
Abstract
Ligamentous ankle injuries are one of the most common injuries regardless of athletic level. Lateral ankle sprains (LAS) are more common, although medial ankle sprains (MAS) have occurred more frequently than expected during the past decade. LAS typically occur from excessive inversion and internal rotation of the foot while the opposite is true for MAS. Both injuries may present with significant pain, swelling, decreased range-of-motion, and inability to bear weight. They are diagnosed with special physical examination maneuvers and imaging studies such as plain radiography to rule out associated fractures or magnetic resonance imaging to identify the extent of ligamentous injury. While most ankle sprains resolve without sequelae, recurrent sprains and subsequent chronic ankle instability with significant functional impairment may develop in some individuals despite adequate nonoperative management. In these cases, operative management is warranted. Here, we provide a general review and discuss management of ligament injuries about the ankle.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
1 Lateral Ankle Injuries (Lateral Ankle Sprain and Chronic Ankle Instability)
1.1 General
1.1.1 Epidemiology
Lateral ankle sprains (LAS) are one of the most common orthopedic injuries encountered with 2 million acute ankle sprains occurring per year in the United States [1]. Ankle injuries can encompass up to 30–50% of all athletic injuries [2]. The sports with the highest reporting of these injuries include basketball, soccer, volleyball, and gymnastics, with injury rates of 1.1 to 1.3/1000 athlete-exposure. The sports with the lowest reporting of these injuries include baseball, softball, and ice hockey at an injury rate of 0.23–0.32/1000 athlete-exposure [3]. The true incidence may be even higher since more than 50% of athletes with ankle sprains do not seek medical treatment [4].
There is conflicting evidence as to whether females are more prone to these injuries than males [3, 5]. Some authors have shown that the risk of ankle sprain is slightly higher for women than men while others show there is no difference [6, 7]. Eighty percent of ankle sprains occur to the lateral ankle [8]. Those ages of 15 and 19 years carry the greatest incidence for ankle sprains at 7.2 per 1000 person-years and over half of all ankle sprains occur in those 10–24 years old [1]. Ankle sprains constitute 7–10% of all admissions to hospital emergency departments and carry a high socioeconomic burden [2, 9]. Annual healthcare costs of acute ankle sprain treatment reach up to $2 billion [1].
1.1.2 Risk Factors
Many studies have investigated risk factors for LAS. These include age, gender, weight, height, body mass index, limb dominance, patient’s anatomy (foot type, foot, and ankle alignment, including foot hyper-pronation), laxity (generalized joint laxity, ankle-joint laxity), ankle and first metatarsophalangeal range-of-motion (ROM), muscle strength, muscle-reaction time, balance and proprioception, and previous history of ankle sprain. Other reported risk factors have included sport-related considerations (including type of sport and level of competition, playing on artificial grass, and playing position), type of sport shoe, lack of warm-up stretching, and landing technique after a jump [2, 10]. Previous history of LAS, high body mass index, ankle joint laxity, and impaired balance are the most important risk factors for sustaining ankle injuries [2].
1.1.3 Anatomy
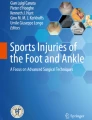
The lateral ankle ligament complex consists of three ligaments: the anterior talofibular ligament (ATFL), the calcaneofibular ligament (CFL), and the posterior talofibular ligament (PTFL) [5] (Fig. 1). The ATFL functions to restrict both internal rotation and adduction while the ankle is plantar flexed. The CFL prevents adduction and inversion of the calcaneus while the ankle is dorsiflexed [11]. The PTFL functions to limit external rotation [11].

Image depicting the lateral ligaments of the ankle
In most cases, the ATFL is the first or only ligament affected. Broström found that combined ruptures of the ATFL and the CFL occurred in 20% of cases and that an isolated rupture of the CFL was very rare [2, 12]. The PTFL is usually not injured in an inversion injury of the ankle because its maximal load to failure is three times that of the ATFL and this ligament is lax when the ankle is plantar flexed [5]. Typically, only gross dislocation of the ankle joint will result in PTFL failure, and it is not seen with ankle sprain injuries.
1.1.4 Mechanism of Injury
Lateral ankle sprains occur from excessive inversion and internal rotation of the hindfoot while the leg is held in external rotation [5, 11]. This happens with a plantar-flexed foot that is placed into supination and adduction (inversion) often seen when landing from a jump or turning during activities [5]. A LAS may also occur with or without contact ranging from impact sports or simple tripping event [3].
The order of injury is typically the lateral joint capsule tearing first, followed by rupture of the ATFL. After complete tear of the ATFL, the CFL fibers are disrupted, followed by a variable injury to the PTFL, and, with increasing force, the deltoid ligament [13]. The injury itself can range from a stretch of the ligaments to a partial or complete tear.
1.1.5 Outcomes
Up to 50% of patients with LAS exhibit residual symptoms and recurrence [2]. In a study, following patients for an average of 6.5 years after LAS found that 17–22% of these patients complained of pain, 26–33% of patients demonstrated persistent swelling, and 35–48% of patients reported an unstable feeling. Moreover, among patients with tenderness in the ATFL during the acute phase of the injury, 32% showed tenderness at the same point 7 years post-injury. In athletes with LAS, who were followed for an average of 6.5 years, 4% had to stop their sport activities due to residual symptoms. Similarly, among nonathletes with ankle sprain, 6% were not able to continue their previous occupation and 15% required external support to continue their original occupation [14]. In another study, previously injured young athletes were followed for 3–15 years and, unfortunately, had more pain and symptoms, poorer self-reported function, ankle-related quality of life, reduced sport participation, balance, and greater fear of pain than those who never sustained an ankle sprain [15].
Recurrent ankle sprains can lead to chronic lateral ankle instability (CLAI) and to significant functional impairment. This can result in a variety of sequelae including an osteochondral injury, chronic pain, and/or a peroneal tendon injury. Accurate assessment and appropriate initial management of the acute ankle sprain may prevent the development of CLAI. However, CLAI may still develop in up to 30% of patients despite adequate nonoperative management [16].
The CLAI may be due to functional and/or mechanical instability and, with repetitive ankle sprains, decreases ankle function and athletic performance. Functional instability is defined by proprioceptive and strength deficits, changes in neuromuscular control, and impaired postural control. It has long been reported that there is an association between muscle weakness and CLAI [16]. In the individual with an ankle sprain, peroneus longus activity decreased in the stance phase during gait, and tibialis anterior activity is increased to compensate.
The normal function of the peroneus longus and soleus, which contribute to landing during jumping activities, are significantly decreased in CLAI patients. Although a recent meta-analysis suggested that concentric eversion strength is decreased in CLAI, there is not yet a consensus regarding the results of inversion and plantar flexion strength [3]. Mechanical ankle instability is defined by laxity of the ankle joint, due to structural damage to any of the three lateral ankle ligaments [11]. In these patients, tibiotalar anterior translation and internal rotation on the injured side were increased compared to the healthy ankle [3].
1.2 Physical Evaluations and Classification
The gold standard for the diagnosis of LAS remains the delayed physical examination (4–5 days post-trauma). Because of the diffuse location of the pain and swelling within 48 h, the examiner may not be able to differentiate hematoma from edema, and stress maneuvers become less reliable [5]. Physical findings for LAS include tenderness to palpation, hematoma, hemarthrosis, and anterior drawer test (ADT). On physical exam, the patient should be sitting or supine, with both ankles exposed. The uninjured ankle should be examined initially to determine what the patient’s baseline exam is. When examining the injured ankle, a thorough exam is necessary.
