
Abstract
Background: The dire state of coronavirus disease (COVID-19) outbreak has had a substantial psychological impact on society.
Methods: A systematic search was performed through Medline, PubMed, Embase, Scopus, and Web of Science, to investigate the impact of the COVID-19 pandemic on the psychological health of individuals in various countries. Subgroup analyses considered gender and classification of countries into three continents of America, Europe, and Asia. Only studies that used the COVID-19 Peritraumatic Distress Index (CPDI) questionnaire as a tool to assess mental distress were included in this meta-analysis. Heterogeneity among studies was assessed by I2 statistic, and the random-effects model was utilized to obtain the pooled prevalence.
Results: This pooled analysis included a large data sample of 21 studies consisting of 94,414 participants. The pooled prevalence of the psychological distress during the time of COVID-19 pandemic by CPDI for the continent of Asia was 43% (34.6% mild-to-moderate and 8.4% severe) which was greater than that for Europe (35%; 30% mild-to-moderate and 5% severe) but lower than that for America (64.3%; 45.8% mild to moderate and 18.5% severe). In addition, the prevalence of psychological distress according to CPDI was higher in females (48%; 40% mild to moderate, 13% severe) compared with males (59%; 36% mild to moderate and 5% severe).
Conclusions: Our findings suggest that psychological distress in the Americas is a larger problem than in Asia and European continents. Females appear to be more vulnerable and may therefore require further attention in terms of preventive and management strategies. Implementation of both digital and molecular biomarkers is encouraged to increase objectivity and accuracy of assessing the dynamic changes in mental health in the current and future pandemics.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others

Keywords
1 Introduction
Coronavirus 2019 (COVID-19) was declared a pandemic after reaching more than 140 thousand cases by the World Health Organization (WHO) on March 11, 2020 [1]. The virus has since spread worldwide rapidly through several waves and emergence of numerous variants and reached more than 620 million cases with 6.5 million deaths by October 2022 [2]. Naturally, pandemics such as this coronavirus have a long-standing history of affecting physical and mental health in all demographic groups [3, 4].
To control and reduce the prevalence of the virus and save human lives, various strategies have been followed in the world, one of the most important being the different lockdown and quarantine approaches [5]. Over one-third of the global population has experienced periods of these steps, which has even been extended in some countries [6]. Due to these policies, the COVID-19 pandemic has had an unprecedented psychological effect on people from all walks of life [7]. While in quarantine, patients with confirmed or suspected COVID-19 disease can experience high levels of anxiety, depression, stress, fear, boredom, isolation, insecurity, posttraumatic stress (PTS) symptoms, confusion, and stigma, all of which are signs of psychological distress [8, 9].
Due to the rapid and evolving nature of this health emergency during the first year of the pandemic, a number of studies on associated emerging mental health problems have been published [10,11,12,13,14,15,16]. It is hoped that such analyses can help to prepare us from new outbreaks of the COVID-19 as well as in the likely event of future pandemics. For these reasons, we have updated these previous reports by conducting a systematic review and meta-analysis of studies published on a global prevalence of the psychological distress impact of COVID-19 pandemic in different countries. In addition, subgroup analyses were conducted to consider the effects of gender and regional distribution across three continents of North America, Europe, and Asia. In addition, we propose a route forward in preparedness for the future pandemics using a combination of psychological and molecular screening tools to aid in patient risk assessment.
2 Materials and Methods
2.1 Database and Search Strategy
We developed a protocol according to the PRISMA guidelines [17]. Published papers indexed in Medline-PubMed, Embase, Web of Science, and Scopus were searched using the following MeSH terms and keywords: “coronavirus diseases 19,” OR “SARS-CoV-2,” OR “COVID-19,” AND “psychological distress,” AND “prevalence”, AND “COVID-19 per traumatic Distress Index,” alone or combination. For preprint articles, we searched medRxiv and the Social Science Research Network (SSRN) COVID-19 Research Topic. References from selected articles were inspected to detect additional potential studies.
2.2 Eligibility Criteria
We selected studies that (a) reported psychological distress due to COVID-19, (b) used the COVID-19 Peritraumatic Distress Index (CPDI) questionnaire for the evaluation of psychological distress, (c) were published in English language, (d) were published between January 1, 2020 to January 1, 2021, and (e) were available as full texts. We excluded (a) interventional studies, (b) studies with incomplete or unclear methods/data, and (c) non-original or duplicate studies.
