
Abstract
As large, heavy, abundant, living parts of the terrestrial environment, trees are so widely distributed and useful to humans that direct interactions between people and trees are common all over the world. Trees are regularly sawed, felled, harvested, and climbed by people, and people are occasionally struck by falling trees, branches, or fruits. This chapter reviews human fatalities in the context of these events, most of which are due to accidental blunt force traumatic injuries. The circumstances, epidemiology, injuries, autopsy findings, and investigative considerations of these cases are discussed.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
Introduction
As large, heavy, abundant, living parts of the terrestrial environment, trees are so widely distributed and useful to humans that direct interactions between people and trees are common all over the world. Trees are regularly sawed, felled, harvested, and climbed by people, and people are occasionally struck by falling trees, branches, or fruits. This chapter reviews human fatalities in the context of these events, most of which are due to accidental blunt force traumatic injuries. The circumstances, epidemiology, injuries, autopsy findings, and investigative considerations of these cases are discussed.
What is a “Tree-Related” Death?
This chapter will cover:
-
Fatalities resulting from a person physically altering a tree, for purposes of harvesting, landscaping, etc.
-
Fatal descents from height, whether the decedent fell directly from a tree or from an elevated position while working on a tree.
-
Other deaths where the presence of a tree is fundamental or central to an activity, such as deaths associated with tree stands used for hunting.
-
Fatalities due to falling trees or tree parts (“tree failures”), including deaths in motor vehicles struck by a fallen tree and in vehicles that struck trees which had fallen onto a roadway.
This chapter will not cover:
-
Suicidal hangings on trees—The tree may be an available means of suspension, but the characteristics of these deaths relate more to the hanging method and suicidal nature.
-
Motor vehicle collision fatalities in which the vehicle veered off a roadway before happening to collide with a tree.
-
Other deaths where the presence of a tree is best classified as incidental.
-
Sawmill fatalities—At this juncture, the raw material is best considered lumber/timber as opposed to a tree.
-
Other deaths involving products derived from trees, but not the perennial woody plant as such. In other words, once a tree is successfully harvested, it is no longer considered a tree and deaths associated with the processing or consumption of products sourced from trees will not be discussed.
Background—The Case of Lucy
One of the most ancient and famous human ancestors likely died while interacting with a tree. The fossilized skeletal remains of A.L. 288-1, better known as “Lucy,” were studied by researchers at The University of Texas at Austin, who examined both the original specimen as well as computed tomographic scans of the skeleton to assess for a possible cause of death for the 3.2-million-year-old adult member of Australopithecus afarensis. This research was undertaken in a particular context: the discovery of Lucy in 1974 in the Afar Depression of what is now Ethiopia sparked a vigorous and ongoing debate about whether this erect-walking species—a capable terrestrial biped—spent time in trees. This question is important to the field of paleoanthropology as it relates to the role of arboreal locomotion in hominin evolution.
Lucy is approximately 40% of a complete skeleton, and analyzing these available elements the researchers described a set of likely perimortem fractures present in a pattern consistent with trauma produced by a vertical deceleration event. This included a four-part fracture of the proximal right humerus, an injury commonly seen when someone stretches out their arm while attempting to break a fall or descent from height. The left humerus was also fractured, and while infrequent, bilateral compressive proximal humerus fractures are usually associated with high-energy trauma from impact on outstretched arms. There were multiple additional fractures in Lucy’s skeleton involving the distal shaft of the right radius, left femur, right tibia and fibula, right talus, cranium, bilateral ribs, and pelvis.
The findings were published in a 2016 article in the scientific journal Nature and the authors concluded that Lucy’s most likely cause of death was blunt trauma from falling out of a tall tree [1]. To support the inference that tall trees would have been part of Lucy’s environment and accessible to her, the authors cite lines of evidence from the fossil record and dating of paleosol carbonates suggesting the region where Lucy was found would have been a grassy woodland with sizable trees. Like many other small primates, Lucy may have foraged in trees or sheltered in them at night. Chimpanzees, similar in body size to the extinct Australopithecus afarensis, have been documented sleeping in tree nests at heights equating to a 16-storey building (50 m), and the search for food and provisions can occur at even greater heights. Unimpeded falls with impact from such heights produce a wide range of concomitant fractures in humans similar to those found in Lucy and often cause fatal damage when vital internal organs are violently compressed and/or penetrated by broken bones. Taken together with the paleohabitat information and resemblance with known clinical cases in humans, the authors propose the overall pattern of fractures—considering specific anatomic locations and fracture types—suggests Lucy fell from of a tree of considerable height and impact progressed sequentially from feet and legs to the hip, then arms, then thorax and head, causing injuries likely to be rapidly lethal.
This vignette is to say that as long as humans have existed, trees have been prominent features of our natural environment and our culture, simultaneously a way of survival and a figure of demise. As we have found more uses for trees, the range and frequency of our interactions with them have grown. It is the editor’s and my opinion that tree-related activities, with the injuries and deaths that may be associated with them, are a subject receiving little attention to date within forensic and autopsy textbooks. This chapter is written in the hopes of covering this topic for an international readership.
Deaths in Logging, Forestry, Tree Care Operations, and Recreational Tree Care
Cutting, pruning, sawing, lopping, trimming, felling, removing, or any version of physically altering a tree is an inherently dangerous thing for a person to do. Several occupations have these activities as integral parts of the job description:
-
Logging—Harvesting trees as a raw material.
-
Forestry worker—May refer to a logger or someone who creates and maintains forests [2].
-
Tree felling—Making an entire tree fall down.
-
Tree lopping—Cutting a branch, limb, or other protrusion off the main trunk of a tree.
-
Landscaper, arborist, or amenity tree service worker—Professional involved in tree removal, maintenance, or other tree care operations (Fig. 8.1) [3].
Fig. 8.1 
Example of urban tree care operations in New Haven, Connecticut, U.S. a Worker removing tree limb segments with a chainsaw while elevated via boom lift bucket truck. b Aerial work platform at height of about 20 m. c Worker carrying cut segments to a woodchipper

These occupations are notorious for unusually high exposure to hazards with resulting high rates of fatalities and severe injuries [4]. Although labor statistics vary by time period, region, and methodology, it is generally accurate to say that logging and forestry workers have continually experienced one of the highest fatality rates all over the world for decades, at over 100 deaths per 100,000 person-years, more than 10 times the all-industry average and 2–3 times higher than other notably dangerous sectors like construction and mining/quarrying [2,3,4,5,6,7,8]. Similar observations have been made in multiple studies spanning Australia, Canada, New Zealand, Russia, Sweden and the Nordic countries, and the United States (U.S.), underscoring the universality of these hazards. The fatality risk for logging is extremely high, even greater than that for commercial fishing [2].
Recreational tree care—“non-occupational” or so-called “do-it-yourself” projects—involves similar hazards, but in the amateur setting. Non-professionals commonly undertake these tasks for reasons including aesthetics, removal of a dead or rotten tree, firewood collection, physical fitness, pride and satisfaction in completing home maintenance, and self-sufficiency; older and retired persons are overrepresented in these accidents, and they have also reported limited ability to afford the specialized labor costs as a factor in choosing to do the work themselves [3, 9]. Since there is substantial overlap in the characteristics of professional and recreational cases, they will be discussed together unless otherwise specifically noted.
One difference is in demographics, where the average age of professionals suffering fatal injury is about 20 years younger than non-professionals (40 years vs. 60 years, respectively) [2, 3, 8, 10]. However, whether occupational or non-occupational, these deaths overwhelmingly occur to males, who have to date comprised 90–100% (usually closer to 100%) of tree cutting-related fatalities in every country they have been investigated [2, 3, 5, 7, 8, 10].
Hazards
The preeminent hazard in working with trees is the unintended release of large amounts of kinetic energy, which takes several forms. Hardwood trees can be 25 m tall and weigh in excess of 10 metric tons, with individual limbs weighing 450 kg or more, and portions of a tree may be under immense gravitational stress [4]. Some parts may be weakened by decay or otherwise unstable in unpredictable ways. Sawing, cutting, or hammering wedges into a tree can release this stored energy directly, or manifest as falling objects. When felling, a tree's trunk can suddenly and violently split vertically into two or more pieces as the forces shift and internal pressure is sent up the stem (colloquially called “barberchairing,” a reference to the sliding action of the old-style barber chair), creating potentially massive and horizontally fast-moving tree fragments as well as haphazardly falling fragments from above (Fig. 8.2). Most fatalities result from being struck by moving trees or branches (about 60–75% of deaths) [2,3,4, 6, 8, 10], and quite often these are not from the tree being felled, but rather originate from a second nearby tree which is disturbed by the felling of the intended tree [2, 4, 10]. Falling trees can knock the branches off neighboring trees and connecting vines can pull branches in the same canopy down upon the worker. Since the questions of when, where, and how a tree will fall are so multifactorial, predicting the fall trajectory is difficult and planning for all contingencies takes great expertise. Experienced loggers are aware of these dangers and know very well that any error in judgement can carry lethal consequences.

