
Abstract
Urbanization in the Global South has often been accompanied by growing informal settlements. Because of inadequate infrastructure, lack of services, and sociopolitical marginalization, these settlements emerge as vulnerable to climate change-related extreme weather events—such as flooding. Chad’s urban areas are heavily affected by floods, and the country is exemplary for being subject to water insecurity, all while displaying low levels of responsiveness. In this chapter, we focus on the risk of waterborne disease infections and the importance of adaptive capacity for risk mitigation. In a departure from mainstream adaptation literature and to underline the gendered nature of adaptation, women are at the heart of our analysis. Using nationally representative DHS data from 2014 to 2015, we construct a multidimensional empowerment index, which includes the domains of employment, income, autonomy, leadership, and time. Using regression analysis, we find that empowerment is an important predictor of adaptive behavior as economically empowered women show higher uptake of adaptive strategies to mitigate risks associated with waterborne diseases. Climate responsiveness is higher in urban areas where women are more empowered. We conclude that an approach to adaptation that encompasses gender-sensitive policy responses that empower women is particularly promising to reduce vulnerability to climate shocks in urban areas.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
1 Introduction
Water insecurity is one of the key risks associated with climate change and can result from changes in the water cycle, water quality, and cryosphere as well as from drought and flood negatively impacting natural and human systems (IPCC, 2022). As climate change exacerbates the frequency and severity of heavy rainfall, cities, river plains, and deltas experience more disruptive flooding, which along with the destruction of property, infrastructure, and services facilitates the spread of waterborne and water-related diseases (Ahmed et al., 2022; Douglas et al., 2008; Few et al., 2004; Levy et al., 2016; Sajid & Bevis, 2021; Semenza, 2020; WHO & WMO, 2012). Direct flood damage is projected to increase globally by four to five times at 4°C compared to 1.5°C (IPCC, 2022). Flooding affects populations by washing away homes and destroying food and stocks of goods in markets as well as livestock and cultivated land. During floods, wells—often the only water source—and latrines can be destroyed (ReliefWeb & UN OCHA, 2022) giving rise to water contamination and forcing households to resort to unsafe floodwaters for daily use. A significant increase in ill health and premature deaths from climate-sensitive diseases and conditions is projected. Between 20,000 and 30,000 additional diarrheal deaths in children are also expected by mid-century under 1.5–2.1°C global warming, with West Africa most affected, followed by East, Central, and Southern Africa (WHO, 2014). Morbidity from cholera is also projected to increase as is E. coli (IPCC, 2022). Intersecting inequalities and context-specific factors such as culture, gender, religion, ability, and disability or ethnicity mean that risks vary at a fine scale across and within communities and societies (IPCC, 2022). While rural areas are also affected, urban areas tend to be more prone to flooding and further subject to climate risks.
Chad, like other countries in the Sahel region, is already experiencing the effects of climate change in the form of increased temperatures and precipitation. The country is subject to a projected increase in heavy rainfall events expected to increase exposure to pluvial and riverine flooding and their related impacts. Chad is exemplary in terms of being subject to various water insecurity-related stresses and shocks and displaying high levels of vulnerability and low levels of responsiveness. The Sahel’s drylands do not readily absorb water, and they are more prone to quick and heavy flooding (Elagib et al., 2021; UN OCHA, 2020). Chad ranks third from last in the Notre Dame Global Adaptation Initiative (ND-GAIN, 2022) vulnerability ranking, meaning that the country experiences one of the highest levels of climate vulnerability globally in terms of the susceptibility to be adversely affected by climate-driven hazards.Footnote 1,Footnote 2 The country also ranks third from last in ND-GAIN’s adaptation readiness index meaning that its governance structures and policy processes ensuring that adaptation takes place are weak or nonexistent (Ford & King, 2015). In 2020, 20 out of Chad’s 23 provinces were affected by water insecurity with a higher incidence in the southern and central ones and more than 64,000 households suffered flood damage or were displaced, and in some regions, increased childhood diarrheal disease was observed during extreme weather events (UN OCHA, 2020). Urban areas, in particular, such as the capital N’Djamena are at risk of being severely impacted (UN OCHA, 2022).
In the absence of the required hard and soft infrastructures, negative effects of climate change, such as increasing care responsibilities, workloads, and limited access to resources, oftentimes affect women disproportionately. Thus, addressing the adaptive capacities, specifically of women, when discussing and planning for climate change in Chad is a necessity. In addition, urban population growth has been accompanied by an increase of vast informal settlements, due to failing housing systems and lack of investment capacity (Dodman et al., 2018; Revi et al., 2014). These informal settlements are vulnerable to flooding due to inadequate infrastructure, general lack of services, and sociopolitical marginalization putting them at high risk from extreme weather events (Haque, 2021; Revi et al., 2014). Thus, this chapter argues that it is all the more important to assess and mobilize the adaptive capacity of the population, women in this case, as well as its drivers especially those in the most vulnerable and exposed regions. Respectively, this research focuses on how adaptable women are in urban Chad and what strategies they employ and the resources they require to mitigate the risk of water insecurity. This chapter aims to pave the way for improved planning and policymaking processes that support the adaptive capacities of women in urban areas of developing countries.
We take adaptive capacity as complementary to readiness and define it as “the potential for actors within a system to respond to changes, and to create changes in that system” (Chapin et al., 2006). Adaptive capacity of individuals, households, and communities is thought to reduce the impact of climate change (van Valkengoed & Steg, 2019; Wouterse et al., 2022). Examples of individual and household-level adaptive capacity are risk mitigation (vaccinating, using emergency and health kits, using nutritional supplements, treating water) and risk management strategies such as purchasing (health) insurance (van Valkengoed & Steg, 2019). While most adaptation efforts have been focused on reducing risk, focusing on increased agency and adaptive capacities of actors to reduce vulnerabilities is urgent, given the low level of adaptation readiness of Chad.
