
Abstract
Pathology of the ovary is complex topic as a wide variety of infrequently encountered inflammatory lesions, other nonneoplastic lesions, and tumors exist. Furthermore, numerous entities exist within each of the major categories of tumors: the surface epithelial tumors, sex cord–stromal tumors, germ cell tumors, and the miscellaneous and secondary tumors. The key histologic features and differential diagnostic considerations of ovarian and peritoneal lesions are discussed.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
Part A ____________________________________The Ovary
Inflammatory Lesions
Pelvic Inflammatory Disease
Clinical
-
♦
Pelvic in flammatory disease is related to bacterial infecti on, most commonly with gonococcus or Chlamydia, and presen ts with abdominal/pelvic pain, fever, vaginal discharge, or urinary tract symptoms
-
♦
The number of sexual partners is the greatest risk factor
-
♦
The infection may begin as salpingitis and progress to a tuboovarian abscess, which may be a palpable adnexal mass
-
♦
Orga nisms are mixed and commonly include anaerobes
Macroscopic
-
♦
The disease c ommonly begins as pyosalpinx and perioophoritis and may later become an abscess involving the parenchyma of the ovary with a fibrous wall
-
♦
Chronic infection may cause xanthogranulomatous oophoritis, which may m imic a neoplasm. Bacteroides may be involved in some cases of xanthogranulomatous oophoritis
Microscopic
-
♦
Peri-oophorit is is seen as neutrophils and fibrin on the surface of the ovary. A tuboovarian abscess may have a fibrous wall, central necrotic debris and neutrophils, and sometimes granulation tissue or lipid-containing macrophages
Actinomyces Infection
Clinical
-
♦
Pelvic ac tinomycosis is usually related to chronic intrauterine device (IUD) use
Macroscopic
-
♦
Grossly, actinomycos is is seen as a mass-like lesion with multiple abscesses with a necrotic center. Yellow granules composed of the organisms (“sulfur granules”) may be seen
Microscopic
-
♦
The lesion is c omposed of zones of necrotic debris and acute inflammat ory cells with chronic inflammatory cells lining the abscess. Clusters of filamentous bacteria with a basophilic core corre sponding to the sulfur granules are seen. The organisms are Gram positive and may stain positively with modified acid-fast stains
Tuberculous Oophoritis
Clinical
-
♦
Tuberculous oophoritis is rare and less co mmon than tuberculous salpingitis, with which it is usually associated. It may clinically mimic ovarian carcinoma in the enlargement of the ovary and an elevated serum CA-125 level
Macroscopic
-
♦
Caseating granulomas are seen
Microscopic
-
♦
Histologi cally, granulomas with central necrosis are seen. The or ganisms may be identified with acid-fast stains
Differential Diagnosis
-
♦
Other causes of granulomatous inflammation (see granulomatous oophoritis below) should be considered
Malakoplakia
Clinical
-
♦
Malakoplakia of the ovary occurs in postmenopausal women and is rare. It is much less common than malakoplakia of the urinary tract. It is thought to represent a granulomatous process related to the reduced the ability of histiocytes to kill bacteria after phagocytosis
Macroscopic
-
♦
It is seen gr ossly as a yellow, focally necrotic mass
Microscopic
-
♦
Microscopically, the lesion is composed of histiocytes with eosinophilic granular cytoplasm (von Hansemann histiocytes), some of which may have 5–8 μm cytoplasmic inclusions that are spherical, concentrically laminated, basophilic, and calcified (Michaelis–Gutmann bodies). Staining for calcium (von Kossa stain) may help demonstrate the Michaelis–Gutmann bodies. E. coli or other bacteria are only occasionally identified by culture
Differential Diagnosis
-
♦
Other causes of g ranulomatous inflammation and possibly neoplasms with clear-to-eosinophilic cytoplasm should be excluded
Fungal Infections
-
♦
Fungal infections are very rare but may occur in association with a pulmonary or disseminated infection. Infecti ons with Blastomyces, Coccidioides, and Aspergillus have been described
Viral Infections
-
♦
Viral infections are in frequently identified, but cytomegalovirus infections may be seen with eosinophilic intranuclear and cytoplasmic inclusions. Cytomegalovirus oophoritis may occur in immunosuppressed patients
-
♦
Mumps oophoritis is less common than mumps orchitis but may result in premature menopause
Granulomatous Oophoritis
Clinical
-
♦
Granulomatous oophoritis may be iatrogenic (suture material, starch granules, talc, or hysterosalpingographic contrast) or due to keratin (ruptured mature cystic teratoma or squamous cell carcinoma), sarcoidosis, Crohn’s disease, or infection (mycobacterial or fungal)
Macroscopic
-
♦
The granul omas are usually small and bilateral
Microscopic
-
♦
Noncasea ting granulomas, with or without giant cells, are seen
Differential Diagnosis
-
♦
Acid-fast ba cterial and fungal staining should be performed to attempt to identify the organisms. Polarization microscopy ma y identify starch or talc granules
Nonneoplastic Lesions
Congenital Abnormalities
-
♦
Absence of one or both ovaries may be associated with gonadal dysgenesis, ataxia-telangiectasia, or ab normalities of the ipsilateral fallopian tube, kidney, and/or ureter
-
♦
Supernumerary or ectopic ovaries are very rare but may be present in the pelvis as an attachment to the bladder, the omentum, or the retroperitoneum
-
♦
Splenic–gonadal fusion is also very rare and results from fusion during embryologic development. A cord-like structure may connect the spleen to the left ovary or the splenic tissue may be seen on the surface of the ovary. This should be distinguished from splenosis
-
♦
Adrenal cortical rests may be seen in the ovary, but less commonly than in the fallopian tube or broa d ligament
Surface Epithelial Inclusions and Cysts
-
♦
Surface epithelial inclusions and cysts are thought to result from the invaginations of the ovarian surface epithelium (Fig. 32.1). When >1 cm, they may be considered a serous cystadenoma. Wh en outside the ovary, similar inclusions are called endosalpingiosis. Ovarian epithelial inclusions and endosalpingiosis may include psammoma bodies. Neither the presence of psammoma bodies or endosalpingiosis within the subcapsular sinus of lymph nodes indicates malignancy
Fig. 32.1. 
Ovarian serous surface inclusion lined by a flattened serous epithelium. Serous surface inclusions lack associated granulosa cells or luteinized stromal cells.

Follicular Cyst
Clinical
-
♦
Follicular cysts develop from preovulatory follicles and can be associated with pain, vomiting, diarrhea, constipation, and dysfunctional uterine bleeding. Most will regress within 2 months
-
♦
Occasionally, ovarian torsion may occur
Macroscopic
-
♦
By definiti on, these cysts are greater than 3 cm in diameter, but they may reach 10 cm or more. They have a smooth lining
Microscopic
-
♦
Follicle cysts are lined by granulosa cells, but the lining may be inapparent or absent in some areas. The surrounding theca cells may be luteinized
Corpus Luteum Cyst
Clinical
-
♦
Corpus luteum cysts develo p from postovulatory follicles (corpora lutea) during menstruation or pregnancy. They are usually asymptomatic
-
♦
Similar to follicular c ysts and spontaneous regression, it is typical
Macroscopic
-
♦
These cysts are usually 2–3 cm in diameter and have a central hemorrhage surrounded by a lining of fibrous connective tiss ue that in turn is surrounded by a convoluted yellow layer of tissue
Microscopic
-
♦
The yellow layer is c omposed of luteinized granulosa cells with abundant eosinophilic cytoplasm
Large Solitary Luteinized Follicle Cyst of Pregnancy and Puerperium
-
♦
This is a variant of follicular cyst that may present as a palpable adnexal mass or may be seen during a cesarean section. It may be up to 25 cm in diameter, and the wall is compose d of luteinized granulosa and theca cells (Fig. 32.2). Prominent nuclear atypia may be seen, but mitotic figures are absent and behavior is benign
Fig. 32.2. 
Large solitary luteinized follicle cyst of pregnancy and puerperium. The cyst is lined by granulosa cells and luteinized stromal cells are present in the fibrous tissue of the cyst wall.

Hyperreactio Luteinalis (Multiple Luteinized Follicular Cysts)
Clinical
-
♦
Hyperreactio luteinalis is a bilateral ovarian enlargement due to multiple luteinized follicular cysts resulting from hCG stimulation. The hCG elevation may result from a molar gestation, a multiple gestation, or a hydropic fetus. Hyperreactio luteinalis occurs in up to 25% of cases of gestational trophoblastic disease
-
♦
This lesion regresses following the removal of the hCG stimulus
Macroscopic
-
♦
The ovaries are enlarged (up to 15 cm) and are composed of multiple smooth-walled cysts
Microscopic
-
♦
Microscopically, the cysts are lined by granulosa cells surrounded by theca cells, both of which may be luteinized
Differential Diagnosis
-
♦
The ovaries may grossly resemble the ovaries of polycystic ovary syndrome, but the clinical situation differs (while hyperreactio luteinalis is usually associated with an abnormal gestation, polycystic ovary syndrome is commonly associated with infertility). Also, the ovaries lack the thick fibrous capsule and smooth surface of polycystic ovary syndrome
Luteoma of Pregnancy (Pregnancy Luteoma)
Clinical
-
♦
These no dular hyperplastic masses are found most commonly incidentally during cesarean section or postpartum tubal ligation
-
♦
About one-quarter of patients will have virilization or hirsutism
-
♦
Incompletely resected tumors regress following the pregnancy
Macroscopic
-
♦
Grossly, they are composed of red-brown soft tissue, and they may be multiple or bilateral. They are commonly 6–12 cm in diameter. Necrosis may be seen postpartum
Microscopic
-
♦
Microscopically, they are composed of polygonal luteinized cells in nodules or of a diffuse pattern with abundant eosinophilic cytoplasm and round nuclei (Fig. 32.3). Small cysts may be present
Fig. 32.3. 
Luteoma of pregnancy. The tumor was an incidental finding during a cesarean section and was composed of polygonal luteinized cells with abundant eosinophilic cytoplasm.

Differential Diagnosis
-
♦
Some sex cord–stromal tu mors may resemble luteoma of pregnancy, but it is unusual for those to be bilateral, in contrast to the commonly bilateral luteoma of pregnancy. The tumors that may appear histologically similar include Leydig cell tum or, thecoma, sclerosing stromal tumor, and juvenile granulosa cell tumors
Polycystic Ovary Syndrome (Stein–Leventhal Syndrome)
Clinical
-
♦
Polycystic ovary syndrome is a rel atively common (5–10% of the female population) disorder characterized by chronic anovulation, multicystic ovaries with a fibrotic cortex, and hyperandrogenism. Clinical findings include dysfunctional uterine bleeding, infertility, obesity, and hirsutism
-
♦
Many patients will have androgen excess, with an elevation of serum testosterone, dehydroepiandrosterone, or other androgens
-
♦
Some patients may also have abnormal glucose tolerance, insulin resistance, and acanthosis nigricans (“HAIR-AN syndrome”: hyperandrogenism, insulin resistance, and acanthosis nigricans)
Macroscopic
-
♦
The ovaries are grossly enlarged (approximately twice the normal size) with a smooth outer surface, a thick fibrous cortex, and multiple small (<1 cm) cysts just under the fibrotic cortex
Microscopic
-
♦
A thickened fibro us capsule at the surface of the ovary is seen with multiple follicle cysts underneath. The cysts are lined by a thinned granulosa cell layer with surrounding theca cells. Evidence of ovulation (such as corpora albi cantia or corpora lutea) is not seen
Differential Diagnosis
-
♦
See hyper reactio luteinalis abo ve
Stromal Hyperthecosis/Stromal Hyperplasia
Clinical
-
♦
These disorders occ ur in perimenopausal or postmenopausal women and may be associated with virilization, increased serum testosterone, hypertension, or decreased glucose tolerance and are seen as bilateral ovarian enlargement
Macroscopic
-
♦
Grossly, the ovaries are enlarged (up to twice normal size), firm, and white, tan, or yellow in color. In some cases, stromal hyperthecosis may be grossly nodular
Microscopic
-
♦
Microscopic ally, the ovaries have a hyperplastic stroma with luteinized stromal cells (stromal hyperthecosis) or densely arranged nonluteinized stromal cells (stromal hyperplasia)
Leydig Cell Hyperplasia (Hilus Cell Hyperplasia)
Clinical
-
♦
Small nests of Leydig cells can be found in t he ovarian hilus where they are known as hilus cells and they occasionally may be found elsewhere in the ovary or in the fallopian tube. Proliferation of hilus cells is observed in pregnancy, after menopause, and in several pathologic conditions including stromal hyperplasia and rete cysts. Leydig cell hyperplasia is usually not clinically significant, but can be associated with increased serum testosterone
Macroscopic
-
♦
Leydig cell hyperplasia is not grossly apparent
Microscopic
-
♦
Leydig cell hyperplasia is seen as nodules of polygonal Leydig cells with abundant eosinophilic granular cytoplasm and round nuclei. Reinke cry stals (eosinophilic rod-shaped cytoplasmic crystalloids) and cytoplasmic yellow-brown lipofuscin pigment may be seen
Differential Diagnosis
-
♦
Masses greater tha n 1 cm com posed of Leydig cells may be considered Leydig cell tumors
Rete Cyst
Clinical
-
♦
Cysts of th e rete ovarii may occur in the ovarian hilus
Macroscopic
-
♦
They are usually unilocular and small, but occasionally, cysts up to 12 cm can occur
Microscopic
-
♦
Microscopically, they are lined by flattened or cuboidal cells. Smooth muscle and nests of hyperpl astic Leydig cells may be seen adjacent to the cyst
Massive Ovarian Edema
Clinical
-
♦
Massive ov arian edema may clinically mimic a neoplasm and often presents with abdominal pain. Patients are young (usually in the second or third decade)
-
♦
The frequent association with torsion suggests that development of massive ovarian edema may be related to int ermittent or partial ovarian torsion that impairs lymphatic and venous drainage from the ovary
Macroscopic
-
♦
The ovary is grossl y greatly enlarged (over 10 cm and occasionally up to 35 cm) and white in color. The cut surface shows edematous-appearing fibrous tissue
Microscopic
-
♦
Microscopically, th e ovary is composed of cytologically bland stromal cells widely separated by edema fluid (Fig. 32.4)
Fig. 32.4. 
Massive ovarian edema. This massively enlarged ovary was grossly white in color with a fibrous and edematous cut surface. Microscopically, cytologically bland, widely spaced spindle cells were seen with occasional collagen fibers.