Recreational tree felling accident. a The decedent’s frozen body was discovered in his wooded backyard, with adjacent sawed and fragmented tree trunk and chainsaw. b Scene likely depicting “barberchair”-type incident, where the trunk splits vertically as the tree falls, generating great lateral force when it suddenly snaps (instead of hinging at the base, the hinge point is higher up on the tree when it tilts and falls). c Left-sided depressed skull fracture, which upon further examination was associated with bilateral fractures of the skull base, subdural and subarachnoid hemorrhage, and intraventricular hemorrhage
Apart from splintering tree fragments and falling tree limbs, other hazards include uneven terrain, extremes of weather, working at elevated heights, contact with overhead power lines, chainsaws and other sharp instruments, working with woodchippers and heavy mechanical equipment, and isolated environments (Fig. 8.1).
Injuries
Regarding type and distribution of injuries in these deaths, the head is the most frequent primary and lethal impact site (40–60% of cases), usually when it is struck by moving/falling tree parts [2,3,4, 8, 10]. It is common for the decedent to have been wearing a helmet at the time of the accident; helmets may be broken or completely shattered as they can fail under the tremendous impact forces seen in many events [2]. Investigation should document the presence and condition of any helmet involved in these fatalities. Skull fractures with associated lacerations of the brain are often encountered at autopsy, as are subdural, subarachnoid, and intraventricular hemorrhages. Atlanto-occipital dislocation and cervical spine trauma may also result.
After isolated head/neck injuries, lethal thoracic or abdominal trauma is the next most common body site (about 20–30% of cases) (Fig. 8.3), followed by severe combined multisite trauma (10–20%) [8, 10].

Severe blunt trauma of the torso sustained when a tree fell onto a non-professional tree cutter, including: extensive bilateral rib fractures; T5/T6 and L1 vertebral fractures; and lacerations of the heart, aorta, liver, and spleen associated with marked hemothorax and hemoperitoneum (not pictured)
About 10% of deaths are due to traumatic compression asphyxia, usually when the worker’s chest is crushed and/or pinned by tree limbs [2, 3, 8]. Autopsy findings to support traumatic asphyxia may include cutaneous or mucosal petechiae, generalized visceral congestion, and pulmonary edema.
Descent from Height
Descent from height is another distinct event leading to fatal injury. Incidence is somewhat variable in the literature, but it appears there is a significant risk difference based on labor type. While industrial loggers typically cut a tree down from the base, landscapers and urban tree professionals will start at the top and delimb sections until there is nothing left but the stump (Fig. 8.4), and consequently falls from elevation mostly occur in landscaping-type tasks [4]. These events account for something between 5–35% of overall deaths depending on the labor activity being measured, and can include descents from the tree itself, ladders, or the aerial work platform of a boom lift bucket truck [2,3,4,5, 8]. One case involved a landscaper who fell out of a tree while trimming branches with ensuing 9 m descent, resulting in skull fracture, subdural hemorrhage, brain contusion, rib fractures, lung contusion, T12 vertebral fracture with spinal cord transection, and sacro-iliac dislocation. (See “Overview of Injuries in Descent from Height Fatalities”—for more discussion of this topic). It is occasionally difficult to determine the primary reason for fatal injury when there are combined elements of moving tree/branch-inflicted trauma and descent from height injuries [8].

Landscaping fatality. a The decedent was felling a tree by delimbing the trunk from top to bottom in large segments, and his body was discovered suspended by the waist high on the tree. b Blunt impact by the cut segment resulted in multiple lethal injuries in this case, including a classic type I hinge fracture of skull (pictured), brainstem injury, atlanto-occipital dislocation, and aortic laceration
Electrocution
Although rare, electrocution deaths are dramatic and more likely to represent fatalities in which a serious workplace safety violation or egregious error in judgement was committed. Alternatively, they may occur in the context of clearing tree debris near damaged power lines in close temporal proximity to storms, reflecting particularly hazard-laden work conditions. Contact with electric current accounts for about 5–10% of fatalities, often from chainsaw or bodily contact with a power line [3, 5, 8]. Thermal electrical burns should be documented if present in a case where electrocution caused or contributed to death.
Chainsaws
Also rare, perhaps surprisingly, is fatal direct chainsaw trauma. Many studies in countries all over the world have shown that while a common source of non-lethal injuries, chainsaw or circular saw accidents seldom result in death, accounting for less than 5% of cases [2, 3, 6, 8, 10]. Engineering safety controls in chainsaw design and effective personal protective gear may explain this non-lethality to some degree [6]. The most common reason for accidental contact with the chainsaw's blades, and the most dangerous, is “kickback”—sudden uncontrolled backwards jerking toward the operator when the chain abruptly stops as a link encounters more solid wood [11]. A fatal case usually involves chainsaw kickback causing lethal injury to the neck region (Fig. 8.5) [12].

Chainsaw accident. a The decedent was cutting a log when a “kickback”-type chainsaw incident occurred, creating a traumatic open wound of the left neck and chest with massive blood loss, causing him to stagger about 4 m before collapsing. b The wound extended through skin, soft tissue and muscle, with partial transection of the left carotid artery (pictured) and unidentifiable internal jugular vein
There are a couple reports of more unusual chainsaw accidents in the literature. One teenage forestry worker fell upon his chainsaw, with the autopsy report stating death was due to extensive disruption of the brain associated with markedly comminuted skull fracture [13]. Another paper details the case of an 80-year-old farmer who was engaged in felling a tree [14]. His chainsaw was found jammed in the tree, with the chain broken but still in place. A single bloody wound of the mid-anterior chest was present, a penetrating wound described as having one sharp end and one blunt end, with greater depth than length, mimicking a stab wound. It penetrated the aortic arch causing a 1,500 mL left hemothorax. Examination of the chainsaw revealed a missing chain link, and a pelvic radiograph obtained at autopsy revealed a metallic foreign body near the head of the right femur. Dissection uncovered a broken chain link measuring 1.7 cm in greatest dimension within the right femoral artery that matched the missing link of the chainsaw in question. This chainsaw link embolization changed certification of both the cause and manner of death, as without this finding the death could have easily been determined to be due to a penetrating stab wound of the chest of probable homicidal origin.
Logs/Trunks
If the worker is involved in loading or unloading a log truck, large piles of logs are a well-known hazard and fatalities may occur when workers are struck by rolling logs causing massive blunt trauma [2, 15].
One case was a boom-claw tree trunk removal mishap. The decedent was working on a two-person crew for a tree removal company, using a boom truck with a giant claw to move large limbs and trunks. He was on the ground while the boom operator was lifting a trunk. The claw lost grip, the trunk fell, and the worker was inappropriately positioned underneath the clear hazard. He was crushed by the falling trunk with lethal blunt injuries of the head and torso.
Drugs/Alcohol
Impairment from drugs or alcohol is not a common factor in these fatalities [8, 10], but rates of alcohol intoxication in fatal occupational injury do appear to be higher in forestry compared to other sectors and the degree of alcohol intoxication has been found to be directly correlated to risk of fatality [7]. Alcohol has been implicated in both recreational and professional tree cutter fatalities. Some notable cases include a 36-year-old who felled a large tree onto his own head while pulling it by a wire with a tractor (0.19 gm% ethanol concentration) and a 32-year-old trimming branches while elevated via boom truck whose chainsaw made contact with a power line, electrocuting him and causing him to fall about 6 m to the ground (0.09 gm% ethanol concentration in addition to positive postmortem tests for benzoylecgonine and oxycodone) [8].
Working in Isolation
Non-occupational deaths usually happen when the person is working alone, with only about 20% of these events being witnessed. In contrast, professionals are rarely alone, but may be outside visual contact with coworkers when the incident occurs [5, 8]. In most cases death occurs at the place of injury before any medical assistance is given, but a minority involve injuries likely survivable if timely treatment is administered; in some of these fatalities, delay in treatment due to worksite remoteness and/or working alone has been identified as a probable contributing factor to the death [2, 10].
Bystander Deaths
Quite often the person who dies is not the person actively cutting, but instead a fellow worker or bystander who is struck by the falling tree or tree parts. Laborers and onlookers have died when they were:
-
Working under the influence of alcohol (0.04 gm% ethanol concentration) on the ground when a coworker in the tree above cut a large branch which fell and crushed him [8].
-
Struck by a felled tree while driving past in a vehicle [3].
-
A child watching from the seat of a nearby tractor whose father misjudged the fall angle, leading to a dead tree falling directly on top of the child [8].
-
Walking down a long driveway adjacent an urban tree care operation when professionals cut a large branch at the exact moment he was underneath [8].