2.3 Introducing the CPDI
CPDI is an instrument for the evaluation of specific phobias and stress disorders due to COVID-19. This questionnaire was originally developed in Chinese [10] and then validated and used in many countries around the world. The 24-item CPDI questionnaire is designed in the form of 5-point Likert-type (0 “never,” 1 “occasionally,” 2 “sometimes,” 3 “often,” 4 “most of the time”). Items in the questionnaire inquire about the frequency of anxiety, depression, specific phobias, cognitive change, avoidance and compulsive behavior, physical symptoms, and loss of social functioning with a range from 0 to 100 and a higher final score indicating higher distress. A score ≤27 indicated normal distress, between 28 and 51 indicated mild-to-moderate distress, and a score ≥52 indicated severe distress [10].
2.4 Data Extraction
After obtaining full texts of relevant articles, two authors (SA and FRB) independently abstracted all studies using a pre-designed form. Inconsistencies between the two reviewers were adjudicated by a third independent reviewer (AVA). The data elements included the name of the first author (or authors if only two are listed), year of publication, place of study (country), population, sample size, study design, gender, age, number of individuals with normal, mild-to-moderate and severe psychological distress based on CPDI scores, and division of studies by country into three continents: The Americas (North and South America counted as one continent), Europe, and Asia which include Middle East countries.
2.5 Quality Assessment
Quality assessment of studies was conducted using the National Institutes of Health (NIH) tool [18]. This consists of 14-item questions and was used for observational cohort and cross-sectional studies. Items in the questionnaire inquired about the research question (Q1), study population (Q2 and Q3), eligibility criteria (Q4), sample size justification (Q5), outcome measurement (Q6), timeframe sufficient (Q7), exposure of interest (Q8), exposure measures and assessment (Q9), repeated exposure assessment (Q10), outcome measures (Q11), blinding of outcome assessors (Q12), follow-up rate (Q13), and statistical analyses (Q14). The details of these questions are available at supplementary file as footnote of Supplemental Table S1. After evaluating all components of any given study and based on the number of “yes” responses, a rating of good (7–9), medium (4–6), or poor (≤3) was determined for each study [19]. Studies with a poor rating were excluded from the meta-analysis. Two reviewers (SA and FRB) assessed the quality of studies and disagreements between them was resolved with the final judgement offered by the senior investigator (AVA). The inter-rater agreement in ratings was also calculated, and the final rate of quality of included studies based on the number of “yes” according to inter-rater agreement is presented in Supplemental Table S1.
2.6 Statistical Analysis
We obtained the globally pooled prevalence for normal, mild-to-moderate, and severe psychological distress based on CPDI scores with confidence intervals (CI) for each study. Prevalence was calculated assuming binomial distribution. In addition, we calculated prevalence of normal, mild-to-moderate, and severe psychological distress for subgroups including gender (females versus males) and continent (Americas, Europe, and Asia). For analyses of pooled prevalence and CI, a random-effects model was used. Heterogeneity among studies was assessed using the I2 index, for which values >70% represented a high heterogeneity. When the data were homogeneous, a fixed-effects model was used, while a random-effects model was employed when the heterogeneity source was unknown. Publication bias was determined through visual inspection of a funnel plot. Additionally, to assess the bias, Egger’s [20] and Begg’s [21] tests were conducted. All analyses were performed using the STATA software (v16.0; College Station, TX, USA), and significant levels were set at p < 0.05.
3 Results
3.1 Search Outcomes
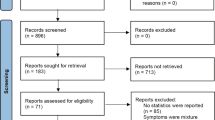
The search strategy yielded 2707 articles. After removal of duplicates (n = 668), a careful assessment of the title and abstracts resulted in the elimination of 1932 articles as they did not meet the inclusion criteria. Following examination of the reference lists of related articles, 8 studies were added, and 95 full text articles were assessed for eligibility. Of these, 74 full text articles were excluded because (1) prevalence was reported as a mean instead of a proportion (n = 29), (2) prevalence was not reported (n = 18), (3) the methodology was unclear or of low quality (n = 19), and (4) it was a review article (n = 8). This left a final 21 articles that met our criteria and were included in the meta-analysis. These 21 studies comprised a total number of 94,414 participants, which included 5 studies with 5532 participants in the Americas [22,23,24,25,26], 6 with 27,269 participants in Europe [13, 26,27,28,29,30,31,32], and 10 with 61,613 participants in Asia [10,11,12, 33,34,35,36,37,38,39]. The PRISMA flowchart of study selections for the systematic review along with the reasons for exclusion is presented in Fig. 4.1.

