
Abstract
The third Sustainable Development Goal sets out to ensure healthy lives and promote well-being for all at all ages. This will be measured in terms of 13 targets, many of which are direct life and death issues. For example, specific targets relate to reduction of maternal, neonatal and under-5 mortality, addressing communicable and non-communicable diseases, and reducing other causes of death including substance abuse (drugs, alcohol, tobacco) and road traffic accidents. A focus on improved quality of life is also seen in the target of ensuring universal access to sexual and reproductive healthcare services, and providing access to quality essential healthcare and safe, effective, quality and affordable essential medicines and vaccines for all. This chapter will begin with an overview of SDG3, outlining the 13 targets and associated indicators. It will then turn to an evaluation of how well we are doing in relation to this goal, drawing on data from 2015, when the SDGs were instigated, the current status of the indicators, and the latest predictions for the 2030 end date of the SDGs. An international and regional comparative perspective will be used in order to set the context. While the perception may be that Europe is ahead of other regions in achieving targets related to SDG3, there are also areas where the region is lagging behind. As we look within Europe, it will also become clear that there are distinct variations at a national level, and that specific challenges remain. Some consideration will be given to the fact that some of the progress made in many health areas before the COVID-19 pandemic, including improving maternal and children health, increasing immunisation coverage, and reducing communicable diseases, has now halted or even been reversed. Disruptions to essential health services, even within relatively wealthy regions such as Europe, have affected services mental, neurological and substance use disorders; HIV and hepatitis B and C; cancer screening and services for other non-communicable diseases. Moving beyond the statistical data, the chapter then turns to consider some of the questions arising out of SDG3 within the European context. Across the continent, the population structure is changing. Two forms of demographic ageing are being experienced. On the one hand, ‘bottom up’ ageing is being seen as birth rates decline and the younger age cohorts of the population pyramid become smaller than the older generations. On the other hand, ‘top down’ ageing is also evident as life expectancy increases. While European governments are attempting to address this issue, one of the consequences of more people living longer is that there is an increase in a range of non-communicable diseases. Furthermore, as we appear to have entered the late stages of epidemiological transition, health issues associated with degenerative diseases, lifestyle and emerging diseases are on the rise. In its final section, the chapter will look outward from the European perspective, considering responsibilities and ethical issues relating to overseas aid, globalisation and policies which impact on the capacity of other regions and nations to achieve the targets set out by SDG3.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
Introduction
About SDG3 and its Targets
The third Sustainable Development Goal sets out to ensure healthy lives and promote well-being for all at all ages. This will be measured in terms of 13 targets, many of which are direct life and death issues. For example, specific targets relate to reduction of maternal, neonatal and under 5-year-old child mortality, addressing communicable and non-communicable diseases, and reducing other causes of death including substance abuse (drugs, alcohol, tobacco) and road traffic accidents. A focus on improved quality of life is also seen in the target of ensuring universal access to sexual and reproductive healthcare services, and providing access to quality essential healthcare and safe, effective, quality and affordable essential medicines and vaccines for all. Readers interested in a brief overview of SDG3 might find this link helpful, as it incorporates the impacts of COVID-19, discusses the concept of equity in health and makes suggestions as to what individuals can do: https://www.youtube.com/watch?v=ZVqSC_hN2lk.
Table 1 gives all 13 targets and associated indicators. Note that the indicator framework is refined annually and was reviewed comprehensively in March 2020. The indicators listed in Table 1 have incorporated refinements up to and including March 2021.
Exploring the Data on SDG3
SDG3 is the largest goal in the entire 2030 Agenda, covering a large range of topics related to preventing and treating sickness and prolonging life expectancy. This section evaluates progress in relation to the majority of the 13 targets and associated indicators of SDG3, drawing on data from 2015, when the SDGs were instigated and the current status of the indicators. An international and regional comparative perspective is used. While the perception may be that Europe is ahead of other regions in achieving targets related to SDG3, there are also areas where the region is lagging behind. As we look within Europe, it will also become clear that there are distinct variations at a national level, and that specific challenges remain.Footnote 2
Although 2015 is used as the starting point for the SDGs in the data presented here, it should be recalled that the SDGs were preceded by the Millennium Development Goals, which ran from 2000 to 2015. At least three of these earlier MDGs specifically related to health and well-being, focusing on reduction in child mortality, improving maternal health and combatting HIV/AIDS, malaria and other diseases. Thus, it could be argued that a targeted battle against certain elements within SDG3 was already underway for 15 years before the formal initiation of the SDGs. Even earlier, in the 1992 Agenda 21, the action plan which arose from the Earth Summit in Rio de Janeiro, devoted Chapter 6 to ‘protecting and promoting human health’. The good health and well-being goals are clearly explained in this 3 min video: https://www.youtube.com/watch?v=HN9Gz7rCFo4.
