
Abstract
Spaceflight has unique effects on spine biomechanics and the central nervous system elements of the spine. We explore the resulting pathologies such as inflight back pain, radicular symptoms, and disc herniation as they apply to the astronaut both during spaceflight and postflight recovery. Biomechanical and pathological effects on spine health caused by adaptions to spaceflight are important to understand not only as barriers to mission success, but with the right countermeasures in place, could represent a preventable occupational hazard. As missions increase in duration and destinations become more remote from a source of outside assistance, the understanding of potential mission-threatening risks on spinal function and health will be paramount in anticipating and mitigating these decrements.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others

Keywords
This chapter will discuss the effects that spaceflight has on spine biomechanics, the central nervous system, and resulting pathology as they apply to the astronaut both during spaceflight and postflight recovery. Both the biomechanical and pathological effects that spaceflight poses on spine health are important to understand not only as barriers to mission success, but with the right countermeasures in place, could also represent a preventable occupational hazard. As missions increase in duration and destinations become more remote from a source of outside assistance, the understanding of potential mission-threatening risks on spinal function and health will be paramount in anticipating and mitigating these decrements.
History of Back Pain and Spinal Injury Associated with Spaceflight
Spinal problems occurring from spaceflight were first reported dating back to 1977 [1, 2] (Fig. 5.1). Symptoms included in-flight back pain during the initial phase of spaceflight “space adaptation back pain” [3], postflight low back pain, and disc herniation [4]. The prevalence of inflight space adaptation back pain (SABP) ranges from 52 to 68%, begins within the first 6 days of spaceflight, and is reported to be mild in severity in 86% of cases [3, 5]. During the shuttle era, back pain was the fifth most common reason given for medication use [6, 7]. The lower back is affected in 86% of SABP cases [3]. An existing history of low back pain (LBP) predicted risk for developing space adaptation back pain, leading to a significantly longer duration of low back pain experienced in space and often impacting additional spinal regions [5]. Space adaptation back pain often resolves within the first 12 days of spaceflight and is most commonly alleviated by assuming a “fetal tuck” stretching position where individuals bring their knees to their chest. Space adaptation back pain is often compared to adaptational back pain experienced during prolonged bedrest [5, 8], however with greater pain intensity, and experienced over a longer duration of time.

Roy Gagnon coinvestigator, conducting a training session on NASA’s KC-135 microgravity simulator with subject Ken Money, Canadian astronaut. Reproduced with permission from(Wing et al. 1991)
Following spaceflight, astronauts experience a heightened risk of intervertebral disc herniation or herniated nucleus pulposus (HNP). Disc herniation results from a bulging or extrusion of the nucleus pulposus due to compressive forces and/or weakened annulus fibrosus tissue [9]. The bulging or extruded disc often compresses or irritates the spinal nerves on the posterolateral side of the disc and compression on the spinal nerve roots can cause radicular pain and neurological deficits. The incidence of disc herniation (both cervical and lumbar) was 4.3 times higher in the US astronaut population compared to matched controls not involved in spaceflight [4]. Notably, astronauts incidence of cervical HNP was significantly elevated over the control group at 35.9 times higher in the first 12 months after spaceflight and a lifetime incidence that was 21.4 times higher than the control population [4]. Despite this increased risk of cervical HNP, the low back remains more affected overall with nearly 60% of postflight disc herniations in astronauts reported to occur in the lumbar spine [4]. The lower incidence of lumbar herniation compared to control group likely reflects the general population’s propensity to manifest injury or wear and tear damage to their low back more often than their cervical spine region.
Importantly, compared with data on terrestrial backpain, there is a paucity of equivalent data as it relates directly to spaceflight. At the time of this publication, less than 600 people have flown into space, and of that number, less than 500 were for long-duration missions. Much of the early spaceflight program did not focus on collecting data on symptoms like back pain, instead, reasonably enough, focusing on hemodynamics, reaction times, and other acute physiologic considerations that could disrupt the mission. However, as missions have changed over time, the medical considerations have broadened to include more chronic pathologies. To date, much of the data supporting the hypotheses behind spinal issues in spaceflight come from the terrestrial bed-rest literature, where analogous symptomology can often be found.
Comparing Epidemiology of Spaceflight-Related Low Back Pain to Terrestrial Low Back Pain
Back pain is a symptom, and not a disease, with many causal factors that are not always clearly associated with each presentation. LBP, in particular, is of concern as it is the leading cause of disability and economic burden due to work absence throughout much of the world [10, 11]. In terrestrial populations, low back pain is an extremely common phenomenon with a global point prevalence of 8% [12]. In astronauts, low back pain is one of the most common problems experienced in flight as well as postflight [3, 13].
There are some important distinctions in astronaut populations compared to terrestrial populations when considering the epidemiology of back pain. For terrestrial populations, both obesity and physical inactivity are significant predictors for low back pain [14]. Astronauts must maintain excellent physical conditioning as part of their training which obviates both obesity and sedentary behavior as factors for developing or exacerbating back pain. The pathology associated with obesity-mediated low back pain likely has to do with chronic hyper-loading of the spine and poor spine mechanics, as opposed to the chronic unloading associated with the microgravity environment of spaceflight. Additionally, there is a significant psychological and psychosocial component to chronic low back pain presentation in the general terrestrial population which often occurs concurrently and is possibly exacerbated by depression, anxiety, stress and economic uncertainty associated with lower-income socioeconomic groups [14, 15]. Among terrestrial populations, there is also a component of possible over-reporting in some cases as a means to gain compensation or time away from work, or in conjunction with the previously mentioned psychological components, as somatization of unaddressed psychological illness [16].