On inspection, note should be taken on where the patient has swelling and if there is any hematoma or discoloration. On palpation it is important to take note of the particular locations that are tender. ROM may be difficult to assess due to pain. Neurovascular status should be evaluated as with any injury examination. Although tenderness alone may have low specificity, a combination of tenderness, hematoma discoloration, and ADT in the subacute phase (5 days after injury) demonstrate a sensitivity of 96% and a specificity of 84% [17]. Only 14% of individuals without all these findings have a lateral ligament rupture [18].
A special test that can be used for LAS physical examination is the anterior drawer test. This is performed by placing one hand to stabilize the anterior distal tibia, and with the foot in approximately 20° of plantar flexion, cupping the patient’s calcaneus and placing an anteriorly directed force to the ankle (Fig. 2). Attention should be paid to how much anterior translation occurs to the lateral ankle, and if it is similar to the contralateral side. Again, the uninjured side should be examined first so that a direct comparison can be made. If exam cannot be performed due to patient pain, an ankle block may be considered. One can inject 10 cc of lidocaine just medial to the tibialis anterior and into the ankle joint. This often results in adequate pain relief. Continuing the evaluation, in an ATFL tear, a dimple sign may also be visible in the anterior side of the joint in 50% of cases [19] (Fig. 3). During posterior to anterior stress of the talus, negative intra-articular pressure due to the tear causes the subcutaneous tissue to produce a divot and create a dimple. Most patients acutely ambulate with an antalgic gait [2]. A previous injury or activity during which the injury occurred, footwear, playing surface, and the use of taping or bracing raise suspicion for LAS [20].

Image demonstrating the anterior drawer test. This is performed by placing one hand to stabilize the distal tibia (down arrow), and with the foot in approximately 20° of plantar flexion, cupping the patient’s calcaneus and placing an anteriorly directed force (up arrow)

Image demonstrating a “dimple sign” (depicted by the arrow) which is seen with ATFL tears
After completion of the physical examination, determining the extent of the injury may help decide the treatment the patient will need. When classifying these injuries, there are several grading and staging systems for lateral ankle ligament injuries, based on anatomical injury, clinical symptoms, trauma mechanism, stability and “severity” of the injury. Hamilton and Kaikkonen introduced a system that incorporates anatomical damage with patient’s symptoms (Table 1). However, their classification system is only reliable when made with delayed physical examination [5]. Ottawa rules about the ankle are another useful tool in the evaluation of acute ankle injuries [21]. These rules were established to help physicians decide which patients should have an x-ray following acute ankle injury. These rules suggest that ankle x-rays should be required only if (1) there is any pain or bony tenderness along the distal 6 cm of the posterior edge of tibia or tip of the medial malleolus or (2) pain or bony tenderness along the distal 6 cm of the posterior edge of fibula or tip of the lateral malleolus or (3) the patient is unable to bear weight both immediately following injury and in the emergency department for four steps. While these rules are primarily used to rule out clinically significant ankle fractures, a negative screen can suggest ligamentous injuries that may require further workup depending on the extent of the injury.
1.3 Imaging
1.3.1 X-ray
Radiographic evaluation of the ankle should begin with plain radiographs. This will help to distinguish between a ligamentous and a bony injury. An anteroposterior (AP), oblique, and lateral views of the ankle should be taken. Non-weight-bearing x-rays are acceptable, especially if the patient is in pain. The goal of these radiographs is to exclude a bony injury. In addition to plain radiographs, stress x-rays can be performed that may add more information on the extent of injury. Although often not used, for completeness of a discussion of ankle evaluation, two radiographic stress tests have been reported. These include the talar tilt test (TTT) and anterior drawer test (ADT) [13].
The TTT measures the angle produced by the tibial plafond and the dome of the talus during forceful inversion of the hindfoot (Fig. 4). A positive test reveals a torn or irreversible stretched lateral ligamentous complex. There is wide disagreement on what constitutes normal tilt of the talus in the ankle. Some studies show that it may range from 5° to 23° of varus tilt in a normal ankle [22, 23]. Comparing both ankles may help to differentiate an abnormal TTT.

Image demonstrating the talar tilt test (TTT). The TTT measures the angle produced by the tibial plafond and the dome of the talus during forceful inversion (arrow) of the hindfoot. A positive test reveals a torn or irreversible stretched lateral ligamentous complex
The ADT was designed to measure the integrity of the ATFL and may be a more reliable measure than the TTT for diagnosing the extent of ligamentous lateral ankle injuries [13]. It is performed by producing anterior movement of the ankle relative to the distal tibia. This is the same exam maneuver described in the physical exam section, performed with a lateral X-ray. The ADT is measured from the posterior lip of the tibial plafond to the nearest posterior articular surface of the talus. The values for accepted normal subluxation ranges from 2 mm to 9 mm [24, 25]. Again, this should be compared to the contralateral side to determine the difference between ankles.
Although high interobserver reliability has been shown on stress X-rays, these examinations often exacerbate pain in the acute phase. In addition, no reports indicate a high sensitivity or specificity for this type of radiographic examination. Some authors feel that ankle stress radiographs are generally unnecessary, unreliable, and outdated for identifying acute ligamentous injuries after ankle sprain. One major reason for this is many studies suggest that ligament laxity, after acute rupture, is not strongly correlated to the development of late symptoms [2, 26].
1.3.2 Ankle Arthrography
Ankle arthrography is not traditionally performed but can be a useful resource in the setting where a magnetic resonance imaging (MRI) is unavailable. Ankle arthrography is performed by injecting approximately 10 cc of contrast material into the ankle joint to identify a ligamentous tear. In a normal exam, the injected contrast will remain within the joint capsule. In up to 10% of cases, the dye may flow into the tendon sheaths of the flexor hallucis longus, flexor digitorum longus, and the subtalar joint, which is not pathological. The dye should not extend beyond the distal end of the lateral malleolus nor should it flow more proximally than 5.5 cm above the distal tip of the fibula [27].
If the ATFL is torn, dye will extravasate anterolaterally. Any extravasation of contrast into the peroneal tendon sheath is abnormal. In most ruptures of the CFL, the medial layer of the peroneal tendon sheath is split longitudinally. If there is flow into the peroneal structures, that is indicative of a tear of both the CFL and ATFL. If the tear in the capsule is very large, there may not be sufficient pressure to force contrast into the sheath even if there is a tear. Therefore, there is a high incidence of false negative rate [13]. In one study, ATFL damage was confirmed by arthrogram in 52% of patients demonstrating tenderness of the ATFL and CFL damage was confirmed in 72% of patients demonstrating tenderness in CFL [3].
This study should not be performed 5 days after the injury. The extravasation of dye may be prevented if performed after 5 days as the tear in the joint capsule or ligament(s) may be closed with blood clots or fibrin tissue.