Target 3.1: Reduce Maternal Mortality
Globally, some 451,000 women and girls died from complications of pregnancy and childbirth in 2000. Target 3.1 of the SDGs is to reduce maternal mortality. Two indicators, maternal mortality ratio and skilled birth attendance, are used to measure progress. Globally, maternal mortalityFootnote 3 declined by 38% between 2000 and 2017 (the most recent date for which data is available). This represents a fall from 342 deaths to 211 deaths per 100,000 live births, according to UN inter-agency estimates. While this is a significant achievement, it still means that over 800 women die each day from complications in pregnancy and childbirth. The goal is to reduce the maternal mortality ratio to less than 70 per 100,000 live births, with no country having more than 140 maternal deaths per 100,000 live birthsFootnote 4 A map of this indicator for Europe shows that already in 2015 this minimum target had been reached by all European countries.
Table 2 gives the changing maternal mortality rates for the world and for selected regions. Europe has the lowest maternal mortality rates in the world, averaging just 5 deaths per 100,000 live births. This is in sharp contrast with Sub-Saharan Africa, the region with the highest maternal mortality rates, at 534 per 100,000 live births in 2017, representing over two-thirds of all maternal deaths worldwide. The countries with the lowest rates, just 2 per 100,000, in Italy, Poland, Belarus and Norway, contrast with highs of 1150, 1140 and 1120 per 100,000 in South Sudan, Chad and Sierra Leone, respectively. Almost all of these maternal deaths are preventable, particularly if births are attended by skilled health personnel.
Target 3.2: End All Preventable Deaths Under 5 years of Age
The second target within SDG3 is to end preventable deaths of newborns and children under-five years of age. As with maternal mortality, European countries had already achieved the targets set for both indicators by 2015. The under-five mortality rateFootnote 5 varies significantly between different parts of the world, as is clear from Table 3. By 2015, in the European Union, fewer than 4 babies out of every 1000 live births would die by the age of five, compared to over 85 babies born in Sub-Saharan Africa. As of 2019, the highest under-five mortality rates in the world are in Somalia (118.3), Nigeria (116.9), Chad (113.5), Sierra Leone (111.9) and Central African Republic (106.6), contrasting with the lowest rates in San Marino (1.8), Iceland (2.0), Estonia, Finland, Norway and Slovenia (2.3). Some of the greatest relative changes between 2015 and 2019 also occurred in Europe, with drops in Estonia (−26%), Lithuania (−27%), Russia (−29%), Montenegro (−35%) and North Macedonia (−40%). However, it is worth noting that some increases have been noted in European countries, albeit from a low base. Thus, the under-five mortality rate in France rose by 2% to 4.3 in 2019, while rates also rose by 2% in Belgium (to 4.2) and the Netherlands (to 4.1), though these rates are still well below the SDG target of 25 per 1000 live births.
Neonatal mortality, which refers to deaths of newborns within their first month of life, is extremely low in Europe (2.32 deaths per 1000 live births in the EU in 2019), again in stark contrast with Sub-Saharan Africa (27.6) and South Asia (24.9).
Target 3.3: Fight Communicable Diseases
The third target of SDG3 is to fight communicable (infectious) diseases, specifically to end the epidemics of AIDS, tuberculosis, malaria and neglected tropical diseases and combat hepatitis, water-borne diseases and other communicable diseases by 2030. In this case, the data is somewhat less clear cut than for maternal and child mortality. A number of indicators fall within this category. The first relating to HIV/AIDS can be measured by looking at the number of new cases of HIV per 1000 uninfected people aged 15 to 49 years of age. Globally, this rate has fallen by 54% between 2000 and 2019. However, Europe has seen its rate grow by 71%, with particularly strong growth in Serbia (+400%), Montenegro (+250%), Greece (+117%) and Croatia (+100%), representing a worrying trend. By contrast, rates of tuberculosis are stable or falling in European countries, with the exception of Sweden which saw a small increase of 2% between 2000 and 2019, but from a very low base. The World Health Organisation’s Stop TB Partnership has set a target (not specifically related to the SDGs) of reducing national incidence of TB to fewer than 20 cases per 100,000 by 2030. Within Europe, there appears to be an east–west divide in relation to tuberculosis incidence (i.e. cases of tuberculosis per 100,000 population) with 2019 data showing the highest incidence occurring in Moldova (80), Ukraine (77), Romania (66), Russia (50), Lithuania (42), Belarus (29), Bosnia and Herzegovina (27), Latvia (26) and Bulgaria (21). In Western Europe, typical figures are under 10 per 100,000, such as Norway (3.3), Netherlands (5.0), Denmark (5.2), Sweden (5.5), Ireland (5.8), Austria and Italy (6.0) .