In terrestrial populations, the medical or musculoskeletal diagnosis associated with back pain is usually not predictive of the degree of persistent disabling back pain [17]. Instead, it is the concurrent presence of psychiatric disease, poor physical function, low general health status. and maladaptive pain coping behaviors that predict the severity of impact from LBP. These difficult-to-quantify aspects of back pain presentation are largely not reflected in the astronaut population. It is not as though astronauts cannot experience anxiety, depression, or maladaptive pain coping behavior, but that if they have, it has not significantly hindered their performance. Astronauts are screened rigorously and selected from a pool of superbly resilient recruits who have already proven themselves to be so by coping well in other high-stress environments over time. Additionally, the astronaut population has been known to under-report symptoms to avoid the loss of flight status and are not typically experiencing socioeconomic hardship. As a result, studying causes of back pain in astronauts can be particularly revealing as they (as a population) lack many of the other confounding features known to influence back pain presentation. Therefore, the possibility of being able to better associate a particular identifiable pathology with the severity of symptoms seems more promising in the astronaut population, who are already so carefully monitored and assessed for optimal health over time.
Spinal Anatomy Affected by Gravitational Load
To better understand how prolonged exposure to microgravity can uniquely influence the incidence of back pain and spinal disorders in humans, we need to consider the effect of altered load on the diverse tissues of a spinal motion segment. An individual spinal motion segment includes two adjacent vertebrae connected by an intervertebral disc (“disc”) and two facet joints. The human lumbar spine includes five motion segments spanning L1 through S1, stabilizing ligaments, and trunk musculature. The vertebral bodies are cylindrical and are built to absorb load without catastrophic fracture [18]. They are comprised mainly of trabecular bone and have a nutrient-rich interior with many blood vessels. The intervertebral disc is essentially a large ligament, serving as a viscoelastic joint between vertebral bodies, permitting intersegmental motion and absorbing axial load. The intervertebral disc is an avascular structure and is dependent on diurnal loading cycles to receive nutrients from adjacent vertebral bodies [19]. Nutrient transfer between the vertebral body and discs is dependent on load bearing, and this, in turn, maintains healthy discs. The well-being of the intervertebral disc can, therefore, be considered load dependent and is disrupted without diurnal gravitational loading. The effects of disuse and unloading are problematic for muscle health at large, and the human spine in particular is dependent on many specialized muscles supporting the mechanical demands of upright posture. Looking across several spinal tissues, including the intervertebral discs and paraspinal muscles, each of which are distinct stabilizing tissues of the spine and could contribute to risk for spaceflight related spinal injuries and pain.
Intervertebral Discs
Spaceflight-associated spinal problems were reported as far back as 1977 [1, 2], including inflight back pain [3] and postflight disc herniations [4, 20]. Originally, the pathophysiology of these inflight and postflight spinal problems was not reported/declared, but it was hypothesized to be a result of possible elevated disc swelling that could be associated with the apparent changes in spinal alignment and height during spaceflight and bed rest [1, 21,22,23,24]. This potential increased swelling during spaceflight could result in discs returning from space with greater hydration and presumably more vulnerability to herniation with compression from load bearing after returning to earth. Bedrest is considered to be an analog for spaceflight, and prolonged bedrest is shown to be associated with increased disc height long after upright posture is resumed [8, 25, 26]. However, there are only two studies that quantify changes in disc swelling following spaceflight, and neither find significant changes in disc size or water content [23, 27, 28]. Furthermore, animal studies on rodent disc properties following spaceflight do not show an increase in lumbar disc height or hydration [29].
Discs may still be swelling due to a supraphysiological state during spaceflight, but previous longitudinal astronaut data along with a previous bedrest study [22, 27] suggest that any effect from prolonged unloading on disc swelling is no longer present shortly after reintroduction of axial spinal loading under gravity.
Paraspinal Muscles
More recently, the effect of spaceflight on the paraspinal muscles has become a point of interest. The paraspinal muscles, particularly the multifidi, serve a key biomechanical role in stabilizing the lumbar spine segments in response to postural load and motion. As such, the paraspinal muscles are also linked to LBP, though the exact relationship between the paraspinal muscle changes and back pain is still under investigation.
Given the important role of the paraspinal muscles in stabilizing the spine and upper body in upright posture under gravitational load, then prolonged unloading would lead to decreased activity and atrophy of these muscles. Spaceflight-induced atrophy of these muscles could lead to postflight biomechanical instability, resulting in low back pain and risk for disc herniation [27]. However, the extent by which the paraspinal muscles are affected by microgravity is unclear. Recent studies do show that the lumbar paraspinal muscles experience some degree of atrophy following spaceflight [27, 28, 30,31,32]. The inconsistency between study results may be, in part, due to variability in imaging methods and assessments. However, another factor that may influence inconsistency in results may be variability in exercises conducted in space by each crew member. These recent muscle studies follow crew that stay at the International Space Station, where there are exercise devices that can engage the spinal muscles by bearing the upper body during more aerobic and resistance exercise. The current version of the treadmill on the ISS, Combined Operational Load-Bearing External Resistance Treadmill, or COLBERT, utilizes a harness that loads the shoulders and, to a lesser degree, the hips. This harness is then connected to the treadmill frame by bungee cords that provide varying degrees of load, up to 60% of body weight. The Advanced Resistance Exercise Device (ARED) allows astronauts to perform up to 29 different free-weight-type resistance exercises with up to 270 kg of resistance force. The ARED uses a combination of lever arms and vacuum pistons to provide the force resistance and is connected to the structure of the ISS via vibration damping mechanism to protect the spacecraft during its use.
