
Abstract
Penetrating brain injury (PBI), although less prevalent than closed head trauma, is associated with significantly worse outcomes. Craniocerebral gunshot wounds are the most common mechanism of civilian PBI, with a mortality rate ranging from 66% to 90% prior to hospital arrival. Additionally, only 50% of those receiving medical care survive. Physical examination considerations specific to patients with PBI include evaluation for CSF leak and focused examination of the site of cranial penetration. PBI is also often associated with direct injury to the brain parenchyma, extra-axial injury, and vascular complications. Radiographic evaluation includes a noncontrast head CT and often warrants a CT angiogram or diagnostic subtraction angiography to establish parenchymal and vascular injury secondary to PBI. MRI is seldom indicated, except for rare penetrating injuries from non-metal objects. Medical management of PBI focuses on seizure prophylaxis, antimicrobial prophylaxis, and ICP management. Surgical management should prioritize removing protruding objects and avoiding debridement of retained fragments. Two common complications of PBI to monitor closely include CSF leak and infection.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
FormalPara Clinical ScenarioAn otherwise healthy 21-year-old male in full protective gear was involved in a motorcycle accident travelling approximately 35 mph, whereby he crashed over an embankment and fell onto a tree. A tree branch penetrated his helmet visor and subsequently his cranial vault via the orbital cavity. Upon arrival to the Emergency Department (ED), he was found to have a large wood fragment penetrating his right orbit. On examination, he was awake, oriented, and following commands without focal neurological deficits.
1 History and Neurologic Exam
Traumatic brain injury (TBI) can be characterized by its severity (mild, moderate, severe) and mechanism (blunt versus penetrating). Penetrating brain injury (PBI) can be further classified as missile or non-missile, where missile PBI includes high velocity projectiles such as bullets and shrapnel, and non-missile PBI consists of penetration of the skull and brain with any low-velocity object such as a knife or, in this case, a piece of wood. Between 2000 and 2019, the Department of Defense estimates there were 5,388 penetrating brain injuries and 422,405 closed head injuries across all branches of the U.S. Military worldwide [1]. Approximately 10% (26,871) of 268,645 TBI patients in a 5-year retrospective study (2010–2014) using the Trauma Quality Improvement Program database were classified as having penetrating injuries [2]. A recent review of patients with craniocerebral gunshot wounds—the most common mechanism of civilian PBI—found a mortality rate of 66–90% prior to hospital arrival; among those reaching medical care, 50% will survive [3, 4]. In one retrospective review of 119 patients admitted to the hospital with craniocerebral gunshot wound, mortality was 49% with 19% achieving a favorable outcome [5]. Conversely, analysis of the Brain Trauma Foundation TBI-trac® database of 2,513 patients who sustained severe non-penetrating TBI who had a GCS motor score >2 with at least one reactive pupil, 14-day mortality was 23% [6]. In the CRASH-3 study evaluating the use of tranexamic acid for patients with TBI and admission GCS <13 or CT evidence of any intracranial hemorrhage, mortality among patients with mild to moderate TBI (GCS 9–15) was 6.6% and mortality in the severe TBI group (GCS 3–8) was 39.8% 28 days after injury [7]. Overall, compared to closed head trauma, PBI is less prevalent and is associated with a significantly worse prognosis. Within PBI, there are often differences in clinical characteristics of patients presenting with missile versus non-missile injuries. However, current clinical data do not support dichotomizing the two injury mechanisms for the purposes of clinical management.
The most immediate consideration in this or any patient with PBI is management of airway, breathing, and circulation in the trauma bay. The patient should be deemed hemodynamically stable prior to initiation of cranial imaging. When possible, a basic neurological examination assessing mental status, cranial nerves, and gross motor strength will take place concurrent with hemodynamic stabilization and prior to administration of sedatives or paralytics, such as those required for intubation or severe agitation. Additionally, a focused medical history should be elicited from the patient, if possible, or a relative.