Malaria, the third specific disease discussed under the third target, is most prevalent in Africa. Nine out of every ten deaths from malaria in 2015 was in Africa; although there has been significant progress in reducing malaria deaths, in 2017, the World Health Organisation (WHO) warned that the fight against malaria had reached a crossroads.Footnote 6 The World Malaria Report 2020 noted that global gains in combatting malaria had levelled off in recent years. While malaria is a disease associated with tropical regions in the present day, prior to about 1900 malaria posed a risk across more than half of the world’s land surface. Historically, malaria was prevalent in Europe and in North America. Oliver Cromwell (1599–1658) contracted malaria in Ireland, while poet Friedrich Schiller (1759–1805) contracted it in Mannheim, Germany. Since then the disease has been eliminated not only there, but also in East Asia and Australia and in many parts in the Caribbean, South America and Africa (Hay et al. 2004). Potentially, climate change could result in a return of malaria to Europe, although current research suggests that this is unlikely.Footnote 7
The two remaining indicators of this target relate to incidence of Hepatitis B and tackling neglected tropical diseases, neither of which will be covered in this chapter.
Target 3.4: Reduce Mortality from Non-communicable Diseases and Promote Mental Health
Unlike communicable diseases, where Europe is in a relatively strong position with low incidence rates, mortality rates from non-communicable diseases and suicide are a cause for concern in the region. Table 4 illustrates the mortality rate attributed to cardiovascular disease, cancer, diabetes or chronic respiratory diseaseFootnote 8 Cardiovascular disease (a blanket term for diseases relating to the heart and blood vessels, including coronary artery disease and stroke) is the number one cause of death globally, followed by cancer. In wealthy countries, non-communicable diseases (i.e. those which are not directly passed from one individual to another) account for the majority of deaths. The goal is to reduce premature mortality from NCDs by one-third in all countries. Between 2015 and 2019, the countries of the European Union experienced a drop of 7% in this rate, but it is unclear whether the downward trend will be sufficient to achieve the SDG target. Many non-communicable diseases are associated with lifestyle choices, including diet/obesity, tobacco use, alcohol consumption and lack of exercise, although other ‘degenerative’ diseases are associated with physical ageing of the body, and become more common as people live longer. The mortality rate for NCDs is defined as the percent of 30-year-old-people who would die before their 70th birthday from one of the following: cardiovascular disease, cancer, diabetes or chronic respiratory diseaseFootnote 9 For the European Union as a whole this figure is 12.35%, compared with a world average of 18.27%. Within Europe, a high of 24.2% in Bulgaria contrasts with 12.1% in Germany, 10.4% in Austria, 9.6% in Spain and just 7.9% in Switzerland. Non-communicable diseases are explained in under one minute in the following video: https://youtu.be/q0scBynXQL8.
The suicide mortality rate is a further indicator used in relation to target 3.4. Suicide is a leading cause of death, particularly among young people. Globally, the suicide mortality rate, defined as the number of deaths from suicide in one year measured per 100,000 individuals in a given population, was 9.17 in 2019. The rate for the European Union was above this world average, at 11.34, while many European countries exceed this level. Indeed, some of the highest suicide mortality rates in the world have been recorded in European countries, with Lithuania (26.1), Russia (25.1), Ukraine (21.6), Belarus (21.2), Montenegro (21) and Latvia (20.1) all exceeding a rate of 20 per 100,000. While this suggests higher rates are occurring in eastern parts of Europe, rates are also well above the global average in Belgium (18.3) and Austria (14.6), among others. The SDGs call for the promotion of mental health and well-being, rather than defining a specific target level of suicide reduction for this indicator. For more on this topic, see https://ourworldindata.org/suicide.
Target 3.5: Prevent and Treat Substance Abuse
Target 3.5 aims to strengthen the prevention and treatment of substance abuse, including narcotic drug abuse and harmful use of alcohol. Once again, Europe’s record in relation to the indicator of alcohol consumption per capita suggests that there is a significant issue to be addressed. The available data for 2018 shows harmful use of alcohol, defined according to the national context as alcohol per capita consumption (aged 15 years and older) within a calendar year in litres of pure alcohol. European countries dominate the league table, with all but three of the top 20 countries in terms of alcohol consumption being located in Europe. There is no distinct east–west or north–south divide. The highest consumption countries in Europe are Czechia (14.45 L), Lithuania (13.22 L), Luxembourg (12.94 L), Germany (12.91 L), Ireland (12.88 L), Latvia (12.77 L), Spain (12.72 L), Bulgaria (12.65 L) and France (12.33 L). Whereas the world average is 6.18 L and the least developed countries average at just 3.34 L per capita, the European Union average alcohol consumption is 11.44 L per capita.
Target 3.6: Reduce Road Injuries and Deaths
Unlike most SDG targets which are set for 2030, target 3.6 to reduce road injuries and deaths was set to be achieved for 2020 and was measured relative to 2010 levels as it was defined as part of the UN Decade of Action for Road Safety (2011–2020). The goal to halve mortality from road traffic accidents (including vehicle drivers, passengers, motorcyclists, cyclists and pedestrians) was not achieved by 2019. World data shows a drop of 6% between 2010 and 2019, while the reduction for the European region (WHO) was 18%. However, some European countries have made significant progress, including: Lithuania (− 44%), Moldova (− 42%), Russia (− 35%), Latvia (− 34%), Bulgaria (− 31%), Estonia (− 27%), Poland and Croatia (both 26%).
