
Abstract
Background
Ankle sprain is one of the most common musculoskeletal injuries, yet a contemporary review and meta-analysis of prospective epidemiological studies investigating ankle sprain does not exist.
Objective
Our aim is to provide an up-to-date account of the incidence rate and prevalence period of ankle sprain injury unlimited by timeframe or context activity.
Methods
We conducted a systematic review and meta-analyses of English articles using relevant computerised databases. Search terms included Medical Search Headings for the ankle joint, injury and epidemiology. The following inclusion criteria were used: the study must report epidemiology findings of injuries sustained in an observed sample; the study must report ankle sprain injury with either incidence rate or prevalence period among the surveyed sample, or provide sufficient data from which these figures could be calculated; the study design must be prospective. Independent extraction of articles was performed by two authors using pre-determined data fields.
Results
One-hundred and eighty-one prospective epidemiology studies from 144 separate papers were included. The average rating of all the included studies was 6.67/11, based on an adapted version of the STROBE (STrengthening the Reporting of OBservational studies in Epidemiology) guidelines for rating observational studies. 116 studies were considered high quality and 65 were considered low quality. The main findings of the meta-analysis demonstrated a higher incidence of ankle sprain in females compared with males (13.6 vs 6.94 per 1,000 exposures), in children compared with adolescents (2.85 vs 1.94 per 1,000 exposures) and adolescents compared with adults (1.94 vs 0.72 per 1,000 exposures). The sport category with the highest incidence of ankle sprain was indoor/court sports, with a cumulative incidence rate of 7 per 1,000 exposures or 1.37 per 1,000 athlete exposures and 4.9 per 1,000 h. Low-quality studies tended to underestimate the incidence of ankle sprain when compared with high-quality studies (0.54 vs 11.55 per 1,000 exposures). Ankle sprain prevalence period estimates were similar across sub-groups. Lateral ankle sprain was the most commonly observed type of ankle sprain.
Conclusions
Females were at a higher risk of sustaining an ankle sprain compared with males and children compared with adolescents and adults, with indoor and court sports the highest risk activity. Studies at a greater risk of bias were more likely to underestimate the risk of ankle sprain. Participants were at a significantly higher risk of sustaining a lateral ankle sprain compared with syndesmotic and medial ankle sprains.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
1 Introduction
Ankle sprain accounts for between 3 and 5 % of all Emergency Department visits in the UK, equating to approximately 5,600 incidences per day [1]. Despite the high prevalence and severity of lifestyle-limiting symptoms that follow the acute episode [2, 3], ankle sprains are often regarded as benign injuries that will resolve quickly with limited treatment [4, 5].
Ankle sprain in sport may result in varying degrees of debilitation, including decreased performance, absence from competition and adverse psychological effects [6]. Following an acute ankle sprain, pain, swelling and ecchymosis are common, which may contribute to reduced mobility and function, as well as occupational absence. The incidence of residual symptoms following acute ankle sprain is variable, but has been reported with rates of between 40 and 50 % [7–10]. The chronicity of injury associated with these symptoms supported a paradigm created by Hertel [11], whereby the causal factors attributable to these symptoms were classified into mechanical and functional insufficiencies, which may interrelate to produce chronic ankle instability (CAI). To be classified as having CAI, residual symptoms (‘giving way’ and feelings of ankle joint instability) should be present for a minimum of 1 year after initial sprain [12].
Ankle sprain has high societal economic costs associated with the diagnosis, treatment and loss of work productivity contingent with the severity of injury. It has been reported that one quarter of all people who sustain an ankle sprain are unable to attend school or work for more than 7 days following the initial injury [13]. The economic burden of ankle sprain cannot be disputed, as the mean total cost of one ankle sprain in the Netherlands in 2001 was reported to be approximately €360 [14], equating to an estimated annual cost of €84,240,000 in the Netherlands alone.
Musculoskeletal injury is also a persistent and primary health concern for military populations as it is a leading cause of hospitalisation and accounts for a significant amount of lost duty time [15]. The yearly cost of military musculoskeletal injuries was estimated to equate to nearly US$1 billion in 1994, with ankle sprain the seventh most prevalent injury subgroup [16]. Military musculoskeletal injuries result in both short-term and long-term disability, and place a substantial burden on the medical system [17]. Ankle sprains are one of the most common musculoskeletal injuries and present a significant issue for military healthcare practitioners [18–22].
The consequences of the developed insufficiencies following an acute ankle sprain extend beyond the context of active populations [23]. It has recently been acknowledged that CAI is a leading cause of post-traumatic ankle joint osteoarthritis [24–26]. Furthermore, it has previously been demonstrated that chronic peripheral joint injury such as CAI negatively alters central mechanisms of motor control, leading to an increased risk of falls [27, 28]. Therefore, investigating the incidence of ankle sprain and including data relating to various populations is of clinical relevance.
The first step of the United States’ public health model of injury prevention and control [17] involves identifying the scope and magnitude of musculoskeletal injuries through injury surveillance. It is only by adopting this paradigm that methodological and intervention specificity can be achieved to meet the demands of distinct groups with the aim of injury prevention and control [17].
Therefore, identifying the scope and magnitude of ankle sprain injury stands to be advanced via the use of appropriate statistical techniques in meta-analysis of eligible studies. The aim of this systematic review and meta-analysis is to examine ankle sprain prevalence period and incidence rate unrestricted by sample activity context. This analysis will be limited to prospective studies only. Our main objectives are to determine if ankle sprain incidence rate and prevalence period is affected by age, sex and the nature of sporting activity. We will also consider whether incidence and prevalence figures are influenced by study quality. Such an analysis will meet the first criterion required to tackle issues of injury prevention and control. Surveillance of ankle sprain in a number of population types stands to elucidate the contrasting patterns of ankle sprain injury in a variety of settings.
2 Methods
The study protocol was developed using the framework outlined in the guidelines provided by the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) statement [29].
2.1 Literature Search Strategy
In July 2012, we undertook a computerised literature search of the following databases from inception: Web of Science, CINAHL, Cochrane Central Register of Controlled Trials, PEDro, Embase, PubMed and SPORTDiscus. The database search was further supplemented with a single related-citation search on PubMed (National Centre for Biotechnology Information, U.S. National Library of Medicine. Home page: http://www.ncbi.nlm.nih.gov/pubmed, Accessed July 2012)—this retrieved a set of articles closely related to ankle sprain injuries. The search strategy was designed with the purpose of extracting epidemiological studies of ankle sprain injury in multiple population groups. Recurrent sprain and CAI are pathologies frequently described in the aforementioned investigations. This was accounted for in the formulation of the following search strategy.
Population-specific and patient-specific search terms were combined using Boolean operators as follows: (1) ankle OR ‘ankle joint’, (2) injury OR injuries OR strain OR strains OR sprain OR sprains OR rupture OR ruptures OR repeated OR multiple OR recurrent OR instability OR ‘recurrent instability’ OR ‘chronic instability’ OR ‘functional instability’ OR ‘mechanical instability’, (3) ‘ankle instability’ OR ‘chronic ankle sprain’ (4) epidemiology OR epidemiologic OR epidemiological OR survey OR statistics OR pattern OR patterns OR incidence OR incidences OR prevalence OR prevalences (5) (1 AND [2 OR 3] AND 4).
The search strategy was limited to full text studies published in the English language. Published abstracts were followed up for full-text publication, but were not included as independent papers.
One investigator (CD) reviewed all the titles produced by the database searches, and retrieved suitable abstracts. Implied suitability via abstract review dictated the retrieval of full texts. These were included in the review if they fulfilled the required selection criteria.
2.2 Selection Criteria
No blinding of study author, place of publication, or results occurred. The following inclusion criteria were used.
-
(1)
The study must report epidemiology findings of injuries sustained in an observed sample.
-
(2)
The study must report ankle sprain injury with either incidence rate or prevalence period among the surveyed sample, or provide sufficient data from which these figures could be calculated.
-
(3)
The study design must be prospective.
No restrictions were placed on the participant age, sex or activity level. Review articles and individual case studies were excluded. Abstracts from conferences were not reviewed for inclusion because of their limited availability in the electronic databases.
2.3 Assessment of Study Quality
Two authors (CD and CB) evaluated study quality, which gives an indication of risk of bias. Study quality was assessed using an adapted version of the STROBE guidelines for rating observational studies [30]. All included studies were rated on 11 specific criteria which were derived from items 5, 6, 7, 8, 9, 12, 14 and 15 of the original checklist (Table 1).
The observational studies were considered as having a low risk of bias if they were determined as high quality (score of ≥7/11) or a high risk of bias if they were low quality (≤6/11). The classification scores for the determination of high- and low-quality papers were established by author consensus. Final study ratings for each reviewer were collated and examined for discrepancies. Any inter-rater disagreement was resolved by consensus decision. Once consensus was reached for all study ratings, overall quality scores were collated by summing those criteria, providing a score out of 11.
2.4 Data Management and Statistical Analysis
Three authors (CD, CB and ED) extracted key data onto a commercially available software package (Excel, Microsoft Corporation, Redmond, WA, USA). Studies were classified by injury focus (whether injuries of all types or ankle injuries in isolation were reported), sample demographics (region, age group, period of completion, sample size, sex, context activity), method of diagnosis (independent trained healthcare worker, author or subject report) and duration (number of seasons). Data relating to prevalence period and incidence rate were recorded for the subgroups of quality (high, low), sex (male, female), age (child, adolescent, adult) and activity (field sports, ice and water sports, court sports, outdoor sports).
Prevalence period represents the ratio of the number of events (ankle sprains) existing in a population over a specified time to the study population in that time. Incidence rate is the ratio of the number of events commencing during a specified time to the average population during the same period of time.
Articles reporting incidence were divided according to the unit of exposure used (e.g., per 1,000 athlete exposures or per 1,000 h). In situations where data was presented in other forms (e.g., per 10,000 units of exposure), efforts were made to synthesize data by converting them to a common unit of exposure where possible. Cumulative incidence rate figures combined the units of athlete exposure and hours of exposure to provide a resultant value. In the presence of any unclear or missing data, authors were contacted by email for clarification.
In instances of provision of data pertaining to the specific diagnosis of the ankle sprain by individual papers, a weighted percentage was calculated.
Weighted percentage was calculated using the following formula.
2.4.1 Meta-Analysis
For each study, standard error and variance were calculated for prevalence period and incidence rate estimates. Individual study estimates were then pooled based on the following subgroups: study quality, sex, age and sport category.
