
Abstract
Nitric oxide (NO) is a diffusible free radical and universal messenger that is produced from L-arginine by three different isoforms of nitric oxide synthases (NOS), neuronal (nNOS), inducible (iNOS) and endothelial NOS (eNOS). NO plays an important role in the regulation of variety of physiological functions including myocardial contractility, vascular tone, blood pressure, cell growth, proliferation and platelet aggregation. Most of the effects of NO are mediated through the activation of soluble guanylate cyclase–cGMP system, however, cGMP-independent pathways have also been shown to be responsible in mediating its effects. The levels of NO are regulated by several factors and cofactors required for the activation of NOS, however, reduced bioavailability of these factors results in the decreased levels of NO and thereby endothelial dysfunction leading to the pathogenesis of cardiovascular diseases including hypertension, diabetes, atherosclerosis etc. This review will focus on the role of NO in physiology and pathophysiology of cardiovascular system including vascular remodeling, hypertension and the underlying molecular mechanisms contributing to these functions.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
Introduction
Cardiovascular disease that affect the heart and/or the blood vessels is considered as leading cause of morbidity and mortality worldwide [1]. Several risk factors including hypertension, vascular remodeling, insulin resistance, endothelial dysfunction, reduced cardiovascular nitric oxide (NO) bioavailability, cardiac hypertrophy [2], and alterations in the circulating lipids are implicated in pathophysiology of cardiovascular disease [3]. Nitric oxide (NO) is a ubiquitous intracellular messenger that acts as an important biological signaling molecule involved in the regulation of variety of physiological functions including myocardial contractility, vascular tone, blood pressure regulation, cell growth, proliferation, platelet aggregation etc. [4] (Fig. 2.1). Under physiological conditions, NO exerts cardiovascular protection, however, dysregulation of NO production contributes to endothelial dysfunction leading to the pathogenesis and progression of cardiovascular diseases including hypertension, diabetes, atherosclerosis etc.

Role of nitric oxide (NO) in the regulation of physiological functions
Nitric Oxide Synthesis
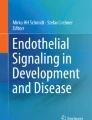
NO is short lived free radical generated by the oxidation of L-arginine to L-citruline, a reaction catalyzed by nitric oxide synthase (NOS) [5, 6] and requires the presence of several cofactors including flavin mononucleotide (FMN), flavin adenine dinucleotide (FAD), NADPH, tetra-hydrobiopterin (BH4), heme prosthetic group as well as the redox cofactor (Fig. 2.2) [7]. Three isoforms of NO synthases are identified named neuronal NOS (nNOS or NOS I), inducible NOS (iNOS or NOS II) and endothelial NOS (eNOS or NOS III). In addition, a novel constitutively active mitochondrial NOS (mtNOS) has also been identified in mitochondria from liver that appears to be involved in Ca2+ regulation [8]. nNOS and eNOS are constitutive enzymes and predominantly expressed in neuronal and endothelial cells (EC) as well as in other cell types including vascular smooth muscle cells (VSMC) [9]. Both nNOS and eNOS are regulated by intracellular Ca2+/ calmodulin (CaM) whereas iNOS is inducible at the level of gene transcription, Ca2+—independent and expressed in macrophages and other tissues in response to inflammatory mediators including cytokines and endotoxins [10–12]. eNOS is also activated independently of Ca2+ upon phosphorylation by Akt in response to shear stress, estrogens and insulin [13]. In addition, nNOS and iNOS are cytosolic enzymes whereas eNOS is associated with the membranes of EC [14, 15]. These two isoforms of NOS are crucial regulators of cardiovascular homeostasis and regulate vascular tone and blood flow, inhibit platelet aggregation and adhesion, modulate cardiac contractility and inhibit VSMC proliferation [4]. The structures of iNOS, eNOS and nNOS have been determined [16, 17]. All three NOS isoforms are dimers and contain two major functional domains fused into a single polypeptide. The N-terminal catalytic domain possesses the binding sites for heme, redox cofactor, BH4 and CaM. The C-terminal reductase domain has binding sites for FMN, FAD and NADPH. NOS activation relies on the presence of the cofactor BH4 and the substrate L-arginine to couple the oxidation of molecular oxygen to produce NO [18]. Two molecules of BH4 bind to each eNOS dimer and facilitate electron transfer for the oxidation of L-arginine. BH4 thus maintains eNOS in a dimeric state and preserves the endothelial function [19].

Nitric oxide synthesis a Under physiological conditions, nitric oxide is synthesized by the oxidation of L-arginine to L-citrulline, a reaction catalyzed by nitric oxide synthase (NOS) and requires the presence of several cofactors including flavin mononucleotide (FMN), flavin adenine dinucleotide (FAD), NADPH, tetra-hydrobiopterin (BH4), heme prosthetic group as well as the redox cofactor b Under pathphysiological conditions the absence or limited availability of either substrate or cofactor BH4 and augmented levels of oxidative stress result in the uncoupled eNOS that produces O2- instead of NO and forms ONOO-that further promotes eNOS uncoupling leading to endothelial dysfunction and the pathogenesis of cardiovascular diseases
Regulation of Intracellular Levels of Nitric Oxide
Several factors which are involved in the activation of NOS play a key role in the regulation of intracellular levels of NO. These include the substrate L-arginine, cofactors including BH4, asymmetrical dimethylarginine (ADMA), NG -mono-methyl-L-arginine (L-NMMA), naturally occurring metabolites that circulate in the plasma [20]. The absence or limited availability of either substrate or cofactor BH4 and increased circulating levels of arginase, a hydrolytic enzyme that converts L-arginine to urea and L-ornithine, ADMA and L-NMMA, inhibitors of NOS, result in the decreased production of NO leading to endothelial dysfunction and the pathogenesis of cardiovascular diseases (Fig. 3a) [20–24]. In addition, oxidative stress also contributes to the decreased levels of NO. The augmented oxidative stress oxidizes BH4 to BH2 resulting in the destabilization of eNOS dimer which becomes uncoupled and leads to the production of superoxide anion \((\text{O}_{2^{-}})\) instead of NO, the process is referred to as eNOS uncoupling (Fig. 2.3a) [25]. \(\text{O}_{2^{-}}\) reacts with NO forming peroxynitrite (ONOO−), a strong cytotoxic oxidant and reactive nitrogen species (RNS) that induces nitrosative stress. ONOO− in turn oxidizes BH4 to BH2 and further promotes eNOS uncoupling [26]. ONOO− reacts with lipids, DNA, and proteins, causing damage to these macromolecule, interferes with important vascular signaling pathways and contributes to various cardiovascular dysfunction [27] (Fig. 2.3).

a Factors that may contribute to reduced bioavailability of nitric oxide leading to endothelial dysfunction and pathogenesis of cardiovascular diseases. Several factors that could reduce NO availability are; the reduced levels of substrate L-arginine, BH4, an essential cofactor and augmented levels of circulating inhibitors such as asymmetrical dimethylarginine (ADMA), NG -mono-methyl-L-arginine (L-NMMA), arginase, Ang II and destruction of NO by reactive oxygen species (ROS). b Factors that increase the expression of eNOS and NO levels and exert vascular protection. These factors include NO donors, antioxidants, adiponectin, AT1 receptor blocker, ACE inhibitor, Statins, C-ANP4-23, a specific agonist of natriuretic peptide receptor-C (NPR-C) and resveratrol
On the other hand, several hormonal factors are also implicated in the regulation of intracellular levels of NO. Angiotensin II (Ang II) that promotes vascular remodeling, increases oxidative stress and blood pressure, has been shown to decrease the levels of eNOS and NO in VSMC [28]. On the other hand, NO donors, antioxidants, adiponectin, AT1 receptor blocker, ACE inhibitor, Statins, C-ANP4-23, a specific agonist of natriuretic peptide receptor-C (NPR-C) and resveratrol were shown to increase the intracellular levels of NO and exert vascular protection and ameliorate hypertension (Fig. 2.3b) [29–39].
Cross-Talk Between Oxidative Stress and Nitrosative Stress
Oxidative stress has been shown to play an important role in the pathogenesis of cardiovascular diseases [40–43]. Oxidative stress is caused by the overproduction of reactive oxygen species (ROS) and a decreased elimination of these ROS by antioxidants. ROS are produced by a wide array of enzymes that include NADPH oxidases, xanthine oxidase, peroxidases, lipoxygenases, cyclooxygenases and complex I and III of mitochondrial respiratory chain and eNOS uncoupling [44]. NADPH oxidases and xanthine oxidase catalyze the formation of \((\text{O}_{2^{-}})\) by single electron reduction of molecular oxygen which is converted to hydrogen peroxide (H2O2) by superoxide dismutase (SOD). Several studies have demonstrated a reciprocal relationship between ROS and RNS. The augmented levels of ROS decrease the levels of NO, whereas decreased levels of ROS have been shown to increase NO synthesis. For example, the antioxidant ascorbate that decreases the levels of \((\text{O}_{2^{-}})\) resulted in increased NO synthesis in EC by improving the binding of BH4 to NOS and stabilizing the dimeric structure of NOS [31, 32]. In addition, Huang et al. have also demonstrated that ascorbate augmented the activity of NOS in endothelial cells by increasing the levels of BH4 [39]. Modulation of O2− by NO through the regulation of SOD-1 in VSMC has also been reported [45]. In addition, in VSMC from spontaneously hypertensive rats (SHR), increased levels of \((\text{O}_{2^{-}})\) are associated with decreased levels of NO and augmented levels of ONOO−. Furthermore, elevating the intracellular levels of NO by NO donors decreased the augmented levels of \((\text{O}_{2^{-}})\) and ONOO− in these cells [29, 46]. Similarly, C-ANP4-23 (natriuretic peptide receptor-C) agonist- induced suppression of enhanced levels of \((\text{O}_{2^{-}})\) provoked by Ang II was associated with augmented levels of NO in VSMC [28]. The increase in ROS and subsequent increased ONOO—formation reduces the bioavailability of NO and results in endothelial dysfunction. Thus the imbalance between the formation of RNS and ROS plays a critical role in the pathogenesis of cardiovascular diseases [40, 47–50].