Differential Diagnosis
-
♦
Grossly, metastati c carcinomas with mucin production or edematous tumors (such as some lymphomas) may resemble massive ovarian edema. Sclerosing stromal tumors may have edematous areas that microscopically resemble massive ovarian edema
Ovarian Torsion
Clinical
-
♦
Ovarian torsion is freque ntly associated with a mass lesion, usually a benign cyst or tumor, but torsion of an otherwise normal ovary may also occur. It occurs most commonly in women of reproductive age, but about one-fourth of cases occur in children. Ovarian torsion in children is associated with a malignant tumor in less than 2% of patients. Patients present with abdo minal pain that may mimic appendicitis
Macroscopic
-
♦
The ovary is grossly swollen (up to 6 cm), hemorrhagic, and, sometimes, infarcted
Microscopic
-
♦
Hemorrhage, edema, and ischemic necrosis are seen. A search should be made for a possible associated neoplasm, but identification of one, even if present, may be difficult due to infarction
Ectopic Decidual Reaction
-
♦
Decidual reac tion may be seen in the ovarian stroma as a result of pregnancy or progestin treatment or adjacent to a corpus luteum. The stromal cells are in the form of small nodules or large sheets and have the typical abundant eosinophilic cytoplasm of endometrial decidual cells. Focally, nuclear atypia or cytoplasmic vacuolization (a potential mimic of signet-ring adenocarcinoma, but PAS negative) may be seen
Endometriosis
Clinical
-
♦
Endometriosis is defined as the presence of benign endometrial glands and stroma, often with evidence of hemorrhage outside the uterus. While the etiology of the condition is incompletely understood, most cases probably result from retrograde menstruation through the fallopian tube with implantation of endometrial tissue on the ovary or peritoneum. Other possibilities include metaplasia of the pelvic peritoneum or, rarely, lymphovascular dissemination of benign endometrial tissue
-
♦
Endometriosis affects 4–10% of women of reproductive age, and it is associated with dysmenorrhea and chronic pelvic pain. Up to 30% of women with endometriosis are infertile. Endometriosis is associated with a three- to eightfold increased incidence of ovarian carcinomas and borderline tumors
-
♦
Low parity and cervical stenosis are risk factors
-
♦
Serum CA-125 may be elevated in women with endometriosis. The ovary and any pelvic or abdominal serosal surface may be involved. Surgical scars (cesarean section scars, episiotomy sites, or scars from other abdomi nal surgeries) may be involved
-
♦
Rarely, carcinomas may arise within endometriosis in the colon or elsewhere
Macroscopic
-
♦
Grossly, small le sions may be seen as patches of blue, red, or brown on a serosal surface. Microscopically, endometrial glands, stroma, and hemosiderin-containing macrophages are seen
-
♦
The ovary is the most common location for endometriotic cysts. These cysts may present as a large mass lesion and may largely replace the normal ovarian tissue. The cysts contain brown degenerated blood (“chocolate cysts”)
-
♦
Other locations for endometriosis include the fallopian tube, uterine serosa, uterine cervix, colon, and the peritoneu m (especially in the cul-de-sac). Very rarely, the lung or pleura may be involved
Microscopic
-
♦
Noncystic lesions of endometriosis are seen as endometrioid glands, which commonly are inactive appearing but may hav e a proliferative or secretory appearance. The stroma may be densely cellular (resembling proliferative endometrial stroma) or edematous (resembling secretory phase stroma) or may show decidual change. Macrophages are commonly seen, but hemosiderin pigment may or may not be visible
-
♦
Endometriotic cysts are lined by endometrial epithelium with underlying endometrial stroma, hemorrhage, and pigmented (hemosiderin-containing) macrophages
-
♦
Decidual reaction, Arias-Stella reaction, hyperplasia, and cytologic atypia may be seen in endometriosis. Malignant tumors also may arise within endometriosis. Clear cell adenocarcinomas are the most common endometriosis-associated carcinoma, but endometrioid adenocarcinomas may also be seen
-
♦
Occasional cases of endometriosis, usually in the ovary, may have a paucity or absence of glands (“benign stromatosis”)
-
♦
Occasionally, the endometrial stroma in an endometriotic cyst may undergo smooth muscle m etaplasia (“endomyometriosis”). This phenomenon may result in the presence of a “uterus-like mass” in the ovary or elsewhere
Differential Diagnosis
-
♦
Grossly, corpus luteum cysts appear as a hemorrhagic cystic lesion in the ovary similar to endometriosis but have a surround ing rim of yellow tissue
-
♦
The epithelium of endometriosis may be focally ciliated, but uniformly ciliated glands not associated with endometrial stroma are considered endosalpingiosis (see “Endosalpingiosis” in the peritoneum section below)
-
♦
Endometriotic glands may be irregular in outline but should not have extensive confluent growth. If this is seen, e ndometrioid carcinoma must be considered
Surface Epithelial Tumors
General Information concerning Surface Epithelial Tumors
-
♦
Ovarian c arcinomas comprise approximately 30% of all gynecologic tract malignancies. Surface epithelial tu mors (also known as surface epithelial-stromal tumors) are the most common type, comprising 90% of ovarian malignancies
-
♦
Risk factors for ovarian surface epithelial malignancies include postmenopausal estrogen replacement therapy and obesity. A history of oral contraceptive use and high parity (both associated with reduced ovulation) are associated with a decreased risk
-
♦
The mean 5-year survival for ovarian malignancies is only 32% as most patients present with advanced stage (outside the pelvis) disease and overall survival has not improved significantly in recent decades
-
♦
The most common genetic abnormality in familial cases of ovarian carcinoma is BRCA1 mutation. BRCA2 and hereditary non-polyposis colorectal carcinoma syndrome (Lynch syndrome) gene abnormalities (MLH1 and MSH2) are less important
-
♦
Immunophenotyping is useful in the differential diagnosis (Table 32.1)
Table 32.1. Immunohistochemical Findings in Ovarian Tumors -
♦
Epithelial ovarian carcinomas have been divided into two broad categories, type I and type II tumors, based on clinic al, histopathologic, and molecular features
-
♦
The type I tumors include low-grade serous carcinoma, low-grade endometrioid carcinoma, mucinous carcinoma, and clear cell carcinoma, develop from precursors such as borderline tumors and endometriosis, are commonly confined to one ovary at presentation, are relatively indolent, and typically have mutations in genes such as KRAS, BRAF, PTEN, and ARID1A
-
♦
The type II tumors include high-grade serous carcinoma, high-grade endometrioid carcinoma, and malignant mixe d Müllerian tumor, develop from serous tubal intraepithelial neoplasia of the fallopian tube or from ovarian epithelium-lined inclusion cysts, typically present at advanced stage, are aggressive, have TP53 mutations in over 95% of cases, and are chromosomally unstable
-
♦
Recently, it has been suggested that the two-type classification is excessively simplistic and, based on differences in behavior, treatment response, and molecular pathology, that reduction to less than five categories (hig h-grade serous carcinoma, low-grade serous carcinoma, mucinous carcinoma, endometrioid carcinoma, and clear cell carcinoma) is inappropriate
High-Grade Serous Carcinoma
Clinical
-
♦
These tumors are aggressive and typically present at advanced stage and with ascites, with only ap proximately 1% of high-grade serous carcinomas confined to the ovary at diagnosis. Screening has not significantly changed this percentage
-
♦
Incidence of this tumor is declining, probably due to the protective effect of oral contraceptives
-
♦
Chemotherapy is effective in treating metastatic disease, with a response rate of about 80%, but the tumor consistently develops resistance to treatment and recurrence
Macroscopic
-
♦
Serous carcin oma is bilateral in two-thirds of cases
-
♦
Tumors vary from microscopic to over 20 cm. The cut surfaces of the tumor are commonly white to tan, and grossly apparent papillary structures, cysts, necrosis, and hemorrhage may be seen
Microscopic
-
♦
Neoplastic serous epithelium ranges from cytologically bland columnar epithelium resembling fallopian tube epithelium to solid nests of epithelium with markedly pleomorphic, enlarged, and hyperchromatic nuclei and scant cytoplasm
-
♦
Serous carcinoma was formerly known as “papillary serous carcinoma” and does commonly have papillary architecture, but tumors also may have entirely solid or glandular/cribriform pattern. “Transitional cell carcinoma of the ovary” has been described, but based on immunophenotype, molecular features, and coexistence with more typical high-grade serous carcinoma (or occasionally endometrioid carcinoma), this appears to be a pattern of high-grade serous carcinoma rather than a distinct tumor type
-
♦
Psammoma bodies are seen in about one-third of high-grade serous carcinomas, but they are also seen in low-grade serous carcinoma, serous tumors of low malignant potential, occasional nonovarian neoplasms, and benign mesothelial hyperplasia
-
♦
Serous carcinoma is usually positive for keratin 7, EMA, and CA125 and is negative for keratin 20 and cal retinin
-
♦
Mutations of TP53 are critical to the development of high-grade serous carcinoma and are seen in over 95% of these tumors. Two patterns of p53 immunohistochemical staining are seen in these tumors with this nuclear marker: strong diffuse staining (indicating a missense mutation) or complete absence of staining (in dicating a nonsense mutation with a truncated protein). The type I carcinomas, in contrast, typically have wild-type TP53 with patchy staining
-
♦
In the past, a three-grade system had been used for serous carcinoma. More recently, a two-grade system has been recommended. The two-grade system recognizes that low- and high-grade serous carcinomas are separate entities in terms of clinical behavior, precursor lesions, and molecular pathology. Furthermore, the prognosis does not differ between grade 2 and grade 3 tumors, using the three-grade system
-
♦
Morphologically, differentiation from low-grade serous carcinoma is made based on nuclear pleomorphism and mitotic rate. High-grade tumors have 3:1 nuclear size variation and more than 12 mitoses per 10 high power fields
-
♦
High-grade tumors (which make up approximately 90% of serous carcinomas) usually have TP53 mutations, lack KRAS mutations, and only very rarely arise from a serous tumor of low malignant potential or a low-grade serous carcinoma, while low-grade serous carcinomas (Fig. 32.6) commonly have KRA S mutations, lack TP53 mutations, and are more likely to arise from a serous tumor of low malignant potential
Molecular Pathology
-
♦
Serous carcinoma had been thought to arise from ovarian surface epithelium inclusions, but recent evidence supports the idea that many of these tumors originate from TP53-mutated precursor lesions within the fallopian tube . These lesions are referred to as serous tubal intraepithelial carcinoma (STIC). This was first suspected based on detection of intraepithelial carcinomas and small, clinically occult carcinomas in the fimbria of prophylactic salpingo-oophorectomy specimens from patients with BRCA1 and BRCA2 mutations
-
♦
Further support for fallopian tube origin of “ovarian” high-grade serous carcinoma includes gene expression studies (including TP53) that demonstrate similarity between “ovarian” high-grade serous carcinoma and STIC and the frequent identification of STIC in association with “ovarian” high-grade sero us carcinoma
Differential Diagnosis
-
♦
Endometrioid carcinoma, especially when poorly differentiated, may resemble serous carcinoma. Both may have papillary, glandular, or solid architecture or a mixture of these patterns. High-grade serous carcinoma s have higher grade nuclear atypia with occasional large, hyperchromatic nuclei, and the glands and papillary structures tend to have scalloped or irregular surfaces and slit-like lumens. Psammoma bodies are seen in about one-third of high-grade serous carcinoma cases. Endometrioid carcinoma glands tend to have round lumens with flat or continuous luminal surfaces and cells with a more columnar appearance. Squamous differentiation is seen in about one-third of endometrioid carcinoma cases, but may rarely also be seen in serous carcinoma
Low-Grade Serous Carcinoma
Clinical
-
♦
These tum ors are usually unilateral and may be confined to the ovary at diagnosis
-
♦
Low-grade serous carcinomas commonly arise in serous cystadenomatous tumors of low malignant potential (serous borderline tumors)
-
♦
Five-year survival is approximately 85% and 10-year survival is approximately 50%, but the tumor respond s poorly to platinum-based chemotherapy
Microscopic
-
♦
These tumors are co mposed of infiltrating small papillary epithelial cell groups, often surrounded by a retraction space, and the low power appearance is characteristic
-
♦
Differentiation from high-grade serous carcinoma is made based on nuclear pleomorphism and mitotic rate. Low-grade tumors lack 3:1 nuclear size variation and have less than 12 mitoses per 10 high power fields
-
♦
Psammoma bodies are typically abundant in low-grade serous carcinomas and in some cases there may be a gr eater volume of psammoma bodies than residual epithelium (the so-called psammocarcinoma, Fig. 32.5)
Fig. 32.5. 
Low-grade serous carcinoma with abundant psammoma bodies (“psammocarcinoma”). This low-grade ovarian serous carcinoma has numerous laminated calcifications (psammoma bodies) that compose almost the same area on the slide as the malignant epithelium.