The study quality subgroup was classified into two categories: high quality (≥7/11) or low quality (≤6/11). Sex was classified as male or female based on a surveyed sample of 60–100 % male or female subjects, respectively. Age was classified by three broad categories: children (aged 0 to ≤12 years); adolescent (aged ≥13 to ≤17 years); adult (aged ≥18 years). Sport was categorised by field, indoor/court, ice/water and outdoor sports (Table 2).
Studies were weighted by sample size and separate analyses were undertaken for prevalence period and incidence rate data. Data were then assessed for heterogeneity using Microsoft Excel 2010 [31], based on the Q test in conjunction with the I 2 statistic. The significance for Chi-square was set at p < 0.1. The I 2 statistic was used to quantify inconsistency using the formula: I 2 = [(Qdf)/Q] × 100 %, where Q is the Chi-square statistic and df its degrees of freedom. I 2 values greater than 50 % were considered to represent substantial heterogeneity [32]. In cases where substantial heterogeneity was present, a random effects model was used for meta-analysis. Accordingly, prevalence and incidence were used to enable several Forest plots. A 95 % CI was used in the analysis.
3 Results
3.1 Search Strategy
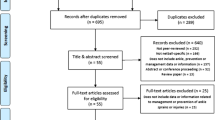
The search strategy returned a total of 10,524 articles for review. Articles were included based on a group consensus. Refer to Fig. 1 for information pertaining to the total number of studies screened, assessed for eligibility and included in the analysis (with reasons for exclusions at each stage). A total of 181 prospective epidemiology studies from 144 separate papers were included in the systematic review and meta-analyses [20, 33–176].

Flow chart of the process and rationale used in selecting papers for inclusion in the review with the outlined search strategy
3.2 Characteristics of the Included Studies
Some studies consisted of entirely male (75) and female (44) samples, while a number of studies included mixed samples (36). Twenty-six studies included mixed samples but did not report the distribution of males and females, and therefore were not included in the analysis by sex.
One hundred and twenty-two of the 181 studies had adult-only samples, 25 had adolescent-only samples and 11 had children-only samples. A number of studies had mixed samples: adults, adolescents and children combined (10), adults and adolescents only (3) or children and adolescents only (4). Six studies were unclear of their sample age demographics, and therefore were not included in the analysis by age.
Ninety-four of the included studies reported injury as a function of exposure. Eighty-seven studies reported ankle sprain as a percentage of all injuries. Of the 94 studies that did report exposure, 42 reported ankle sprain per 1,000 athlete exposures, 44 per 1,000 h, 5 per 1,000 days, and 1 each per 1,000 jumps, player games and person years. All except 16 of these 94 studies also reported ankle sprain period prevalence.
Similarly, the nature of injury diagnosis differed substantially between studies. 153 studies used the diagnosis of an independent medical professional, 4 used that of the authors themselves, 4 used coaches, 11 used the subjects’ own report and 7 used a mix of all.
One hundred and seventy-three studies reported on sporting populations and the remaining eight included military populations.
Twenty-one (12 %) papers included a surveyed sample of 0–100 participants, 75 (41 %) had 100–200 participants, 19 (10 %) had 500–1,000 participants, 17 (9 %) had 1,000–2,000 participants, 14 (8 %) had 2,000–5,000 participants, 25 (14 %) had 5,000–10,000 participants and 10 (6 %) had over 10,000 participants. A group of authors responsible for 13 of the included studies was contacted to provide clarification of their surveyed sample sizes.
The total number of sports analysed was 37.
Five papers reported re-sprains within the surveyed sample. Three of these five were surveying ankle sprain injuries in isolation [55, 62, 177] and two reported ankle sprains among all injuries [96, 114]. For the purposes of prevalence period and incidence rate estimates, the total number of sprains/re-sprains were used in the prevalence period and incidence rate calculations.
4 Methodological Quality
The average rating of all the included studies was 6.67/11 (6.94 for all the male studies, 7.41 for all the female studies and 5.81 for all the studies with mixed sex samples; 6.57 for all studies with only child samples, 7.56 for adolescent-only samples and 6.64 for adult-only samples). 116 studies were considered high quality (≥7/11), having a low risk of bias, and 65 were considered low quality (≤6/11), having a high risk of bias. Consensus was reached for all items on initial discussion. No studies were excluded from analysis based on the rating of methodological quality.
4.1 Meta-Analysis Findings
Figures 2, 3, 4, 5, 6, 7, 8 and Table 3 present pooled estimates (95 % CIs) for each sub-group. There was a high degree of heterogeneity across studies within each of the subgroups (p < 0.01), and random effects models were used in all cases.
Indoor and court sports were the highest risk activity, based on cumulative incidence and prevalence figures, whereas outdoor sports presented the lowest risk activity subgroup. Females were more likely to sustain an ankle sprain than males, and children more likely than adolescents and adults.
4.1.1 Study Quality
High quality (≥7/11) studies had a pooled cumulative incidence rate of 11.55 per 1,000 exposures (95 % CI 11.54–11.55) and a pooled prevalence period of 11.88 % (95 % CI 10.56–13.19). Pooled incidence rate figures were reduced in low quality (≤6/11) studies with 0.54 ankle sprains per 1,000 exposures (95 % CI 0.49–0.59) and a pooled prevalence of 11.19 % (95 % CI 6.59–15.78). See Fig. 2.

Ankle sprain incidence estimates by quality. Vertical bars represent overall effect size estimates, and horizontal bars represent 95 % confidence intervals, and give an indication of the study weight (smaller width = larger weight)
4.1.2 Sex
Meta-analysis for sex revealed a cumulative incidence rate of 13.6 per 1,000 exposures (95 % CI 13.25–13.94) for females and 6.94 per 1,000 exposures (95 % CI 6.8–7.09) for males. Incidence figures for sex were also calculated separately per 1,000 h and per 1,000 athlete exposures. Pooled prevalence of ankle sprains was 10.55 % (95 % CI 10.84–11.15) in females and 10.99 % (95 % CI 10.84–11.15) for males. See Figs. 3 and 4.

Ankle sprain incidence estimates by sex. Vertical bars represent overall effect size estimates, and horizontal bars represent 95 % confidence intervals, and give an indication of the study weight (smaller width = larger weight)

Ankle sprain prevalence estimates by sex. Horizontal bars represent 95 % confidence intervals, and give an indication of the study weight (smaller width = larger weight)
4.1.3 Age
Meta-analysis for age sub-groups revealed a pooled cumulative incidence of 0.72 per 1,000 exposures (95 % CI 0.67–0.77) in adults, 1.94 (95 % CI 1.73–2.14) for adolescents and 2.85 (95 % CI 2.51–3.19) for children. A total of 12.62 % of all injuries were ankle sprains in children (95 % CI 11.81–13.43), 10.55 % in adolescents (95 % CI 9.92–11.17) and 11.41 % (95 % CI 11.28–11.54) in adults (see Figs. 5 and 6).

Ankle sprain incidence estimates by age. Vertical bars represent overall effect size estimates, and horizontal bars represent 95 % confidence intervals, and give an indication of the study weight (smaller width = larger weight)

Ankle sprain prevalence estimates by age. Horizontal bars represent 95 % confidence intervals, and give an indication of the study weight (smaller width = larger weight)
4.1.4 Sport
Pooled cumulative incidence was 7 ankle sprains per 1,000 exposures (95 % CI 6.8–7.2) for court sports, 3.7 per 1,000 exposures (95 % CI 3.3–4.17) for ice/water sports, 1.0 per 1,000 exposures (95 % CI 0.95–1.05) for field sports and 0.88 per 1,000 exposures (95 % CI 0.73–1.02) for outdoor sports. There was a high degree of heterogeneity in all subgroups. We found similar findings when incidence data was reported based on exposures per 1,000 h and per 1,000 athlete exposures.
Pooled prevalence of ankle sprain for indoor/court sports was 12.17 % (95 % CI 12.01–12.33), 4.36 % for water/ice sports (95 % CI 3.92–4.79), 11.3 % for field-based sports (95 % CI 11.15–11.44) and 11.65 % for outdoor pursuits sports (95 % CI 11.33–11.97); see Figs. 7 and 8.

Ankle sprain incidence estimates by sport. Vertical bars represent overall effect size estimates, and horizontal bars represent 95 % confidence intervals, and give an indication of the study weight (smaller width = larger weight)

Ankle sprain prevalence estimates by sport. Horizontal bars represent 95 % confidence intervals, and give an indication of the study weight (smaller width = larger weight)
4.1.5 Sprain Diagnosis
Eleven of the 181 included studies reported specific diagnoses pertaining to the type of ankle sprain incurred by the surveyed sample (lateral, medial or syndesmotic). Four of these studies were investigating lateral/inversion sprains in isolation; one reported incidence as a percentage of all injuries (and not by specific sprain diagnosis) and therefore could not be considered for this aspect of analysis.
Data collected from the six included studies identified a weighted prevalence period of 15.31 for lateral ankle sprains. Lateral ankle sprain was also the most commonly incurred type of ankle sprain based on incidence rate units of athlete exposure, years and hours when compared with medial and syndesmotic ankle sprains (Table 4).
4.1.6 Military Populations
Seven studies with entirely military samples were included in the analysis. Each paper surveying military population subgroups employed unique methods of reporting exposure. The risk of ankle sprain was determined per 1,000 (parachute) jumps (3.8 lateral ankle sprains per 1,000 jumps; 1.08 syndesmotic sprains per 1,000 jumps), per 1,000 person-years (58.4 per 1,000 person-years) and as a percentage (2.8 % in one study, and 17.7 % in another).
5 Discussion
The search strategy identified data pertaining to the incidence rate and prevalence period of ankle sprain in a variety of settings from 181 prospective studies in 144 separate research papers. Injury patterns were reported for 37 different sports and military populations (174 studies were sports-related and 7 were military-related). Separate meta-analyses were completed for incidence rate and prevalence period data for the subgroups of age, sex, sport and study quality, thus providing evidence for the highest risk activities and populations. Results of these analyses identify the scope and magnitude of ankle sprain injury, thus allowing for methodological and intervention specificity to meet the demands of distinct groups.