1.3.3 Ultrasound
Ultrasound can be useful in diagnosing an associated injury during the acute phase, within the first week, and are routinely used in professional athletes [5]. There are reports of up to 95% ATFL and 90% CFL injury diagnostic accuracy [28]. Using ultrasound evaluations for a ligament rupture, has identified a sensitivity is 92% and a specificity of 64%. The positive predictive value is 85% and negative predictive value is 77% [5]. Ultrasound imaging is especially valuable in acute ligamentous injuries, with an accuracy up to 93.8% sensitivity and a 100% specificity, when compared with magnetic resonance imaging (MRI) in diagnosing ATFL tears [29]. The two notable limitations are that acute tears may be difficult to view due to swelling and that its accuracy is highly dependent on the operator and/or equipment [2]. If the images are not interpreted accurately, this often results in a false negative.
1.3.4 MRI
An MRI scan is considered the gold standard for evaluating ligamentous injuries. It can also be useful in diagnosing associated injuries (bone, chondral or tendon) [5]. It is not usually indicated in the routine investigation of acute ankle injuries, within the few weeks, due to high incidence of false-positive findings [2]. In a study, out of 37 complete ATFL tears, 9 were determined to be false positives during surgery (approximately 24%) [30]. As previously stated, it is also useful in detecting osteochondral lesions of the talus and determining whether any injuries occurred to the ankle syndesmotic ligaments [2]. A high percentage of patients identified with ATFL and CFL injuries have also demonstrated injury to the posterior tibialis tendon, peroneus brevis, or peroneus longus [3]. The accuracy of MRI for ATFL partial and complete tears was 74% and 79%, respectively, with a sensitivity and specificity of 64% and 86% for partial tears and 78% and 80% for complete tears, respectively. The accuracy of MRI for CFL partial and complete tears was 66% and 88%, respectively, with a sensitivity and specificity of 41% and 87% for partial tears and 61% and 95% for complete tears, respectively [30].
1.4 Treatment
1.4.1 Nonoperative Management
After performing a physical examination, imaging studies of the ankle, and classifying the ligamentous injury, a discussion with the patient should then be undertaken about the treatment needed to manage the injury. Successful treatment of acute lateral ankle ligament injuries, regardless of grade, can be achieved with individualized aggressive, non-operative measures. Protection, Rest, Ice, Compression, and Elevation (PRICE) therapy is the treatment of choice for the first 4–5 days. This initial approach is designed to reduce pain and swelling. The authors also believe that 2 weeks of immobilization is beneficial, either in an air cast or brace. After 2 weeks, the authors’ preferred treatment is the use of a lace-up brace or functional taping, to reduce the risk of recurrent injury. Ankle bracing or taping improves mechanical and functional stability which reduces reinjury rates, improves proprioception, and allows individuals to continue their activities of daily living. Functional taping is typically reserved for athletes, while the majority of patients receive a brace. A study discussing athletes, who have taped or braced after an acute injury, reported 70% fewer ankle injuries compared to individuals without any external support [31]. There is debate between early mobilization versus short-term immobilization upon initial injury. The Collaborative Ankle Support Trial (CAST) study demonstrated faster recovery with a short period of immobilization when compared to treatment solely a compression bandage [32]. Controlling the stress on the ligaments promotes proper orientation of collagen fibers, which allows for full return to activities, between 4 and 8 weeks post-injury [5].
Physical rehabilitation includes proprioceptive training and eversion strengthening of the peroneus brevis, typically beginning 2–3 weeks after the injury, when the swelling decreases. The addition of ultrasound or electrical muscle stimulation have not demonstrated any effectiveness in symptom relief or resolution [2].
In addition to PRICE therapy and acute immobilization, the authors recommend the use of nonsteroidal anti-inflammatory drugs (NSAIDs). This has been shown to provide pain and swelling relief within the first 3 weeks, without any negative long-term effects [5, 11]. Acetaminophen and opioids seem to be equally effective as NSAIDs for pain, swelling, and ROM in the first 2 weeks following acute sprain, although opioids have significantly more adverse effects and should be avoided all together [2].
In addition to the use of PRICE, immobilization, NSAIDs and braces, the treatment of ligamentous injuries has also included biologics (such as platelet-rich plasma (PRP) and hyaluronic acid) injections. These are more recent developments where the efficacy continues to be studied. To date, there is no literature supporting its efficacy in reducing pain and improving functional outcomes to be greater than placebos. As such, further study in this field is warranted.
1.5 Operative Management
Surgery for the repair of acute injuries is not without higher costs, longer recovery times, higher incidences of ankle stiffness, impaired ankle mobility, and increased risk of complications, such as wound-healing problems, nerve damage, and possible infections [26]. Unless the patient is a high performing athlete, surgery is typically not recommended for the management of acute injuries. Although acute repair of the lateral ankle ligaments in grade III injuries in professional athletes may give better results than nonoperative treatment, major reviews have failed to demonstrate a clearly superior treatment approach for LAS between surgical and conservative management [33]. This may be due to a higher proportion of objective stability observed on stress radiography, compared to non-operative treatment, which results in fewer recurrences of LAS [5].
1.5.1 Primary Repair (Broström and Its Modifications)
In patients with chronic lateral ankle instability, the operative standard of care is an anatomic repair of the lateral ligamentous complex. The most common anatomic repair is the use of the Broström procedure and its modifications (Table 2). This approach is used to correct instability that has occurred with chronic injuries to the ATFL and the CFL.
The procedure for isolated ligament repair uses a curved incision over the anterior border of the lateral malleolus or an extensile longitudinal incision along the distal fibula when additional tendon or retinaculum needs to be repaired (Fig. 5). The ATFL and CFL are identified at the lateral aspect of the capsule when the tissues are retracted anteriorly. The ATFL and CFL are dissected from the surrounding tissue and repaired in a pants-over-vest technique. To confirm that the repair has not limited the ankle ROM, full dorsi- and plantar flexion should be performed intraoperatively. This procedure is highly effective with 91% of patients reporting good or excellent results, based on the Good Ankle Function Scale [34]. A total of 87% of the patients had full ankle joint ROM restored postoperatively [34].

Image depicting the Broström procedure (a) and its modifications, namely the Gould modification (b) and the Karlsson modification (c)
A second type of ligament repair is the Karlsson technique. This surgical approach is performed by excising scar tissue, sectioning the ligaments 3–5 mm from their insertions on the fibula, and then reattaching them to the fibula using drill holes or suture anchors. The advantage of this technique is that it promotes ligament-to-bone healing versus ligament-to-ligament healing as seen in the Broström procedure. Eighty-eight percent of patients treated with this procedure demonstrated good to excellent functional results, including stability, pain, activity levels, and swelling [35]. Patients with generalized hypermobility, long-standing ligamentous insufficiency, or previous tenodesis surgery are more likely to have unsatisfactory results regardless of technique used [16].
Modifications have also been discussed to improve the strength of these reconstructions. One such technique is the Gould modification [36]. This approach consists of elevating and suturing the extensor retinaculum to the distal fibula by pulling it proximally. The addition of the Gould modification has also been shown to limit inversion of the ankle and to stabilize the subtalar joint with no statistically significant differences of ankle kinematics between repaired ankles and contralateral normal ankles [36].
