
Abstract
Spasticity arises after a neurological injury; hence it clearly has a neural basis. However, it has many definitions and manifestations, and the underlying mechanisms are still not clearly understood. This chapter reviews the definitions of spasticity, the time course of its development, and the types of neural injury that may cause it by disinhibiting inhibitory brainstem pathways as well as by facilitating excitatory brainstem pathways that result in an excitatory-inhibitory imbalance in the spinal cord interneuronal network. The descending pathways modulate persistent inward currents via serotonin and norepinephrine, which provide a low-level depolarizing synaptic drive to the resting motoneuron pool resulting in increased afferent sensitivity and can account for hyperreflexia. However, the abnormal brainstem descending inputs and persistent inward currents cannot fully account for other spasticity-related motor impairments, such as muscle stiffness.
…dissolution is not only a “taking off” of the higher but is at the very same time a “letting go” of the lower.
– John Hughlings Jackson,Croonian lectures, Royal College of Physicians, London, 1884.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others

Keywords
-
Spasticity arises after a neurological injury; hence it clearly has a neural basis. However, it has many definitions and manifestations, and the underlying mechanisms are still not clearly understood.
-
This chapter reviews the definitions of spasticity, the time course of its development, and the types of neural injury that may cause it by disinhibiting inhibitory brainstem pathways as well as by facilitating excitatory brainstem pathways, that result in an excitatory-inhibitory imbalance in the spinal cord interneuronal network.
-
The descending pathways modulate persistent inward currents via serotonin and norepinephrine, which provide a low-level depolarizing synaptic drive to the resting motoneuron pool resulting in increased afferent sensitivity and can account for hyperreflexia.
-
However, the abnormal brainstem descending inputs and persistent inward currents cannot fully account for other spasticity-related motor impairments, such as muscle stiffness.
Definition of Spasticity
It is well-known that damage to the descending motor pathways anywhere from the cerebral cortex to the lower end of the spinal cord can give rise to a set of symptoms called the upper motor neuron syndrome. John Hughlings Jackson observed in the late nineteenth century that neural injury often leads to dual symptomatology. For example in hemiplegia, in addition to loss of movement (negative symptoms), excess activity also develops (positive symptoms) such as increased tendon reflexes and excess muscle tone, which he attributed to the “release” of the lower centers from control by the damaged higher centers that are “taken-off” [1]. The idea of “release” phenomena characterizing the upper motor neuron syndrome continues to inform our understanding of spasticity.
In fact, Lance and colleagues defined spasticity at a consensus symposium in 1980 [2] as:
a motor disorder characterized by a velocity-dependent increase in tonic stretch reflexes with exaggerated tendon jerks, resulting from hyperexcitability of the stretch reflex as one component of the upper motor neuron syndrome.
Subsequently, Pandyan et al. [3] attempted to validate Lance’s definition by reviewing the literature since, and concluded that spasticity is not a pure motor disorder and that it does not result exclusively from hyperexcitability of the stretch reflex. The changes in resistance to imposed passive movement were also not found to be uniquely related to increased muscle activity, and the phenomenon of velocity dependence was not exclusive to stretch reflex hyperexcitability. Hence spasticity was redefined as:
disordered sensorimotor control, resulting from an upper motor neuron lesion, presenting as intermittent or sustained involuntary activation of muscles.
This definition suggests that spasticity is a disorder of sensorimotor control, rather than a motor disorder alone. Furthermore, it suggests that spasticity presents as muscle overactivity, rather than solely as stretch reflex hyperexcitability, which had major implications for treatment that was then directed to reducing muscle overactivity.
A more recent definition of spasticity proposed by Li et al. [4] is even broader, and specifies a neuroanatomical substrate for the hyperexcitability, rather than the release of control by the higher centers as alluded to by Hughlings Jackson. By this definition, spasticity is:
manifested as velocity- and muscle length–dependent increase in resistance to externally imposed muscle stretch. It results from hyperexcitable descending excitatory brainstem pathways and from the resultant exaggerated stretch reflex responses. Other related motor impairments, including abnormal synergies, inappropriate muscle activation, and anomalous muscle coactivation, coexist with spasticity and share similar pathophysiological origins.
Abnormal excitability of the stretch reflex is still the central mechanism as per this latest definition of spasticity. However, it also attributes spasticity-related motor impairments to the excitatory brainstem pathways.
Time Course of the Development of Spasticity
Although hyperreflexia is central to defining spasticity, several studies have shown nonreflex-related resistance to movement in patients with “spasticity” [5,6,7]. Furthermore, although hyperreflexia is elicited relatively early after injury, the resistance to passive movement measured using the Modified Ashworth Scale (MAS), which is commonly used to assess spasticity clinically, tends to increase in prevalence over the ensuing weeks and months [8,9,10]. Even mild hyperreflexia early on is an important predictor of severe spasticity and increased resistance to passive movement later [11, 12], suggesting that hyperreflexia may trigger a cascade of events that lead to a build up of the resistance to movement. In a retrospective study of chronic stroke survivors with moderate-to-severe upper limb motor impairment, 97% of subjects demonstrated increased resistance to passive movement which was associated with impaired motor control [13]. Thus, it is important to understand the characteristics of the neurologic injury that lead to the development of spasticity and the ensuing resistance to movement to initiate measures for prevention and early treatment. Untreated, spasticity leads to fatigue, pain, sleep problems, and urinary dysfunction among others, affecting physical health [14], and restricting activities of daily living (ADL) and mobility that contribute to disability and increased health care costs [15, 16].
