
Abstract
Diffuse lepromatous leprosy (DLL) or pure and primitive leprosy or lazarine leprosy or Lucio–Latapí leprosy is a systemic and peculiar form of leprosy, a polar lepromatous type of the disease in which the patient has no response to lepromin skin test, has no lepromas but diffuse infiltration of the whole skin, is multibacillary, and develops an acute reaction known as Lucio’s phenomenon. Patients also have dysesthesia, anhidrosis, hair loss not only on the scalp but also on other areas of the skin or even the whole skin, and a “succulent” aspect which in time becomes atrophic. Histopathologically, there is wide infiltration by macrophages filled with acid-fast bacilli, belonging to a particular strain named Mycobacterium lepromatosis, which is the specific cause of it.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
Among the protean clinical and histopathological features of leprosy, diffuse lepromatous leprosy is a multibacillary systemic disease, with multiple organ involvement, and with a negative intradermal reaction to the Mitsuda test (or lepromin skin test, which in the past, it was used as an aid to classification of cases). It presents as a diffuse variant, in which there are no circumscribed elements, i.e., nodules or lepromas, macules, or plaques, but which is characterized by diffuse and massive infiltration of the skin, known as diffuse lepromatous leprosy (DLL) or Lucio–Latapí leprosy. This is a distinct form of multibacillary leprosy reported mainly in Mexico, where it represents 15%–23% of all leprosy diagnoses [1]. Nevertheless, it is also seen in other areas of Central and South America such as Colombia and Brazil. Exceptionally, it has been diagnosed in other regions.
It was Ladislao de la Pascua who first described spotted or lazarine leprosy in 1844; when physicians were not aware of the etiology and nature of this illness, it was known as a chronic and destructive disease. In 1852, Lucio and Alvarado [2], working at the Saint Lazaro Hospital in Mexico City, which assisted only persons with leprosy, studied 41 patients (21 men and 20 women) with this diffuse infiltration of the skin without lepromas (Lucio’s leprosy). They observed that 13 of them (6 men and 7 women) developed peculiar painful, red spots on the skin: Lucio’s phenomenon.
Almost a century later, Latapí and Chévez-Zamora studied the subject and recognized both aspects observed by Lucio and Alvarado, coining the terms Lucio’s leprosy and Lucio’s phenomenon, identified as a vasculitis [3].
It is widely accepted that Mycobacterium leprae is the causative agent of several forms of leprosy; however, the identification of the new strain of mycobacterium in 2008 by Han et al. [4] in tissues from patients with DLL suggests that the peculiar geographical and ethnic prevalence, as well as the particular severity of this form of the disease, is due to this distinctive strain: Mycobacterium lepromatosis . DLL carries a higher mortality rate than other forms of leprosy [1].
Nowadays, it has been demonstrated that Lucio-Latapí leprosy is caused mostly, if not only, by M. lepromatosis. According to Han et al., at least 63.2% of patients with Lucio-Latapí leprosy had M. lepromatosis, 20.7% had M. leprae, and 16.1% had both bacteria [1].
Patients with lepromatous leprosy have a poor Th1 response, or a dominant Th2 response, with production of IL-4, IL-5, and IL-10, which are able to suppress activation of macrophages against the causal mycobacterium; there is production of antibodies, which may result in an immune-complex disease. Lymphocytes infiltrating the skin of patients show a predominance of CD8 subset (CD4/CD8 = 1/2).
The clinical sine qua non criterion is diffuse nonnodular infiltration of the skin [5]. At the beginning, the skin shows wide infiltration that has been compared with myxedema, the face looks “healthy” (lepra bonita or pretty leprosy), and the earlobe turns thick. Later on in the progression of the disease, hands become swollen, puffy, and red, and the legs look edematous. In time, all the skin becomes flaccid and atrophic (Fig. 11.1), giving to some areas such as the legs an ichthyosiform aspect.