Empowerment refers to agency or the ability to pursue relevant goals and the institutional environment enabling people to exercise this agency successfully (Butler et al., 2015). So far, the concept of empowerment has received little empirical attention within adaptation research where the focus has been more on the role of education (see, e.g., Feinstein & Mach, 2020; Lutz et al., 2014). Most existing empirical studies focus on the role of empowerment in relation to agricultural production, poverty reduction, or food and nutrition security (see, e.g., Malapit & Quisumbing, 2015; Wouterse, 2019). This chapter contributes to filling this gap and assesses the role of empowerment in adaptive capacity in the form of the adoption of strategies that mitigate health risks associated with floods. In a departure from mainstream climate adaptation literature and to underline the gendered nature of adaptation policy and practice, our study focuses specifically on women who are often claimed to be more vulnerable to the effects of climate change.
We use the nationally representative Demographic and Health Survey data collected in 2015 and construct a multidimensional economic empowerment index akin to the Women’s Empowerment in Agriculture Index (WEAI) with indicators on control over personal decisions, autonomy, access to income, involvement in decision-making, and time dedicated to leisure activities. We then use regression analysis to reveal the relationship between this index and adaptive capacity in the form of four selected strategies that mitigate the risk of health impacts of floods.Footnote 3 We find that empowerment is an important predictor for the adoption of adaptive health strategies and that empowerment levels of women are significantly lower than those of men both in urban and rural areas. However, climate responsiveness is higher in Chad’s urban areas as they host women who are more empowered in terms of access to resources and autonomy with improved decision-making capacities. Specifically, economically empowered women have higher uptake of adaptive health strategies such as taking up health insurance, treating water before drinking, administering nutritional supplements to children, and vaccinating them, which are likely to mitigate the risk associated with waterborne diseases.
Based on our findings, we call for an integrated approach to climate adaptation, which encompasses gender-sensitive policy and planning responses targeting economic empowerment as means of greater inclusion of women in urban development initiatives in Chad.
2 Climate Change and Water Insecurity in Chad
Chad is a landlocked African country situated in the Sahel, and its climate is overall desertic, with higher precipitation in the southern regions and more arid weather in the north of the country. Rainfall incidence increases during the wet season, which stretches from May to October with July and August as the wettest months. There is a high variability in temperatures (4 to 6 degrees depending on the month) with a general warming trend over the hottest months of the year (+3°C on average between 1970 and 2020 for the months of May to September). In general, it is assumed that if the average annual precipitation varies little, it will be concentrated in more intense rainfall events, and more intense floods followed by prolonged dry periods. Data from the climate change portal of the World Bank confirm a scenario of increased drought episodes, with a decrease in the number of wet days but an increase in volumes per rainy day.Footnote 4 Figures 1 and 2 show some recent climatic trends for the country’s regions.

Number of wet days per year. Source: DHS 2014–2015

Precipitation 1985–2015 (Source: DHS 2014–2015)
N’Djamena, the country’s capital where nearly 17 million people live, is located 100 km from Lake Chad. Lake Chad is a good example of the climate variability affecting the N’Djamena region in relation to climate change. Since the 1970s and 1980s, the Sahel was confronted with a period of severe drought that has significantly affected water resources, including Lake Chad, which is said to have shrunk dramatically. Since the 1990s, there has been an increase in rainfall in the region with a peak in water volume attained in 2013 in Lake Chad (Pham-Duc et al., 2020). N’Djamena is located almost 300 meters above sea level at the intersection of the Chari and Lagone rivers on an alluvial plain where the quality of its soil, made up mainly of clay, silt, and sand, has a low absorption capacity (Fig. 3).

N’Djamena city. Source: the authors
This particular topography causes flooding during the rainy season, which runs roughly from May to October, as exemplified by the recent severe floods of October 2022 (Fig. 4).

Satellite detected water extent as of 30 October 2022. Source: Map by authors showcasing data from the UN Operational Satellite Application Programme (UNOSAT)
During flooding events and in their aftermath, water contamination is frequent and can happen through a variety of mechanisms such as overwhelmed or damaged sewer treatment facilities discharging untreated wastewater into rivers and streams, contaminated floodwater transporting pathogens to drinking water wells and the water distribution system, contamination of irrigation water that pollutes food, damaging of water supply and treatment systems and displacement of population toward areas with inadequate sanitation infrastructure (Semenza, 2020). Contaminated water used for drinking, sanitation, and recreation is associated with the contraction of a number of different viral, bacterial, and parasitic diseases and especially diarrheal disease (Levy et al., 2016). When flooding disrupts sewage systems, people are at increased risk of transmission of gastrointestinal pathogens, particularly E. coli, norovirus, rotavirus, cryptosporidium, giardia, campylobacter, different salmonella enterica serotypes, and hepatitis A. Other diseases such as leptospirosis and tetanus may also occur more frequently (Semenza & Menne, 2009). Large outbreaks of waterborne diseases due to flooding present a severe threat particularly that disproportionally affect more biologically sensitive age groups, such as children and the elderly (Semenza, 2020).
While rural areas can also be affected, urban areas are particularly prone to flooding and concentrate many of the present exacerbating climate risks. In Chad, rapid increase in the population of urban areas also increased the demand for freshwater, which has already put excessive stress on the water and sanitation infrastructure (Howard, 2016; World Bank, 2007).
3 Climate Risk, Vulnerability, and Adaptive Capacity
Climate risk, defined as the probability of hazardous events or trends multiplied by impacts if these occur, is the result of the interaction between exposure, vulnerability, and hazards (IPCC, 2022). According to the IPCC risk framework, exposure is the presence of livelihoods in places and settings that could be adversely affected, whereas vulnerability is the propensity or predisposition to be adversely affected. Hazards, instead, are interpreted as the likelihood of actual climate physical events or trends multiplied by their magnitude (IPCC, 2022).
