
Abstract
Leprosy neuropathy can occur in every phase of the disease, often representing illness’s beginning. All the peripheral nerves can be involved at the same time or in different periods. Being treatable, early recognition of neuropathy is primary to reduce disability.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
1 General Picture of the Leprosy Neuropathy
Most of the disabilities occurring in leprosy are sequelae of damage to the peripheral nervous system. Mycobacterium leprae (M. leprae), the causative organism of leprosy, has a peculiar affinity for the Schwann cell, where it multiplies and leads to damage of the nerve and its functions. In borderline leprosy, peripheral nerve damage is often acute and occurs during type 1 leprosy reaction (T1R); in lepromatous leprosy, it develops over years and has acute exacerbations during episodes of erythema nodosum leprosum (ENL) reaction, also called type 2 leprosy reaction (T2R). The distribution of nerve involvement is related to the position of the patient in the leprosy spectrum (cell-mediated immunity). In the hyperergic forms, tuberculoid and borderline tuberculoid leprosy, nerve damage is early and affects one or a few nerves asymmetrically. In the hypoergic or anergic forms (mid-borderline, borderline lepromatous, and lepromatous leprosy), nerve involvement tends to be late, widespread, and symmetric.
In diagnosis, it is useful to distinguish the peripheral neuropathies as mononeuropathy when affecting one nerve, multineuropathy when affecting more nerves, and polyneuropathy when nerve involvement is bilateral and symmetric. It starts as a demyelinating process and evolves to axonal damage. All three components of the peripheral nervous system are affected: sensory, motor, and autonomic. Sensory damage often occurs earlier than motor damage and, at the beginning, tends also to be more pronounced than motor deficit. Neural deficit may be clinically silent until 30% of the nerve fibers of the nerve are damaged [1]. Sensory loss causes anesthesia (loss of touch sensation), analgesia (loss of pain sensation), and inability to discriminate hot and cold. Motor deficit causes muscle weakness, up to complete paralysis and atrophy. Damage to autonomic nerve fibers impairs sweating and causes dry skin. Sensory, motor, and autonomic nerve damages are directly (or primarily) caused by leprosy. The complications that result from this direct nerve damage (often grouped as “anesthetic deformities” because of their relation to unprotected use of insensitive hands and feet) are called secondary impairments, e.g., ulcers, contractures, bone destruction, and shortening of fingers and toes. Secondary impairments may lead to a variety of disabilities and handicaps. In extreme cases, the leprosy patient may suffer de-habilitation and destitution [2].
2 Patient History and Physical Examination
2.1 Patient History
Patient history regarding symptoms, e.g., time of onset, type of onset (acute or chronic), parts of the body involved, if symptoms are associated with weight- bearing activities, medications used, and other medical conditions, may provide important information. The patient may refer symptoms of acute neuritis such as tingling sensation (paresthesia), or sometimes pain along the course of the nerve. He may refer numbness or motor deficit. Often, he may present already with history of advanced nerve damage, for example, weakness in closing eyes and using hands or feet, or the appearance of blisters or ulcers on hands and feet, which have occurred unnoticed.
2.2 Testing for Loss of Tactile Sensation on Skin Lesions
Testing for loss of sensation on skin lesions is relatively simple and, when positive, confirms diagnosis of leprosy [3]. Quietness in the environment or in the room where it is performed is important. Both the patient and the examiner must be positioned comfortably while examining. A fine, pointed wisp of cotton wool is used to touch the part to be tested. The process is first explained to the patient and then demonstrated while he watches and points carefully to the exact spot touched. When he comprehends fully, testing continues at various sites inside and outside the lesions, but with the patient’s eyes covered. Only touch should be applied, not brushing across the skin. The patient with closed eyes can either point with one finger to the exact spot where the cotton wool touched the skin or he can confirm the exact place verbally when he feels the touch. Patient reliability should be tested by asking for the point of contact when not touching the skin at all. If he feels it but cannot point to the exact spot, it is called “misreference,” the earliest sign of hypoesthesia [4]. Inability to identify the point stimulated at all denotes loss of sensation to the stimulus used. Cotton wool may be too delicate to test for sensory loss in lesions on thickened skin of palms and soles; here, monofilaments or nylon bristles can be used.
2.3 Palpation of Peripheral Nerves
Palpation of nerves at “sites of predilection” is performed during physical examination of the patient. This is a fundamental procedure in diagnosis and follow-up of both leprosy and leprosy reactions. Nerve palpation is performed gently using the pulp of the fingers, not the fingertip or fingernail. The person’s face should be observed to make sure that unnecessary pain is not caused when touching the nerve. The tenderness (spontaneous or when palpating), consistency (soft, hard, irregular), and size (enlarged, normal, small) of the nerve are evaluated. Tenderness when palpating the nerve or spontaneous nerve pain is a sign of reaction. It is essential to know the normal limits by constant practice in palpating nerves. During examination, one should compare nerves on the opposite site of the body. Enlarged nerves should be differentiated from tendons, blood vessels, or lymph nodes. In leprosy all peripheral nerves may be enlarged. Cutaneous branches associated with a skin lesion may be enlarged as well. The two most commonly affected are the ulnar nerve and the common peroneal nerve. The following paragraphs describe how to locate and palpate the peripheral nerves of predilection in leprosy. They will be described systematically, starting from the head, then those of the upper limbs, and finally those of the lower limbs.
2.3.1 Supraorbital Nerve
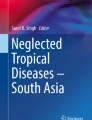
An enlarged supraorbital nerve is palpable as it passes upward out of the orbit. To palpate it, run your index finger across the forehead from the midline laterally (Fig. 15.1).