In patients who present with absent or excessively damaged ligaments, these procedures will likely not be possible or effective. In these situations, an anatomic versus non-anatomic reconstruction must be considered using either allograft, autograft, or tendon transfer [11]. Non-anatomic reconstruction techniques involve rerouting the peroneus brevis tendon through bone tunnels in the distal fibula and include the Watson-Jones, Evans, and Chrisman-Snook procedures (Table 3). These non-anatomic reconstructions have been shown to have poorer long-term outcomes with a greater risk of progression to arthritis, due to alterations in ankle and hindfoot kinematics and the loss of subtalar motion [11, 16].
For anatomic graft reconstructions, the anatomy and mechanics of the ATFL and CFL are recreated via autogenous or allogenic tendon graft placement at the native ligament insertion sites. These are then routed through tunnels in the distal fibula, the talus, and the calcaneus. The tendon grafts can be fixed with interference screws into the tunnels or sutured to themselves [11]. Graft augmentation can also be helpful in patients with CLAI, those that have poor tissue quality, a failed previous repair, generalized ligamentous laxity, and a cavovarus foot deformity. One noted potential risk of both anatomic and nonanatomic reconstructions is an iatrogenic fracture through the fibular tunnels.
1.5.2 Ankle Arthroscopic and Arthroscopic Ligament Repair
Arthroscopy is useful in diagnosing intra-articular conditions associated with CLAI, such as impingement, loose bodies, osteochondral lesions, chondromalacia, and bone spurs [16]. It is commonly performed in combination with open lateral ankle ligament reconstruction, for diagnostic purposes, as well as addressing concomitant intra-articular lesions. In addition, an arthroscopic Broström repair has been shown to restore ankle function equivalent to open repair but with the advantages of smaller scars, less pain, less swelling, less disturbance of cutaneous sensation, and possibly faster recovery [11, 16]. However, this type of repair may be dependent on the surgeon’s skill when using this technique.
1.6 Post-operative Management
Postoperatively, the authors’ approach is to place patients into a non-weight-bearing Arbeitsgemeinschaft für Osteosynthesefragen (AO) splint for the first 2 weeks. After the cast is removed, patients are placed into a removable boot and physical therapy is started focusing on ROM activities, muscle strengthening and proprioceptive training. Partial weight-bearing is begun 4 weeks postoperatively with full weight-bearing allowed at 6 weeks postoperatively. A graduated functional return to a training program is set on an individual basis, aiming for return to training and/or play within 12 weeks of injury [5].
For athletes, return to sport timelines are not well defined and are dependent on the specific injury and the surgery performed. Once 90% of ankle strength has been restored, at approximately 3-months post-operatively, patients may return to play. Ankle bracing or taping for at least 6 months after surgery must be considered for all athletes returning to play as these interventions have been shown to have a 70% decrease in recurrent ankle sprains [11].
2 Medial Ankle Injuries
2.1 General
2.1.1 Epidemiology
Approximately 3–4% of all ankle sprains consist of isolated deltoid ligament injuries [29]. Twelve percent of ankle osteoarthritis cases are the result of medial ligament lesions and 3% are due to combined medial and lateral ligament lesions [29]. The most common cause of recurrent medial ankle instability is an uncorrected hindfoot valgus or pes planovalgus. Inappropriate treatment of both combined or isolated medial ankle sprains can result in chronic rotational ankle instability. In addition, osteochondral lesions (OCL) are often found concurrently with injuries involving the medial ligamentous complex in as high as 20% of cases [29].
2.1.2 Anatomy
The deltoid ligament is the primary stabilizer of the ankle against plantar flexion [29]. It is composed of a superficial and deep layer (Fig. 6). The superficial component deltoid ligament is primarily attached to the anterior colliculus of the medial malleolus and spans both the ankle and the subtalar joints. It consists of the tibionavicular, tibiospring, tibiocalcaneal, and superficial posterior talotibial ligaments. The deep layer is primarily attached to the posterior colliculus of the medial malleolus and the intercollicular groove. It crosses only the ankle joint and consists of the deep anterior and posterior tibiotalar ligaments. The superficial component has been shown to limit external rotation and resist valgus stress of the ankle and hindfoot. The deep component resists ankle eversion and lateral migration of the talus. An additional ligamentous structure, that helps augment the deltoid ligament and aids in stabilization of the medial ankle, is the calcaneonavicular (spring) ligament. It is part of the deltoid ligament complex and consists of two components: the superomedial and inferior ligaments. The spring ligament assists in stabilizing the medial ankle structures of the ankle joint through its connection to the deltoid via the tibiospring ligament [29].

Image depicting the deltoid ligament of the medial ankle
2.1.3 Mechanism
The mechanism of injury is suspected to be a combination of external rotation and eversion of the foot. Alternatively, a fixed foot with an inward twist of the body places stress on the medial ligamentous complex. Deltoid injuries can also occur with pronation and external rotation ankle fractures (Weber C), pronation abduction ankle fractures and less frequently with supination external rotation (Weber B) ankle fractures [29]. It has been reported that the deltoid ligament is involved in up to 40% of ankle fractures [37].
2.1.4 Outcomes
Chronic medial ligamentous instability contributes to chronic medial ankle instability (CMAI). This occurs due to pathologic laxity of the deltoid ligament. The talus falls medially, with talonavicular subluxation, creating a varus deformity in chronic injuries. This contributes to a laxity of the spring ligament and results into the development of pes planus [29]. In addition to chronic ligamentous instability, abnormal bony pathology, seen in patients with a wider talar dome and smaller tibial plafond, can also contribute to chronic mechanical instability [29].
Mechanical ankle instability is defined by laxity of the ankle joint due to the damaged structures, while functional instability is the result of an impaired proprioception and a slowed neuromuscular reflex. However, mechanical instability may result in functional instability. End stage functional instability can be identified when CMAI patients have difficulty maintaining their position during single leg stance [29].
2.2 Physical Examination and Classification
Patients with an acute injury of the deltoid ligament often present with acute swelling, hematoma, and the inability to bear weight. On physical exam, the patient should be sitting or supine, with both ankles exposed. The uninjured ankle should be examined initially to determine what the patient’s baseline exam is, similar to the lateral ankle exam. On inspection, note should be taken on where the patient has swelling and if there is any hematoma or discoloration, particularly over the medial ankle complex. On palpation, tenderness will be present over the deltoid complex, just distal to the medial malleolus. ROM may be difficult to assess due to pain. Neurovascular status should be evaluated, as with any injury examination. To evaluate the superficial deltoid ligament, an external rotation test should be utilized, while an eversion stress test is used to assess the deep deltoid ligament [29]. This is performed with the patient in the supine position. One hand is used to stabilize the distal tibia, and with the foot in dorsiflexion, the ankle is either internally or externally rotated.
In CMAI, the patient will complain about the ankle instability. They will demonstrate pain over the anteromedial surface of the ankle, posterior tibial tenderness, and a correctable hindfoot valgus deformity [29]. With the development of intra-articular impingement in CMAI, defined as structures entrapped within the ankle joint during terminal dorsiflexion and/or plantar flexion, mechanical symptoms such as catching, or locking may also be present [29]. Further evaluation of a deltoid injury should be performed with the patient standing. During weight-bearing one should inspect gait and ankle position of the affected ankle, to identify whether there is any planovalgus and abductus of the hindfoot (flat foot with ankle appearing to be pointing inward and heel pointing outward) [29]. After evaluating the ankle for a deltoid injury, the examiner should consider classifying these injuries. Valderrabano et al. classified clinical CMAI into four grades based on increasing severity and ligamentous damage and also created an arthroscopic and intraoperative classification, to determine the severity of the injury [38] (Table 4).