What Types of Neural Injury Lead to the Development of Spasticity?
Several recent studies have shown a positive correlation between spasticity and the overall degree of injury to the sensorimotor system – the greater the lesion volume and severity of injury, the greater the likelihood of developing spasticity [17]. However, small lesions involving specific regions of the brain such as the putamen, internal (posterior limb) and external capsule, thalamus, and insula, which are involved in sensorimotor processing, have also shown to be correlated with the degree of spasticity [18]. Note that in these studies, the resistance to passive movement on the MAS, which is not specific to the neural component, was used to measure spasticity (see Chaps. 3 and 4). More recently, the velocity-dependent neural component of hand spasticity was shown to be related to lesion load of the corticospinal tract (CST), after controlling for motor impairment and lesion volume [11].
To fully comprehend the effect of neural injury, especially given the strong correlation between motor impairment and spasticity reported recently [13], it is helpful to review the origin and termination of the CST, which modulates brain stem and spinal cord activity. The CST originates from a wide range of cortical areas having different functions, including the primary motor cortex (M1) which is involved in the execution of movement, the dorsal (PMd) and ventral (PMv) premotor areas involved in the sensory guidance of movement, the supplementary motor area (SMA) involved in planning and coordination of internally generated movement sequences, the cingulate motor areas involved in emotional aspects of voluntary movement, including changes in autonomic function [19], and corticospinal projections from the parietal lobe including the primary somatosensory cortex, posterior parietal cortex, and parietal operculum (SII) [20, 21].
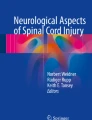
The termination of the corticospinal projections within the spinal gray matter is also varied (Fig. 1.1) [22,23,24]. Projections from the somatosensory cortex terminate mainly in the more dorsal parts of the spinal gray matter (Rexed laminae I–V) and are involved in the descending control of sensory afferent input. These projections are an important source of presynaptic inhibition of primary sensory afferent fibers [25, 26], and are responsible for sensory reafference or gating of inputs arising from one’s own movement [27, 28]. Projections from M1 target most areas of the intermediate zone of the spinal cord gray matter (Rexed lamina VII). These are the indirect oligosynaptic projections that mediate corticospinal input to motor neurons via a premotoneuronal network [22]. Inputs to the premotoneuronal network originate in a variety of descending motor pathways, in ascending and descending propriospinal pathways, in local segmental interneurons, as well as in sensory afferent inputs from the periphery. Integration of information in this network is critical to achieve the precise timing and balance of activity in the motoneuron pool, contributing to highly flexible movement responses in the healthy state [29]. Recent evidence suggests that corticospinal projections from the dorsal and ventral premotor areas terminate in laminae VII and VIII, and govern proximal upper limb musculature involved in postural stabilization and control of the proximal limb during reaching and grasping through the indirect oligosynaptic neural networks [30]. These projections, as well as the corticospinal projections from the leg area of M1 to motoneurons of more proximal leg muscles, are bilateral [30, 31]. Injury to these pathways can account for increased spasticity when standing [32, 33].

Schematic diagram of the general anatomical organization of the spinal cord adapted from Kuypers [23]. (a) The ventral horn consists of lamina IX (green), the intermediate zone laminae V, VI, VII, VIII, and the reticulated marginal border (RMB) (yellow), and the dorsal horn laminae I–III and IV (orange). (b) The Rexed laminae are further subdivided into 20 subdivisions in each half of the spinal cord. The blue shaded regions of laminae VII and IX represent spinal components of Kuypers “lateral motor system” [24]. The red shaded region of lamina VII and lamina VIII constitute parts of his “medial motor system”. (From Morecraft et al. [22], with permission)
In contrast, direct cortico-motoneuronal connections in the ventral horn (Rexed lamina IX) originate from both M1 and SMA, but the corticospinal projections from M1 to the hand muscle motor nuclei are denser than those from the SMA [34]. In humans, fast-conducting direct mono-synaptic cortico-motoneuronal connections have been found to be responsible for precision grasp, but not power grasp [35, 36]. Selective lesions of the CST may therefore only impede individuated finger movements as has been shown in monkeys [37].
Thus, injury to the CST at its origin, especially when it involves both sensory and motor areas [38, 39], along its path, or at the level of the spinal cord, regardless of etiology leads to widespread consequences depending on the corticospinal projections affected and their particular function. The function of the CST reflects its origins and terminations and includes: (1) descending control of afferent inputs, including nociception [25, 26]; (2) selection, gating, and gain control of spinal reflexes [40]; (3) direct and indirect excitation of motoneurons [41, 42]; (4) inhibition of motoneurons [43, 44]; (5) autonomic control [45]; (6) long-term plasticity of spinal cord circuits [46]; and (7) trophic functions during development [47, 48]. Individuals who present with spasticity invariably present with symptoms reflecting additional corticospinal dysfunction depending on the pathways affected.