PRISMA flowchart showing the selection of studies
3.2 Study Characteristics
The characteristics of studies included in the meta-analysis are presented in Table 4.1. The majority of studies were cross-sectional in nature and conducted during the period of the COVID-19 pandemic between January 2020 and January 2021. Out of the 21 studies, 10 were from Asia (including the Middle East) (1 from China, 1 from Iran, 1 from Saudi Arabia, 2 from India, 2 from Nepal, 1 from Egypt, 1 from Philippines, and 1 from Bangladesh), 6 from Europe (5 from Italy and 1 from Germany), and 5 from the Americas (1 from USA, 1 from Peru, and 3 from Brazil). All studies used the CPDI tool for assessment of psychological distress. Out of 21 studies, 15 were performed across the general population and 3 were on child welfare workers [22], students [24], and endodontists [36]. The study from Egypt estimated the prevalence of psychological distress based on CPDI among the general population and healthcare workers separately [39]. Two of the papers were designed as case-control studies on adults with autoimmune arthritis [27] or with cystic fibrosis [31], both compared to the general population. The mean age of study participants ranged from 32.0 to 57.7 years. The sample sizes in the studies varied from 45 to 52,730. Seventeen studies were of good quality and 4 were of medium quality based on use of the NIH tool.
3.3 Pooled Prevalence of Psychological Distress
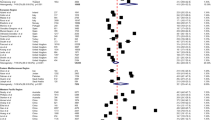
Psychological distress was estimated using CPDI scores into normal, mild-to-moderate, and severe across categories as detailed in the methods section. We estimated the pooled prevalence of each category separately over the 21 studies with a sample size 94,414. The pooled prevalence percentages of the determined normal (Fig. 4.2), mild-to-moderate (Fig. 4.3a), and severe (Fig. 4.3b) psychological distress groups were 55% (95% CI: 47–63%, I2 = 98.97%, p < 0.001), 36% (30–41%, I2 = 97.42%, p < 0.001), and 10% (6–13%, I2 = 93.39%, p < 0.001), respectively.

Forest plot of CPDI-based pooled prevalence for normal psychological distress (note that years followed by a and b indicate different aspects of the same study). USA United States of America


Forest plot of CPDI-based pooled prevalence for (a) mild-to-moderate psychological distress and (b) severe psychological distress
3.4 Pooled Prevalence of Psychological Distress According to Continents
The normal, mild-to-moderate, and severe pooled prevalence percentages of psychological distress in the 5 studies from the Americas (sample size = 5532) were estimated at 35.7% (19.7–51.8%, I2 = 96.99%, p < 0.001), 45.8% (39.8–51.8%, I2 = 77.78%, p < 0.001), and 18.5% (8–28%, I2 = 92.54%, p < 0.001), respectively. For the European continent, the same pooled prevalence percentages of psychological distress across 8 studies (sample size = 27,269) were 65% (55.4–75.4%, I2 = 96.67%, p < 0.001), 30% (20.5–39.7%, I2 = 96.38%, p < 0.001), and 5% (4.1–6.5%, I2 = 10%, p < 0.001), respectively. For the 11 studies from the Asian continent (sample size = 61,613), the normal, mild-to-moderate, and severe pooled prevalence percentages of psychological distress were 57% (46–67.8%, I2 = 98.07%, p < 0.001), 34.6% (27.1–41.7%, I2 = 95.42%, p < 0.001), and 8.4% (5.1–11.8%, I2 = 72.61%, p < 0.001), respectively. Heterogeneity tests (I2) indicated low heterogeneity in the prevalence of severe psychological distress in European countries. However, significant heterogeneity existed across the prevalence of all levels of psychological distress for Asia and the Americas as described above.
3.5 Pooled Prevalence of Psychological Distress According to Gender
Prevalence data of CPDI-based psychological distress according to gender was available in seven studies (Table 4.2). The pooled prevalence of normal, mild-to-moderate, and severe psychological distress for females were 48% (34–63%, I2 = 97.52%, p < 0.001), 40% (31–48%, I2 = 91.17%, p < 0.001), and 13% (6–20%, I2 = 88.29%, p < 0.001), respectively. The pooled prevalence of normal, mild-to-moderate, and severe psychological distress for males were 59% (47–71%, I2 = 94.17%, p < 0.001), 34% (25–43%, I2 = 90.22%, p < 0.001), and 5% (2–9%, I2 = 26.36%, p = 0.38), respectively. A forest plot of the CPDI-based pooled prevalence for normal psychological distress in males and females is presented in Fig. 4.4 and for mild-to-moderate and severe psychological distress in Fig. 4.5a, b. I2 tests indicated low heterogeneity in the prevalence of severe psychological distress among males and in the separate male and female analyses. However, the I2 test indicated significant heterogeneity among the prevalence of psychological distress for females. Overall, the pooled prevalence of psychological distress was significantly higher in females than males (53% versus 39% p < 0.001).

Forest plot of CPDI-based pooled prevalence among females and males for normal psychological distress


Forest plot of CPDI-based pooled prevalence in females and males for (a) mild-to-moderate psychological distress and (b) severe psychological distress
3.6 Publication Bias
Egger’s and Begg’s tests were used to assess publication bias. As indicated by the p-values for the pooled prevalence of normal CPDI-based psychological distress (Egger: p = 0.369, Begg: p = 0.551) (Fig. 4.6a), mild-to-moderate psychological distress (Egger: p = 0.439, Begg: p = 0.785) (Fig. 4.6b), and severe psychological distress (Egger: p = 0.995, Begg: p = 0.655) (Fig. 4.6c), the funnel plots showed asymmetry and visual inspection confirmed the presence of publication bias.