Human Factors and Prevention
Investigations have suggested the main human factors contributing to fatal accidents are misjudgment of a hazardous situation, failure to preplan an escape route when felling, and improper felling techniques [2, 4, 10].
For prevention of serious injury and death, there is a particularly useful document published by WorkSafe Victoria of the government of Victoria, Australia, which outlines safety measures to mitigate many of the hazards discussed here including overhead powerlines, working at height, chainsaws, falling objects, and more (https://www.worksafe.vic.gov.au/resources/working-safely-trees) [16]. Since the most dangerous activity is felling an entire tree, safety ought to be especially stressed for these workers. Any measure that puts more physical distance between the worker and the tree being felled will improve safety, such as mechanized logging methods that decrease the need for chainsaws [4]. Widespread fatalities from falling trees and tree parts imply those in felling operations should be taught to “look up” and consider hazards from above [4]. It has also been suggested that ideally, non-professionals should not participate in tree felling [10]. This may also extend to “non-timber workers,” those employed outside a relevant tree profession who nevertheless participate in these activities while often considered insufficiently qualified or experienced to do so. These workers, often employed in farming, construction, utilities or general labor, comprise at least one quarter of tree care or landscaping-type work fatalities [3, 5].
Death from Tree Failures
Unlike deaths while purposefully interacting with a tree, fatalities due to accidental impact by falling trees or branches during a storm or from “spontaneous” failures appear to be more “act of God”–type events. A simple web query using a search engine demonstrates how easy it is to find news reports of people killed by falling trees, seemingly at random or inexplicably, from a 55-m-tall redwood in the western U.S. collapsing in unremarkable weather to a tree uprooted by high winds falling on a moving car in Tasmania. Images of horizontal trees, crushed vehicles, obstructed roadways, and damaged houses are visually dramatic and readily shared via electronic media. A study in Australia has provided evidence of just how newsworthy journalists consider these deaths, as the researchers’ database showed that since the beginning of the twenty-first century the media reported almost all, if not all fatalities from tree failures in that country [17].
Of course, trees and branches fail for an underlying reason, even if the reasons are not entirely discernible. Inclement weather conditions such as storms and high winds are without question the most significant identifiable factor in tree failures, accounting for up to 90% of fatal incidents [17]. The risk of being killed or seriously injured is greatest during or immediately after a severe weather event, as even healthy and structurally sound trees can be broken or felled by strong winds or water/ice accumulations [18]. So-called “widow-makers” are broken-off tree limbs initially trapped at high levels, only to fall to the ground later. Therefore some “spontaneous” failures represent a delayed consequence of storm-induced damage. This makes cleaning up debris during or after a storm in a wooded area a hazardous activity. Drought, fire, and insect infestations also render trees more susceptible to failure, and weakened or dead trees can cause fatalities in the absence of severe weather [8, 18].
The specifics of disease data collection such as broad categories that subsume all deaths and injuries related to falling objects of many types, not just trees and branches, mean most if not all governments worldwide cannot simply analyze accidental tree failures. Epidemiologic and other data rely on targeted, time-intensive research projects. The available studies suggest death from these incidents is very rare [19], and that if you live in Australia, mortality from accidental tree failure is 250 times less likely than death from driving in a vehicle [17]. From years 1995–2007 in the U.S., there were about 30 deaths per year from wind-related tree failure in a country with about 280,000,000 population, equating to a little less than one death for every 10,000,000 people [18].
Depending on the country and region, the most common scenario is either tree strike while in a moving vehicle (U.S. and United Kingdom) or while engaged in outdoor activities (Australia) [17, 18, 20], a difference possibly explained by the climate and lifestyle of the region. In certain places such as the New England region of the U.S., it is not necessarily uncommon to see motor vehicle incidents involving trees falling onto the travel portion of a roadway (Fig. 8.6) [8]. Other settings include tents and, exceedingly rarely, death by tree failure while cycling. Perhaps surprisingly, Schmidlin reported about 20% of wind-related events in the U.S. were deaths while the person was inside their house, with half being mobile homes and half frame houses [18].

Examples of tree failures involving trees falling onto roadways, all causing fatal accidents in motor vehicles. a A tree which fell due to high winds, landing on the roof of a moving mail delivery truck, crushing the cabin and entrapping the driver, ultimately resulting in death due to chest compression with traumatic asphyxia. b Large oak tree which failed during torrential rain and high winds, landing upon and crushing a sport utility vehicle c. Fragment of a large tree with attached fragment of a school bus, which broke off the main trunk when failing for unclear reasons, striking the bus on the driver's compartment; the bus then coasted off the roadway before striking a utility pole
To my awareness, only one published study has described injuries and autopsy findings in tree failure deaths [8]. The lethal injury site is a roughly even mix of head trauma, severe combined multisite trauma, torso injuries, and even isolated neck injuries. Two deaths were due to atlanto-occipital dislocation, an injury involving the ligaments and/or bony structures connecting the skull to the cervical spine which leads to secondary brainstem and upper cervical spinal cord damage (Fig. 8.7); atlanto-occipital dislocation is also a common cervical spine injury in motor vehicle collision fatalities [21]. Another case was that of a driver navigating a rural road in high winds when a 55 cm long tree limb smashed through the windshield, penetrating the right side of the neck and exiting on the left upper back, causing a C7 vertebral fracture as well as a severed right external jugular vein (Fig. 8.8) [8]. This case highlights how vehicles may not be able to withstand these forces, as even a falling 55 cm branch can shatter a windshield and still possess sufficient energy to perforate the total anteroposterior depth of an adult neck/thorax.

Death due to atlanto-occipital dislocation. a Heavy rain and wind uprooted a 15-m-long tree, which fell on a parked vehicle. b At autopsy, this decedent had minimal head injury, and cause of death was attributable to isolated atlanto-occipital joint dislocation

Lethal penetrating blunt force trauma due to a falling branch. a The decedent was driving in windy conditions when a 55-cm-long tree limb smashed through the windshield and pierced the right side of her neck, exiting at the left upper back. b The wound after removal of the branch, where examination revealed a C7 vertebral fracture and severed vasculature including the right external jugular vein
The pruning and removal of trees discussed in the previous section are often performed at least partly to reduce risk of accidental tree failure [17]. Tree risk assessment and management programs have been suggested, especially for parks and along roadways [18]. However, given the hazards of physically altering a tree combined with the very low frequency of injuries to persons not interacting with trees, it has also been proposed that pushing over or cutting down trees is obviously more dangerous than leaving them alone, limiting the benefit of these programs [19]. In severe storms and high winds shelter ought to be sought in sturdy buildings and, if outdoors, openings are much safer than sheltering under trees (coincidentally, this is also valuable advice to avoid being killed by lightning if the inclement weather happens to be a thunderstorm) [17, 18].
Overview of Injuries in Descent from Height Fatalities
Before further discussion in particular tree-related contexts, there are general concepts in fatal descents from height worth summarizing.
Injuries sustained in falls from height are a distinct form of blunt trauma. Most cases in developed areas are accidental or suicidal falls from buildings, bridges, construction sites, or ladders. For purposes of this section, falls onto solid impact surfaces will be considered, as opposed to descending into water. There are two broad injury categories [22]:
-
Direct impact injuries—Damage caused by direct contact between tissue and impact surface. These are predominantly fractures.
-
Deceleration type injuries—Occur when tissue is forcefully displaced upon motion arrest during impact. These are predominantly internal organ lacerations, including large vessels. Another important indirect-type injury is cervical spine hyperflexion or hyperextension.
Factors influencing the distribution and severity of injuries in descents from height include [23,24,25,26]:
-
Fall height—Directly relates to velocity at impact.
-
Orientation of the body at impact.
-
Composition of the impact surface—Relates to duration of impact. Surfaces such as rocks or concrete allow minimal deformation which decreases impact duration, thus increasing force and injury severity. To the contrary, soil or snow are more deformable, resulting in decreased injury risk [27].
-
Secondary impacts with other objects.
-
The individual’s age and body mass.
-
The individual’s psychological/neurological state—May affect body tone or behavioral response to the fall. Examples include drug or alcohol intoxication.
Of these, the height of the fall is a major contributor to the pattern and extent of injuries in fatal descents, for both direct and deceleration type injuries [24,25,26, 28,29,30]. At lower fall heights, lethality is more closely linked to the body orientation at impact such that head/neck injuries are the typical cause of death and may even be the sole significant injury. As fall height increases, injuries increase, and polytrauma with multiple fatal injuries predominates. One autopsy study found that about 30% of fall deaths from less than 10 m showed multiple lethal injuries, while this figure increased to 90% when fall height was greater than 30 m [24]. Although the frequency of head fractures does not appear to be significantly correlated with descent height, the greater magnitude of impact from higher falls results in more comminuted skull fractures. Injury to the rest of the body is more dependent on fall height than the head/neck region; the frequency and extent of fractures to the thorax, pelvis, and extremities all increase, and with additional fractures come adjacent tissue damage, particularly lung lacerations accompanying multiple bilateral rib fractures. Deceleration injuries are directly proportional to fall height, and some cases are marked by death due to a single organ laceration with internal bleeding.