How Does Injury to the Corticospinal Tract Lead to Spasticity?
In 1946, Magoun and Rhines found an area in the brainstem, the ventromedial medullary reticular formation, which when stimulated could inhibit any type of muscle activity, including stretch reflex activity. This region receives facilitatory influences from the premotor cortex [49]. Extensive lesions involving premotor and supplementary motor areas, and/or their projections were found to inhibit the medullary reticular formation, leading to release or disinhibition of stretch reflex activity, causing hyperreflexia [50]. The inhibitory influences from the medullary reticular formation are transmitted to the spinal cord by the dorsal reticulospinal tract (RST), which runs very close to the lateral corticospinal tract. Stimulation of the dorsal RST in decerebrate cats was also shown to inhibit excitability in the spinal interneurons [51, 52]. Section of the dorsal half of the lateral funiculus, which contains the dorsal RST in humans, to treat parkinsonism was also followed by spasticity [53]. This lent further support to the idea that the disruption of cortical inputs to the brainstem, specifically injury to cortico-reticulospinal fibers, and/or damage to the dorsal RST, releases the spinal neural network from inhibitory control causing an imbalance between excitatory and inhibitory inputs [54, 55].
While disinhibition can explain hyperreflexia that is seen soon after injury, the question of what leads to the development of increased resistance to passive movement, abnormal synergies, inappropriate muscle activation, and anomalous muscle coactivation remains. One possibility is that the imbalanced neural excitability becomes amplified through increased facilitatory influences involving alternative brainstem control pathways. Magoun and Rhines also found that stimulation of the reticular formation of the dorsal brain stem (pontine reticular formation) can facilitate or exaggerate any type of muscle activity, including the stretch reflexes [49]. The facilitatory influences from the pontine reticular formation are transmitted to the spinal cord by the medial RST, which along with the vestibulospinal tract (VST) provides excitatory input to the spinal neural network. The VST is thought to play a minor role, as section of the anterior funiculus of the cord to relieve hypertonia resulted in only transient reduction in spasticity [56]. In contrast, extensive unilateral or bilateral anterior cordotomy, which is likely to have destroyed both the VST and the medial RST, was followed by a dramatic reduction in spasticity [57].
Recent studies in monkeys demonstrate that the projections from nonprimary motor cortices (PM and SMA) are denser and end mainly ipsilaterally in the pontine reticular formation, whereas the projections from the primary motor cortex (M1) are less dense and end contralaterally [58]. The importance of the denser ipsilateral projections from the uninjured PM and SMA is that these projections are thought to compensate for injury to the contralateral CST and enable at least partial recovery of motor function in monkeys [59,60,61,62], and in humans with mild impairment [63,64,65,66,67,68]. However, severely impaired individuals also show increased activation of the ipsilesional premotor regions [69,70,71] associated with compensatory movement strategies [72,73,74]. Hence it is hypothesized that the motor overflow from the ipsilesional to the impaired side contributes to increased spasticity and disordered motor control [75]. Indirect support for this hypothesis was noted in an imaging study which showed strong correlation of synergistic arm movements with the functional reorganization in the reticulospinal pathways suggesting a contributory role in the development of compensatory motor strategies [76]. Hence it is suggested that spasticity and the related motor impairments are exacerbated by the ipsilateral excitatory contribution from the medial RST to the spinal neural network as shown by the dashed line in Fig. 1.2 [77].