Funnel plot showing publication bias on CPDI-based prevalence of psychological distress ranked as (a) normal, (b) mild-to-moderate, and (c) severe
4 Discussion
To our knowledge, this is the first study to report the prevalence of CPDI-based psychological distress impact of the COVID-19 pandemic in various countries, across the continents of the Americas, Europe, and Asia. We incorporated Middle East countries into the Asian continent as this region is officially classified as part of southwestern Asia [40]. We also included Egypt into the Asian continent as it officially recognized as part of the Middle East [41]. The analysis showed that the prevalence of the psychological distress in the mild-to-moderate and severe levels during the COVID-19 pandemic from January 2020 to January 2021 was highest for the Americas, followed by Asia and then Europe. In addition, the psychological distress in the mild-to-moderate and severe categories over this period was higher for females compared to males. However, it should be noted that this finding was not analyzed across the separate continents.
The finding of greater psychological stress in females is consistent with the fact that women are generally more susceptible to depression and more likely to experience posttraumatic stress symptoms over time compared to males [42, 43]. In line with previous studies from Brazil [23] and Italy [28], women appear to show more psychological symptoms during quarantine in pandemics as compared to men. In this difficult situation, women can be faced with additional responsibilities, such as an increased role in family care, child support and teaching responsibilities due to school closures, as well existing gender inequalities and the potential for abuse from their partners [44]. In addition, the loss of daily routines, as well as social and physical contact with friends and family, can lead to isolation, boredom, or frustration [11, 34, 36, 38]. Moreover, previous studies have shown that fear of COVID-19 infection from family members and obsessive-compulsive disorders is higher in women [45, 46]. Taken together, these findings indicate that more careful attention to risk identification and early intervention policies should be adopted for females during pandemics and other crises.
We found that the highest prevalence of psychological distress during the time of the COVID-19 lockdowns was highest in Brazil at 87.9% and lowest in Nepal (11.5%) for the combined mild-to-moderate and severe categories [24, 34]. The main difference in the prevalence of psychological distress between Brazil and Nepal is likely to be related to the more than 8.5 million persons in Brazil who had been infected by COVID-19 as of January 22, 2021 [2]. However, only 267 thousand cases of COVID-19 had been confirmed in Nepal over this same time period [2]. It is perhaps not surprising that the evidence shows a higher risk of mental distress in communities and countries with a higher prevalence of the disease [47], and this can also be related to the ensuing prolonged periods of quarantine and lockdown [3].
The finding that the pandemic-related psychological distress in the Americas was a larger problem than in Asia and Europe has not been reported previously. This is most likely driven by the high number of cases in both Brazil in South America and the USA in North America. In fact, the USA recorded the highest number of infections by January 22, 2021, at over 24 million cases [2]. Although COVID-19 infections were higher in Europe compared with Asia, a comparison of the two continents showed that the prevalence of psychological distress was significantly higher in Middle-East and Asian countries. Overall, this difference may be due to the higher testing rate in Europe and the potentially associated higher sense of security in the infected population. Moreover, European countries such as Germany and Italy had a lower COVID-19 case-fatality rate compared to China or Iran [2]. The results of previous studies on automobile accidents have suggest that self-reported fear is positively associated with mortality rate and differs across countries [48]. Other potential factors that may account for the observed variation in prevalence of COVID-19-related psychological distress across countries and continents include differences in restrictive measures, economic recessions, healthcare systems, biological, immunological, socio-demographics, and cultural differences [49,50,51].
There are some limitations to this study that should be considered in the interpretation of the data. First, all of the research in this meta-analysis were cross-sectional as they only gave a snapshot of the current situation with no longitudinal exploration. Second, there was lack of representation of studies in European countries other than Italy and Germany. Therefore, countries such as the UK where COVID-19 cases had reached over 3.5 million by the end of January, 2021 [2], were not represented. Third, it was not possible to assess gender differences between continents due to lack of data. For the same reasons, it was not possible to assess the prevalence of psychological distress for healthcare professionals compared to the general population. This is particularly important as many of these were on the front line exposed to high levels of physical and mental stress and had to cope with high levels of uncertainty, fear of contamination, and perceived lack of support [52,53,54,55]. Finally, the data provided by the studies included in this meta-analysis depended on the self-reported symptoms and signs via online survey. Thus, there is uncertainty related to actual mental status.