2.3 Imaging
2.3.1 X-ray
Standard ankle radiographs, including supine AP, oblique and lateral views should be used to evaluate the medial ankle clear space, to identify whether there is a bony deltoid avulsion fragment, to assess whether any widening of the syndesmosis has occurred, and whether there are any other associated ankle fractures. Standing views can be utilized to place weight-bearing stress on the ankle complex but is often deferred due to pain.
An increased medial clear space, compared to the contralateral extremity, is indicative of complete tear of the deltoid ligament [39]. Normal medial clear space ranges from 3–4 mm [40]. Other conditions that can be evaluated using plain X-rays include the presence of a foot deformity (such as pes planovalgus and abductus of the hindfoot), OCL of the talus and plafond, bony impingements, and early osteoarthritic changes [29].
2.3.2 Ankle Arthrography
As stated previously, ankle arthrography is not traditionally performed but can be a useful resource in the setting where MRI is unavailable. It is performed by injecting nearly 10 cc of contrast into the ankle joint to identify any ligamentous tears. The injected contrast will remain within the joint capsule if there are no ligamentous injuries present. If the deltoid complex is torn, the dye will extravasate medially. Similar to lateral ligamentous injuries, this should be performed within the first week as fibrinous tissue may block extravasation of dye and effect results.
2.3.3 Ultrasound
Ultrasonography is a valuable tool in assessing medial ankle instability. It is not used as often as it is in lateral ligament injuries but may still be useful. The benefits are accessibility, cost, and it can also be performed in real time using joint stress maneuvers to assess for ankle ligament stability and bony impingement [29]. The greatest downfall of this tool is that it is very user dependent which can result in a high false negative if a ruptured deltoid complex is misinterpreted.
2.3.4 MRI
An MRI scan is often used in the diagnosis of acute and chronic medial ankle injuries. It can identify the extent of the injury and associated pathologic conditions, as well as assist in preoperative planning. It has been reported that up to 20% of patients may have false negative MRI findings in the setting of acute deltoid ligament complex injury associated with ankle fractures [41].
2.4 Nonoperative Management
Nonoperative management is often utilized as the initial treatment for isolated deltoid ligament complex injuries. PRICE is encouraged during the first 2 weeks. The use of a soft ankle orthosis, such as air cast or compression wrap, is indicated for simple sprains (grade I) until the patient is pain-free and has reached pre-injury strength levels. This often takes 3–4 weeks. More severe sprains (grades II–III) require eversion avoidance and may require a functional ankle brace that should be worn for at least 6 weeks.
Physical therapy should focus on ROM followed by neuromuscular and strength training, especially of the posterior tibial muscle [29]. Physical therapy should begin after 3–4 weeks of immobilization and should continue until preinjury strength returns, which can be 6–12 weeks after the injury. The use of NSAIDs can also be used as an adjuvant anti-inflammatory and for pain relief, during the first few weeks following injury, and as a method of pain relief during physical therapy sessions.
2.5 Operative Management
Operative treatment may be pursued in patients who have failed to improve with conservative measures, over 6 months in duration [29]. Chronic complaints of instability, recurrent sprains, persistent pain, and a worsening pes planovalgus deformity of the ankle may be an indication for surgical intervention. Treatment options for the deltoid include primary repair, primary repair with augmentation, and occasionally supplementation with bony work if there is fracture or chronic deformity.
Primary repair is dependent on the level of ligament injury and soft tissue structure. The authors’ preferred approach is to repair the deltoid ligament from distal to proximal and attach it to the medial malleolus via transosseous sutures or anchors (Fig. 7). Sutures should be tightened with the ankle held at 90° of dorsiflexion. Augmentation reconstruction is an option if the soft tissues are inadequate for a stable direct repair. In settings of posterior tibial tendon insufficiency, a hindfoot reconstruction may be required to augment any posterior tibial tendon reconstruction that is necessary.

Image depicting deltoid ligament reconstruction utilizing transosseous sutures and anchors
In up to 40 % of ankle fractures the deltoid ligament is injured [37]. In patients presenting with both a deltoid ligament injury and a medial malleolus fracture, both ligament repair and fracture fixation are recommended, in certain circumstances [41, 42]. Associated medial malleolus fractures and ligamentous injuries, with a fracture width of less than 17 mm, risk residual deltoid insufficiency despite satisfactory fragment fixation [42]. In lateral malleolar fractures, the medial ligament should heal adequately if the lateral malleolus is well reduced. However, a persistent increase in the medial clear space or a demonstrated intraoperative valgus instability may require surgical exploration and deltoid repair [43].
2.5.1 Arthroscopy
Although not routinely performed, diagnostic arthroscopy can help detect deltoid ligament insufficiency and evaluate anatomic structural abnormalities within the deltoid, spring ligament, and posterior tibial tendon. Many studies support visualizing the deltoid ligament complex and associated injuries intraoperatively prior to surgical intervention [29, 37].
2.6 Post-operative Management
For the first 6 weeks, the authors’ preference is to put the patient into a high stabilizing walking boot and placed on partial weight-bearing protocols. The boot will maintain the ankle at 90° (neutral position) and physical therapy, focusing on ROM, should begin after the 2 week post-operative visit. After 6 weeks, the authors recommend discontinuation of the boot and utilization of a sneaker with a soft ankle orthosis (compression wrap air cast), until 12 weeks post-operative. After ROM, physical therapy should focus on proprioception, coordination, and muscle strengthening exercises [29]. A graduated functional return to training program is set on an individual basis aiming for return to activities within 12-weeks post-injury [5].
3 Syndesmotic Injuries
3.1 General
3.1.1 Epidemiology
The syndesmosis refers to the ligaments of the ankle that connect the tibia and fibula. In the United States, it is estimated that there are nearly 6500 syndesmotic injuries per year [44]. The majority of these injuries occur in those 18–34 years of age but affects individuals of all ages. In the athlete, a study that looked at European professional soccer teams, revealed that 7% of all ankle injuries (both fractures and sprains) sustained by players were isolated syndesmotic injuries [45]. Syndesmotic injuries can be in isolation, known as high ankle sprains, or with associated ankle fractures. High ankle sprains encompass up to 12% of all ankle sprains in the common population and 25% of ankle sprains sustained in collision sports [46]. In individuals with lateral ankle sprains, the rate of additional syndesmotic injury was nearly 18% [47]. This underscores the need for a careful examination of ankle injuries, regardless of the reported mechanism of injury, particularly given the possibility of concomitant ligamentous injury.
Approximately 10% of all ankle fractures are associated with syndesmotic damage. If the patient’s ankle fracture requires operative fixation, nearly 20% have been found to have an associated syndesmotic injury [48]. When breaking down incidence, using the Danis-Weber classification of lateral malleolus fractures, a Weber A injury (inferior to level of syndesmosis) is rarely associated with syndesmotic injury (less than 3%). A Weber B (at level of syndesmosis) and Weber C (superior to syndesmosis) have been shown to have a 30–40% incidence and up to 80% incidence, respectively [49].
