a specular reflector. A specular reflector reflects sound waves at an angle equal to the incident angle without producing a pattern of interference caused by scattering
Correcting for Reflection
Recognizing reflection as a normal occurrence with ultrasound as opposed to a pathological abnormality of tissue is important. This is a physical property of ultrasound waves and there are no machine settings to correct for reflection. When reflection impedes the interpretation of some portion of the ultrasound field, it can be mitigated by changing the angle of insonation.
Impedance
Impedance occurs when a certain amount of energy is reflected at the interface between tissues of differing tissue density. The amount of energy reflected increases when there is a greater difference between the tissue. For example, there is very little difference in impedance between kidney (1.63) and liver (1.64) so it is difficult to distinguish between these two organs unless there is a layer of fat around the kidney which has a lower impedance factor of 1.38 (Table 1.1).
Fat has a sufficient impedance difference from both kidney and liver that the borders of the two organs can be distinguished by virtue of the intervening fat (Fig. 1.9).

Image (a) demonstrates that when kidney and liver are directly adjacent to each other it is difficult to appreciate the boundary between the capsules of the kidney and liver (arrow). Image (b) demonstrates that when fat, which has significantly lower impedance (arrow) is interposed it is far easier to appreciate the boundary between liver capsule and fat
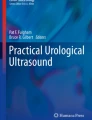
If the impedance differences between tissues are very high, complete reflection of sound waves may occur, resulting in acoustic shadowing (Fig. 1.10).

In the urinary bladder, reflection of sound waves is the result of large impedance differences between urine and the bladder calculus (thin arrow). Acoustic shadowing results from nearly complete reflection of sound waves (area between the thick arrows)
Correcting for Impedance
There are no machine settings to correct for impedance. Imaging the patient from different angles to avoid the interface with large impedance differences may be helpful. In the case of a patient with bladder stones, having the patient physically turn or rotate will cause the stones to move, confirm the presence of the mobile stones and allow imaging of different parts of the bladder.
Common Artifacts
Sound waves are emitted from the ultrasound transducer with a known amplitude, direction, and frequency. However, interactions with tissues in the body result in alterations of these parameters. Because of the physical properties of ultrasound and the assumption by software algorithms in the ultrasound machine that returning sound waves have undergone alterations according to expected physical principles such as attenuation with distance, images are sometimes produced which do not accurately reflect the underlying anatomy. These are known as artifacts. Knowing the most common artifacts in ultrasound and how to correct for them is important when performing and interpreting ultrasound
Increased Through-Transmission
When sound waves pass through tissue that has less attenuation than surrounding tissue “increased through-transmission” will result. For example, the area distal to a fluid-filled bladder will appear brighter than surrounding histologically identical tissue. This hyperechogenicity may obscure structures within the area of increased through-transmission (Fig. 1.11).

(a) The fluid-filled bladder results in a region of decreased attenuation which produces a hyperechoic appearance in the tissue posterior to the urinary bladder (bracket). (b) This artifact called “increased thru-transmission” (bracket) can be corrected by decreasing the TGC curve in this region (arrow)
Correcting for Increased Through-Transmission
This artifact can be overcome by changing the angle of insonation or adjusting the time-gain compensation (TGC) (Fig. 1.11b). Reducing the gain level in the area distal to the bladder will decrease the brightness. The relative echogenicity of tissues known to be structurally or histologically identical should be consistent from the top of the image to the bottom.
Acoustic Shadowing
If there is significant attenuation of sound waves, acoustic shadowing may occur. This may occur at the interface between tissues of different impedance and will result in an anechoic or hyperechoic shadow. Information about the region distal to the interface will be lost or diminished.
Correcting for Acoustic Shadowing
The problems with acoustic shadowing are most appropriately overcome by changing the angle of insonation or changing the position of the target organ. This can be done by turning the patient (e.g. turning a patient on their side to gain access to the kidney lateral to the intestine) or by compression of the abdomen with the probe to move bowel gas aside. In pelvic scanning a roll can be placed beneath the buttock to improve the angle of insonation to the prostate posterior to the pubic bone (Fig. 1.12).