Supraorbital nerve : enlarged (Reproduced with permission, © Enrico Nunzi 2021. All Rights Reserved)
2.3.2 Great Auricular Nerve
The great auricular nerve (Fig. 15.2) can be seen and palpated in the neck, emerging from the posterior border of the sternocleidomastoid muscle. The patient turns his/her head to one side, thus stretching this muscle. The great auricular nerve courses anteriorly and superiorly across the muscle toward the earlobe.

Great auricular nerve: enlarged
2.3.3 Ulnar Nerve
The forearm of the patient is bent at 90–110° over the arm. The examiner uses his left hand to palpate the right ulnar nerve and his right hand to palpate the left ulnar nerve. The nerve can be palpated first at the elbow in the olecranon groove, between the olecranon and the medial epicondyle of the humerus. Then, it can be felt and evaluated immediately above the groove. In comparing right and left ulnar nerves, it is useful to ask the patient to put his hands on the examiner’s shoulders; in this case, the bending is about 135° (Naafs, 2010, personal communication). Alternatively, the patient may hold his own hands in front of his body.
2.3.4 Radial Nerve
The radial nerve is difficult to palpate. It can be appreciated and rolled against the humerus at approximately halfway down the lateral side of the arm, below the insertion of the deltoid muscle and anterior to the lateral head of the triceps muscle.
2.3.5 Radial Cutaneous Nerve
The radial cutaneous nerve branches from the radial nerve at the elbow. It is palpated at the lower third of the forearm. It can be rolled under the tips of the examiner’s fingers as it crosses the lateral border of the radius just proximal to the wrist and courses onto the dorsum of the hand. For diagnosis of leprosy, no other clinical or laboratory test has the same high sensitivity and specificity [5].
2.3.6 Median Nerve
The median nerve is felt in front of the wrist when the wrist joint is semiflexed, proximal to the flexor retinaculum. It is often easier to see than to palpate due to the presence (if present) of the tendon of the palmaris longus muscle.
2.3.7 Common Peroneal Nerve (Lateral Popliteal Nerve)
The common peroneal nerve is the continuation of the lateral component of the sciatic nerve, from which it separates in the upper part of the popliteal fossa; it then runs behind the head of the fibula and obliquely around its neck. It continues for about 10 cm in contiguity with the bone and enters the fibular tunnel to reach the muscles of the leg. While palpating the common peroneal nerve, the patient has the knee joints semiflexed and the examiner kneels in front of him; alternatively, the patient and examiner are seated in front of each other. The nerve is palpated in the popliteal fossa, just medial to the biceps femoris tendon and as it passes round the neck of the fibula.
2.3.8 Superficial Peroneal Nerve
The superficial peroneal nerve (also called dorsalis pedis) can be palpated on the dorsum of the foot and of the ankle.
2.3.9 Posterior Tibial Nerve
The posterior tibial nerve anatomically is the continuation of the medial portion of the sciatic nerve. It can be palpated as it passes posteriorly and inferiorly to the medial malleolus to supply the sole of the foot. It is difficult to palpate due to tendons and blood vessels which also pass this location.
2.3.10 Sural Nerve
The sural nerve can be palpated along the midline of the back of the lower leg, in the mid- to lower part of the leg, where calf muscles join to the Achilles’ tendon.
The sural nerve can also be palpated as it runs down behind and under the lateral malleolus and along the lateral side of the foot.
2.4 Tinel’s and Phalen’s Signs
Tinel’s sign is evocated by manually squeezing the nerve in areas of possible “entrapment.” Examples are the ulnar nerve at the olecranon groove, the median nerve at the wrist, the lateral popliteal nerve (common peroneal) at the head of the fibula, and the posterior tibial nerve at the medial malleolus. When positive, the patient refers a small shock (transient paresthesia) propagating distally to the area supplied by the tested nerve. Phalen’s sign applies to the median nerve only; when positive, dorsal hyperflexion of the wrist with hands in opposition causes paresthesia or pain in the first three fingers.
2.5 Neurological Examination
Clinical assessment of the leprosy patient includes accurate neurological examination. We have already discussed testing for loss of tactile sensation on skin lesions and palpation of nerves. These are followed by neurological examination targeting exclusion of sensory, motor, and autonomic deficits. The evaluation of both sensitivity and muscular strength needs full collaboration of the patient, particularly when the deficit is bilateral and no comparison is possible. Lack of communication skills, a confused patient, suffering, old, or child may involuntarily alter the results.
The sensory system is evaluated first. Proprioceptive sensations (which arise from muscles, ligaments, bones, tendons, and joints) are studied by gently moving the patient’s first toe and asking him to define its position in space (sense of motion and position), or placing a tuning fork over a bony prominence and asking the patient about perception of vibration (sense of vibration or pallesthesia).
