
Abstract
Peritoneal washing is usually performed to rule out neoplasia or malignancy. Often benign findings such as endometriosis and endosalpingiosis pose a diagnostic challenge to differentiate from a low-grade malignancy. This chapter describes the nonneoplastic lesions seen in peritoneal washings and ovary, along with the differential diagnosis.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
Peritoneal Washings
-
Benign findings and immunohistochemical study [1, 2].
-
Mesothelial cells are arranged in flat sheets (Fig. 4.1) with some space (“windows”) between each cell. They have round or oval nuclei and a moderate amount of cytoplasm. Immunochemistry study shows positive mesothelial markers such as calretinin (+), WT1(+), and cytokeratin 5/6 (+).
-
Collagen balls are spheres of collages surrounded by flattened mesothelial cells (Fig. 4.2), which are seen in up to 50% peritoneal washing. They have no known significance.
-
Histocytes usually are present as aggregates or as isolated cells. They have granular or vacuolated cytoplasm, oval or folded nuclei, and show immunoactivity for CD68 and CD163.
-
Skeletal and adipose tissue can occasionally be found in peritoneal washings. Detached ciliary tufts (Fig. 4.3), presumed from endosalpingiosis, can also be seen.
-
-
Benign/reactive findings and their mimickers [3, 4].
-
Endometriosis is a potential diagnostic pitfall and is rarely diagnosed solely by peritoneal washing. All essential diagnostic elements should be present for definitive diagnosis, including hemosiderin-laden macrophages (Fig. 4.4) or hemolyzed blood, endometrial epithelial cells, and endometrial stromal cells [5]. Additionally, the presence of glandular cells (endometrial cells) within the peritoneal washing may raise a differential diagnosis of malignancy, especially adenocarcinoma, which also stains positive for epithelial markers (Ber-Ep4 and Moc-31). In such cases, a cautious approach is advisable to avoid overinterpretation.
-
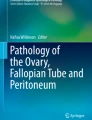
Endosalpingiosis (Fig. 4.5) is present as benign ciliated epithelial cells with small nuclei and vacuolated cytoplasm in peritoneal washing. Association with psammoma bodies is common (Fig. 4.6). The differential diagnosis includes endometriosis and malignancy (Table 4.1).
-
Peritoneal washing usually shows flat sheets of mesothelial cells, but frequently reactive mesothelial proliferations and hyperplasia can be seen, which can be diagnostically challenging. Reactive mesothelial proliferation can morphologically present as clusters, including papillary groups with prominent nucleoli, and may show some atypia, multinucleation, cytoplasmic vacuoles, and occasionally psammoma bodies. Psammoma bodies are concentric lamination of calcification. The presence of psammoma bodies is not a sign of malignancy [6, 7]. However, it includes a list of differential diagnoses such as serous carcinoma, borderline serous tumors, serous cystadenoma, serous adenofibroma, benign mesothelial proliferation, endometriosis, and other Mullerian inclusion cysts.
-
-
Artifacts
-
Mucoid-like material produced in surgical suction liner bags, made from thick opaque material, can mimic mucin. Diagnostically, it will pose more challenges if there is a prior history of the mucinous tumor.
-
Adhesion artifacts bring fibrin and histocytes in peritoneal washings.
-

Flat sheets of mesothelial cells are present (ThinPrep × 100)

Collagen ball (ThinPrep × 400)

Scattered detached ciliary tufts can be seen (ThinPrep × 600)

Hemosiderin-laden histiocytes, few inflammatory cells and mesothelial cells are present (ThinPrep × 200)

Endosalpingiosis: bland columnar epithelial cells seen (ThinPrep × 400)

Psammoma body with surrounding bland epithelial cells (ThinPrep × 400)
Ovary
-
-
Ultrasound-guided fine needle aspiration (FNA) of cystic ovarian lesions occasionally is performed. This procedure is usually used to evaluate small, incidental cystic masses that appear benign on ultrasound or laparoscopic examination, tubo-ovarian abscesses, or rarely to confirm malignancy.
-
Ovarian cystic lesion FNA has variable sensitivity and false-negative rates, especially for borderline tumors [10].
-
-
Non-neoplastic cysts [8,9,10].
Follicle cyst, corpus luteum cyst, endometrioma, and paratubal cyst are non-neoplastic cystic lesions and cytomorphology features, and differential diagnosis are summarized in Table 4.2.
References
Zuna RE. Diagnostic cytopathology of peritoneal washings. Cytojournal. 2022;19:9.
Schulte JJ, Lastra RR. Abdominopelvic washings in gynecologic pathology: A comprehensive review. Diagn Cytopathol. 2016;44:1039–57.
Selvaggi SM. Diagnostic pitfalls of peritoneal washing cytology and the role of cell blocks in their diagnosis. Diagn Cytopathol. 2003;28:335–41.
Yu GH, Song SJ. Cytology of benign peritoneal fluids and pelvic washing specimens: diagnostic cytomorphologic features and pitfalls. Acta Cytol. 2023;10:1–9.
Cantley RL, Yoxtheimer L, Molnar S. The role of peritoneal washings in the diagnosis of endometriosis. Diagn Cytopathol. 2018;46:447–51.
Sun T, Pitman MB, Torous VF. Determining the significance of psammoma bodies in pelvic washings: a 10-year retrospective review. Cancer Cytopathol. 2021;129:83–9.
Parwani AV, Chan TY, Ali SZ. Significance of psammoma bodies in serous cavity fluid: a cytopathologic analysis. Cancer. 2004;102:87–91.
Zhou AG, Levinson KL, Rosenthal DL, VandenBussche CJ. Performance of ovarian cyst fluid fine-needle aspiration cytology. Cancer Cytopathol. 2018;126:112–21.
Gupta N, Rajwanshi A, Dhaliwal LK, Khandelwal N, Dey P, Srinivasan R, Nijhawan R. Fine needle aspiration cytology in ovarian lesions: an institutional experience of 584 cases. Cytopathology. 2012;23:300–7.
Papathanasiou K, Giannoulis C, Dovas D, Tolikas A, Tantanasis T, Tzafettas JM. Fine needle aspiration cytology of the ovary: is it reliable? Clin Exp Obstet Gynecol. 2004;31:191–3.
Acknowledgments
None.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Ethics declarations
None.
Rights and permissions
Copyright information
© 2023 The Author(s), under exclusive license to Springer Nature Switzerland AG
About this chapter

Cite this chapter
Sun, T., Gilani, S.M. (2023). Peritoneal Washings and Ovary. In: Gilani, S.M., Cai, G. (eds) Non-Neoplastic Cytology. Springer, Cham. https://doi.org/10.1007/978-3-031-44289-6_4
Download citation
DOI: https://doi.org/10.1007/978-3-031-44289-6_4
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-031-44288-9
Online ISBN: 978-3-031-44289-6
eBook Packages: MedicineMedicine (R0)