
Abstract
Optical biometry is essential for intraocular lens (IOL) power calculation. The validity and reliability of measurement results has improved greatly over the last decades. This increased accuracy allows a more precise measurement of the eye and relatively good predictability for IOL power calculation.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
- Partial coherence interferometry (PCI)
- Optical biometry
- Swept source optical coherence tomography (OCT)
One of the most important developments in the calculation of IOLs was the introduction of optical biometry [1]. This is followed closely by developments in IOL power calculation formulae [2]. In this chapter, the evolution, fundamentals and latest developments of optical biometry will be discussed.
Partial Coherence Interferometry (PCI )
Before the introduction of optical biometry, the measurement of the eye length was the second largest source of error [3,4,5]. The introduction of optical biometry to the field was a milestone and took place in Austria, in Vienna at the Institute for Medical Physics specifically. Prof. Fercher [6] was the original pioneer of this method, which was then further developed together with Profs. Hitzenberger and Drexler. The first studies were eventually carried out on cataract patients, in cooperation with Prof. Findl [7]. In the 1980s the concept of partial coherence interferometry was already in clinical use in the measurement of ocular axial length [8] and the first clinical studies for the measurement of the anterior segment and axial length followed in the 1990s [3, 9, 10]. The PCI method had some clear advantages over the ultrasound method. PCI could be performed without touching the globe, so the eye length s not manipulated during the examination. This was a significant advantage over contact ultrasound where the act of touching the globe can induce a dent making the measurement inaccurate. Immersion ultrasound avoids this risk but still requires some manipulation to create the fluid interface.—PCI biometry required no contact with the eye at all, unlike any other type of ultrasound. Some further advantages of optical biometry are that the examination is technician independent and can be carried out much faster and with much higher precision and resolution than the previous ultrasound devices [11]. Finally, the measurement is based on the fixation axis of the eye, which is not necessarily the case with ultrasound.
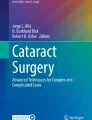
Over 10 years ago, Norrby [5] showed that axial length measurement with contact ultrasound accounted for 17% of the total error in the calculation of IOLs. However, when this study is re-evaluated using PCI technology instead of contact ultrasound, the error of the measurement decreases from 17 to 3% (Fig. 1).

Sverker Norrbys graphic from 2008 in modified form [5]. The individual bars represent the sources of error. For axial length, the value for contact ultrasound (17%) and for partial coherence interferometry technology (3%) is given—the remaining bars refer to the PCI method. Augenlänge = axial eye length; Hornhautmessung = corneal radii, Pupillengröße = pupil size; IOL Ungenauigkeit = IOL labelling error
While the underlying physical principles of the PCI method are out of the scope of this chapter, basically, a “dual beam” version of the classic Michelson interferometer using a light source with a wavelength of usually 780 nm (Fig. 2) [3]. The measuring distance is another point that should be considered. With classical ultrasound, the measurement is made from the anterior corneal surface to the inner limiting membrane but with PCI procedures the measurement is to the retinal pigment epithelium. This difference was “converted” to ultrasound when optical biometry devices were originally introduced.