There are several pieces of patient history that must be elicited upon arrival for any patient with head trauma with known or suspected PBI:
-
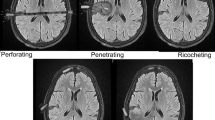
Mechanism of injury: Determine if the injury is missile or non-missile PBI. There is far greater kinetic energy in missile injury and thus more transfer of energy to and destruction of brain tissue. If the patient suffered a missile injury, especially a gunshot wound, the distance from which the patient was shot and the caliber of bullet can provide more information about the degree of kinetic energy transfer and associated underlying parenchymal injury.
-
Field examination and course: The gross neurological examination in the field is important to obtain from the primary responder upon arrival to the ED. A change in neurological status such as a decrease in GCS score between the time of initial traumatic incident to arrival in the ED could signal a rapidly progressive space-occupying lesion such as a hematoma. Additionally, loss of consciousness and duration of such an episode should be relayed to the examining physician.
-
Past medical and surgical history: Bleeding disorders and coagulopathies will require physicians to pay special attention to optimizing blood clotting in the setting of intracerebral hemorrhage.
-
Medications: The most pertinent medication history to elicit is regarding the use of antiplatelets and anticoagulants, as use of these agents can exacerbate bleeding.
-
Drug or alcohol use: Recent intoxication with drugs or alcohol can cloud the clinical examination. Routine drug screening is recommended, as elicit drug use and polypharmacy can cause altered mental status unrelated to brain injury.
Following the initial trauma evaluation and hemodynamic stabilization of the patient, a focused neurological examination should assess mental status, cranial nerve function, gross motor strength, sensation, and reflexes. Additionally, the primary neurosurgical concern to be evaluated in a patient with obvious or suspected PBI is underlying injury to the cranial vault and its contents. The integrity of the orbit, skull base, calvarial bone, and skin should be assessed, particularly at the site of cranial penetration. In the case of injury to the skull base, the clinician should thoroughly assess the patient for rhinorrhea and otorrhea. The entry site (and possibly a corresponding exit site) should be inspected carefully for blood, brain, and CSF and then cleaned thoroughly and covered with a sterile dressing to avoid communication between the atmosphere and the central nervous system. Involvement of the orbit or ear should prompt consultation of ophthalmology and otolaryngology, respectively.
In this particular case, the patient was found to be neurologically intact except for loss of vision in his right eye secondary to a tree branch completely obliterating the right globe with an unknown depth of penetration into the orbit and possibly the cranial vault (Fig. 4.1). The object was not moved or removed, and his right eye and protruding branch fragment were covered with a sterile dressing. The periorbital area was auscultated for a bruit, which, if found, would indicate a possible traumatic carotid-cavernous fistula. In addition to a full trauma evaluation in the ED, the ophthalmology service was consulted.

The patient initially presented to the ED with a large wood fragment penetrating his right orbit and an abrasion above his right eye
2 Differential Diagnosis
The diagnosis of PBI is self-evident at presentation and does not lend itself to the exercise of formulating a differential diagnosis. However, it is worthwhile to consider the range of injuries that are potentially associated with PBI, including direct injury to brain parenchyma along the tract of the object, extra-axial injury (SDH, EDH), intra-axial injury (tSAH, ICH, IVH), as well as vascular complication such as traumatic aneurysms/pseudoaneurysms and arteriovenous fistulas. The incidence of traumatic aneurysms ranges from 3.2% to 60% among several small studies [8,9,10]. A retrospective review of 55 consecutive patients with missile (43 gunshot wounds) and non-missile (7 stab wounds, 4 nail gun accidents, 1 impaled by wooden piece) PBI and diagnostic subtraction angiography revealed the following risk factors associated with arterial injury: entry wound over the frontobasal-temporal regions, wound trajectory involving bilateral hemispheres, wound trajectory in proximity to the Circle of Willis (<2 cm), SAH, and IVH. Patients presenting with gunshot wounds with a trajectory proximal to the Circle of Willis were far more likely to have an arterial injury when compared with the PBI cohort as a whole (OR 6.8 for all PBI, OR 13.3 for gunshot wounds) [11].
3 Diagnostic Evaluation
3.1 Imaging Studies
3.1.1 CT
Initial diagnostic evaluation after the patient is hemodynamically stable is performed with a non-contrast head CT. This study will provide gross information about the extent and anatomical location of intracranial injury, as well as the location of the foreign body if still present in the cranial vault.