Findings from this review revealed a wide variation in ankle sprain incidence estimates, and meta-analyses indicate that females and children were the highest risk population subgroups for sustaining an ankle sprain, with indoor and court sports the highest risk activity. Furthermore, studies with a high risk of bias underestimated the risk of ankle sprain. The meta-analysis revealed minimal variation in ankle sprain prevalence related to the sample subgroups. The prevalence of ankle sprain was equal between males and females, between studies of high and low bias, and between age sub-groups. Ice and water sports had the lowest overall prevalence within the sport subcategory.
We devised a rating system for the purpose of determining the methodological quality of the included studies. Assessing the quality of observational epidemiology research has been the focus for a number of research groups [178–182]. Hagglund et al. [183] outline key attributes that an epidemiological study should possess, recommending that the design should be prospective, with a clear definition of injury (prospective studies provide a more realistic representation of injury patterns as a result of superior experimental control and data collection techniques), whereby exposure data is collected over the course of at least one entire season [183]. Our rating system was a modified version of the STROBE guidelines for rating observational studies [30], and was based on 11 separate variables. We considered this checklist of 11 items essential for good reporting of these observational studies, thus facilitating a feasible means to assess the quality and potential bias of 181 studies.
Meta-analysis of the cumulative incidence rate and prevalence period data by study quality revealed clear differences between high-and low-quality papers. One hundred and sixteen studies were considered high quality and 65 were considered low quality based on this system. Only two studies scored full marks on the criteria outlined, with nine studies scoring 10/11. The pooled estimate of ankle sprain incidence rate in low-quality studies (0.54 per 1,000 cumulative units of exposure) was 21 times less than that of high-quality studies (11.55 per 1,000 cumulative units of exposure). Very few of the included studies adhered to the criteria described by Hagglund et al. [183]. A potential reason for the tendency of lower quality studies (as measured by our rating system) to underestimate the incidence rate of ankle sprain injury could relate to the absence of a medical professional to appropriately diagnose potential injuries. Indeed, 12 of the included low-quality studies did not use an independent medical professional for the diagnosis of injuries in the surveyed sample, with coaches, authors or subjects themselves reporting injury, raising concerns over internal validity secondary to investigator error through reporting bias. Additionally, the lack of a qualified medical professional will corrupt the definition and classification of injury (Table 1; criteria 1 and 3). Considering the high rate of morbidity following an acute ankle sprain [2, 3], the consequences of this methodological inadequacy could theoretically put the injured population at risk of prolonged lifestyle-limiting symptoms secondary to the absence of astute intervention in the acute phase of injury.
Findings of the meta-analysis of cumulative incidence rate and prevalence period by sex elucidated a higher risk of ankle sprain in females compared with males. Of the 94 studies that did report exposure figures for sex, 42 reported ankle sprain per 1,000 athlete exposures and 44 reported ankle sprain per 1,000 h, giving a cumulative incidence rate of 13.6 sprains per 1,000 exposures for females versus 6.94 per 1,000 exposures for males. Sex was the only sub-group whereby sufficient data existed to analyse incidence rate per cumulative exposures, and per hour and athlete exposure separately. Thirty-six of the included studies had mixed-sex samples, reporting the exact sample size with specific details of the number of male and female participants. Fifteen of these 36 studies reported injury as a function of exposure (hours or athlete exposures); six reported no differences in injury rates between males and females [63, 79, 140, 184, 93, 171], two reported a higher risk of injury for men [56, 113] and two a higher risk for women [95, 144]. Two papers did not report separate injury data for males and females [105, 131] (five separate studies). Differences in study design, such as definition of the injury or different data collection methods, may explain these contradictory results.
Women have been reported to sustain more knee joint injuries than men, especially anterior cruciate ligament injuries [185]. However, to the authors’ knowledge, this is the first meta-analysis to determine a higher incidence rate of ankle sprain in females compared with males. Efforts to prevent ankle sprain injury in females should therefore focus on the factors that increase the susceptibility of women to injury and, furthermore, to developing interventions to facilitate the prevention of these injuries. The anatomical [186–188], hormonal [188–190] and neuromuscular [190–192] differences that exist between the sexes [193] do not necessarily explain the observed increased risk of ankle sprain in females; this analysis serves to expose possible differences in injury risks between the sexes, but can only hypothesize as to their cause. Future research could focus on whether sex differences are activity-specific, and thus related to training behaviours, or whether the difference in risk is related to anatomical or physiological sex differences.
The existence of a higher risk of ankle sprain in children compared with adolescents (2.85 vs 1.94 per 1,000 exposures) and adolescents compared with adults (1.94 vs 0.72 per 1,000 exposures) as demonstrated by the meta-analysis is a significant finding, as injury at a young age can negatively affect a child’s ability to participate in activity and may trigger long-term sequelae such as early onset of osteoarthritis [194, 195]. None of the included studies surveyed a sample of children, adolescents and adults giving specific data relating to exposure and number of ankle sprains for each distinct age group. Childhood and adolescence are considered to be periods of development in which the individual is at an amplified risk of injury [196]. Appropriate neuromuscular control is ubiquitous to the successful completion of dynamic sporting manoeuvres. Whereas preferred patterns of coordination are established in adults [197, 198], young children do not show the same consistency in patterns of coordination [199]. Similarly, increased ‘motor awkwardness’ during adolescence may result from an immaturely developed sensorimotor system, thus increasing the challenge of even simple motor control tasks [195]. The increased risk of ankle sprain in children and adolescents compared with adults could therefore be the result of a developing dynamic motor control system exploring the state space of movement patterns prior to settling in a number of preferred movement ‘attractor’ states [200, 201].
Meta-analysis by sport category revealed that indoor and court sports (7 per 1,000 cumulative exposures) had the highest risk of ankle sprain followed by ice and water sports (3.7 per 1,000 cumulative exposures), field sports (0.9 per 1,000 exposures) and finally outdoor sports (0.87 per 1,000 exposures). Pooled prevalence estimates revealed that ice/water sports had the lowest prevalence of ankle sprains of the four sub-groups of sport. The high incidence rate combined with low prevalence period can be explained by a higher overall incidence of injury in these sports but a greater tendency toward shoulder, knee and predominantly head injuries [33, 34].
Several studies not included in our analysis have previously reported that ankle sprain is one of the most common, if not the most common, injury in indoor and court sports such as basketball [202–208], volleyball [209–212], tennis [94, 213, 214] and wrestling [215–217], thus explaining the trend for a higher risk of ankle sprain in indoor/court sports. There is also an abundance of literature investigating injury epidemiology in field-based sports (98 of the studies included in our analysis were field-based focused). The high risk of ankle sprain has promoted an appropriate research response, as a large number of methodologically rigorous randomised control trials now exist investigating the effect of different interventions in injury rehabilitation [53, 218–221] and prevention [222–224].
In contrast to the clear disparity illustrated by the meta-analyses of incidence rate estimates between the subcategories of quality, sex, age and sport, meta-analyses of the same sub-categories elucidated very similar prevalence period estimates.
Prevalence is a measure independent of exposure. Ninety-seven of 181 studies reported injury as a function of exposure. By incorporating exposure in the calculation of injury rates across a surveyed sample, incidence rate determines the number of events of interest occurring per projected amount of activity undertaken, thus providing an estimation of risk. In contrast, prevalence is a ratio of the number of the surveyed sample incurring an ankle sprain to the total sample, and is independent to the amount of activity undertaken. A possible reason for the contrasting findings between incidence rate and prevalence period is that in a given group or activity the proportion of people who sustain ankle sprains is similar, but the introduction of exposure separates these groups via the determination of risk per unit of activity completed; females and children are at a higher risk of sustaining an ankle sprain per exposure in the same activities compared with males or adolescents and adults, respectively. The disparity of incidence rate estimates by study quality and the lack thereof regarding prevalence period estimates cannot, however, be explained by the introduction of a unit of exposure. Rather, we propose that a study of higher quality will be predisposed to a more accurate determination of injury as a function of exposure, both in the correct and appropriate diagnosis of injury and the evaluation of levels of exposure for each surveyed subject.
Findings from the systematic review indicate that of the three most common clinical classifications of ankle sprain, lateral ankle sprain presents the greatest risk, followed by syndesmotic (high) ankle sprain and finally deltoid (medial) ligament sprain (based on incidence rate figures for exposure units of athlete exposure, year and hour). Only 6 of the 181 included studies reported sprain diagnosis without focusing on ankle sprain injury in isolation, giving sufficient data to determine incidence rate and/or prevalence period [44, 96, 143, 154, 225]. Both a muscle-driven computer simulation [226] and a cadaveric model [227] have shown that plantarflexion and inversion increase strain on the lateral ligaments of the ankle. The higher risk of sustaining a lateral ligament sprain can be attributed to relative lower load to failure rate of the lateral ligamentous complex when compared with the medial and syndesmotic ligament groups [228] and reduced arthrokinematic restriction credited to decreased contact of the talus within the ankle mortise in the plantar-flexed and inverted position [229].
The systematic review identified that injury surveillance in military populations utilised varying measures of exposure, limiting the pooling of data. Seven studies were included in the review investigating military samples [20, 42, 44, 225, 230–232]. Ankle sprain was reported per 1,000 (parachute) jumps (3.8 lateral ankle sprains per 1,000 jumps; 1.08 syndesmotic sprains per 1,000 jumps) [44], per 1,000 person-years (58.4 per 1,000 person years) [163] and as a percentage (2.8 % in one study [42], and 17.7 % in another [20]).
These data outline the extent to which ankle sprain injury is a persistent and primary health concern for military populations; an abundance of available military epidemiology research also exists that did not meet our inclusion criteria. Six papers surveying military populations were excluded from our analysis as they were retrospective in design [19, 233–237]. In accordance with this, several intervention studies have been conducted with the primary aim of reducing the incidence of ankle sprains in military populations [44, 238].
This is the first systematic review to incorporate meta-analyses of data from epidemiological studies relating to ankle sprain injury. A similar review was published in 2007 and included studies from 1977 to 2005 [239]. Apart from the incorporation of meta-analyses of injury data, several key factors separate this study from the study by Fong et al. [239]. The review by Fong et al. did not use a rating system for the included studies and did not report specific data relating to sprain diagnosis. Another key difference is that for studies that reported the injury incidence for several body sites, the combined percentages were divided evenly for each included body site, thus introducing a critical source of bias. Furthermore, the search undertaken for the present study was completed in July 2012, and as such adds over 6 years of prospective evidence to the results presented in the review by Fong et al. [239].
Despite the strengths of this systematic review and meta-analyses, it is important to consider several limitations when interpreting the results. Studies were not included if they were published in non-English languages, which may influence the outcomes of our analyses, despite the probability that authors of high quality surveys would aim for publication in high-impact journals published in the English language in the pursuit of superior dissemination of output data.