Representation of partial coherence interferometry (taken over from [3]). The eye is illuminated by means of an external interferometer, which generates a co-axial double beam with a specific wavelength. Important components of the external interferometer are a semitransparent mirror and a reference mirror. Both parts of the double beam have a common time delay which is twice the interferometer length difference (2d). In the eye, the two beam components are changed (“delayed”) due to contact with different refractive indices and a partial coherence interferometry signal (PCI signal) is produced. Reflected signals from the eye (in the figure as an example C1, C2, R1 and R2) are detected by a photodetector, whereupon the PCI signal of the axial length is generated as optical distance (OL). A scanning mirror is used for this. Finally, the optical signal has to be corrected according to the refractive indices in the eye (usually a group refractive index) to obtain an anatomical distance
Composite Scan
While PCI technology has many clear advantages, it is not without a disadvantage. If the media is too opacified, optical biometric measurements may not be possible and an ultrasonic measurement should be used. The reason for this is a mixture of different optical phenomena such as absorption, reflection and scattered light (especially Rayleigh scattering) can distort the PCI measurement. There are different approaches to reduce this problem. The first approach, known as composite scanning, was introduced in the IOL master (Carl Zeiss Meditec AG, Jena, Germany) by upgrading the software [12]. Prior to the introduction of the composite scan, each measurement (i.e., each A-scan) was evaluated individually. Each peak of the A-scan was evaluated using the signal to noise ratio (SNR) and if the main peak was not sufficiently distinct from the remaining peaks (noise), the scan was not successful. In the composite scan, the individual scans are superimposed (Fig. 3a). This amplifies real peaks because they occur in several scans and the other peaks (noise) cancel each other out. In a clinical evaluation of the composite scan, the rate of unsuccessful scans was reduced from 10% to less than 5% [12]. Later, another biometric device using the same method was launched on the market, the AL-Scan (Nidek Co., LTD, Japan) [13].


a Four PCI-based A-scans (red) of a patient with dense cataract. As the signal to noise ratio (SNR) is too low, and the individual scans do not show clear peaks. In the composite scan (blue), the four individual scans are superimposed on each other, thus amplifying the real signals. This results in an improved signal to noise ratio and a clear peak representing the length of the eyes (adopted from [12]). b The longitudinal ssOCT based B-scan of the IOLMaster 700 produces an image with visible anatomical details instead of individual peaks. ssOCT based is the axial section (upper image), as well as the macular scan (far right) for fixation control. The keratometry, white-to-white measurement and the red-free image (for intra-operative alignment for toric artificial lenses) are not ssOCT based (from the ESCRS presentation in London 2014). c ssOCT based B-Scan of the Anterion with tomographic corneal image (top right) and signal intensity display for cornea, lens and axial length in mm (bottom)
PCI -Like Procedures
The best-known A-scan alternative is optical low coherence reflectometry (OLCR). The first instrument on the market using this approach was the Lenstar (Haag-Streit Diagnostics, Switzerland) followed by the Aladdin (Topcon, Japan) [14]. Similar to the PCI method, an A-scan is used and the concept is also based on a Michelson interferometer but in contrast to the PCI method, a slightly longer wavelength is used (820 nm) [15].
In various comparative studies, the differences in axial length measurements between OLCR and PCI technology were not considered clinically relevant [15,16,17]. PCI and OLCR methods are also not different for the measurement of anterior chamber depth in any clinically relevant way [18].
Due to a software update, the number of successful scans could be increased from 94 to 98% [19]. However, the more modern generation of optical coherence tomography (OCT) technology appears to be even better than OLCR technology in terms of successful scans [20].
OCT Based Optical Biometry
Another development is the use of swept source OCT (ssOCT) for axial eye length. The principle is also based on the PCI method, but there are a few major differences. The first device on the market for longitudinal B-scans was the IOLMaster 700 [21] (Carl Zeiss Meditec AG, Germany), followed by Argos [22] (Movu, a Santec Company, USA) and Anterion [23] (Heidelberg Engineering, Germany). Spectral domain OCT-based methods have also made it to the market (B-OCT module for Revo OCT from Optopol, Poland) [24].
The comparison between ssOCT and PCI/OLCR technology showed a very good comparability between the two methods but with a better reproducibility for the ssOCT method [25]. The ssOCT technology also has some advantages over the PCI/OLCR method that should be considered. While the PCI/OLCR method is fundamentally based on A scans, ssOCT devices provide longitudinal B scans. In other words, instead of an amplitude (A scan) a brightness scan (B scan) is used, or more simply, instead of a one dimensional scan, a two-dimensional image is used (Fig. 3a–c). The image has the advantage that the anatomical structures can be clearly identified. Thus, the clinician can see with a glance whether, for example, the macula has been correctly recognized. We recently showed that this longitudinal B-scan can also be used directly for a rough macular screening [26].