Target 3.7: Universal Access to Sexual and Reproductive Care, Family Planning and Education
According to target 3.7, by 2030 there should be universal access to sexual and reproductive healthcare services, including for family planning, information and education, and the integration of reproductive health into national strategies and programmes. In general, European countries perform well in terms of the indicators used. Indicator 3.7.1 considers the percentage of married women ages 15–49 years whose need for family planning is satisfied with modern methods of contraception. For most of Europe, no data is available, although the World Population Data Sheet 2021Footnote 10 suggests that across Europe an average of 59% of married women in the relevant age cohort are accessing modern methods of contraception, which is the same as for developed countries worldwide.
The second indicator for this target looks at the adolescent birth rate, considering the birth rate per 1000 females aged 15–19 years. Compared to a world average of 41.58 births per 1000 women aged 15–19 years, the figure for the European Union is just 8.74, while some of the lowest rates in the world are seen in European countries including Switzerland (2.52), Slovenia (3.53) and the Netherlands (3.62). However, there are some European countries where adolescent birth rates are significantly higher, particularly Bulgaria (38.79) and Romania (34.86). Furthermore, in Slovakia (26.19) and Hungary (24.57), although the overall rate is lower, the trend between 2015 and 2019 was in an upward direction, with increases of 7% and 9%, respectively. This suggests that access to family planning and education needs to be improved.
Target 3.8: Achieve Universal Health Coverage
This target aims to achieve universal health coverage, including financial risk protection, access to quality essential healthcare services and access to safe, effective, quality and affordable essential medicines and vaccines for all. The Universal Health Coverage (UHC) Index, which operates on a scale from 0 (worst) to 100 (optimal), is a metric use to track progress on this target. It combines information on 14 indicators measuring the coverage of essential services including reproductive, maternal, newborn and child health, infectious diseases, non-communicable diseases and service capacity and access, among the general and the most disadvantaged population. On average, Europe scores 79 on the index in 2019, the most recent year for which data is available. This compares with a world average score of 67. Countries with the highest UHC index are Canada (89), United Kingdom, Sweden, Australia, Switzerland, Norway and South Korea (all 87), contrasting markedly with the lowest scores in Somalia (27) and Chad (28).
Target 3.9: Reduce Illnesses and Deaths from Hazardous Chemicals and Pollution
Under target 3.9, the goal is to substantially reduce the number of deaths and illnesses from hazardous chemicals and air, water and soil pollution and contamination. The death rate from ambient and household air pollutionFootnote 11 varies from as low as 7 per 100,000 in Finland and 8 per 100,000 in Iceland, Norway, Canada and Sweden, to 315 deaths per 100,000 population in the Central African Republic.Footnote 12 The world average is 105 deaths per 100,000. Once again, Europe benefits from a relatively safe environment with excellent regulation of chemicals and pollution.
Indicator 3.9.2 is the mortality rate attributed to unsafe water, sanitation, and lack of hygiene, known as WASH factors. The world average in 2019 stood at 18.21 deaths per 100,000, with European countries having a rate of just 3.23 deaths per 100,000. Sub-Saharan Africa is the region which suffers the highest mortality rate in this category, as in Lesotho (108), Chad and Somalia (both 99) and Central African Republic (97).
Target 3.A: Implement the WHO Framework Convention on Tobacco Control
The goal of strengthening the implementation of the World Health Organisation Framework Convention on Tobacco Control in all countries, as appropriate, does not carry any specific targets. However, it is worth noting that some European countries have a relatively high rate of daily tobacco smokers, including Serbia (40.6% of the adult population), Greece (39.1%), Bulgaria (38.9%), Bosnia and Herzegovina (38.3%) and a further nine countries where over 30% of the adult population are daily smokers.Footnote 13 Tobacco use is directly linked to a number of non-communicable diseases and this lifestyle choice may help to explain some of the problems for European countries in achieving Target 3.4.
Target 3.B: Support Research, Development and Universal Access to Affordable Vaccines and Medicines
Target 3.b has become more relevant than ever in the light of the COVID-19 pandemic. The indicators used specifically focus on four vaccines (three-dose diphtheria, pertussis and tetanus (DPT3); second-dose measles vaccine recommended dose of pneumococcal conjugate vaccine (PCV3) and recommended dose of human papillomavirus vaccine). These vaccines are hugely important. Before the measles vaccine was introduced in 1963 and widespread vaccination became possible, major epidemics occurred approximately every 2–3 years and measles caused an estimated 2.6 million deaths each year. Complications from measles were once a leading cause of blindness. Despite the availability of a safe, effective vaccine, more than 140,000 people died from measles in 2018. Most of them were children under the age of five. The World Health Organisation estimates that measles vaccination prevented an estimated 23.2 million deaths between 2000 and 2018, making measles vaccine one of the best buys in public health. These ‘facts in pictures’ give a good overview: https://www.who.int/news-room/facts-in-pictures/detail/measles. Another indicator used in this category is the proportion of health facilities that have a core set of relevant essential medicines available and affordable on a sustainable basis. Learn more about the concept of universal health coverage in this video: https://www.youtube.com/watch?v=FlETZ202Ovg.