Changes in Spinal Biomechanics During and After Spaceflight
The human lumbar spine biomechanically supports upright posture and provides three functions: to protect the spinal cord, to facilitate motion between the upper body and pelvis, and to transfer load from the upper body to the pelvis [33]. During spaceflight, gravitational load is removed and astronauts often experience mild to moderate adaptational low back pain that develops within the first few days of orbit [3]. The cause of the SABP is unknown but thought to be a result of the assumed stretching and elongation of the spine in space [1, 24]. The spinal column is shown to elongate by 6% on average during the first few days of spaceflight which is thought to be attributed to a decrease in spinal curvature and increase in disc volume [24]. Bedrest studies are considered an analog to unloading from microgravity by removing vertical load from the spine and prompting adaptational spinal pain. Diurnal changes in spinal length have shown a 1% increase following bedrest from nightly sleep [34]. Adaptational pain associated with spaceflight and bedrest is thought to be a result of the sudden lengthening during the initial unloading phase [1, 35, 36].
Following spaceflight, astronauts often experience postflight spinal stiffness soon after return to earth and a heightened incidence of disc herniation and chronic low back pain well beyond the immediate reintroduction to gravitational load [4, 27]. Few studies have examined astronaut spine biomechanics following long-duration spaceflight. Recent work by Bailey et al. demonstrates an association between reduced spinal kinematics and reduced multifidus muscle quality following spaceflight [27, 37]. This work indicates that spaceflight-induced changes in paraspinal muscle leads to compromised post-spaceflight spinal biomechanics [27]. Additionally, disc hydration or height is not shown to significantly change with spaceflight and is therefore not supported as a factor influencing post-spaceflight spinal stiffness [27, 28]—running contrary to long held hypotheses that intervertebral disc swelling following spaceflight is a causal factor for disc herniations.
Spinal pain both during and after spaceflight appears to be due to changes in spinal mechanics, whether it be sudden lengthening inflight or stiffness and reduced stability following spaceflight. Localized pain in the spine is likely due to changes in forces on spinal tissues and not neurogenic. However, more work needs to be done on the effects of spaceflight on proprioception, balance, and how this may influence risk for spinal pain during and after spaceflight [38].
Backpain and Spaceflight
Pain Pathways for Low Back Pain
The perception of pain is not a unified single stimulus reflected in one conscious experience. Instead, it is the subjective experience resulting from the cortical processing of many different afferent nociceptive signals coming from a variety of sources.
Regarding low back in particular, the presentation and localization can be quite frustrating for both patient and clinician, as the innervation of many structures may produce a vague subjective location of pain. Many pathological origins that are quite distinct can have presenting symptoms of pain in similar locations. An example is that facet or zygapophyseal joint (z-joint)-mediated pain often refers to areas that appear to be remote from the facet but have other structures in that local area which could also be mistaken for the pain generator. Figure 5.2 shows a pain map of locations where pain is perceived when a certain z-joint is the cause of pain. The pain pathway that facilitates back pain is complex, but a simplified view of it is that a peripherally innervated structure receives a stimulus that triggers an afferent pain signal. This stimulus could be from a multitude of stimuli such as the stretch receptors in a muscle or joint capsule reaching a certain threshold of stretch, a noxious local environment facilitated by inflammation such as a tendinopathy at myotendinous insertion, a muscle overuse cramp, or mechanical disruption such as a tear in muscle or connective tissue. Each of these afferent peripheral signals then travels to the central nervous system and are integrated and further modulated in the spinal cord before being transmitted toward the brain. Habitual stimulation of these pathways can result, in some cases, in a consolidation of signal processing at the point where the peripheral nervous system meets the central nervous system, and the modulation can act to amplify the pain signal. Such centralization is a leading theory behind the development of chronic back pain.

Facet joint pain-referral map demonstrates regions where pain can be referred remote to the joint in question
The innervation of the structures in the back and known pain pathways can give some clues as to the cause of the pain, but often cannot account for the whole picture of the pathologic state. Muscle tightness in response to nearby zygapophyseal joint inflammation may generate the pain in the form of a cramping muscle. Alternatively, the pathological tightness of a muscle after a strain injury may place uneven forces across the joint complex, exacerbating any dysfunction already present there and causing pain to be generated (over and above the pain caused by the muscular strain) from the structures innervated at the joint complex. It is often impossible to tease one cause out entirely from another, as there can be overlapping and mutually reinforcing pain generators or pathologic states.