Nitric Oxide Signaling
The canonical signaling mechanism by which NO exerts most of its biological effects is through the activation of soluble guanylate cyclase (sGC), The sGC is a heterodimeric protein composed of two subunits, α and β, of which the β subunit contains a heme moiety that confers the NO-sensitivity of the enzyme [51, 52]. Binding of NO to heme results in a conformational change of cGC and activation of the catalytic domain [52] that converts intracellular GTP into the second messenger cyclic guanosine 3′5′-monophosphate (cGMP) [52, 53], cGMP interacts with a variety of effector proteins including cGMP-dependent protein kinases (PKGs) [53], cGMP-regulated phosphodiesterases (PDEs) and ion channels. Two different types of PKGs, type I (PKG-1) and type II (PKG-2) are expressed in mammalian tissues, however, their relative distribution is tissue- and species- dependent [54, 55]. In cardiovascular tissues, a predominant expression of PKG-1 has been reported that mediates the anti-proliferatve effect of cGMP [54, 56–58]. PKG-1 is a serine/threonine kinase and elicits its effects through the phosphorylation of multiple targets which include IP3 receptor, phospholamban, troponin, myosin light chain phosphatase, c-raf kinase, Ca2+ and K+ channels. All these signaling targets are implicated in the reduction of intracellular levels of Ca2+ or in decreasing the Ca2+ sensitivity of contraction or both, resulting in the vasorelaxation (Fig. 2.4) [53, 59–63]. In addition, NO has also been shown to mediate some of its effects through cGMP-independent pathways because 1H- [1, 2, 4] oxadiazolol [4,3-α]quinoxalin-1-one, ODQ, a selective inhibitor of sGC was unable to inhibit these NO-mediated effects. For example, NO decreases the levels of Giα proteins as well as proliferation of VSMC by cGMP-independent pathway [29]. The cGMP-independent pathways implicated in NO-mediated effects include Ras, MAP kinase [46, 64], cyclin dependent kinase inhibitor P21, [65, 66] and cAMP\PKA signaling pathway [67–69]. In addition, posttranslational modification such as S-nitrosylation [70, 71], eNOS S-glutathionylation [72] and tyrosine nitration [73] mediated effects of NO are also independent of sCG and cGMP and regulate downstream pathways contributing to cell proliferation [74–77]. Furthermore, S-nitrosylation-induced activation of VSMC Ca2+-dependent K+ channels has also been shown as a potential mechanism of cGMP-independent vasorelaxation (Fig. 2.4) [78].

Signaling mechanisms implicated in NO-mediated cardiovascular protection. NO induces vasorelaxation through S-nitrosylation-induced activation of Ca2+-dependent K+ channels as well as via sGC/cGMP/protein kinase G-dependent pathway. The beneficial effects of NO on remodeling of the vessels include the attenuation of signaling pathways involved in the activation of the hypertrophic, migratory and proliferative program in the cardiovascular tissues. NO through the inhibition of G12/G13-Rho/ROCK pathway exerts antimigratory and antihypertrophic effects. In addition, NO decreases ROS which through the inhibition of growth factor receptor activation and MAPK signaling inhibits Giα protein expression and modulates cell cycle regulatory proteins leading to decreased proliferation
Nitric Oxide and Cardiovascular Diseases
NO plays an important role in the protection against the onset and progression of cardiovascular disease that include regulation of blood pressure and vascular tone, inhibition of platelet aggregation and smooth muscle cell proliferation [4]. Endothelial dysfunction due to the decreased availability of NO is the contributing factor in the pathogenesis of cardiovascular diseases. In the following section, the protective role of NO will be discussed in different pathologies.
Vascular Remodeling and Molecular Mechanisms
Vascular remodeling refers to alterations in the structure of resistance vessels and contributes to the pathophysiology of vascular diseases, such as atherosclerosis, restenosis, and hypertension [79] and is associated with alteration in VSMC growth, hypertrophy, migration etc. [80, 81]. Vascular remodeling is influenced by dynamic interactions between local growth factors, vasoactive substances, and hemodynamic stimuli [82]. Several intracellular signaling pathways that regulate the expression of upstream and downstream target genes are involved in the proliferation, hypertrophy and migration of VSMC. Vasoactive peptides such as Ang II and endothelin-1(ET-1) as well as growth factors receptors such as epidermal growth factor receptor (EGFR) and platelet derived growth factor receptor (PDGFR) all contribute to VSMC hypertrophy, proliferation and migration through the activation of several signaling pathways including Giα/Gqα, MAP kinase and Rho-kinase (ROCK), an effector of a small G protein [83–94]. In addition, enhanced oxidative stress induced by Ang II is also implicated in the enhanced expression of Giα proteins and proliferation of VSMC through the transactivation of EGF-R and MAP kinase signaling [91]. Furthermore, the augmented levels of endogenous vasoactive peptides including Ang II and ET-1 have also been shown to contribute to hyperproliferation as well as hypertrophy of VSMC from SHR through ROS and ROS-mediated transactivation of EGF-R/PDGF-R and MAP kinase signaling pathways [95–99]. Hyperproliferation of VSMC is associated with accelerated entry of cells from G0/G1 phase of cell cycle to the synthetic phase [100]. Ang II- and FBS-induced exaggerated growth of VSMC from SHR is associated with progression from G1 to S phase [98, 101]. The role of enhanced expression of Giα proteins in the overexpression of cell cycle proteins including cyclin D1, cyclin D1-dependent kinase (Cdk)4 and phospho-retinoblastoma protein (pRb) and resultant hyper-proliferation of VSMC from SHR has been demonstrated [102, 103]. Furthermore, we and others have demonstrated that several distinct signal transduction pathways including c-Src, reactive oxygen species (ROS), growth factor receptor transactivation, MAP kinase, PI3Kinase, that are implicated in the overexpression of Giα proteins, also contribute to the overexpression of the cell cycle proteins and vascular remodeling by promoting VSMC proliferation [48, 92, 103–106].
Nitric Oxide and Vascular Remodeling
A multitude of studies using in vitro and in vivo models have shown that an increase in the cellular levels of NO, either by direct delivery of NO donors or gene transfer of eNOS or iNOS, potently suppressed proliferation, migration and hypertrophy in VSMC and, neointimal growth [107–112]. Although the precise molecular events that provoke these responses remains elusive, accumulated evidence has suggested that modulation of key components of cell cycle regulatory proteins and signaling pathways responsible to drive these events play an important role. For example, eNOS overexpression in VSMC isolated from pig coronary arteries resulted in attenuation of PDGF-induced proliferation that was accompanied by reduced levels of cell cycle regulatory proteins cyclin A, and a delayed expression of cyclin E [113]. Similarly, a reduction in the expression levels of cyclin A and cyclin-dependent kinase (cdk) 2 was associated with diethylenetriamine NONOate (DETNONOate)-induced reduction of fetal calf serum (FCS)-induced cell proliferation in human VSMC [114]. S-nitroso-N-acetylpenicillamine (SNAP) was also reported to inhibit FCS- and FGF-induced cell cycle progression in VSMC via inhibition of Cdk2 and upregulation of p21 [115]. In addition, SNAP was also shown to inhibit the overexpression of Giα proteins and hyperproliferation of VSMC from SHR by cGMP-independent mechanism and involves ROS and ROS-mediated transactivation of EGF-R/PDGF-R and MAP kinase signaling pathways [46]. More recent in vivo studies have demonstrated that NO donor, sodium nitroprusside (SNP), reduced the increased BP in SHR and reduced the heightened expression of Giα, cyclin D1, Cdk 4 and pRb and augmented the reduced levels of cdk inhibitors p27 and p21 (Fig. 2.4) [116]. Interestingly, NO has been shown to upregulate p21 levels by preventing its degradation in rat aortic VSMC and in pulmonary VSMC [65, 66]. The antihypertensive effect of SNP in SHR was associated with a reduction in the overexpression of AT1R, growth factor receptor phosphorylation, ERK1/2 activation an Giα protein expression in VSMC [116]. SNP as well as 8-bromo cyclic GMP were also reported to block ET-1 and EGF-induced Ras/ MEK/ ERK1/2 pathway while suppressing DNA and protein synthesis in VSMC [117, 118]. Thus, inhibition of the signaling events involved in cell cycle progression appears to be a key mechanism for the antiproliferative effects of NO. Furthermore, the implication of both cGMP—dependent and—independent pathways have been suggested to elicit this response [46, 109, 119, 120].
Several NO donors including SNP, SNAP, DETNONOate, spermineNONOate and S-nirosoglutathione have also been shown to reduce Ang II-evoked VSMC migration [108, 121, 122]. In addition, increasing the intracellular levels of NO by eNOS gene transfer also suppressed the migration of VSMC induced by Ang II or PDGF [112, 123, 124]. The molecular mechanism implicated in these events appear to be mediated through the inhibition of matrix metalloproteases (MMPs) 2 and 3 as well as the Ras family of small G- protein, Rho A and its effector, RhoA kinase (ROCK) [112]. However, these effects were shown to be independent of growth factor receptor transactivation and ERK signaling pathway [112]. An involvement of RhoA/ROCK pathway in mediating the antihypertrophic action of adiponectin and NO was also reported (Fig. 2.4) [35]. Interestingly, this inhibitory response was associated with a reduction in Ang II-induced phosphorylation of cofilin and actin cytoskeletal remodeling as judged by altered F-actin/G-actin ratio [35].
Consistent with the antiproliferative, antimigratory and antihypertrophic effects of NO, several studies have reported protective effects of NO donors and NOS overexpression on neointimal growth and hyperplasia in animal models. Among the first reports to implicate NO in blocking neointimal hyperplasia in a rabbit model of vascular injury, utilized L-arginine, a substrate of NOS to raise tissue levels of NO [125]. These studies demonstrated that administration of L-arginine by gavage reduced the intimal hyperplasia by about 39% in balloon catheter-injured rabbit thoracic aorta and co-administration of L-NAME reversed the protective effect of L–arginine and suggest that NO generation was responsible for this effect [125]. This observation was quickly confirmed, and showed that as compared to systemic delivery, the topical application of L-arginine was slightly more effective in inhibiting neointimal growth in a rat carotid artery injury model [126]. These studies prompted several investigators to further explore the usefulness of NO donors in conferring beneficial effects in rat, rabbit or porcine models of vascular injury [127–131]. For example, intravenous infusion of 4-hydoxymethy-furazone-3 carboxylic acid-2 oxide, an organic NO donor not only reduced neointimal thickening in injured rat carotid artery but also inhibited the proliferation of VSMC [127, 129]. In addition, continuous chronic inhalation of NO also resulted in a similar response and decreased the intimal growth by about 43% after 14 days of therapy [129]. Moreover, perivascular, topical delivery of short and long acting NO donors, 1-[2-(carboxylato)pyrrolidin-1-yl]dazen-1-ium-1,2-diolate (PROLI/NO) (short half-life) and diazeniumdiolated poly(acrylonitrile) (PAN/NO) (long half-life) was also found to suppress neointimal hyperplasia in rat carotid artery model [132, 133]. This group also reported that systemic administration of S-nitrosylated(S-NITROSYL(SNO))-targeted nanofibre suppressed neointimal hyperplasia in rat model of carotid artery injury [45]. Similar to NO donors, local delivery of eNOS or iNOS genes were also reported to suppress the neointimal growth in both rodent and porcine models of vessel injury [134–141]. Thus, there is ample evidence to support that NO donors or gene transfer of NOS exert beneficial effects in suppressing vascular remodeling and inhibiting neointimal hyperplasia in cellular and animal model systems. However, because of the labile nature of NO and, confounding factors of targeted gene delivery and appropriate transfer vectors, some limitations for its translational use have been noted [142]. To overcome these issues, several groups are engaged in developing nanofiber and stent-based delivery systems for NO production and gene delivery for therapy of vasculopathies [143, 144].
