
Abstract
Successful routine cardiac surgery dates back to 1950s, when the development of cardiopulmonary bypass (CPB) machine allowed for more complex surgical approach. Percutaneous coronary interventions were introduced in 1977. The first transcatheter aortic valve replacement was performed in 2002, followed by percutaneous replacements and repairs of other valves. As modern cardiac surgical management trends towards less invasive procedures, there has been a debate which patients would benefit from interventional cardiology management and who requires surgical intervention. Notably both interventional cardiology and surgical equipment and operator skills have improved significantly since they were introduced to everyday practice. So has the perioperative management as well as post-operative care. Taking all this into consideration the simple answer that everybody would benefit from the least invasive approach might not be correct. Improvements in management have been seen along with changes in patients’ population. In the dawn of cardiac surgery, only otherwise fit patients were considered to be suitable for such a risky and straining procedure. Nowadays, cardiac surgeons are faced with much older patients with multiple comorbidities and it is the role of a multidisciplinary team, including anesthetist to choose proper cardiac intervention in the most optimal approach.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
Introduction
Anesthesia preoperative assessment for cardiac surgical patient is in essence not very different to one for any other general anesthesia. All cardiac surgical patients are having extensive cardiac workup and this needs to be reviewed thoroughly in context of perioperative planning and possible intraoperative and postoperative complications. On the other hand, several aspects of assessment are unique to this population and require additional expertise and knowledge, which is an essential part of training of cardiothoracic anesthesiologist. The size of this chapter does not allow for comprehensive discussion of all facets of preoperative assessment and optimization, therefore, we will focus only on some important topics, which recently became a challenge and task for cardiac anesthesiologist.
Frailty
Due to complexity of cardiac interventions, in particular those requiring use of CPB and their impact on normal body physiology, more attention is being paid to these patient characteristics that may influence the perioperative outcome. Among all comorbidities and conditions, frailty seems to have been out of focus of researches for many years. However, as the patient’s population is aging and demands from society increasing, it becomes one of the most important factors, which impact on recovery and outcome cannot be overrated. Frailty focuses not only on age, but rather all these characteristics that might be age related, yet in a non-linear manner like malnutrition, wasting, weakness, slowness, inactivity and dependence. Unlike any specific medical condition, frailty is believed to express patients’ vulnerability and influences health and recovery even from minor insults in a disproportional manner. Since none of the features regarded as frailty is easy to be quantified, there are numerous scales that try to grade and describe frailty, some better validated than others. Out of all, Clinical Frailty Scale (CFS) (Table 1) is worth mentioning, as it is a simple 9-point scale that assesses patient clinically, often on a basis of first impression. It is being mentioned as a screening tool in a systematic review focused on the impact of frailty on outcomes after cardiac surgery, where this characteristic is identified as a risk factor increasing mortality by fivefold. It also increases morbidity, functional decline and incidence of major adverse cardiac and cerebrovascular events. It is essential to recognize these vulnerable patients before planning surgery and post-operative care, providing information to patients and their families, particularly in context of protracted ICU stay. Cardiac rehabilitation programs, especially these run before surgery improve patients outcomes (prehabilitation), partially by improving their nutritional status, activity level, muscle mass so by addressing some of the components of frailty syndrome. Therefore it is advocated that all elective patients presenting with frailty should be considered to be enrolled in prehabilitation programs that need to be continued after surgery.