Serous Borderline Tumor (Serous Tumor of Low Malignant Potential, Atypical Proliferative Serous Tumor)
Clinical
-
♦
Borderline ovaria n tumors may be serous (approximately 2/3 of cases) or mucinous (approximately 1/3 of cases)
-
♦
Patients with serous tumors of low malignant potential are on average younger than patients with serous carcinoma (approximately 45 years old vs. 60 years for serous carcinoma). The tumors may be are bilateral and 22% of cases are associated with implants
-
♦
Prognosis is far better than serous carcinoma, with 99% 5-year survival for stage I cases and 55–75% 5-year survival for stage III. Mortality is seen in tumors that progress to low-grade s erous carcinoma
Macroscopic
-
♦
These tumors are commonly cystic with grossly identifiable nodularity or papillary structures in the cyst lining
Microscopic
-
♦
Serous tumors of low malignant potential (serous borderline tumors) have papillary architecture (with fibrovascular cores) and low-grade nuclear atypia (Figs. 32.6 and 32.7). Papillary tufting and epithe lial hyperplasia of several cells in thickness are present, but stromal invasion and extensive solid or cribriform architecture are absent
Fig. 32.6. 
Low-grade serous carcinoma. The nuclei are enlarged but relatively uniform with only mild-to-moderate nuclear atypia and less than 12 mitoses per 10 high power fields.
Fig. 32.7. 
Serous cystadenomatous tumor of low malignant potential (serous borderline tumor). This cystic tumor has papillary architecture with papillae covered by serous epithelium with mild nuclear atypia, nuclear stratification, and papillary tufting. Solid, cribriform, or invasive growth is not seen.
-
♦
A micropapillary variant of serous tumor of low malignant potential (comprising 5–15% of cases) exists. This tumor has thin micropapillae, without stromal support that are at least five times as long as they are wide arising directly from the surface of papillary structures with stromal cores (“nonhierarchical branching” or “medusa-head” appearance, Fig. 32.8) in at least a continuous 5 mm area. This variant (also termed, by some, “noninvasive low-grade serous carcinoma”) is associated with an increased likelihood of advanced stage and may have worse prognosis
Fig. 32.8. 
Micropapillary architecture. This serous tumor of low malignant potential had focal micropapillary architecture with thin micropapillae, with length greater than five times their width and lacking stromal cores.
-
♦
Peritoneal surface implants may be seen in association with serous tumors of low malignant potential. Noninvasive implants may be epithelial type (not associated with fibrotic stroma) or desmoplastic type. Noninvasive implants have minimal impact on prognosis, but invasive implants have behavior similar to low-gr ade serous carcinoma and it is now recommended that they should be diagnosed as foci of low-grade serous carcinoma
-
♦
Inclusions of serous epithelium with features of a low malignant potential tumor or endosalpingiosis may be seen in pelvic lymph nodes in association with ovarian serous tumors of low malignant potential. These may represent metastatic or independently arising tumors and do not appear to affect survival (if features sufficient for a diagnosis of low-grade serous carcinoma are absent)



Differential Diagnosis
-
♦
The usual considerations in the differential diagnosis are serous carcinoma (which has an invasive, cribriform/in terconnecting glandular, or solid pattern) and serous cystadenoma/serous cystadenofibroma (which may have papillary architecture within the cyst but lacks nuclear stratification and papillary tufting)
-
♦
Serous tumor of low malignant potential with microinvasion is diagnosed when clusters of tumor cells in the stroma measuring less than 5 mm are seen. This is seen in approximately 5% of serous tumors of low malignant potential and does not appear to alter progression-free survival
-
♦
Occasional metastatic tumors, such as pancreatic adenocarcinoma, may mimic serous low malignant potential tumors
Benign Serous Tumors
Macroscopic
-
♦
These lesions ar e greater than 1 cm; smaller lesions are considered cortical inclusion cysts
-
♦
Benign serous tumors (serous cystadenoma and serous cystadenofibroma) are cystic and are bilateral in approximately 20% of cases. Nodularity/papillary structures may be apparent in the cyst wall (this does not necessarily indicate that the tumor is a low malignant potential tumor)
Microscopic
-
♦
Serous cystadenomas are lined by a flat (one cell layer) epithelium that may be ciliated
-
♦
Serous cystadenofibromas have papillary architecture with the flat epithelium covering broad, “club-like” fibrous stromal cores. Some cases may also have a glandular pattern with dense fibrous stroma surrounding the glands
-
♦
Foci of epithelial changes, similar to those seen in a serous borderline tumor but involving less than 10% of the neoplasm, are termed “serous cystadenoma with focal epithelial proliferation” and benign behavior is expected
Mucinous Carcinoma
Clinical
-
♦
Ovarian mucinous carcinomas (approximately 3% of ovarian carcinomas) have a good prognosis if stage I
-
♦
Many older case series of ovarian mucinous carcinomas have likely contained many cases of metastatic carcinoma involving the ovary, but ovarian mucinous carcinoma, if high stage, has a poor prognosis that is worse than serous carcinoma and not significantly different from metastatic mucinous carcinoma f rom other sites involving the ovary
Macroscopic
-
♦
Mucinous carcino mas are usually large unilateral cystic masses filled with mucoid material
Microscopic
-
♦
Invasive growth pattern (“destructive stromal invasion”) or sheets of closely arranged glands with minimal or no intervening stroma must be seen for the diagnosis of ovarian mucinous carcinoma. Mucinous carcinom as are commonly seen with areas of mucinous tumor of low malignant potential and/or mucinous cystadenoma
Differential Diagnosis
-
♦
The primary concern when making a diagnosis of mucinous carcinoma in an ovarian specimen is the distinction of primary from metastatic tumors. Colorectal adenocarcinoma, low-grade appendiceal mucinous carcinoma, pancreatic adenocarcinoma, gastric adenocarcinoma, and cervical adenocarcinoma may all be mistaken for a primary ovarian adenocarcinoma. Primary ovarian mucinous tumors are usually limited to one ovary at presentation. Tumors which are disseminated at presentation are only rarely ovarian. The presence of bilaterality, ovarian surface involvement, and lymphovascular invasion should all raise suspicion of a metastatic carcinoma
-
♦
The appendix should be considered as a possible primary site for mucinous neoplasms in the ovary, but, if the appendix is grossly normal at the time of oophorectomy, routine appendectomy only rarely identifies an occult tumor
-
♦
It should be remembered that keratin 20 and CDX2, usually thought of as intestinal markers, are typically positive in primary ovarian mucinous tumors. Keratin 7 is positive in ovarian mucinous tumors but is also commonly positive in rectal and pancreatic carcinomas, so expression of keratin 7 does not exclude gas trointestinal tract origin
Mucinous Borderline Tumors (Atypical Proliferative Mucinous Tumor, Formerly also Known as “Mucinous Tumor of Low Malignant Potential”)
Clinical
-
♦
These tumors a re large (commonly 15–20 cm and sometimes larger) and cystic. Prognosis is excellent with up to 100% survival in recent studies (provided associated mucinous carcinoma is excluded)
Macroscopic
-
♦
These tum ors are multicystic and are bilateral in about 5% of cases
Microscopic
-
♦
The epithelium is s tratified (2–3 cells) and shows greater nuclear atypia than in a mucinous cystadenoma; it has a “filiform” papillary architecture, and epithelial tufting is commonly seen
-
♦
Focal intraepithelial carcinoma, defined as grade 3 nuclei and traditionally not thought to have prognostic significance, has been prognostically significant one study, especially if greater than 10% of the tumor is involved
-
♦
Microinvasion is diagnosed when foci of invasion measure less than 5 mm. This has similarly been found to influence the prognosis in some studies, but not others
Differential Diagnosis
-
♦
As with mucinous carcinoma, the primary consideration is metastatic neoplasia, especially colorectal adenocarcinoma and low-grade appendiceal mucinous neoplasm. Metastatic colorectal carcinoma commonly has “dirty necrosis” with basophilic n uclear debris and a keratin 7−/keratin 20+ immunophenotype. Ovarian mucinous tumors are usually keratin 7+, but keratin 20 expression is variable
Mucinous Cystadenoma
Clinical
-
♦
Mucinous cy stadenomas are commonly large, commonly seen in young women, and may be associated with pregnancy or torsion. These tumors are only rarely bilateral
Macroscopic
-
♦
Mucinous cyst adenomas are large, usually multilocular, cystic mucin-containing tumors
Microscopic
-
♦
The epitheliu m has minimal stratification and nuclear atypia. Most mucinous cystadenomas have an endocervical-like morphology, but some cases may have an intestinal (containing goblet cells) or mixed pattern
-
♦
A mature cystic teratoma may be seen in association with the tumor in 3–5% of cases
Differential Diagnosis
-
♦
Mucino us cystadenoma may have broad papillary structures, but lacks the epithelial tufting and nuclear atypia seen in a mucinous borderline tumor
Mucinous Tumors with Mural Nodules
-
♦
Rarely, cy stic mucinous tumors may contain mural nodules composed of histologically distinct anaplastic carcinoma (Fig. 32.9) or sarcoma. The anaplastic carcinoma in such a nodule is composed of rhabdoid or spindle-shaped cells with keratin positivity. A sarcomatous nodule may be rhabdomyosarcoma or undifferentiated sarcoma. Cytologically atypical but well-circumscribed sarcoma-like nodules may also be seen
Fig. 32.9. 
Mural nodule of anaplastic carcinoma in a mucinous borderline tumor. The mural nodule was composed of anaplastic rounded tumor cells with a “rhabdoid” appearance. The anaplastic cells were positive for keratin and negative for muscle markers by immunohistochemistry.
-
♦
The presence of anaplastic carcinoma nodules does not appear to be a poor prognostic factor in stage I tumors. Mucinous borderline tumors with sarcoma-like mural nodules have had benign behavior

Pseudomyxoma Peritonei
Clinical
-
♦
Pseudomyx oma peritonei is the presence of abundant mucin in the peritoneal cavity. This lesion is associated with either an ovarian mucinous tumor or a gastrointestinal (usually appendiceal) mucinous tumor
Macroscopic
-
♦
The lesion is seen as gelatinous mucin in the peritoneal cavity
Microscopic
-
♦
Epithelial cells may or may not be present in the mucin
Differential Diagnosis
-
♦
The primary concern is identifying the site of origin, which requires gross and histologic examination of the ovaries and appendix. Histologically similar mucinous tumor may be present in both the ovaries and appendix. In this case (even if the appendiceal tumor is much smaller), it is thought that the appendiceal tumor should be considered the primary and that the ovarian tumor should be considered the secondary (although this remains controversial)
Endometrioid Tumors
Clinical
-
♦
Endometri oid carcinomas comprise approximately 10–15% of all ovarian carcinomas. Association with endometriosis is seen in approximately 40% of cases and approximately one-quarter of cases are bilateral
-
♦
Approximately 15–20% of endometrioid ovarian carcinomas are associated with a synchronous endometrial carcinoma. The prognosis in this situation is relatively good, and it is believed that the tumors are usually separate primaries, not a single primary with metastasis from the endometrium to ovary or the ovary to endometrium
-
♦
Endometriosis-associated ovarian endometrioid carcinomas have distinctive clinical features including presentation at younger age, lower stage, lower likelihood of high grade, and higher likelihood of coexisting endo metrial carcinoma. Prognosis, however, is similar
Macroscopic
-
♦
Endometrioid carcinomas are cystic masses with soft, sometimes hemorrhagic or necrotic, centers. Sometimes the tumor is a nodule in the lining of an endometriotic cyst
-
♦
Endometrioid borderline tumors and benign endometrioid adenofibromas are firm fibrous tumors with a variable amount of cystic component
Microscopic
-
♦
Endometrial c arcinomas are composed of glands resembling endometrial epithelium with varying amounts of solid architecture. Squamous differentiation is seen in about one-third of cases. Villous or villoglandular architecture is commonly seen (Fig. 32.10) and this should not be mistaken for serous carcinoma if the other features of serous carcinoma (marked nuclear pleomorphism, scalloped cell group margins, etc.) are not seen
Fig. 32.10. 
Ovarian endometrioid adenocarcinoma. This ovarian endometrioid adenocarcinoma was focally cystic with villoglandular architecture. The villous architecture should not be mistaken for papillary serous carcinoma. In endometrioid carcinoma (in contrast to serous carcinoma), the margin of the cell groups is relatively flat, the cells are columnar, nuclear pleomorphism is not pronounced, and psammoma bodies are absent.
-
♦
Most ovarian endometrioid carcinomas are low grade (grade 1 out of 3), which aids in their distinction from serous carcinoma
-
♦
Endometrioid borderline tumors (Fig. 32.11) are much less common than ovarian endometrioid adenocarcinomas and are usually with associated endometriosis. These tumors are composed of endometrioid glands with cytologic atypia that, similar to endometrial hyperplasia, lack confluent or invasive growth patterns. Some cases may be cystic and have villoglandular architecture. Squamous morules may be seen in association with the epithelium and the associated stroma may be densely fibrotic. Prognosis is excellent
Fig. 32.11. 
Ovarian endometrioid borderline tumor. This tumor shows features similar to endometrial atypical hyperplasia, including crowded but separate architecturally complex glands, nuclear stratification, and nuclear atypia.
-
♦
Benign endometrioid cystadenomas and adenofibromas are rare. They lack the cytologic atypia seen in endom etrioid borderline tumors. They are differentiated from ovarian endometriosis by their absence of endometrial-type stroma