3.1.2 Cerebrovascular Imaging
A CT angiogram of the head and neck or digital subtraction angiography (DSA) of the head and neck is indicated in PBI, whether missile or non-missile, when the foreign body passes through or near a large named artery, passes near dural sinuses, or there is evidence of arterial bleeding that could be controlled with intervention. A retrospective review comparing CTA to DSA in 56 patients with both missile (48/56 gunshot wounds) and non-missile PBI who underwent both studies revealed the sensitivity and specificity of CTA to be 72% and 63%, respectively, when compared to the gold standard DSA for identifying penetrating cerebrovascular injuries [12].
3.1.3 Spine Imaging
If the injury is associated with a fall or traumatic whiplash injury of the cervical spine, a non-contrast CT of the cervical spine should be obtained to rule out acute fracture or subluxation.
3.1.4 MRI
An MRI study is both time-consuming and prohibited in patients with PBI involving metal. It is infrequently used in the initial diagnostic algorithm for workup of PBI. However, MRI can be used in the non-emergent setting for patients presenting with PBI by a wooden foreign body.
This particular patient’s initial imaging consisted of a CT/CT angiogram head and neck and revealed the following: a linear foreign body object (measuring 7.1 cm × 1.7 cm) with intrinsic low density, penetrating the right orbit into the right frontal lobe; intraparenchymal hemorrhage in the right frontal lobe with associated vasogenic edema; displacement of the right globe inferiorly with herniation of the inferior rectus muscle and orbital fat into the right maxillary sinus; and multiple facial fractures, including a comminuted right superior orbital fracture, right orbital floor fracture, and right medial orbit fracture of the lamina papyracea with hemorrhage into the ethmoid air cells (Fig. 4.2). CTA showed patent anterior and posterior intracranial circulation, without evidence of flow-limiting stenosis or cerebral aneurysm. Dural venous sinuses were found to be patent. CT cervical spine was negative for acute fracture or subluxation. MRI was deferred, as the patient required emergent surgical intervention.

CT findings upon arrival to the ED. (a–a″) Sequential axial non-contrast CT scan slices demonstrating a hypodense object penetrating the right orbit with associated hematoma. (b–b′) Corresponding CT bone windows demonstrating fractured bone fragment penetrating the brain parenchyma. (c) Sagittal view of the wood object penetrating the right orbit and brain parenchyma
3.2 Laboratory Studies
Laboratory studies should include a basic metabolic panel, complete blood count, coagulation studies, and a type and screen in the event the patient is hemodynamically unstable or requires surgical intervention. If the patient has increased urine output concerning for diabetes insipidus, a urine specific gravity and urine electrolytes should be obtained.
4 Clinical Decision-Making and Next Steps
4.1 Trauma Bay Management
4.1.1 ICP Management
There is a paucity of evidence evaluating the use of ICP monitoring in patients with PBI. When the Penetrating Brain Injury Guidelines were published in 2001, there were insufficient data to support treatment guidelines for monitoring ICP in this patient population [13]. However, the literature suggests that increased ICP is associated with worse outcomes, as is the case in blunt traumatic brain injury. Patients should be closely monitored for signs of increased ICP, and, without evidence for or against ICP monitoring in this population, we apply the Brain Trauma Foundation guidelines for ICP monitoring and management to the PBI population.
4.1.2 Seizure Prophylaxis
The use of anticonvulsants after PBI has not been systematically evaluated in large, controlled studies. Aarabi et al. retrospectively evaluated 489 patients from the Iran-Iraq War with PBI; 32% developed epilepsy during the study period [14]. Multivariate analysis revealed Glasgow Outcome Score and presence of a motor deficit to be significant predictors of late post-traumatic epilepsy. Patients with PBI disrupting brain cortex should be placed on a 7-day course of prophylactic anticonvulsants, consistent with the current Brain Trauma Foundation TBI guidelines.
4.1.3 Antibiotics
Use of prophylactic antibiotics in PBI varies significantly, as robust data supporting the use and type of agent is lacking. However, cephalosporins are the most preferred antibiotics among historical reviews addressing antibiotics in the last 30 years [15]. The British Society for Antimicrobial Chemotherapy performed an extensive review of the literature regarding antimicrobial use in penetrating craniocerebral injuries in both civilian and military incidents and recommends that broad-spectrum antibiotic prophylaxis is necessary. They recommend IV cefuroxime 1.5 g, then 750 mg every 8 h with IV metronidazole 500 mg every 8 h. Administration should begin as soon as possible after injury and continue for 5 days [16].