Vulnerability is a highly complex dimension arising from a wide range of institutional, geographic, environmental, socioeconomic, biological, and other factors, which can vary spatially and temporally. It is also often associated with poverty, as impoverished populations are more reliant on ecosystem services for livelihoods, are more likely to live in environmentally exposed locations such as flood plains or degraded hill slopes, and possess fewer resources to adapt to changing environmental conditions and recover from disasters. Poverty also influences how people perceive the risks to which they are exposed, how they respond to evacuation orders and other emergency warnings, and their ability to evacuate or relocate to a less risk-prone location (US Global Change Research Program, 2016). Poorer households are more likely to be forced into low-agency migration as a means of adapting to climate risks and at the same time are the most likely to be immobile or trapped in deteriorating circumstances where migration would be a preferred response (Fazey et al., 2016; Leichenko & Silva, 2014). However, the poor cannot be addressed as a homogenous group, and so far, studies have failed to sufficiently acknowledge the linkages between climate vulnerability, poverty, and heterogeneity (Dodman et al., 2018; Eriksen & O'Brien, 2007). In an attempt to increase resilience and prepare for the effects of climate change, it is critical to acknowledge and address the distinct experiences and difficulties that many groups, notably women and disadvantaged communities, confront. Thus, vulnerability must also be considered as a gendered dimension.
Women are often claimed to be more vulnerable to the effects of climate change for a number of reasons. For instance, women are said to represent a disproportionate share of the poor and, together with children, are found to be more likely than men to die during disasters. One example is the Asian Tsunami where the largest number of fatalities were said to be women and children under the age of 15. Additionally, it has been documented that women in Bangladesh did not leave their houses during floods due to cultural constraints on female mobility and those who did were largely unable to swim in flood waters. Neumayer and Plümper’s analysis (Neumayer & Plümper, 2007) of a sample of 141 countries between 1981 and 2002 indicated that the adverse impact of disasters on life expectancy of females compared to males is clearly contingent on the extent of socially constructed vulnerability. They show that women died more when they were socioeconomically disadvantaged. An exception to the contention about women’s higher mortality is the case of Hurricane Mitch where more men were said to have died than women. It has been suggested that this was due to existing gender norms, as ideas about masculinity encouraged risky, “heroic” action in disaster situations (Röhr, 2006). It needs to be noted that the empirical evidence base for the feminization of poverty thesis (Arora-Jonsson, 2011; Jackson, 1996) is rather scant. The insistence on women’s universal vulnerability can have an opposite effect, that is, gender is made invisible in the debates on climate change since it is assumed that we know what the problem is—the vulnerability of women (Arora-Jonsson, 2011).
Alongside socioeconomic positionality, biological sensitivity is a determining factor of vulnerability to climate risk. Sensitivity has been associated with developmental stage (e.g., children are at increased mortality risk from diarrheal diseases), pre-existing medical conditions (e.g., diabetics are at increased risk during heat waves), acquired conditions (e.g., malaria immunity), and genetic factors (Balbus & Malina, 2009). Given their immature physiology and metabolism and their high intake of air, food, and water relative to their body weight as compared with adults (US Global Change Research Group, 2016), children often have unique pathways of sensitivity to climate hazards. Hazards are expected to increase childhood risks of malnutrition and infectious disease through their impacts on household food access, dietary diversity, nutrient quality, water, and changes in maternal and childcare access and breastfeeding (FAO, IFAD, UNICEF, WFP,, & WHO, 2018; Perera, 2017; Tirado et al., 2010). Children living in locations with poor sanitation are especially vulnerable to gastrointestinal illnesses, with rates of diarrheal diseases expected to rise under many climate change scenarios (Wang et al., 2022).
Throughout this article, we put vulnerability in conversation with the concept of adaptive capacity, which we outlined in the previous sections. Some of the key attributes of adaptive capacity are thought to be social learning and knowledge exchange, empowerment, and “bridging” social networks that link stakeholders and their resources across administrative levels and spatial scales (Armitage & Plummer, 2010; Smit & Wandel, 2006). Notably, empowerment (especially of women), when integrated with other attributes of adaptive capacity, is considered useful for addressing complex problems (Butler et al., 2015). Empowerment has been interpreted and defined in multiple ways, but generally, it is embedded within agency-structure ontologies and defined as the improved potential for individuals to make changes and decisions in their lives (Alkire et al., 2013; Eyben & Napier-Moore, 2009; Woroniecki et al., 2019). Additionally, empowerment must be understood relationally as it is not just a factor of women’s attainments but also of their equality with respect to men. In this sense, empowerment entails increasing power of the low-power group.
Several studies have suggested that improvements in empowerment have multiplier effects on the three pillars of sustainable development: economic, social, and environmental (Charbit, 2018). Control over household income and education of women have been shown to have direct positive consequences on health of the household and for children’s access to schooling (World Bank, 2012). Using the Women’s Empowerment in Agriculture Index, Malapit and Quisumbing (2015) find for Ghana that women’s empowerment is more strongly associated with the quality of infant and young child feeding practices. Wouterse (2017) finds for Niger that more educated, experienced, and empowered households are more to have put in place zaï pits, an on-farm adaptive production strategy. Seymour (2017) demonstrates for rural Bangladesh that reduced gender disparities within households are associated with higher levels of technical efficiency in agriculture.
While empowerment has been linked to the adoption of adaptive production strategies in agriculture, there is not much literature on the role of empowerment in the adoption of resilience-enhancing strategies in urban settings. This is surprising because, particularly under uncertainty, subjectively defined adaptive strategies become progressively more important in adaptation action. Higher levels of empowerment are expected to positively affect adaptive capacity by increasing the uptake of adaptive strategies to mitigate climate risk. As Fig. 5 shows, the expected result of the adoption of adaptive strategies is lower vulnerability. This means that households are able to maintain their welfare in the face of climate hazards such as extreme flooding.