A somewhat more futuristic approach is to use preoperative B-scans to make predictions for the postoperative lens position [27]. The most important advantage, however, is the longer wavelength (just over 1000 nm) of the ssOCT technology compared to the PCI/OLCR technology. This longer wavelength leads to a better penetration through dense media, such as a dense cataract. This even deeper penetration can increase the number of successful scans from about 95% [12] to over 99% [28], even in dense posterior subcapsular cataracts.
While it is not yet available, an even newer concept s to perform intra-operative ssOCT measurements [29] of the aphakic eye (Hienert et al., ESCRS 2019 in Marrakesh). This could be a good alternative for a number of patient groups where preoperative biometry is particularly difficult. Paediatric patients with cataract and adult patients who cannot be successfully measured with optical biometry in a sitting position, whether due to compliance problems, physical limitations or a very dense cataract could benefit greatly from this approach.
Prediction of the Post-Operative IOL
The current greatest source of error in IOL calculation is the prediction of the IOL position, which currently accounts for more than 50% of the total error of the IOL power calculation [5, 30]. This uncertainty is also the reason why various IOL power calculation formulae have been developed in recent decades. While these formulae are discussed in detail elsewhere in this book, it is important to note that the prediction is difficult for two reasons: firstly, it is difficult to predict the post-operative IOL position [29, 31, 32] and secondly, in the weeks following implantation, there is an axial displacement of the IOL, which depends on the type of IOL and the degree of capsular fibrosis which varies greatly between patients [33,34,35,36].
Basically, there are three groups of IOL power calculations. Firstly, there is the optical approach which includes the simple vergence formulae (“thin” lens formulae) [2] all the way to complex ray tracing systems [37]. The calculation is subject to clear and established physical laws. Unfortunately, direct prediction of the IOL position is not possible with this model and either a fixed value must be assumed (very outdated model) or other non-ray tracing-based methods must be used.
Secondly, the empirical approach group, which is based on pre-existing data (biometric values, IOL power and measured post-operative refraction). These formulae are a sort of “black box” approach which always generates a constellation of a constants and various parameters that are taken into account for the prediction. By optimizing the constant, an IOL power calculation formula can then be used for different types of IOLs. This also underlines the importance of optimizing the constants for every new lens.
References
Findl O, Drexler W, Menapace R, Heinzl H, Hitzenberger CK, Fercher AF. Improved prediction of intraocular lens power using partial coherence interferometry. J Cataract Refract Surg. 2001;27(6):861–7.
Olsen T. Calculation of intraocular lens power: a review. Acta Ophthalmol Scand. 2007;85(5):472–85.
Drexler W, Findl O, Menapace R, Rainer G, Vass C, Hitzenberger CK, et al. Partial coherence interferometry: a novel approach to biometry in cataract surgery. At J Ophthalmol. 1998;126(4):524–34.
Findl O, Kriechbaum K, Sacu S, Kiss B, Polak K, Nepp J, et al. Influence of operator experience on the performance of ultrasound biometry compared to optical biometry before cataract surgery. J Cataract Refract Surg. 2003;29(10):1950–5.
Norrby S. Sources of error in intraocular lens power calculation. J Cataract Refract Surg. 2008;34(3):368–76.
Hitzenberger CK. Adolf Friedrich Fercher: a pioneer of biomedical optics. J Biomed Opt. 2017;22(12):1–8.
Hitzenberger CK, Drexler W, Leitgeb RA, Findl O, Fercher AF. Key developments for partial coherence biometry and optical coherence tomography in the human eye made in Vienna. Invest Ophthalmol Vis Sci. 2016; 57(9):OCT460–74.
Hitzenberger C, Mengedoht K, Fercher AF. Laser optic measurements of the axial length of the eye. Progress Ophthalmol. 1989;86(2):159–61.
Findl O, Drexler W, Menapace R, Hitzenberger CK, Fercher AF. High precision biometry of pseudophakic eyes using partial coherence interferometry. J Cataract Refract Surg. 1998;24(8):1087–93.