The head is the most commonly injured site and often traumatized regardless of fall height or even site of primary impact in cases presenting to autopsy. In one series, more than half of decedents who had been known to land on their feet had evidence of brain damage due to secondary impact of the head [29]. Direct impact is usually to the frontal and parietal regions with associated cranial lacerations and hematomas [31]. Subdural and subarachnoid hemorrhages are frequent, and it is common to see a combination of skull base and cranial vault fracture [30]. In feet- or buttocks-first impact, force transmitted upward through the pelvis and spine may cause a classic pattern ring fracture of the skull base [26, 29]. Those who land head-first tend not to reach medical care alive. Craniocerebral trauma is also more common in children because their center of gravity is more superior due to larger head: body size ratio [30].
The neck is an important anatomic region in these autopsies, for a couple specific reasons:
-
Cervical hyperextension injuries—Falls with primary impact on the face or forehead can cause cervical vertebrae injury due to neck hyperextension. Osawa and colleagues describe 14 cases of isolated cervical hyperextension as a cause of death in falls of low height [32]. All decedents had abrasions and bruises of the upper part of the face at autopsy, but there were often no other external injuries. Internal examination revealed linear tears of the anterior longitudinal ligament in the cervical vertebra with associated hemorrhage into prevertebral fascia in all 14 cases. 12 decedents had inter-vertebral disc space disruptions at the ligament tear site characterized by dislocated small bone fragments, evident upon sectioning the cervical vertebral column. An anterior-inferior corner fracture of the vertebral body may also be present behind the anterior longitudinal ligament tear, typically appearing as a thin avulsed bone fragment. The lower cervical vertebrae tend to be affected, with disc disruptions and bone fractures usually located between C4 and C7. Sectioning the spinal cord usually reveals gross evidence of trauma in the form of a linear or round central cord hemorrhage, although this is not always present. Histopathologic examination in a subset of these cases demonstrated, based on microscopic findings of edema and macrophage invasion in the cord, that some decedents may have survived for several hours after the accident before death occurred.
-
Laryngohyoid fractures—Important from a forensic perspective, laryngohyoid fractures have been discovered in about 10% of autopsied non-homicidal falls from height, with incidence of hyoid bone fracture corresponding to increasing fall height and thyroid cartilage fracture increasing with decedent age [33]. Hyoid and thyroid cartilage fractures are also seen accompanying cervical spine fractures in these cases. It is also possible to have cervical soft tissue/muscle hemorrhage or bruising without laryngohyoid fracture [34]. The predominant mechanism is probably indirect fracture secondary to cervical hyperflexion or hyperextension, or mandible or cervical vertebral fractures. One study found that these particular neck injuries were limited to fall heights of more than 10 m, and were not present in autopsied cases of falls from less than 10 m [26]. Therefore, although these findings normally direct the pathologist's thoughts toward homicide, in these instances they do not in isolation suggest strangulation prior to the descent.
Spinal injury is common. Feet- or buttock-first impacts can cause axial loading, transmitting force upward through the spine, resulting in compression or burst fractures of the vertebrae. Spinal cord injury is associated more strongly with thoracic vertebrae fractures as the spinal canal has a relatively small diameter in this region [22].
The sternum can be broken by either direct impact or, interestingly, by the decedent’s own mandible secondary to extremely forceful hyperflexion of the neck [22]. Sternal fractures are strongly associated with myocardial contusion.
For visceral injuries, aortic laceration is a classic autopsy finding in descents from height, and damage to the aorta or heart may be due to deceleration injury, compression between skeletal components of the thorax, or penetration by fractured bone ends [26, 29]. The liver appears to be the most vulnerable abdominal organ.
Pelvic fractures are often associated with life-threatening hemorrhage and may be caused by direct impact or force transmitted through the femur across the hip joint. The latter is seen when primary impact is on the feet or knees [35]. A great amount of force is required to disrupt the strong junctures of the posterior pelvic ring, so fractures of the posterior aspect are more indicative of high falls [25].
Finally, while landing on both feet is more common in intentional jumpers committing suicide, it may also occur in accidental falls [22, 25]. Primary impact onto both feet has some specific findings like calcaneus fracture and fracture of bilateral lower extremities. While open fractures of the soles of the feet or splitting of the bilateral heels has been described as a classic or even pathognomonic pattern, this external examination finding is present in less than 20% of cases where a feet-first landing is known [26, 29]. Overall, because so many factors potentially influence the injury distribution, attempting to reconstruct the circumstances of death based on autopsy findings alone is not advised [36]. Fortunately, it does not appear that suicidal descent from height involving a tree has been reported, and only deaths due to accidental falls from trees are known.
Tree-Related Deaths and Injuries in Melanesia and Tropical Regions
Tropical regions of Earth, located near the Equator between the Tropic of Cancer and the Tropic of Capricorn, are characterized by latitudes at which the Sun can be directly overhead. Land in these areas receives more direct sunlight, and the tropics are on average warmer with more precipitation compared to other climates. Tropical plant life is particularly biodiverse and includes a number of culturally and economically important fruit-bearing trees, some of which grow to considerable heights with the fruit located high in the crown of the tree.
Tropical regions are home to a large and actively increasing percentage of the world’s population. As an illustration, there are 400 million people who live on just nine tropical islands—Sumatra, Java, Sulawesi, Luzon, Mindanao, Borneo, Hispaniola, Sri Lanka, and New Guinea. The encompassed countries are essentially all of low- or middle-income, where injuries represent a neglected problem in global public health; greater than 90% of deaths and 94% of disability-adjusted life years from injuries worldwide occur in low- and middle-income countries [37]. High population growth rates accompany progress in economic development and public infrastructure in most areas. Still, many individuals and families rely on subsistence agriculture. For example, as of year 2016, an estimated 85% of the Solomon Islands population are subsistence farmers reportedly living a traditional Solomon Islander lifestyle [38].
The available literature on tree-related mortality and morbidity mainly comes from rural Melanesia, a geographical subregion of islands in the southwestern Pacific Ocean [38,39,40,41,42,43]. Tree-associated injuries, especially involving coconut palm trees, are an enduring and leading cause of trauma here, accounting for about 20–40% of trauma-related hospital admissions [38, 39].
A few trees are worth emphasis:
-
Coconut palm trees—Coconut trees are ubiquitous in coastal tropical regions and are among the most useful trees in the world to humans, providing a source of food, fuel, cosmetics, and building material. They are integral to life in the Solomon Islands given the widespread dependence on subsistence agriculture [42]. The coconut fruits grow in clusters and hang from the top of a tall, smooth, slender trunk. The trees can grow to 30–35 m tall. With this height and slender trunk in combination with fruits and long pinnate leaves at the very top, the trees will sway in high winds.
-
Betel palm trees—Also known as the areca nut palm. It is a medium-sized palm, usually growing to about 20 m tall. Like the coconut tree, it has a long, smooth, slender trunk. If a climber falls from a coconut or betel palm there is seldom anything to grasp on the way down [39].
-
Mango trees—Mangoes are the national fruit of the Philippines. These are large trees which may reach heights up to 40 m [41]. They have a greater trunk circumference and are closer in resemblance to an oak tree than a coconut palm tree.
-
Breadfruit trees—Another important and ubiquitous tropical fruit tree which can grow to heights of 20–25 m. It is not a palm type of tree.
Deaths and injuries will be divided into two general categories for discussion: those occurring when climbers fall out of the tree, and those resulting from either fruits or tree limbs falling and striking people underneath the tree.
Falls of Climbers While Harvesting from Fruit Trees
Climbing trees is important to rural life in many developing tropical regions and is frequently performed as a harvesting method, making falls from trees a significant public health problem and occupational hazard [44]. This is uniquely true given how many of these harvesters are children and adolescents. In the tropics, falling out of trees is a more common cause of trauma than being hit by falling objects. Many tree types have been implicated including coconut, mango, betel palm, guava, apple and nut trees [39, 43].
Coconut palms have received the most attention in the literature and may be the most common and fatal descents from height. The physical features of the tree are such that climbers must ascend a slender unbranched trunk to retrieve fruits at the very top. This is a cultural tradition requiring skill. The person assumes a body posture that enables them to exert pressure on the tree trunk with their feet, sometimes with the assistance of looped rope, twine, or cloth around the ankles. This helps the climber keep their feet close together as they advance up the tree using their hands and the soles of their feet [39]. Workers on some islands use a variant method whereby they tie a bolo knife or similar machete-type cutting tool to their waste, notching grooves in the coconut tree trunk to serve as a ladder and protective measure against falling. Another sharp instrument may be introduced if the harvester uses a blade to cut the coconuts free instead of merely plucking them manually. Harvesting coconut sap sometimes entails a system of bamboo or rope bridges connecting the canopies, and the worker moves from tree to tree on these high bridges [45].