Target 3.C: Increase Health Financing and Support Health Workforce in Developing Countries
The UN goal is to substantially increase health financing and the recruitment, development, training and retention of the health workforce in developing countries, especially in least developed countries and small island developing states. Health worker density, the size of the health workforce per 1000 people, based on the density of physicians, surgeons, nurses and midwives, dentistry and pharmaceutical personnel is an important indicator. European countries come close to the top of the global list for density of medical doctors, just after Cuba which tops the list at 8.42 physicians per 1000 people. The lowest physician density countries are Tanzania (0.01), Somalia (0.02) and Sierra Leone (0.03).Footnote 14 Recruitment of healthcare workers from the global south to the wealthier countries of the global north has helped to further impact the density of doctors, nurses and health scientists in the poorer parts of the world, despite in the USA in 2018, more than 2.6 million immigrants, including 314,000 refugees, were employed as healthcare workers. Immigrants make up 28% of physicians and 38% of home health aides in the USA.Footnote 15 These immigrant healthcare workers were also more likely to die from COVID-19 during the pandemicFootnote 16 A study of Britain’s National Health Service (NHS) hospitals in 2019 found that 29% of doctors and 28% of nurses were non-British nationals.Footnote 17 Healthcare migration to OECD countries was interrupted during 2020 due to travel restrictions, despite an increasing demand for healthcare workers, see https://onesite.eiu.com/data-focus-healthcare-migration-slows/. Although it is expected that migration of healthcare workers will resume, developing countries are trying to reduce this medical brain-drain from further weakening their healthcare systems further.
Overall Progress in Relation to SDG3
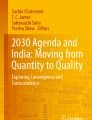
The UN’s annual Sustainable Development Report presents progress towards meeting the goals. The trend assessment uses traffic light colours to measure progress from a baseline year to the most recent data point. While this is based on a limited number of indicators and on the information available as at June 2021, it nevertheless provides a useful overall impression of progress.Footnote 18 The 2021 world map for SDG3 (see Fig. 1) suggests that only two countries in the world, Norway and Australia, have achieved this goal. The majority of European countries fall into the next category ‘challenges remain’, although parts of Eastern Europe are classified as having ‘significant challenges’ remaining, e.g. Romania, Bulgaria and Greece.Footnote 19

Progress in relation to SDG3 (Sustainable development report 2021)
Even before the COVID-19 pandemic, the world was already off track in achieving its targets for 2030. The unfolding pandemic has magnified many deep-rooted problems in relation to structural inequalities, weak public health systems, inadequate health coverage and insufficient social protection. This is further discussed below.
COVID-19 Impacts on SDG3
At the time of writing in Autumn 2021, concerns were being raised that the progress made in relation to SDG3 had been halted, and in some cases even reversed, by the impact of the COVID-19 pandemic. Even before the COVID-19 outbreak, it was clear that progress on the global goals was uneven and that more focused attention was needed in most areas. Unfortunately, the disruption caused by the pandemic has had a negative impact in relation to the implementation of the goals, sometimes turning back progress. For example, the World Health Organisation’s 2021 Global TB Report has shown that deaths from tuberculosis have increased for the first time in a decade as a direct result of the COVID-19 pandemic.Footnote 20 In its 2021 Sustainable Development Goals Report, the UN noted that 90% of countries were still reporting one or more disruptions to essential health services.Footnote 21 Furthermore, the interrelated nature of the goals has led to knock-on effects on the different Sustainable Development Goals as a result of the pandemic (Shulla et al. 2021). The UN has produced a short video highlighting some of the key aspects of SDG3 which have been impacted: https://www.youtube.com/watch?v=J5wZiVd-x4g.
Improving maternal and children health, increasing immunisation coverage and reducing communicable diseases has halted or even been reversed. Many of these are indirect health impacts of the pandemic, caused due to a range of factors including loss of income, poorer nutrition, disruption in seeking or receiving medical care. Early studies have attempted to quantify likely additional maternal deaths and child deaths, which could be very substantial. Disruption to family planning services is also expected to result in an increase in unintended pregnancies.
Interruptions to essential health services, even within relatively wealthy regions such as Europe, have affected services relating to mental, neurological and substance use disorders; HIV and hepatitis B and C; cancer screening and services for other non-communicable diseases. Impacts on healthcare workers, already in short supply in many regions, have been severe. The UN has argued that scaling up investment in universal health coverage (Target 3.8) is essential in the light of the pandemic. They have also pointed out that COVID-19 has highlighted the critical need for preparedness for health emergencies and may be a watershed moment both for such emergency readiness and for investment in critical twenty-first century public services.Footnote 22 Quoted in the UN’s annual report on the SDGs for 2020, António Guterres, Secretary-General of the UN stressed that ‘Everything we do during and after this crisis [COVID-19] must be with a strong focus on building more equal, inclusive and sustainable economies and societies that are more resilient in the face of pandemics, climate change, and the many other global challenges we face.’Footnote 23 Certainly the experience of the COVID-19 pandemic has highlighted the importance of Target 3.D of the SDGs, which is to strengthen the capacity of all countries, in particular developing countries, for early warning, risk reduction and management of national and global health risks.