4.1.4 Foreign Body Management
If the foreign body is still embedded in the patient and protruding from the head, careful planning is necessary to remove the object. The object should be stabilized during transport to imaging and the operating room. However, fragments of the penetrating object should not be surgically removed if it puts brain tissue at risk.
4.2 Operative Indications
There are no well-established guidelines for surgical intervention for patients suffering from missile or non-missile PBI. Several small studies have used criteria such as GCS, size of SDH/EDH/ICH, midline shift, and cranial nerve exam to determine when to consider surgery. When considering surgical intervention, there are two primary goals: manage malignant intracranial hypertension and isolate the CNS from the atmosphere at the site of penetration and exit, if one is present. To address the second goal, foreign objects that remain protruding from the skull must be removed or amputated to close the dura and skin. Additionally, if the dura does not close spontaneously or there is a large defect, operative intervention may be required to obtain a watertight dural seal to prevent infection and ongoing CSF leak.
In this particular case, the patient was administered 2 g ceftriaxone upon arrival in the ED. At that time, his neurological examination was reassuring, and there were no concerns for elevated ICP. Pain in his orbit was managed with IV fentanyl. He was taken to the operating room for a right frontal craniotomy for removal of foreign object, wound washout, repair of CSF leak and repair of right anterior cranial base with the assistance of ophthalmology. A piece of wood was sent for culture (Fig. 4.3). The patient did not require enucleation, as the globe was intact and displaced into the maxillary sinus.

Intraoperative images demonstrating the (a) the fragment in situ, (b) the orbit after fragment removal, and (c) the removed foreign body
The patient was admitted to the ICU for monitoring, loaded with levetiracetam (with a plan for a 7-day prophylactic course), and started on a 7-day course of vancomycin, cefepime, and metronidazole. He was transferred to the floor in stable condition, and the infectious disease team was consulted to assist with transitioning to oral antibiotics. The wood fragment sent for culture from the OR grew very rare coagulase negative Staphylococcus. Infectious diseases recommended 14 days of oral cephalexin and levofloxacin. The patient was discharged home on postoperative day 6. On postoperative day 10, ophthalmology performed a temporary right tarsorrhaphy.
4.3 Complications
4.3.1 CSF Leak
CSF leaks are common complications of PBI, and they have been reported to occur in as many as 28% of patients in one series of 163 consecutive military PBI cases [17]. They are associated with higher risk of infection [18, 19] and, in turn, mortality. As such, all CSF leaks—regardless of location (entry site, exit site, or sinus injury/temporal bone injury)—should be repaired primarily with a watertight closure if they do not close spontaneously or respond to lumbar drainage. The use of allograft for watertight closure should give the surgeon pause as the foreign body can become infected in a PBI wound considered to be contaminated.
4.3.2 Infection
Both CSF leak and retained foreign body put patients at risk of wound infection and abscess. In a prospective study of 192 patients with non-missile penetrating brain injury, 27 patients (14%) developed an infection. Infection was associated with delayed admission to the hospital more than 24 h, no antibiotic prophylaxis, and weapon/foreign object in situ. Multivariate analysis did not reveal surgical intervention to be independently associated with infection [20].
On postoperative day 18, the patient had a near syncopal episode and was brought to an outside hospital emergency department where he had a mild leukocytosis and was hypotensive. There was fluid draining from his right eye. He was transferred to our institution for concern of orbital cellulitis and possible sepsis. He was started on vancomycin, piperacillin-tazobactam, and fluconazole prior to transfer. Upon arrival, his antibiotic regimen was changed to vancomycin, cefepime, and metronidazole. MRI brain and orbit pre- and post-gadolinium were obtained, revealing an approximately 3 × 3 cm right frontal postsurgical cavity with significant restricted diffusion without a clear fluid-fluid level. There was peripheral enhancement—suspicious for cerebral abscess—with contiguous extension into the right orbit (Fig. 4.4). The original bone flap was removed, and a dural incision revealed granular and purulent material consistent with infected brain parenchyma/abscess. Contents of the surgical cavity were evacuated, cultures were sent, the area was irrigated, and a decision was made to perform a complete tarsorrhaphy to seal the orbit and thus the intracranial cavity from the atmosphere. His cultures did not grow bacterial or fungal colonies, and he was discharged on his intravenous antibiotic regimen. He recovered well and did not have recurrence of his abscess.