Potential Pain Pathways Associated with Back Pain During Spaceflight
There are several hypothesized pathologies in the production of back pain during spaceflight. At this point it is important to highlight the potential differences between possible etiologies for SABP and back pain from other sources during the flight. There is a predictable nature of SABP presentation in the majority of astronauts entering microgravity, and this might warrant a different approach to treatment or mitigation than other backpain causes. SABP tends to appear within the first day or so of exposure to microgravity and last as long as about 12 days, with the majority lasting around 6 days [1, 39]. The pain ranges from moderate to severe and is reported by the majority of astronauts [3]. Looking at the potential pain generators that could be consistent with the SABP presentation, it is important to consider the clinical presentation as well as the alleviating factors, most importantly that relief occurs in most cases with the astronaut assuming the fetal-tuck position, exercise, or spinal loading [3].
Upon reaching space, microgravity completely unloads the spinal column, allowing for a nearly total state of rest for all the muscles involved. Importantly, this includes the postural muscles like the deep multifidi and erector spinae that normally fire continuously at a low rate, controlled largely at a subconscious level, to resist gravity and prevent the trunk from falling over during upright posture in gravity. In microgravity, the body assumes what is known as the neutral body posture, where the hips and knees are slightly flexed, with a general loss of the normal spinal curvature. This unloaded state not only sets in motion the catabolic pathways within the muscle that begins the process of atrophy, but biomechanically it also starts to flatten out the natural spinal curvature. This unnatural flattening can have several possible effects which may act as pain generators. Traditionally, in a terrestrial population, a presentation of back pain that is relieved with forward flexion is suggestive of facet-mediated pain. Again, in the terrestrial population, disc-mediated pain is exacerbated by forward flexion and alleviated by back extension. In contrast, SABP is more commonly relieved with flexion [3] and extension has no effect [13]. Thus, we have to consider more closely the unique unloaded environment of microgravity and what physiologic features could contribute to this presentation. An explanation postulated by Sayson et al. is that the lower mechanical compression and subsequent over-hydration of discs for prolonged periods of time may contribute to SABP through the mechanism of excessive collagen deformation of the annuli with disc expansion and subsequent stimulation of type IV mechanoreceptors and nerve impulse propagation through the sinuvertebral nerves.
Another hypothesis for why this potential disc-mediated back pain is relieved with forward flexion is that it has metabolic origins. The traditional idea of disc-mediated back pain, such as an annular tear, should become more painful when a spine flexed posture is assumed and the load on the disc and subsequently the damaged tissue is increased. However, the disruption of the diurnal compression cycle on the disc could be causing a problem of microcirculation. The intervertebral disc (IVD) is the largest avascular structure in the human body and requires the slow influx of fluid containing nutrients via osmosis from the microvasculature of the vertebral body endplate [9, 13]. This process is facilitated through the diurnal compression and rehydration cycle produced with the normal human patterns of sleep (rehydration via proteoglycan-mediated osmosis during unloading) and compression (upright posture within a gravity environment causing increased hydrostatic pressure through compression and subsequent fluid efflux from the disc). This cycle is important because it is the only way that the chondrocytes and other metabolically active tissues that maintain the IVD can receive nutrients and remove waste (mostly lactic acid byproduct) [40]. The innervation of the outer third of the IVD is also provided by branches of the recurrent sinuvertebral nerve which is an unmyelinated mixed nerve with nociceptive fibers that may respond with pain signals to a metabolically deficient environment produced by the poor circulation of normal IVD nutrient and waste cycle caused by microgravity. If the astronauts are spending an unnatural amount of time unloaded without facilitating this nutrient and waste exchange, and subsequently developing a buildup of metabolic wastes in that local tissue, it may be enough to irritate the nociceptive fibers of the sinuvertebral nerves in the outer third of the annulus fibrosis of the IVD.
Alternatively, there could be facet-mediated pain unique to the microgravity environment caused by the change in biomechanical forces. An increase in disc height due to hydration without the normal diurnal compression may produce a new and unnatural form of mechanical strain on the zygapophyseal joints (z-joint). The increased disc size might act as a lever, which pushes the vertebral bodies away from one another using the z-joint as the fulcrum. Such non-physiologic pressure may provide enough noxious stimulus, when not relieved by diurnal compression, to produce back pain that has its local origin in the facet joint and is then relieved by the forward flexion (fetal tuck) that most astronauts have reported finding relief with. This forward flexion would preferentially reload the discs, potentially causing some fluid shift, but more immediately relieving the unnatural pressure placed on the z-joint.
Other Factors Contributing to Back Pain During Spaceflight
There are other aspects of spaceflight that might contribute to development of back pain in flight, starting with the actual launch from Earth itself. Astronauts spend a long time sitting in the seat of the spacecraft while launch preparations are being made. Hours in a cramped seat in a pressure suit could exacerbate any issues already present with respect to asymmetrically tight muscles, prior injuries that predispose the astronaut to recurrent pain, or other osseoligamentous deficiencies that may only produce pain when put in extreme circumstances. Another potential pathway for back pain generation in spaceflight is pain from an acute back injury. The COLBERT and ARED have been a huge improvement to inflight countermeasures for muscle atrophy and bone loss [41], but they also represent one of the largest generators of acute injury in space [42]. A strained muscle or inflamed disc from poor mechanics during a high-load exercise maneuver can cause significant impairment. While the injuries would be similar to terrestrial sports injuries, the recovery may follow a different trajectory, as the patient would otherwise be unloaded due to microgravity after the injury and remain so unless deliberately loading themselves using an exercise device. This complete unloading will change the muscle utilization across the spinal column as well as the diurnal loading pattern of the discs, resulting in a both poor spine biomechanics and a disc that is likely experiencing micro-circulation disruptions. Such changes may serve to predispose the tissue to injury over and above what might be seen with the same loads in a population that had not experienced microgravity. Additionally, and of paramount importance to inflight recovery from injury, many tissues, including the chondrocytes responsible for maintaining and repairing connective tissue, require load in order to be activated to repair a damaged area effectively [43]. Complete unloading acts as a net inhibitor of connective tissue repair over the long term [43].