Differential Diagnosis
-
♦
Intermediate to high grade (grade 2–3) ovarian endometrioid carcinoma may resemble serous carcinoma, but endometrioid carc inoma has less pronounced nuclear pleomorphism, has round glandular lumens, may have squamous differentiation, and may be associated with endometriosis
-
♦
Metastatic colorectal adenocarcinoma may, in some cases, appear histologically similar
-
♦
Occasional cases of endometrioid carcinoma have a tubular or solid tubular pattern (“sertoliform variant of endometrioid carcinoma”) that resembles the pattern of sex cord–stromal tumors such as Sertoli cell tumor or granulosa cell tumor. Endometrioid carcinomas resembling sex cord–stromal tumors, however, are in hibin-alpha negative, while sex cord–stromal tumors are inhibin positive
Clear Cell Tumors
Clinical
-
♦
Clear cell carcinomas compri se approximately 10–15% of ovarian carcinomas and occur at a somewhat younger average age (approximately 55 for clear cell carcinoma) compared to high-grade serous carcinomas
-
♦
50–70% of patients will have endometriosis and about 25% of clear cell carcinomas arise in an endometriotic cyst
-
♦
Ovarian clear cell carcinomas are occasionally associated with paraneoplastic hypercalcemia or thromboembolism
-
♦
When clear cell carcinoma is limited to the ovary, prognosis is better than high-grade serous carcinoma, but advanced stage clear cell carcinoma has a worse prognosis than high-grade serous carcinoma
-
♦
These tumors respond poorly to platinum-based chemotherapy, with a response rate of about 15%
Macroscopic
-
♦
These tumors are comm only large thick-walled cystic masses with nodules of tumor projecting into the cyst
Microscopic
-
♦
Clear cell car cinomas are composed of polygonal epithelial cells with large and often irregular nuclei, which may resemble the cells of Arias-Stella reaction in gestational endometrium. The architecture is described as tubulocystic, papillary, or solid architecture. “Hobnail cells” with scant cytoplasm and hyperchromatic nuclei protruding into the lumens of the tubular structures may be seen
-
♦
The cytoplasm is clear due to the presence of glycogen (Fig. 32.12), but it must be remembered that some cases, particularly on frozen section examination, may have eosinophilic cytoplasm (Fig. 32.13). PAS (without diastase) is positive
Fig. 32.12. 
Clear cell carcinoma. Ovarian clear cell carcinomas commonly have a “tubulocystic” architectural pattern and clear to pale eosinophilic cytoplasm.
Fig. 32.13. 
Frozen Section of ovarian clear cell carcinoma. On frozen section, this ovarian clear cell carcinoma (same case as in Fig. 32.12) had eosinophilic, somewhat granular-appearing cytoplasm and a solid architecture, mimicking a stromal tumor containing Leydig cells.
-
♦
Occasional cases may have prominent eosinophilic cytoplasmic globules (similar to those seen in yolk sac tumor). Some cases may be composed primarily or entirely of cells with oxyphilic cytoplasm
-
♦
Clear cell borderline tumors are very rare and composed of separate round glands lined by a clear cell epithelium w ith notable atypia in a fibrous background. Behavior is almost always benign
-
♦
Clear cell adenofibromas are also very rare and appear similar to borderline tumors but have minimal nuclear atypia


Molecular pathology
-
♦
Genetic ab normalities in ARID1A, PIK3CA, and HNF-1β genes are seen and these abnormalities may also be seen in endometriosis associated with clear cell carcinomas
Differential Diagnosis
-
♦
Yolk sac tumor may resemble clear cell carcinoma (and was once categorized with clear cell carcinoma as “mes onephroma”). Yolk sac tumor occurs in younger patients; it is highly malignant and alpha-fetoprotein positive and may be associated with other germ cell tumor components
-
♦
Clear cell renal cell carcinoma metastatic to the ovary is very rare but could be a consideration if there is a history of renal neoplasia
Transitional Cell Tumors
Clinical
-
♦
Benign Brenner tumors comprise approximately 2% of all ovarian neoplasms and are commonly incidental findings
-
♦
Borderline and malignant Brenner tumors are extremely rare
Macroscopic
-
♦
Benign Brenner tu mors are small (usually less than 2 cm) gray-white hard tumors, sometimes with calcification
-
♦
Borderline and malignant tumors are larger and partially cystic
Microscopic
-
♦
Transitional cell tumors have epithelium arranged in nests or papillary structures that resembles urothelium or Walthard cell rests. The epithelial cells are polygonal with oval nuclei, often with a longitudinal nuclear groove (“coffee-bean nuclei”). Cytoplasm is scant to moderate in volume and generally palely eosinophilic
-
♦
Transitional cell carcinomas are not associated with a benign or borderline Brenner component. Squamous differentiation may be seen. These tumors may be pure or mixed with other tumor types, such as serous carcinoma
-
♦
Malignant Brenner tumors are associated with a benign or borderline Brenner component
-
♦
Borderli ne Brenner tumors are commonly cystic with papillary structures (Fig. 32.14) with fibrovascular cores extending into the cysts. Nuclear atypia is variable
Fig. 32.14. 
Borderline Brenner tumor. This Brenner tumor was partially cystic with papillary structures projecting into the cyst lumen. There were a low-grade nuclear pleomorphism and occasional mitotic figures.
-
♦
In contrast to the malignant and borderline transitional cell tumors above (all of which are very rare), benign Brenner tumors are relatively common (3–5% of all ovarian tumors). These tumors are composed of a dense fibrous stroma, which is often focally calcified, with occasional nests of transitional cells (Fig. 32.15). The nests are rounded and may have central lumens with secretion
Fig. 32.15. 
Benign Brenner tumor. Benign Brenner tumors are composed of nests of cells resembling urothelial cells with moderately abundant, pale eosinophilic cytoplasm. The nuclei are round to oval and often have longitudinal nuclear grooves. The surrounding stroma is fibroma-like and occasional calcifications are typical.


Differential Diagnosis
-
♦
The “transiti onal cell carcinoma” pattern of high-grade serous carcinoma may look similar to malignant Brenner tumor, but it lacks a benign/borderline Brenner tumor component
Squamous Cell Tumors
-
♦
Most ovarian squamous carcinomas arise in mature cystic teratomas or are seen as a component of other epithelial tumors, but pure primary ovarian squamous cell carcinomas may rarely be seen
Mixed Epithelial-Stromal Tumors
Clinical
-
♦
Malignant mixed Müllerian tumors (carcinosarcomas) comprise 1–3% of all ovarian malignancies
-
♦
Because shared clonality has been demonstrated, using TP53 mutation and X chromosome inactivation analysis, between the epithelial and stromal components, it is believed that these tumors represent a carcinoma with transformation of part of the tumor into a mesenchymal phenotype
-
♦
Prognosis is very poor, even worse than high-grade serous carcinoma, with 15–30% 5-year survival. Some studies have reported worse prognosis with the presence of a heterologous component within the ovarian tumor, while others have not. Recurrences/metastases are usually high-grade serous carcinoma. Presence of sarcomatous component outside the ovary appears to be associated with worse prognosis
Macroscopic
-
♦
Most present at high stage, and 90% are bilateral. The tumors are large and solid but may also be partially cystic. In some cases with heterologous differentiation, cartilage may be grossly apparent
Microscopic
-
♦
The tumors have a malignant epithelial component (which may be undifferentiated, serous, or endometri oid) and a malignant stromal component (Fig. 32.16). The stromal component may be undifferentiated or show heterologous differentiation (differentiation toward tissue not expected in the ovary, such as chondrosarcoma or rhabdomyosarcoma, Fig. 32.17). The epithelial and stromal components share genetic losses and the stromal component may show focal keratin immuno positivity, findings that support a common clonal origin for the two components
Fig. 32.16. 
Malignant mixed Müllerian tumor. These tumors have a malignant epithelial component (most often resembling a serous carcinoma, as seen on the right) and a malignant stromal component (which commonly resembles an undifferentiated sarcoma, as seen on the left) with marked nuclear pleomorphism and stromal mitoses, including atypical mitoses.
Fig. 32.17. 
Malignant mixed Müllerian tumor with a heterologous rhabdomyosarcomatous component. This malignant mixed Müllerian tumor had skeletal muscle differentiation in the stromal component in the form of morphologically undifferentiated but actin and desmin positive cells, rhabdoid cells, and strap cells.
-
♦
Chondrosarcoma is the most commonly seen heterologous component, but rhabdomyoblasts, osteoid, or lipoblasts may be seen


Differential Diagnosis
-
♦
The differential diagnosis may include adenosarcomas, which are also rare and are composed of a benign-appearing Müll erian epithelium associated with a malignant stromal component. The tumors are usually unilateral, 10-year survival is 46%, and sarcomatous overgrowth is a poor prognostic finding
Undifferentiated Carcinomas
-
♦
These tumors are composed of malignant epithelial cells with a solid architecture lacki ng evidence of serous, mucinous, or any other differentiation. The prognosis is even worse than that of serous carcinoma
Sex Cord–Stromal Tumors
Granulosa Cell Tumor, Adult Type
Clinical
-
♦
Sex cord–stromal tumors represent approximately 7% of ovarian malignant tumors and adult type granulosa cell tumor is the most common, comprising 70–90% of sex cord–stromal tumors
-
♦
Over 95% of granulosa cell tumors are of adult type and, while most occur following menopause, a small percentage of cases occur in young women or girls
-
♦
Adult type granulosa cell tumors may be hormonally active, usually estrogenic, but they may also be androgenic. Postmenopausal patients may have abnormal uterine bleeding or, rarely, endometrial adenocarcinoma related to h ormone production by the tumor
-
♦
The tumors may be cystic and may rupture and present with hematoperitoneum in 5–15% of cases
-
♦
Lymph node metastases are very rare in sex cord–stromal tumors and lymphadenectomy does not appear to be necessary for staging
-
♦
Between 10 and 50% of patients develop recurrences, which may be late (20 years or more after excision of the primary tumor). Tumor rupture is a risk factor for recurrence
Macroscopic
-
♦
It is usu ally a unilateral encapsulated solid and cystic mass that, on sectioning, is yellow or tan in color
Microscopic
-
♦
Microscopically, the t umors are usually composed of rounded nests or cords of cells divided by a fibrous stroma (Fig. 32.18). The nests may have peripheral palisading. The cells have relatively uniform oval nuclei, often with longitudinal nuclear grooves. Cytoplasm is scant and weakly eosinophilic
Fig. 32.18. 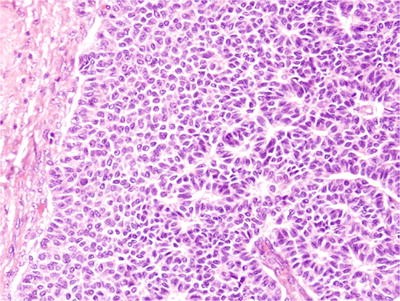
Granulosa cell tumor (adult type). Granulosa cell tumors commonly are composed of large nests of small, relatively uniform cells with minimal cytoplasm. Rosette-like Call-Exner bodies may be seen and longitudinal nuclear grooves (“coffee-bean nuclei”) are apparent at high magnification.
-
♦
Microfollicular, macrofollicular (resembling preovulatory follicles), and trabecular patterns may be seen. A convoluted trabecular pattern with little associated stroma has been described as the “watered silk” pattern
-
♦
Rosette-like Call-Exner bodies with central eosinophilic material may be seen in one-third to one-half o f these tumors
-
♦
Inhibin-alpha is positive (Fig. 32.19). Reticulin staining surrounds cords of cells but does not surround individual cells (in contrast to thecomas)
Fig. 32.19. 
Granulosa cell tumor (adult type). Immunohistochemical stain for inhibin. Cytoplasmic immunoreactivity for inhibin is expected in granulosa cell tumors and other sex cord–stromal tumors.