Another maneuver for assessing deep sensitivities is Romberg’s test: The patient is asked to stand erect with eyes closed and feet together; swaying, sometimes irregular swaying, and even toppling over are suggestive of deficit of these sensitivities. Study of superficial sensations (or exteroceptive sensations) includes three types: pain, temperature, and tactile; this has greater importance in leprosy, particularly for establishing diagnosis and the region and nerve affected. For tactile sense, light touch sensation may be assessed by gently touching the suspected region with the examiner’s finger pulp or with a piece of cotton wool (see testing for loss of tactile sensation). Thermal sense, the first sensation to be lost, can be tested using two test tubes, one containing hot water and the other cold water. A pinprick test may be used to test pain sensation. Qualitative and quantitative assessment of sensation is performed by use of graded nylon monofilaments. Once a sensory deficit is appreciated, it is necessary to determine its topography. Circumscribed areas of hypoesthesia or anesthesia, particularly in correspondence with cutaneous lesions, indicate damage of cutaneous nerves. On the contrary, when the sensory deficit reproduces the distribution of a peripheral nerve, a lesion of the relevant nerve trunk is suspected even without motor deficit or muscle atrophy. In the next section, we describe the consequences of nerve damage for each nerve of predilection affected in leprosy.
Assessment of motor deficit is done by evaluating deep tendon reflexes, and muscular bulk and power. Bilateral comparison helps in appreciating unilateral deficit. Deep tendon reflexes, differently from other neuropathies, are commonly preserved in leprosy. Evaluation of muscular bulk should take into account patient gender and age, as well as the panniculus adiposus and physical activity; forced rest reduces muscular bulk also without peripheral nerve lesions. Muscle hypotrophy can be minimal, moderate, or serious (atrophy). While evaluating muscular bulk, the presence of fasciculations should be noted. These are random, spontaneous twitchings of a group of muscle fibers visible through the skin (better under sidelight), commonly absent in leprosy neuropathy; their presence suggests other pathologies. When an important motor deficit is caused by nerve damage, as is the case in leprosy neuropathy, both muscular power and bulk should be decreased; otherwise, other diagnoses should be considered (e.g., diseases of the central nervous system or tendons/lesions). For evaluating motor strength, it is customary to use the 0–5 scale proposed by the British Medical Research Council. Grade 5 is normal power; grade 4 is active movement against moderate resistance; grade 3 is active movement against gravity; grade 2 is active movement with gravity eliminated; grade 1 is trace of contraction; and grade 0 is no contraction.
An isolated sensory deficit is common at the onset of leprosy neuropathy, while an isolated motor deficit is rarer; the latter is commonly accompanied by the former and by autonomic deficit.
Evaluation of the clinical picture is based on the topography of the sensory, motor, and autonomic damage. To determine the specific nerve affected, all parameters (bulk, power, sensation, and hydration) should be consistent; for example, a lesion of the ulnar nerve at the elbow clinically causes muscle weakness and hypotrophy, sensory deficit, and dryness of the skin in the medial part of the hand. Evaluation of the affected nerve is easier in the case of mononeuropathy, but leprosy tends to produce multineuropathy, and the clinical picture may be complicated, particularly in advanced cases due to damage to several nerves.
Gait in leprosy can be seriously altered. In the “stepping gait,” the patient has to lift the affected leg high during walking in order to keep the foot clear of the ground (as if he or she is climbing up steps) [2]. It is caused by paralysis of the tibialis anterior and peroneal muscles that are responsible for dorsiflexion and eversion of the foot.
There may also be inability to walk on the heels.
3 Clinical Features
Symptoms and signs of neuritis may appear acutely, during reactions, with nerve enlargement, nerve pain or tenderness, loss of sensation, dry skin, and paralysis. More often, they appear slowly with gradual loss of sensory functions, decreased muscular power, and muscular hypotrophy. Neuritis can also be “silent” for weeks and months. In this case, the patient reports no symptoms, and, without clinical and electrophysiological investigations, undue delay in diagnosis and management of nerve damage may occur. Virtually, all peripheral nerves may be involved, but those that supply the face, eyes, hands, and feet need major attention and systematic evaluation.
3.1 Supraorbital and Great Auricular Nerves
Enlargement of these nerves represents an important diagnostic sign of leprosy, but their involvement produces minimal clinical damage to the patient. The supraorbital nerve can rarely cause headache and pain in the orbital cavity, while the great auricular nerve has virtually no relevance to the patient (Figs. 15.1 and 15.2).
3.2 Facial Nerve
In leprosy, the facial nerve (cranial nerve VII) can be damaged at different levels. When it is affected only in its upper (or zygomatic) branch, there is weakness or paralysis of the orbicularis oculi muscle. This causes inability to close the eyelid, a condition called lagophthalmos, which may lead to a serious secondary keratoconjunctivitis. When paralysis of cranial nerve VII is complete, one may find Bell’s palsy, where frontal, orbicularis oculi muscles and the muscles of the lower portion of the face are all affected (Fig. 15.3).