Pain Pathways Associated with Back Pain Following Spaceflight
Following spaceflight, astronauts have a protracted period of recovery that is necessary, even with the current inflight countermeasures in place. Modern rehabilitation programs for astronauts returning from a standard 6 month stay onboard the ISS involves 2 h of rehab a day, for 45–60 days after landing. Even with this deliberate reconditioning, joint issues can persist for astronauts for many months after landing, often exceeding the amount of time spent in space [44]. It has been well established that many of the postural muscles of the back, especially those supporting the lumbar area, show significant atrophy during prolonged unloading [13, 27, 28, 39, 45]. This atrophy can lead to poor spine biomechanics and cause new pathology or exacerbate existing pathology within the spinal column when re-exposed to the 1G environment of Earth. This could trigger pain from a simple muscle strain, as weaker muscles and poor mechanics attempt to cope with the load that has been absent for many months. A strained muscle might begin with the immediate pain transmitted by the muscle nociceptors sensitive to noxious (tissue-threatening) stretch. Following the initial pain signals generated by stretch receptors, chemo-sensitive nociceptors pick up chemical changes in the local tissue milieu such as pH or molecular signals like ATP spilled from damaged tissue continuing the perceived sensation of pain [46]. In addition, poor spine mechanics and weakened muscular support could result in a disc injury. An annular tear would first be sensed through both mechanoreceptors and chemoreceptors from the sinuvertebral nerve, which innervate only the outer third of the annulus fibrosis in a typical healthy IVD [47, 48]. More dramatic pathology, like a herniated nucleus pulposus, might not only be sensed at the outer third of the IVD but also could manifest as pain from compression as the displaced nucleus pulposus presses against a nerve root or against the cauda equina (Fig. 5.3).

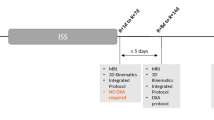
Mid-sagittal views of T2-weighted 3 T lumbar spine MRIs for all six subjects (taken at preflight). Example sites for injury and potential sources of pain are pointed out in additional T1-weighted sagittal images (a–c) from two of the subjects who presented postflight symptoms: (a) indent end plate defect indicated with a yellow asterisk at the cranial L4 end plate, (b) images of postflight (left) and 30 days recovery following postflight (right), demonstrating a posterolateral disc herniation indicated with a yellow arrow, (c) T1- (left) and T2-weighted (right) images demonstrated a type 2 Modic change with severe end plate defect (Modic change indicated with a yellow arrow and end plate defect indicated with a yellow asterisk). Reproduced with permission from Bailey et al. 2018
Risk Factors for Spine Injury or Pain
As mentioned by Pool-Goudzwaard et al., a history of back pain prior to prolonged unloading correlates highly with spaceflight adaptation back pain syndrome. This could be due to the previously mentioned changes in pain sense propagation that takes place in the chronic pain states, or as a result of prior pathology being exacerbated by the conditions of spaceflight. Additionally, there is likely a contribution of prior risk factors. As the person in question probably already had poor spine biomechanics (hence their previous injuries, or because of them) and these poor mechanics accompany them to space, including when they engage in exercise countermeasures which load the spine [41]. Of interest, there are still a substantial number of astronauts without a history of back pain that nevertheless experience SABP [5, 13]. This suggests that there is an independently developing pathology associated with the environment of spaceflight. In the setting of someone who has prior pathology, this may exacerbate it, or represent a separate pathology.
Inflight risk factors are less well understood, but certainly an acute injury while in flight, either during an exercise countermeasure or some other activity like a spacewalk, would likely predispose the astronaut to further back pain issues when coupled with the unloaded environment of microgravity. There is also the potentially tumultuous spacecraft landing to add to the picture, which can be rather violent and may exacerbate some existing or subclinical pathology.
Of note, the pathology that is associated with back pain and disc herniations upon return to Earth (or another gravitational environment) is likely different from the etiology of SABP. Regarding the increased risk of disc pathology, there is likely a component of disc dehydration and accelerated degeneration in microgravity as the regular diurnal pattern of loading the discs during the day and unloading at night that facilitates micro-circulation of nutrients is lost. In Fig. 5.4 we see that an astronaut’s spine MRI showed an IVD herniation at L4–5 prior to flight, though notably not symptomatic at the time. Immediately postflight shows that the herniation had reduced, but clear endplate pathology here is detectable with modic changes in L2–3 and L3–4 endplates. One month into the astronaut’s postflight recovery, they experienced symptoms consistent with lumbar radiculopathy and MRI imaging then showed a more dramatic herniation at the same site that had a prior asymptomatic herniation. While not enough data exists to make definitive predictions on risk factors like these, they can begin to inform decisions on not only countermeasures inflight, but also on directed rehabilitation programming upon return.