Schematic diagram illustrating the descending pathways contributing to the medial reticulospinal tract in the pathophysiology of spasticity. The pontine reticular formation receives cortical input primarily from the ipsilateral premotor (PM) cortex and supplementary motor area (SMA), and via the medial reticulospinal tract (RST) provides excitatory descending input to the spinal circuitry. The medullary reticular formation receives cortical input primarily from the contralateral primary motor cortex (M1), and via the dorsal RST provides inhibitory descending inputs to the spinal circuitry. Injury to the corticospinal tract (indicated in red) leads to reduced inhibition of the spinal circuitry via the dorsal RST causing an excitatory-inhibitory imbalance. In addition, it is proposed that the contribution of the contralesional hemisphere to the excitatory medial RST becomes gradually upregulated and unopposed further increasing spinal hyperexcitability. (+) excitatory; (–) inhibitory. (From Li et al. [77], with permission (open access))
Consequences of Excitatory-Inhibitory Imbalance in Spinal Circuitry
The descending RST inputs are primarily mediated by the monoamines serotonin (5-HT) and norepinephrine (NE), which have neuromodulatory effects that correlate with the level of behavioral arousal and/or the behavioral state, for example when awake and in fight or flight situations [78]. These neuromodulatory effects, in turn, have been shown to be mediated via persistent inward currents (PIC). A PIC is a depolarizing current generated by voltage-sensitive channels that stay open as long as the membrane potential remains above the threshold of activation. This persistence stands in marked contrast to the inward currents that generate the action potential, which inactivate within 1–2 ms, even during prolonged membrane depolarization [79]. PICs increase the sensitivity of neurons to both excitation and inhibition – they have strong excitatory actions on motoneurons involved in tonic motor activity, for example in antigravity muscles and other muscle groups associated with gross motor activity. These neuromodulatory inputs have been shown to be critical for the production of high forces and have a major influence on input-output behavior of the whole system [80, 81]. Turning off these sustained outputs also requires considerably large inhibitory inputs [82]. In contrast to their strong excitatory actions on motoneurons, monoamines inhibit many of the synaptic inputs to interneurons [78]. This inhibition is largely presynaptic and focused on sensory afferents that mediate both high- and low-threshold cutaneous inputs [83], and high-threshold muscle afferents [84]. The differential role of monoaminergic actions on motoneurons and interneurons occurs via their action on different receptor subtypes – facilitation of PICs in motoneurons appears to occur via 5HT2 and NE alpha 1 receptors, whereas inhibition occurs via 5HT1b/d and NE alpha 2 receptors [85]. In effect, monoamines increase the sensitivity of motoneurons to both excitation and inhibition in a movement-dependent manner [86]. Accumulating evidence indicates that the movement-related motor excitability is related to coactivation of the sympathetic nervous system and to modulation of afferent inputs [79].
When descending pathways are interrupted following CNS injury, the overall excitability of the spinal motoneuronal pool is initially reduced, producing weakness and flaccidity. However, the acute loss of descending brainstem inhibition of presynaptic afferent inputs, especially cutaneous inputs, is thought to increase intrinsic motoneuron excitability via the development of PICs [87, 88]. At first, these low-threshold polysynaptic inputs do not produce long-lasting reflexes because of lack of motoneuron excitability in a monoamine-deficient state. Over time, the PICs become supersensitive to the residual monoamines below the level of the injury [89], which more than compensate for the monoamine deficiency, leading to the development of large PICs and hyperexcitable motoneurons which trigger sustained motoneuron discharges associated with long-lasting reflexes and muscle spasms to innocuous stimulation, such as gently rubbing the skin or passive movement [88]. In fact, indirect measurements of PIC amplitude from paired motor unit recordings in human subjects suggest that PICs in motor neurons contribute to muscle spasms after spinal cord injury [90]. Pharmacologically blocking the PICs on the motoneurons, without inhibiting the synaptic inputs, can eliminate the long-lasting reflexes [91].
However, in individuals with stroke, PIC estimates have not been found to be larger in spastic-paretic motoneurons, compared with contralateral, and age-matched healthy control motoneurons. Instead, following voluntary isometric contractions, the majority of the low-threshold motor units in spastic-paretic muscles exhibit spontaneous discharges, suggesting that firing changes are likely due to low-level depolarizing synaptic drive to the resting motoneuron pool [92, 93], which can account for hyperreflexia. However, voluntary activation of the spastic-paretic motoneuron pool results in saturation in firing profiles of the individual motor units, and an inability to modulate firing rates [94], suggesting lack of synaptic drive for voluntary muscle activation or paresis. The contradiction in the PIC estimates of the spastic-paretic motorneurons can be reconciled by considering that the net excitability of the alpha motor neuron is achieved via a complex and poorly quantified afferent pool that influences the central state of the cells, which is influenced by the function of both lesioned and nonlesioned areas contributing to the tracts. This is in contrast to the more simplistic view of hyperreflexia described historically (Fig. 1.3) [95, 96].

Schematic illustration of the spinal stretch reflex. (a) The classically described spinal reflex arc demonstrating hyperreflexia (indicated by the arrows) after corticospinal tract injury. (b) Contemporary summary of the afferent pool of the alpha motor neuron showing significant contributions from the spinal interneuron pool whose inputs include projections received from the corticospinal tract. (From Florman et al. [95], with permission (open access))
Conclusion
Injury to the central nervous system results in both negative symptoms such as paresis and positive symptoms such as spasticity. While findings from both animal studies and studies with human subjects support the role of the dorsal reticulospinal tract in producing hyperexcitability of the spinal stretch reflexes, a more contemporary view is that the overall state of excitability of the spinal afferent pool is influenced by cortical input from both lesioned and nonlesioned areas and their descending pathways.
References
Walshe FM. Contributions of John Hughlings JACKSON to neurology. A brief introduction to his teachings. Arch Neurol. 1961;5:119–31.
Lance JW. Symposium synopsis. In: Feldman RG, Young RR, Koella WP, editors. Spasticity: disordered motor control. Chicago: Year Book Medical Publishers; 1980.
Pandyan AD, Gregoric M, Barnes MP, Wood D, Van Wijck F, Burridge J, et al. Spasticity: clinical perceptions, neurological realities and meaningful measurement. Disabil Rehabil. 2005;27(1–2):2–6.