In future studies, the subjective nature of the online survey approach to assess psychological distress found be supported by more objective biomarker-based approaches. For example, the P1vital® PReDicT Test developed in Oxford, UK, provides an objective means of assessing a patient’s mental state through a 15 min online test comprised of facial expression recognition tasks and a series of health-related questions [56]. The facial recognition aspect of the test works as people with a mental illness such as depression often show a negative bias by interpreting indistinct expressions as less happy compared to non-depressed controls [57]. In addition, there is now considerable evidence for the utility of easily accessible molecular biomarkers in assessing the mental state. For example, evening levels of salivary cortisol have been linked with anxiety, depression, and posttraumatic stress disorder [58]. The cortisol awakening response (CAR) which measures the increase in cortisol secretion 30 to 45 min after awakening has been used as a marker of hypothalamic-pituitary-adrenal (HPA) axis activation, which can occur in both physical and mental health conditions including psychological stress [59,60,61]. In these studies, cortisol can be measured by enzyme-linked immunoadsorbent assay (ELISA) [62]. In addition, salivary amylase enzymatic activity has been used to monitor the effects on workers in stressful or isolated environments [63]. There has been considerable interest in the application of blood-based biomarkers such as cytokines, hormones, and growth factors in the study of mental disorders, which can be measured simultaneously using multiplex immunoassay platforms [64,65,66]. As examples, increased levels of C-reactive protein (CRP) and pro-inflammatory cytokines have been associated with depression following stroke [67], interleukins (IL)-1β, IL-5, and IL-6 have been detected in people with panic disorder [68], and the levels of brain-derived neurotrophic factor (BDNF) have been correlated with the disease progression of schizophrenia and depressive disorders [69]. Perhaps most critically, two studies also demonstrated the concept that mental illnesses could be detected several months or years before full manifestation with development of blood-based molecular biomarker algorithms for detection of individuals with a high risk of developing psychosis [70, 71]. In addition to assessing risk and current condition, all of the above digital and multiplex immunoassay approaches could be used to monitor any upsurge or recovery in mental status.
5 Conclusions and Future Perspectives
This meta-analysis suggested a high psychological impact due to the COVID-19 pandemic in many countries, with the highest levels detected in the Americas followed by Asian and European countries. In general, the distribution of the diverse spatiotemporal parameters of the pandemic may explain the heterogeneity in the degree of psychological distress among different geographical regions and countries. In addition, females appear to be more vulnerable to such distress and require further attention in terms of preventive and management strategies. However, the present study was limited by lack of a longitudinal analysis, poor representation of data from some countries in each continental group, and lack of data for assessment of gender differences on a per continent basis, and the reports of psychological stress levels were obtained by online survey and were therefore subjective in nature. Given these challenges, it will be important to incorporate the use of both digital and molecular biomarkers to increase the objectivity and accuracy of assessing the dynamic changes in mental health in the event of further disruptive waves of COVID-19 disease. There is also an urgent need for introduction of effective mental health interventions to assess and treat individuals in the highest risk groups for the best possible therapeutic outcomes.
References
Huang C, Wang Y, Li X, et al (2020) Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 395(10223):497–506
Worldometer: COVID-19 Coronavirus Outbreak; https://www.worldometers.info/coronavirus/ (accessed October 1, 2022).
Xiong J, Lipsitz O, Nasri F, et al (2020) Impact of COVID-19 pandemic on mental health in the general population: A systematic review. J Affect Disord 277:55–64
Preti E, Di Mattei V, Perego G, et al (2020) The Psychological Impact of Epidemic and Pandemic Outbreaks on Healthcare Workers: Rapid Review of the Evidence. Curr Psychiatry Rep 22(8):43. https://doi.org/10.1007/s11920-020-01166-z