Whereas life expectancy has tended to rise over time, with an average increase in lifespan of three years for every decade of the twentieth century in Britain, research has shown that life expectancy at birth dropped between 2019 and 2020 in 27 out of 29 countries studied (Aburto et al. 2021). The mortality increases triggered by the COVID-19 pandemic are of a magnitude not witnessed since World War II in Western Europe or the breakup of the Soviet Union in Eastern Europe. These shifts are largely attributable to increased mortality of people aged 60 and over, from official COVID-19 deaths. Males in the USA and Lithuania experienced the largest losses in life expectancy at birth during 2020 (2.2 and 1.7 years, respectively), More than one year was wiped off expected lifespans in 11 countries for males and 8 countries for females. The most significant drops in male life expectancy were recorded for the USA (a drop of 2.2 years) and Lithuania (1.7 years).
Aburto et al.’s (2021) study of changes in life expectancy concludes with the observation that, ‘although COVID-19 might be seen as a transient shock to life expectancy, the evidence of potential long-term morbidity due to long COVID and impacts of delayed care for other illnesses (cancer, cardiovascular disease) as well as health effects and widening inequalities stemming from the social and economic disruption of the pandemic suggest that the scars of the COVID-19 pandemic on population health may be longer-lasting.’
Certainly, the pandemic has halted the significant progress which had been made in increasing life expectancy and in reducing child and maternal mortality. In some ways, it has also helped to focus our thinking on the way forward to achieve the SDGs. Ground-breaking research considering the impact of COVID-19 on the Sustainable Development Goals was published in April 2021 (Hughes et al. 2021). Using modelling to consider three potential recovery scenarios, this research shows the ongoing likely impacts of the pandemic over the next decade. As might be expected, the gap between rich and poor countries is likely to widen due to the social and economic impacts of the pandemic. Even prior to the COVID-19 pandemic, the data suggests that the world would have been unlikely to reach the SDG target values for maternal mortality, child mortality or neonatal mortality rates by 2030. On a global average basis, these three targets did appear reachable by 2050, and this appears to be the case in spite of the impacts of COVID-19. However, their modelling also suggests that an ‘SDG Push’, involving a combination of policies and investment in governance, social protection, the green economy and digitalisation, could enable the least developed countries to exceed their pre-COVID-19 development trajectories. By accelerating progress to the targets, the SDG Push scenario could enable the world on average to achieve each of the health goals by 2030, although at the country level, some of the lowest income countries would still struggle to attain these targets.
From a geographical perspective, during the pandemic, we have witnessed major issues regarding disruption in supply chains, especially in relation to medical products, PPE and other essential goods. The challenges caused by the distance between locations of production and consumption have highlighted the globalised economic system and illustrated that the current neoliberal system of production and supply is out of sync with health and social needs on the ground. Furthermore, such a system is not sustainable either environmentally (due to the CO2 emissions occasioned by long-distance transport routes), economically (due to the disruptions in these supply chains) or socially (with rising tensions). For more discussion of the impacts of the coronavirus pandemic, see https://www.eiu.com/n/novel-coronavirus-outbreak/.
Future research will tell very different narratives regarding the effects of the pandemic, for instance within India, a major pharmaceutics producer and between India and other countries. Similarly, appraisal of the pandemic experiences within and between European countries and Israel will doubtlessly be significant.
Demographic Futures in Europe and Beyond
As already noted, SDG3 sets out to ensure healthy lives and promote well-being for all at all ages. This last element, ‘at all ages’, is becoming increasingly relevant in a European context. Across the continent, the population structure is changing and two forms of demographic ageing are being experienced. ‘Bottom up’ ageing is being seen as birth rates decline and the younger age cohorts of the population pyramid become smaller than the older generations. Meanwhile, ‘top down’ ageing is also evident as life expectancy increases and the height of the population pyramid grows, representing increasing numbers living into old age. While increased life expectancy should be a cause for celebration, it can also cause policy issues for governments. The ratio of workers to pensioners in Europe is decreasing. Whereas in 1990, there were 5.8 workers for every one pensioner, and this ratio had fallen to 3.9:1 by 2000 and is predicted to fall further, putting a strain on social services and pensions provision.
This long-term shift in disease and cause of death patterns in Europe was explained by Omran (1971) in the epidemiological transition model. Paralleling the demographic transition model, this suggests that there is a shift over time from high mortality (largely from infectious diseases, with most deaths at young ages) to low mortality (with most deaths at older ages, largely due to degenerative diseases). Europe is now experiencing an increase in chronic disease associated with ageing, with heart disease (cardiovascular disease), cancer and diabetes among the major causes of death. Longer life is also associated with a relatively long period of morbidity, so a focus on promoting healthy ageing is needed, including tackling social and cultural behaviour around patterns of food and alcohol consumption. An increased demand for healthcare is inevitable for ageing populations, and this must be recognised in future planning. A 2006 report on healthcare in Europe noted that demographic ageing would increase demands for health services while simultaneously shrinking the pool of workers available to offer these services.Footnote 24 Already, European countries have been recruiting healthcare staff, including workers in long-term care homes for the elderly, from non-EU countries. This trend is likely to persist, despite the negative impact that this brain-drain will have on the countries of origin.