Drexler W, Baumgartner A, Findl O, Hitzenberger CK, Sattmann H, Fercher AF. Submicrometer precision biometry of the anterior segment of the human eye. Invest Ophthalmol Vis Sci. 1997;38(7):1304–13.
Kiss B, Findl O, Menapace R, Wirtitsch M, Drexler W, Hitzenberger CK, et al. Biometry of cataractous eyes using partial coherence interferometry: clinical feasibility study of a commercial prototype I. J Cataract Refract Surg. 2002;28(2):224–9.
Hirnschall N, Murphy S, Pimenides D, Maurino V, Findl O. Assessment of a new averaging algorithm to increase the sensitivity of axial eye length measurement with optical biometry in eyes with dense cataract. J Cataract Refract Surg. 2011;37(1):45–9.
Srivannaboon S, Chirapapaisan C, Chonpimai P, Koodkaew S. Comparison of ocular biometry and intraocular lens power using a new biometer and a standard biometer. J Cataract Refract Surg. 2014;40(5):709–15.
Mandal P, Berrow EJ, Naroo SA, Wolffsohn JS, Uthoff D, Holland D, et al. Validity and repeatability of the Aladdin ocular biometer. Br J Ophthalmol. 2014;98(2):256–8.
Hoffer KJ, Shammas HJ, Savini G. Comparison of 2 laser instruments for measuring axial length. J Cataract Refract Surg. 2010;36(4):644–8.
Chen YA, Hirnschall N, Findl O. Evaluation of 2 new optical biometry devices and comparison with the current gold standard biometer. J Cataract Refract Surg. 2011;37(3):513–7.
Rabsilber TM, Jepsen C, Auffarth GU, Holzer MP. Intraocular lens power calculation: clinical comparison of 2 optical biometry devices. J Cataract Refract Surg. 2010;36(2):230–4.
Air N, brain sound N, Farrokhi S, Findl O. Comparability of anterior chamber depth measurements with partial coherence interferometry and optical low-coherence reflectometry in pseudophakic eyes. J Cataract Refract Surg. 2015; 41(8):1678–84.
Shammas HJ, Wetterwald N, Potvin R. New mode for measuring axial length with an optical low-coherence reflectometer in eyes with dense cataract. J Cataract Refract Surg. 2015;41(7):1365–9.
Kurian M, Negalur N, Das S, Puttaiah NK, Haria D, J TS, et al. Biometry with a new swept-source optical coherence tomography biometer: Repeatability and agreement with an optical low-coherence reflectometry device. J Cataract Refract Surg. 2016; 42(4):577–81.
Srivannaboon S, Chirapapaisan C, Chonpimai P, Loket S. Clinical comparison of a new swept-source optical coherence tomography-based optical biometer and a time-domain optical coherence tomography-based optical biometer. J Cataract Refract Surg. 2015;41(10):2224–32.
Shammas HJ, Ortiz S, Shammas MC, Kim SH, Chong C. Biometry measurements using a new large-coherence-length swept-source optical coherence tomographer. J Cataract Refract Surg. 2016;42(1):50–61.
Asam JS, Polzer M, Tafreshi A, Hirnschall N, Findl O. Anterior segment OCT. In: Bille JF, editor. High resolution imaging in microscopy and ophthalmology: new frontiers in biomedical optics. Cham (CH); 2019, pp. 285–99.
Kanclerz P, Hoffer KJ, Rozema JJ, Przewlocka K, Savini G. Repeatability and reproducibility of optical biometry implemented in a new optical coherence tomographer and comparison with an optical low-coherence reflectometer. J Cataract Refract Surg. 2019;45(11):1619–24.
Kunert KS, Peter M, Blum M, Haigis W, Sekundo W, Schutze J, et al. Repeatability and agreement in optical biometry of a new swept-source optical coherence tomography-based biometer versus partial coherence interferometry and optical low-coherence reflectometry. J Cataract Refract Surg. 2016;42(1):76–83.