Hypertension and Molecular Mechanisms
Hypertension is a multifactorial disease where the interplay between neuronal, hormonal and cellular signaling processes contributes to the pathogenesis. Several factors including vasoactive peptides, the renin–angiotensin–aldosterone system (RAAS), activation of the sympathetic nervous system, abnormalities in G protein-coupled receptor (GPCR) signaling, oxidative and nitrosative stress and inflammation are implicated in the pathophysiology of hypertension.
Ang II, a dominant player of renin–angiotensin system plays an important role in the development of blood pressure through the activation of downstream signaling pathways including oxidative stress. Ang II has been shown to increase the levels of ROS, ONOO- as well as of Giα proteins and decrease the levels of eNOS and NO in aortic VSMC [28], which appear to be important contributing factors in the development of hypertension [145, 146]. Furthermore, NO has also been shown to decrease the expression of Giα proteins in aortic VSMC [64] which may be one of the molecular pathways responsible for NO-induced reduction in blood pressure in SHR [29]. Consistent with this notion, the enhanced oxidative stress, decreased levels of eNOS and NO have been shown to be associated with the overexpression of Giα proteins and downstream signaling pathways including growth factor receptor transactivation and MAP kinase and PI3Kinase in VSMC from SHR [147]. Studies showing that reduction in ROS generation by C-ANP4-23 and resveratrol attenuated increased blood pressure through the inhibition of exaggerated levels of Gi \(\alpha\) proteins provide additional evidence for the role of this pathway in the pathogenesis of hypertension [148, 149].
Nitric Oxide and Hypertension
Accumulating evidence demonstrates that NO produced by the endothelial nitric oxide synthase (eNOS) in the vascular endothelium, plays a critical role in the regulation of blood pressure [150, 151]. NO stimulates guanylyl cyclase to increase cGMP production, which promotes vasodilatation of VSMC [152, 153], prevents platelet adhesion and aggregation, exerts antiproliferative and antimigratory effects on EC and VSMC [154, 155]. Reduction in NO bioavailability is the hallmark of endothelial dysfunction and contributes to the development of hypertension and other vascular diseases [156–158]. This has been demonstrated by several studies using knockout mice as well as hypertensive patients and rat models. eNOS knockout mice develop high blood pressure and display decreased vasodilation, whereas nNOS or iNOS deficient mice did not show any changes in the blood pressure [159, 160]. In addition, the role of sGC and PKG1, the downstream signaling molecules of NO in NO-mediated vasorelaxation and blood pressure regulation has also been demonstrated by using knockout mice. sGC deficient mice (sGCβ1−/−) as well as smooth muscle cell specific sGCβ1−/− mice exhibit higher blood pressure than wild type mice [161, 162], however,in these mice, NO donor was ineffective in reducing the blood pressure and the vasodilatation of isolated aortic rings [162]. These results suggest that NO-inducible sGC activity is required for NO in mediating vasorelaxation in these vessels. Similarly, PKG1 deficient mice also developed hypertension and elicited an impaired dilation of large conductance and small resistance arteries in response to NO-cGMP signaling [163, 164]. In addition, the inhibition of eNOS by Nω‐nitro‐l‐arginine methyl ester (L-NAME) was also shown to result in the development of hypertension in rats and was associated with increased levels of Giα proteins, decreased cGMP levels and increased levels of Ang II [165, 166]. The decreased levels of NO due to increased oxidative stress has also been shown to contribute to high blood pressure in other models of hypertensive rats. In SHR, the levels of AT1 receptor, Giα proteins, \((\text{O}_{2^{-}})\) and ONOO- were increased whereas the levels of eNOS and NO were decreased [116, 148]. Similarly, the expression of eNOS mRNA was downregulated in mesenteric arterioles of high-salt treated Dahl hypertensive rats [167]. Deoxycorticosterone acetate-salt hypertensive rats (DOCA-Salt HR) exhibited reduced eNOS phosphorylation that resulted in decreased NO/cGMP signaling in mesenteric arteries [168]. In addition, NO-mediated relaxation was depressed in mesenteric arteries of hypertensive rats with reduced renal mass, due to decreased bioavailabilty of NO [169, 170]. An impairment of NO-mediated vasodilatation in patients with essential hypertension has also been demonstrated [171]. On the other hand, several studies have demonstrated that the elevation of intracellular NO by NO donors ameliorates the development of hypertension in different models of hypertensive rats (HR). SNP was shown to attenuate high blood pressure in SHR through the inhibition of oxidative stress, overexpression of AT1 receptor, Giα proteins and ONOO− levels [116]. In addition, supplementation of exogenous nitrite that augments the intracellular levels of NO [172] also attenuated blood pressure [173] and endothelium‐dependent relaxation in isolated aortae of SHR through activating the eNOS‐NO‐soluble guanylyl cyclase (sGC)‐cGMP pathway [174, 175]. The attenuation of hypertension and NADPH oxidase activity by nitrite\nitrate treatment has also been demonstrated in two-kidney one-clip (2K1C) HR, DOCA-Salt HR and Ang II-induced HR [176–178]. In addition, a cohort study of European ancestry also showed that genetic predisposition to enhanced NO signaling is associated with decreased blood pressure and reduced risks of coronary artery and peripheral arterial disease [179]. Furthermore, C-ANP4-23 and resveratrol that possess antioxidant property were also shown to attenuate hypertension in SHR through the inhibition of enhanced levels of Giα proteins, \((\text{O}_{2^{-}})\) and ONOO− [148]. In addition, several studies have shown that antihypertensive drugs including ACE inhibitors and Ang II AT1 receptor blocker mediate their effects through the release of NO [33, 34, 38].
Role of eNOS uncoupling in hypertension
eNOS uncoupling occurs when eNOS produces \((\text{O}_{2^{-}})\) instead of NO resulting in the decreased bioavailability of NO and increased oxidative stress causing endothelial dysfunction leading to the pathogenesis and progression of hypertension. The decreased levels of L-arginine\cofactors required to activate eNOS and NO synthesis, increased NO inactivation by \((\text{O}_{2^{-}})\) and increased levels of circulating ADMA, NMMA and arginase contribute to eNOS uncoupling and endothelial dysfunction resulting in the development of hypertension (Fig. 3a) [23, 24, 180–184]. This was supported by the study showing that a defect in l-arginine transport exists in hypertensive and genetically predisposed normotensive subjects [183]. In addition, offsprings of essential hypertensive patients display a reduced vasodilatory response to acetylcholine linked to a defect in the L-arginine-nitric oxide pathway [182]. These studies suggest a role of decreased levels of L-arginine in the pathogenesis of hypertension. This was supported by the study showing that the intravenous administration of L-arginine decreased the mean arterial pressure as well as total peripheral resistance in hypertensive patients [185]. In addition, L-arginine was also reported to reduce blood pressure in animal models of hypertension including salt–sensitive hypertensive rats [186]. Furthermore, perinatal dietary supplementation of L-arginine with antioxidants including vitamin C, vitamin E and taurine was also shown to attenuate the development of hypertension in aging SHR [187]. In addition, the inhibition of arginase that is upregulated in hypertension and decreases the intracellular levels of L-arginine also attenuated blood pressure, vascular function and cardiac fibrosis in SHR and suggests a link between L-arginine and development of hypertension [188].
The cofactor BH4 is an important regulator of eNOS activation and NO generation. Numerous studies have demonstrated that reduced bioavailability of BH4 is associated with endothelial dysfunction contributing to the pathogenesis of vascular disease states including hypertension. Inhibition of BH4 biosynthesis has been shown to impair endothelium-dependent relaxations in canine basilar artery [22]. In addition, BH4 oxidation-induced eNOS uncoupling has also been demonstrated in endothelial cells from DOCA-Salt hypertension [189]. Furthermore, in SHR, the supplementation of BH4 was shown to diminish the eNOS-dependent generation of \((\text{O}_{2^{-}})\) associated with increased production of NO [190]. Coronary endothelial cells from the diabetic BB rats also exhibited BH4 deficiency which was attributed to the decreased expression of GTP cyclohydrolase, the rate-limiting enzyme for de novo synthesis of BH4 [191]. Furthermore, the hypertensive and diabetic patients also displayed the reduced levels of BH4 and eNOS uncoupling [184, 192] and supplementation of BH4 improved endothelial cell function in patients with diabetes, coronary artery disease and hypertension [192–196]. The antioxidant ascorbate was shown to increase NO synthesis in endothelial cells by increasing the levels of BH4 and improving its binding to eNOS [31, 32, 39]. This was further supported by the study showing that both ascorbate and BH4 prevented the ONOO−—induced uncoupling of eNOS in bovine aortic endothelial cells [26].
In addition to L-arginine and cofactor BH4, ADMA an inhibitor of eNOS also plays a role in the regulation of NO synthesis [197]. An upregulation of ADMA was shown to impair the bioavailability of NO leading to eNOS uncoupling and vascular dysfunction [198]. In support of this, several studies showed that increased levels of ADMA were associated with the pathogenesis and progression of vascular diseases including hypertension and diabetes mellitus [199]. However, exogenous supplementation of L-arginine was shown to relieve the inhibitory effect of ADMA on NO synthesis and NO-mediated vascular functions [200]. Thus, strategies to maintain the physiologically relevant levels of these cofactors is essential to prevent eNOS uncoupling associated pathologies.
Nitric oxide and Atherosclerosis
Atherosclerosis is a chronic vascular disease that leads to myocardial infarction and ischemic stroke due to thrombotic occlusion and stenosis of blood vessels. The precise sequence of events responsible for the initiation and progression of atherosclerosis remains currently elusive, however, studies done during the last decade have demonstrated an important role of dyslipidemia and associated changes in the milieu of the vessel wall as crucial mediators of this process [201, 202]. Exaggerated levels of oxidized form of low density lipoproteins (ox-LDL) and endothelial dysfunction, along with the activation of pro-inflammatory pathway are among the key contributors of atherogenesis [201–204]. Enhanced adhesion, migration, accumulation and proliferation of immune and non-immune cells such as monocytes, VSMC, macrophages, foam cells, leucocytes have also been associated with thrombogenesis [205, 206]. A decreased bioavailability of NO has been suggested as a hall mark of endothelial dysfunction associated with atherosclerotic vascular disease [207]. As alluded earlier, eNOS ‘uncoupling’ appears to be one of the prominent mechanisms resulting in reduced NO generation in the vessel wall. Ox-LDL has been shown to suppress NO levels in EC via excessive production of ROS through lectin-like ox-LDL receptor-1(LOX-1) [208]. Suboptimal concentrations of L-arginine or BH4 or higher levels of ADMA may also limit catalytic activity of eNOS to generate sufficient amount of NO in EC. Studies showing that L-arginine supplementation in LDL receptor knockout (KO) mice or hypercholesterolemic rabbit models of atherosclerosis resulted in a reduction in the lesion surface area in aorta, support a role of NO as an antiatherogenic molecule [209, 210]. Additional support for a role of NO in inhibiting the progression of atherosclerotic disease was provided by the observations that treatment of either apolipoprotein E (apo-E) KO mice or cholesterol clamped rabbits with L-NAME accelerated the plaque formation [211, 212].