Atalan A (2020) Is the lockdown important to prevent the COVID-9 pandemic? Effects on psychology, environment and economy-perspective. Ann Med Surg (Lond) 56:38–42
Brooks SK, Webster RK, Smith LE, et al (2020) The psychological impact of quarantine and how to reduce it: rapid review of the evidence. Lancet 395(10227):912–920
Vahedian-Azimi A, Moayed MS, Rahimibashar F, et al (2020) Comparison of the severity of psychological distress among four groups of an Iranian population regarding COVID-19 pandemic. BMC Psychiatry 20(1):402. https://doi.org/10.1186/s12888-020-02804-9
Park SC, Park YC (2020) Mental Health Care Measures in Response to the 2019 Novel Coronavirus Outbreak in Korea. Psychiatry Investig 17(2):85–86
Duan L, Zhu G (2020) Psychological interventions for people affected by the COVID-19 epidemic. Lancet Psychiatry 7(4):300–302
Qiu J, Shen B, Zhao M, et al (2020) A nationwide survey of psychological distress among Chinese people in the COVID-19 epidemic: implications and policy recommendations. Gen Psychiatr 33(2):e100213. https://doi.org/10.1136/gpsych-2020-100213
Al-Hanawi MK, Mwale ML, Alshareef N, et al (2020) Psychological Distress Amongst Health Workers and the General Public During the COVID-19 Pandemic in Saudi Arabia. Risk Manag Healthc Policy 13:733–742
Ramasubramanian V, Mohandoss AA, Rajendhiran G, et al (2020) Statewide Survey of Psychological Distress Among People of Tamil Nadu in the COVID-19 Pandemic. Indian J Psychol Med 42(4):368–373
Liu S, Heinz A (2020) Cross-Cultural Validity of Psychological Distress Measurement During the Coronavirus Pandemic. Pharmacopsychiatry 53(5):237–238
Moayed MS, Vahedian-Azimi A, Mirmomeni G, et al (2021) Coronavirus (COVID-19)-Associated Psychological Distress Among Medical Students in Iran. Advances in Experimental Medicine and Biology 1321, 245–251. https://doi.org/10.1007/978-3-030-59261-5_21
Moayed MS, Vahedian-Azimi A, Mirmomeni G, et al (2021) A Survey of Psychological Distress Among the Community in the COVID-19 Epidemic: A Cross-Sectional Study. Advances in Experimental Medicine and Biology 1321, 253–260. https://doi.org/10.1007/978-3-030-59261-5_22
Moayed MS, Vahedian-Azimi A, Mirmomeni G, et al (2021) Survey of Immediate Psychological Distress Levels Among Healthcare Workers in the COVID-19 Epidemic: A Cross-Sectional Study. Advances in Experimental Medicine and Biology 1321, 237–243. https://doi.org/10.1007/978-3-030-59261-5_20
Moher D, Liberati A, Tetzlaff J, Altman DG (2009) Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med 6(7):e1000097. https://doi.org/10.1371/journal.pmed.1000097
National Heart, Lung, and Blood Institute (2021) Study Quality Assessment Tools; https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools. Accessed September 28, 2022
Batra K, Singh TP, Sharma M, Batra R,Schvaneveldt N (2020) Investigating the Psychological Impact of COVID-19 among Healthcare Workers: A Meta-Analysis. Int J Environ Res Public Health 17(23):9096. https://doi.org/10.3390/ijerph17239096
Egger M, Davey Smith G, et al (1997) Bias in meta-analysis detected by a simple, graphical test. Bmj 315(7109):629–634
Begg CB, Mazumdar M (1994) Operating characteristics of a rank correlation test for publication bias. Biometrics 50(4):1088–1101
Miller JJ, Niu C, Moody S (2020) Child welfare workers and peritraumatic distress: The impact of COVID-19. Child Youth Serv Rev 119:105508. https://doi.org/10.1016/j.childyouth.2020.105508
Abad A, da Silva J, de Paiva Teixeira L, et al (2020) Evaluation of Fear and Peritraumatic Distress during COVID-19 Pandemic in Brazil. Advances in Infectious Diseases 101:84–194. https://doi.org/10.4236/aid.2020.103019
Hübner CVK, Lima Bruscatto M, Dourado Lima R (2020) Distress among Brazilian university students due to the Covid-19 pandemic: survey results and reflections. medRxiv. https://doi.org/10.1101/2020.06.19.20135251
Zhang SX, Wang Y, Afshar Jahanshahi A, et al (2020) First study on mental distress in Brazil during the COVID-19 crisis. medRxiv. https://doi.org/10.1101/2020.04.18.20070896
Krüger-Malpartida H, Pedraz-Petrozzi B, Arevalo-Flores M, et al (2020) Effects on Mental Health After the COVID-19 Lockdown Period: Results From a Population Survey Study in Lima, Peru. medRxiv. https://doi.org/10.21203/rs.3.rs-81117/v1
Picchianti Diamanti A, Cattaruzza MS, Di Rosa R, et al (2020) Psychological Distress in Patients with Autoimmune Arthritis during the COVID-19 Induced Lockdown in Italy. Microorganisms 8(11):1818. https://doi.org/10.3390/microorganisms8111818