(a) In this sagittal, transabdominal image of the bladder and prostate, there is a shadow distal to the pubis obscuring the apex of the prostate (arrow). (b) In this image, a roll has been placed under the patient’s buttocks (arrow) to lift this pelvis enabling the probe to be angled thus displaying more of the apex of the prostate
Edging Artifact
Edging artifact occurs when an ultrasound wave strikes a curved surface. The sound wave is refracted at the critical angle of insonation resulting in a shadow and a loss of information distal to the interface (Fig. 1.13).

(a) Edging artifact seen in this transverse image of the prostate is the result of the lack of reflection of the sound wave from the curved lateral surface of the transition zone (thick arrows). (b) Edging artifact caused by the rounded upper pole of the kidney (thick arrows)
Correcting for Edging Artifact
Edging artifact is usually corrected by changing the angle of insonation.
Reverberation Artifact
Reverberation artifact occurs when there are large differences in impedance between two adjacent structures or surfaces resulting in two strong reflective interfaces. The sound wave reverberates between the two interfaces. As the sound wave is successively reflected there is ongoing attenuation with each reverberation. This produces echoes that are equally spaced but progressively less intense (Fig. 1.14). This artifact may also be seen when the incident wave strikes smaller reflective objects such as the gas-fluid mixture in the small bowel. This results in a hyperechoic reflection distal to the structure with progressive attenuation of the sound wave (Fig. 1.15).

A reverberation artifact occurs when a sound wave is repeatedly reflected between two interfaces. The resultant echo pattern is a collection of artifactual hyperechoic echoes distal to the structure with progressive attenuation of the sound wave

In this transverse image of the seminal vesicles (A), a loop of small bowel (B) containing gas and fluid creates an example of a reverberation artifact (arrows)
Reverberation artifact is often seen posterior to bowel (which contains air bubbles).
Correcting for Reverberation Artifact
Reverberation artifact may be overcome by changing the angle of insonation. When reverberation is caused by gas, compressing the abdominal wall with the probe may help to displace some of the gas.
Modes of Ultrasound
The most common modes of ultrasound used in clinical urological ultrasound are gray-scale (B-mode ultrasound) and Doppler ultrasound.
Gray-scale ultrasound
Gray-scale ultrasound images are produced when ultrasound waves are transmitted in a timed and sequential way (pulsed wave). The time of travel and degree of attenuation of the wave are reflected by the position on the monitor and the intensity by “brightness”, respectively, of the corresponding pixel. Each sequential echo is displayed as a vertical line of pixels side-by-side and the entire image refreshed at 15–40 frames/s. This results in the illusion of continuous motion or “real-time” scanning. The intensity of the reflected sound waves may vary by a factor of 1012 or 120 dB [3]. Ultrasound units internally process and compress ultrasound data to allow it to be displayed on a monitor. Evaluation of gray-scale imaging requires the ability to recognize the normal patterns of echogenicity from anatomic structures. Variations from these expected patterns of echogenicity may indicate disorders of anatomy or may represent artifacts.
Doppler ultrasound
The Doppler ultrasound Mode depends on the physical principle of frequency shift which occurs when a sound waves strikes a moving object. The frequency of sound waves will be shifted or changed based on the direction and velocity of the moving object they strike as well as the angle of insonation. This phenomenon allows for the characterization of motion; most commonly the motion of blood through vessels. Detecting flow may also be useful for detecting the flow of urine from the ureteral orifices. In pelvic ultrasound for example demonstration of flow by Doppler can distinguish a dilated ureter from a pelvic blood vessel.
Doppler effect
The Doppler effect is a shift in the frequency of the transmitted sound wave based on the velocity and direction of the reflecting object that it strikes. If the reflecting object is stationary relative to the transducer then the returning frequency will be equal to the transmitted frequency. However, if the echo-generating object is traveling towards the transducer the returning frequency will be higher than the transmitted frequency. If the object generating the echo is traveling away from the transducer then the reflected frequency will be lower than the transmitted frequency. This is known as the frequency shift, or “Doppler shift” (Fig. 1.16).