The molecular mechanisms by which NO exerts its atheroprotective role include its ability to increase vasodilation, inhibit platelet aggregation and monocyte adhesion to endothelium [213, 214]. NO also suppresses the expression of key mediators of cell adhesion including intercellular adhesion molecule-1 (ICAM-1) and vascular cell adhesion molecule-1 (VCAM-1) and monocyte chemoattractant-1(MCP-1), [215, 216] as well as reduces the hypertrophic, proliferative and migratory responses in VSMC [46, 107–112, 116]. Thus, modulation of these key cellular pathways by NO appear to be responsible for the atheroprotective properties of NO. Consistent with this notion, lipid lowering HMG CoA reductase inhibitors of the statin family in addition to lowering plasma LDL levels and atherosclerotic plaque stability also increased eNOS expression and improved endothelial functions [217].
Conclusions
Nitric oxide (NO) is an important vasoprotective molecule that serves as a vasodilator and is a key regulator of endothelial functions. A dysfunctional NO generating system causes oxidative and nitrosative stress due to eNOS uncoupling resulting in impaired endothelial functions as well as remodeling of the vessels. NO donors or gene transfer of NOS exert beneficial effects in improving endothelial functions, lowering hypertension and suppressing vascular remodeling and neointimal hyperplasia in cellular and animal model systems. The potential mechanisms by which NO exerts these beneficial effects include the attenuation of signaling pathways responsible for inducing the hypertrophic, migratory and proliferative cellular responses that are often upregulated in cardiovascular pathologies. Thus, NO remains a promising therapeutic molecule for the treatment of cardiovascular diseases, however, the labile nature of NO and confounding factors of targeted gene delivery, limit its translational use. To overcome these issues, several groups are engaged in developing nanofiber and stent-based delivery systems for NO production and gene delivery for eventual use in cardiovascular therapy.
References
Zordoky BN, Robertson IM, Dyck JR (2015) Preclinical and clinical evidence for the role of resveratrol in the treatment of cardiovascular diseases. Biochim Biophys Acta 1852(6):1155–1177
Pokharel S, Sharma UC, Pinto YM (2003) Left ventricular hypertrophy: virtuous intentions, malign consequences. Int J Biochem Cell Biol 35(6):802–806
Reaven GM, Laws A (1994) Insulin resistance, compensatory hyperinsulinaemia, and coronary heart disease. Diabetologia 37(9):948–952
Forstermann U, Sessa WC (2012) Nitric oxide synthases: regulation and function. Eur Heart J 33(7):829–37, 37a–37d
Knowles RG, Moncada S (1994) Nitric oxide synthases in mammals. Biochem J 298(Pt 2):249–258
Palmer RM, Ashton DS, Moncada S (1988) Vascular endothelial cells synthesize nitric oxide from L-arginine. Nature 333(6174):664–666
Li H, Poulos TL (2005) Structure-function studies on nitric oxide synthases. J Inorg Biochem 99(1):293–305
Ghafourifar P, Richter C (1997) Nitric oxide synthase activity in mitochondria. FEBS Lett 418(3):291–296
Liu VW, Huang PL (2008) Cardiovascular roles of nitric oxide: a review of insights from nitric oxide synthase gene disrupted mice. Cardiovasc Res 77(1):19–29
Merrill JE, Murphy SP, Mitrovic B, Mackenzie-Graham A, Dopp JC, Ding M et al (1997) Inducible nitric oxide synthase and nitric oxide production by oligodendrocytes. J Neurosci Res 48(4):372–384
Moncada S, Bolanos JP (2006) Nitric oxide, cell bioenergetics and neurodegeneration. J Neurochem 97(6):1676–1689
Nathan C (1992) Nitric oxide as a secretory product of mammalian cells. FASEB J 6(12):3051–3064
Dimmeler S, Fleming I, Fisslthaler B, Hermann C, Busse R, Zeiher AM (1999) Activation of nitric oxide synthase in endothelial cells by Akt-dependent phosphorylation. Nature 399(6736):601–605
Busconi L, Michel T (1993) Endothelial nitric oxide synthase. N-terminal myristoylation determines subcellular localization. J Biol Chem 268(12):8410–3
Marletta MA (1994) Nitric oxide synthase: aspects concerning structure and catalysis. Cell 78(6):927–930
Daff S (2010) NO synthase: structures and mechanisms. Nitric Oxide 23(1):1–11
Zhang YH, Casadei B (2012) Sub-cellular targeting of constitutive NOS in health and disease. J Mol Cell Cardiol 52(2):341–350
Ignarro LJ (1990) Nitric oxide. A novel signal transduction mechanism for transcellular communication. Hypertension 16(5):477–83
Cai S, Khoo J, Mussa S, Alp NJ, Channon KM (2005) Endothelial nitric oxide synthase dysfunction in diabetic mice: importance of tetrahydrobiopterin in eNOS dimerisation. Diabetologia 48(9):1933–1940
Vallance P, Leiper J (2004) Cardiovascular biology of the asymmetric dimethylarginine:dimethylarginine dimethylaminohydrolase pathway. Arterioscler Thromb Vasc Biol 24(6):1023–1030
Cosentino F, Katusic ZS (1995) Tetrahydrobiopterin and dysfunction of endothelial nitric oxide synthase in coronary arteries. Circulation 91(1):139–144
Kinoshita H, Milstien S, Wambi C, Katusic ZS (1997) Inhibition of tetrahydrobiopterin biosynthesis impairs endothelium-dependent relaxations in canine basilar artery. Am J Physiol 273(2 Pt 2):H718–H724
Rodriguez S, Richert L, Berthelot A (2000) Increased arginase activity in aorta of mineralocorticoid-salt hypertensive rats. Clin Exp Hypertens 22(1):75–85
Zhang C, Hein TW, Wang W, Miller MW, Fossum TW, McDonald MM et al (2004) Upregulation of vascular arginase in hypertension decreases nitric oxide-mediated dilation of coronary arterioles. Hypertension 44(6):935–943
Stroes E, Hijmering M, van Zandvoort M, Wever R, Rabelink TJ, van Faassen EE (1998) Origin of superoxide production by endothelial nitric oxide synthase. FEBS Lett 438(3):161–164
Kuzkaya N, Weissmann N, Harrison DG, Dikalov S (2003) Interactions of peroxynitrite, tetrahydrobiopterin, ascorbic acid, and thiols: implications for uncoupling endothelial nitric-oxide synthase. J Biol Chem 278(25):22546–22554
Pacher P, Beckman JS, Liaudet L (2007) Nitric oxide and peroxynitrite in health and disease. Physiol Rev 87(1):315–424
Madiraju P, Hossain E, Anand-Srivastava MB (2018) Natriuretic peptide receptor-C activation attenuates angiotensin II-induced enhanced oxidative stress and hyperproliferation of aortic vascular smooth muscle cells. Mol Cell Biochem 448(1–2):77–89
Hossain E, Sarkar O, Li Y, Anand-Srivastava MB (2018) Inhibition of overexpression of Gialpha proteins and nitroxidative stress contribute to sodium nitroprusside-induced attenuation of high blood pressure in SHR. Physiol Rep 6(6):e13658
Balakumar P, Kathuria S, Taneja G, Kalra S, Mahadevan N (2012) Is targeting eNOS a key mechanistic insight of cardiovascular defensive potentials of statins? J Mol Cell Cardiol 52(1):83–92
Heller R, Munscher-Paulig F, Grabner R, Till U (1999) L-Ascorbic acid potentiates nitric oxide synthesis in endothelial cells. J Biol Chem 274(12):8254–8260
Heller R, Unbehaun A, Schellenberg B, Mayer B, Werner-Felmayer G, Werner ER (2001) L-ascorbic acid potentiates endothelial nitric oxide synthesis via a chemical stabilization of tetrahydrobiopterin. J Biol Chem 276(1):40–47
Ignjatovic T, Stanisavljevic S, Brovkovych V, Skidgel RA, Erdos EG (2004) Kinin B1 receptors stimulate nitric oxide production in endothelial cells: signaling pathways activated by angiotensin I-converting enzyme inhibitors and peptide ligands. Mol Pharmacol 66(5):1310–1316
Mason RP, Jacob RF, Kubant R, Jacoby A, Louka F, Corbalan JJ et al (2012) Effects of angiotensin receptor blockers on endothelial nitric oxide release: the role of eNOS variants. Br J Clin Pharmacol 74(1):141–146
Nour-Eldine W, Ghantous CM, Zibara K, Dib L, Issaa H, Itani HA et al (2016) Adiponectin attenuates angiotensin II-induced vascular smooth muscle cell remodeling through nitric oxide and the RhoA/ROCK pathway. Front Pharmacol 7:86
Wallerath T, Deckert G, Ternes T, Anderson H, Li H, Witte K et al (2002) Resveratrol, a polyphenolic phytoalexin present in red wine, enhances expression and activity of endothelial nitric oxide synthase. Circulation 106(13):1652–1658
Wallerath T, Poleo D, Li H, Forstermann U (2003) Red wine increases the expression of human endothelial nitric oxide synthase: a mechanism that may contribute to its beneficial cardiovascular effects. J Am Coll Cardiol 41(3):471–478
Wiemer G, Linz W, Hatrik S, Scholkens BA, Malinski T (1997) Angiotensin-converting enzyme inhibition alters nitric oxide and superoxide release in normotensive and hypertensive rats. Hypertension 30(5):1183–1190
Huang A, Vita JA, Venema RC, Keaney JF Jr (2000) Ascorbic acid enhances endothelial nitric-oxide synthase activity by increasing intracellular tetrahydrobiopterin. J Biol Chem 275(23):17399–17406
Griendling KK, Alexander RW (1997) Oxidative stress and cardiovascular disease. Circulation 96(10):3264–3265
Baradaran A, Nasri H, Rafieian-Kopaei M (2014) Oxidative stress and hypertension: possibility of hypertension therapy with antioxidants. J Res Med Sci 19(4):358–367
Senoner T, Dichtl W (2019) Oxidative stress in cardiovascular diseases: still a therapeutic target? Nutrients 11(9)
Tsutsui H, Kinugawa S, Matsushima S (2011) Oxidative stress and heart failure. Am J Physiol Heart Circ Physiol 301(6):H2181–H2190
Montezano AC, Touyz RM (2012) Reactive oxygen species and endothelial function–role of nitric oxide synthase uncoupling and Nox family nicotinamide adenine dinucleotide phosphate oxidases. Basic Clin Pharmacol Toxicol 110(1):87–94
Bahnson ES, Koo N, Cantu-Medellin N, Tsui AY, Havelka GE, Vercammen JM et al (2015) Nitric oxide inhibits neointimal hyperplasia following vascular injury via differential, cell-specific modulation of SOD-1 in the arterial wall. Nitric Oxide 44:8–17
Sarkar O, Li Y, Anand-Srivastava MB (2017) Nitric oxide attenuates overexpression of Gialpha proteins in vascular smooth muscle cells from SHR: role of ROS and ROS-mediated signaling. PLoS ONE 12(7):e0179301
Chen Q, Wang Q, Zhu J, Xiao Q, Zhang L (2018) Reactive oxygen species: key regulators in vascular health and diseases. Br J Pharmacol 175(8):1279–1292
Atef ME, Anand-Srivastava MB (2016) Oxidative stress contributes to the enhanced expression of Gqalpha/PLCbeta1 proteins and hypertrophy of VSMC from SHR: role of growth factor receptor transactivation. Am J Physiol Heart Circ Physiol 310(5):H608–H618
Gomez Sandoval YH, Anand-Srivastava MB (2011) Enhanced levels of endogenous endothelin-1 contribute to the over expression of Gialpha protein in vascular smooth muscle cells from SHR: role of growth factor receptor activation. Cell Signal 23(2):354–362
Lappas G, Daou GB, Anand-Srivastava MB (2005) Oxidative stress contributes to the enhanced expression of Gialpha proteins and adenylyl cyclase signaling in vascular smooth muscle cells from spontaneously hypertensive rats. J Hypertens 23(12):2251–2261
Hobbs AJ (1997) Soluble guanylate cyclase: the forgotten sibling. Trends Pharmacol Sci 18(12):484–491
Ignarro LJ, Degnan JN, Baricos WH, Kadowitz PJ, Wolin MS (1982) Activation of purified guanylate cyclase by nitric oxide requires heme. Comparison of heme-deficient, heme-reconstituted and heme-containing forms of soluble enzyme from bovine lung. Biochim Biophys Acta 718(1):49–59.