Bonati M, Campi R, Zanetti M, et al (2021) Psychological distress among Italians during the 2019 coronavirus disease (COVID-19) quarantine. BMC Psychiatry 21(1):20. https://doi.org/10.1186/s12888-020-03027-8
Pakenham KI, Landi G, Boccolini G, et al (2020) The moderating roles of psychological flexibility and inflexibility on the mental health impacts of COVID-19 pandemic and lockdown in Italy. J Contextual Behav Sci 17:109–118
Landi G, Pakenham KI, Boccolini G, et al (2020) Health Anxiety and Mental Health Outcome During COVID-19 Lockdown in Italy: The Mediating and Moderating Roles of Psychological Flexibility. Front Psychol 11:2195. https://doi.org/10.3389/fpsyg.2020.02195
Ciprandi R, Bonati M, Campi R, et al (2020) Psychological distress in adults with and without cystic fibrosis during the COVID-19 lockdown. J Cyst Fibros 20(2):198–204
Costantini A, Mazzotti E (2020) Italian validation of CoViD-19 Peritraumatic Distress Index and preliminary data in a sample of general population. Riv Psichiatr 55(3):145–151
Marzo RR, Singh A, Mukti RF (2021) A survey of psychological distress among Bangladeshi people during the COVID-19 pandemic. Clin Epidemiol Glob Health 10:100693. https://doi.org/10.1016/j.cegh.2020.100693
Shrestha DB, Thapa BB, Katuwal N, et al (2020) Psychological distress in Nepalese residents during COVID-19 pandemic: a community level survey. BMC Psychiatry 20(1):491. https://doi.org/10.1186/s12888-020-02904-6
Jahanshahi AA, Dinani MM, Madavani AN, et al (2020) The distress of Iranian adults during the Covid-19 pandemic - More distressed than the Chinese and with different predictors. Brain Behav Immun 87:124–125
Nair AKR, Karumaran CS, Kattula D, et al (2020) Stress levels of Indian endodontists during COVID-19 pandemic. Rev Cubana Estomatol 57(3):e3445. https://www.redalyc.org/journal/3786/378664876002/html/. Accessed September 28, 2022
Samson P, Narayan Shah J (2020) Peritraumatic distress and perceived mental healthcare needs among residents of a community housing during COVID-19. Journal of Patan Academy of Health Sciences 7(2):14–22
Marzo RR, Quilatan Villanueva III E, Martinez Faller E, Moralidad Baldonado A (2020) Factors Associated with Psychological Distress among Filipinos during Coronavirus Disease-19 Pandemic Crisis. Open Access Maced J Med Sci 8(T1):309–313
El-Abasiri RA, RilleraMarzo R, Abdelaziz H, et al (2020) Evaluating the Psychological Distress of the Coronavirus Disease 2019 Pandemic in Egypt. European Journal of Molecular & Clinical Medicine 7(5):1–12
Political Map of Countries of Western Asia. https://www.nationsonline.org/oneworld/map/Political-Map-of-Countries-of-Western-Asia.htm. Accessed September 29, 2022
Middle East region, Asia, Africa, and Europe. https://www.britannica.com/place/Middle-East. Accessed September 29, 2022
Sareen J, Erickson J, Medved MI, et al (2013) Risk factors for post-injury mental health problems. Depress Anxiety 30(4):321–327
Chaplin TM (2015) Gender and Emotion Expression: A Developmental Contextual Perspective. Emot Rev 7(1):14–21
COVID-19 and gender equality: Countering the regressive effects; July 15, 2020. https://www.mckinsey.com/featured-insights/future-of-work/covid-19-and-gender-equality-countering-the-regressive-effects. Accessed September 29, 2022
Chakraborty A, Karmakar S (2020) Impact of COVID-19 on Obsessive Compulsive Disorder (OCD). Iran J Psychiatry 15(3):256–259
Yassa M, Yassa A, Yirmibeş C, et al (2020) Anxiety levels and obsessive compulsion symptoms of pregnant women during the COVID-19 pandemic. Turk J Obstet Gynecol 17(3):155–160
Marques de Miranda D, da Silva Athanasio B, Sena Oliveira AC, Simoes ESAC (2020) How is COVID-19 pandemic impacting mental health of children and adolescents? Int J Disaster Risk Reduct 51:101845. https://doi.org/10.1016/j.ijdrr.2020.101845
Kovess-Masfety V, Sowa D, Keyes K, et al (2017) The association between car accident fatalities and children’s fears: A study in seven EU countries. PLoS One 12(8):e0181619. https://doi.org/10.1371/journal.pone.0181619
Mortensen CR, Becker DV, Ackerman JM, et al (2010) Infection breeds reticence: the effects of disease salience on self-perceptions of personality and behavioral avoidance tendencies. Psychol Sci 21(3):440–447
Derivois D, Cénat JM, Joseph NE, et al (2017) Prevalence and determinants of post-traumatic stress disorder, anxiety and depression symptoms in street children survivors of the 2010 earthquake in Haiti, four years after. Child Abuse Negl 67:174–181
Amerio A, Bianchi D, Santi F, et al (2020) Covid-19 pandemic impact on mental health: a web-based cross-sectional survey on a sample of Italian general practitioners. Acta Biomed 91(2):83–88