Diffuse lepromatous leprosy in a late stage: flaccid skin, in particular that of the earlobe
Other features are telangiectasias, nonvisible subcutaneous plaques, widening of nasal root, rhinitis, hoarseness, and septal perforation of cartilage. Patients first notice numbness and then impairment of sensation in hands and feet.
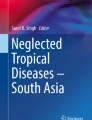
Loss of hair is common, not only from the scalp, which is never total, but also from eyebrows and eyelashes, total or partial (Fig. 11.2). However, this is not a constant finding, and some patients do not lose hair from any area.

Diffuse lepromatous leprosy with hair loss and damage to the nasal cartilaginous septum
Lucio–Latapí leprosy or DLL usually presents in adults of both sexes; it is exceptional in childhood and the elderly. Clinical changes may be so subtle that often the patient notices the disease only because of sudden development of an acute reaction, namely, Lucio’s phenomenon.
Although the histopathology of DLL depends on the stage of the disease, there are always acid-fast bacilli (AFB) in variable amounts but usually many, outside and inside of foamy macrophages or Virchow cells; these are the two least criteria to reach the diagnosis under the microscope. Macrophages are mixed with lymphocytes around blood vessels, adnexal structures, and nerves.
In early stages of the disease, the cellular infiltrates localized around vessels are slight and apparently insignificant [6]. In time, there is progressive dissemination of AFB and increasing numbers of Virchow cells, not only throughout the dermis but also into subcutaneous fat. In well-developed stages, macrophages are prominent in number and infiltrate in a diffuse pattern; blood vessels begin to show involvement as thickening of their walls.
Besides the clinical and histopathological parameters, bacillary assessment is also very useful for diagnosis, and mostly for classification of a patient with leprosy.
In advanced diffuse lepromatous leprosy, the bacteriological index (see Chap. 20) is usually 5+ or 6+ and decreases after 6 months or more of treatment.
According to the World Health Organization, treatment should be with multibacillary multidrug therapy: rifampicin 600 mg/month, clofazimine 50 mg/day or 300 mg/month, and dapsone 100 mg/day, all three for at least 1 year. However, in Mexico, these patients are treated for 2 years and sometimes even longer, depending on their clinical, bacteriological, and histopathological response.
References
Han XY, Sizer KC, Velarde-Félix J, Frias-Castro LO, Vargas-Ocampo F. The leprosy agents Mycobacterium lepromatosis and Mycobacterium leprae in Mexico. Int J Dermatol. 2012;51:952–9.
Lucio R, Alvarado I. Opúsculo sobre el mal de San Lazaro o elefanciasis de los Griegos: M. México: Murguía y Cía; 1852. p. 53.
Latapí F, Chévez-Zamora A. The “spotted” leprosy of Lucio: an introduction to its clinical and histological study. Int J Leprosy. 1948;16:421–37.
Han Y, Seo YH, Sizer KC, et al. A new Mycobacterium species causing diffuse lepromatous leprosy. Am J Clin Pathol. 2008;130:856–64.
Rea TH, Jerskey RS. Clinical and histologic variations among thirty patients with Lucio’s phenomenon and pure primitive diffuse lepromatosis (Latapi’s lepromatosis). Int J Leprosy. 2005;72:169–88.
Vargas-Ocampo F. Diffuse leprosy of Lucio and Latapí: a histologic study. Lepr Rev. 2007;78:248–60.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2022 Springer Nature Switzerland AG
About this chapter

Cite this chapter
Magaña, M. (2022). Lucio–Latapí Leprosy. In: Nunzi, E., Massone, C., Portaels, F. (eds) Leprosy and Buruli Ulcer. Springer, Cham. https://doi.org/10.1007/978-3-030-89704-8_11
Download citation
DOI: https://doi.org/10.1007/978-3-030-89704-8_11
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-89703-1
Online ISBN: 978-3-030-89704-8
eBook Packages: MedicineMedicine (R0)