Postoperative infection demonstrated on brain MRI with and without contrast. From left to right: axial T1 post-contrast, coronal T1 post-contrast, axial DWI, and axial flair series
5 Clinical Pearls
-
Initial management of PBI should be according to ACS and Brain Trauma Foundation guidelines.
-
Vascular imaging may be necessary prior to considering neurosurgical intervention, especially when a foreign body passes near large named vasculature or there is evidence of arterial bleeding that could be controlled with intervention. CTA and DSA are the imaging modalities of choice, with DSA being the gold standard to establish parenchymal and vascular injury secondary to PBI.
-
The optimal medical management of PBI, including ICP monitoring and seizure prophylaxis, has not been well-studied in large trials and currently reflects the well-established Brain Trauma Foundation guidelines for TBI.
-
Surgical management should focus on removing foreign objects protruding from the skull, while avoiding unnecessary debridement and retrieval of deep retained fragments, which could cause further parenchymal injury.
-
CSF leaks and infections are common complications associated with PBI and should be monitored closely.
References
https://health.mil/About-MHS/OASDHA/Defense-Health-Agency/Research-and-Development/Traumatic-Brain-Injury-Center-of-Excellence/DoD-TBI-Worldwide-Numbers. Accessed 12/2/2020.
Skarupa DJ, Khan M, Hsu A, Madbak FG, Ebler DJ, Yorkgitis B, Rahmathulla G, Alcindor D, Joseph B. Trends in civilian penetrating brain injury: a review of 26,871 patients. Am J Surg. 2019;218(2):255–60. https://doi.org/10.1016/j.amjsurg.2018.11.034. Epub 2018 Nov 27.
Rosenfeld JV, Bell RS, Armonda R. Current concepts in penetrating and blast injury to the central nervous system. World J Surg. 2015;39(6):1352–62. https://doi.org/10.1007/s00268-014-2874-7.
Aarabi B, Tofighi B, Kufera JA, Hadley J, Ahn ES, Cooper C, Malik JM, Naff NJ, Chang L, Radley M, Kheder A, Uscinski RH. Predictors of outcome in civilian gunshot wounds to the head. J Neurosurg. 2014;120(5):1138–46. https://doi.org/10.3171/2014.1.JNS131869. Epub 2014 Feb 7.
Gressot LV, Chamoun RB, Patel AJ, Valadka AB, Suki D, Robertson CS, Gopinath SP. Predictors of outcome in civilians with gunshot wounds to the head upon presentation. J Neurosurg. 2014;121(3):645–52. https://doi.org/10.3171/2014.5.JNS131872. Epub 2014 Jul 4.
Roozenbeek B, Chiu YL, Lingsma HF, et al. Predicting 14-day mortality after severe traumatic brain injury: application of the IMPACT models in the brain trauma foundation TBI-trac® New York State database. J Neurotrauma. 2012;29(7):1306–12. https://doi.org/10.1089/neu.2011.1988.
CRASH-3 Trial Collaborators. Effects of tranexamic acid on death, disability, vascular occlusive events and other morbidities in patients with acute traumatic brain injury (CRASH-3): a randomised, placebo-controlled trial. Lancet. 2019;394(10210):1713–23. https://doi.org/10.1016/S0140-6736(19)32233-0. Epub 2019 Oct 14. Erratum in: Lancet. 2019;394(10210):1712.
Levy ML, Rezai A, Masri LS, Litofsky SN, Giannotta SL, Apuzzo ML, Weiss MH. The significance of subarachnoid hemorrhage after penetrating craniocerebral injury: correlations with angiography and outcome in a civilian population. Neurosurgery. 1993;32(4):532–40. https://doi.org/10.1227/00006123-199304000-00007.