Conceptual framework. Source: the authors
4 Empowerment and Adaptation
4.1 An Empowerment Index for Adaptation
We draw on data from the Demographic and Health Survey (DHS) for Chad from 2014 to 2015 to assess the relationship between empowerment and household uptake of adaptative strategies that mitigate the risk of children contracting or being severely affected by waterborne diseases. DHS are nationally representative and provide a wide range of data to monitor areas such as health and sanitation of both adults and children in a household, which matches the purpose of this research. Moreover, DHS constitute the largest source of data on women’s participation in decision-making (Calder et al., 2020). The data is georeferenced and collected in both urban and rural areas across all of Chad’s administrative regions, which allows us to assess within-country variation. This is particularly important when analyzing empowerment in connection with location-specific challenges such as climate vulnerability and adaptation. In order to obtain an unbiased estimation and to be able to evaluate the sampling errors, a scientific probability sampling methodology is used in DHS surveys. A probability sample is defined as one in which the units are selected randomly with known and nonzero probabilities. Also, DHS data are available for many countries over multiple years, enabling the replication of this study.Footnote 5
Given the multidimensionality of empowerment, which includes concepts such as control over personal decisions, autonomy, access to income, involvement in decision-making, time poverty, etc. (Alkire et al., 2013; Calder et al., 2020), it is common to resort to an index to measure it. An index is a composite measure that, based on a set of indicators, provides an indication of the empowerment level in a given community, city, or country. An empowerment index can be used to enhance evidence-based policymaking, monitor progress toward gender equality in the context of certain projects and for policy evaluation purposes in many different areas. For our research, we focus on the WEAI, an index that is embedded in a broader household setting and captures both individual and household-level empowerment (Alkire et al., 2013). The WEAI indicators are reflected in the DHS data available for Chad. However, because the WEAI measures empowerment in agriculture and we are interested in the role of empowerment in adaptive health capacity in both urban and rural areas, we have made some adjustments. Our Multidimensional Empowerment Index (MEI) captures the economic and social agency dimensions of empowerment through the combination of five domains—employment, income, autonomy, leadership, and time. This index reflects the extent to which an individual has control of and ability to act upon their own decisions. Each domain features one or more binary indicator (see Table 1), which takes the value of 1 when an individual is considered adequate in a specific empowerment component and 0 when instead the individual is considered inadequate.
The employment domain features one indicator that measures the current employment status of the respondent. Employment is considered a crucial element of economic independence and often used as a partial proxy for empowerment as it provides access to an income based on one’s own work engagement (Greig & Koopman, 2003). However, access to an income without the possibility to control it and choose how to allocate it would mean less independence and reduced agency. Therefore, the second domain, income, considers a respondent to be adequate if he or she has sole or joint control over their own earnings. For the autonomy domain, two indicators are used, each capturing a different aspect of autonomy, which is often taken to mean independent decision-making and freedom of physical mobility (Bloom et al., 2001; Nigatu et al., 2014). We thus select freedom of movement and control over one’s own health and well-being as our indicators. To capture them, we use, respectively, the ability of an individual to leave the house by him or herself and the control over one’s own healthcare decisions. To measure leadership within the household, we use an indicator of control over household purchases. Due to data limitations, leadership outside of the household (e.g., among the community) could not be included in the index. Finally, the time domain captures the availability of free time to read a newspaper or listen to the radio outside of work or household care. Adequacy cutoff scores for all the above indicators are displayed in Table 1.
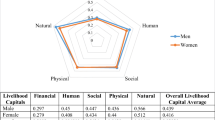
The MEI is computed for both men and women, to capture the relational component of empowerment and compare men’s and women’s scores, but also because we consider empowerment as an increase of agency applicable to both women and men. Figs. 6 and 7 show important differences in empowerment level with women’s total score averaging at 0.25 and men’s total score at 0.48.

Adequacy in empowerment of women and men in Chad. Source DHS 2014–2015

Adequacy in empowerment of women in rural and urban areas. Source: DHS 2014–2015
Fig. 6 shows that women are particularly inadequate in the income, autonomy, time, and leadership domains. To further understand the relevance of urbanization for empowerment, we computed urban and rural average empowerment scores for women.
Fig. 7 shows that adequacy in empowerment of women in urban areas is higher compared to women in rural areas. We see that the former are more adequate mainly because they score higher in terms of adequacy in time.
Fig. 8 shows how empowerment scores are distributed across the country. Wadi Fira, in eastern Chad, displays the lowest average empowerment score, and this is true when looking at overall scores as well as at rural and urban scores. The Wadi Fira region also falls into the higher-risk category of the INFORM subnational risk index (2022).Footnote 6 If we find an association between economic empowerment and adaptive capacity, this could mean that in Wadi Fira, high vulnerability and low empowerment significantly hamper adaptation. In contrast, N’djamena yields the highest average empowerment score. It is important to specify that all data from N’Djamena are collected from urban households as it is a city; therefore, only urban results make up its average empowerment score.

Mean MEI score per region. Source: DHS 2014–2015; the authors
4.2 Linking Empowerment and Adaptive Capacity
To study the relationship between empowerment and adaptive capacity, we select four adaptation strategies undertaken at the individual level (see Table 2), which can contribute to building resilience to infection by waterborne pathogens. We draw on existing adaptation research and the specific risk under examination in order to identify these strategies. Even though not solely pertaining to the adaptation domain, when considered in relation to the risk (contraction of waterborne diseases), these strategies can be judged to enhance specific adaptive capacity. For instance, water and sanitation interventions are widely regarded as the most effective strategies against waterborne infections (Levy et al., 2016). Specifically, water filtration and treatment are effective adaptive measures for diarrheal diseases (Mellor et al., 2016). However, climate change’s impact on waterborne diseases does not solely depend on a system’s ability to respond to a hazard such as flooding but on socio-environmental circumstances that increase pathogen exposure (e.g., lack of sanitation facilities, proximity to riverbanks, presence of haphazard urbanization) and, importantly, on individual susceptibility (e.g., malnourishment or absence of vaccination) (IPCC, 2022; Levy et al., 2016). The provision of nutritional supplements (Vitamin A) to children and child vaccination (BCG and/or DTP) are therefore also selected as adaptive health strategies. Footnote 7 It is important to note that the surveyed individuals for the latter two adaptation markers are mothers and that only the observations for the firstborn child are used. Footnote 8 Table 2 shows the incidence of the different strategies as well as differences between urban and rural households.