Doppler effect. FT is the transmitted frequency. When the FT strikes a stationary object the returning frequency FR is equal to the FT (a). When the FT strikes a moving object the FR is “shifted” to a higher (b) or lower frequency (c)
The frequency shift of the transmitted wave is also dependent on the angle of the transducer relative to the object in motion. The maximum Doppler frequency shift occurs when the transducer is oriented directly on the axis of motion of the object being insonated. That is, when the transducer is oriented parallel (angle θ = 0°) to the direction of motion, the shift is maximal. Conversely, when the transducer face is oriented perpendicular to the direction of motion (angle θ = 90°) there will be no shift in Doppler frequency detected regardless of the transmitted frequency (Fig. 1.17).

Maximum frequency shifts are detected when the transducer axis is parallel to the direction of motion Angle θ = 0° (A). No frequency shift is detected when the transducer axis is perpendicular to the direction of motion Angle θ = 90° (B)
An accurate representation of velocity of flow depends on the angle (θ) between the transducer and the axis of motion of the object being insonated (Fig. 1.18). The angle should be less than or equal to 60° to minimize the error in calculation of the frequency shift.

Angle of insonation. The calculated velocity of an object using Doppler shift is dependent on the transducer angle (θ). If the transducer axis is perpendicular to the direction of flow (90o) then the cosign of θ is 0 (A). Based on this formula for Doppler shift (ΔF), the detected frequency change would be 0 (Adapted from Radiographics. 1991;11:109–119)
Color Doppler
Color Doppler ultrasonography allows for an evaluation of the velocity and direction of an object in motion. A color map may be applied to the direction. The most common color map uses blue for motion away from the transducer and red for motion toward the transducer (Fig. 1.19).

In this image of the radial artery, blood is flowing through the curved vessel from A to C. (inset image designated by arrow) Flow towards the transducer (A) is depicted in red. Flow in the middle of the vessel (B) is perpendicular to the transducer axis and produces no Doppler shift thus, no color is assigned even though the velocity and intensity of flow are uniform through the vessel. Flow away from the transducer (C) is depicted in blue
The velocity of motion is designated by the intensity of the color. The greater the velocity of the motion, the brighter is the color displayed. Color Doppler may be used to characterize blood flow in the kidney, testis, penis and prostate. In pelvic imaging Color Doppler may be useful in the detection of “jets” of urine emerging from the ureteral orifices (Fig. 1.20).

Ureteral jets (arrows) appear red or orange in these color Doppler images since the urine is flowing towards the transducer
An accurate representation of flow characteristics requires attention to transducer orientation relative to the object in motion. Therefore, in most clinical circumstances the angle between the transducer and the direction of motion should be less than or equal to 60° (Fig. 1.21).

The transducer angle should be ≤60° relative to the axis of fluid motion to allow a more accurate calculation of the velocity of flow
When it is not possible to achieve an angle of 60° or less by manipulation of the transducer the beam may be “steered” electronically to help create the desired angle θ (Fig. 1.22).

Beam steering. In image (a) the angle of insonation is 75° (yellow circle) relative to the vessel which is unfavorable for accurate velocity calculations. This is because the axis of the transducer is perpendicular to the vessel. The beam angle is indicated by the green line. In image (b) the beam has been “steered” to produce an angle of 55° (yellow circle) without changing the physical position of the transducer. Note the beam angle (green line). The resultant velocity calculation is more accurate at 55°
Power Doppler
Power Doppler ultrasonography is a mode which assigns the amplitude of the waves associated with a given frequency shift to a color map. This does not permit evaluation of velocity or direction of flow but is less affected by back-scattered waves. Power Doppler is therefore less angle-dependent than color Doppler and is more sensitive for detecting flow [4].
When a sound wave strikes an object within the body, the sound wave is altered in a variety of ways including changes in frequency and changes in amplitude (Fig. 1.23).

Backscatter is defined as a combination of changes in frequency and amplitude which occur in the reflected sound wave of a primary frequency
While color Doppler assigns the changes in frequency to a color map, power Doppler assigns changes in integrated amplitude (or power) to a color map. It is possible to assign low level back scattered information to a color which is unobtrusive on the color map, thereby allowing increased gain without interference from this backscattered information (Fig. 1.24). Power Doppler may be more sensitive than color Doppler for the detection of diminished flow [4].