Krumenacker JS, Hanafy KA, Murad F (2004) Regulation of nitric oxide and soluble guanylyl cyclase. Brain Res Bull 62(6):505–515
Feil R, Lohmann SM, de Jonge H, Walter U, Hofmann F (2003) Cyclic GMP-dependent protein kinases and the cardiovascular system: insights from genetically modified mice. Circ Res 93(10):907–916
Pfeifer A, Ruth P, Dostmann W, Sausbier M, Klatt P, Hofmann F (1999) Structure and function of cGMP-dependent protein kinases. Rev Physiol Biochem Pharmacol 135:105–149
Burley DS, Ferdinandy P, Baxter GF (2007) Cyclic GMP and protein kinase-G in myocardial ischaemia-reperfusion: opportunities and obstacles for survival signaling. Br J Pharmacol 152(6):855–869
Lincoln TM, Wu X, Sellak H, Dey N, Choi CS (2006) Regulation of vascular smooth muscle cell phenotype by cyclic GMP and cyclic GMP-dependent protein kinase. Front Biosci 11:356–367
Wang S, Li Y (2009) Expression of constitutively active cGMP-dependent protein kinase inhibits glucose-induced vascular smooth muscle cell proliferation. Am J Physiol Heart Circ Physiol 297(6):H2075–H2083
Fukao M, Mason HS, Britton FC, Kenyon JL, Horowitz B, Keef KD (1999) Cyclic GMP-dependent protein kinase activates cloned BKCa channels expressed in mammalian cells by direct phosphorylation at serine 1072. J Biol Chem 274(16):10927–10935
Jahn H, Nastainczyk W, Rohrkasten A, Schneider T, Hofmann F (1988) Site-specific phosphorylation of the purified receptor for calcium-channel blockers by cAMP- and cGMP-dependent protein kinases, protein kinase C, calmodulin-dependent protein kinase II and casein kinase II. Eur J Biochem 178(2):535–542
Layland J, Li JM, Shah AM (2002) Role of cyclic GMP-dependent protein kinase in the contractile response to exogenous nitric oxide in rat cardiac myocytes. J Physiol 540(Pt 2):457–467
Lucas KA, Pitari GM, Kazerounian S, Ruiz-Stewart I, Park J, Schulz S et al (2000) Guanylyl cyclases and signaling by cyclic GMP. Pharmacol Rev 52(3):375–414
Suhasini M, Li H, Lohmann SM, Boss GR, Pilz RB (1998) Cyclic-GMP-dependent protein kinase inhibits the Ras/Mitogen-activated protein kinase pathway. Mol Cell Biol 18(12):6983–6994
Bassil M, Anand-Srivastava MB (2006) Nitric oxide modulates Gi-protein expression and adenylyl cyclase signaling in vascular smooth muscle cells. Free Radic Biol Med 41(7):1162–1173
Kibbe MR, Nie S, Seol DW, Kovesdi I, Lizonova A, Makaroun M et al (2000) Nitric oxide prevents p21 degradation with the ubiquitin-proteasome pathway in vascular smooth muscle cells. J Vasc Surg 31(2):364–374
Stotz WH, Li D, Johns RA (2004) Exogenous nitric oxide upregulates p21(waf1/cip1) in pulmonary microvascular smooth muscle cells. J Vasc Res 41(3):211–219
Arejian M, Li Y, Anand-Srivastava MB (2009) Nitric oxide attenuates the expression of natriuretic peptide receptor C and associated adenylyl cyclase signaling in aortic vascular smooth muscle cells: role of MAPK. Am J Physiol Heart Circ Physiol 296(6):H1859–H1867
Bian K, Ke Y, Kamisaki Y, Murad F (2006) Proteomic modification by nitric oxide. J Pharmacol Sci 101(4):271–279
Cornwell TL, Arnold E, Boerth NJ, Lincoln TM (1994) Inhibition of smooth muscle cell growth by nitric oxide and activation of cAMP-dependent protein kinase by cGMP. Am J Physiol 267(5 Pt 1):C1405–C1413
Lima B, Forrester MT, Hess DT, Stamler JS (2010) S-nitrosylation in cardiovascular signaling. Circ Res 106(4):633–646
Schulman IH, Hare JM (2012) Regulation of cardiovascular cellular processes by S-nitrosylation. Biochim Biophys Acta 1820(6):752–762
Chen CA, Wang TY, Varadharaj S, Reyes LA, Hemann C, Talukder MA et al (2010) S-glutathionylation uncouples eNOS and regulates its cellular and vascular function. Nature 468(7327):1115–1118
Jia M, Mateoiu C, Souchelnytskyi S (2011) Protein tyrosine nitration in the cell cycle. Biochem Biophys Res Commun 413(2):270–276
Batista WL, Ogata FT, Curcio MF, Miguel RB, Arai RJ, Matsuo AL et al (2013) S-nitrosoglutathione and endothelial nitric oxide synthase-derived nitric oxide regulate compartmentalized ras S-nitrosylation and stimulate cell proliferation. Antioxid Redox Signal 18(3):221–238
Gow AJ, Duran D, Malcolm S, Ischiropoulos H (1996) Effects of peroxynitrite-induced protein modifications on tyrosine phosphorylation and degradation. FEBS Lett 385(1–2):63–66
Hellberg CB, Boggs SE, Lapetina EG (1998) Phosphatidylinositol 3-kinase is a target for protein tyrosine nitration. Biochem Biophys Res Commun 252(2):313–317
Sun J, Steenbergen C, Murphy E (2006) S-nitrosylation: NO-related redox signaling to protect against oxidative stress. Antioxid Redox Signal 8(9–10):1693–1705
Bolotina VM, Najibi S, Palacino JJ, Pagano PJ, Cohen RA (1994) Nitric oxide directly activates calcium-dependent potassium channels in vascular smooth muscle. Nature 368(6474):850–853
Hadrava V, Kruppa U, Russo RC, Lacourciere Y, Tremblay J, Hamet P (1991) Vascular smooth muscle cell proliferation and its therapeutic modulation in hypertension. Am Heart J 122(4 Pt 2):1198–1203
Intengan HD, Schiffrin EL (2001) Vascular remodeling in hypertension: roles of apoptosis, inflammation, and fibrosis. Hypertension 38(3 Pt 2):581–587
Touyz RM (2005) Intracellular mechanisms involved in vascular remodelling of resistance arteries in hypertension: role of angiotensin II. Exp Physiol 90(4):449–455
Intengan HD, Deng LY, Li JS, Schiffrin EL (1999) Mechanics and composition of human subcutaneous resistance arteries in essential hypertension. Hypertension 33(1 Pt 2):569–574
Ross R, Glomset J, Kariya B, Harker L (1974) A platelet-dependent serum factor that stimulates the proliferation of arterial smooth muscle cells in vitro 71(4):1207–1210
Raines EWJ (2004) PDGF and cardiovascular disease 15(4):237–254
Inagami T, Eguchi S (2000) Angiotensin II-mediated vascular smooth muscle cell growth signaling 33(6):619–624
Li Y, Lévesque L-O, Anand-Srivastava MB (2010) Epidermal growth factor receptor transactivation by endogenous vasoactive peptides contributes to hyper proliferation of vascular smooth muscle cells of SHR. Am J Physiol 299(6):H1959–H1967
Atef ME, Anand-Srivastava MB (2016) Oxidative stress contributes to the enhanced expression of Gqα/PLCβ1 proteins and hypertrophy of VSMC from SHR: role of growth factor receptor transactivation. Am J Physiol Heart Circ Physiol 310(5):H608–H618
Gomez Y-H, Anand-Srivastava M (2010) Enhanced levels of endogenous endothelin-1 contribute to the over expression of Giα protein in vascular smooth muscle cells from SHR: role of growth factor receptor activation. Cell Signal 23:354–362
Almajdoob S, Hossain E, Anand-Srivastava MBJVp (2018) Resveratrol attenuates hyper proliferation of vascular smooth muscle cells from spontaneously hypertensive rats: role of ROS and ROS-mediated cell signaling 101:48–56
Hashim S, Li Y, Anand-Srivastava MB (2006) Small cytoplasmic domain peptides of natriuretic peptide receptor-C attenuate cell proliferation through Gialpha protein/MAP kinase/PI3-kinase/AKT pathways. Am J Physiol Heart Circ Physiol 291(6):H3144–H3153