This sequence of lumbar MRI images of an astronaut preflight (left), immediately post 6-month flight (middle) and 1 month post-flight (right), shows a relevant progression of disc pathology at L4/5 (yellow arrows) and accompanying modic changes (orange arrows) in the L2,3,4 vertebral bodies
Associating Symptoms and Pathology Using Imaging
Spinal imaging is commonly used to assess any structural pathology underlying back pain symptoms. Imaging modalities used for spinal patients can include standard plain film X-rays and CT for evaluating the bony structures and ultrasound and MRI for evaluating soft tissue. More specialized nuclear imaging can give information about bone mineralization and density. Attaining high-quality imaging of the astronaut’s spine is essential to improving our understanding of the pathologies responsible for their pain or dysfunction. However, this effort is limited by the fact that they are aboard a spacecraft while much of the relevant physiologic changes are occurring, as well as the difficulty in getting imaging in a timely fashion after the astronauts have landed. Additionally, interpretation of pathology seen on imaging like MRI is often unrelated to the pain a patient (astronaut) might be having. This is a key maxim in clinical practice—that pathology apparent on imaging does not necessarily mean that it is the pain generator, as imaging findings are only weakly associated with related back pain symptoms, and rarely statistically predictive. In one cross-sectional study of asymptomatic patients over 60, when evaluating an MRI, 36% had disc herniations, 21% showed evidence of spinal stenosis, and over 90% had a degenerated or bulging disc [15]. Therefore, caution must be exercised when interpreting pathology on imaging, and it should be carefully correlated with the clinical presentation. To date, inflight imaging has been limited, due to the constraints of spaceflight, though occasionally astronauts have been able to get MRI very shortly after landing, when such imagining is given priority during landing recovery operations. Other available forms of inflight imaging have included ultrasound (US), which has been used to assess muscle cross-sectional area as well as changes to the IVD during flight [45, 49]. US, unlike the other imaging modalities, adds in a factor of operator-dependence for the quality of imaging obtained, which can further limit data collection.
Treatment Possibilities
Preflight Surveillance
It has been noted that astronauts with a previous history of chronic back pain were much more likely to experience back pain in space [5]. There may also be a correlation to spine issues in space and injuries later, like herniated nucleus pulposus upon returning to Earth.
Astronaut-Specific Inflight Exercise and Postflight Rehab
Given an astronaut’s experience with back pain, either prior history or inflight symptoms, an exercise program specifically tailored to address back pain would likely be beneficial. Taking the approach similar to terrestrial physical therapy, when a patient experiences back pain that affects their day-to-day activities, many benefit from a targeted exercise program to shorten the duration and severity of their symptoms. Likewise, if an astronaut is deemed to be higher risk for back injuries upon returning to gravity, a specific postflight rehab program could help to mitigate some of this risk is a more targeted fashion.
Inflight Spinal Assessment and Intervention
It has been noted, mostly anecdotally, that in addition to forward flexion (fetal tuck position) astronauts experience some relief from exercise or loading the spine [39]. It has also been noted that the cosmonauts of the Russian space program report a lower incidence of inflight backpain than their US counterparts. This may be due, in part, to the Russian space program’s utilization of the Pingvin (Penguin) exercise suit, which has elastic bands that provide axial load and tension from the feet up through the shoulders. Such compression and/or proprioceptive cuing that the suit provides may act as a protective factor in certain pathologies related to inflight back pain. Though specific data to this effect has not been collected, there are other avenues of inquiry looking at employing similar compression suits to help mitigate some of these effects.
Clinical Impact of Spine Health in Spaceflight
The pathologies discussed in this chapter reflect important health and operational considerations for the current state of spaceflight. However, it is essential to make the distinction that these same issues represent critical factors for future planned spaceflight. While SABP on the ISS is inconvenient, there have been other occasional inflight issues associated with spine health, notably a delayed spacewalk in 2021 due to cervical radicular symptoms in the astronaut schedule to walk. Fortunately, these issues did not threaten to end the mission or place the astronauts in serious peril. Conversely, spinal health-related problems represent mission critical and life-threatening issues with upcoming planned Artemis missions. Even more profound would be those missions aiming to place humans on Mars. These mission profiles would require the astronauts to experience microgravity for many months and then reenter a gravity loaded environment before returning to the safety of Earth. In contrast to microgravity living, the human spine is the indispensable central nexus of locomotion and limb force generation required for setting up critical mission infrastructure and exploring new terrain on the gravity environments of the Moon and Mars. Such transitions between microgravity and gravitational re-loading currently represent the largest risk for spine-health-related mission failures, as a herniated disc on the surface of Mars could mean a crew member taken entirely out of operational status. Even a significant back spasm during surface operations, caused by weakened muscular support after many months in microgravity, could result in significant danger for the crew and their mission. Because of this added risk of gravitational transition in the settling of an extremely remote and austere support environment, careful consideration and planning must go into mitigating spine-related health issues in future crewed mission design.
References
Wing P, Tsang I, Susak L, Gagnon F, Gagnon R, Tech D, et al. Back pain and spinal changes in microgravity. Orthop Clin N Am. 1991;22:255–62.