It was also our intention to adhere to the framework outlined in the guidelines provided by the PRISMA statement [29]. With specific reference to criteria 15 relating to the assessment of publication bias, we encountered difficulty in assessing and establishing the possibility of selective reporting of outcomes by individual studies. It was unfeasible to check if all the included 144 papers had published a protocol prior to their collection of data and compare the predicted outcomes to those published to determine any discrepancy. Furthermore, as required by our outlined inclusion criteria, all included studies reported the primary outcome—incidence rate or prevalence period, so there is no risk of selective reporting at an individual study level. Funnel plotting to determine cumulative risk of publication bias was considered to be more applicable to reviews involving interventional type studies, rather than descriptive epidemiology.
A number of methodological issues were identified among the included studies that should be addressed in future observational studies. Only one study scored full marks on the checklist developed for this analysis. We would recommend that epidemiological studies standardise their reporting according to the STROBE guidelines for reporting observational studies [30], thus allowing for proper interpretation of the available data to produce better estimates of incidence rate and prevalence period of ankle sprain injury [240].
6 Conclusions
Female sex, lower age and athletes competing in indoor and court sports are the subgroups most at risk of ankle sprain. Lower quality studies are more likely to underestimate the risk of ankle sprain. Participants were at a significantly higher risk of sustaining a lateral ankle sprain compared with syndesmotic and medial ankle sprains. This analysis provides valuable information for researchers internationally in studies of epidemiology and intervention.
References
Cooke MW, Lamb SE, Marsh J, Dale J. A survey of current consultant practice of treatment of severe ankle sprains in emergency departments in the United Kingdom. Emerg Med J. 2003;20(6):505–7.
Braun BL. Effects of ankle sprain in a general clinic population 6 to 18 months after medical evaluation. Arch Fam Med. 1999;8(2):143–8.
Kerkhoffs GM, Rowe BH, Assendelft WJ, Kelly K, Struijs PA, van Dijk CN. Immobilisation and functional treatment for acute lateral ankle ligament injuries in adults. Cochrane Database Syst Rev. 2002(3):CD003762. doi:10.1002/14651858.cd003762.
Birrer RB, Fani-Salek MH, Totten VY, Herman LM, Politi V. Managing ankle injuries in the emergency department. J Emerg Med. 1999;17(4):651–60.
Wilkerson GB, Horn-Kingery HM. Treatment of the inversion ankle sprain: comparison of different modes of compression and cryotherapy. J Orthop Sports Phys Ther. 1993;17(5):240–6.
McGowan RW, Pierce EF, Williams M, Eastman NW. Athletic injury and self diminution. J Sports Med Phys Fitness. 1994;34(3):299–304.
Smith RW, Reischl SF. Treatment of ankle sprains in young athletes. Am J Sports Med. 1986;14(6):465–71.
Gerber JP, Williams GN, Scoville CR, Arciero RA, Taylor DC. Persistent disability associated with ankle sprains: a prospective examination of an athletic population. Foot Ankle Int. 1998;19(10):653–60.
Verhagen RA, de Keizer G, van Dijk CN. Long-term follow-up of inversion trauma of the ankle. Arch Orthop Trauma Surg. 1995;114(2):92–6.
van Rijn RM, van Os AG, Bernsen RM, Luijsterburg PA, Koes BW, Bierma-Zeinstra SM. What is the clinical course of acute ankle sprains? A systematic literature review. Am J Med. 2008;121(4):324–31 e6. doi:10.1016/j.amjmed.2007.11.018.
Hertel J. Functional anatomy, pathomechanics, and pathophysiology of lateral ankle instability. J Athl Train. 2002;37(4):364–75.
Delahunt E, Coughlan GF, Caulfield B, Nightingale EJ, Lin CW, Hiller CE. Inclusion criteria when investigating insufficiencies in chronic ankle instability. Med Sci Sports Exerc. 2010;42(11):2106–21. doi:10.1249/MSS.0b013e3181de7a8a.
de Bie RA, de Vet HC, van den Wildenberg FA, Lenssen T, Knipschild PG. The prognosis of ankle sprains. Int J Sports Med. 1997;18(4):285–9. doi:10.1055/s-2007-972635.
Verhagen EA, van Tulder M, van der Beek AJ, Bouter LM, van Mechelen W. An economic evaluation of a proprioceptive balance board training programme for the prevention of ankle sprains in volleyball. Br J Sports Med. 2005;39(2):111–5. doi:10.1136/bjsm.2003.011031.
Lauder TD, Baker SP, Smith GS, Lincoln AE. Sports and physical training injury hospitalizations in the army. Am J Prev Med. 2000;18(3 Suppl):118–28.
Songer TJ, LaPorte RE. Disabilities due to injury in the military. Am J Prev Med. 2000;18(3 Suppl):33–40.
Sell TC, Abt JP, Crawford K, Lovalekar M, Nagai T, Deluzio JB, et al. Warrior model for human performance and injury prevention: Eagle Tactical Athlete Program (ETAP) Part I. J Spec Oper Med. 2010;10(4):2–21.
Bar-Dayan Y. Parachuting injuries: a retrospective study of 43,542 military jumps. Mil Med. 1998;163(1):1–2.
Billings CE. Epidemiology of injuries and illnesses during the United States Air Force Academy 2002 Basic Cadet Training program: documenting the need for prevention. Mil Med. 2004;169(8):664–70.
Milgrom C, Shlamkovitch N, Finestone A, Eldad A, Laor A, Danon YL, et al. Risk factors for lateral ankle sprain: a prospective study among military recruits. Foot Ankle Int. 1991;12(1):26–30.
Lillywhite LP. Analysis of extrinsic factor associated with 379 injuries occurring during 34,236 military parachute descents. J R Army Med Corps. 1991;137(3):115–21.
Kragh JF Jr, Taylor DC. Parachuting injuries: a medical analysis of an airborne operation. Mil Med. 1996;161(2):67–9.
Hiller CE, Nightingale EJ, Raymond J, Kilbreath SL, Burns J, Black DA, et al. Prevalence and impact of chronic musculoskeletal ankle disorders in the community. Arch Phys Med Rehabil. 2012;93(10):1801–7. doi:10.1016/j.apmr.2012.04.023.
Valderrabano V, Hintermann B, Horisberger M, Fung TS. Ligamentous posttraumatic ankle osteoarthritis. Am J Sports Med. 2006;34(4):612–20.
Hirose K, Murakami G, Minowa T, Kura H, Yamashita T. Lateral ligament injury of the ankle and associated articular cartilage degeneration in the talocrural joint: anatomic study using elderly cadavers. J Orthop Sci. 2004;9(1):37–43. doi:10.1007/s00776-003-0732-9.
Croy T, Saliba SA, Saliba E, Anderson MW, Hertel J. Differences in lateral ankle laxity measured via stress ultrasonography in individuals with chronic ankle instability, ankle sprain copers, and healthy individuals. J Orthop Sports Phys Ther. 2012;42(7):593–600. doi:10.2519/jospt.2012.3923.
Hass CJ, Bishop MD, Doidge D, Wikstrom EA. Chronic ankle instability alters central organization of movement. Am J Sports Med. 2010;38(4):829–34. doi:10.1177/0363546509351562.
Wikstrom EA, Bishop MD, Inamdar AD, Hass CJ. Gait termination control strategies are altered in chronic ankle instability subjects. Med Sci Sports Exerc. 2010;42(1):197–205. doi:10.1249/MSS.0b013e3181ad1e2f.
LA Moher D, Tetzlaff J, et al. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Br Med J. 2009;339:332–6.
von Elm E, Altman DG, Egger M, et al. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. J Clin Epidemiol. 2008;61(4):344–9.
Neyeloff JL, Fuchs SC, Moreira LB. Meta-analyses and Forest plots using a microsoft excel spreadsheet: step-by-step guide focusing on descriptive data analysis. BMC Res Notes. 2012;20(5):52–8.
Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ. 2003;327(7414):557–60.
Agel J, Dick R, Nelson B, Marshall SW, Dompier TP. Descriptive epidemiology of collegiate women’s ice hockey injuries: National Collegiate Athletic Association Injury Surveillance System, 2000–2001 through 2003–2004. J Athl Train. 2007;42(2):249–54.
Agel J, Dompier TP, Dick R, Marshall SW. Descriptive epidemiology of collegiate men’s ice hockey injuries: National Collegiate Athletic Association Injury Surveillance System, 1988–1989 through 2003–2004. J Athl Train. 2007;42(2):241–8.
Agel J, Evans TA, Dick R, Putukian M, Marshall SW. Descriptive epidemiology of collegiate men’s soccer injuries: National Collegiate Athletic Association Injury Surveillance System, 1988–1989 through 2002–2003. J Athl Train. 2007;42(2):270–7.
Agel J, Olson DE, Dick R, Arendt EA, Marshall SW, Sikka RS. Descriptive epidemiology of collegiate women’s basketball injuries: National Collegiate Athletic Association Injury Surveillance System, 1988–1989 through 2003–2004. J Athl Train. 2007;42(2):202–10.
Agel J, Palmieri-Smith RM, Dick R, Woitys EM, Marshall SW. Descriptive epidemiology of collegiate women’s volleyball injuries: National Collegiate Athletic Association injury surveillance system, 1988–1989 through 2003–2004. J Athl Train. 2007;42(2):295–302.
Agel J, Ransone J, Dick R, Oppliger R, Marshall SW. Descriptive epidemiology of collegiate men’s wrestling injuries: National Collegiate Athletic Association Injury Surveillance System, 1988–1989 through 2003–2004. J Athl Train. 2007;42(2):303–10.
Albright JP, Powell JW, Martindale A, Black R, Crowley E, Schmidt P, et al. Injury patterns in big ten conference football. Am J Sports Med. 2004;32(6):1394–404. doi:10.1177/0363546504264159.
Almeida SA, Trone DW, Leone DM, Shaffer RA, Patheal SL, Long K. Gender differences in musculoskeletal injury rates: a function of symptom reporting? Med Sci Sports Exerc. 1999;31(12):1807–12.
Alonso JM, Tscholl PM, Engebretsen L, Mountjoy M, Dvorak J, Junge A. Occurrence of injuries and illnesses during the 2009 IAAF World Athletics Championships. Br J Sports Med. 2010;44(15):1100–5. doi:10.1136/bjsm.2010.078030.