Gomez Sandoval YH, Levesque LO, Anand-Srivastava MB (2009) Contribution of epidermal growth factor receptor transactivation in angiotensin II-induced enhanced expression of Gi protein and proliferation in A10 vascular smooth muscle cells. Can J Physiol Pharmacol 87(12):1037–1045
Gomez Sandoval YH, Levesque LO, Li Y, Anand-Srivastava MB (2013) Role of epidermal growth factor receptor transactivation in endothelin-1-induced enhanced expression of Gi protein and proliferation in A10 vascular smooth muscle cells. Can J Physiol Pharmacol 91(3):221–227
Eguchi S, Numaguchi K, Iwasaki H, Matsumoto T, Yamakawa T, Utsunomiya H et al (1998) Calcium-dependent epidermal growth factor receptor transactivation mediates the angiotensin II-induced mitogen-activated protein kinase activation in vascular smooth muscle cells. J Biol Chem 273(15):8890–8896
Ohtsu H, Mifune M, Frank GD, Saito S, Inagami T, Kim-Mitsuyama S et al (2005) Signal-crosstalk between Rho/ROCK and c-Jun NH2-terminal kinase mediates migration of vascular smooth muscle cells stimulated by angiotensin II. Arterioscler Thromb Vasc Biol 25(9):1831–1836
Atef ME, Anand-Srivastava MB (2014) Enhanced expression of Gqalpha and PLC-beta1 proteins contributes to vascular smooth muscle cell hypertrophy in SHR: role of endogenous angiotensin II and endothelin-1. Am J Physiol Cell Physiol 307(1):C97-106
Hahn AW, Resink TJ, Scott-Burden T, Powell J, Dohi Y, Buhler FR (1990) Stimulation of endothelin mRNA and secretion in rat vascular smooth muscle cells: a novel autocrine function. Cell Regul 1(9):649–659
Kanse SM, Takahashi K, Warren JB, Perera T, Porta M, Ghatei M et al (1991) Production of endothelin by vascular smooth muscle cells. J Cardiovasc Pharmacol 17(Suppl 7):S113–S116
Kubo A, Fukuda N, Soma M, Izumi Y, Kanmatsuse K (1996) Inhibitory effect of an angiotensin II type 1 receptor antagonist on growth of vascular smooth muscle cells from spontaneously hypertensive rats. J Cardiovasc Pharmacol 27(1):58–63
Lu MH, Chao CF, Tsai SH, Chen JY, Chang LT (2006) Autocrine effects of endothelin on in vitro proliferation of vascular smooth muscle cells from spontaneously hypertensive and normotensive rats. Clin Exp Hypertens 28(5):463–474
Hadrava V, Tremblay J, Hamet P (1989) Abnormalities in growth characteristics of aortic smooth muscle cells in spontaneously hypertensive rats. Hypertension 13(6 Pt 1):589–597
Tanner FC, Greutert H, Barandier C, Frischknecht K, Luscher TF (2003) Different cell cycle regulation of vascular smooth muscle in genetic hypertension. Hypertension 42(2):184–188
Bou Daou G, Li Y, Anand-Srivastava MB (2016) Enhanced expression of Gialpha proteins contributes to the hyperproliferation of vascular smooth muscle cells from spontaneously hypertensive rats via MAP kinase- and PI3 kinase-independent pathways. Can J Physiol Pharmacol 94(1):49–58
El Andalousi J, Li Y, Anand-Srivastava MB (2013) Natriuretic peptide receptor-C agonist attenuates the expression of cell cycle proteins and proliferation of vascular smooth muscle cells from spontaneously hypertensive rats: role of Gi proteins and MAPkinase/PI3kinase signaling. PLoS ONE 8(10):e76183
Li Y, Levesque LO, Anand-Srivastava MB (2010) Epidermal growth factor receptor transactivation by endogenous vasoactive peptides contributes to hyperproliferation of vascular smooth muscle cells of SHR. Am J Physiol Heart Circ Physiol 299(6):H1959–H1967
Rahali S, Li Y, Anand-Srivastava MB (2018) Contribution of oxidative stress and growth factor receptor transactivation in natriuretic peptide receptor C-mediated attenuation of hyperproliferation of vascular smooth muscle cells from SHR. PLoS ONE 13(1):e0191743
Saito S, Frank GD, Mifune M, Ohba M, Utsunomiya H, Motley ED et al (2002) Ligand-independent trans-activation of the platelet-derived growth factor receptor by reactive oxygen species requires protein kinase C-delta and c-Src. J Biol Chem 277(47):44695–44700
Dubey RK (1994) Vasodilator-derived nitric oxide inhibits fetal calf serum- and angiotensin-II-induced growth of renal arteriolar smooth muscle cells. J Pharmacol Exp Ther 269(1):402–408
Dubey RK, Jackson EK, Luscher TF (1995) Nitric oxide inhibits angiotensin II-induced migration of rat aortic smooth muscle cell. Role of cyclic-nucleotides and angiotensin1 receptors. J Clin Invest 96(1):141–9
Garg UC, Hassid A (1989) Nitric oxide-generating vasodilators and 8-bromo-cyclic guanosine monophosphate inhibit mitogenesis and proliferation of cultured rat vascular smooth muscle cells. J Clin Invest 83(5):1774–1777
Tsihlis ND, Oustwani CS, Vavra AK, Jiang Q, Keefer LK, Kibbe MR (2011) Nitric oxide inhibits vascular smooth muscle cell proliferation and neointimal hyperplasia by increasing the ubiquitination and degradation of UbcH10. Cell Biochem Biophys 60(1–2):89–97
Bahnson ES, Kassam HA, Moyer TJ, Jiang W, Morgan CE, Vercammen JM et al (2016) Targeted nitric oxide delivery by supramolecular nanofibers for the prevention of restenosis after arterial injury. Antioxid Redox Signal 24(8):401–418
Suzuki H, Kimura K, Shirai H, Eguchi K, Higuchi S, Hinoki A et al (2009) Endothelial nitric oxide synthase inhibits G12/13 and rho-kinase activated by the angiotensin II type-1 receptor: implication in vascular migration. Arterioscler Thromb Vasc Biol 29(2):217–224
Sharma RV, Tan E, Fang S, Gurjar MV, Bhalla RC (1999) NOS gene transfer inhibits expression of cell cycle regulatory molecules in vascular smooth muscle cells. Am J Physiol 276(5):H1450–H1459
Tanner FC, Meier P, Greutert H, Champion C, Nabel EG, Luscher TF (2000) Nitric oxide modulates expression of cell cycle regulatory proteins: a cytostatic strategy for inhibition of human vascular smooth muscle cell proliferation. Circulation 101(16):1982–1989
Ishida A, Sasaguri T, Kosaka C, Nojima H, Ogata J (1997) Induction of the cyclin-dependent kinase inhibitor p21(Sdi1/Cip1/Waf1) by nitric oxide-generating vasodilator in vascular smooth muscle cells. J Biol Chem 272(15):10050–10057
Hossain E, Sarkar O, Li Y, Anand-Srivastava MB (2020) Sodium nitroprusside attenuates hyperproliferation of vascular smooth muscle cells from spontaneously hypertensive rats through the inhibition of overexpression of AT1 receptor, cell cycle proteins, and c-Src/growth factor receptor signaling pathways. Can J Physiol Pharmacol 98(1):35–43
Yu SM, Hung LM, Lin CC (1997) cGMP-elevating agents suppress proliferation of vascular smooth muscle cells by inhibiting the activation of epidermal growth factor signaling pathway. Circulation 95(5):1269–1277
Bouallegue A, Daou GB, Srivastava AK (2007) Nitric oxide attenuates endothelin-1-induced activation of ERK1/2, PKB, and Pyk2 in vascular smooth muscle cells by a cGMP-dependent pathway. Am J Physiol Heart Circ Physiol 293(4):H2072–H2079
Lehners M, Dobrowinski H, Feil S, Feil R. cGMP Signaling and Vascular Smooth Muscle Cell Plasticity. J Cardiovasc Dev Dis. 2018;5(2).