Li S, Francisco GE, Rymer WZ. A new definition of poststroke spasticity and the interference of spasticity with motor recovery from acute to chronic stages. Neurorehabil Neural Repair. 2021;35(7):601–10. https://doi.org/10.1177/15459683211011214.
Schindler-Ivens SM, Shields RK. Soleus H-reflex recruitment is not altered in persons with chronic spinal cord injury. Arch Phys Med Rehabil. 2004;85(5):840–7.
Sinkjaer T, Toft E, Larsen K, Andreassen S, Hansen HJ. Non-reflex and reflex-mediated ankle joint stiffness in multiple sclerosis patients with spasticity. Muscle Nerve. 1993;16(1):69–76.
Willerslev-Olsen M, Lorentzen J, Sinkjaer T, Nielsen JB. Passive muscle properties are altered in children with cerebral palsy before the age of 3 years and are difficult to distinguish clinically from spasticity. Dev Med Child Neurol. 2013;55(7):617–23.
Nam KE, Lim SH, Kim JS, Hong BY, Jung HY, Lee JK, et al. When does spasticity in the upper limb develop after a first stroke? A nationwide observational study on 861 stroke patients. J Clin Neurosci. 2019;66:144–8.
Sommerfeld DK, Eek EU, Svensson AK, Holmqvist LW, von Arbin MH. Spasticity after stroke: its occurrence and association with motor impairments and activity limitations. Stroke. 2004;35(1):134–9.
Dornak T, Justanova M, Konvalinkova R, Riha M, Muzik J, Hoskovcova M, et al. Prevalence and evolution of spasticity in patients suffering from first-ever stroke with carotid origin: a prospective, longitudinal study. Eur J Neurol. 2019;26(6):880–6.
Plantin J, Pennati GV, Roca P, Baron JC, Laurencikas E, Weber K, et al. Quantitative assessment of hand spasticity after stroke: imaging correlates and impact on motor recovery. Front Neurol. 2019;10:836.
Sunnerhagen KS, Opheim A, Alt MM. Onset, time course and prediction of spasticity after stroke or traumatic brain injury. Ann Phys Rehabil Med. 2019;62(6):431–4.
Pundik S, McCabe J, Skelly M, Tatsuoka C, Daly JJ. Association of spasticity and motor dysfunction in chronic stroke. Ann Phys Rehabil Med. 2019;62(6):397–402.
Milinis K, Young CA. Trajectories of outcome in neurological conditions. Systematic review of the influence of spasticity on quality of life in adults with chronic neurological conditions. Disabil Rehabil. 2016;38(15):1431–41.
Lundstrom E, Smits A, Borg J, Terent A. Four-fold increase in direct costs of stroke survivors with spasticity compared with stroke survivors without spasticity: the first year after the event. Stroke. 2010;41(2):319–24.
Lundstrom E, Terent A, Borg J. Prevalence of disabling spasticity 1 year after first-ever stroke. Eur J Neurol. 2008;15(6):533–9.
Picelli A, Tamburin S, Gajofatto F, Zanette G, Praitano M, Saltuari L, et al. Association between severe upper limb spasticity and brain lesion location in stroke patients. Biomed Res Int. 2014;2014:162754.
Cheung DK, Climans SA, Black SE, Gao F, Szilagyi GM, Mochizuki G. Lesion characteristics of individuals with upper limb spasticity after stroke. Neurorehabil Neural Repair. 2016;30(1):63–70.
Holstege G, Bandler R, Saper CB. The emotional motor system. Prog Brain Res. 1996;107:3–6.
Lemon RN, Griffiths J. Comparing the function of the corticospinal system in different species: organizational differences for motor specialization? Muscle Nerve. 2005;32(3):261–79.
Lemon RN. Descending pathways in motor control. Annu Rev Neurosci. 2008;31:195–218.
Morecraft RJ, Ge J, Stilwell-Morecraft KS, McNeal DW, Pizzimenti MA, Darling WG. Terminal distribution of the corticospinal projection from the hand/arm region of the primary motor cortex to the cervical enlargement in rhesus monkey. J Comp Neurol. 2013;521(18):4205–35.
Kuypers HGJM. Anatomy of the descending pathways. In: Brooks VB, editor. Handbook of physiology. Bethesda: American Physiological Society; 1981.
Kuypers HG. A new look at the organization of the motor system. Prog Brain Res. 1982;57:381–403.
Wall PD, Lidierth M. Five sources of a dorsal root potential: their interactions and origins in the superficial dorsal horn. J Neurophysiol. 1997;78(2):860–71.
Cheema SS, Rustioni A, Whitsel BL. Light and electron microscopic evidence for a direct corticospinal projection to superficial laminae of the dorsal horn in cats and monkeys. J Comp Neurol. 1984;225(2):276–90.
Prochazka A. Sensorimotor gain control: a basic strategy of motor systems? Prog Neurobiol. 1989;33(4):281–307.