Amako M, Oda T, Masuoka K, Yokoi H, Campisi P. Effect of static stretching on prevention of injuries for military recruits. Mil Med. 2003;168(6):442–6.
Amamilo SC, Samuel AW, Hesketh KT, Moynihan FJ. A prospective study of parachute injuries in civilians. J Bone Joint Surg Br. 1987;69(1):17–9.
Amoroso PJ, Ryan JB, Bickley B, Leitschuh P, Taylor DC, Jones BH. Braced for impact: reducing military paratroopers’ ankle sprains using outside-the-boot braces. J Trauma. 1998;45(3):575–80.
Andersen TE, Floerenes TW, Arnason A, Bahr R. Video analysis of the mechanisms for ankle injuries in football. Am J Sports Med. 2004;32(1 Suppl):69S–79S.
Aoki H, O’Hata N, Kohno T, Morikawa T, Seki J. A 15-year prospective epidemiological account of acute traumatic injuries during official professional soccer league matches in Japan. Am J Sports Med. 2012;40(5):1006–14. doi:10.1177/0363546512438695.
Arnason A, Tenga A, Engebretsen L, Bahr R. A prospective video-based analysis of injury situations in elite male football—football incident analysis. Am J Sports Med. 2004;32(6):1459–65. doi:10.1177/0363546504262973.
Junge A, Dvorak J. Injury risk of playing football in Futsal World Cups. Br J Sports Med. 2010;44(15):1089–92. doi:10.1136/bjsm.2010.076752.
Backous DD, Friedl KE, Smith NJ, Parr TJ, Carpine WD Jr. Soccer injuries and their relation to physical maturity. Am J Dis Child. 1988;142(8):839–42.
Bahr R, Bahr IA. Incidence of acute volleyball injuries: a prospective cohort study of injury mechanisms and risk factors. Scand J Med Sci Sports. 1997;7(3):166–71.
Baumhauer JF, Alosa DM, Renstrom FH, Trevino S, Beynnon B. A prospective study of ankle injury risk factors. Am J Sports Med. 1995;23(5):564–70.
Beneka A, Malliou P, Gioftsidou A, Tsigganos G, Zetou H, Godolias G. Injury incidence rate, severity and diagnosis in male volleyball players. Sport Sci Health. 2010;5(3):93–9.
Bennell K. Neuromuscular training reduces the risk of leg injuries in female floorball players. Aust J Physiother. 2008;54(4):282.
Beynnon BD, Renstrom PA, Alosa DM, Baumhauer JF, Vacek PM. Ankle ligament injury risk factors: a prospective study of college athletes. J Orthop Res. 2001;19(2):213–20. doi:10.1016/s0736-0266(00)90004-4.
Beynnon BD, Vacek PM, Murphy D, Alosa D, Paller D. First-time inversion ankle ligament trauma: the effects of sex, level of competition, and sport on the incidence of injury. Am J Sports Med. 2005;33(10):1485–91. doi:10.1177/0363546505275490.
Bird YN, Waller AE, Marshall SW, Alsop JC, Chalmers DJ, Gerrard DF. The New Zealand Rugby Injury and Performance Project: V. Epidemiology of a season of rugby injury. Br J Sports Med. 1998;32(4):319–25.
Bottini E, Poggi EJT, Luzuriaga F, Secin FP. Incidence and nature of the most common rugby injuries sustained in Argentina (1991–1997). Br J Sports Med. 2000;34(2):94–7. doi:10.1136/bjsm.34.2.94.
Brito J, Rebelo A, Soares JM, Seabra A, Krustrup P, Malina RM. Injuries in youth soccer during the preseason. Clin J Sport Med. 2011;21(3):259–60. doi:10.1097/JSM.0b013e31821a6025.
Brooks JH, Fuller CW, Kemp SP, Reddin DB. Epidemiology of injuries in English professional rugby union: part 2 training Injuries. Br J Sports Med. 2005;39(10):767–75. doi:10.1136/bjsm.2005.018408.
Brooks JH, Fuller CW, Kemp SP, Reddin DB. Epidemiology of injuries in English professional rugby union: part 1 match injuries. Br J Sports Med. 2005;39(10):757–66. doi:10.1136/bjsm.2005.018135.
Brudvik C. Injuries caused by small wheel devices. Prev Sci. 2006;7(3):313–20. doi:10.1007/s11121-006-0031-8.
Cloke DJ, Ansell P, Avery P, Deehan D. Ankle injuries in football academies: a three-centre prospective study. Br J Sports Med. 2011;45(9):702–8. doi:10.1136/bjsm.2009.067900.
Cumps E, Verhagen E, Meeusen R. Efficacy of a sports specific balance training programme on the incidence of ankle sprains in basketball. J Sports Sci Med. 2007;6(2):212–9.
Dick R, Ferrara MS, Agel J, Courson R, Marshall SW, Hanley MJ, et al. Descriptive epidemiology of collegiate men’s football injuries: National Collegiate Athletic Association Injury Surveillance System, 1988–1989 through 2003–2004. J Athl Train. 2007;42(2):221–33.
Dick R, Hertel J, Agel J, Grossman J, Marshall SW. Descriptive epidemiology of collegiate men’s basketball injuries: National Collegiate Athletic Association Injury Surveillance System, 1988–1989 through 2003–2004. J Athl Train. 2007;42(2):194–201.
Dick R, Hootman JM, Agel J, Vela L, Marshall SW, Messina R. Descriptive epidemiology of collegiate women’s field hockey injuries: National Collegiate Athletic Association Injury Surveillance System, 1988–1989 through 2002–2003. J Athl Train. 2007;42(2):211–20.
Dick R, Lincoln AE, Agel J, Carter EA, Marshall SW, Hinton RY. Descriptive epidemiology of collegiate women’s lacrosse injuries: National Collegiate Athletic Association injury surveillance system, 1988–1989 through 2003–2004. J Athl Train. 2007;42(2):262–9.
Dick R, Putukian M, Agel J, Evans TA, Marshall SW. Descriptive epidemiology of collegiate women’s soccer injuries: National Collegiate Athletic Association Injury Surveillance System, 1988–1989 through 2002–2003. J Athl Train. 2007;42(2):278–85.
Dick R, Romani WA, Agel J, Case JG, Marshall SW. Descriptive epidemiology of collegiate men’s lacrosse injuries: National Collegiate Athletic Association Injury Surveillance System, 1988–1989 through 2003–2004. J Athl Train. 2007;42(2):255–61.
Dick R, Sauers EL, Agel J, Keuter G, Marshall SW, McCarty K, et al. Descriptive epidemiology of collegiate men’s baseball injuries: National Collegiate Athletic Association Injury Surveillance System, 1988–1989 through 2003–2004. J Athl Train. 2007;42(2):183–93.
Dompier TP, Powell JW, Barron MJ, Moore MT. Time-loss and non-time-loss injuries in youth football players. J Athl Train. 2007;42(3):395–402.
Doyle C, George K. Injuries associated with elite participation in women’s rugby over a competitive season: an initial investigation. Phys Ther Sport. 2004;5(1):44–50. doi:10.1016/j.ptsp.2003.11.001.
Dvorak J, Junge A, Derman W, Schwellnus M. Injuries and illnesses of football players during the 2010 FIFA World Cup. Br J Sports Med. 2011;45(8):626–30. doi:10.1136/bjsm.2010.079905.
Dvorak J, Junge A, Grimm K, Kirkendall D. Medical report from the 2006 FIFA World Cup Germany. Br J Sports Med. 2007;41(9):578–81 (discussion 81). doi:10.1136/bjsm.2006.034579.
Dyson R, Buchanan M, Hale T. Incidence of sports injuries in elite competitive and recreational windsurfers. Br J Sports Med. 2006;40(4):346–50.
Ekstrand J, Hagglund M, Walden M. Epidemiology of muscle injuries in professional football (soccer). Am J Sports Med. 2011;39(6):1226–32. doi:10.1177/0363546510395879.
Ekstrand J, Walden M, Hagglund M. Risk for injury when playing in a national football team. Scand J Med Sci Sports. 2004;14(1):34–8.
Ekstrand J, Hagglund M, Fuller CW. Comparison of injuries sustained on artificial turf and grass by male and female elite football players. Scand J Med Sci Sports. 2011;21(6):824–32. doi:10.1111/j.1600-0838.2010.01118.x.
Emery CA, Meeuwisse WH, Hartmann SE. Evaluation of risk factors for injury in adolescent soccer implementation and validation of an injury surveillance system. Am J Sports Med. 2005;33(12):1882–91.
Faude O, Junge A, Kindermann W, Dvorak J. Injuries in female soccer players—a prospective study in the German national league. Am J Sports Med. 2005;33(11):1694–700. doi:10.1177/0363546505275011.
Feeley BT, Kennelly S, Barnes RP, Muller MS, Kelly BT, Rodeo SA, et al. Epidemiology of National Football League training camp injuries from 1998 to 2007. Am J Sports Med. 2008;36(8):1597–603. doi:10.1177/0363546508316021.
Finestone A, Novack V, Farfel A, Berg A, Amir H, Milgrom C. A prospective study of the effect of foot orthoses composition and fabrication on comfort and the incidence of overuse injuries. Foot Ankle Int. 2004;25(7):462–6.
Flik K, Lyman S, Marx RG. American collegiate men’s ice hockey: an analysis of injuries. Am J Sports Med. 2005;33(2):183–7.
Fourchet F, Horobeanu C, Loepelt H, Taiar R, Millet GP. Foot, ankle, and lower leg injuries in young male track and field athletes. Int J Athl Ther Train. 2011;16(3):19–23.
Frey C, Feder KS, Sleight J. Prophylactic ankle brace use in high school volleyball players: a prospective study. Foot Ankle Int. 2010;31(4):296–300. doi:10.3113/fai.2010.0296.
Fuller CW, Taylor A, Molloy MG. Epidemiological study of injuries in international rugby sevens. Clin J Sport Med. 2010;20(3):179–84. doi:10.1097/JSM.0b013e3181df1eea.
Gabbe BJ, Finch CF, Wajswelner H, Bennell KL. Predictors of lower extremity injuries at the community level of Australian football. Clin J Sport Med. 2004;14(2):56–63.
Garrick JG, Requa RK. Injury patterns in children and adolescent skiers. Am J Sports Med. 1979;7(4):245–8.