Differential Diagnosis
-
♦
Serous and endometrioid carcinomas, carcinoid tumor, and some metastatic carcinomas may at times show ne sted and trabecular patterns that may mimic granulosa cell tumor
-
♦
FOXL2 gene mutations are present in over 90% of adult type granulosa cell tumors and appear to be highly specific, so molecular testing for mutation in this gene may be useful in differentiating this tum or from other sex cord–stromal tumors
Granulosa Cell Tumor, Juvenile Type
Clinical
-
♦
Approximately 5% of gra nulosa cell tumors are of juvenile type, and these tumors usually occur before the age of 30
-
♦
Most cases in young girls result in isosexual pseudoprecocity
-
♦
Juvenile type granulosa cell tumors may be seen in association with several congenital syndromes including Ollier disease, Maffucci syndrome, and Goldenhar syndrome. These tumors lack the FOXL2 mutation that is characteristic of the adult type tumors
-
♦
If it is limited to the ovary in its presentation, prognosis is very good with only rare recurrences
Microscopic
-
♦
Microsc opically, juvenile type granulosa cell tumors are composed of large follicle-like structures filled with fluid and solid areas (Fig. 32.20). There may be marked nuclear atypia. Oval nuclei with longitudinal nuclear groove characteristic of adult type granulosa cell tumor are usually not seen
Fig. 32.20. 
Granulosa cell tumor (juvenile type). Juvenile type granulosa cell tumors are composed of solid areas with variable cellularity and follicle-like structures filled with fluid. Significant nuclear atypia may be seen, but the oval nuclei with longitudinal nuclear grooves typical of adult type granulosa cell tumor are not seen.

Sertoli–Leydig Cell Tumor
Clinical
-
♦
Sertoli–Le ydig tumors (formerly known as androblastoma or arrhenoblastoma) are rare, approximately 0.5% of all ovarian neoplasms
-
♦
More than one-third of patients have hormonal symptoms, most commonly virilization, but estrogen overproduction-related symptoms may also occur
-
♦
Malignant be havior is seen in 10–30% of cases
Macroscopic
-
♦
These are solid, fir m, lobulated masses, often yellow in color
Microscopic
-
♦
The tumors a re composed of solid cords (Fig. 32.21), hollow tubules (Fig. 32.22), or sheets of oval, more basophilic Sertoli cells with clusters of round Leydig cells with round nuclei and abundant eosinophilic granular cytoplasm
Fig. 32.21. 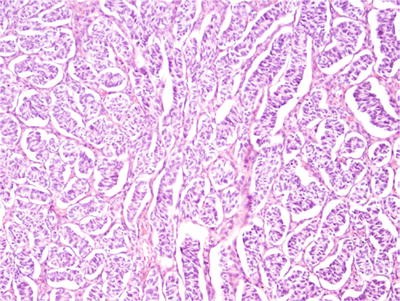
Sertoli–Leydig cell tumor. The Sertoli cell component of Sertoli–Leydig cell tumors commonly has a “solid tubule” pattern.
Fig. 32.22. 
Sertoli–Leydig cell tumor. The Sertoli cell component may also be seen as hollow tubules. Between the tubules, the Leydig cell component is seen as round to polygonal cells with round nuclei and abundant eosinophilic granular cytoplasm.
-
♦
The tumors are classified as well differentiated, intermediate differentiated, and poorly differentiated. Behavior varies by grade
-
♦
About 20% of tumors have heterologous elements such as mucinous epithelium (Fig. 32.23), cartilage, or skele tal muscle differentiation
Fig. 32.23. 
Sertoli–Leydig cell tumor with heterologous mucinous differentiation. In this tumor in addition to the Sertoli cell component (basophilic spindle-shaped cells) and the Leydig cell component (clusters of eosinophilic cells), there were also glands lined by cytologically bland mucin-producing epithelium with goblet cells that resembled intestinal epithelium.
-
♦
Inhibin-alpha is positive



Differential Diagnosis
-
♦
Poorly diff erentiated Sertoli–Leydig cell tumors may have a trabecular pattern that may resemble granulosa cell tumor
-
♦
A retiform pattern with anastomosing gland-like spaces has been described and may mimic a serous tumor, yolk sac tumor, or metastatic adenocar cinoma
Thecoma
Clinical
-
♦
Thecomas us ually occur in postmenopausal women and over half of postmenopausal patients will have abnormal uterine bleeding related to estrogen production by the tumor. Occasional (about 20%) patients may have an associated endometrial adenocarcinoma
Macroscopic
-
♦
These tum ors are grossly yellow
Microscopic
-
♦
These tum ors are composed of luteinized stromal cells with finely vacuolated cytoplasm in a background of collagen fibers (Fig. 32.24)
Fig. 32.24. 
Thecoma. This tumor is composed of luteinized stromal cells with moderately abundant, vacuolated, pale-staining cytoplasm separated by occasional collagen fibers.

Differential Diagnosis
-
♦
Granulosa cel l tumors may look similar, but reticulin staining is seen around individual cells in thecomas (in contrast to granulosa cell tumors)
Fibroma
Clinical
-
♦
Fibromas co mprise about 4% of ovarian tumors and are often small incidental tumors, but they may be large (less than 10 cm) and symptomatic
-
♦
Meigs syndrome is the combination of ascites and pleural effusion associated with an ovarian fibroma that resolves following excision of the tumor. This syndrome is seen only rarely (1–2% of fibromas)
-
♦
Fib romas are seen with increased frequency in patients with Gorlin syndrome (nevoid basal cell carcinoma syndrome)
Macroscopic
-
♦
Grossly t he tumors are hard and gray white
Microscopic
-
♦
Microscopically, smal l oval-to-spindle-shaped cells are seen in a collagenous background. At the most, mild cytologic atypia and three mitoses per high power field are seen (see fibrosarcoma below). Inhibin expression is variable
Differential Diagnosis
-
♦
Exclusion of fibrosar coma (see below) is the primary consideration
-
♦
Edematous fibromas may resemble massive ovarian edema or sclerosing stromal tumor
Fibrosarcoma
Clinical
-
♦
Fibrosarcom as are rare, but they are the most common primary ovarian sarcoma
Microscopic
-
♦
Four or more mitoses per ten high power fields and moderate to severe nuclear atypia are required for this diagnosis
Sclerosing Stromal Tumor
Clinical
-
♦
Sclerosing s tromal tumors are benign, usually occur in young women (usually younger than 30 years), and are usually hormonally inactive
Macroscopic
-
♦
These are unilateral and usually relatively small (approximately 5 cm) tumors
Microscopic
-
♦
These tumors ar e composed of cellular pseudo-lobules composed of fibroblasts and luteinized stromal cells (Fig. 32.25) and intervening hypocellular, edematous zones
Fig. 32.25. 
Sclerosing stromal tumor. The tumor is variably cellular with cellular zones with stromal cells with a luteinized appearance alternating with densely collagenized zones with a banded or “keloid-like” appearance.

Differential Diagnosis
-
♦
Some fib romas or thecomas may resemble sclerosing stromal tumor. More importantly, metastatic carcinomas (especially gastric and breast) may sometimes be seen as single pale cells in fibrous background, similar to sclerosing stromal tumor. Immunohistochemical staining for keratin will resolve this differential diagnosis
Steroid Cell Tumor
Clinical
-
♦
Steroid cell t umors occur over a wide age range and about half are hormonally active
-
♦
About one-third will have malignant behavior and features predictive of behavior include size, mitotic rate, and necrosis
Microscopic
-
♦
They are comp osed of luteinized stromal cells with clear-to-eosinophilic cytoplasm that lack crystals of Reinke. The cells are usually arranged in a solid pattern. Tumors composed of small nodules (less than 1 cm) of cells in the ovarian cortex have been referred to as “stromal luteoma” (Fig. 32.26). Inhibin is positive
Fig. 32.26. 
Stromal luteoma. These tumors are benign steroid cell tumors composed of small nodules of luteinized stromal cells that lack crystals of Reinke.

Leydig Cell Tumors
Clinical
-
♦
Leydig cell tumors are rare benign steroid cell tumors. Cases occurring near the hilus of the ovary are also known as hilus cell tumors
Macroscopic
-
♦
They are us ually small (less than 5 cm), involve the hilus of the ovary, and are yellow or brown in color
Microscopic
-
♦
They are com posed of cells with abundant eosinophilic cytoplasm that characteristically have at least occasional Reinke crystals (eosinophilic rod-shaped cytoplasmic inclusions)
-
♦
Inhibin-alp ha is positive
Gynandroblastoma
Clinical
-
♦
Gynandroblastoma is a very rare tumor that is usually hormonally active (virilizing) and benign
Microscopic
-
♦
These tumors are c omposed of a mixture of Sertoli cells forming tubules and nodules of granulosa cells that may include Call-Exner bodies
Differential Diagnosis
-
♦
Tumors withou t unequivocal Sertoli cell and granulosa cell differentiation should be classified as some other type of tumor or as sex cord–stromal tumors of indeterminate type
Sex Cord Tumor with Annular Tubules
Clinical
-
♦
This is a very rare tumor
-
♦
One-third of cases occur in association with Peutz–Jeghers syndrome. The Peutz–Jeghers-associated tumors are benign.
-
♦
Malignant behavior is seen in approximately one-quarter of cases not associated with Peutz–Jegh ers syndrome
Macroscopic
-
♦
The Pe utz–Jeghers-associated cases are usually small and bilateral and might represent hamartomas (rather than neoplasms)
-
♦
The cases not associated with Peutz–Jeghers syndrome are usually large and unilateral
Microscopic
-
♦
The tumor is composed of Sertoli cells arranged in concentric circles around hyaline globules (Fig. 32.27)
Fig. 32.27. 
Sex cord tumor with annular tubules. These tumors are composed of Sertoli cells arranged in concentric circles around hyaline globules.
-
♦
Inhibin is positive

Differential Diagnosis
-
♦
Granulosa c ell tumors with a microfollicular pattern and gonadoblastoma may resemble sex cord tumor with annular tubules
Germ Cell Tumors
General Information Concerning Ovarian Germ Cell Tumors
-
♦
While ovarian germ cell tumors as a group are relatively common (30% of ovarian tumors), mature cystic teratomas are the only tumors seen with great frequency. Mature cystic teratomas make up 95% of all ovarian germ cell tumors
-
♦
Among females in the first two decades of life, however, malignant germ cell tumors (tumors in this group other than mature cystic teratoma) are the most common type of malignant ovarian tumor
Dysgerminoma
Clinical
-
♦
Most dysgerminomas are d iagnosed before the age of 30. The tumors are usually confined to the ovary at diagnosis
-
♦
Dysgerminoma is malignant but is responsive to chemotherapy and radiotherapy and prognosis is relatively good with treatment
Macroscopic
-
♦
The tumors are large, solid multinodular masses with a pale tan or gray cut surface
Microscopic
-
♦
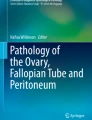
Dysgerminoma res embles testicular seminoma and is composed of a proliferation of primitive germ cells arranged in nests that are characteristically divided by occasional fibrous bands with lymphocytes (Fig. 32.28). Sometimes, small granulomas are also seen. The individual cells have large nuclei that are often round but often have flat sides
Fig. 32.28. 
Dysgerminoma. The tumor most commonly is composed of nests of cells separated by bands of collagenous stroma with associated lymphocytes. The tumor cells have large, round nuclei often with flat sides and moderately abundant clear to pale eosinophilic cytoplasm. The cytoplasm is usually eosinophilic and pale staining but may also be clear. The architecture is usually solid, but low intercellular cohesion may result in retraction spaces that mimic gland formation.
-
♦
In some cases, syncytiotrophoblastic giant cells may be seen, but these do not, by themselves, justify a diagnosis of mixed germ cell tumor
-
♦
Similar to seminoma, an isochromosome 12p cytogenetic abnormality can usually be observed by fluorescent in situ hybridization

Differential Diagnosis
-
♦
Some other tumo rs that may have a diffuse/solid pattern in the ovary and resemble dysgerminoma include juvenile granulosa cell tumor, diffuse large B-cell lymphoma, and metastatic melanoma
-
♦
Occasionally, cord-like or tubule-like patterns may be seen in dysgerminoma that may resemble sex cord–stromal tumors or glandular neoplasms
-
♦
Immunohistochemical stains for placental-like alkaline phosphatase (PLAP), c-kit (CD117), and OCT3/4 are positive in dysgerminoma. Staining is negative for alpha-fetoprotein (in contrast to yolk sac tumor), CD30 (in contrast to embryonal carcinoma), and inhibin (in contrast to sex cord–stromal tumors)
Yolk Sac Tumor (Endodermal Sinus Tumor)
Clinical
-
♦
Yolk sac tumors are malignant germ cell tumors that show evidence of differentiation into endodermal structures. Serum alpha-fetoprotein elevation and immunohistochemical expression of alpha-fetoprotein are characteristic
-
♦
Ovarian yolk sac tumors can occur in infancy and the majority occur before age 30
-
♦
These tumors tend to metastasize early even when apparently limited to the ovary. They are responsive to modern combination chemotherapy
Macroscopic
-
♦
The tumors are usually unilateral and solid, and the cut surface is gray yellow
Microscopic
-
♦
These tumors have a variety of histologic patterns including microcystic/reticular pattern and alveolar-glandular, intestinal-type, and hepatic differentiation
-
♦
In less than 20% of cases, characteristic fibrovascular projections covered by epithelium are seen (Schiller-Duval bodies). More commonly, PAS-positive eosinophilic hyaline globules are seen in association with the neoplastic epithelium (Fig. 32.29)
Fig. 32.29. 
Yolk sac tumor. Malignant glandular epithelium with associated hyaline globules and small cyst-like areas with eosinophilic secretion are seen in this tumor.