Brooks JX, Cullen KE. Predictive sensing: the role of motor signals in sensory processing. Biol Psychiatry Cogn Neurosci Neuroimaging. 2019;4(9):842–50.
Prut Y, Perlmutter SI, Fetz EE. Distributed processing in the motor system: spinal cord perspective. In: Nicolelis MAL, editor. Advances in neural population coding. Amsterdam: Elsevier; 2001. p. 267–78.
Morecraft RJ, Ge J, Stilwell-Morecraft KS, Rotella DL, Pizzimenti MA, Darling WG. Terminal organization of the corticospinal projection from the lateral premotor cortex to the cervical enlargement (C5-T1) in rhesus monkey. J Comp Neurol. 2019;527(16):2761–89.
Lacroix S, Havton LA, McKay H, Yang H, Brant A, Roberts J, et al. Bilateral corticospinal projections arise from each motor cortex in the macaque monkey: a quantitative study. J Comp Neurol. 2004;473(2):147–61.
Qin W, Yang M, Li F, Chen C, Zhen L, Tian S. Influence of positional changes on spasticity of the upper extremity in poststroke hemiplegic patients. Neurosci Lett. 2019;712:134479.
Kline TL, Schmit BD, Kamper DG. Exaggerated interlimb neural coupling following stroke. Brain. 2007;130(Pt 1):159–69.
Maier MA, Armand J, Kirkwood PA, Yang HW, Davis JN, Lemon RN. Differences in the corticospinal projection from primary motor cortex and supplementary motor area to macaque upper limb motoneurons: an anatomical and electrophysiological study. Cereb Cortex. 2002;12(3):281–96.
Lemon RN, Mantel GW, Muir RB. Corticospinal facilitation of hand muscles during voluntary movement in the conscious monkey. J Physiol. 1986;381:497–527.
Lemon RN, Baker SN, Davis JA, Kirkwood PA, Maier MA, Yang HS. The importance of the cortico-motoneuronal system for control of grasp. Novartis Found Symp. 1998;218:202–15; discussion 15–8.
Lawrence DG, Kuypers HG. The functional organization of the motor system in the monkey. I. The effects of bilateral pyramidal lesions. Brain. 1968;91(1):1–14.
Morecraft RJ, Ge J, Stilwell-Morecraft KS, McNeal DW, Hynes SM, Pizzimenti MA, et al. Vulnerability of the medial frontal corticospinal projection accompanies combined lateral frontal and parietal cortex injury in rhesus monkey. J Comp Neurol. 2015;523(4):669–97.
Morecraft RJ, Ge J, Stilwell-Morecraft KS, McNeal DW, Hynes SM, Pizzimenti MA, et al. Frontal and frontoparietal injury differentially affect the ipsilateral corticospinal projection from the nonlesioned hemisphere in monkey (Macaca mulatta). J Comp Neurol. 2016;524(2):380–407.
Evarts EV, Tanji J. Reflex and intended responses in motor cortex pyramidal tract neurons of monkey. J Neurophysiol. 1976;39(5):1069–80.
Alstermark B, Lundberg A. The C3-C4 propriospinal system: target-reaching and food-taking. In: Jami L, Pierrrot-Deseilligny E, Zytnicki D, editors. Muscle afferents and spinal control of movement Oxford. UK: Pergamon Press; 1992. p. 327–54.
Porter R, Lemon RN. Corticospinal function and voluntary movement. Oxford: Oxford University Press; 1993.
Jankowska E, Padel Y, Tanaka R. Disynaptic inhibition of spinal motoneurones from the motor cortex in the monkey. J Physiol. 1976;258(2):467–87.
Maier MA, Illert M, Kirkwood PA, Nielsen J, Lemon RN. Does a C3-C4 propriospinal system transmit corticospinal excitation in the primate? An investigation in the macaque monkey. J Physiol. 1998;511(Pt 1):191–212.
Bacon SJ, Smith AD. A monosynaptic pathway from an identified vasomotor centre in the medial prefrontal cortex to an autonomic area in the thoracic spinal cord. Neuroscience. 1993;54(3):719–28.
Wolpaw JR. The complex structure of a simple memory. Trends Neurosci. 1997;20(12):588–94.
Eyre JA, Miller S, Clowry GJ, Conway EA, Watts C. Functional corticospinal projections are established prenatally in the human foetus permitting involvement in the development of spinal motor centres. Brain. 2000;123(Pt 1):51–64.
Martin JH, Kably B, Hacking A. Activity-dependent development of cortical axon terminations in the spinal cord and brain stem. Exp Brain Res. 1999;125(2):184–99.
Magoun HW, Rhines R. An inhibitory mechanism in the bulbar reticular formation. J Neurophysiol. 1946;9:165–71.
Woolsey CN. Discussion on experimental hypertonia in the monkey: interruption of pyramidal or pyramidal-extra pyramidal cortical projections. Trans Am Neurol Assoc. 1971;96:164–6.
Engberg I, Lundberg A, Ryall RW. Reticulospinal inhibition of interneurones. J Physiol. 1968;194(1):225–36.