Gaulrapp H, Becker A, Walther M, Hess H. Injuries in women’s soccer: a 1-year all players prospective field study of the women’s Bundesliga (German premier league). Clin J Sport Med. 2010;20(4):264–71. doi:10.1097/JSM.0b013e3181e78e33.
Gibbs N. Injuries in professional rugby league. A three-year prospective study of the South Sydney Professional Rugby League Football Club. Am J Sports Med. 1993;21(5):696–700.
Giza E, Fuller C, Junge A, Dvorak J. Mechanisms of foot and ankle injuries in soccer. Am J Sports Med. 2003;31(4):550–4.
Hagglund M, Walden M, Ekstrand J. Previous injury as a risk factor for injury in elite football: a prospective study over two consecutive seasons. Br J Sports Med. 2006;40(9):767–72. doi:10.1136/bjsm.2006.026609.
Harringe ML, Renström P, Werner S. Injury incidence, mechanism and diagnosis in top-level teamgym: a prospective study conducted over one season. Scand J Med Sci Sports. 2007;17(2):115–9.
Hjelm N, Werner S, Renstrom P. Injury profile in junior tennis players: a prospective two year study. Knee Surg Sports Traumatol Arthrosc. 2010;18(6):845–50. doi:10.1007/s00167-010-1094-4.
Hosea TM, Carey CC, Harrer MF. The gender issue: epidemiology of ankle injuries in athletes who participate in basketball. Clin Orthop Relat Res. 2000;372:45–9.
Wadley GH, Albright JP. Women’s intercollegiate gymnastics. Injury patterns and “permanent” medical disability. Am J Sports Med. 1993;21(2):314–20.
Johansson C. Injuries in elite orienteers. Am J Sports Med. 1986;14(5):410–5.
Johansson C. Training, injury and disease in senior and junior elite orienteers. Sci J Orienteering. 1988;4(1):3–13.
Johnson RJ, Ettlinger CF, Campbell RJ, Pope MH. Trends in skiing injuries. Analysis of a 6-year study (1972 to 1978). Am J Sports Med. 1980;8(2):106–13.
Jones BH, Cowan DN, Tomlinson JP, Robinson JR, Polly DW, Frykman PN. Epidemiology of injuries associated with physical training among young men in the army. Med Sci Sports Exerc. 1993;25(2):197–203.
Junge A, Chomiak J, Dvorak J. Incidence of football injuries in youth players. Comparison of players from two European regions. Am J Sports Med. 2000;28(5 Suppl):S47–50.
Junge A, Dvorak J. Injuries in female football players in top-level international tournaments. Br J Sports Med. 2007;41(Suppl 1):i3–7. doi:10.1136/bjsm.2007.036020.
Junge A, Dvorak J, Graf-Baumann T. Football injuries during the World Cup 2002. Am J Sports Med. 2004;32(1 Suppl):23S–7S.
Junge A, Engebretsen L, Alonso JM, Renstrom P, Mountjoy M, Aubry M, et al. Injury surveillance in multi-sport events: the International Olympic Committee approach. Br J Sports Med. 2008;42(6):413–21. doi:10.1136/bjsm.2008.046631.
Junge A, Engebretsen L, Mountjoy ML, Alonso JM, Renstrom P, Aubry MJ, et al. Sports injuries during the Summer Olympic Games 2008. Am J Sports Med. 2009;37(11):2165–72. doi:10.1177/0363546509339357.
Junge A, Lamprecht M, Stamm H, Hasler H, Bizzini M, Tschopp M, et al. Countrywide campaign to prevent soccer injuries in swiss amateur players. Am J Sports Med. 2011;39(1):57–63. doi:10.1177/0363546510377424.
Junge A, Langevoort G, Pipe A, Peytavin A, Wong F, Mountjoy M, et al. Injuries in team sport tournaments during the 2004 Olympic Games. Am J Sports Med. 2006;34(4):565–76.
Junge A, Rosch D, Peterson L, Graf-Baumann T, Dvorak J. Prevention of soccer injuries: a prospective intervention study in youth amateur players. Am J Sports Med. 2002;30(5):652–9.
Kirkpatrick DP, Hunter RE, Janes PC, Mastrangelo J, Nicholas RA. The snowboarder’s foot and ankle. Am J Sports Med. 1998;26(2):271–7.
Kofotolis N, Kellis E. Ankle sprain injuries: a 2-year prospective cohort study in female Greek professional basketball players. J Athl Train. 2007;42(3):388–94.
Kostopoulos N, Dimitrios P. Injuries in basketball. Biol Exerc. 2010;6(1):47–55.
Kucera KL, Marshall SW, Kirkendall DT, Marchak PM, Garrett WE Jr. Injury history as a risk factor for incident injury in youth soccer. Br J Sports Med. 2005;39(7):462–6. doi:10.1136/bjsm.2004.013672.
Langevoort G, Myklebust G, Dvorak J, Junge A. Handball injuries during major international tournaments. Scand J Med Sci Sports. 2007;17(4):400–7. doi:10.1111/j.1600-0838.2006.00587.x.
Le Gall F, Carling C, Reilly T. Injuries in young elite female soccer players: an 8-season prospective study. Am J Sports Med. 2008;36(2):276–84. doi:10.1177/0363546507307866.
Le Gall F, Carling C, Reilly T, Vandewalle H, Church J, Rochcongar P. Incidence of injuries in elite French youth soccer players: a 10-season study. Am J Sports Med. 2006;34(6):928–38. doi:10.1177/0363546505283271.
Leary T, White JA. Acute injury incidence in professional county club cricket players (1985–1995). Br J Sports Med. 2000;34(2):145–7.
Linde F. Injuries in orienteering. Br J Sports Med. 1986;20(3):125–7.
Linko PE, Blomberg HK, Frilander HM. Orienteering competition injuries: injuries incurred in the Finnish Jukola and Venla relay competitions. Br J Sports Med. 1997;31(3):205–8.
Maehlum S, Daljord OA. Acute sports injuries in Oslo: a one-year study. Br J Sports Med. 1984;18(3):181–5.
Malliou P, Beneka A, Tsigganos G, Gioftsidou A, Germanou E, Michalopoulou M. Are injury rates in female volleyball players age related? Sport Sci Health. 2007;2(3):113–7.
Marchi AG, Di Bello D, Messi G, Gazzola G. Permanent sequelae in sports injuries: a population based study. Arch Dis Child. 1999;81(4):324–8.
Marfleet P. Ultimate injuries: a survey. Br J Sports Med. 1991;25(4):235–40.
Marshall SW, Covassin T, Dick R, Nassar LG, Agel J. Descriptive epidemiology of collegiate women’s gymnastics injuries: National Collegiate Athletic Association injury surveillance system, 1988–1989 through 2003–2004. J Athl Train. 2007;42(2):234–40.
Marshall SW, Hamstra-Wright KL, Dick R, Grove KA, Agel J. Descriptive epidemiology of collegiate women’s softball injuries: National Collegiate Athletic Association Injury Surveillance System, 1988–1989 through 2003–2004. J Athl Train. 2007;42(2):286–94.
McGuine TA, Brooks A, Hetzel S. The effect of lace-up ankle braces on injury rates in high school basketball players. Am J Sports Med. 2011;39(9):1840–8.
McGuine TA, Hetzel S, Wilson J, Brooks A. The effect of lace-up ankle braces on injury rates in high school basketball players. Am J Sports Med. 2012;40(1):49–57. doi:10.1177/0363546511422332.
McMaster WC, Walter M. Injuries in soccer. Am J Sports Med. 1978;6(6):354–7.
Michelson JD, Durant DM, McFarland E. The injury risk associated with pes planus in athletes. Foot Ankle Int. 2002;23(7):629–33.
Nelson NG, McKenzie LB. Rock climbing injuries treated in emergency departments in the US, 1990–2007. Am J Prev Med. 2009;37(3):195–200. doi:10.1016/j.amepre.2009.04.025.
Nelson WE, DePalma B, Gieck JH, McCue FC, Kulund DN. Intercollegiate lacrosse injuries. Phys Sportsmed. 1981;9(10):86–92.
Nickel C, Xernial O, Musahl V, Hansen U, Zantop T, Petersen W. A prospective study of kitesurfing injuries. Am J Sports Med. 2004;32(4):921–7.
Nysted M, Drogset JO. Trampoline injuries. Br J Sports Med. 2006;40(12):984–7. doi:10.1136/bjsm.2006.029009.
Orchard J, Seward H. Epidemiology of injuries in the Australian Football League, seasons 1997–2000. Br J Sports Med. 2002;36(1):39–44.
Orchard J, Wood T, Seward H, Broad A. Comparison of injuries in elite senior and junior Australian football. J Sci Med Sport. 1998;1(2):82–8.
Pasanen K, Parkkari J, Kannus P, Rossi L, Palvanen M, Natri A, et al. Injury risk in female floorball: a prospective one-season follow-up. Scand J Med Sci Sports. 2008;18(1):49–54.
Price RJ, Hawkins RD, Hulse MA, Hodson A. The Football Association medical research programme: an audit of injuries in academy youth football. Br J Sports Med. 2004;38(4):466–71.
Purdam C. A survey of netball and basketball injuries. Excel. 1987;3(3):9–11.
Putukian M, Knowles WK, Swere S, Castle NG. Injuries in indoor soccer. The Lake Placid Dawn to Dark Soccer Tournament. Am J Sports Med. 1996;24(3):317–22. doi:10.1177/036354659602400312.
Ramirez M, Schaffer KB, Shen H, Kashani S, Kraus JF. Injuries to high school football athletes in California. Am J Sports Med. 2006;34(7):1147–58. doi:10.1177/0363546505284385.
Rebella GS, Edwards JO, Greene JJ, Husen MT, Brousseau DC. A prospective study of injury patterns in high school pole vaulters. Am J Sports Med. 2008;36(5):913–20. doi:10.1177/0363546507313571.
Romiti M, Finch CF, Gabbe B. A prospective cohort study of the incidence of injuries among junior Australian football players: evidence for an effect of playing-age level. Br J Sports Med. 2008;42(6):441–6. doi:10.1136/bjsm.2007.042721.
Sadat-Ali M, Sankaran-Kutty M. Soccer injuries in Saudi Arabia. Am J Sports Med. 1987;15(5):500–2.
Sankey RA, Brooks JHM, Kemp SPT, Haddad FS. The epidemiology of ankle injuries in professional rugby union players. Am J Sports Med. 2008;36(12):2415–24. doi:10.1177/0363546508322889.