Differential Diagnosis
-
♦
Yolk sac tumor may at times be difficult to distinguish from primary ovarian carcinomas (especially clear cell carcinoma), dysgerminoma, or metastatic carcinomas. In addition to alpha-fetoprotein, glypican 3 is also a useful marker for yolk sac tumor, staining almost all cases. It should be noted that occasional (17%) ovarian clear cell carcinomas may also show at least focal staining. Keratins are usually diffusely positive (in contrast to dysgerminoma that is at most focally positive for keratin). CD30 and OCT3/4 are negative (in contrast to embryonal carcinoma which is CD30 and OCT3/4 positive). SALL4 is a germ cell tumor marker, useful if the differential diagnosis includes yolk sac tumor and somatic adenocarcinoma
-
♦
Clear cell carcinomas especially may resemble yolk sac tumor and both may have eosinophilic globules. Clear cell carcinomas, however, are usually seen in older women and are negative for alpha-fetoprotein and alpha-1-antitrypsin
Embryonal Carcinoma
Clinical
-
♦
Pure ovarian e mbryonal carcinoma is extremely rare, but embryonal carcinoma may be seen as a component of a mixed germ cell tumor
Microscopic
-
♦
The tumor is histologically seen as disorganized glands and solid areas of high nuclear grade malignant epithelium. The glands commonly have long, narrow, “slit-like” lumens. The nuclei are large and irregular but often have a pale or clear appearance in the c enter. Cytoplasm is scant
-
♦
CD30 is positive
Differential Diagnosis
-
♦
Dysgerminoma an d poorly differentiated/undifferentiated primary and metastatic carcinomas are the usual considerations
Choriocarcinoma
Clinical
-
♦
Choriocarcinoma may occur as an ovarian tumor (nongestational choriocarcinoma) or related to pregnancy (gestational choriocarcinoma)
-
♦
Pure ovarian nongestational choriocarcinoma is very rare, but choriocarcinoma can be seen as a component of a mixed germ cell tumor
Macroscopic
-
♦
The cut surfaces of these tumors are largely solid and hemorrhagic
Microscopic
-
♦
Choriocarcinoma is composed of a mixture of cytotrophoblast and syncytiotrophoblast, commonly associated with hemorrhage. The tumor cells immunohistochemically express beta-human chorionic gonadotropin
Differential Diagnosis
-
♦
In rare cases, gestational and nongestational choriocarcinoma may be difficult to distinguish. Obtaining adequate history (of pregnancy, gestational trophoblastic disease, and prior tumors) and search for other germ cell tumor components (which, if present, indicate nongestational choriocarcinoma) are critical in this situation
-
♦
Pure ovarian nongestational choriocarcinoma is rare, so a pure choriocarcinoma in a woman of reproductive age should be suspected to represent gestational choriocarcinoma
Mature Cystic Teratoma (Dermoid Cyst)
Clinical
-
♦
Mature cystic teratoma is benign and the only common ovarian germ cell tumor
-
♦
These tumors have a wide age distribution but usually present in premenopausal women. They are the most common pediatric ovarian neoplasm. They may present with symptoms relating to torsion or cyst rupture
Macroscopic
-
♦
Grossly, the tumors are cystic, often filled with grayish granular keratinized debris and hair. Gross examination may identify cartilage, pigmented areas (retinal differentiation), or brain-like glial tissue. Often the cyst has a nodule at one side with more or less well-formed toothlike structures and bone (the “Rokitansky protuberance”)
Microscopic
-
♦
These tumors are usually biphasic or triphasic, meaning that they show differentiation into tissues formed by two or three embryonic germ layers
-
♦
Microscopically, the tumors are composed of cytologically bland, highly differentiated tissues of a variety of types. Skin, hair, sebaceous glands, cartilage, adipose tissue, respiratory and gastrointestinal-type epithelium, and glial tissue are among the most common but many other recognizable tissue types may also be seen
-
♦
Rare cases of mature cystic teratoma may undergo malignant transformation with a squamous cell carcinoma being the most common malignancy to develop (80% of cases). Adenocarcinomas, sarcomas, and a large number of other tumors may also occur
Differential Diagnosis
-
♦
Exclusion of an immature teratoma component is the main concern
Monodermal Teratoma
-
♦
Monodermal teratomas are composed entirely or predominantly of a single type of tissue from one embryonic layer
-
♦
The most common type of monodermal teratoma is struma ovarii, a tumor composed of thyroid tissue (Figs. 32.30 and 32.31). Struma ovarii is an ovarian tumor that is composed predominantly (>50%) of thyroid tissue or contains hormonally functional or histologically malignant thyroid tissue. While struma ovarii is almost always benign, thyrotoxicosis is seen in 5% of cases, and rare cases of malignant struma ovarii (usually resembling papillary thyroid carcinoma) are seen
Fig. 32.30. 
Struma ovarii. This g ross photo shows an ovarian tumor with a nodular, red-brown, somewhat gelatinous cut surface resembling a multinodular goiter of the thyroid.
Fig. 32.31. 
Struma ovarii. Microscopically, the tumor is composed of follicles filled with dense eosinophilic colloid. The lining epithelium is cuboidal and cytologically bland. “Scolloping” (the presence of clear vacuole-like spaces at the interface between the epithelium and colloid) is seen.
-
♦
Carcinoid tumors may occur in the ovary as a pure carcinoid tumor, associated with a mature cystic teratoma (Fig. 32.32), associated with a Brenner tumor, or as a strumal carcinoid (associated with struma ovarii, Fig. 32.33)
Fig. 32.32. 
Carcinoid tumor in association with mature cystic teratoma. This teratoma had areas of carcinoid tumor.
Fig. 32.33. 
Strumal carcinoid. This t umor was composed primarily of carcinoid tumor with nested and trabecular architecture. Occasional clusters of colloid containing thyroid follicles were also present.
-
♦
Rarely, other tumors probably representing monodermal teratomas can be seen, including pituitary adenomas, ependymomas, and primitive neuroectodermal tumors (PNET)




Immature Teratoma
-
♦
Approximately 3% of ovarian teratomas have immature foci composed of neuroectodermal rosettes and tubules, often in a background of glial tissue, and these tumors have the potential for malignant behavior
-
♦
The immature teratoma component is positive for glial fibrillary acidic protein (GFAP), neuron-specific enolase, and S-100 protein
-
♦
Immature teratoma is graded based on the extent of the immature component. Grade 1 tumors have less than one low power field with immature neuroepithelial tissue on any one slide. Grade 2 tumors have 1–3 low power (×40) fields per slide. Grade 3 tumors have immature neuroepithelium in more than three low power fields per slide. A two-tier grading system (with grade 1 being considered low grade and grades 2–3 equivalent to high grade) has also been proposed
Gonadoblastoma
-
♦
Gonadoblastoma is a mixed germ cell–sex cord–stromal tumor composed of mixture of a dysgerminoma-like component and a sex cord component that may be similar to Sertoli cells, granulosa cells, or luteinized stromal cells (Fig. 32.34). The cells are arranged in nests with the germ cells in the middle and the stromal cell component arranged around the outside of the nest and around rounded collections of hyaline material. Calcification of the hyaline material may be prominent, producing rounded, sometimes fused calcifications
Fig. 32.34. 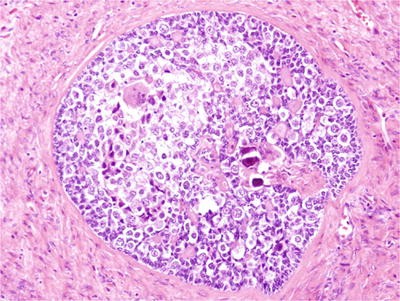
Gonadoblastoma. Gonadoblastoma is a mixed germ cell–sex cord–stromal tumor composed of dysgerminoma-like cells and a sex cord component in the form of Sertoli cells, granulosa cells, or luteinized stromal cells. The cells are arranged in a nested pattern with the germ cells in the middle and the stromal cell component arranged around the outside. Collections of hyaline material and calcifications are seen.
-
♦
Dysgerminoma is found in association with gonadoblastoma in a large fraction of cases. In some cases only the rounded calcifications of the gonadoblastoma remain (“burnt-out gonadoblastoma”)
-
♦
Most patients with gonadoblastoma have gonadal dysgenesis. These individuals are phenotypically female, have a Y chromosome or Y chromosome material, and have a mutation in a gene necessary for gonadal development (including WT1, SRY, SOX9, DHH, ARX, SF1, and TSPYL1). Gonadoblastoma may also be seen in patients with Turner syndrome (45, XO), but in this situation it is believed that at least the TSPY gene from the Y chromosome is present in at least some cells (undetected mosaicism)

Miscellaneous Tumors Including Stromal Neoplasms, Secondary Carcinomas, and Other Neoplasms
Small Cell Carcinoma, Hypercalcemic Type
Clinical
-
♦
This is a malignant tumor with a poor prognosis (10% 5-year survival). It is associated with paraneoplastic hypercalcemia in two-thirds of cases (due to production of parathyroid hormone-related protein)
-
♦
Patient age is usually young (10–40 years). SMARCA4 mutations are seen in most cases, often with germline mutation, supporting the interpretation that this tumor may represent a “malignant rhabdoid tumor” of the ovary
Macroscopic
-
♦
The tumors are unilateral and solid
Microscopic
-
♦
It is composed of cells in a diffuse pattern with scant cytoplasm and pleomorphic nuclei (Fig. 32.35). Prominent nucleoli and moderately abundant eosinophilic cytoplasm may be seen in some cases, and these features help distinguish the tumor from ovarian pulmonary-type small cell carcinoma
Fig. 32.35. 
Small cell carcinoma, hypercalcemic type. This tumor is composed of cells in a solid pattern with very scant cytoplasm and large, pleomorphic nuclei.