As for mango trees, falls may be more likely to occur when branches break as the climber works their way distal from the trunk, toward the fruit [41].
There is a sex and age predisposition which varies somewhat depending on societal norms. About 75% of those injured in falls from trees are male, and about 75% are less than 16 years of age. Not many studies have documented fall height. One prospective study of emergency department visits in Burkina Faso showed a mean fall distance of 5.2 m, although these were mostly from mango and other trees with fruit accessible at lower elevations compared to palm trees [44]. In this study, the most common circumstances reported for the accidents were slipping on a branch (60%) and the breaking of a branch (35%), with an interesting cause being insect bites leading to loss of balance (3%).
The most frequent injury across all tree types is upper extremity fracture, especially of the distal radius, suggesting falls on outstretched arms predominate. This is consistent with the patient population skewing young and fit with better reflexes relative to older individuals, with attempts to break their falls by reaching out with their arms. However, thoracic injuries appear to be rare, possibly due to greater costal grid flexibility in childhood [44]. Abdominal trauma is more likely and may include splenic laceration.
Information on deaths has seemingly gone almost entirely uncaptured. Barss and colleagues created a questionnaire for their 1984 study in Papua New Guinea and distributed it to regional health centers in an attempt to acquire some data on pre-hospital mortality [39]. The responses revealed at least 28 deaths in a four-year period due to falls from trees, where death occurred prior to reaching medical care. Every case was reported as a lethal head injury, and a few also had thoracic, abdominal, or spinal injuries. One climber fell after accidently cutting his arm with a bush knife. Another case involved a harvester with an epileptic condition who fell from a mango tree during a seizure and died. Further characteristics of the fatalities were not described.
If women and girls are tasked with climbing trees to collect fruit, an important population to consider is pregnant females. Dakouré and colleagues report three of these patients who fell and while they survived, all three suffered secondary abortions [44].
Being remote and rural settings in developing countries, time interval to medical treatment for these injuries is a persistent issue. The skeletal fractures are often complicated by osteomyelitis at presentation if the climber survives, and it is not uncommon for the interval to last multiple days to weeks [39, 44].
Although safety harnesses and head protection have been recommended, many village tree climbers do not employ any safety equipment [45]. Some countries have pioneered the use of mechanical tree climbing devices and robots as an alternative to manual fruit harvesting.
Deaths and Injuries from Falling Coconuts and Tree Limbs
While less common in the tropics than climbers falling out of trees, trauma to those on the ground from being struck by falling trees/limbs and fruits is still a hazard. These will be discussed separately, as the falling coconut injuries are fairly idiosyncratic.
Falling Trees and Tree Limbs
Clearing land for traditional rainforest gardens usually requires tree felling. When these large tropical trees fall, very often they will pull down branches from adjacent trees by numerous connected vines, generating dangerous falling objects [39]. Instead of cutting them down, large trees are occasionally burnt or ring-barked and left standing, leaving them damaged and more susceptible to failure. Weather can play a factor, as tropical cyclones sometimes uproot even massive rainforest trees and blow them over or cause wind-induced breaks of tree limbs.
Escoffery and Shirley report a death in Jamaica which came to autopsy [46]. The decedent was a previously healthy 10-year-old female who was sitting under a tree in a park when a branch broke for unspecified reasons, fell, and hit her on the head. She arrived at the emergency unit with fixed and dilated pupils. She was bleeding from the nostrils, ears, and mouth. She died soon after presentation. Autopsy showed bruising over the left side of the forehead. There were extensive basilar skull fractures and diffuse subgaleal, subdural, and subarachnoid hemorrhages with accompanying marked cerebral edema. Additional findings included disrupted supraspinous and interspinous ligaments between the C1 and C2 vertebrae. The size of the tree limb and the type of tree were not specified.
Falling Coconuts
For a 1984 paper, Dr. Peter Barss enlisted the help of a clerk to weigh immature and mature and wet and dry coconuts, and had astronomer A.E. Whitford assist in calculating the physical forces of these dropping fruits [40]. They ranged from 1–4 kg. The paper states that a coconut weighing two kilograms which falls 25 m will be traveling 80 km/hour upon impact with a victim’s head. Although the impact force depends on direct versus glancing strike angles as well as the distance over which the coconut decelerates, they calculated that for a direct blow with a stopping distance of 5 cm, the force would be 1,000 kg.
Coconuts are the seeds of the tree and so naturally fall to the ground when they mature, or occasionally get knocked down during high winds or heavy rain. Being positioned under a coconut palm therefore makes a hit by a falling coconut possible, and this happens with some frequency wherever the trees and people coexist. The events are rarely fatal, as a direct strike to the head represents a spatiotemporal improbability.
Nonetheless, the sheer oddity of such accidents has made them fodder for news outlets. Several media reports have spotlighted the concern for death by falling coconut. Some articles warn travelers to the tropics, cautioning them about camping underneath coconut trees. Cities in northeastern Australia have removed or de-fruited coconut palms in populated areas to prevent the dreaded falling-drupe fatality. The phenomenon of getting hit on the head by a coconut has even been depicted for comedic effect on popular American television shows, including Gilligan's Island and SpongeBob SquarePants.
The fatal cases likely suffer the same problem of underreporting due to pre-hospital mortality and survivorship bias in the existing literature as the deaths due to climbers falling from trees [38, 39, 42]. Escoffery and Shirley again have the only published autopsy case I could find [46]. The decedent was a 79-year-old female standing under a coconut tree when she was struck on the head by a plummeting coconut. She was unconscious upon presentation to the emergency unit. A 4 cm stellate laceration was present on the right parietal scalp with associated palpable skull defect. Status epilepticus ensued, and the patient died on the third day of admission. Autopsy revealed subgaleal hemorrhage associated with the scalp laceration and a subjacent depressed skull fracture, cerebral edema, and cerebellar tonsillar herniation.
In 1973, a 2-year-old died during a diaper change in the shade of a coconut tree in Hawaii, U.S. A cluster of 57 coconuts fell and landed on the child [47].
In addition to Jamaica and Hawaii, deaths from falling coconuts have been reported in Sri Lanka, Singapore, Papua New Guinea, Vanuatu, Thailand, India, and Colombia.
As a combination of circumstances, coconuts sometimes fall and strike people who are actively climbing the trunk of the tree [39].
On a final and bizarre note, there is a harvesting method employed by some farmers in Thailand and Malaysia whereby trained macaques pick the fruits. In 2001 in Malaysia, an adult male reportedly died instantly when one of these monkeys dropped a coconut on his head [48].
Deaths and Injuries Associated with Falls from Walnut Trees in the Agricultural Setting
Walnut trees are native to large swaths of land ranging from southeast Europe to southwest Asia, central Asia and southwestern China, and the fruit of the walnut tree is a key feature of several regional economies as it has uses in the food and drug industries. Especially in rural areas where walnut harvesting is an important source of income, falls have been widespread among farmers who climb the trees to harvest the fruit [49,50,51].
Walnut trees are large deciduous trees growing to about 15–30 m with some attaining heights of 35 m. They typically have a broad crown and most fruits are located toward the distal end of long branches. Characteristics of the walnut tree unfavorable to climbers include a surface of smooth bark which is commonly described as slippery, and air space-containing chambered piths in the branches which make them especially frangible if the tree’s health is compromised [49,50,51].
Where studied, greater than 90% of farmers who fall from walnut trees are male, mean age is about 35 years, and many harvesters are classified as illiterate [49,50,51].
Most falls occur when the branches break during climbing. Some harvesting methods include standing on a branch while dislodging nuts with a stick and vigorously shaking branches to force the nuts free, both of which increase risk of fracturing a tree limb [50]. Falls also occur due to loss of balance on the slippery surface of the branch [49, 51]. A disproportionate number of cases present to hospitals during the evening shift, suggesting loss of visibility and worker fatigue may play significant roles [50].
The most frequent serious injuries to surviving patients are of the spinal column, particularly of the lumbar spine in the form of burst and wedge compression fractures. A subset of these have caused complete paraplegia. There appears to be an approximately equal mixture of upper and lower extremity trauma in these walnut tree falls.
In studies from Iran, Turkey, and the Kashmir region of the Indian subcontinent, mortality in these falls ranges from about 5–25% [51,52,53]. This is likely an underestimate given most methodologies do not account for pre-hospital deaths. Therefore, mortality is considerable even though fall victims tend to be relatively young and fit males. In a study of 127 patients referred to a trauma center, five patients died on the day of admission, all due to traumatic brain injuries [50]. In another study, there were two deaths attributed to complete paraplegia complicated by pressure ulcers with superimposed infection and bacteremia [51]. Deaths due to dislocations and fractures of the cervical spine have also been reported [49].