Schafle MD, Requa RK, Patton WL, Garrick JG. Injuries in the 1987 national amateur volleyball tournament (Blessures dans le cadre du tournoi national amateur de volleyball). Am J Sports Med. 1990;18(6):624–31.
Schick DM, Meeuwisse WH. Injury rates and profiles in female ice hockey players. Am J Sports Med. 2003;31(1):47–52.
Schick DM, Molloy MG, Wiley JP. Injuries during the 2006 Women’s Rugby World Cup. Br J Sports Med. 2008;42(6):447–51. doi:10.1136/bjsm.2008.046672.
Schulz MR, Marshall SW, Yang J, Mueller FO, Weaver NL, Bowling JM. A prospective cohort study of injury incidence and risk factors in North Carolina high school competitive cheerleaders. Am J Sports Med. 2004;32(2):396–405.
Shields BJ, Fernandez SA, Smith GA. Epidemiology of cheerleading stunt-related injuries in the United States. J Athl Train. 2009;44(6):586–94. doi:10.4085/1062-6050-44.6.586.
Shields BJ, Smith GA. Epidemiology of strain/sprain injuries among cheerleaders in the United States. Am J Emerg Med. 2011;29(9):1003–12. doi:10.1016/j.ajem.2010.05.014.
Sinha A, McGlone RG, Montgomery K. Study of aeroball injuries. Br J Sports Med. 1997;31(3):200–4.
Snellman K, Parkkari J, Kannus P, Leppala J, Vuori I, Jarvinen M. Sports injuries in floorball: a prospective one-year follow-up study. Int J Sports Med. 2001;22(7):531–6.
Soderman K, Adolphson J, Lorentzon R, Alfredson H. Injuries in adolescent female players in European football: a prospective study over one outdoor soccer season. Scand J Med Sci Sports. 2001;11(5):299–304.
Solgard L, Nielsen AB, Moller-Madsen B, Jacobsen BW, Yde J, Jensen J. Volleyball injuries presenting in casualty: a prospective study. Br J Sports Med. 1995;29(3):200–4.
Starkey C. Injuries and illnesses in the National Basketball Association: a 10-year. J Athl Train. 2000;35(2):161–7.
Steffen K, Pensgaard AM, Bahr R. Self-reported psychological characteristics as risk factors for injuries in female youth football. Scand J Med Sci Sports. 2009;19(3):442–51. doi:10.1111/j.1600-0838.2008.00797.x.
Tegnander A, Olsen O, Moholdt T, Engebretsen L, Bahr R. Injuries in Norwegian female elite soccer: a prospective one-season cohort study. Knee Surg Sports Traumatol Arthrosc. 2008;16(2):194–8.
Timpka T, Risto O, Bjormsjo M. Boys soccer league injuries: a community-based study of time-loss from sports participation and long-term sequelae. Eur J Public Health. 2008;18(1):19–24. doi:10.1093/eurpub/ckm050.
Turbeville SD, Cowan LD, Asal NR, Owen WL, Anderson MA. Risk factors for injury in middle school football players. Am J Sports Med. 2003;31(2):276–81.
Tyler TF, McHugh MP, Mirabella MR, Mullaney MJ, Nicholas SJ. Risk factors for noncontact ankle sprains in high school football players—the role of previous ankle sprains and body mass index. Am J Sports Med. 2006;34(3):471–5. doi:10.1177/0363546505280429.
Verhagen E, van der Beek A, Twisk J, Bouter L, Bahr R, van Mechelen W. The effect of a proprioceptive balance board training program for the prevention of ankle sprains: a prospective controlled trial. Am J Sports Med. 2004;32(6):1385–93. doi:10.1177/0363546503262177.
Volpi P, Pozzoni R, Galli M. The major traumas in youth football. Knee Surg Sports Traumatol Arthrosc. 2003;11(6):399–402.
Walden M, Hagglund M, Ekstrand J. Injuries in Swedish elite football—a prospective study on injury definitions, risk for injury and injury pattern during 2001. Scand J Med Sci Sports. 2005;15(2):118–25. doi:10.1111/j.1600-0838.2004.00393.x.
Waterman BR, Owens BD, Davey S, Zacchilli MA, Belmont PJ Jr. The epidemiology of ankle sprains in the United States. J Bone Joint Surg Am. 2010;92(13):2279–84. doi:10.2106/jbjs.i.01537.
Watson AW. Ankle sprains in players of the field-games Gaelic football and hurling. J Sports Med Phys Fitness. 1999;39(1):66–70.
Watson AWS. Sports injuries in the game of hurling—a one-year prospective study. Am J Sports Med. 1996;24(3):323–8. doi:10.1177/036354659602400313.
Watson MD, DiMartino PP. Incidence of injuries in high school track and field athletes and its relation to performance ability. Am J Sports Med. 1987;15(3):251–4.
Wedderkopp N, Kaltoft M, Holm R, Froberg K. Comparison of two intervention programmes in young female players in European handball—with and without ankle disc. Scand J Med Sci Sports. 2003;13(6):371–5. doi:10.1046/j.1600-0838.2003.00336.x.
Wedderkopp N, Kaltoft M, Lundgaard B, Rosendahl M, Froberg K. Injuries in young female players in European team handball. Scand J Med Sci Sports. 1997;7(6):342–7.
Wheeler BR. Slow-pitch softball injuries. Am J Sports Med. 1984;12(3):237–40.
Wiesler ER, Hunter M, Martin DF, Curl WW, Hoen H. Ankle flexibility and injury patterns in dancers. Am J Sports Med. 1996;24(6):754–7. doi:10.1177/036354659602400609.
Wikstrom J, Andersson C. A prospective study of injuries in licensed floorball players (Une etude prospective des blessures chez les joueurs licencies de balle au sol, sport pratique en Suede). Scand J Med Sci Sports. 1997;7(1):38–42.
Williamson DM, Lowdon IM. Ice-skating injuries. Injury. 1986;17(3):205–7.
Woods C, Hawkins R, Hulse M, Hodson A. The Football Association Medical Research Programme: an audit of injuries in professional football: an analysis of ankle sprains. Br J Sports Med. 2003;37(3):233–8. doi:10.1136/bjsm.37.3.233.
Yard EE, Shcroeder MJ, Fields SK, Collins CL, Comstock RD. The epidemiology of United States high school soccer injuries, 2005–2007. Am J Sports Med. 2008;36(10):1930–7.
Yde J, Nielsen AB. Sports injuries in adolescents’ ball games: soccer, handball and basketball. Br J Sports Med. 1990;24(1):51–4.
Zillmer DA, Powell JW, Albright JP. Gender-specific injury patterns in high school varsity basketball. J Women Health. 1992;1(1):69–76.
Cumps E, Verhagen E, Meeusen R. Prospective epidemiological study of basketball injuries during one competitive season: ankle sprains and overuse knee injuries. J Sports Sci Med. 2007;6(2):204–11.
Junge A, Dvorak J, Graf-Baumann T, Peterson L. Football injuries during FIFA tournaments and the Olympic Games, 1998–2001: development and implementation of an injury-reporting system. Am J Sports Med. 2004;32(1 Suppl):80S–9S.
Finch CF, Valuri G, Ozanne-Smith J. Injury surveillance during medical coverage of sporting events–development and testing of a standardised data collection form. J Sci Med Sport. 1999;2(1):42–56.
Peterson L, Junge A, Chomiak J, Graf-Baumann T, Dvorak J. Incidence of football injuries and complaints in different age groups and skill-level groups. Am J Sports Med. 2000;28(5 Suppl):S51–7.
Keller CS, Noyes FR, Buncher CR. The medical aspects of soccer injury epidemiology. Am J Sports Med. 1987;15(3):230–7.
Levy IM. Formulation and sense of the NAIRS athletic injury surveillance system. Am J Sports Med. 1988;16(Suppl 1):S132–3.
Hagglund M, Walden M, Bahr R, Ekstrand J. Methods for epidemiological study of injuries to professional football players: developing the UEFA model. Br J Sports Med. 2005;39(6):340–6. doi:10.1136/bjsm.2005.018267.
Verhagen E, Van der Beek AJ, Bouter LM, Bahr RM, Van Mechelen W. A one season prospective cohort study of volleyball injuries. Br J Sports Med. 2004;38(4):477–81. doi:10.1136/bjsm.2003.005785.
Ristolainen L, Heinonen A, Waller B, Kujala UM, Kettunen JA. Gender differences in sport injury risk and types of injuries: a retrospective twelve-month study on cross-country skiers, swimmers, long-distance runners and soccer players. J Sports Sci Med. 2009;8(3):443–51.
Rozzi SL, Lephart SM, Gear WS, Fu FH. Knee joint laxity and neuromuscular characteristics of male and female soccer and basketball players. Am J Sports Med. 1999;27(3):312–9.
Quatman CE, Myer GD, Khoury J, Wall EJ, Hewett TE. Sex differences in “weightlifting” injuries presenting to United States emergency rooms. J Strength Cond Res. 2009;23(7):2061–7. doi:10.1519/JSC.0b013e3181b86cb9.
Agel J, Bershadsky B, Arendt EA. Hormonal therapy: ACL and ankle injury. Med Sci Sports Exerc. 2006;38(1):7–12.
Hesar NGZ, Calders P, Thijs Y, Roosen P, Witvrouw E. The influence of menstrual cycle on ankle proprioception. Isokin Exerc Sci. 2008;16(2):119–23.
Beaulieu ML, Lamontagne M, Xu LY. Lower limb muscle activity and kinematics of an unanticipated cutting manoeuvre: a gender comparison. Knee Surg Sports Traumatol Arthrosc. 2009;17(8):968–76. doi:10.1007/s00167-009-0821-1.
Joseph MF, Rahl M, Sheehan J, MacDougall B, Horn E, Denegar CR, et al. Timing of lower extremity frontal plane motion differs between female and male athletes during a landing task. Am J Sports Med. 2011;39(7):1517–21.
McLean SG, Walker KB, Van den Bogert AJ. Effect of gender on lower extremity kinematics during rapid direction changes: an integrated analysis of three sports movements. J Sci Med Sport. 2005;8(4):411–22.
Hewett TE, Ford KR, Myer GD. Anterior cruciate ligament injuries in female athletes: part 2, a meta-analysis of neuromuscular interventions aimed at injury prevention. Am J Sports Med. 2006;34(3):490–8. doi:10.1177/0363546505282619.