(a) For power Doppler the intensity of color is related to changes in amplitude (power) rather than changes in frequency. (b) In this image of the testes, power Doppler blood flow is demonstrated. Note that the color maps depicted (green arrows) do not have a scale since a quantitative measurement of velocity is not displayed with standard power Doppler
The integrated amplitude (power) of the Doppler signal is signified by the brightness of the color. Because the positive and negative frequency shifts are not assigned a unique corresponding color on the color map in standard power Doppler the direction and velocity of flow are not indicated. Power Doppler may be useful in the interrogation of tissues where there is relatively low blood flow (e.g. prostate, testes and ovaries).
Color Doppler with spectral display
Color Doppler with spectral display is a mode which allows the simultaneous display of a color Doppler image mapped onto the gray scale image and a representation of flow as a wave form within a discrete area of interrogation. This mode is commonly used to evaluate the pattern and velocity of blood flow in the kidney and testis (Fig. 1.25).

In this example, (inset indicated by arrow) the radial artery is shown in real-time gray scale ultrasound with color Doppler overlay. The interrogation box or gate (A) is positioned over the vessel of interest. The gate should be positioned and sized to cover about 75 % of the lumen of the vessel. The angle of insonation is indicated by marking the orientation of the vessel with a cursor (B). The velocity of the flow within the vessel is depicted quantitatively in the spectral display (C)
The spectral waveform provides information about peripheral vascular resistance in the tissues. The most commonly used index of these velocities is the resistive index (Fig. 1.26).

The resistive index (RI) is the peak systolic velocity (A) minus the end-diastolic velocity (B) over the peak systolic velocity (A)
The resistive index may be helpful in characterizing a number of clinical conditions including renal artery stenosis and ureteral obstruction. Since the velocity is represented on a scaler axis, it is necessary to set appropriate scaler limits and adjust the pulse repetition frequency to prevent artifacts. Therefore, it is necessary to know the expected velocity within vessels pertinent to urologic practice (Table 1.2). The clinical use of resistive index is described in subsequent chapters.
Harmonic Scanning
Harmonic scanning makes use of aberrations related to the non-linear propagation of sound waves within tissue. These asymmetrically propagated waves generate fewer harmonics but those which are generated have greater amplitudes (Fig. 1.27).

Non-linear propagation of sound waves in tissue results in fewer but more energetic harmonics which may be selectively evaluated in the returning echo
Since these harmonics are less subject to scattering associated with the incident wave there is less noise associated with the signal. By selectively displaying the harmonic frequencies which are produced within the body and reflected to the transducer, it is possible to produce an image with less artifact. Harmonic imaging is often a useful tool in improving the image quality in obese patients.
Spatial compounding
Spatial compounding is a scanning mode whereby the direction of insonation is sequentially altered electronically to produce a composite image. This technique reduces the amount of artifact and noise producing a scan of enhanced clarity [8] (Fig. 1.28).

Conventional scanning (A) constructs an image from echoes transmitted and received from a single angle. Spatial compounding (B) results in a composite image by combining data from multiple scanning angles produced by automated beam steering. The resulting image is more detailed with less artifact
Artifacts Associated with Doppler Ultrasound
Twinkle artifact
The twinkle artifact is produced when a sound wave encounters an interface which reflects and scatters the sound wave. Recent studies have shown that twinkle artifact is more likely to be produced by a reflective object with an irregular surface [9]. In the power and color Doppler mode this pattern of reflection gives the appearance of motion distal to that interface. The resulting Doppler signal appears as a trailing acoustic pattern of varying intensity and direction known as twinkle artifact. Although this artifact may be seen in a variety of clinical circumstances it is most often helpful clinically in evaluating hyperechoic objects in the kidney. Stones often demonstrate a twinkle artifact whereas arcuate vessels and other hyperechoic structures in the kidney usually do not. Calcifications of the renal artery and calcifications within tumors and cysts may also produce the twinkle artifact, though less consistently than stones [10]. Corpora amylacea in the prostate on transrectal ultrasound may produce the twinkle artifact (Fig. 1.29).