Differential Diagnosis
-
♦
In some cases follicle-like spaces may be present that resemble juvenile type granulosa cell tumor, but small cell carcinoma of hypercalcemic type is EMA positive and inhibin negative
-
♦
Metastatic small cell carcinoma of pulmonary origin, dysgerminoma, lymphoma, and other “small-celled” tumors must be excluded
Small Cell Carcinoma, Pulmonary Type
Clinical
-
♦
This is a rare malignant tumor, usually presenting in postmenopausal patients, with a poor prognosis
-
♦
Occasionally, this tumor can be associated with another tumor type (such as a Brenner tumor or endometrioid carcinoma)
Microscopic
-
♦
This tumor resembles small cell carcinoma of the lung with moderate size nuclei, nuclear molding, and very scant cytoplasm
Differential Diagnosis
-
♦
Metastatic pulmonary small cell carcinoma must be excluded. Other tumors (including ovarian small cell carcinoma, hypercalcemic type) may also be considered
Hepatoid Carcinoma
Clinical
-
♦
This is a very rare highly aggressive neoplasm with a poor prognosis
Microscopic
-
♦
The tumor histologically resembles hepatocellular carcinoma
Differential Diagnosis
-
♦
It must be distinguished from hepatoid pattern yolk sac tumor. Both are immunohistochemically positive for alpha-fetoprotein. Hepatoid carcinoma is not associated with other germ cell tumor components, while hepatoid pattern yolk sac tumor may be admixed with other patterns of yolk sac tumor or other germ cell tumor elements. Also, hepatoid carcinoma is usually seen in postmenopausal patients, while yolk sac tumor is usually seen in patients under 30 years of age
Ovarian Tumor of Probable Wolffian Origin (Wolffian Tumor)
Clinical
-
♦
This tumor may occur in the broad ligament or ovary
-
♦
A fraction of cases may have malignant behavior
Microscopic
-
♦
It may have tubular, hollow tubular, solid, and “sieve-like” patterns
Differential Diagnosis
-
♦
The tumor is positive for some keratins (7, 19, CAM 5.2) and CD10, which may be helpful in differentiating it from Sertoli–Leydig cell tumor, which it may resemble
Benign Stromal Neoplasms
-
♦
A variety of stromal neoplasms not specific to the ovary, such as hemangiomas, may be seen as an ovarian tumor, but all are rare
-
♦
Myxomas are rare benign tumors composed of cytologically bland spindle cells in a background of abundant pale-staining basophilic stroma composed of hyaluronic acid
-
♦
Primary leiomyoma of the ovary is rare and often an incidental finding. Immunohistochemical staining for smooth muscle markers may be useful for distinguishing leiomyoma from the much more common ovarian fibroma
Sarcomas
-
♦
A variety of histologic types of sarcoma (including undifferentiated sarcoma) not specific to the ovary have been reported as a primary ovarian tumor. All are very rare
-
♦
Primary ovarian rhabdomyosarcoma has been reported, but the presence of a coexisting carcinoma component in the tumor (indicating a malignant mixed Müllerian tumor) must be exclu ded
Metastatic Carcinomas
Clinical
-
♦
Metastatic carcinom as frequently involve the ovary and are identified in approximately one-third of women dying of cancer
-
♦
General features favoring a metastatic carcinoma over a primary ovarian carcinoma include bilaterality, the presence of small superficial tumor deposits, vascular invasion, and a desmoplastic stromal response. Obtaining adequate history, particularly concerning previous malignancies and gastrointestinal symptoms, is also critical
-
♦
Carefully selected immunohistochemical stains may be useful in some cases. PAX8 is a newer nuclear marker that is positive in most gynecologic tract, renal, and thyroid tumors. WT1, CA125, p53, and ER are similarly useful in certain circumstances, but all also stain nonovarian tumors (see Table 32.1)
Macroscopic
-
♦
Bilaterality and the presence of multiple nodules of tumor within an ovary are suggestive of metastatic disease
Microscopic
-
♦
Krukenberg tumors are metastatic adenocarcinomas with signet-ring morphology involving the ovary (Fig. 32.36). These tumors most often originate from a diffuse-type gastric adenocarcinoma, but this morphology can also represent a metastatic colorectal, appendiceal, breast, or other adenocarcinomas. Metastatic gastric carcinoma is especially likely to be clinically mistaken for a primary ovarian carcinoma as diffuse-type gastric carcinoma may be clinically occult, may be associated with ascites, and the ovarian mass may be the first tumor identified
Fig. 32.36. 
Metastatic gastric diffuse-type adenocarcinoma (Krukenberg tumor). The tumor is highly cellular with round, pleomorphic cells, some of which contain mucin vacuoles, which indent the nucleus (signet-ring cells).
-
♦
Colorectal adenocarcinomas commonly involve the ovaries and may in some cases present as a unilateral or bilateral ovarian mass prior to detection of the colorectal primary. Histologic clues to the proper diagnosis include the presence of large malignant glands with necrosis of segments of the lining epithelium (“segmental necrosis”) and the presence of abundant necrotic debris with basophilic nuclear debris (“dirty necrosis,” Fig. 32.37). Some tumors may be difficult to distinguish from a primary ovarian mucinous carcinoma or mucinous borderline tumor. Immunohistochemical staining may, in some cases, be useful as colorectal carcinomas are usually CDX2+/keratin 7−, and ovarian mucinous tumors are usually CDX2−/keratin 7+, but the expression of both of these markers is variable in both of these tumor types so the staining pattern must be evaluated along with the patient history and gross and morphologic findings. Keratin 20 is usually positive in both colorectal adenocarcinoma and ovarian mucinous tumors so it is not especially useful in this situation
Fig. 32.37. 
Metastatic colorectal adenocarcinoma involving the ovary. Features suggestive of metastatic colorectal adenocarcinoma include the presence of necrotic debris with basophilic nuclear debris in the glands (“dirty necrosis”) and columnar cell architecture with occasional goblet cells.
-
♦
Low-grade appendiceal mucinous neoplasm metastatic to the ovary (Fig. 32.38) may be mistaken for ovarian mucinous borderline tumors or even mucinous cystadenomas. Free mucin dissecting through stroma is commonly seen in low-grade appendiceal mucinous neoplasms and is a possible clue, but this may also be seen in primary ovarian mucinous tumors. A low-grade mucinous ovarian tumor received for frozen section examination should prompt the pathologist to ask the surgeon about the status of the appendix and excision and histologic examination of the appendix may be indicated
Fig. 32.38. 
Metastatic low-grade appendiceal mucinous neoplasm involving the ovary. Appendiceal tumors may closely mimic a primary ovarian mucinous neoplasm.
-
♦
Pancreatic adenocarcinoma may be clinically occult and rarely presents as an ovarian mass, which may be cystic and histologically mimic a primary ovarian borderline tumor (Fig. 32.39) or a carcinoma
Fig. 32.39. 
Metastatic pancreatic adenocarcinoma involving the ovary. Metastatic pancreatic adenocarcinomas may involve the ovary, be cystic, and have prominent papillary architecture, mimicking a low malignant potential tumor. This ovarian mass histologically closely resembles a serous low malignant potential tumor, but a morphologically similar primary pancreatic adenocarcinoma was resected in the same operation.
-
♦
Breast carcinoma may metastasize to the ovary and immunohistochemical stains such as ER a nd PR are not useful to distinguish carcinomas of breast and ovarian origin as these stains are commonly positive in each. GATA3 is a nuclear stain, useful as a consistent marker of breast origin, but it should be remembered that GATA3 staining is typical of germ cell tumors and can be seen in rare ovarian epithelial tumors. Mammaglobin and GCDFP-15 are negative in ovarian carcinomas
-
♦
Renal cell carcinoma, carcinoid tumor, melanoma, and sarcomas all also may metastasize to the ovary




Lymphomas and Leukemias
Clinical
-
♦
Diffuse large B-cell lymphoma (Fig. 32.40), Burkitt lymphoma, and follicular lymphomas are the most common types. Burkitt lymphoma occurs primarily in children, but may also affect adults. It may present with abdominal pain and swelling with bilateral ovarian involvement
Fig. 32.40. 
Diffuse large B-cell lymphoma involving the ovary. The histologic appearance of lymphoma may, in some cases, be difficult to distinguish from some carcinomas and stromal tumors without immunohistochemical stains.
-
♦
The ovaries may be secondarily involved by leukemia, but primary ovarian myeloid sarcoma is extremely rare. Occasional myeloid sarcomas are green in color (“chloroma”)

Macroscopic
-
♦
Ovarian lymphomas are bilateral in one-half of cases, but Burkitt lymphoma is almost always bilateral. The cut surface of the tumor is usually soft, solid, and gray white in color
Microscopic
-
♦
Either a diffuse infiltrate or nodules of lymphoid cells may be seen
-
♦
Staining with CD45 and (for B-cell neoplasms) CD20 is expected. EMA and keratins will be negative
Part B ____________________________________The Peritoneum
Mesothelial Lesions
Peritonitis
-
♦
Acute peritonitis is usually bacterial or chemical, such as following a perforated viscus. Spontaneous bacterial peritonitis may also occur and risk factors include cirrhosis and immunosuppression. Peritonitis is seen histologically as a serosal fibrinopurulent exudate
-
♦
Granulomatous peritonitis can result from infections (tuberculosis, fungal infections, or parasitic infections) or from foreign body reaction (starch or talc from surgical gloves, hysterosalpingographic contrast medium, keratin from ruptured teratomas, or spillage of amnionic fluid or meconium at cesarean section)
Mesothelial Hyperplasia
Clinical
-
♦
Mesothelial hyperplasia may result from chronic salpingitis, endometriosis, or adnexal tumors or cysts
Microscopic
-
♦
Significant cellular enlargement, cellular stratification, and nuclear atypia may be seen. In some cases, papillary architecture or even psammoma bodies may be seen
Differential Diagnosis
-
♦
Mesothelial hyperplasia is a potential pitfall in peritoneal fluid or pelvic washing cytology. Identification of features of mesothelial cells such as a generally low nucleus-to-cytoplasm ratio, oval nuclei, peripheral attenuation of the cytoplasm, and “scalloped” cell group margins is helpful. In problematic cases, preparation of a cell block for immunohistochemical staining is useful. The cells of mesothelial hyperplasia will usually stain for calretinin, thrombomodulin, and podoplanin/D2-40 and are usually negative for MOC-31/ERA and Ber-Ep4. The usual carcinomas in this differential diagnosis will usually be positive for MOC-31 and Ber-Ep4 and negative for calretinin, thrombomodulin, and podoplanin/D2-40. It should be remembered that no single marker appears to be perfectly reliable for the differentiation of mesothelial cells (or mesothelioma) and carcinoma
Endometriosis
-
♦
See “Endo metriosis” in the ovary section
Endosalpingiosis
Clinical
-
♦
Endosalpingiosis is a benign incidental finding, present in approximately 7% of premenopausal women
Microscopic
-
♦
It is seen microscopically as glands composed of ciliated tubal-type simple columnar epithelium in a peritoneal surface or within a pelvic or retroperitoneal lymph node (Fig. 32.41). Occasionally, associated psammoma bodies may be seen
Fig. 32.41. 
Epithelial inclusions in a pelvic lymph node. Benign glandular inclusions composed of a ciliated columnar epithelium, sometimes with associated psammoma bodies, may be seen in pelvic lymph nodes. Care must be taken to avoid over diagnosis as metastatic adenocarcinoma.

Differential Diagnosis
-
♦
Endosalpingiosis can potentially be mistaken for adenocarcinoma. The presence of glandular epithelium in lymph n odes or other unexpected sites is a potential pitfall and can lead to overdiagnosis of metastatic malignancy. Recognition of the cilia and bland cytology are important clues that may help avoid this error, but cilia may be difficult to i dentify on frozen sections
Splenosis
-
♦
Splenosis is the finding of splenic tissue implants on peritoneal surfaces following a remote history of traumatic splenic rupture
Peritoneal Inclusion Cysts
-
♦
Peritoneal inclusion cysts are benign and are usually an incidental finding. They may be solitary or multiple and are thin-walled translucent cysts with a flattened mesothelial lining
-
♦
Multilocular peritoneal inclusion cysts (also known as benign cystic mesotheliomas, Fig. 32.42) may form tumorlike masses and be associated with pelvic pain. Most patients with multilocular peritoneal inclusion cysts will have a history of abdominal surgery, pelvic inflammatory disease, and/or endometriosis. Occasional cases may recur locally
Fig. 32.42. 
Multilocular peritoneal inclusion cyst. The lesion is composed of multiple cyst-like structures lacking a prominent epithelial lining.

Well-Differentiated Papillary Mesothelioma
-
♦
Well-differentia ted papillary mesotheliomas are rare lesions, usually less than 2 cm in size, which are usually incidental findings. The tumors are composed of fibrovascular papillae covered by a single layer of cuboidal mesothelial cells. Behavior is usually benign, but progression to malignant mesothelioma may rarely occur
-
♦
Mesothelial markers such as calretinin and D2-40 are positive, but it should be remembered that epithelial cell markers such as EMA and keratin 7 also stain mesothelial lesions
Peritoneal Malignant Mesothelioma (Diffuse Malignant Mesothelioma)
Clinical
-
♦
Peritoneal malignant mesothelioma is less common (only 10–20% of all mesotheliomas) than pleural malignant mesothelioma. In women, peritoneal malignant mesothelioma is not related to asbestos exposure. Ascites is usually present, and ovarian involvement may occur, possibly mimicking an ovarian carcinoma (Fig. 32.43)
Fig. 32.43. 
Peritoneal malignant mesothelioma involving the ovary. The glandular and papillary architecture may closely resemble a serous carcinoma.
-
♦
These tumors have a poor prognosis, but approximately 40% of women with peritoneal malignant mesothelioma may survive for more than 4 years

Macroscopic
-
♦
The tumor is seen grossly as multiple nodules of tumor on a peritoneal surface
Microscopic
-
♦
The tumor cells are usually epithelioid with abundant eosinophilic cytoplasm, but sarcomatoid or biphasic mesotheliomas can also occur. Papillary, tubular, and solid architecture may be seen and the tumor may be mistaken for ovarian or primary peritoneal serous carcinoma (Fig. 32.44). Psammoma bodies may occasionally be present
Fig. 32.44. 
Peritoneal malignant mesothelioma replacing the omentum. Mesothelioma may have a gross distribution of disease and a papillary histology that may be result in a misdiagnosis of an ovarian or primary peritoneal serous carcinoma.

Differential Diagnosis
-
♦
Immunoh istochemical staining is commonly necessary to distinguish mesothelioma from other malignancies, and any panel of i mmunohistochemical stains used for this purpose should include multiple mesothelial and epithelial markers (see “Mesothelial Hyperplasia” above)
Desmoplastic Small Round Cell Tumor
Clinical
-
♦
The origin of this extremely rare tumor is uncertain. It is more common in males than females, the mean age at presentation is approximately 19, and the prognosis is very poor, with more than 90% of patients dying of the tumor even with aggressive treatment
Microscopic
-
♦
Histologically, it is c omposed of well-circumscribed nests of small malignant cells surrounded by a densely fibrous stroma. The tumor cells have an unusual immunophenotype with coexpression of keratin, epithelial membrane antigen, neuron-specific enolase, desmin, vimentin, and WT1
-
♦
The tumor has a characteristic t(11:22) resulting in the fusion of the EWS (Ewing’s sarcoma) gene and the WTI (Wilms’ tumor) gene, so cytogenetic analysis may be helpful in the diagnosis
Epithelial Tumors of Müllerian Type
Primary Peritoneal Carcinoma
-
♦
Primary peritoneal carcinomas are microscopically indistinguishable from ovarian high-grade serous carcinomas, but, by definition, the ovary and fallopian tube are grossly and microscopically free of tumor. Serous carcinomas are the most common subtype of primary peritoneal carcinoma. Staging, treatment, and prognosis are similar to those of ovarian carcinomas
-
♦
Low-grade serous carcinomas (often with abundant psammoma bodies, the so-called psammocarcinoma) and serous tumors of low malignant potential may also occur
Miscellaneous Peritoneal Lesions
Infarcted Appendix Epiploica
-
♦
Colonic appendices epiploicae may undergo torsion and become infarcted and calcified. These may be encountered surgically as a hard mass and may be submitted for pathologic examination. Occasionally, autoamputation may occur, and the appendix epiploica may be found free in the peritoneal space. Histologically, necrotic fat and calcification are seen
Walthard Nest
-
♦
The female pelvic peritoneum may undergo metaplastic change into any of the types of Müllerian epithelium. One of the most commonly seen examples of metaplasia of the peritoneum is the presence of Walthard cell rests, which may be cystic, on the serosal surface of the fallopian tube. These small (approximately 1 mm) whitish nodules are composed of nests of benign epithelial cells that histologically resemble urothelium (Fig. 32.45)

Walthard cell rests. Walthard cell rests, which may be cystic, may be seen in the fallopian tube serosa or elsewhere in the pelvic peritoneum.
Tailgut Cyst (Retrorectal Cystic Hamartoma)
Clinical
-
♦
Tailgut cysts are benign cystic lesions found between the rectum and sacrum. Rare cases of malignant transformation have been reported, usually as an adenocarcinoma component arising in the tailgut cyst
-
♦
Synonyms for tailgut cyst include retrorectal cystic hamartoma and epidermoid cyst
Macroscopic
-
♦
These are thin-walled cysts filled with granular keratin debris
Microscopic
-
♦
They are usually lined by a squamous epithelium (Fig. 32.46). The lining may occasionally be lined by a mucinous or ciliated glandular epithelium. The wall of the cyst is composed of fibrous connective tissue and smooth muscle
Fig. 32.46. 
Tailgut cyst. These benign cystic lesions occur between the rectum and sacrum. They are most commonly lined by a squamous epithelium and have fibrous tissue and smooth muscle in the wall.