Lohmander LS, Ostenberg A, Englund M, Roos H. High prevalence of knee osteoarthritis, pain, and functional limitations in female soccer players twelve years after anterior cruciate ligament injury. Arthritis Rheum. 2004;50(10):3145–52. doi:10.1002/art.20589.
Quatman-Yates CC, Quatman CE, Meszaros AJ, Paterno MV, Hewett TE. A systematic review of sensorimotor function during adolescence: a developmental stage of increased motor awkwardness? Br J Sports Med. 2012;46(9):649–55.
Conn JM, Annest JL, Bossarte RM, Gilchrist J. Non-fatal sports and recreational violent injuries among children and teenagers, United States, 2001–2003. J Sci Med Sport. 2006;9(6):479–89. doi:10.1016/j.jsams.2006.03.004.
Kelso JA. Phase transitions and critical behavior in human bimanual coordination. Am J Physiol. 1984;246(6 Pt 2):R1000–4.
Kelso JA, Holt KG, Rubin P, Kugler PN. Patterns of human interlimb coordination emerge from the properties of non-linear, limit cycle oscillatory processes: theory and data. J Mot Behav. 1981;13(4):226–61.
Robertson SD, Zelaznik HN, Lantero DA, Bojczyk KG, Spencer RM, Doffin JG, Schneidt T. Correlations for timing consistency among tapping and drawing tasks: evidence against a single timing process for motor control. J Exp Psychol Hum Percept Perform. 1999;25(5):1316–30.
Davids K, Glazier P, Araújo D, Bartlett R. Movement systems as dynamical systems: the functional role of variability and its implications for sports medicine. Sports Med. 2003;33(4):245–60.
Davids K, Glazier P. Deconstructing neurobiological coordination: the role of the biomechanics-motor control nexus. Exerc Sport Sci Rev. 2010;38(2):86–90.
Barrett JR, Tanji JL, Drake C, Fuller D, Kawasaki RI, Fenton RM. High- versus low-top shoes for the prevention of ankle sprains in basketball players. A prospective randomized study. Am J Sports Med. 1993;21(4):582–5.
Borowski LA, Yard EE, Fields SK, Comstock RD. The epidemiology of US high school basketball injuries, 2005–2007. Am J Sports Med. 2008;36(12):2328–35. doi:10.1177/0363546508322893.
Chan KM, Yuan Y, Li CK, Chien P, Tsang G. Sports causing most injuries in Hong Kong. Br J Sports Med. 1993;27(4):263–7.
Gomez E, DeLee JC, Farney WC. Incidence of injury in Texas girls’ high school basketball. Am J Sports Med. 1996;24(5):684–7.
Henry JH, Lareau B, Neigut D. The injury rate in professional basketball. Am J Sports Med. 1982;10(1):16–8.
Zelisko JA, Noble HB, Porter M. A comparison of men’s and women’s professional basketball injuries. Am J Sports Med. 1982;10(5):297–9.
Castro M, Janeira MA, Fernandes O, Cunha L. Biomechanical analysis of an inciting event of ankle sprain on basketball players. Br J Sports Med. 2008;42(6):511–2.
Briner WW Jr, Kacmar L. Common injuries in volleyball. Mechanisms of injury, prevention and rehabilitation. Sports Med. 1997;24(1):65–71.
Gross P, Marti B. Risk of degenerative ankle joint disease in volleyball players: study of former elite athletes. Int J Sports Med. 1999;20(1):58–63. doi:10.1055/s-2007-971094.
Reeser JC. Volleyball injury epidemiology. Int J Vol Res. 2000;3(1):26–30.
Reeser JC, Verhagen E, Briner WW, Askeland TI, Bahr R. Strategies for the prevention of volleyball related injuries. Br J Sports Med. 2006;40(7):594–600 (discussion 599–600). doi:10.1136/bjsm.2005.018234.
Iwamoto J, Takeda T, Sato Y, Matsumoto H. Retrospective case evaluation of gender differences in sports injuries in a Japanese sports medicine clinic. Gend Med. 2008;5(4):405–14. doi:10.1016/j.genm.2008.10.002.
Zecher SB, Leach RE. Lower leg and foot injuries in tennis and other racquet sports. Clin Sports Med. 1995;14(1):223–39.
Jackson DS, Furman WK, Berson BL. Patterns of injuries in college athletes: a retrospective study of injuries sustained in intercollegiate athletics in two colleges over a two-year period. Mt Sinai J Med. 1980;47(4):423–6.
Jarret GJ, Orwin JF, Dick RW. Injuries in collegiate wrestling. Am J Sports Med. 1998;26(5):674–80.
Strauss RH, Lanese RR. Injuries among wrestlers in school and college tournaments. JAMA. 1982;248(16):2016–9.
Bleakley CM, McDonough SM, MacAuley DC, Bjordal J. Cryotherapy for acute ankle sprains: a randomised controlled study of two different icing protocols. Br J Sports Med. 2006;40(8):700–5 (discussion 5). doi:10.1136/bjsm.2006.025932.
Bleakley CM, O’Connor SR, Tully MA, Rocke LG, Macauley DC, Bradbury I, et al. Effect of accelerated rehabilitation on function after ankle sprain: randomised controlled trial. BMJ. 2010;340:c1964. doi:10.1136/bmj.c1964.
Boyce SH, Quigley MA, Campbell S. Management of ankle sprains: a randomised controlled trial of the treatment of inversion injuries using an elastic support bandage or an Aircast ankle brace. Br J Sports Med. 2005;39(2):91–6. doi:10.1136/bjsm.2003.009233.
Lamb SE, Marsh JL, Hutton JL, Nakash R, Cooke MW. Mechanical supports for acute, severe ankle sprain: a pragmatic, multicentre, randomised controlled trial. Lancet. 2009;373(9663):575–81. doi:10.1016/s0140-6736(09)60206-3.
Emery CA, Meeuwisse WH. The effectiveness of a neuromuscular prevention strategy to reduce injuries in youth soccer: a cluster-randomised controlled trial. Br J Sports Med. 2010;44(8):555–62. doi:10.1136/bjsm.2010.074377.
Janssen KW, van Mechelen W, Verhagen E. Ankles back in randomized controlled trial (ABrCt): braces versus neuromuscular exercises for the secondary prevention of ankle sprains. Design of a randomised controlled trial. BMC Musculoskelet Disord. 2011;12(210). doi:10.1186/1471-2474-12-210.
Wedderkopp N, Kaltoft M, Lundgaard B, Rosendahl M, Froberg K. Prevention of injuries in young female players in European team handball. A prospective intervention study. Scand J Med Sci Sports. 1999;9(1):41–7.
Waterman BR, Belmont PJ Jr, Cameron KL, Deberardino TM, Owens BD. Epidemiology of ankle sprain at the United States Military Academy. Am J Sports Med. 2010;38(4):797–803. doi:10.1177/0363546509350757.
Wright IC, Neptune RR, van den Bogert AJ, Nigg BM. The influence of foot positioning on ankle sprains. J Biomech. 2000;33(5):513–9.
Attarian DE, McCrackin HJ, DeVito DP, McElhaney JH, Garrett WE Jr. Biomechanical characteristics of human ankle ligaments. Foot Ankle. 1985;6(2):54–8.
Fong DT, Chan YY, Mok KM, Yung PSh, Chan KM. Understanding acute ankle ligamentous sprain injury in sports. Sports Med Arthrosc Rehabil Ther Technol. 2009;1:14. doi:10.1186/1758-2555-1-14.
Loudon JK, Bell SL. The foot and ankle: an overview of arthrokinematics and selected joint techniques. J Athl Train. 1996;31(2):173–8.
Almeida SA, Williams KM, Shaffer RA, Brodine SK. Epidemiological patterns of musculoskeletal injuries and physical training. Med Sci Sports Exerc. 1999;31(8):1176–82. doi:10.1097/00005768-199908000-00015.
Finestone A, Milgrom C, Evans R, Yanovich R, Constantini N, Moran DS. Overuse injuries in female infantry recruits during low-intensity basic training. Med Sci Sports Exerc. 2008;40(11 Suppl):S630–5. doi:10.1249/MSS.0b013e3181892ff9.
Jones BH, Bovee MW, Harris JM 3rd, Cowan DN. Intrinsic risk factors for exercise-related injuries among male and female army trainees. Am J Sports Med. 1993;21(5):705–10.
Belmont PJ Jr, Goodman GP, Waterman B, DeZee K, Burks R, Owens BD. Disease and nonbattle injuries sustained by a U.S. Army Brigade Combat Team during Operation Iraqi Freedom. Mil Med. 2010;175(7):469–76.
Davidson PL, Chalmers DJ, Wilson BD, McBride D. Lower limb injuries in New Zealand Defence Force personnel: descriptive epidemiology. Aust N Z J Public Health. 2008;32(2):167–73. doi:10.1111/j.1753-6405.2008.00195.x.
Hughes CD, Weinrauch PCL. Military static line parachute injuries in an Australian commando battalion. ANZ J Surg. 2008;78(10):848–52. doi:10.1111/j.1445-2197.2008.04581.x.
Kragh JF Jr, Taylor DC. Fast-roping injuries among Army Rangers: a retrospective survey of an elite airborne battalion. Mil Med. 1995;160(6):277–9.
Miser WF, Doukas WC, Lillegard WA. Injuries and illnesses incurred by an army ranger unit during Operation Just Cause. Mil Med. 1995;160(8):373–80.
Dettori JR, Pearson BD, Basmania CJ, Lednar WM. Early ankle mobilization, part I: the immediate effect on acute, lateral ankle sprains (a randomized clinical trial). Mil Med. 1994;159(1):15–20.
Fong DT, Hong Y, Chan LK, Yung PS, Chan KM. A systematic review on ankle injury and ankle sprain in sports. Sports Med. 2007;37(1):73–94.
Da J. Improving the reporting of clinical case series. Am J Ophthalmol. 2005;139(5):900–5.
Acknowledgments
This study was supported by the Health Research Board (HRA_POR/2011/46) as follows: PI—Eamonn Delahunt; Co-investigators—Chris Bleakley and Jay Hertel; PhD student—Cailbhe Doherty. The authors have no potential conflicts of interest that are directly relevant to the content of this study.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Doherty, C., Delahunt, E., Caulfield, B. et al. The Incidence and Prevalence of Ankle Sprain Injury: A Systematic Review and Meta-Analysis of Prospective Epidemiological Studies. Sports Med 44, 123–140 (2014). https://doi.org/10.1007/s40279-013-0102-5
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40279-013-0102-5