Anemia
One of the very few chronic conditions that can and should be optimized before elective cardiac surgery is anemia. It is a disease, which can be easily diagnosed and rising of hemoglobin (Hb) (treating anemia) level requires only 14 days prior to surgery. It is defined as a Hb concentration < 12 g/dL for women or < 13 g/dL for men. It is proven, that there is an independent association of anemia with transfusion rates (odds ratio (95% confidence interval) 2.75 (2.55–2.95), p < 0.001), mortality (1.42 (1.18–1.71), p < 0.001) and length of hospital stay (geometric mean ratio (95% confidence interval) 1.15 (1.13–1.17), p < 0.001). Its prevalence in cardiac surgical population is 20–30% and is a result of either impaired erythropoiesis (iron deficiency, vitamin B6 or B12 deficiency, malabsorption, chronic kidney failure, bone marrow disorders) or chronic blood loss. All sorts of chronic occult bleeding sources must be investigated, as they pose risk of severe, unexpected bleeding once full anticoagulation is instituted. More often, however, it is the impaired erythropoiesis due to iron deficiency that leads to anemia, hence preoperative substitutive therapy is proven to be beneficial in cardiac surgical population. There is evidence that preoperative supplementation with intravenous iron and erythropoietin improves perioperative outcomes. In case of documented vitamin B12/B6 deficiency they should be substituted as well (Fig. 1). Even ultra-short anemia treatment with single dose of iron/erythropoietin/Vit B12/Folic acid right before surgery reduces perioperative transfusion rates, yet there is no data supporting any difference in perioperative mortality. Therefore the problem of pre-operative anemia needs to be addressed as part of the routine preoperative assessment and preferably supplemented in a timely, elective manner prior to surgery.

Diagnostic algorithm of perioperative anemia. Algorithm modified from Muñoz et al. [2]
Heart Team
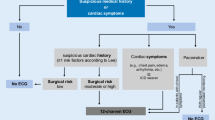
There are three main approaches to the management of heart conditions. The first one is medical treatment and optimization of symptoms that is usually reserved for patients who are presenting too early or too late for invasive intervention. The second and third are percutaneous or surgical interventions, respectively. Our initial understanding of risk–benefit balance for surgical revascularization vs percutaneous intervention (PCI) for coronary artery disease comes from SYNTAX trial. Rates of major adverse cardiac or cerebrovascular events (primary end point: death from any cause, stroke, myocardial infarction, or repeat revascularization) at 12 months were significantly higher in the PCI group than in surgical (17.8, vs. 12.4% for CABG; P = 0.002), in large part because of an increased rate of repeat revascularization (13.5% vs. 5.9%, P < 0.001). Despite the fact that stroke was significantly more likely to occur with CABG (2.2%, vs. 0.6% with PCI; P = 0.003), SYNTAX trial proved that cardiopulmonary bypass grafting (CABG) is superior to PCI in patients with left main stenosis or multivessel disease. This prompted publication of guidelines on cardiopulmonary revascularization in 2010, later revised in 2019. In this document the authors introduced the concept of Heart Team as a multidisciplinary decision making team that proposes treatment based on evidence-based guidelines. The core of the team comprises of cardiologist, interventional cardiologist and cardiac surgeon but it is expected that additional input may be needed from general practitioners, anesthetists, geriatricians and intensivists. Revised 2019 version of guidelines not only stresses the importance of Heart Team in proper patient management, but also gives positive feedback on this intervention by minimizing specialty bias (cardiologists as “gate keepers”) and optimizing patient care. Successful introduction of Heart Team concept into perioperative management of patients suffering from coronary artery disease led to incorporation this form of decision making in qualification for valvular procedures, and surgical treatment of patients with end stage congestive heart failure. It is being mentioned in 2012 update of Guidelines on the Management of Valvular Heart Disease (VHD), where the authors emphasize “the importance of collaborative approach between cardiologists and cardiac surgeons in the management of patients with VHD—in particular when they are at increased perioperative risk”. This approach was feasible with the advancement in diagnostic as well as minimal invasive surgical and percutaneous interventional techniques. More recent guidelines (2017) define a Heart Team as a group of specialists with particular expertise in VHD comprising cardiologists, cardiac surgeons, imaging specialists, anesthetists and, if needed, general practitioners, geriatricians and heart failure, electrophysiology or intensive care specialists, who are all involved in decision-making regarding valvular intervention. Over the years, the concept of Heart Team has proven to be a part of routine evaluation tool for all cardiac patients that guarantees adequate management compatible with up-to-date evidence-based standards.
Scores
One of the tools used for decision making are scores predicting perioperative morbidity and mortality. Numerous scores have been developed and further validated but unfortunately the complexity of the intervention itself, along with heterogeneity of patients and their comorbidities make such multifactorial analysis very difficult. Yet, scores are being designed in order to balance risk–benefit. They are important for decision-making process and for explaining the potential risk to patient and his family, finally comparing center outcomes with expected morbidity and mortality. Choosing a score that is tailored for given patient is very difficult, and one needs to keep in mind, that some older scores might not reflect up-to-date protocols, that there might be some intercontinental differences in prevalence of some conditions or interventional approaches and last but not least, that despite very little predicted risk, unpredictable could take place that might completely change the outcome of the particular patient.