3.1.2 Risk Factors
A variety of risk factors have been explored. A frequently investigated factor, gender, is not determined to be a risk factor for injury [50]. Sports that may expose the individual to high-speed collisions, high torque cutting, and jumping may increase risk of syndesmotic injury. Other risk factors include artificial surfaces and uneven terrains [46]. Mechanisms of injury other than those observed in sporting activities include falls or tripping accidents with twisting weight-bearing injuries and motor vehicle accidents.
3.1.3 Anatomy
The ligaments that compose the syndesmosis (Fig. 8) are the anterior-inferior tibiofibular ligament (AITFL), interosseous ligament, interosseous membrane, posterior-inferior tibiofibular ligament (PITFL), transverse tibiofibular ligament, and inferior transverse ligament. The tibia has a concave triangular groove, just above the lateral articular surface, described as the incisura that the fibula lies in. The syndesmosis maintains this important relationship between the tibia and fibula and preserves ankle stability.

Image depicting the syndesmotic ligaments of the ankle, which is composed of several structures including the anterior-inferior tibiofibular ligament (AITFL), interosseous membrane (IOM), posterior-inferior tibiofibular ligament (PITFL), and transverse tibiofibular ligament (TTFL)
The AITFL runs from the distal anterolateral tibial (Chaput’s) tubercle to the distal anterior (Wagstaffe’s) tubercle on the fibula. The PITFL runs from the posterolateral tibial tubercle to the posterolateral malleolus, above the digital fossa. The inferior transverse ligament runs from the posterolateral tibia to the posteromedial distal fibula. The interosseous membrane runs from the tibia periosteum to the fibula down to the tibiotalar joint. At that level, it is known as the interosseous ligament [46, 51].
3.1.4 Mechanism of Injury
Typically, injuries to the syndesmosis occur when an external rotation force is applied to a dorsiflexed ankle. The talus then places a lateral force on the fibula, separating the fibula from the tibia. This results in the fibula externally rotating and displacing posteriorly. If the foot is pronated during the external rotation, it often results in injury to the AITFL. If the foot is in neutral, it often affects the deltoid [52]. Up to 55% of high ankle sprains may be caused by a collision injury while the foot is externally rotated and planted on the ground [53].
3.2 Physical Evaluations and Classification
On physical exam, the patient should be sitting or supine, with both ankles exposed. Historically, the patient will often complain of feeling a diffuse, generalized ankle pain. On inspection, determine if the patient has swelling and whether there is any hematoma or discoloration about the ankle. This is diffuse and often seen at the level of the ankle joint but it can extend to the junction of the distal third of the leg. On palpation, patients often have tenderness at the tibiofibular joint that extends proximally. ROM may be difficult to assess due to pain. Neurovascular status should be evaluated as with any injury examination.
Special maneuvers that can be used for a syndesmotic injury include the squeeze test, the tibiofibular shuck or Cotton test, abduction and external rotation test and the fibular translation test. A complete explanation of how to perform these tests and references is listed in chapter “Evaluation of Ankle Pain”.
Regarding classification, there is no definitive agreed upon system. In all, the sprain is classified from Grade 1 to 3, with 3 being the most severe. Grade 1 is described as mild injury with a stable joint and normal X-rays. Grade 2 is a moderate injury and indicates that there has been a partial ligament disruption, with positive provocative exams, but normal X-rays. There is no established agreement on if there is ankle stability in this grade of sprains. The authors believe this is an unstable injury and treat it as so. Grade 3 is a severe, complete injury to the syndesmotic ligaments. X-rays show a widened clear space between the tibia and fibula and provocative exams that are positive.
3.3 Imaging
3.3.1 Plain Radiography
Standard ankle radiographs, including supine AP, oblique and lateral views should be used to evaluate the medial ankle clear space, if any widening (diastasis) of the syndesmosis has occurred, and to determine whether there are any associated ankle fractures. Some may find weight-bearing X-rays helpful to place stress on the syndesmotic ligaments and evaluate for tibiofibular diastasis. The three factors used to evaluate this diastasis is tibiofibular clear space, tibiofibular overlap and medial clear space. On the mortise view the normal values for each are <6 mm, >1 mm, and <4 mm, respectively [54].
The tibiofibular clear space is measure from the lateral border of the posterior tibial malleolus to the medial border of the distal fibula, 1 cm above the plafond. This can be measured on the AP or mortise view with normal <6 mm. This is the authors’ preferred method of measurement as it is not affected by ankle rotation. The tibiofibular overlap is measured from the anterior tibial tubercle’s lateral edge and the medial distal fibula. Normal value on the AP is >6 mm and the mortise is >1 mm. Because this measurement is affected by foot rotation it is not as reliable. Medial clear space is measured from the lateral edge of the medial malleolus to the medial border of the talus. This is measured on the mortise view and normal is <4 mm. As it can only be accurately measured on the mortise view, it is affected by ankle rotation. If there are any questions about abnormal findings, a comparison view of the non-injured contralateral extremity should also be taken.
3.3.2 Ankle Arthrography and Ultrasound
Unlike with medial and lateral ligamentous complex injuries, ultrasound and ankle arthrography are not diagnostic modalities commonly utilized for syndesmosis evaluation. Ankle arthrography has limited value in syndesmotic injury and, has previously been stated, is often used for lateral ankle injury suspicions and sometimes medial. Ultrasound may have a role in the future to determine tibiofibular diastasis but is not often useful at this point in time.
3.3.3 MRI
As with near all soft tissue ligamentous injury, MRI is the most accurate tool for diagnosis. It is fundamental to confirming suspicion when there is doubt on simply clinical exam and plain radiographs [54]. An MRI has a sensitivity, specificity, and accuracy of 100%, 93%, and 96%, respectively for diagnosing AITFL ruptures and 100%, 100%, and 100%, respectively, for diagnosing PITFL tears [46]. MRI also can diagnose associated injuries of the bone, cartilage, other ligaments and tendons.
3.4 Nonoperative Management
Grade I stable, purely ligamentous injuries are treated nonoperatively. PRICE therapy is a mainstay of this treatment. They are placed in a supportive CAM boot and remain non-weight-bearing for the first 4 days, to allow the acute inflammation and pain to reside. The patient is then instructed to continue the CAM boot but begin weight-bearing as tolerated and may remove the boot and begin active ROM [46]. After the first week, and after the inflammation has subsided, the patient may discontinue the boot and replace it with a soft brace or ace wrap. Patients will continue to weight bear as tolerated, continue their ROM exercises, and begin a strengthening program. Some patients may benefit from NSAIDs, as a pain reliever for the first week. Patients often do not need formal physical therapy but if they have not fully recovered within 4–6 weeks, physical therapy may be started.
3.5 Operative Management
Unstable syndesmotic injuries should be treated with operative management. The authors believe this includes Grade 2 and Grade 3 high ankle sprains and nearly all fractures with concomitant syndesmotic injuries. The treatment involves stabilization of the syndesmosis, and reduction and fixation of the fractures.
The fracture should be anatomically reduced and fixed first, then syndesmotic stability should be assessed. This is performed under fluoroscopy. The authors’ preference is to use an external rotation stress test, or the cotton hook test can be used intraoperatively. The Cotton hook test is performed by translating the fixed fibula laterally via a clamp [55]. Both tests assess for widening of the syndesmosis. If normal parameters are not restored, the surgeon should proceed with syndesmotic stabilization.