Engberg I, Lundberg A, Ryall RW. Reticulospinal inhibition of transmission in reflex pathways. J Physiol. 1968;194(1):201–23.
Putnam TJ. Treatment on unilateral paralysis agitans by section of the lateral pyramidal tract. Arch Neurol Psychiatr. 1940;44:950–76.
Sheean G. The pathophysiology of spasticity. Eur J Neurol. 2002;9(Suppl 1):3–9; dicussion 53–61.
Burke D, Knowles L, Andrews C, Ashby P. Spasticity, decerebrate rigidity and the clasp-knife phenomenon: an experimental study in the cat. Brain. 1972;95(1):31–48.
Bucy PC. Studies on the human neuromuscular mechanism. II Effect of ventromedial cordotomy on muscular spasticity in man. Arch Neurol Psychiatr. 1938;40:639–62.
Hyndman OR, Jarvis FJ. Gastric crises of tabes dorsalis: treatment by anterior chordotomy in eight cases. Arch Surg. 1940;40(5):997–1013.
Fregosi M, Contestabile A, Hamadjida A, Rouiller EM. Corticobulbar projections from distinct motor cortical areas to the reticular formation in macaque monkeys. Eur J Neurosci. 2017;45(11):1379–95.
Darling WG, Ge J, Stilwell-Morecraft KS, Rotella DL, Pizzimenti MA, Morecraft RJ. Hand motor recovery following extensive frontoparietal cortical injury is accompanied by upregulated corticoreticular projections in monkey. J Neurosci. 2018;38(28):6323–39.
Fregosi M, Contestabile A, Badoud S, Borgognon S, Cottet J, Brunet JF, et al. Changes of motor corticobulbar projections following different lesion types affecting the central nervous system in adult macaque monkeys. Eur J Neurosci. 2018;48(4):2050–70.
Herbert WJ, Powell K, Buford JA. Evidence for a role of the reticulospinal system in recovery of skilled reaching after cortical stroke: initial results from a model of ischemic cortical injury. Exp Brain Res. 2015;233(11):3231–51.
Ortiz-Rosario A, Berrios-Torres I, Adeli H, Buford JA. Combined corticospinal and reticulospinal effects on upper limb muscles. Neurosci Lett. 2014;561:30–4.
Chollet F, DiPiero V, Wise RJ, Brooks DJ, Dolan RJ, Frackowiak RS. The functional anatomy of motor recovery after stroke in humans: a study with positron emission tomography. Ann Neurol. 1991;29(1):63–71.
Weiller C, Chollet F, Friston KJ, Wise RJ, Frackowiak RS. Functional reorganization of the brain in recovery from striatocapsular infarction in man. Ann Neurol. 1992;31(5):463–72.
Fries W, Danek A, Scheidtmann K, Hamburger C. Motor recovery following capsular stroke. Role of descending pathways from multiple motor areas. Brain. 1993;116(Pt 2):369–82.
Cramer SC, Nelles G, Benson RR, Kaplan JD, Parker RA, Kwong KK, et al. A functional MRI study of subjects recovered from hemiparetic stroke. Stroke. 1997;28(12):2518–27.
Seitz RJ, Hoflich P, Binkofski F, Tellmann L, Herzog H, Freund HJ. Role of the premotor cortex in recovery from middle cerebral artery infarction. Arch Neurol. 1998;55(8):1081–8.
Schulz R, Braass H, Liuzzi G, Hoerniss V, Lechner P, Gerloff C, et al. White matter integrity of premotor-motor connections is associated with motor output in chronic stroke patients. Neuroimage Clin. 2015;7:82–6.
Pantano P, Formisano R, Ricci M, Di Piero V, Sabatini U, Di Pofi B, et al. Motor recovery after stroke. Morphological and functional brain alterations. Brain. 1996;119(Pt 6):1849–57.
Rehme AK, Eickhoff SB, Rottschy C, Fink GR, Grefkes C. Activation likelihood estimation meta-analysis of motor-related neural activity after stroke. NeuroImage. 2012;59(3):2771–82.
Backhaus W, Braass H, Higgen FL, Gerloff C, Schulz R. Early parietofrontal network upregulation relates to future persistent deficits after severe stroke-a prospective cohort study. Brain Commun. 2021;3(2):fcab097.
Brihmat N, Tarri M, Gasq D, Marque P, Castel-Lacanal E, Loubinoux I. Cross-modal functional connectivity of the premotor cortex reflects residual motor output after stroke. Brain Connect. 2020;10(5):236–49.
Harrington RM, Chan E, Rounds AK, Wutzke CJ, Dromerick AW, Turkeltaub PE, et al. Roles of lesioned and nonlesioned hemispheres in reaching performance poststroke. Neurorehabil Neural Repair. 2020;34(1):61–71.
Tscherpel C, Hensel L, Lemberg K, Vollmer M, Volz LJ, Fink GR, et al. The differential roles of contralesional frontoparietal areas in cortical reorganization after stroke. Brain Stimul. 2020;13(3):614–24.