One possible prevention measure is to eliminate the need to climb trees by use of a mechanized walnut harvesting device; of course, preventing injury and death from walnut tree falls requires these machines to be available and affordable [49].
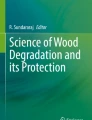
Deaths and Injuries Associated with Tree Stands Used for Hunting
Tree stands, also known as hunting stands or deer stands, are elevated platforms affixed to trees upon which someone perches to gain an advantage while hunting. These stands are commonly used for hunting deer, a popular recreation in many regions of North America. A tree stand gives the hunter an expanded field of vision, removes the hunter from the deer’s normal line of sight, reduces ground scent, and decreases the likelihood of being struck by stray projectiles launched by other hunters. Most deer hunters in the U.S. employ tree stands, and time trends of trauma registries from two U.S. states suggest there is an increasing number and rate of serious tree stand-related injuries which likely reflect the growing popularity of these stands [54, 55].
Concomitantly, there is a small but distinct literature in the U.S. dedicated to the epidemiology and features of tree stand-associated injury, as falls from stands actually represent the leading cause of hunting-related accidents in the country, even when restricting the analysis to only those injuries severe enough to warrant admission at a major trauma center [54,55,56,57,58,59,60,61,62,63]. This contradicts the prevailing stereotype, which views hunting injuries as intoxicated friends accidently shooting themselves or each other. The classic case is a male, about 40 years of age, hunting with a bow and arrow who presents to a small- or medium-sized hospital with a skeletal fracture after falling from a tree stand, without involvement of alcohol or drugs of abuse. A survey of over 38,000 visits to U.S. emergency departments for hunting stand injuries found that patients were 93% male [60].
Although it is somewhat unclear why these falls occur and naturally the reasons will vary on a case-by-case basis, there are some reported common factors precipitating the events:
-
Structural failures—Include both failures of the stand itself (e.g., broken stand parts) and failures of the tree to which the stand was attached. Structural failures are typically due to poor design or construction of the perch. Although commercial tree stands are now available, some hunters still make their own. One study reported a high rate of falls were attributable to homemade stands [62]. These rudimentary stands often consist of an elevated wooden platform nailed to the tree, with either a wooden ladder or wooden steps nailed to the trunk (Fig. 8.9) [64]. Even with industry-constructed stands, errors in placement may result in failure. Evidence of structural failure at a scene might include a collapsed or broken stand at the base of the tree, snapped or broken cables or carabiners, two pieces of a climbing tree stand that are separated (not tethered together), cracked or damaged tree limbs, and loose or unstable fastenings.
Fig. 8.9 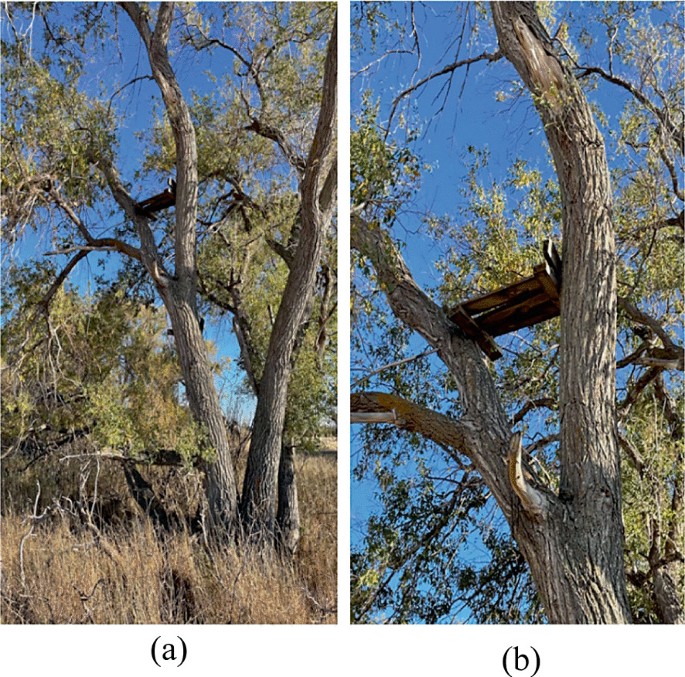
A tree stand located north of Ray, North Dakota, U.S. a The hunter constructed this stand in his youth, creating an elevated wooden platform and nailing wood steps to the trunk b Closer view of the homemade tree stand
-
Loss of balance while entering or exiting the stand—The moment of climbing into or getting out of a hang-on platform type tree stand appears to be especially prone to slips and loss of control. Assembling and disassembling the stand while elevated can also be difficult to navigate. However, ascertaining this information is reliant upon history provided by the victim or a witness.
-
Descending a tree in the evening—A disproportionate percentage of falls occur in the evening hours [63]. There are some interesting points to consider. Aside from the loss of visibility, intrinsic factors related to the hunter may play a significant role. As an example, to maximize the hunt’s potential, some hunters will perform an “all-day sit” where they are perched in the tree stand nearly continuously from dawn until nightfall. Physical and mental fatigue at the end of a marathon day may contribute to accidents as they are exiting the stand and descending the tree. Furthermore, hunters may view the act of eating in the stand as detrimental to the success of the hunt due to excess movement and scent, and so hunger may exacerbate the fatigue. These hunts in tree stands can be physiologically strenuous activities requiring constant diligence, prolonged time spent in one body position, and possible exposures to frigid environments, wind, and other taxing weather conditions.

These factors can occur in combination. For example, a lapse in judgment in the context of fatigue may lead to a hunter choosing a suboptimal tree branch for balance while exiting a stand.
In most cases, alcohol is not a factor. Nearly all studies show alcohol involved at rates of less than 10%. However, one study demonstrated that for 325 victims with available data, 7% were legally intoxicated with blood alcohol content >0.1% [55]. Alcohol use appears to be overrepresented in severe and lethal injuries. Drugs of abuse are involved in less than 5% of cases.
It is no surprise that falls causing severe injury occur when the hunter does not wear a safety harness. As deadly or life-altering injuries are largely preventable, proper use of a full-body fall restraint device is now routinely recommended and promoted by hunter education programs, as well as public awareness campaigns in some U.S. states.
People can hunt from quite high elevations in these tree stands. Average fall heights are between 4–6 m; it is not uncommon to see stands positioned greater than 6 m above the ground, and falls from over 9 m have been reported [59].
The most frequent serious injuries are fractures of the spinal column and long bones of the lower extremities. Paraparesis to complete quadriplegia may result from spinal cord injury, depending on location and extent of the traumatic central nervous system lesion. Fractures of the thoraco-lumbar spine appear to vastly outnumber those of the cervical spine; while survivorship bias may skew this proportion in the literature, the overall evidence suggests impact forces in most cases predominantly involve the torso and lower extremities, suggesting a preponderance of lower body-first falls. Incapacitating injuries may be peculiarly relevant as hunting by its very nature occurs in rural, remote areas. This is borne out in the literature, where the average time between the fall and presentation to a medical facility is about four hours, with very few victims arriving in less than one hour [55, 63].
Fatalities in tree stand incidents are nevertheless presumably rare. Usually, the injuries are not lethal. When they are, they may include the expected blunt trauma-associated vertebrae and rib fractures, solid organ lacerations, and head injuries. Shields and Stewart report a medical examiner case of a typical death for the forensic pathology literature [64]. The decedent was a 65-year-old male discovered under a tree in the early morning by his fellow hunters. He had fallen approximately 6 m to the ground from a homemade tree stand and was not secured by any safety equipment. He was pronounced dead upon arrival at a neighboring county's emergency department. Pertinent autopsy findings were limited to evidence of blunt force trauma, including superficial abrasions and contusions, multiple rib fractures, a left superior ramus pelvic fracture, 1,000 mL left-sided hemothorax, and 500 mL hemoperitoneum. Cause of death was truncal blunt force injuries, and manner of death was accident.
Interestingly and worth highlighting, Shields and Stewart also report a second tree stand-associated death in the same article, this one by an appreciably different cause and mechanism [64]. This decedent was a 65-year-old male with significant obesity discovered in the evening while hanging upside-down from a tree. He was tethered by a rope around his waist extending from a homemade hunting stand, which was wedged between two trees in a rudimentary fashion. At autopsy, there was evidence of asphyxiation including dark red–purple suffusion of the face, dark purple livor mortis with petechial hemorrhages of the upper torso, scleral injection, and palpebral conjunctival petechial hemorrhages. The heart weighed 900 g, with left ventricular hypertrophy and dilation. Microscopic examination demonstrated myocardial fibrosis. Postmortem toxicological and electrolyte studies were unremarkable. The cause of death was attributed to positional asphyxia due to reverse suspension from the tree stand, and ischemic heart disease was judged a significant contributing condition. The manner of death was accident.
