
Abstract
Here, we describe the pathogenesis, treatment recommendations and surgical considerations pertaining to penetrating brain injuries. These injuries have a high fatality rate, but patients who survive the acute phase can have favourable outcomes. Combinations of primary injuries can be challenging to manage, and high energy injuries are often associated with detrimental intracranial hypertension.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
FormalPara RecommendationsLevel I
There are insufficient data to support a Level I recommendation for this topic.
Level II
There are insufficient data to support a Level II recommendation for this topic.
Level III
Patients with penetrating brain injuries that are otherwise stabilized and demonstrate neurological function or deterioration referable to a mass lesion should be considered for surgery.
1 Overview
Penetrating brain injuries (PBIs) have high fatality rates. Patients who survive the initial phase can however demonstrate favourable outcomes. The primary injuries can entail a combination of scalp lesions, cranial fractures, intracranial haematomas and cerebral lacerations. High energy PBIs frequently encompass distant lesions and are often followed by a detrimental increase in intracranial pressure (ICP).
There is no defined threshold for whom surgery should be withheld, but the patient must have a possibility of a reasonable functional outcome. Patients with devastating brain injuries and/or high probability of a poor outcome should generally not be subjected to surgical treatment.
Tips, Tricks and Pitfalls
-
Consider ICP monitoring and/or EVD.
-
Carefully plan the way in and out (vascularity, exposure, wound closure).
-
If you plan a skin flap, you have to take the wound into consideration: is it most suitable to incorporate the wound in the skin incision or is it better to place the incision around it, with a broad base to ensure a sufficient blood supply to the entire flap?
-
Perform a thorough debridement of all tissue layers.
-
If possible, do not add foreign material.
-
Antibiotics and antiepileptic medication should be liberally applied.
2 Background
2.1 Pathogenesis
The majority of PBIs in the civilian setting are caused by low-velocity gunshot wounds to the head (GSWH) (Potapov et al. 2001). These injuries have a mortality rate of more than 90% (Aarabi et al. 2014). However, survivors may experience a favourable recovery. Significant factors related to outcome in PBI are admission Glasgow Coma Scale (GCS) score, missile trajectory, pupillary status and patency of basal cisterns (Aarabi et al. 2014).
Shrapnel (fragments thrown out by an exploding bomb or shell), and not GSWH, is the major cause of PBIs in military conflicts. The overall mortality rate is therefore lower; it is generally reported to be around 20% (Potapov et al. 2001).
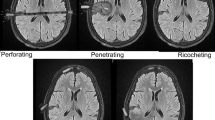
A combination of soft tissue injuries, fractures and parenchymal lesions may constitute the primary injuries from GSWH. The impact velocity of a projectile reflects the true wounding potential, and deformation and fragmentation of the missile enhance energy delivery to the tissue. Comminute fractures may injure the directly underlying structures, and bone fragments may be driven into the brain as secondary projectiles. Brain injuries can occur along the path of the projectile(s), as well as in more distant locations, due to pressure waves and coup/contrecoup lesions. A rapid rise in ICP may follow a GSWH.
2.2 Treatment Options
No surgical intervention is generally warranted for patients with a post-resuscitation GCS score of 3, dilated and nonreactive pupils and no significant mass lesion on the CT scan. Patients that are otherwise stabilized and demonstrating some neurological function (motor or brain stem) or deterioration referable to a mass lesion should be considered for urgent surgical treatment.
Small entrance bullet wounds to the head can be treated with local wound care and closure if the scalp is not devitalized and there are no surgical intracranial lesions. Treatment of more extensive wounds requires extensive debridement before primary closure to secure a watertight wound. In the presence of significant mass effect, debridement of necrotic brain tissue and safely accessible bone fragments, together with evacuation of intracranial haematomas with significant mass effect, is recommended. A minimal invasive approach is prudent in the absence of significant mass effect (Potapov et al. 2001).
If possible, any protruding part of a foreign body should not be removed before the patient is in the operating room.
Infection is an important secondary complication, and liberal use of antibiotics is recommended.
Seizures in the acute phase are unfavourable and liberal use of antiepileptic drugs (AEDs) is recommended. About 50% of survivors will suffer seizures and require antiepileptic medication.
The neurosurgeon must carefully consider the need for intracranial pressure measurement and/or external ventricular drainage, in addition to the primary surgical treatment.
2.3 Surgical Considerations
The cranium is examined for external injuries. Thorough irrigation of the wound site(s) is performed. Consultation with a plastic surgeon may be warranted in selected cases. The skin incision must be carefully planned in order to, first, ensure vascularity and enable wound closure following excision of devitalized tissue and, second, to secure sufficient exposure of the bony defect and underlying haematomas. The cranial opening should extend well beyond the visible bone injury until intact dura is visualized.
Herniated brain tissue and the intracerebral penetration tract are flushed through the dural lesion, and accessible necrotic tissue, bone fragments and foreign bodies are gently removed.
The dural opening may need to be enlarged to accommodate adequate debridement and haematoma evacuation. A thorough exploration must be performed, but preservation of viable brain tissue supersedes removal of deeply located fragments (Potapov et al. 2001). Haemostasis is preferably ensured by bipolar electrocautery and dural repair by autologous grafts (e.g. temporalis fascia or pericranium).
Bone replacement should be performed in case of no present or anticipated future significant brain swelling. High-velocity injuries are often associated with substantial oedema development, and it may be wise not to replace the bone in these cases. Before replacement of the bone flap or fragments, ample debridement and cleaning must be secured. Foreign materials must be utilized at a minimum, but miniplates, titanium wires and craniofix devices are often needed to assemble multiple bony fragments. The importance of meticulous scalp closure is previously stated.
References
Aarabi B, Tofighi B, Kufera JA, Hadley J, Ahn ES, Cooper C, Malik JM, Naff NJ, Chang L, Radley M, Kheder A, Uscinski RH. Predictors of outcome in civilian gunshot wounds to the head. J Neurosurg. 2014;120:1138–46.
Potapov AA, Shahinian GG, Kravtchouk AD. Surgical management of penetrating brain injury. J Trauma. 2001;51:16–25.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2020 Springer Nature Switzerland AG
About this chapter

Cite this chapter
Sundstrøm, T., Helseth, E., Wester, K.G. (2020). Surgical Management of Penetrating Brain Injuries. In: Sundstrøm, T., Grände, PO., Luoto, T., Rosenlund, C., Undén, J., Wester, K. (eds) Management of Severe Traumatic Brain Injury. Springer, Cham. https://doi.org/10.1007/978-3-030-39383-0_25
Download citation
DOI: https://doi.org/10.1007/978-3-030-39383-0_25
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-39382-3
Online ISBN: 978-3-030-39383-0
eBook Packages: MedicineMedicine (R0)