As the previous sections have demonstrated, the countries of Europe have a mixed score card in relation to SDG3, but are performing better overall than many regions which have fewer socio-economic advantages. While there are clearly aspects which individual European countries need to address internally, in relation to alcohol consumption and non-communicable diseases for example, it is important to the overall achievement of the SDGs that European countries and institutions look outwards. Global inequalities have been brought into sharp focus due to the COVID-19 pandemic, and it is clear that the negative impacts will be keenly felt into the future. In order for the ‘SDG Push’ to be successful, wealthy countries and regions must provide support. This includes direct financial support through overseas development aid (ODA) budgets. The United Nations target is for governments to contribute at least 0.7% of GNI to ODA. Preliminary OECD data for 2020 shows that only six countries (of 29 listed) had reached or exceeded that target, namely Luxembourg, Norway, Sweden, Denmark, Germany and the United Kingdom.Footnote 25 The institutions of the European Union are also significant donors of ODA, indeed the EU is one of the top three donors of development aid in the world, although it has yet to reach the target of donating at least 0.7% of its gross national income annually. In the light of the pandemic and the effects of climate change, the European Commission increased its 2021 annual humanitarian budget by over 60% compared with that adopted in 2020.Footnote 26 However, as is stated in official EU documentation, financial aid alone is not sufficient to achieve the sustainable development goals. Political action is also required.Footnote 27
One example of where political action could assist in relation to SDG3 relates to vaccine equity. During the pandemic, the international legal agreement in relation to intellectual property—known as Agreement on Trade-Related Aspects of Intellectual Property Rights (TRIPS)—came into sharp focus. This agreement which is administered by the World Trade Organisation concerns the regulation by national governments of different forms of intellectual property (IP) as applied to nationals of other WTO member countries. Controversy previously arose over AIDS drugs in Africa, where it was shown that patents had resulted in high drug costs for public health programmes. This resulted in the Doha Declaration, issued in November 2001, which indicated that TRIPS should not prevent states from dealing with public health crises. However, in spite of this interpretative statement, in 2020 new conflicts emerged in relation to patents and copyrights related to the vaccines, diagnostics and treatments associated with COVID-19. As of 17 June 2021, around 68 vaccines were administered for every 100 people in Europe and Northern America compared with fewer than 2 in sub-Saharan Africa.Footnote 28 In October 2020, it was proposed that the WTO would grant a temporary waiver (the TRIPS waiver) to enable more widespread production of the vaccines, which would be beneficial to the global population. Although this was supported by over 100 developing nations, the proposal was blocked by the G7 members (which include France, Germany, Italy and the UK). Learn more about the call for affordable access to COVID-19 vaccines for everyone in this video from DW News: https://youtu.be/CTEGQMJVLZ8.
The European Parliament failed to reach consensus in relation to a revised TRIPS waiver proposal in May 2021, although the Parliament's resolution of 20 May 2021 on accelerating progress and tackling inequalities towards ending AIDS as a public health threat by 2030 also called on the EU to support the TRIPS waiver.Footnote 29 Indeed, this resolution called for the EU to set up a clear and coherent EU global COVID-19 vaccination strategy, focusing on ensuring equal, affordable and timely access to vaccination for people in developing countries. It also called on the Commission and Member States ‘to ensure that the global response to COVID-19 includes lessons learned from the fight against HIV, such as: protecting human rights and addressing stigma and discrimination, particularly among key and other vulnerable populations; fighting gender barriers to health; supporting healthcare practitioners and researchers, especially in low-resource settings; engaging communities in the response; and fairly allocating limited resources and new tools so that no one is left behind’. The resolution urged the EU to establish a comprehensive global strategy and road map for the achievement of the SDGs, called for an effective long-term EU global health strategy and insisted ‘that the Commission needs to redouble its efforts and intensify its work towards effective global health programmes targeting healthcare systems in developing countries’.
The need for political action in order to achieve the SDGs, including SDG3, is evident from the work of the United Nations and is also clearly recognised within Europe, as the resolution of 20 May 2021 demonstrates. The interconnected nature of our world has come into sharp focus with the COVID-19 pandemic. It has also become clear that actions to improve public health and preparedness will be beneficial for all. Therefore, if European countries fail to act from a moral and ethical standpoint, perhaps they can be prevailed upon to do so for pragmatic reasons. ‘We are at a critical juncture in human history’, according to the Under-Secretary-General of the UN Department of Economic and Social Affairs, Liu Zhenmin. If we learn from the pandemic, we can rise to the challenges which face us now and into the future. As the most recent Sustainable Development Goals Report (2021) highlights, addressing COVID-19 has demonstrated community resilience, decisive government action, rapid expansion of social protection and unique collaboration to develop life-saving treatments in record time. All of these positive impacts could form the basis for unprecedented action to achieve the Sustainable Development Goals not just in Europe, but globally.