The asphyxia death is intriguing for a couple reasons. First, it is conceivable that this type of event represents an underreported tree stand-associated injury, as these accidents are likely not medically attended and therefore may not be captured by study methods. Second, these deaths occur in the presence of harnesses and safety devices, likely makeshift or worn improperly. The paper by Shields and Stewart appears to be the only report of tree stand-related injury tailored for the forensic literature to date, and their review found only two previously published cases describing asphyxiation as a cause of death. These were a teenager wearing an ill-fitting harness which compressed too tightly around his waist [65] and a man who fell while using a belt-type safety harness which slid up around his neck [61]. Falling with a harness on still necessitates both an uncontrolled fall and a sudden termination or alteration of momentum. There are online anecdotes of hunters who fell while wearing safety harnesses only to then swing into the sharp edges of affixed climbing sticks or slam into the tree trunk. As demonstrated in the reverse suspension case, the fallen hunter can be effectively trapped in the harness while hanging from the tree, with no dependable mode of extrication.
Additional topics of greater uncertainty include the involvement of firearms, such as unintentional discharges while hunters carry firearms up to or down from a tree stand, or discharge upon impact after a fall. Only rarely have gunshot wounds been reported in these cases, and it is unclear whether the injured was shot by another hunter, suffered a self-inflicted gunshot wound prior to falling out of the stand, or shot themselves upon hitting the ground after the fall. While these hunts tend to make use of bows and arrows and therefore the risk of firearm incidents may be reduced, hunters will often carry accessories such as shears and folding saws for pruning any tree branches that might interfere with the archery, and therefore introduce a potentially tricky activity with a sharp object executed at a considerable height.
In addition to properly utilizing a full-body safety harness, other practices to reduce the risk of hunting stand accidents include using a commercial model instead of a homemade stand, proper methods of stand placement, careful assessment of tree branch strength prior to applying any weight to the branch, avoidance of fatigue and alcohol, and proper methods of stand entrance and exit. If a firearm is used instead of a bow and arrow, anticipation of recoil is pertinent. Equipment ought to be lifted or lowered to or from the tree stand with a haul line, as opposed to being carried on the hunter.
Summary
Hopefully this chapter has addressed a gap in the available literature on environmental and occupational deaths. The global scope of this writing almost guarantees that certain types of tree-related deaths and injuries have been overlooked. Still, for events with such worldwide prevalence, it seems worthwhile to start somewhere.
References
Kappelman J, Ketcham RA, Pearce S, Todd L, Akins W, Colbert MW, Feseha M, Maisano JA, Witzel A. Perimortem fractures in Lucy suggest mortality from fall out of tall tree. Nature. 2016;537(7621):503–7. https://doi.org/10.1038/nature19332.
Driscoll TR, Ansari G, Harrison JE, Frommer MS, Ruck EA. Traumatic work-related fatalities in forestry and sawmill workers in Australia. J Safety Res. 1995;26(4):221–33. https://doi.org/10.1016/0022-4375(95)00018-L.
Brodie LR, Ibrahim JE. Fatal injury in tree felling and related activities, Victoria, Australia 1992–2007. Inj Prev. 2010;16(1):53–6. https://doi.org/10.1136/ip.2009.021683.
Michael J, Gorucu S. Occupational tree felling fatalities: 2010–2020. Am J Ind Med. 2021;64(11):969–77. https://doi.org/10.1002/ajim.23286.
Centers for Disease Control and Prevention (CDC). Work-related fatalities associated with tree care operations–United States, 1992–2007. MMWR Morb Mortal Wkly Rep. 2009;58(15):389–93.
Lindroos O, Burström L. Accident rates and types among self-employed private forest owners. Accid Anal Prev. 2010;42(6):1729–35. https://doi.org/10.1016/j.aap.2010.04.013.
Varakina ZhL, Vyazmin AM, Sannikov AL, Nygard CH, Grjibovski AM. Fatal occupational injuries in the Arkhangelsk region. Northwest Russia Occup Med (Lond). 2010;60(6):470–5. https://doi.org/10.1093/occmed/kqq068.
Weyrauch D, Gill JR. Accidental deaths involving trees: professional and nonprofessional woodcutting and tree failures with autopsy findings. Am J Forensic Med Pathol. 2021;42(4):350–3. https://doi.org/10.1097/PAF.0000000000000686.
Ashby K, Ozanne-Smith J, Fox B. Investigating the over-representation of older persons in do-it-yourself home maintenance injury and barriers to prevention. Inj Prev. 2007;13(5):328–33. https://doi.org/10.1136/ip.2006.012328.
Centers for Disease Control and Prevention (CDC). Nonoccupational logging fatalities–Vermont, 1997–2007. MMWR Morb Mortal Wkly Rep. 2008;57(10):260–2.
Dąbrowski A. Kickback risk of portable chainsaws while cutting wood of different properties: laboratory tests and deductions. Int J Occup Saf Ergon. 2015;21(4):512–23. https://doi.org/10.1080/10803548.2015.1095547.
Koehler SA, Luckasevic TM, Rozin L, et al. Death by chainsaw: fatal kickback injuries to the neck. J Forensic Sci. 2004;49(2):345–50.
Macfarlane I, Harry N. Severe chainsaw injuries. Aust N Z J Surg. 1977;47(2):183–5. https://doi.org/10.1111/j.1445-2197.1977.tb04264.x.
Choi CS, Jordan FB, Balding LE. The missing link. an unusual case of embolization. Am J Forensic Med Pathol. 1994;15(3):211–2. https://doi.org/10.1097/00000433-199409000-00006.
Myers JR, Fosbroke DE. Logging fatalities in the United States by region, cause of death, and other factors—1980 through 1988. J Safety Res. 1994;25(2):97–105. https://doi.org/10.1016/0022-4375(94)90021-3.
WorkSafe Victoria. Working safely with trees. State Government of Victoria;2020. https://www.worksafe.vic.gov.au/resources/working-safely-trees. Last Accessed 22 Nov 2021.
Hartley MA, Chalk JJ. A review of deaths in Australia from accidental tree failures. Arboriculture Australia;2019. https://arboriculture.org.au/getassets/a2bd3064-7acd-ea11-90fb-00505687f2af/A%20Review%20of%20Deaths%20in%20Australia%20from%20Accidental%20Tree%20Failures.pdf. Last Accessed 19 Nov 2021.
Schmidlin TW. Human fatalities from wind-related tree failures in the United States, 1995–2007. Nat Hazards. 2009;50:13–25. https://doi.org/10.1007/s11069-008-9314-7.
Walsh RA, Ryan L. Hospital admissions in the Hunter Region from trees and other falling objects, 2008–2012. Aust N Z J Public Health. 2017;41(2):121–4. https://doi.org/10.1111/1753-6405.12614.
Ball DJ, Watt J. The risk to the public of tree fall. J Risk Res. 2013;16(2):261–9. https://doi.org/10.1080/13669877.2012.737827.
Hall GC, Kinsman MJ, Nazar RG, et al. Atlanto-occipital dislocation. World J Orthop. 2015;6(2):236–43. https://doi.org/10.5312/wjo.v6.i2.236.
Teh J, Firth M, Sharma A, Wilson A, Reznek R, Chan O. Jumpers and fallers: a comparison of the distribution of skeletal injury. Clin Radiol. 2003;58(6):482–6. https://doi.org/10.1016/s0009-9260(03)00064-3.
Buckman RF Jr, Buckman PD. Vertical deceleration trauma. Principles of management. Surg Clin North Am. 1991;71(2):331–44. https://doi.org/10.1016/s0039-6109(16)45383-1.
Li L, Smialek JE. The investigation of fatal falls and jumps from heights in Maryland (1987–1992). Am J Forensic Med Pathol. 1994;15(4):295–9. https://doi.org/10.1097/00000433-199412000-00003.
Petaros A, Slaus M, Coklo M, Sosa I, Cengija M, Bosnar A. Retrospective analysis of free-fall fractures with regard to height and cause of fall. Forensic Sci Int. 2013;226(1–3):290–5. https://doi.org/10.1016/j.forsciint.2013.01.044.
Türk EE, Tsokos M. Pathologic features of fatal falls from height. Am J Forensic Med Pathol. 2004;25(3):194–9. https://doi.org/10.1097/01.paf.0000136441.53868.a4.
Gupta SM, Chandra J, Dogra TD. Blunt force lesions related to the heights of a fall. Am J Forensic Med Pathol. 1982;3(1):35–43. https://doi.org/10.1097/00000433-198203000-00008.
Çakı İE, Karadayı B, Çetin G. Relationship of injuries detected in fatal falls with sex, body mass index, and fall height: An autopsy study. J Forensic Leg Med. 2021;78: 102113. https://doi.org/10.1016/j.jflm.2020.102113.