Facial nerve: bilateral lagophthalmos
3.3 Ulnar Nerve
In leprosy, the ulnar nerve can be affected at the arm (Fig. 15.4), elbow, and wrist. Damage at the elbow is more common, precisely at two sites: posteriorly to the medial epicondyle and in the cubital tunnel. The cubital tunnel is a rigid anatomical structure whose roof is made up of an aponeurosis and the fibers of the flexor carpi ulnaris muscle, while the floor is made up of the medial ligament of the elbow and other muscular fibers. During leprosy reactions and neuritis, the enlarged nerve will be entrapped between those rigid structures with worsening of the neural lesion. Finally, the ulnar nerve can be affected in the Guyon canal as it passes through the wrist. Lesions at the elbow or at the wrist cause similar symptoms and signs. There may be tenderness or pain at the affected points and positive Tinel’s sign. Sensory impairment is present at the fifth finger, at the medial region of the fourth finger, and at the medial region of the hand. Motor damage affects the intrinsic muscles of the hand. There is deficit of abduction of the fifth finger, and hypotrophy of the hypothenar and interossei muscles with creation of four grooves between the metacarpals. The weakness of the interossei muscles that bend the first phalanx bone and extend the last two causes the deformity called “claw fingers.” Damage of the autonomic fibers causes dryness of the skin in the medial region of the hand (Figs. 15.4, 15.5, and 15.6).