Differential Diagnosis
-
♦
The term mature cystic teratoma should be reserved for lesions with differentiated components other than those described above for tailgut cysts. Tissue types such as glial tissue, teeth, cartilage, or peripheral nerve in a presacral cystic lesion would merit a diagnosis of teratoma and imply greater potential for recurrence
Ectopic Decidual Reaction
-
♦
Ectopic decidual reaction may be seen in the pelvic peritoneum, as well as in the ovary, fallopian tube, and pelvic lymph nodes. The stromal cells become enlarged in response to progesterone and are seen as nodules of plump, rounded cells with eosinophilic cytoplasm that may have some nuclear atypia. Associated stromal hemorrhage may be seen. This finding, especially when within a lymph node, could potentially be mistaken for malignancy
Metastatic Tumors
-
♦
Metastatic ovarian carcinoma is the most common carcinoma to be seen as peritoneal carcinomatosis. Endometrial, fallopian tube, and primary peritoneal carcinomas may also be seen and are histologically similar to ovarian carcinomas
-
♦
Nongynecologic carcinomas that may have peritoneal involvement include breast, colorectal, gastric, and pancreatic carcinomas
Pseudomyxoma Peritonei
-
♦
The presence of abundant intraabdominal mucin is clinically termed pseudomyxoma peritonei. This finding is most commonly associated with a low-grade appendiceal mucinous neoplasm. See also “Metastatic Tumors” in the ovary section above
TNM Classification of Ovarian Tumors (2010 Revision)
-
♦
Prim ary Tumor (T)
-
TX: Primary tumor cannot be assessed
-
T0: No evidence of primary tumor
-
T1: Tumor limited to ovaries (one or both)
-
T1a: Tumor limited to one ovary; capsule intact, and no tumor on the ovarian surface. No malignant cells in ascites or peritoneal washings
-
T1b: Tumor limited to both ovaries; capsules intact, and no tumor on the ovarian surface. No malignant cells in ascites or peritoneal washings
-
T1c: Tumor limited to one or both ovaries with any of the following: capsule ruptured, tumor on the ovarian surface, and malignant cells in ascites or peritoneal washings
-
T2: Tumor involves one or both ovaries with pelvic extension
-
T2a: Extension and/or implants on uterus and/or tube(s). No malignant cells in ascites or peritoneal washings
-
T2b: Extension to and/or implants on other pelvic tissues. No malignant cells in ascites or peritoneal washings
-
T2c: Pelvic extension and/or implants (T2a or T2b) with malignant cells in ascites or peritoneal washings
-
T3: Tumor involves one or both ovaries with microscopically confirmed peritoneal metastasis outside the pelvis
-
T3a: Microscopic peritoneal metastasis beyond pelvis (no macroscopic tumor)
-
T3b: Macroscopic peritoneal metastasis beyond pelvis 2 cm or less in greatest dimension
-
T3c: Peritoneal metastasis beyond pelvis more than 2 cm in greatest dimension and/or regional lymph node metastasis
-
-
♦
Regional Lymph Nodes (N)
-
NX: Regional lymph nodes cannot be assessed
-
N0: No regional lymph node metastasis
-
N1: Regional lymph node metastasis
-
-
♦
Distant Metastasis (M)
-
MX: Distant metastasis cannot be assessed
-
M0: No distant metastasis
-
M1: Distant metastasis (excludes peritoneal metastasis)
-
Suggested Reading
Bodurka DC, Deavers MT, Tian C, et al. Reclassification of serous ovarian carcinoma by a 2-tier system. Cancer. 2012;118:3087–94.
Buis CCM, van Leeuwen FE, Mooij TM, et al. Increased risk for ovarian cancer and borderline ovarian tumors in subfertile women with endometriosis. Hum Reprod. 2013;28:3358–69.
Clement PB. Nonneoplastic lesions of the ovary (Chapter 16). In: Kurman RJ, editor. Blaustein’s pathology of the female genital tract. 5th ed. New York: Springer; 2002a. p. 675–727.
Clement PB. Diseases of the peritoneum (Chapter 17). In: Kurman RJ, editor. Blaustein’s pathology of the female genital tract. 5th ed. New York: Springer; 2002b. p. 729–89.
Cribb B, Vishwanath N, Upadhyay V. Paediatric ovarian lesions—the experience at Starship Children’s Hospital, New Zealand. N Z Med J. 2014;127:41–51.
Crum CP, Herfs M, Ning G, et al. Through the glass darkly: intraepithelial neoplasia, top-down differentiation, and the road to ovarian cancer. J Pathol. 2013;231:402–12.
del Carmen MG, Birrer M, Schorge JO. Carcinosarcoma of the ovary: a review of the literature. Gynecol Oncol. 2012a;125:271–7.
del Carmen MG, Birrer M, Schorge JO. Clear cell carcinoma of the ovary: a review of the literature. Gynecol Oncol. 2012b;126:481–90.
du Bois A, Ewald-Riegler N, de Gregorio N, et al. Borderline tumors of the ovary: a cohort study of the Arbeitsgmeinschaft Gynäkologische Onkologie (AGO) Study Group. Eur J Cancer. 2013;49:1905–14.
Esheba GE, Pate LL, Longacre TA. Oncofetal protein glypican-3 distinguishes yolk sac tumor from clear cell carcinoma of the ovary. Am J Surg Pathol. 2008;32:600–7.
Foulkes WD, Clarke BA, Hasselblatt M, et al. No small surprise—small cell carcinoma of the ovary, hypercalcemic type, is a malignant rhabdoid tumor. J Pathol. 2014;233:209–14.
Gounaris I, Charnock-Jones DS, Brenton JD. Ovarian clear cell carcinoma—bad endometriosis or bad endometrium? J Pathol. 2011;225:157–60.
Khunamornpong S, Settakorn J, Sukpan K, et al. Mucinous tumor of low malignant potential (“borderline” or “atypical proliferative” tumor) of the ovary: a study of 171 cases with the assessment of intraepithelial carcinoma and microinvasion. Int J Gynecol Pathol. 2011;30:218–30.
Kohn EC, Romano S, Lee JM. Clinical implications of using molecular diagnostics for ovarian cancers. Ann Oncol. 2013;24 Suppl 10:x22–6.
Kommoss S, Anglesio MS, Mackenzie R, et al. FOXL2 molecular testing in ovarian neoplasms: diagnostic approach and procedural guidelines. Mod Pathol. 2013;26:860–7.
Kunkel J, Peng Y, Tao Y, et al. Presence of a sarcomatous component outside the ovary is an adverse prognostic factor for primary ovarian malignant mixed mesodermal/Mullerian tumors: a clinicopathologic study of 47 cases. Am J Surg Pathol. 2012;36:831–7.
Kurman RJ. Origin and molecular pathogenesis of ovarian high-grade serous carcinoma. Ann Oncol. 2013;24 Suppl 10:x16–21.
Kurman RJ, Carcangiu ML, Herrington CS, Young RH, editors. WHO classification of tumours of female reproductive organs. Lyon: International Agency for Research on Cancer (IARC); 2014.
Lee S, Nelson G, Duan Q, et al. Precursor lesions and prognostic factors in primary peritoneal serous carcinoma. Int J Gynecol Pathol. 2013;32:547–55.
Lin JE, Seo S, Kushner DM, et al. The role for appendectomy for mucinous ovarian neoplasms. Am J Obstet Gynecol. 2013;208:46.e1–4.
Mangili G, Bergamini A, Taccagni G, et al. Unraveling the two entities of endometrioid ovarian cancer: a single center clinical experience. Gynecol Oncol. 2012;126:403–7.
McCluggage WG. Immunohistochemistry in the distinction between primary and metastatic ovarian mucinous neoplasms. J Clin Pathol. 2012;65:596–600.
Miettinen M, McCue PA, Sarlomo-Rikala M, et al. GATA3: a multispecific but potentially useful marker in surgical pathology: a systemic analysis of 2500 epithelial and nonepithelial tumors. Am J Surg Pathol. 2014;38:13–22.
Offman SL, Longacre TA. Clear cell carcinoma f the female genital tract (not everything is as clear as it seems). Adv Anat Pathol. 2012;19:296–312.
Prat J. Ovarian carcinomas: five distinct diseases with different origins, genetic alterations, and clinicopathological features. Virchows Arch. 2012;460:237–49.
Rabban JT, Barnes M, Chen LM, et al. Ovarian pathology in risk-reducing salpingo-oophorectomies from women with BRCA mutations, emphasizing the differential diagnosis of occult primary and metastatic carcinoma. Am J Surg Pathol. 2009;33:1125–36.
Roth LM. Recent advances in the pathology and classification of ovarian sex cord–stromal tumors. Int J Gynecol Pathol. 2006;25:199–215.
Roth LM, Talerman A. Recent advances in the pathology and classification of ovarian germ cell tumors. Int J Gynecol Pathol. 2006;25:305–20.
Russell P, Robboy SJ, Anderson MC. The ovaries: normal appearances and nonneoplastic conditions (Chapter 18). In: Robboy SJ, Anderson MC, Russel P, editors. Pathology of the female reproductive tract. Edinburg: Churchill Livingstone; 2002a. p. 475–690.
Russell P, Robboy SJ, Anderson MC. Epithelial/stromal ovarian tumors (Chapter 20). In: Robboy SJ, Anderson MC, Russel P, editors. Pathology of the female reproductive tract. Edinburg: Churchill Livingstone; 2002b. p. 539–605.
Russell P, Robboy SJ, Anderson MC. Sex cord–stromal and steroid cell tumors of the ovaries (Chapter 21). In: Robboy SJ, Anderson MC, Russel P, editors. Pathology of the female reproductive tract. Edinburg: Churchill Livingstone; 2002c. p. 607–40.
Russell P, Robboy SJ, Anderson MC. Germ cell tumors of the ovaries (Chapter 22). In: Robboy SJ, Anderson MC, Russel P, editors. Pathology of the female reproductive tract. Edinburg: Churchill Livingstone; 2002d. p. 641–90.
Seidman JD, Russel P, Kurman RJ. Surface epithelial tumors of the ovary (Chapter 18). In: Kurman RJ, editor. Blaustein’s pathology of the female genital tract. 5th ed. New York: Springer; 2002. p. 791–904.
Tadahisa T, Ohishi Y, Imamura H, et al. Ovarian transitional cell carcinoma represents a poorly differentiated form of high-grade serous or endometrioid adenocarcinoma. Am J Surg Pathol. 2013;37:1091–9.
Talerman A. Germ cell tumors of the ovary (Chapter 20). In: Kurman RJ, editor. Blaustein’s pathology of the female genital tract. 5th ed. New York: Springer; 2002a. p. 967–1033.
Talerman A. Nonspecific tumors of the ovary, including mesenchymal tumors and malignant lymphoma (Chapter 21). In: Kurman RJ, editor. Blaustein’s pathology of the female genital tract. 5th ed. New York: Springer; 2002b. p. 1035–61.
Thrall MM, Paley P, Pizer E, et al. Patterns of spread and recurrence of sex cord–stromal tumors of the ovary. Gynecol Oncol. 2011;122:242–5.
Ulbright TM, Young RH. Gonadoblastoma and selected other aspects of gonadal pathology in young patients with disorders of sex development. Semin Diagn Pathol. 2014;31:427–40.
Young RH, Scully RE. Sex cord–stromal, steroid cell, and other ovarian tumors with endocrine, paraendocrine, and paraneoplastic manifestations (Chapter 19). In: Kurman RJ, editor. Blaustein’s pathology of the female genital tract. 5th ed. New York: Springer; 2002a. p. 905–66.
Young RH, Scully RE. Metastatic tumors of the ovary (Chapter 22). In: Kurman RJ, editor. Blaustein’s pathology of the female genital tract. 5th ed. New York: Springer; 2002b. p. 1063–101.
Zaino RJ, Brady MF, Lele SM, et al. Advanced stage mucinous adenocarcinoma of the ovary is both rare and highly lethal. Cancer. 2011;117:554.62.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2016 Springer International Publishing Switzerland
About this chapter
Cite this chapter
Emerson, R.E. (2016). Ovary and Peritoneum. In: Cheng, L., Bostwick, D. (eds) Essentials of Anatomic Pathology. Springer, Cham. https://doi.org/10.1007/978-3-319-23380-2_32
Download citation
DOI: https://doi.org/10.1007/978-3-319-23380-2_32
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-23379-6
Online ISBN: 978-3-319-23380-2
eBook Packages: MedicineMedicine (R0)