Segura-Puimedon M, Mergia E, Al-Hasani J, Aherrahrou R, Stoelting S, Kremer F et al (2016) Proatherosclerotic effect of the alpha1-subunit of soluble guanylyl cyclase by promoting smooth muscle phenotypic switching. Am J Pathol 186(8):2220–2231
Maruhashi T, Noma K, Iwamoto Y, Iwamoto A, Oda N, Kajikawa M et al (2014) Critical role of exogenous nitric oxide in ROCK activity in vascular smooth muscle cells. PLoS ONE 9(10):e109017
Sarkar R, Meinberg EG, Stanley JC, Gordon D, Webb RC (1996) Nitric oxide reversibly inhibits the migration of cultured vascular smooth muscle cells. Circ Res 78(2):225–230
Gurjar MV, Sharma RV, Bhalla RC (1999) eNOS gene transfer inhibits smooth muscle cell migration and MMP-2 and MMP-9 activity. Arterioscler Thromb Vasc Biol 19(12):2871–2877
Largiader T, Eto M, Payeli SK, Greutert H, Viswambharan H, Lachat M et al (2008) Endothelial nitric oxide synthase gene transfer inhibits human smooth muscle cell migration via inhibition of Rho A. J Cardiovasc Pharmacol 52(4):369–374
McNamara DB, Bedi B, Aurora H, Tena L, Ignarro LJ, Kadowitz PJ et al (1993) L-arginine inhibits balloon catheter-induced intimal hyperplasia. Biochem Biophys Res Commun 193(1):291–296
Taguchi J, Abe J, Okazaki H, Takuwa Y, Kurokawa K (1993) L-arginine inhibits neointimal formation following balloon injury. Life Sci 53(23):PL387–PL392
Guo JP, Panday MM, Consigny PM, Lefer AM (1995) Mechanisms of vascular preservation by a novel NO donor following rat carotid artery intimal injury. Am J Physiol 269(3 Pt 2):H1122–H1131
Kaul S, Cercek B, Rengstrom J, Xu XP, Molloy MD, Dimayuga P et al (2000) Polymeric-based perivascular delivery of a nitric oxide donor inhibits intimal thickening after balloon denudation arterial injury: role of nuclear factor-kappaB. J Am Coll Cardiol 35(2):493–501
Lee JS, Adrie C, Jacob HJ, Roberts JD Jr, Zapol WM, Bloch KD (1996) Chronic inhalation of nitric oxide inhibits neointimal formation after balloon-induced arterial injury. Circ Res 78(2):337–342
Schwarzacher SP, Lim TT, Wang B, Kernoff RS, Niebauer J, Cooke JP et al (1997) Local intramural delivery of L-arginine enhances nitric oxide generation and inhibits lesion formation after balloon angioplasty. Circulation 95(7):1863–1869
Fulton GJ, Davies MG, Barber L, Gray JL, Svendsen E, Hagen PO (1998) Local effects of nitric oxide supplementation and suppression in the development of intimal hyperplasia in experimental vein grafts. Eur J Vasc Endovasc Surg 15(4):279–289
Havelka GE, Moreira ES, Rodriguez MP, Tsihlis ND, Wang Z, Martinez J et al (2013) Nitric oxide delivery via a permeable balloon catheter inhibits neointimal growth after arterial injury. J Surg Res 180(1):35–42
Pearce CG, Najjar SF, Kapadia MR, Murar J, Eng J, Lyle B et al (2008) Beneficial effect of a short-acting NO donor for the prevention of neointimal hyperplasia. Free Radic Biol Med 44(1):73–81
Groves PH, Banning AP, Penny WJ, Newby AC, Cheadle HA, Lewis MJ (1995) The effects of exogenous nitric oxide on smooth muscle cell proliferation following porcine carotid angioplasty. Cardiovasc Res 30(1):87–96
Harnek J, Zoucas E, Sjuve R, Arner A, Ekblad E, Schou H et al (2003) Local infusion of the nitric oxide donor Sin-1 after angioplasty. Effects on intimal hyperplasia in porcine coronary arteries. Acta Radiol 44(4):395–402
Janssens S, Flaherty D, Nong Z, Varenne O, van Pelt N, Haustermans C et al (1998) Human endothelial nitric oxide synthase gene transfer inhibits vascular smooth muscle cell proliferation and neointima formation after balloon injury in rats. Circulation 97(13):1274–1281
Kibbe MR, Tzeng E, Gleixner SL, Watkins SC, Kovesdi I, Lizonova A et al (2001) Adenovirus-mediated gene transfer of human inducible nitric oxide synthase in porcine vein grafts inhibits intimal hyperplasia. J Vasc Surg 34(1):156–165
Shears LL 2nd, Kibbe MR, Murdock AD, Billiar TR, Lizonova A, Kovesdi I et al (1998) Efficient inhibition of intimal hyperplasia by adenovirus-mediated inducible nitric oxide synthase gene transfer to rats and pigs in vivo. J Am Coll Surg 187(3):295–306
Varenne O, Pislaru S, Gillijns H, Van Pelt N, Gerard RD, Zoldhelyi P et al (1998) Local adenovirus-mediated transfer of human endothelial nitric oxide synthase reduces luminal narrowing after coronary angioplasty in pigs. Circulation 98(9):919–926
von der Leyen HE, Gibbons GH, Morishita R, Lewis NP, Zhang L, Nakajima M et al (1995) Gene therapy inhibiting neointimal vascular lesion: in vivo transfer of endothelial cell nitric oxide synthase gene. Proc Natl Acad Sci USA 92(4):1137–1141
von der Thusen JH, Fekkes ML, Passier R, van Zonneveld AJ, Mainfroid V, van Berkel TJ et al (2004) Adenoviral transfer of endothelial nitric oxide synthase attenuates lesion formation in a novel murine model of postangioplasty restenosis. Arterioscler Thromb Vasc Biol 24(2):357–362
Lei J, Vodovotz Y, Tzeng E, Billiar TR (2013) Nitric oxide, a protective molecule in the cardiovascular system. Nitric Oxide 35:175–185
Fishbein I, Guerrero DT, Alferiev IS, Foster JB, Minutolo NG, Chorny M et al (2017) Stent-based delivery of adeno-associated viral vectors with sustained vascular transduction and iNOS-mediated inhibition of in-stent restenosis. Gene Ther 24(11):717–726
Rao J, Pan Bei H, Yang Y, Liu Y, Lin H, Zhao X (2020) Nitric oxide-producing cardiovascular stent coatings for prevention of thrombosis and restenosis. Front Bioeng Biotechnol. 8:578
Ali El-Basyuni Y, Li Y, Anand-Srivastava MB (2016) Knockdown of Inhibitory guanine nucleotide binding protein gialpha-2 by antisense oligodeoxynucleotides attenuates the development of hypertension and tachycardia in spontaneously hypertensive rats. J Am Heart Assoc 5(11)
Li Y, Anand-Srivastava MB (2002) Inactivation of enhanced expression of G(i) proteins by pertussis toxin attenuates the development of high blood pressure in spontaneously hypertensive rats. Circ Res 91(3):247–254
Sandoval YH, Li Y, Anand-Srivastava MB (2011) Transactivation of epidermal growth factor receptor by enhanced levels of endogenous angiotensin II contributes to the overexpression of Gialpha proteins in vascular smooth muscle cells from SHR. Cell Signal 23(11):1716–1726
Li Y, Sarkar O, Brochu M, Anand-Srivastava MB (2014) Natriuretic peptide receptor-C attenuates hypertension in spontaneously hypertensive rats: role of nitroxidative stress and Gi proteins. Hypertension 63(4):846–855
Sarkar O, Li Y, Anand-Srivastava MB (2019) Resveratrol prevents the development of high blood pressure in spontaneously hypertensive rats through the inhibition of enhanced expression of Giα proteins. Canadian J Physiol Pharmacol 97(9):872–879. https://doi.org/10.1139/cjpp-2019-0040/
Hermann M, Flammer A, Lüscher TFJTJoCH (2006) Nitric oxide in hypertension 8:17–29
Demougeot C, Prigent-Tessier A, Marie C, Berthelot AJJoh (2005) Arginase inhibition reduces endothelial dysfunction and blood pressure rising in spontaneously hypertensive rats. 23(5):971–978
Archer SL, Huang JM, Hampl V, Nelson DP, Shultz PJ, Weir EK (1994) Nitric oxide and cGMP cause vasorelaxation by activation of a charybdotoxin-sensitive K channel by cGMP-dependent protein kinase. Proc Natl Acad Sci USA 91(16):7583–7587
Tanaka Y, Tang G, Takizawa K, Otsuka K, Eghbali M, Song M et al (2006) KV channels contribute to nitric oxide-and atrial natriuretic peptide-induced relaxation of a rat conduit artery 317(1):341–354
Lüscher TF, Spieker LE, Noll G, Cosentino FJJocp (2001) Vascular effects of newer cardiovascular drugs: focus on nebivolol and ACE-inhibitors 38:S3–S12
Sandoo A, van Zanten JJCSV, Metsios GS, Carroll D, Kitas GD (2010) The endothelium and its role in regulating vascular tone. Open Cardiovasc Med J 4:302–312
Brunner H, Cockcroft JR, Deanfield J, Donald A, Ferrannini E, Halcox J et al (2005) Endothelial function and dysfunction. Part II: association with cardiovascular risk factors and diseases. A statement by the Working Group on Endothelins and Endothelial Factors of the European Society of Hypertension 23(2):233–246
Lüscher T, Vanhoutte PMJH (1986) Endothelium-dependent contractions to acetylcholine in the aorta of the spontaneously hypertensive rat 8(4):344–348
Panza JA, Quyyumi AA, Brush JE Jr (1990) Epstein SEJNEJoM. Abnormal endothelium-dependent vascular relaxation in patients with essential hypertension 323(1):22–27
Nelson RJ, Demas GE, Huang PL, Fishman MC, Dawson VL, Dawson TM et al (1995) Behavioural abnormalities in male mice lacking neuronal nitric oxide synthase. Nature 378(6555):383–386
Sun Y, Carretero OA, Xu J, Rhaleb NE, Yang JJ, Pagano PJ et al (2009) Deletion of inducible nitric oxide synthase provides cardioprotection in mice with 2-kidney, 1-clip hypertension. Hypertension 53(1):49–56
Friebe A, Koesling D (2009) The function of NO-sensitive guanylyl cyclase: what we can learn from genetic mouse models. Nitric Oxide 21(3–4):149–156
Friebe A, Mergia E, Dangel O, Lange A, Koesling D (2007) Fatal gastrointestinal obstruction and hypertension in mice lacking nitric oxide-sensitive guanylyl cyclase. Proc Natl Acad Sci USA 104(18):7699–7704
Pfeifer A, Klatt P, Massberg S, Ny L, Sausbier M, Hirneiss C et al (1998) Defective smooth muscle regulation in cGMP kinase I-deficient mice. EMBO J 17(11):3045–3051
Koeppen M, Feil R, Siegl D, Feil S, Hofmann F, Pohl U et al (2004) cGMP-dependent protein kinase mediates NO- but not acetylcholine-induced dilations in resistance vessels in vivo. Hypertension 44(6):952–955
Di Fusco F, Anand-Srivastava MB (1997) Nitric oxide synthase inhibition by N(omega)-nitro-L-arginine methyl ester modulates G-protein expression and adenylyl cyclase activity in rat heart. Am J Hypertens 10(4 Pt 1):471–475
Arnal JF, el Amrani AI, Chatellier G, Menard J, Michel JB (1993) Cardiac weight in hypertension induced by nitric oxide synthase blockade. Hypertension 22(3):380–387
Gadkari TV, Cortes N, Madrasi K, Tsoukias NM, Joshi MS (2013) Agmatine induced NO dependent rat mesenteric artery relaxation and its impairment in salt-sensitive hypertension. Nitric Oxide 35:65–71
Sasser JM, Sullivan JC, Elmarakby AA, Kemp BE, Pollock DM, Pollock JS (2004) Reduced NOS3 phosphorylation mediates reduced NO/cGMP signaling in mesenteric arteries of deoxycorticosterone acetate-salt hypertensive rats. Hypertension 43(5):1080–1085