Chen YT, Li S, Magat E, Zhou P, Li S. Motor overflow and spasticity in chronic stroke share a common pathophysiological process: analysis of within-limb and between-limb EMG-EMG coherence. Front Neurol. 2018;9:795.
Owen M, Ingo C, Dewald JPA. Upper extremity motor impairments and microstructural changes in bulbospinal pathways in chronic hemiparetic stroke. Front Neurol. 2017;8:257.
Li S, Chen YT, Francisco GE, Zhou P, Rymer WZ. A unifying pathophysiological account for post-stroke spasticity and disordered motor control. Front Neurol. 2019;10:468.
Jacobs BL, Fornal CA. Serotonin and motor activity. Curr Opin Neurobiol. 1997;7(6):820–5.
Heckmann CJ, Gorassini MA, Bennett DJ. Persistent inward currents in motoneuron dendrites: implications for motor output. Muscle Nerve. 2005;31(2):135–56.
Lee RH, Kuo JJ, Jiang MC, Heckman CJ. Influence of active dendritic currents on input-output processing in spinal motoneurons in vivo. J Neurophysiol. 2003;89(1):27–39.
Binder MD, Powers RK, Heckman CJ. Nonlinear input-output functions of motoneurons. Physiology (Bethesda). 2020;35(1):31–9.
Kuo JJ, Lee RH, Johnson MD, Heckman HM, Heckman CJ. Active dendritic integration of inhibitory synaptic inputs in vivo. J Neurophysiol. 2003;90(6):3617–24.
Clarke RW, Eves S, Harris J, Peachey JE, Stuart E. Interactions between cutaneous afferent inputs to a withdrawal reflex in the decerebrated rabbit and their control by descending and segmental systems. Neuroscience. 2002;112(3):555–71.
Jankowska E. Interneuronal relay in spinal pathways from proprioceptors. Prog Neurobiol. 1992;38(4):335–78.
Hochman S, Garraway SM, Machacek DW, Shay BL. 5-HT receptors and the neuromodulatory control of spinal cord function. In: Cope TC, editor. Motor neurobiology of the spinal cord. London: CRC Press; 2001. p. 47–87.
Heckman CJ, Kuo JJ, Johnson MD. Synaptic integration in motoneurons with hyper-excitable dendrites. Can J Physiol Pharmacol. 2004;82(8–9):549–55.
D’Amico JM, Condliffe EG, Martins KJ, Bennett DJ, Gorassini MA. Recovery of neuronal and network excitability after spinal cord injury and implications for spasticity. Front Integr Neurosci. 2014;8:36.
Bennett DJ, Sanelli L, Cooke CL, Harvey PJ, Gorassini MA. Spastic long-lasting reflexes in the awake rat after sacral spinal cord injury. J Neurophysiol. 2004;91(5):2247–58.
Harvey PJ, Li X, Li Y, Bennett DJ. 5-HT2 receptor activation facilitates a persistent sodium current and repetitive firing in spinal motoneurons of rats with and without chronic spinal cord injury. J Neurophysiol. 2006;96(3):1158–70.
Gorassini MA, Knash ME, Harvey PJ, Bennett DJ, Yang JF. Role of motoneurons in the generation of muscle spasms after spinal cord injury. Brain. 2004;127(Pt 10):2247–58.
Li Y, Gorassini MA, Bennett DJ. Role of persistent sodium and calcium currents in motoneuron firing and spasticity in chronic spinal rats. J Neurophysiol. 2004;91(2):767–83.
Mottram CJ, Suresh NL, Heckman CJ, Gorassini MA, Rymer WZ. Origins of abnormal excitability in biceps brachii motoneurons of spastic-paretic stroke survivors. J Neurophysiol. 2009;102(4):2026–38.
Mottram CJ, Wallace CL, Chikando CN, Rymer WZ. Origins of spontaneous firing of motor units in the spastic-paretic biceps brachii muscle of stroke survivors. J Neurophysiol. 2010;104(6):3168–79.
Mottram CJ, Heckman CJ, Powers RK, Rymer WZ, Suresh NL. Disturbances of motor unit rate modulation are prevalent in muscles of spastic-paretic stroke survivors. J Neurophysiol. 2014;111(10):2017–28.
Florman JE, Duffau H, Rughani AI. Lower motor neuron findings after upper motor neuron injury: insights from postoperative supplementary motor area syndrome. Front Hum Neurosci. 2013;7:85.
Ditunno JF, Little JW, Tessler A, Burns AS. Spinal shock revisited: a four-phase model. Spinal Cord. 2004;42(7):383–95.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2022 Springer Nature Switzerland AG
About this chapter

Cite this chapter
Raghavan, P. (2022). Neural Basis of Spasticity. In: Raghavan, P. (eds) Spasticity and Muscle Stiffness. Springer, Cham. https://doi.org/10.1007/978-3-030-96900-4_1
Download citation
DOI: https://doi.org/10.1007/978-3-030-96900-4_1
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-96899-1
Online ISBN: 978-3-030-96900-4
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)