Goonetilleke UK. Injuries caused by falls from heights. Med Sci Law. 1980;20(4):262–75. https://doi.org/10.1177/002580248002000407.
Türkoğlu A, Sehlikoğlu K, Tokdemir M. A study of fatal falls from height. J Forensic Leg Med. 2019;61:17–21. https://doi.org/10.1016/j.jflm.2018.10.008.
Thierauf A, Preuss J, Lignitz E, Madea B. Retrospective analysis of fatal falls. Forensic Sci Int. 2010;198(1–3):92–6. https://doi.org/10.1016/j.forsciint.2010.01.010.
Osawa M, Satoh F, Hasegawa I. Acute death due to hyperextension injury of the cervical spine caused by falling and slipping onto the face. J Forensic Leg Med. 2008;15(7):457–61. https://doi.org/10.1016/j.jflm.2008.02.006.
Eş H, Şahin MF, Özdemir E. Laryngohyoid fractures in fatal nonhomicidal falls from a height. Am J Forensic Med Pathol. 2017;38(4):289–93. https://doi.org/10.1097/PAF.0000000000000350.
de la Grandmaison GL, Krimi S, Durigon M. Frequency of laryngeal and hyoid bone trauma in nonhomicidal cases who died after a fall from a height. Am J Forensic Med Pathol. 2006;27(1):85–6. https://doi.org/10.1097/01.paf.0000201104.10652.08.
Lowenstein SR, Yaron M, Carrero R, Devereux D, Jacobs LM. Vertical trauma: injuries to patients who fall and land on their feet. Ann Emerg Med. 1989;18(2):161–5. https://doi.org/10.1016/s0196-0644(89)80107-6.
Gill JR. Fatal descent from height in New York City. J Forensic Sci. 2001;46(5):1132–7.
Hyder AA. Injuries in low- and middle-income countries: a neglected disease in global public health. Injury. 2013;44(5):579–80. https://doi.org/10.1016/j.injury.2013.01.028.
Rehan R, Jones PD, Abdeen H, Rowas H, Dhaliwal J. The dangers to children from coconut tree trauma, in KiraKira, Solomon Islands: a retrospective clinical audit. Arch Public Health. 2016;74:14. https://doi.org/10.1186/s13690-016-0125-0.
Barss P, Dakulala P, Doolan M. Falls from trees and tree associated injuries in rural Melanesians. Br Med J (Clin Res Ed). 1984;289(6460):1717–20. https://doi.org/10.1136/bmj.289.6460.1717.
Barss P. Injuries due to falling coconuts. J Trauma. 1984;24(11):990–1. https://doi.org/10.1097/00005373-198411000-00012.
Gupta A, Reeves B. Fijian seasonal scourge of mango tree falls. ANZ J Surg. 2009;79(12):898–900. https://doi.org/10.1111/j.1445-2197.2009.05141.x.
Mulford JS, Oberli H, Tovosia S. Coconut palm-related injuries in the Pacific Islands. ANZ J Surg. 2001;71(1):32–4. https://doi.org/10.1046/j.1440-1622.2001.02021.x.
Negin J, Vizintin P, Houasia P, Martiniuk AL. Barking up the wrong tree: injuries due to falls from trees in Solomon Islands. Med J Aust. 2014;201(11):698–700. https://doi.org/10.5694/mja14.01083.
Dakouré PW, Diallo M, Traoré AC, et al. Trauma related to falls from trees treated in a specialized trauma centre in Burkina-Faso-one hundred and six cases treated in one year. Int Orthop. 2015;39(12):2451–6. https://doi.org/10.1007/s00264-015-2966-5.
International Labour Organization: tropical tree and palm crops;2011. https://www.iloencyclopaedia.org/part-x-96841/agriculture-and-natural-resources-based-industries/tree-bramble-and-vine-crops/item/548-tropical-tree-and-palm-crops. Last Accessed 14 Oct 2021.
Escoffery CT, Shirley SE. Fatal head trauma from tree related injuries. Med Sci Law. 2001;41(4):298–300. https://doi.org/10.1177/002580240104100404.
Baby dies after being hit by falling cluster of coconuts. In: Honolulu star-bulletin;1973. https://www.newspapers.com/clip/18012093/baby-dies-after-being-hit-by-falling/. Last Accessed 12 Oct 2021.
Monkey kills man with coconut. In: New Straits Times;2001. https://www.news24.com/News24/Monkey-kills-man-with-coconut-20010813. Last Accessed 12 Oct 2021.
Ersoy S, Sonmez BM, Yilmaz F, et al. Analysis and injury paterns of walnut tree falls in central anatolia of turkey. World J Emerg Surg. 2014;9:42. https://doi.org/10.1186/1749-7922-9-42.
Hoseini Azizi T, Hejazi SS, Kameli A. Frequency of complications of falling from the walnut tree, as an occupational-seasonal injury. J Inj Violence Res. 2018;10(2):91-96. https://doi.org/10.5249/jivr.v10i2.980.
Nabi DG, Rashid TS, Kangoo KA, Ahmed DF. Fracture patterns resulting from falls from walnut trees in Kashmir. Injury. 2009;40(6):591–4. https://doi.org/10.1016/j.injury.2008.11.013.
Baba AN, Paljor SD, Mir NA, et al. Walnut tree falls as a cause of musculoskeletal injury–a study from a tertiary care center in Kashmir. Ulus Travma Acil Cerrahi Derg. 2010;16(5):464–8.
Javadi SA, Naderi F. Pattern of spine fractures after falling from walnut trees. World Neurosurg. 2013;80(5):e41-3. https://doi.org/10.1016/j.wneu.2012.12.014.
Crockett A, Stawicki SP, Thomas YM, et al. Tree stands, not guns, are the midwestern hunter’s most dangerous weapon. Am Surg. 2010;76(9):1006–10.
Smith JL, Lengerich EJ, Wood GC. Injuries due to falls from hunters’ tree stands in Pennsylvania. Am J Prev Med. 2009;37(5):433–6. https://doi.org/10.1016/j.amepre.2009.06.019.
Centers for Disease Control (CDC). Tree stand-related injuries among deer hunters–Georgia, 1979–1989. MMWR Morb Mortal Wkly Rep. 1989;38(41):697–700.
Gates RL, Helmkamp JC, Wilson SL, Denning DA, Beaver BL. Deer stand-related trauma in West Virginia: 1994 through 1999. J Trauma. 2002;53(4):705–8. https://doi.org/10.1097/00005373-200210000-00014.
Lawrence DW, Gibbs LI, Kohn MA. Spinal cord injuries in Louisiana due to falls from deer stands, 1985–1994. J La State Med Soc. 1996;148(2):77–9.
Lazzara AA Jr, Ditmer BI, Doughty KW, Reynolds KR. Tree stand-related injuries in nonadmitted and admitted patients at a level 2 trauma center in Michigan: 2015–2019. Wilderness Environ Med. 2021;S1080–6032(21):00160–5. https://doi.org/10.1016/j.wem.2021.08.006.
Loder RT. Epidemiology of hunting stand injuries presenting to US emergency departments, 2008–2013. Wilderness Environ Med. 2015;26(3):387–94. https://doi.org/10.1016/j.wem.2014.07.004.
Metz M, Kross M, Abt P, Bankey P, Koniaris LG. Tree stand falls: a persistent cause of sports injury. South Med J. 2004;97(8):715–9. https://doi.org/10.1097/00007611-200408000-00003.
Urquhart CK, Hawkins ML, Howdieshell TR, Mansberger AR Jr. Deer stands: a significant cause of injury and mortality. South Med J. 1991;84(6):686–8.
VanWormer JJ, Holsman RH, Petchenik JB, Dhuey BJ, Keifer MC. Epidemiologic trends in medically-attended tree stand fall injuries among Wisconsin deer hunters. Injury. 2016;47(1):220–5. https://doi.org/10.1016/j.injury.2015.09.012.
Shields LB, Stewart D. Deer stand fatalities in Kentucky: two cases of reverse suspension and blunt force trauma. Am J Forensic Med Pathol. 2011;32(1):39–43. https://doi.org/10.1097/PAF.0b013e3181eafe05.
Forks TP. Hunting injuries in Mississippi. J Miss State Med Assoc. 2002;43(11):339–43.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2022 The Author(s), under exclusive license to Springer Nature Switzerland AG
About this chapter

Cite this chapter
Weyrauch, D. (2022). Death Associated with Trees. In: Rutty, G.N. (eds) Essentials of Autopsy Practice. Springer, Cham. https://doi.org/10.1007/978-3-031-11541-7_8
Download citation
DOI: https://doi.org/10.1007/978-3-031-11541-7_8
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-031-11540-0
Online ISBN: 978-3-031-11541-7
eBook Packages: MedicineMedicine (R0)