Kimura K, Nishio I (1999) Impaired endothelium-dependent relaxation in mesenteric arteries of reduced renal mass hypertensive rats. Scand J Clin Lab Invest 59(3):199–204
Stankevicius E, Martinez AC, Mulvany MJ, Simonsen U (2002) Blunted acetylcholine relaxation and nitric oxide release in arteries from renal hypertensive rats. J Hypertens 20(8):1571–1579
Li Q, Youn JY, Cai H (2015) Mechanisms and consequences of endothelial nitric oxide synthase dysfunction in hypertension. J Hypertens 33(6):1128–1136
Cosby K, Partovi KS, Crawford JH, Patel RP, Reiter CD, Martyr S et al (2003) Nitrite reduction to nitric oxide by deoxyhemoglobin vasodilates the human circulation. Nat Med 9(12):1498–1505
Classen HG, Stein-Hammer C, Thoni H (1990) Hypothesis: the effect of oral nitrite on blood pressure in the spontaneously hypertensive rat. Does dietary nitrate mitigate hypertension after conversion to nitrite? J Am Coll Nutr 9(5):500–502
Ling WC, Lau YS, Murugan DD, Vanhoutte PM, Mustafa MR (2015) Sodium nitrite causes relaxation of the isolated rat aorta: by stimulating both endothelial NO synthase and activating soluble guanylyl cyclase in vascular smooth muscle. Vascul Pharmacol 74:87–92
Ling WC, Murugan DD, Lau YS, Vanhoutte PM, Mustafa MR (2016) Sodium nitrite exerts an antihypertensive effect and improves endothelial function through activation of eNOS in the SHR. Sci Rep 6:33048
Amaral JH, Ferreira GC, Pinheiro LC, Montenegro MF, Tanus-Santos JE (2015) Consistent antioxidant and antihypertensive effects of oral sodium nitrite in DOCA-salt hypertension. Redox Biol 5:340–346
Guimaraes DD, Cruz JC, Carvalho-Galvao A, Zhuge Z, Marques SM, Naves LM et al (2019) Dietary nitrate reduces blood pressure in rats with angiotensin II-induced hypertension via mechanisms that involve reduction of sympathetic hyperactivity. Hypertension 73(4):839–848
Montenegro MF, Amaral JH, Pinheiro LC, Sakamoto EK, Ferreira GC, Reis RI et al (2011) Sodium nitrite downregulates vascular NADPH oxidase and exerts antihypertensive effects in hypertension. Free Radic Biol Med 51(1):144–152
Emdin CA, Khera AV, Klarin D, Natarajan P, Zekavat SM, Nomura A et al (2018) Phenotypic consequences of a genetic predisposition to enhanced nitric oxide signaling. Circulation 137(3):222–232
Achan V, Broadhead M, Malaki M, Whitley G, Leiper J, MacAllister R et al (2003) Asymmetric dimethylarginine causes hypertension and cardiac dysfunction in humans and is actively metabolized by dimethylarginine dimethylaminohydrolase. Arterioscler Thromb Vasc Biol 23(8):1455–1459
Cai H, Harrison DG (2000) Endothelial dysfunction in cardiovascular diseases: the role of oxidant stress. Circ Res 87(10):840–844
Taddei S, Virdis A, Mattei P, Ghiadoni L, Sudano I, Salvetti A (1996) Defective L-arginine-nitric oxide pathway in offspring of essential hypertensive patients. Circulation 94(6):1298–1303
Schlaich MP, Parnell MM, Ahlers BA, Finch S, Marshall T, Zhang WZ et al (2004) Impaired L-arginine transport and endothelial function in hypertensive and genetically predisposed normotensive subjects. Circulation 110(24):3680–3686
Higashi Y, Sasaki S, Nakagawa K, Fukuda Y, Matsuura H, Oshima T et al (2002) Tetrahydrobiopterin enhances forearm vascular response to acetylcholine in both normotensive and hypertensive individuals. Am J Hypertens 15(4 Pt 1):326–332
Hishikawa K, Nakaki T, Suzuki H, Kato R, Saruta T (1992) L-arginine as an antihypertensive agent. J Cardiovasc Pharmacol 20(Suppl 12):S196–S197
Chen PY, Sanders PW (1991) L-arginine abrogates salt-sensitive hypertension in Dahl/Rapp rats. J Clin Invest 88(5):1559–1567
Racasan S, Braam B, van der Giezen DM, Goldschmeding R, Boer P, Koomans HA et al (2004) Perinatal L-arginine and antioxidant supplements reduce adult blood pressure in spontaneously hypertensive rats. Hypertension 44(1):83–88
Bagnost T, Ma L, da Silva RF, Rezakhaniha R, Houdayer C, Stergiopulos N et al (2010) Cardiovascular effects of arginase inhibition in spontaneously hypertensive rats with fully developed hypertension. Cardiovasc Res 87(3):569–577
Landmesser U, Dikalov S, Price SR, McCann L, Fukai T, Holland SM et al (2003) Oxidation of tetrahydrobiopterin leads to uncoupling of endothelial cell nitric oxide synthase in hypertension. J Clin Invest 111(8):1201–1209
Cosentino F, Patton S, d’Uscio LV, Werner ER, Werner-Felmayer G, Moreau P et al (1998) Tetrahydrobiopterin alters superoxide and nitric oxide release in prehypertensive rats. J Clin Invest 101(7):1530–1537
Meininger CJ, Marinos RS, Hatakeyama K, Martinez-Zaguilan R, Rojas JD, Kelly KA et al (2000) Impaired nitric oxide production in coronary endothelial cells of the spontaneously diabetic BB rat is due to tetrahydrobiopterin deficiency. Biochem J 349(Pt 1):353–356
Heitzer T, Krohn K, Albers S, Meinertz T (2000) Tetrahydrobiopterin improves endothelium-dependent vasodilation by increasing nitric oxide activity in patients with Type II diabetes mellitus. Diabetologia 43(11):1435–1438
Channon KM (2004) Tetrahydrobiopterin: regulator of endothelial nitric oxide synthase in vascular disease. Trends Cardiovasc Med 14(8):323–327
Maier W, Cosentino F, Lutolf RB, Fleisch M, Seiler C, Hess OM et al (2000) Tetrahydrobiopterin improves endothelial function in patients with coronary artery disease. J Cardiovasc Pharmacol 35(2):173–178
Moens AL, Kass DA (2006) Tetrahydrobiopterin and cardiovascular disease. Arterioscler Thromb Vasc Biol 26(11):2439–2444
Katusic ZS (2001) Vascular endothelial dysfunction: does tetrahydrobiopterin play a role? Am J Physiol Heart Circ Physiol 281(3):H981–H986
Vallance P, Leone A, Calver A, Collier J, Moncada S (1992) Accumulation of an endogenous inhibitor of nitric oxide synthesis in chronic renal failure. Lancet 339(8793):572–575
Anderssohn M, Schwedhelm E, Luneburg N, Vasan RS, Boger RH (2010) Asymmetric dimethylarginine as a mediator of vascular dysfunction and a marker of cardiovascular disease and mortality: an intriguing interaction with diabetes mellitus. Diab Vasc Dis Res 7(2):105–118
Das UN, Repossi G, Dain A, Eynard AR (2011) L-arginine, NO and asymmetrical dimethylarginine in hypertension and type 2 diabetes. Front Biosci (Landmark Ed) 16:13–20
Boger RH (2004) Asymmetric dimethylarginine, an endogenous inhibitor of nitric oxide synthase, explains the “L-arginine paradox” and acts as a novel cardiovascular risk factor. J Nutr 134(10 Suppl):2842S–2847S. discussion 53S
Libby P, Buring JE, Badimon L, Hansson GK, Deanfield J, Bittencourt MS et al (2019) Atherosclerosis. Nat Rev Dis Primers 5(1):56
Steinberg D, Witztum JL (2010) Oxidized low-density lipoprotein and atherosclerosis. Arterioscler Thromb Vasc Biol 30(12):2311–2316
Glass CK, Witztum JL (2001) Atherosclerosis. The road ahead. Cell 104(4):503–516
Libby P (2002) Inflammation in atherosclerosis. Nature 420(6917):868–874
Falk E (2006) Pathogenesis of atherosclerosis. J Am Coll Cardiol 47(8 Suppl):C7-12
Libby P, Bornfeldt KE, Tall AR (2016) Atherosclerosis: successes, surprises, and future challenges. Circ Res 118(4):531–534
Feron O, Dessy C, Moniotte S, Desager JP, Balligand JL (1999) Hypercholesterolemia decreases nitric oxide production by promoting the interaction of caveolin and endothelial nitric oxide synthase. J Clin Invest 103(6):897–905
Cominacini L, Rigoni A, Pasini AF, Garbin U, Davoli A, Campagnola M et al (2001) The binding of oxidized low density lipoprotein (ox-LDL) to ox-LDL receptor-1 reduces the intracellular concentration of nitric oxide in endothelial cells through an increased production of superoxide. J Biol Chem 276(17):13750–13755
Aji W, Ravalli S, Szabolcs M, Jiang XC, Sciacca RR, Michler RE et al (1997) L-arginine prevents xanthoma development and inhibits atherosclerosis in LDL receptor knockout mice. Circulation 95(2):430–437
Cooke JP, Singer AH, Tsao P, Zera P, Rowan RA, Billingham ME (1992) Antiatherogenic effects of L-arginine in the hypercholesterolemic rabbit. J Clin Invest 90(3):1168–1172
Holm P, Korsgaard N, Shalmi M, Andersen HL, Hougaard P, Skouby SO et al (1997) Significant reduction of the antiatherogenic effect of estrogen by long-term inhibition of nitric oxide synthesis in cholesterol-clamped rabbits. J Clin Invest 100(4):821–828
Kauser K, da Cunha V, Fitch R, Mallari C, Rubanyi GM (2000) Role of endogenous nitric oxide in progression of atherosclerosis in apolipoprotein E-deficient mice. Am J Physiol Heart Circ Physiol 278(5):H1679–H1685
Kubes P, Suzuki M, Granger DN (1991) Nitric oxide: an endogenous modulator of leukocyte adhesion. Proc Natl Acad Sci USA 88(11):4651–4655
Alheid U, Frolich JC, Forstermann U (1987) Endothelium-derived relaxing factor from cultured human endothelial cells inhibits aggregation of human platelets. Thromb Res 47(5):561–571
Takahashi M, Ikeda U, Masuyama J, Funayama H, Kano S, Shimada K (1996) Nitric oxide attenuates adhesion molecule expression in human endothelial cells. Cytokine 8(11):817–821
Zeiher AM, Fisslthaler B, Schray-Utz B, Busse R (1995) Nitric oxide modulates the expression of monocyte chemoattractant protein 1 in cultured human endothelial cells. Circ Res 76(6):980–986
Bea F, Blessing E, Bennett B, Levitz M, Wallace EP, Rosenfeld ME (2002) Simvastatin promotes atherosclerotic plaque stability in apoE-deficient mice independently of lipid lowering. Arterioscler Thromb Vasc Biol 22(11):1832–1837
Acknowledgements
Original work contributing to this chapter was supported by grants from the Heart Stroke Foundation of Canada and Canadian Institutes of Health Research to M.B.A.-S. and A.K.S.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2023 The Author(s), under exclusive license to Springer Nature Switzerland AG
About this chapter

Cite this chapter
Li, Y., Srivastava, A.K., Anand-Srivastava, M.B. (2023). Nitric Oxide and Cardiovascular Health. In: Ray, A., Gulati, K. (eds) Nitric Oxide: From Research to Therapeutics. Advances in Biochemistry in Health and Disease, vol 22. Springer, Cham. https://doi.org/10.1007/978-3-031-24778-1_2
Download citation
DOI: https://doi.org/10.1007/978-3-031-24778-1_2
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-031-24777-4
Online ISBN: 978-3-031-24778-1
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)