Notes
- 1.
The Agreement on Trade-Related Aspects of Intellectual Property Rights (TRIPS) is an international legal agreement between all the member nations of the World Trade Organisation, which is discussed later in this chapter.
- 2.
- 3.
The maternal mortality ratio is defined as the number of women who die from pregnancy-related causes while pregnant or within 42 days of pregnancy termination per 100,000 live births.
- 4.
- 5.
Under-five mortality rate is the probability per 1,000 that a newborn baby will die before reaching age five, if subject to age-specific mortality rates of the specified year.
- 6.
World Malaria Report 2020, available at https://cdn.who.int/media/docs/default-source/malaria/world-malaria-reports/world-malaria-report-2020-briefing-kit-eng.pdf?sfvrsn=eda98467_18&download=true.
- 7.
- 8.
This is defined as the percent of 30-year-old-people who would die before their 70th birthday from any of cardiovascular disease, cancer, diabetes, or chronic respiratory disease, assuming that they would experience current mortality rates at every age and would not die from any other cause of death (e.g. injuries or HIV/AIDS).
- 9.
Assuming that they would experience current mortality rates at every age and would not die from any other cause of death (e.g. injuries or HIV/AIDS).
- 10.
World Population Data Sheet 2021, Population Reference Bureau: https://interactives.prb.org/2021-wpds/
- 11.
The age-standardized annual number of deaths attributed to household and ambient air pollution per 100,000 people.
- 12.
Data is for 2019, drawn from the Global Burden of Disease Study (2019), while WASH data is drawn from the UN. Source: http://ghdx.healthdata.org/gbd-results-tool
- 13.
Data for 2018 is sourced from World Health Organization (WHO) Department of the Prevention of Noncommunicable Diseases; Secretariat of the WHO Framework Convention on Tobacco Control.
- 14.
Data for 2018, sourced from http://data.worldbank.org/data-catalog/world-development-indicators.
- 15.
- 16.
- 17.
- 18.
A baseline year of around 2015 or 2010 is used for the trend assessment. For most of the indicators, the latest available data are from 2019 to 2020; for a few indicators, the data are from 2017.
- 19.
- 20.
- 21.
- 22.
- 23.
Quote available from: https://www.un.org/en/desa/sustainable-development-goals-report-2020.
- 24.
European Observatory on Health Systems and Policies (2006) The Health Care workforce in Europe: learning from experience. Available at https://www.euro.who.int/__data/assets/pdf_file/0008/91475/E89156.pdf.
- 25.
- 26.
- 27.
- 28.
https://www.un.org/en/desa/sustainable-development-goals-sdgs, page 32 of the report, accessed 14 October 2021.
- 29.
References
Aburto JM, Schöley J, Kashnitsky I, Zhang L, Rahal C, Missov TI, Mills MC, Dowd JB, Kashyap R (2021) Quantifying impacts of the COVID-19 pandemic through life-expectancy losses: a population-level study of 29 countries. Int J Epidemiol 2021:dyab207. https://doi.org/10.1093/ije/dyab207
Hay SI, Guerra CA, Tatem AJ, Noor AM, Snow RW (2004) The global distribution and population at risk of malaria: past, present, and future. The Lancet Infect Dis 4(6):327–336, June 01, 2004. https://doi.org/10.1016/S1473-3099(04)01043-6
Hughes BB, Hanna T, McNeil K, Bohl DK, Moyer JD (2021) Pursuing the sustainable development goals in a world reshaped by COVID-19. Frederick S. Pardee Center for International Futures and United Nations Development Programme (April 2021), Denver, CO and New York, NY. https://sdgintegration.undp.org/sites/default/files/Foundational_research_report.pdf. Accessed 10 Oct 2021
Omran AR (1971) The epidemiologic transition, a theory of the epidemiology of population change. The Milbank Memorial Fund Quarterly, 49 (4): 509–38
Shulla K, Voigt BF, Cibian S et al (2021) Effects of COVID-19 on the sustainable development goals (SDGs). Discov Sustain 2:15. https://doi.org/10.1007/s43621-021-00026-x
Acknowledgements
The author would like to acknowledge the constructive comments and suggestions from Dr. Gerry O’Reilly and an anonymous reviewer on a previous draft of this chapter.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2023 The Author(s), under exclusive license to Springer Nature Switzerland AG
About this chapter

Cite this chapter
McManus, R. (2023). Exploring Health and Well-Being in a European Context. In: De Lázaro Torres, M.L., De Miguel González, R. (eds) Sustainable Development Goals in Europe. Key Challenges in Geography. Springer, Cham. https://doi.org/10.1007/978-3-031-21614-5_3
Download citation
DOI: https://doi.org/10.1007/978-3-031-21614-5_3
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-031-21613-8
Online ISBN: 978-3-031-21614-5
eBook Packages: Earth and Environmental ScienceEarth and Environmental Science (R0)