Ulnar nerve: enlarged at the arm

Ulnar nerve : the right hand shows an erythematous skin lesion in the medial region, hypotrophy of the hypothenar region, hollowing of the interosseous spaces, extension of the fourth and fifth metacarpal phalangeal joints, and flexion of the proximal interphalangeal joints

Ulnar nerve : hollowing of the first interosseous space. Flexion of the proximal interphalangeal joint of the fourth and fifth fingers
3.4 Median Nerve
The median nerve is frequently affected in leprosy, alone or together with the ulnar nerve. It is rarely affected at the arm, elbow, or forearm. In leprosy, most commonly, the damage is just before the wrist or at the wrist where it runs within the carpal tunnel; here, the clinical features are related to the amount of compression. Sensory deficit is almost always present and similar to that produced by lesions at more proximal sites. There are paresthesia, hypoesthesia , and even anesthesia involving the first three fingers, the lateral region of the fourth finger, and the lateral region of the hand, with sparing of the skin above the thenar muscle (the latter being affected only when the lesion is proximal to the carpal tunnel). In advanced damage, there is atrophy of the thenar, abduction and opposition of the first finger are compromised, and there is clawing of the second and third fingers. The skin in the area of the hand supplied by the nerve is dry. The diagnosis is based on evidence of sensory, motor, and autonomic deficit, pain at the wrist, and positive Tinel’s and Phalen’s signs. In case of carpal tunnel syndrome, electro-neurographic (ENG) studies show increased distal latency for motor fibers and, for sensory fibers, decreased conduction velocity in the length finger–wrist sparing of the proximal segments. Frequently, median and ulnar nerves are both affected, forming the picture of complete claw hand and causing severe hand deformity (Figs. 15.7, 15.8, 15.9, 15.10, and 15.11).

Median nerve (left): enlarged at the wrist

Median nerve : sensitive damage, bulla on the third finger; the patient inadvertently burnt himself while cooking

Median and ulnar nerves : sensory median nerve damage with traumatic wounds to the insensitive first and second fingers; motor ulnar nerve damage with hypotrophy of the hypothenar muscle. Dry skin over the palm (autonomic damage)

Median and ulnar nerves : sensory, motor, and autonomic damage of both nerves, claw fingers, calluses on the tips of the fingers

Medial and ulnar nerves : bilateral damage
3.5 Radial Nerve
The clinical picture depends on the site of the lesion. In leprosy, the radial nerve is rarely damaged at the upper arm (the triceps muscle is normally spared). Also, lesion just below the elbow (posterior interosseous nerve syndrome) is uncommon.
Commonly, in leprosy, motor abnormalities involve the brachioradialis muscle and the extensor muscles of wrist and fingers; the result may be a severely disabling wrist drop. Sensory disturbance is in the dorsomedial region of the hand (Fig. 15.12).

Radial and ulnar nerves : wrist drop and hypotrophy of the hypothenar muscle
3.6 Radial Cutaneous (Superficial Radial) Nerve
When enlarged, the radial cutaneous nerve is very useful for diagnosis of leprosy. Its involvement does not cause important clinical problems to the patient other than an area of loss of sensation over the dorsum of the hand (Fig. 15.13).

Radial cutaneous nerve : enlarged at the lower part of the forearm, wrist, and dorsum of the hand
3.7 Sciatic and Common Peroneal Nerves
In leprosy, the common peroneal (syn.: lateral popliteal) nerve is commonly damaged in the popliteal fossa or proximally and around the neck of the fibula. The patient may complain of pain or tenderness along the area of the nerve. There is loss of sensation in the anterior and lateral aspects of the lower leg, dorsum of the foot, and toes. The motor deficit is in the anterior and lateral muscles of the leg. In the early stage, there is difficulty in dorsiflexion and eversion of the foot against resistance. Complete damage causes paralysis of the foot in ventral flexion (foot drop) and in inversion, with a stepping gait. In case of a focal lesion of the peroneal nerve, ENG study shows nerve conduction slowing or “blocking.” If the ENG test is normal, a proximal lesion should be suspected, namely, a L5 radiculopathy (clinically producing low back pain) or a partial lesion of the sciatic nerve (more difficult to diagnose). In these cases, electromyography is useful for detecting subclinical abnormalities in muscles not innervated by the common peroneal nerve such as gluteal muscles (in L5 radiculopathy) and the short head of the biceps femoris in a lesion of the lateral trunk of the sciatic nerve. Correct localization of the site of the lesion will guide further diagnostic or therapeutic interventions (Fig. 15.14).