There are two common methods for syndesmotic fixation: screw fixation and suture button fixation [56].
3.5.1 Screw Fixation
Screw fixation, under fluoroscopic guidance, is used most commonly, but there is no consensus on screw size, number of screws, number of cortices, and need for implant removal [56]. Either 3.5 mm or 4.5 mm screws are used and are placed 2–5 cm proximal to the ankle joint and parallel to the articular surface. Due their size and strength, 4.5 screws break less often although such a rigid construct may not be a benefit. They are easier to remove but often leave a larger defect, which may create a stress on the fibula, resulting in a fracture. Regardless of the screw size used, there is no difference between a three to four cortex fixation, in regard to loss of reduction, screw breakage, or the need for implant removal [57].
3.5.2 Suture Button
A newer surgical implant with a promising future is the use of an endobutton (suture) device. A strong (fiber wire) suture loop is secured between two metal buttons that are placed on the outer cortices of the tibia and fibula, or through a fibular plate. It is placed in the same location and trajectory as the syndesmotic screws. It is then tensioned after placed appropriately. This construct is less rigid than screws and may allow the tibiofibular joint more physiologic motion.
3.5.3 Arthroscopy
Arthroscopy may be used as a diagnostic tool to assess syndesmosis. A length-labeled prob or small shaver can be used to measure the diastasis and determine instability [46]. If there is instability diagnosed, the surgeon may proceed with the stabilization methods described above. Arthroscopy is also beneficial in that it can diagnose other concurrent lesions the patient may have sustained such as osteochondral lesions or medial and lateral ligament injuries. In addition, it can also be used to confirm syndesmotic reduction under direct visualization.
3.6 Post-operative Management
The authors preference is to have the patient splinted in a short leg AO splint, which is a posterior splint with stirrup, for 2–3 weeks, non-weight-bearing. At the first postoperative visit (at 2–3 weeks), the splint is removed, and the patient is placed in a removable CAM boot. The patient is to remain non-weight-bearing for approximately 6 weeks postoperatively to allow proper healing but may begin gentle ROM at 3–4 weeks. After 6 weeks postoperatively, patient may begin weight-bearing. Patient with poorly controlled diabetes or other factors such as smoking, alcohol use, vascular disease, or neuropathy, may require longer timelines of immobilization and non-weight-bearing. Although some surgeons remove these screws routinely, the authors reserve the additional procedure, the earliest at 3–4 months postoperatively, and only for those who are experiencing irritation or reduced ROM.
4 Conclusion
Ligamentous ankle injuries are one of the most commonly diagnosed musculoskeletal injuries. These include lateral ankle sprains (LAS), medial ankle sprains (MAS), and syndesmotic injuries, any of which may occur as an isolated or associated with an ankle fracture. The LAS typically occurs from excessive inversion and internal rotation of the foot while the opposite is true for MAS. Syndesmotic injuries occur during supination or pronation with external or internal rotation about the ankle. All these injuries may present with significant pain, swelling, decreased range-of-motion, and inability to bear weight. They are diagnosed with special physical examination maneuvers along with plain radiography, used to rule out associated fractures, or magnetic resonance imaging to identify the extent of ligamentous injury. While most ankle sprains resolve using non-operative care, recurrent sprains and subsequent chronic ankle instability, with significant functional impairment may develop in some individuals. In cases of significant or chronic instability, operative management is warranted.
References
Waterman BR, Owens BD, Davey S, et al. The epidemiology of ankle sprains in the United States. J Bone Jt Surg Ser A. 2010;92(13):2279–84.
Halabchi F, Hassabi M. Acute ankle sprain in athletes: clinical aspects and algorithmic approach. World J Orthop. 2020;11(12):534–58.
Kobayashi T, Gamada K. Lateral ankle sprain and chronic ankle instability: a critical review. Foot Ankle Spec. 2014;7(4):298–326. Available from https://pubmed.ncbi.nlm.nih.gov/24962695/.
McKay GD, Goldie PA, Payne WR, et al. Ankle injuries in basketball: injury rate and risk factors. Br J Sports Med. 2001;35(2):103–8.
van den Bekerom MPJ, Kerkhoffs GMMJ, McCollum GA, et al. Management of acute lateral ankle ligament injury in the athlete. Knee Surg Sport Traumatol Arthrosc. 2013;21(6):1390–5.
Beynnon BD, Vacek PM, Murphy D, et al. First-time inversion ankle ligament trauma: the effects of sex, level of competition, and sport on the incidence of injury. Am J Sports Med. 2005;33(10):1485–91.
Doherty C, Delahunt E, Caulfield B, et al. The incidence and prevalence of ankle sprain injury: a systematic review and meta-analysis of prospective epidemiological studies. Sports Med. 2014;44(1):123–40.
Gerber JP, Williams GN, Scoville CR, et al. Persistent disability associated with ankle sprains: a prospective examination of an athletic population. Foot Ankle Int. 1998;19(10):653–60.
Viljakka T, Rokkanen P. The treatment of ankle sprain by bandaging and antiphlogistic drugs. Ann Chir Gynaecol. 1983;72(2):66–70.
Tyler TF, McHugh MP, Mirabella MR, et al. Risk factors for noncontact ankle sprains in high school football players: the role of previous ankle sprains and body mass index. Am J Sports Med. 2006;34(3):471–5.
Camacho LD, Roward ZT, Deng Y, et al. Surgical management of lateral ankle instability in athletes. J Athl Train. 2019;54(6):639–49.
Broström L. Sprained ankles. V. Treatment and prognosis in recent ligament ruptures. Acta Chir Scand. 1966;132(5):537–50.
Boruta PM, Bishop JO, Braly WG, et al. Acute lateral ankle ligament injuries: a literature review. Foot Ankle Int. 1990;11(2):107–13.
Verhagen RAW, de Keizer G, van Dijk CN. Long-term follow-up of inversion trauma of the ankle. Arch Orthop Trauma Surg. 1995;114(2):92–6.
Owoeye OBA, Whittaker JL, Toomey CM, et al. Health-related outcomes 3-15 years following ankle sprain injury in youth sport: what does the future hold? Foot Ankle Int. 2022;43(1):21–31.
Ferkel E, Nguyen S, Kwong C. Chronic lateral ankle instability: surgical management. Clin Sports Med. 2020;39(4):829–43.
Van Dijk CN, Lim LSL, Bossuyt PMM, et al. Physical examination is sufficient for the diagnosis of sprained ankles. J Bone Jt Surg Ser B. 1996;78(6):958–62.
Ivins D. Acute ankle sprain: an update. Am Fam Physician. 2006;74(10):1714–20.
Aradi AJ, Wong J, Walsh M. The dimple sign of a ruptured lateral ligament of the ankle: brief report. J Bone Joint Surg Br. 1988;70(2):327–8.
Chen ET, McInnis KC, Borg-Stein J. Ankle sprains: evaluation, rehabilitation, and prevention. Curr Sports Med Rep. 2019;18(6):217–23.
Stiell IG. Decision rules for the use of radiography in acute ankle injuries. Refinement and prospective validation. JAMA. 1993;269(9):1127–32.