Kanellopoulos D, Solomonov N, Ritholtz S, et al (2021) The CopeNYP program: A model for brief treatment of psychological distress among healthcare workers and hospital staff. Gen Hosp Psychiatry 73:24–29
Khaing NEE, Lim CS, Soon SP, Oh HC (2022) Prevalence and correlates of psychological distress and coronavirus anxiety among hospital essential services workers in Singapore. Ann Acad Med Singap 51(5):283–291
Osório FL, Zuardi AW, Silveira ILM, et al (2022) Monitoring the Mental Health and Professional Overload of Health Workers in Brazil: A Longitudinal Study Considering the First Wave of the COVID-19 Pandemic. Front Psychiatry 13:852157. https://doi.org/10.3389/fpsyt.2022.852157
Beck E, Daniels J (2022) Intolerance of uncertainty, fear of contamination and perceived social support as predictors of psychological distress in NHS healthcare workers during the COVID-19 pandemic. Psychol Health Med; Jul 6:1–13. https://doi.org/10.1080/13548506.2022.2092762
P1vital® PReDicT Test. https://www.p1vital.com/healthcare/p1vital-predict-test/. Accessed September 30, 2022
Browning M, Bilderbeck AC, Dias R, et al (2021) The clinical effectiveness of using a predictive algorithm to guide antidepressant treatment in primary care (PReDicT): an open-label, randomised controlled trial. Neuropsychopharmacology 46(7):1307–1314
Aardal-Eriksson E, Eriksson TE, Holm AC, Lundin T (1999) Salivary cortisol and serum prolactin in relation to stress rating scales in a group of rescue workers. Biol Psychiatry 46(6):850–855
Wüst S, Wolf J, Hellhammer DH, et al (2000) The cortisol awakening response - normal values and confounds. Noise Health 2(7):79–88
Fekedulegn DB, Andrew ME, Burchfiel CM, et al (2007) Area under the curve and other summary indicators of repeated waking cortisol measurements. Psychosom Med 69(7):651–659
Stalder T, Kirschbaum C, Kudielka BM, et al (2016) Assessment of the cortisol awakening response: Expert consensus guidelines. Psychoneuroendocrinology 63:414–432
Voller A (1978) The enzyme-linked immunosorbent assay (ELISA) (theory, technique and applications). Ric Clin Lab 8(4):289–298
Hunter MR, Gillespie BW, Chen SY (2019) Urban Nature Experiences Reduce Stress in the Context of Daily Life Based on Salivary Biomarkers. Front Psychol 10:722. https://doi.org/10.3389/fpsyg.2019.00722
Stephen L (2017) Multiplex Immunoassay Profiling. Methods Mol Biol 1546:169–176
Stephen L, Schwarz E, Guest PC (2017) Multiplex Immunoassay Profiling of Serum in Psychiatric Disorders. Adv Exp Med Biol 974:149–156
Guest PC, Abbasifard M, Jamialahmadi T, et al (2022) Multiplex Immunoassay for Prediction of Disease Severity Associated with the Cytokine Storm in COVID-19 Cases. Methods Mol Biol 2511:245–256
Engeland CG, Bosch JA, Rohleder N (2019) Salivary Biomarkers in Psychoneuroimmunology. Curr Opin Behav Sci 28:58–65
Young JJ, Bruno D, Pomara N (2014) A review of the relationship between proinflammatory cytokines and major depressive disorder. J Affect Disord 169:15–20
Quagliato LA, Nardi AE (2018) Cytokine alterations in panic disorder: A systematic review. J Affect Disord 228:91–96
Perkins DO, Jeffries CD, Addington J, et al (2015) Towards a psychosis risk blood diagnostic for persons experiencing high-risk symptoms: preliminary results from the NAPLS project. Schizophr Bull 41(2):419–428
Chan MK, Krebs MO, Cox D, et al (2015) Development of a blood-based molecular biomarker test for identification of schizophrenia before disease onset. Transl Psychiatry 5(7):e601. https://doi.org/10.1038/tp.2015.91
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
1 Electronic Supplementary Material
Supplementary Table 4.ST1
Methodological quality assessment of included studies using the National Institutes of Health (NIH) tool (DOCX 16 kb)
Rights and permissions
Copyright information
© 2023 The Author(s), under exclusive license to Springer Nature Switzerland AG
About this chapter

Cite this chapter
Ashtari, S. et al. (2023). Psychological Distress Impact of Coronavirus Disease (COVID-19) Outbreak on Three Continents: A Systematic Review and Meta-analysis. In: Guest , P.C. (eds) Application of Omic Techniques to Identify New Biomarkers and Drug Targets for COVID-19. Advances in Experimental Medicine and Biology(), vol 1412. Springer, Cham. https://doi.org/10.1007/978-3-031-28012-2_4
Download citation
DOI: https://doi.org/10.1007/978-3-031-28012-2_4
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-031-28011-5
Online ISBN: 978-3-031-28012-2
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)