Common peroneal nerve : the patient is not able to dorsiflex the right foot. Hypotrophy of the right anterior tibial muscle. Dry skin
3.8 Posterior Tibial Nerve
In leprosy, the posterior tibial nerve is frequently affected just proximally or within the tarsal tunnel. Early damage results in pain in the region of the medial malleolus radiating to the leg and foot, and paresthesia on the sole of the foot. The importance of the sensory deficit is in relation to the intensity of the damage and the affected branches (medial and lateral plantar and calcaneal). Advanced damage at the tarsal tunnel results in anesthesia of the sole, with sparing of two small areas, a medial one served by the saphenous nerve and a lateral one served by the sural nerve. If the lesion affects the calcaneal nerve, the sensory loss will be at the heel; if the medial plantar nerve is affected, loss of sensation will be at the medial region of the sole and at the first, second, third, and part of the fourth toe; when the lateral plantar nerve is affected, loss of sensation will be at the lateral region of the sole, fifth toe, and part of the fourth toe.
Motor deficit is difficult to assess clinically in early stages; when advanced and added to damage of the common peroneal nerve, it results in paralysis of the intrinsic muscles, clawing of the toes, and collapse of the arch of the foot. Deficit of the autonomic system causes loss of sweating and dryness of the sole. Damage to the posterior tibial nerve is the most common and most important cause of injury to the feet in leprosy [4]. Combination of common peroneal and posterior tibial nerve involvement causes devastating deformities to the feet (Fig. 15.15).

Posterior tibial nerve : damage to this nerve results in anesthesia of the sole of the foot and plantar ulcers
A distal lesion of the plantar nerves in the region of the metatarsal heads with pain in the sole irradiating to the second and third toe produces Morton’s syndrome, sometimes also associated with sensory deficit.
3.9 Sural Nerve
The sural nerve is a sensory nerve producing, when damaged, an area of hypoesthesia confined to the lateral region of the foot, with minimal clinical consequences for the patient. ENG has demonstrated high incidence of lesions of this nerve in leprosy, as in other peripheral neuropathies. It is the preferred site for diagnostic nerve biopsy because it lacks motor fibers and is easily accessible at the lower third of the back of the leg. When possible, the biopsy should be preceded by ENG, with abnormal ENG confirming the utility of proceeding with biopsy.
WHO classification of grades of disability in leprosy [6] | ||
|---|---|---|
Grade | Hands and feet | Eyes |
0 | No disability found | No disability found |
1 | Loss of sensation | The eyes are not given a grade of 1 |
2 | Visible damage or disability is noted | Lagophthalmos, obvious redness of the eye, visual impairment, or blindness |
References
Nunzi E, Leiker DL. Manuale di leprologia. Bologna: AIFO; 1990.
Srinivasan H. Prevention of disabilities in patients with leprosy. Geneva: WHO; 1993. p. 3–15.
Noto S, Schreuder PAM. Diagnosis of leprosy, leprosy mailing list; 2010. http://leprosy mailinglist.blogspot.com.
Pfaltzgraff RE, Bryceson A. Clinical leprosy. In: Hastings RC, editor. Leprosy. Edinburgh: Churchill Livingstone; 1985. p. 140–76.
van Hees C, Naafs B. Common skin diseases in Africa. An illustrated guide. Voorburg: Stichtiing Troderma; 2009.
WHO. Operational guidelines for the enhanced global strategy (2011–2015). 2009.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2022 Springer Nature Switzerland AG
About this chapter

Cite this chapter
Reni, L., Noto, S., Schreuder, P.A.M. (2022). The Leprosy Neuropathy. In: Nunzi, E., Massone, C., Portaels, F. (eds) Leprosy and Buruli Ulcer. Springer, Cham. https://doi.org/10.1007/978-3-030-89704-8_15
Download citation
DOI: https://doi.org/10.1007/978-3-030-89704-8_15
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-89703-1
Online ISBN: 978-3-030-89704-8
eBook Packages: MedicineMedicine (R0)