Thornton W, Hoffler GW, Rummel J. Anthropometric changes and fluid shifts. NASA SP-377; 1977.
Kerstman EL, Scheuring RA, Barnes MG, DeKorse TB, Saile LG. Space adaptation back pain: a retrospective study. Aviat Sp Environ Med. 2012;83(1):2–7.
Johnston SL, Campbell MR, Scheuring R, Feiveson AH. Risk of herniated nucleus pulposus among U.S. astronauts. Aviat Sp Environ Med. 2010;81(6):566–74.
Pool-Goudzwaard AL, Belavý DL, Hides JA, Richardson CA, Snijders CJ. Low back pain in microgravity and bed rest studies. Aerosp Med Hum Perform. 2015;86(6):541–7.
Putcha L, Berens KL, Marshburn TH, Ortega HJ, Billica RD. Pharmaceutical use by U.S. astronauts on space shuttle missions. Aviat Space Environ Med. 1999;70:705–8.
Putcha L. Pharmacotherapeutics in space. J Gravit Physiol [Internet] 1999 [cited 2021 Sep 23];6(1). Available from: https://pubmed.ncbi.nlm.nih.gov/11543005/
Belavý DL, Armbrecht G, Richardson CA, Felsenberg D, Hides JA. Muscle atrophy and changes in spinal morphology: is the lumbar spine vulnerable after prolonged bed-rest? Spine (Phila Pa 1976). 2011;36(2):137–45.
Tomaszewski KA, Saganiak K, Gładysz T, Walocha JA. The biology behind the human intervertebral disc and its endplates. Folia Morphologica (Poland). 2015;74:157–68.
Kim LH, Vail D, Azad TD, Bentley JP, Zhang Y, Ho AL, et al. Expenditures and health care utilization among adults with newly diagnosed lowback and lower extremity pain. JAMA Netw Open. 2019;2(5):e193676.
Murray CJL, Vos T, Lozano R, Naghavi M, Flaxman AD, Michaud C, et al. Disability-adjusted life years (DALYs) for 291 diseases and injuries in 21 regions, 1990-2010: a systematic analysis for the global burden of disease study 2010. Lancet. 2012;380(9859):2197–223.
Wu A, March L, Zheng X, Huang J, Wang X, Zhao J, et al. Global low back pain prevalence and years lived with disability from 1990 to 2017: estimates from the global burden of disease study 2017. Ann Transl Med. 2020;8(6):299.
Sayson JV, Hargens AR. Pathophysiology of low back pain during exposure to microgravity. Aviat Space Environ Med. 2008;79:365–73.
Hoy D, Brooks P, Blyth F, Buchbinder R. The epidemiology of low back pain. Vol. 24, Best Practice and Research: Clinical Rheumatology. Baillière Tindall; 2010. p. 769–81.
Allegri M, Montella S, Salici F, Valente A, Marchesini M, Compagnone C, et al. Mechanisms of low back pain: A guide for diagnosis and therapy [version 1; referees: 3 approved] Vol. 5, F1000Research. Faculty of 1000 Ltd; 2016.
Waddell G, editor. Illness behavior. In: the Backpain revolution. Edinburgh: Churchill Livingstone; 2000.
Barr KP, Concannon LG, Harrast MA. Low back pain. In: Braddom’s physical medicine and rehabilitation. 5th ed. Philadelphia: Elsevier, Inc.; 2016. p. 711–46.
McBroom RJ, Hayes WC, Edwards WT, Goldberg RP, White AA. Prediction of vertebral body compressive fracture using quantitative computed tomography - PubMed. J Bone Joint Surg Am. 1985;67(8):1206–14.
McMillan DW, Garbutt G, Adams MA. Effect of sustained loading on the water content of intervertebral discs: implications for disc metabolism. Ann Rheum Dis. 1996;55(12):880–7.
Jennings RT, Bagian JP. Musculoskeletal injury review in the U.S. space program. Aviat Space Environ Med. 1996;67(8):762–6.
Belavy DL, Adams M, Brisby H, Cagnie B, Danneels L, Fairbank J, et al. Disc herniations in astronauts: what causes them, and what does it tell us about herniation on earth? Eur Spine J. 2016;25(1):144–54.
Hutton WC, Malko JA, Fajman WA. Lumbar disc volume measured by MRI: effects of bed rest, horizontal exercise, and vertical loading. Aviat Sp Environ Med. 2003;74(1):73–8.
Leblanc AD, Wendt RE, Schneider VS, Hedrick TD. Changes in intervertebral disc cross-sectional area with bed rest and space flight. Spine (Phila Pa 1976). 1994;19(7):812–7.
Young KS, Rajulu S. Changes in seated height in microgravity. Appl Ergon. 2020;83:102995.
Belavý DL, Bansmann PM, Böhme G, Frings-Meuthen P, Heer M, Rittweger J, et al. Changes in intervertebral disc morphology persist 5 mo after 21-day bed rest. J Appl Physiol. 2011;111(5):1304–14.
Belavý DL, Armbrecht G, Felsenberg D. Incomplete recovery of lumbar intervertebral discs 2 years after 60-day bed rest. Spine (Phila Pa 1976). 2011;37(14):1245–51.
Bailey JF, Miller SL, Khieu K, O’Neill CW, Healey RM, Coughlin DG, et al. From the international space station to the clinic: how prolonged unloading may disrupt lumbar spine stability. Spine J. 2018;18(1):7–14.