Given that urban areas are overall more vulnerable to flooding and often the hardest hit, higher levels of empowerment could represent a constructive element if empowerment is found to positively affect adaptive capacity. A simple pairwise correlation between women’s empowerment scores in urban and rural areas and the four adaptive strategies to mitigate the risk of waterborne disease infection is performed in order to understand the last hypothesis in more depth. Table 3 shows strong correlations between women’s empowerment and the four adaptive strategies: the uptake of personal health insurance, administering vitamin A to the firstborn, vaccination against BCG and/or DTP, and water treatment before use. These positive correlations suggest that more empowerment is associated with an increase in adaptive capacity through the uptake of individual strategies. A stronger correlation with health insurance in urban areas and with vitamin A supplements and vaccinations in rural areas is found when urban and rural women’s empowerment was looked at separately.
We use regression analysis to obtain a clearer understanding of the effect of empowerment on adaptive capacity. In addition to the empowerment index, human capital variables of the respondent and of the household head, asset ownership variables, and an indicator for the location of the respondent (either urban or rural) are included within the analysis as well as climate variables. A system of equations is specified as follows:
In Eq. 1, the probability of the household being covered by health insurance (pi) is explained by our variable of interest MEI, a vector of individual and household characteristics; M, age and education, a vector of household assets; A, ownership of land or of a home, a vector of household-level geographical variables (G), including a binary variable, which takes the value of 1 is the household is located in an urban area and 0 if not and a vector of climate variables, R. Similarly, in Eqs. 2, 3, and 4, the dependent variables are, respectively, the probability of the administration of nutritional supplements to the firstborn, the probability of water treatment, and the probability that the firstborn is vaccinated against BCG and/or DTP. The system of Eqs. 1–4 is estimated as a seemingly unrelated probit regression with regional fixed effects and clustered standard errors.
5 Results
Regression results for determinants of the uptake of the various adaptation strategies are given in Table 4. A positive significant relation between empowerment, uptake of health insurance, water treatment, and the decision to vaccinate the firstborn child is observed. The latter result is similar to that of Wendt et al. (2022) who finds for low- and middle-income countries that children of more empowered women are less likely to be left out of complete vaccination cycles and that women’s intrinsic agency is a strong determinant of child vaccination. Contrary to expectations, see, for example, Santoso et al. (2019), no statistically significant relationship is observed between empowerment and administration of vitamin A supplements. Instead, education seems to be a better predictor here. In addition to empowerment, education is a strong determinant of the uptake of all four adaptive health strategies. The average formal education level of women in our sample is less than 2 years against almost 4 years for men. The sex of the household head also plays an important role in the administration of vitamin A as well as in vaccination decisions, which are both more likely in households headed by a male. In terms of assets, land ownership is positively correlated with the uptake of health insurance. Location—urban or rural—explains the uptake of the four adaptive health strategies but not in the same direction. Women in urban areas are more likely to have taken up health insurance, administered vitamin A to their firstborn, and treated their water before drinking and to have vaccinated their firstborn against BCG and/or DTP. Our climatic variables, the z-scores for the number of wet days in 2015 as well as the z-score for 2015 rainfall are, respectively, negatively and positively associated with uptake of health insurance. The z-score for the number of wet days in 2015 is also negatively associated with vaccinations.
To further unpack the location effect, some interaction terms are introduced. Results are given in Table 5. Indirect effects suggest that there is significant complimentary role of location in the uptake of health insurance. Women in urban locations who are more empowered and more educated are more likely to have taken up health insurance. For the administration of vitamin A, there is no complimentary location effect, and more educated women in either location are more likely to administer vitamin A to their firstborn. Similarly, for water treatment, there is no complimentary effect of location with respect to education and empowerment, while education remains strongly significant. Lastly, a trade-off between empowerment and location was noted for vaccinations, where women who were more empowered were less likely to vaccinate their firstborn when in an urban setting. The direct effects of empowerment and education on vaccination remain strongly significant.
6 Conclusion and Policy Implications
Water insecurity is one of the key risks associated with climate change and can manifest with the spread of waterborne diseases during flooding events. Chad is subject to a multiplicity of water insecurity-related stresses and shocks, including flooding, but levels of responsiveness have remained low. Urban areas in Chad are particularly affected by flooding, while the lack of services in and marginalization of informal urban settlements make them especially vulnerable to water insecurity. Various adaptive strategies can be adopted to mitigate the risk of waterborne diseases: health insurance uptake, provision of nutritional supplements, water treatment, and child vaccination. But so far, it has not yet been understood what the drivers of the uptake of these strategies are. In particular, the role of empowerment has remained relatively under analyzed although it has been identified as a critical element of adaptive capacity.
In this chapter, we used the 2014–2015 DHS data to formulate an empowerment index based on adequacy in the employment, income, autonomy, leadership, and time domains and assess the role of empowerment in relation to the uptake of four adaptive health strategies that could mitigate the risk of waterborne diseases, which are particularly prevalent during flooding. Empowerment scores indicate that there is a significant gap between men and women in both rural and urban areas. In particular, women are found to be less adequate compared to men in terms of employment, autonomy, and leadership. Women in urban areas are more empowered compared to women in rural areas, in particular because they are more adequate in the time domain.
Our regression results for the adoption of the four adaptive strategies demonstrate the role of women’s empowerment in the uptake of various adaptive health strategies. More empowered women are more likely to have taken up health insurance, to treat their water before drinking, and to vaccinate their firstborn. This means that, when women are more empowered, they themselves as well as their children are less at risk of water insecurity. Interaction effects reveal that there are important differences between urban and rural areas where there is a positive indirect effect of empowerment and an urban location on insurance uptake but a negative indirect effect of empowerment and an urban location on vaccination.