Twinkle artifact. The effect produced by the interaction of sound waves at an interface with high impedance differences which produces an artifact suggesting turbulent motion (arrow). In this transverse transrectal ultrasound image of the prostate the twinkle artifact is produced by corpora amylacea (thin arrows)
Aliasing
Aliasing is an artifact which occurs when the ultrasound interrogation (determined by pulse repetition frequency) of an event occurs at a frequency which is insufficient to accurately represent the event. When interrogation occurs at infrequent intervals, only portions of the actual event are depicted. Aliasing occurs when the interrogation frequency is less than twice the shifted Doppler frequency (Fig. 1.30).

Aliasing. In this illustration where a sine wave is the real-time event and the vertical arrows represent the frequency of interrogation we see that frequent interrogation produces an accurate representation of the event (a). An accurate depiction of an ultrasound event must meet the condition: fs ≥ 2b, where fs is the sampling frequency and 2b is the highest frequency in the event. This is known as the Nyquist limit. (b) When the interrogation frequency is inadequate, the penetration of the event is inaccurate (Diagram adapted from Diagnostic Ultrasound, 3rd ed., Fig. 1–40, p. 33)
Normal laminar unidirectional blood flow is depicted as a single color on color Doppler. In this circumstance, spectral Doppler shows a complete waveform (Fig. 1.31). During color Doppler scanning, aliasing is most commonly seen as apparent turbulence and change in direction of blood flow within a vessel. During spectral Doppler scanning the aliasing phenomenon is seen as truncation of the systolic velocity peak with projection of the peak below the baseline (Fig. 1.32).

Spectral Doppler. (a) Blood flow appears unidirectional on color mapping in this color Doppler image with spectral flow analysis. (b) The waveform is accurately depicted on spectral analysis

In this color Doppler ultrasound with spectral flow, aliasing is demonstrated by apparent changes in velocity and direction on the color map assigned to the vessel in panel (a) indicated by arrow. Aliasing of the spectral waveform is seen as truncation of the peak systolic velocity in panel (b) as indicated by arrow with projection of the peak below the baseline in panel (c) as indicated by arrow
This artifact can be overcome by decreasing the frequency of the incident sound wave, increasing the angle of insonation (θ) or increasing the pulse repetition frequency (PRF).
References
Mason WP. Piezoelectricity, its history and applications. J Acoust Soc Am. 1981;70(6):1561–6.
Rumack CM, Wilson SR, Charboneau JW. Diagnostic ultrasound. 3rd ed. St. Louis: William. Mosby, Inc; 2005. p. 8.
Rumack CM, Wilson SR, Charboneau JW. Diagnostic ultrasound. 3rd ed. St. Louis: William. Mosby, Inc; 2005. p. 10.
Rubin JM, Bude RO, Carson PL, et al. Power Doppler US: a potentially useful alternative to mean frequency-based color Doppler US. Radiology. 1994;190:853–6.
Rifkin MD, Cochlin DL. Imaging of the scrotum & penis. Martin Dunitz Ltd; London, 2002. p. 276.
Zucchelli PC. Hypertension and atherosclerotic renal artery stenosis: diagnostic approach. J Am Soc Nephrol. 2002;13:S184–6.
Bluth EI, Benson CB, Ralls PW. Ultrasonography in vascular diseases: a practical approach to clinical problems. Thieme Medical Publishers; New York, 2008. p. 87.
Merritt CR. Technology update. Radiol Clin North Am. 2001;39:385–97.
Sharma G, Sharma A. Clinical implications and applications of the twinkling sign in ureteral calculus: a preliminary study. J Urol. 2013;189:2132–5.
Kim HC, Yang DM, Wook J, Jung Kyu R, Hyeong Cheol S. Color Doppler twinkling artifacts in various conditions during abdominal and pelvic sonography. J Ultrasound Med. 2010;29:621–32.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2015 Springer International Publishing Switzerland
About this chapter
Cite this chapter
Fulgham, P.F. (2015). The Physics and Technique of Ultrasound. In: Chan, L., Tse, V., The, S., Stewart, P. (eds) Pelvic Floor Ultrasound. Springer, Cham. https://doi.org/10.1007/978-3-319-04310-4_1
Download citation
DOI: https://doi.org/10.1007/978-3-319-04310-4_1
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-04309-8
Online ISBN: 978-3-319-04310-4
eBook Packages: MedicineMedicine (R0)