Hirnschall N, Leisser C, Radda S, Maedel S, Findl O. Macular disease detection with a swept-source optical coherence tomography-based biometry device in patients scheduled for cataract surgery. J Cataract Refract Surg. 2016;42(4):530–6.
Brain sound N, Buehren T, Bajramovic F, Trost M, Teuber T, Findl O. Prediction of postoperative intraocular lens tilt using swept-source optical coherence tomography. J Cataract Refract Surg. 2017; 43(6):732–6.
Hirnschall N, Varsits R, Doeller B, Findl O. Enhanced penetration for axial length measurement of eyes with dense cataracts using swept source optical coherence tomography: a consecutive observational study. Ophthalmol Ther. 2018;7(1):119–24.
Hirnschall N, Farrokhi S, Amir-Asgari S, Hienert J, Findl O. Intraoperative optical coherence tomography measurements of aphakic eyes to predict postoperative position of 2 intraocular lens designs. J Cataract Refract Surg. 2018;44(11):1310–6.
Olsen T. Sources of error in intraocular lens power calculation. J Cataract Refract Surg. 1992;18(2):125–9.
Hirnschall N, Amir-Asgari S, Maedel S, Findl O. Predicting the postoperative intraocular lens position using continuous intraoperative optical coherence tomography measurements. Invest Ophthalmol Vis Sci. 2013;54(8):5196–203.
Shajari M, Sonntag R, Niermann T, Holland D, Kohnen T, Priglinger S, et al. Determining and comparing the effective lens position and refractive outcome of a novel rhexis-fixated lens to established lens designs. At J Ophthalmol. 2020.
Findl O, Hirnschall N, Nishi Y, Maurino V, Crnej A. Capsular bag performance of a hydrophobic acrylic 1-piece intraocular lens. J Cataract Refract Surg. 2015;41(1):90–7.
Findl O, Struhal W, Dorffner G, Drexler W. Analysis of nonlinear systems to estimate intraocular lens position after cataract surgery. J Cataract Refract Surg. 2004;30(4):863–6.
Kriechbaum K, Findl O, Preussner PR, Koppl C, Wahl J, Drexler W. Determining postoperative anterior chamber depth. J Cataract Refract Surg. 2003;29(11):2122–6.
Wirtitsch MG, Findl O, Menapace R, Kriechbaum K, Koeppl C, Buehl W, et al. Effect of haptic design on change in axial lens position after cataract surgery. J Cataract Refract Surg. 2004;30(1):45–51.
Hirnschall N, Buehren T, Trost M, Findl O. Pilot evaluation of refractive prediction errors associated with a new method for ray-tracing-based intraocular lens power calculation. J Cataract Refract Surg. 2019.
Ladas JG, Siddiqui AA, Devgan U, Jun AS. A 3-D “Super Surface” combining modern intraocular lens formulae to generate a “Super Formula” and maximize accuracy. JAMA Ophthalmol. 2015;133(12):1431–6.
Darcy K, Gunn D, Tavassoli S, Sparrow J, Kane JX. Assessment of the accuracy of new and updated intraocular lens power calculation formulae in 10 930 eyes from the UK National Health Service. J Cataract Refract Surg. 2020;46(1):2–7.
Siddiqui AA, Devgan U. Intraocular lens power calculations in atypical eyes. Indian J Ophthalmol. 2017;65(12):1289–93.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2023 The Author(s), under exclusive license to Springer Nature Switzerland AG
About this chapter

Cite this chapter
Findl, O., Hirnschall, N. (2023). Optical Biometry. In: Shajari, M., Priglinger, S., Kohnen, T., Kreutzer, T.C., Mayer, W.J. (eds) Cataract and Lens Surgery. Springer, Cham. https://doi.org/10.1007/978-3-031-05394-8_14
Download citation
DOI: https://doi.org/10.1007/978-3-031-05394-8_14
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-031-05393-1
Online ISBN: 978-3-031-05394-8
eBook Packages: MedicineMedicine (R0)