While adaptive capacity remains strongly associated with the level of education, the important role of empowerment opens up a window for understanding and planning interventions that enhance empowerment. As women are particularly inadequate compared to men in the domains of leadership, autonomy, and employment, various channels for strengthening empowerment can be explored. For instance, creating employment opportunities for women could be a particularly promising strategy. To help households adapt and mitigate the risk of water insecurity, local and central government authorities, nongovernmental organizations, and external funding and/or implementing agencies could adopt policies and collaborate with local institutions to create jobs and build skills.
Finally, the higher levels of empowerment and adaptive capacity found in urban areas, which tend to be more heavily affected by flooding and the related spread of waterborne disease, constitute a promising finding. An understanding of the specific impact pathways for enhanced adaptive capacity would offer opportunities to design interventions that can be scaled. Further research on the topic should also include dedicated data collection in urban and rural areas to understand different trends and needs. An expansion of our research through an analysis with georeferenced climate vulnerability data (flooding, extreme temperature, extreme precipitation) as well as additional waves of nationally representative household-level data presents an important next step.
Notes
- 1.
The ND-GAIN Country Index, as developed by the researchers of the Notre Dame Global Adaptation Initiative, encapsulated a country’s vulnerability to climate change and other planetary challenges with respect to its adaptive capacity.
- 2.
Chad | ND-GAIN Index
- 3.
WEAI is the first comprehensive measure to assess women’s empowerment and participation in agriculture. As initiated by International Food Policy Research Institute (IFPRI), Oxford Poverty and Human Development Initiative (OPHI), and USAID’s Feed the Future in 2012, it not only measures the levels of empowerment of women within the agricultural sector but also their relative position to men within the household.
- 4.
- 5.
Two components of the DHS are used for this study: the individual women’s survey, which contains data on 17,719 women (as well as data for up to six children under the age of 5) of which 4285 live in urban areas and 13,434 in rural ones; and the individual men’s survey, which contains data on 5248 men for all surveyed women.
- 6.
INFORM is a composite multidimensional risk index for disasters and humanitarian crises developed by the Joint Research Center of the European Commission. It measures domains such as hazard and exposure, vulnerability, and lack of coping capacity and is available both at the national and subnational levels.
- 7.
(Bacille Calmette–Guerin primarily against tuberculosis and Diphtheria, Tetanus, and Pertussis).
- 8.
The decision to only use data for one child rather than for several was driven by a lack of comprehensive information for subsequent children in the dataset, which would have significantly reduced our sample and returned an incomplete picture. We are aware of the limitations this might generate, namely because of the existing gender bias in decisions over health expenditures and care (Khera et al., 2014), which relates to higher observed health expenditure and care for boys.
References
Ahmed, T., Faridullah, & Kanwal, R. (2022). Infectious diseases, challenges, and their impacts on human health under changing climate. In T. Ahmed & M. Z. Hashmi (Eds.), Hazardous environmental micro-pollutants, health impacts and allied treatment technologies (pp. 21–36). Springer International Publishing. https://doi.org/10.1007/978-3-030-96523-5_2
Alkire, S., Meinzen-Dick, R., Peterman, A., Quisumbing, A., Seymour, G., & Vaz, A. (2013). The Women’s empowerment in agriculture index. World Development, 52, 71–91.
Armitage, D. R., & Plummer, R. (2010). Adaptive capacity and environmental governance. Springer.
Arora-Jonsson, S. (2011). Virtue and vulnerability: Discourses on women, gender and climate change. Global Environmental Change, 21(2), 744–751.
Balbus, J. M., & Malina, C. (2009). Identifying vulnerable subpopulations for climate change health effects in the United States. Journal of Occupational and Environmental Medicine, 51(1), 33–37.
Bloom, S. S., Wypij, D., & Gupta, M. D. (2001). Dimensions of women’s autonomy and the influence on maternal health care utilization in a North Indian City. Demography, 38(1), 67–78.
Butler, J. R. A., Wise, R. M., Skewes, T. D., Bohensky, E. L., Peterson, N., Suadnya, W., Yanuartati, Y., Handayani, T., Habibi, P., Puspadi, K., Bou, N., Vaghelo, D., & Rochester, W. (2015). Integrating top-down and bottom-up adaptation planning to build adaptive capacity: A structured learning approach. Coastal Management, 43(4), 346–364. https://doi.org/10.1080/08920753.2015.1046802
Calder, R., Rickard, S., & Kalsi, K. (2020). Measurement of women’s economic empowerment (WOW Guidance Note No. 2). WOW Helpdesk.
Chapin, F. S., Lovecraft, A. L., Zavaleta, E. S., Nelson, J., Robards, M. D., Kofinas, G. P., Trainor, S. F., Peterson, G. D., Huntingdon, H. P., & Naylor, R. L. (2006). Policy strategies to address sustainability of Alaskan boreal forests in response to a directionally changing climate. Proceedings of the National Academy of Sciences of the United States of America, 103, 1663716643.
Charbit, Y. (2018). Women as actors in addressing climate change. In N. Riley & J. Brunson (Eds.), International handbook on gender and demographic processes. International handbooks of population (Vol. 8). Springer. https://doi.org/10.1007/978-94-024-1290-1_21
Dodman, D., Archer, D., & Mayr, M. (2018). Addressing the most vulnerable first – Pro-poor climate action in informal settlements. UN-HABITAT. https://apo.org.au/node/219601
Douglas, I., Alam, K., Maghenda, M., Mcdonnell, Y., Mclean, L., & Campbell, J. (2008). Unjust waters: Climate change, flooding and the urban poor in Africa. Environment and Urbanization, 20(1), 187–205.