Jinkins JR, Dadsetan MR, Sener RN, Desai S, Williams RG. Value of acute-phase angiography in the detection of vascular injuries caused by gunshot wounds to the head: analysis of 12 cases. AJR Am J Roentgenol. 1992;159(2):365–8. https://doi.org/10.2214/ajr.159.2.1632358.
Mansour A, Loggini A, El Ammar F, Ginat D, Awad IA, Lazaridis C, Kramer C, Vasenina V, Polster SP, Huang A, Olivera Perez H, Das P, Horowitz PM, Zakrison T, Hampton D, Rogers SO, Goldenberg FD. Cerebrovascular complications in early survivors of civilian penetrating brain injury. Neurocrit Care. 2020; https://doi.org/10.1007/s12028-020-01106-y. Epub ahead of print.
Bodanapally UK, Saksobhavivat N, Shanmuganathan K, Aarabi B, Roy AK. Arterial injuries after penetrating brain injury in civilians: risk factors on admission head computed tomography. J Neurosurg. 2015;122(1):219–26. https://doi.org/10.3171/2014.9.JNS14679.
Ares WJ, Jankowitz BT, Tonetti DA, Gross BA, Grandhi R. A comparison of digital subtraction angiography and computed tomography angiography for the diagnosis of penetrating cerebrovascular injury. Neurosurg Focus. 2019;47(5):E16. https://doi.org/10.3171/2019.8.FOCUS19495.
Intracranial pressure monitoring in the management of penetrating brain injury. J Trauma Inj Inf Crit Care. 2001;51(2):S12–5.
Aarabi B, Taghipour M, Haghnegahdar A, Farokhi M, Mobley L. Prognostic factors in the occurrence of posttraumatic epilepsy after penetrating head injury suffered during military service. Neurosurg Focus. 2000;8(1):e1. https://doi.org/10.3171/foc.2000.8.1.155.
Kazim SF, Shamim MS, Tahir MZ, Enam SA, Waheed S. Management of penetrating brain injury. J Emerg Trauma Shock. 2011;4(3):395–402. https://doi.org/10.4103/0974-2700.83871.
Bayston R, de Louvois J, Brown EM, Johnston RA, Lees P, Pople IK. Use of antibiotics in penetrating craniocerebral injuries. “Infection in Neurosurgery” Working Party of British Society for Antimicrobial Chemotherapy. Lancet. 2000;355(9217):1813–7. https://doi.org/10.1016/s0140-6736(00)02275-3.
Arendall RE, Meirowsky AM. Air sinus wounds: an analysis of 163 consecutive cases incurred in the Korean War, 1950-1952. Neurosurgery. 1983;13(4):377–80. https://doi.org/10.1227/00006123-198310000-00005.
Gönül E, Baysefer A, Kahraman S, Ciklatekerlioğlu O, Gezen F, Yayla O, Seber N. Causes of infections and management results in penetrating craniocerebral injuries. Neurosurg Rev. 1997;20(3):177–81. https://doi.org/10.1007/BF01105561.
Meirowsky AM, Caveness WF, Dillon JD, Rish BL, Mohr JP, Kistler JP, Weiss GH. Cerebrospinal fluid fistulas complicating missile wounds of the brain. J Neurosurg. 1981;54(1):44–8. https://doi.org/10.3171/jns.1981.54.1.0044.
Harrington BM, Gretschel A, Lombard C, Lonser RR, Vlok AJ. Complications, outcomes, and management strategies of non-missile penetrating head injuries. J Neurosurg. 2020;19:1–9. https://doi.org/10.3171/2020.4.JNS20122. Epub ahead of print.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2022 The Author(s), under exclusive license to Springer Nature Switzerland AG
About this chapter

Cite this chapter
Harris, O.A., Herrick, D.B. (2022). Penetrating Brain Injury. In: Raksin, P.B. (eds) Acute Care Neurosurgery by Case Management. Springer, Cham. https://doi.org/10.1007/978-3-030-99512-6_4
Download citation
DOI: https://doi.org/10.1007/978-3-030-99512-6_4
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-99511-9
Online ISBN: 978-3-030-99512-6
eBook Packages: MedicineMedicine (R0)