Chang DG, Healey RM, Snyder AJ, Sayson JV, Macias BR, Coughlin DG, et al. Lumbar spine paraspinal muscle and intervertebral disc height changes in astronauts after long-duration spaceflight on the international Space Station. Spine (Phila Pa 1976). 2016;41(24):1917–24.
Bailey JF, Hargens AR, Cheng KK, Lotz JC. Effect of microgravity on the biomechanical properties of lumbar and caudal intervertebral discs in mice. J Biomech. 2014;47(12):2983–8.
Hides JA, Lambrecht G, Stanton WR, Damann V. Changes in multifidus and abdominal muscle size in response to microgravity: possible implications for low back pain research. Eur Spine J. 2016;25:175–82.
McNamara KP, Greene KA, Moore AM, Lenchik L, Weaver AA. Lumbopelvic muscle changes following long-duration spaceflight. Front Physiol. 2019;10.
Burkhart K, Allaire B, Bouxsein ML. Negative effects of long-duration spaceflight on Paraspinal muscle morphology. Spine (Phila Pa 1976). 2019;44(12):879–86.
White AA, Panjabi MM. Clinical biomechanics of the spine; 1990.
Tyrrell AR, Reilly T, Troup JDG. Circadian variation in stature and the effects of spinal loading. Spine (Phila Pa 1976). 1985;10(2):161–4.
Thornton WE. NASA-TM-58280: height changes in microgravity - results of the life sciences DSOs conducted aboard the space shuttle 1981–1988. National Aeronautics and Space Administration; 1987.
Hutchinson KJ, Watenpaugh DE, Murthy G, Convertino VA, Hargens AR. Back pain during 6 deg head-down tilt approximates that during actual microgravity. Aviat Space Environ Med. 1995;66:256–9.
Bailey JF, Nyayapati P, Johnson GTA, Dziesinski L, Scheffler AW, Crawford R, et al. Biomechanical changes in the lumbar spine following spaceflight and factors associated with postspaceflight disc herniation. Spine J. 2021;22:197–206.
Mulavara AP, Peters BT, Miller CA, Kofman IS, Reschke MF, Taylor LC, et al. Physiological and functional alterations after spaceflight and bed rest. Med Sci Sports Exerc. 2018;50(9):1961–80.
Sayson JV, Lotz J, Parazynski S, Hargens AR. Back pain in space and post-flight spine injury: mechanisms and countermeasure development. Acta Astronaut. 2013;86:24–38.
Grunhagen T, Wilde G, Mokhbi Soukane D, Shirazi-Adl SA, Urban JPG. Nutrient supply and intervertebral disc metabolism Aboulfazl Shirazi-Adl Polytechnique Montréal. Artic J Bone Jt Surg. 2006;88:30–6.
Green DA, Scott JPR. Spinal health during unloading and reloading associated with spaceflight. Vol. 8, Frontiers in physiology. Frontiers Media S.A.; 2018. p. 1126.
Scheuring RA, Mathers CH, Jones JA, Wear ML. Musculoskeletal injuries and minor trauma in space: incidence and injury mechanisms in U.S. astronauts. Aviat Sp Environ Med. 2009;80(2):117–24.
Salter DM. Connective tissue response to mechanical stress. In: Rheumatology, Vol 1, 6th Edition; 2015. p. 61–4.
Williams D, Kuipers A, Mukai C, Thirsk R. Acclimation during space flight: effects on human physiology. Vol. 180, CMAJ; 2009. p. 1317–23.
Harrison MF, Garcia KM, Sargsyan AE, Ebert D, Riascos-Castaneda RF, Dulchavsky SA. Preflight, in-flight, and postflight imaging of the cervical and lumbar spine in astronauts. Aerosp Med Hum Perform. 2018;89(1):32–40.
Schaible H. Joint pain: basic mechanisms. In: Textbook of pain; 2013. p. 609–19.
Shayota B, Wong TL, Fru D, David G, Iwanaga J, Loukas M, et al. A comprehensive review of the sinuvertebral nerve with clinical applications. Anatomy Cell Biol Korean Assoc Anatomists. 2019;52:128–33.
García-Cosamalón J, del Valle ME, Calavia MG, García-Suárez O, López-Muñiz A, Otero J, et al. Intervertebral disc, sensory nerves and neurotrophins: who is who in discogenic pain? J Anat. 2010;217:1–15.
Garcia KM, Harrison MF, Sargsyan AE, Ebert D, Dulchavsky SA. Real-time ultrasound assessment of astronaut spinal anatomy and disorders on the international Space Station. J Ultrasound Med. 2018;37(4):987–99.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2022 The Author(s), under exclusive license to Springer Nature Switzerland AG
About this chapter

Cite this chapter
Brane, L., Bailey, J.F. (2022). Spine Biomechanics and Pathology. In: Michael, A.P., Otto, C., Reschke, M.F., Hargens, A.R. (eds) Spaceflight and the Central Nervous System. Springer, Cham. https://doi.org/10.1007/978-3-031-18440-6_5
Download citation
DOI: https://doi.org/10.1007/978-3-031-18440-6_5
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-031-18439-0
Online ISBN: 978-3-031-18440-6
eBook Packages: MedicineMedicine (R0)