Elagib, N. A., Zayed, I. S. A., Saad, S. A. G., Mahmood, M. I., Basheer, M., & Fink, A. H. (2021). Debilitating floods in the Sahel are becoming frequent. Journal of Hydrology, 599, 126362. https://doi.org/10.1016/j.jhydrol.2021.126362
Eriksen, S. H., & O’Brien, K. (2007). Vulnerability, poverty and the need for sustainable adaptation measures. Climate Policy, 7(4), 337–352. https://doi.org/10.1080/14693062.2007.9685660
Eyben, R., & Napier-Moore, R. (2009). Choosing words with care? Shifting meanings of women’s empowerment in international development. Third World Quarterly, 30(2), 285–300. https://doi.org/10.1080/01436590802681066
FAO, IFAD, UNICEF, WFP, & WHO. (2018). The state of food security and nutrition in the world 2018: Building climate resilience for food security and nutrition. FAO. http://www.fao.org/3/I9553EN/i9553en.pdf
Fazey, I., Wise, R. M., Lyon, C., Câmpeanu, C., Moug, P., & Davies, T. E. (2016). Past and future adaptation pathways. Climate and Development, 8(1), 26–44. https://doi.org/10.1080/17565529.2014.989192
Feinstein, N. W., & Mach, K. J. (2020). Three roles for education in climate change adaptation. Climate Policy, 20(3), 317–322.
Few, R., Ahern, M., Matthies, F., & Kovats, S. (2004). Floods, health and climate change: A strategic review. (Working Paper No. 63). Tyndall Centre for Climate Change Research.
Ford, J. D., & King, D. (2015). A framework for examining adaptation readiness. Mitigation and Adaptation Strategies for Global Change, 20(4), 505–526.
Greig, F. E., & Koopman, C. (2003). Multilevel analysis of Women’s empowerment and HIV prevention: Quantitative survey results from a preliminary study in Botswana. AIDS and Behavior, 7, 195–208. https://doi.org/10.1023/A:1023954526639
Haque, A. N. (2021). Climate risk responses and the urban poor in the global south: The case of Dhaka’s flood risk in the low-income settlements. International Journal of Disaster Risk Reduction, 64, 102534. https://doi.org/10.1016/j.ijdrr.2021.102534
Howard, T. (2016). Failed states and the origins of violence. Routledge.
IPCC. (2022). In H.-O. Pörtner, D. C. Roberts, M. Tignor, E. S. Poloczanska, K. Mintenbeck, A. Alegría, M. Craig, S. Langsdorf, S. Löschke, V. Möller, A. Okem, & B. Rama (Eds.), Climate Change 2022: Impacts, Adaptation, and Vulnerability. Contribution of Working Group II to the Sixth Assessment Report of the Intergovernmental Panel on Climate Change (p. 3056). Cambridge University Press. https://doi.org/10.1017/9781009325844
Jackson, C. (1996). Rescuing gender from the poverty trap. World Development, 24(3), 489–504.
Khera, R., Jain, S., Lodha, R., & Ramakrishnan, S. (2014). Gender bias in child care and child health: Global patterns. Archives of Disease in Childhood, 99(4), 369–374. https://doi.org/10.1136/archdischild-2013-303889
Leichenko, R., & Silva, J. A. (2014). Climate change and poverty: Vulnerability, impacts, and alleviation strategies. Wiley Interdisciplinary Reviews: Climate Change, 5(4), 539–556. https://doi.org/10.1002/wcc.287
Levy, K., Woster, A. P., Goldstein, R. S., & Carlton, E. J. (2016). Untangling the impacts of climate change on waterborne diseases: A systematic review of relationships between diarrheal diseases and temperature, rainfall, flooding, and drought. Environmental Science & Technology, 50(10), 4905–4922. https://doi.org/10.1021/acs.est.5b06186
Lutz, W., Muttarak, R., & Striessnig, E. (2014). Universal education is key to enhanced climate adaptation. Science, 346(6213), 1061–1062.
Malapit, H. J. L., & Quisumbing, A. R. (2015). What dimensions of women’s empowerment in agriculture matter for nutrition in Ghana? Food Policy, 52, 54–63. https://doi.org/10.1016/j.foodpol.2015.02.003
Mellor, J. E., Levy, K., Zimmerman, J., Elliott, M., Bartram, J., Carlton, E., et al. (2016). Planning for climate change: The need for mechanistic systems-based approaches to study climate change impacts on diarrheal diseases. The Science of the Total Environment., 548–549, 82–90. https://doi.org/10.1016/j.scitotenv.2015.12.087
Neumayer, E., & Plümper, T. (2007). The gendered nature of natural disasters: The impact of catastrophic events on the gender gap in life expectancy, 1981–2002. Annals of the Association of American Geographers, 97(3), 551–566. https://doi.org/10.1111/j.1467-8306.2007.00563.x
Nigatu, D., Gebremariam, A., Abera, M., Setegn, T., & Deribe, K. (2014). Factors associated with women’s autonomy regarding maternal and child health care utilization in Bale Zone: A community based cross-sectional study. BMC Women’s Health, 14(1), 79. https://doi.org/10.1186/1472-6874-14-79
Notre Dame Global Adaptation Initiative (ND-GAIN). (2022). ND-GAIN country index, n.d. https://gain-new.crc.nd.edu/
Perera, F. P. (2017). Multiple threats to child health from fossil fuel combustion: Impacts of air pollution and climate change. Environmental Health Perspectives, 125(2), 141–148. https://doi.org/10.1289/ehp299
Pham-Duc, B., Sylvestre, F., Frappart, F., Bouchez, C., & Créteau, J. F. (2020). The Lake Chad hydrology under current climate change. Scientific Reports: Nature Research, 10, 5489.
ReliefWeb & UN OCHA. (2022, July 6). Chad: Floods - June 2021. ReliefWeb. https://reliefweb.int/disaster/fl-2021- 000084-tcd#overview
Revi, A., Satterthwaite, D. E., Aragón-Durand, F., Corfee-Morlot, J., Kiunsi, R. B. R., Pelling, M., Roberts, D. C., & Solecki, W. (2014). In C. B. Field, V. R. Barros, D. J. Dokken, K. J. Mach, M. D. Mastrandrea, T. E. Bilir, M. Chatterjee, K. L. Ebi, Y. O. Estrada, R. C. Genova, B. Girma, E. S. Kissel, A. N. Levy, S. MacCracken, P. R. Mastrandrea, & L. L. White (Eds.), Urban areas. In: Climate Change 2014: Impacts, Adaptation, and Vulnerability. Part A: Global and Sectoral Aspects. Contribution of Working Group II to the Fifth Assessment Report of the Intergovernmental Panel on Climate Change (pp. 535–612). Cambridge University Press.