Cox CJS, Hewes TF. “Normal” talar tilt angle. Clin Orthop Relat Res. 1979;140:37–41.
Chrisman OD, Snook GA. Reconstruction of lateral ligament tears of the ankle. An experimental study and clinical evaluation of seven patients treated by a new modification of the Elmslie procedure. J Bone Joint Surg Am. 1969;51(5):904–12.
Laurin CA, Ouellet R, St-Jacques R. Talar and subtalar tilt: an experimental investigation. Can J Surg. 1968;11(3):270–9.
Al-Mohrej OA, Al-Kenani NS. Chronic ankle instability: current perspectives. Avicenna J Med. 2016;06(04):103–8.
Karlsson J, Sancone M. Management of acute ligament injuries of the ankle. Foot Ankle Clin. 2006;11(3):521–30.
Emerson R. Surgical treatment of third-degree lateral ankle ligament ruptures to ensure stability. J Am Osteopath Assoc. 1978;78(4):273–80.
Peetrons P, Creteur V, Bacq C. Sonography of ankle ligaments. J Clin Ultrasound. 2004;32(9):491–9.
Alshalawi S, Galhoum AE, Alrashidi Y, et al. Medial ankle instability: the deltoid dilemma. Foot Ankle Clin. 2018;23(4):639–57.
Tan DW, Teh DJW, Chee YH. Accuracy of magnetic resonance imaging in diagnosing lateral ankle ligament injuries: a comparative study with surgical findings and timings of scans. Asia-Pac J Sport Med Arthrosc Rehabil Technol. 2017;7:15–20.
Dizon JMR, Reyes JJB. A systematic review on the effectiveness of external ankle supports in the prevention of inversion ankle sprains among elite and recreational players. J Sci Med Sport. 2010;13(3):309–17.
Lamb SE, Marsh JL, Hutton JL, et al. Mechanical supports for acute, severe ankle sprain: a pragmatic, multicentre, randomized controlled trial. Lancet. 2009;373(9663):575–81.
Kerkhoffs GMMJ, Handoll HHG, De Bie R, et al. Surgical versus conservative treatment for acute injuries of the lateral ligament complex of the ankle in adults. Cochrane Database Syst Rev. 2007;2:CD000380.
Roos EM, Brandsson S, Karlsson J. Validation of the foot and ankle outcome score for ankle ligament reconstruction. Foot Ankle Int. 2001;22(10):788–94.
Karlsson J, Bergsten T, Lansinger O, et al. Surgical treatment of chronic lateral instability of the ankle joint. A new procedure. Am J Sports Med. 1989;17(2):268–73.
Wainright WB, Spritzer CE, Lee JY, et al. The effect of modified Broström-Gould repair for lateral ankle instability on in vivo tibiotalar kinematics. Am J Sports Med. 2012;40(9):2099–104.
Hintermann B, Boss A, Schäfer D. Arthroscopic findings in patients with chronic ankle instability. Am J Sports Med. 2002;30(3):402–9.
Valderrabano V, Hintermann B. Diagnostik und Therapie der medialen Sprunggelenkinstabilität. Arthroskopie. 2005;18(2):112–8.
Close JR. Some applications of the functional anatomy of the ankle joint. J Bone Joint Surg Am. 1956;38(4):761–81.
Gibson PD, Ippolito JA, Hwang JS, et al. Physiologic widening of the medial clear space: what’s normal? J Clin Orthop Trauma. 2019;10(1):S62–4.
Yu GR, Zhang MZ, Aiyer A, et al. Repair of the acute deltoid ligament complex rupture associated with ankle fractures: a multicenter clinical study. J Foot Ankle Surg. 2015;54(2):198–202.
Tornetta P. Competence of the deltoid ligament in bimalleolar ankle fractures after medial malleolar fixation. J Bone Jt Surg Ser A. 2000;82(6):843–8.
Harper MC. The deltoid ligament. An evaluation of need for surgical repair. Clin Orthop Relat Res. 1988;226:156–68.
Vosseller JT, Karl JW, Greisberg JK. Incidence of syndesmotic injury. Orthopedics. 2014;37(3):e226.
Lubberts B, D’Hooghe P, Bengtsson H, et al. Epidemiology and return to play following isolated syndesmotic injuries of the ankle: a prospective cohort study of 3677 male professional footballers in the UEFA Elite Club Injury Study. Br J Sports Med. 2019;53(15):959–64.
Hunt KJ, Phisitkul P, Pirolo J, et al. High ankle sprains and syndesmotic injuries in athletes. J Am Acad Orthop Surg. 2015;23(11):661–73.
De César PC, Ávila EM, De Abreu MR. Comparison of magnetic resonance imaging to physical examination for syndesmotic injury after lateral ankle sprain. Foot Ankle Int. 2011;32(12):1110–4.
Pogliacomi F, De Filippo M, Casalini D, et al. Acute syndesmotic injuries in ankle fractures: from diagnosis to treatment and current concepts. World J Orthop. 2021;12(5):269–92.
Kennedy JG, Soffe KE, Vedova PD, et al. Evaluation of the syndesmotic screw in low Weber C ankle fractures. J Orthop Trauma. 2000;14(5):359–66.
Prakash AA. Epidemiology of high ankle sprains: a systematic review. Foot Ankle Spec. 2020;13(5):420–30.
Hermans JJ, Beumer A, De Jong TAW, et al. Anatomy of the distal tibiofibular syndesmosis in adults: a pictorial essay with a multimodality approach. J Anat. 2010;217(6):633–45.
Wei F, Villwock MR, Meyer EG, et al. A biomechanical investigation of ankle injury under excessive external foot rotation in the human cadaver. J Biomech Eng. 2010;132(9):091001.
Nussbaum ED, Hosea TM, Sieler SD, et al. Prospective evaluation of syndesmotic ankle sprains without diastasis. Am J Sports Med. 2001;29(1):31–5.
Tourné Y, Molinier F, Andrieu M, et al. Diagnosis and treatment of tibiofibular syndesmosis lesions. Orthop Traumatol Surg Res. 2019;105(8):S275–86.
Cotton F. Dislocations and joint-fractures. JAMA J Am Med Assoc. 1910;55(22):1916.
Schepers T. Acute distal tibiofibular syndesmosis injury: a systematic review of suture-button versus syndesmotic screw repair. Int Orthop. 2012;36(6):1199–206.
Moore JA, Shank JR, Morgan SJ, et al. Syndesmosis fixation: a comparison of three and four cortices of screw fixation without hardware removal. Foot Ankle Int. 2006;27(8):567–72.
Author information
Authors and Affiliations
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2023 The Author(s), under exclusive license to Springer Nature Switzerland AG
About this chapter

Cite this chapter
Deliso, M., Tang, A., Yoon, R.S., Liporace, F.A. (2023). Management of Ligament Injuries of the Ankle. In: Herscovici Jr., D., Anglen, J.O., Early, J.S. (eds) Evaluation and Surgical Management of the Ankle. Springer, Cham. https://doi.org/10.1007/978-3-031-33537-2_6
Download citation
DOI: https://doi.org/10.1007/978-3-031-33537-2_6
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-031-33536-5
Online ISBN: 978-3-031-33537-2
eBook Packages: MedicineMedicine (R0)