Röhr, U. (2006). Gender and Climate Change. Tiempo: A Bulletin on Climate and Development.. http://www.tiempocyberclimate.org
Sajid, O., & Bevis, L. E. M. (2021). Flooding and child health: Evidence from Pakistan. World Development, 146, 105477. https://doi.org/10.1016/j.worlddev.2021.105477
Santoso, M. V., Kerr, R. B., Hoddinott, J., Garigipati, P., Olmos, S., & Young, S. L. (2019). Role of women’s empowerment in child nutrition outcomes: A systematic review. Advances in Nutrition, 10(6), 1138–1151.
Semenza, J. C. (2020). Climate change: An enduring challenge for vector-borne disease prevention and control. Nature Immunology, 21(5), 479–483. https://doi.org/10.1038/s41590-020-0648-y
Semenza, J. C., & Menne, B. (2009). Climate change and infectious diseases in Europe. The Lancet Infectious Diseases, 9(6), 365–375.
Seymour, G. (2017). Women’s empowerment in agriculture: Implications for technical efficiency in rural Bangladesh. Agricultural Economics, 48(4), 513–522.
Smit, B., & Wandel, J. (2006). Adaptation, adaptive capacity and vulnerability. Global Environmental Change, 16(3), 282–292.
Tirado, M. C., Clarke, R., Jaykus, L. A., McQuatters-Gollop, A., & Frank, J. M. (2010). Climate change and food safety: A review. Food Research International, 43(7), 1745–1765. https://doi.org/10.1016/j.foodres.2010.07.003
UN OCHA. (2020, 10 November). Situation Report - Nearly 400,000 people affected by the floods in Chad. https://reports.unocha.org/en/country/chad/card/4N6LzoDRhD/
UN OCHA. INFORM (Index for Risk Management) (2022) Chad, Inform Risk Profile. https://reliefweb.int/map/chad/chad-inform-risk-profile-2022-30-september-2022
US Global Change Research Program. (2016). In A. Crimmins, J. Balbus, J. L. Gamble, C. B. Beard, J. E. Bell, D. Dodgen, R. J. Eisen, N. Fann, M. D. Hawkins, S. C. Herring, L. Jantarasami, D. M. Mills, S. Saha, M. C. Sarofim, J. Trtanj, & L. Ziska (Eds.), The impacts of climate change on human health in the United States: A scientific assessment. US Global Change Research Program.
van Valkengoed, A. M., & Steg, L. (2019). Meta-analyses of factors motivating climate change adaptation behaviour. Nature Climate Change, 9(2), 158–163. https://doi.org/10.1038/s41558-018-0371-y
Wang, P., Asare, E., Pitzer, V. E., et al. (2022). Associations between long-term drought and diarrhea among children under five in low- and middle-income countries. Nature Communications, 13, 3661. https://doi.org/10.1038/s41467-022-31291-7
Wendt, A., Santos, T. M., Cata-Preta, B. O., Costa, J. C., Mengistu, T., Hogan, D. R., Victora, C. G., & Barros, A. J. D. (2022). Children of more empowered women are less likely to be left without vaccination in low- and middle-income countries: A global analysis of 50 DHS surveys. Journal of Global Health, 12, 04022. https://doi.org/10.7189/jogh.12.04022
World Health Organization (WHO). (2014). The country cooperation strategy brief – chad. WHO. https://apps.who.int/iris/bitstream/handle/10665/137148/ccsbrief_tcd_en.pdf;jsessionid=B1A91B8F9B3E4C45141A61F371C47602?sequence=1
World Health Organization (WHO) and World Meteorological Organization (WMO). (2012). Atlas of Health and Climate. WMO No. 1098 (p. 64). WHO Press.
World Bank. (2007). Chad - urban development project (English). World Bank Group. http://documents.worldbank.org/curated/en/149591468214211494/Chad-Urban-Development-Project
World Bank. (2012). World development report on gender equality and development. World Bank.
Woroniecki, S., Wamsler, C., & Boyd, E. (2019). The promises and pitfalls of ecosystem-based adaptation to climate change as a vehicle for social empowerment. Ecology and Society, 24(2) https://www.jstor.org/stable/26796957
Wouterse, F. (2017). Empowerment, climate change adaptation, and agricultural production: Evidence from Niger. Climatic Change, 145(3–4), 367–382. https://doi.org/10.1007/s10584-017-2096-8
Wouterse, F. (2019). The role of empowerment in agricultural production: Evidence from rural households in Niger. The Journal of Development Studies, 55(4), 565–580. https://doi.org/10.1080/00220388.2017.1408797
Wouterse, F., Andrijevic, M., & Schaeffer, M. (2022). The microeconomics of adaptation: Evidence from smallholders in Ethiopia and Niger. World Development, 154, 105884. https://doi.org/10.1016/j.worlddev.2022.105884
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Annex
Annex
Rights and permissions
Copyright information
© 2023 The Author(s), under exclusive license to Springer Nature Switzerland AG
About this chapter

Cite this chapter
Lazzati, S., Tuçaltan, G., Wouterse, F. (2023). Empowerment and Adaptive Capacity of Women in Urban Areas: Mitigating the Risk of Water Insecurity in Chad. In: Čamprag, N., Uğur, L., Suri, A. (eds) Rethinking Urban Transformations. Diversity and Inclusion Research. Springer, Cham. https://doi.org/10.1007/978-3-031-37224-7_11
Download citation
DOI: https://doi.org/10.1007/978-3-031-37224-7_11
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-031-37223-0
Online ISBN: 978-3-031-37224-7
eBook Packages: Economics and FinanceEconomics and Finance (R0)