STS Short Term Risk Calculator
STS (The Society of Thoracic Surgeons) risk calculator is a tool design to assess the impact of patient risk factors on perioperative mortality and morbidity. The latest update, released in 2018 acknowledges recent changes in both patient population’s characteristics and surgical and perioperative management. In essence this online calculator predicts the risk for operative mortality, stroke, renal failure, prolonged ventilation, reoperation, composite major morbidity or mortality, deep sternal wound infection/mediastinitis and prolonged (> 14 days) or short (< 6 days) postoperative length of stay for patients undergoing isolated coronary artery bypass grafting surgery (CABG), isolated aortic or mitral valve surgery and combined valve plus CABG procedures. Predicted risk models are validated against patients’ outcomes database, and are subject to elicit statistical analysis hence their accuracy is expected to reflect true patient’s risk. Older versions of STS calculator were believed to overestimate the risk in low risk patients, as well as older patients and combined surgeries and the latest revision is yet to be further validated in terms of observed-to-expected ratio of adverse effects.
Euroscore
The most recent revision of The European System for Cardiac Operative Risk Evaluation called EuroSCORE II was published in 2012, replacing older versions dating back in late 90’s. Similarly to other scores it focuses on patients characteristics (age, gender), comorbidities (creatinine clearance, presence of extracardiac arteriopathy, chronic lung disease, severe muscular/neurologic condition, insulin dependent diabetes, infective endocardiatis), critical preoperative state (ventricular tachycardia or fibrillation or aborted sudden death, cardiac massage, ventilation before arrival in the operating room, use of inotropes, intra-aortic balloon counterpulsation or ventricular-assist device before arrival in the anaesthetic room, acute renal failure (anuria or oliguria <10 ml/h)), cardiac function and symptoms (LV function, history of recent MI, NYHA class, CCS class, presence of pulmonary hypertension) and urgency and complexity of surgery (first time vs redo surgery, isolated procedure vs revascularization and valve procedure, involvement of thoracic aorta) in predicting risk of in-hospital mortality. Its accuracy was subject of a meta-analysis and proved to significantly overestimate risk in isolated coronary artery bypass grafting (observed/expected ratio of 0.829) and slightly underestimate the predictions in high-risk patients (observed/expected ratio 1.253). However, the overall performance of the EuroSCORE II in terms of discrimination and accuracy of model predictions for operative mortality is believed to be good. Therefore, it is routinely used in most of European countries.
Summary
Current review briefly summarized the most important aspects of preoperative assessment and cardiac surgical patients. Authors focus on these aspects which relates to risk assessment and multidisciplinary approach towards qualification. Additionally, we briefly discussed essential principles of perioperative blood management. This single intervention is one of the easiest to implement in every department and has potentially huge influence on outcome. Concluding this chapter, we would like to emphasize once again that all other aspects or preoperative anesthesia assessment applies to every cardiac surgical patient.
Recommended Readings
Muñoz M, Gómez-Ramírez S, Besser M, Pavía J, Gomollón F, Liumbruno GM, Bhandari S, Cladellas M, Shander A, Auerbach M. Current misconceptions in diagnosis and management of iron deficiency. Blood Transfus. 2017;15(5):422–437. https://doi.org/10.2450/2017.0113-17.
Muñoz M et al., Perioperative anemia management in colorectal cancer patients: a pragmatic approach. World J Gastroenterol. 2014;20(8):1972–85.
McCann et al., Cardiac prehabilitation. J Cardiothorac Vasc Anesth. 2019;33(8):2255–65.
Meybohm P et al., Perioperative anemia management as part of PBM in cardiac surgery—a narrative updated review. J Cardiothorac Vasc Anesth. 2019.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2022 Springer Nature Switzerland AG
About this chapter

Cite this chapter
Jarosz, A., Wąsowicz, M. (2022). Preoperative Assessment and Decision-Making. In: Vives, M., Hernandez, A. (eds) Cardiac Anesthesia and Postoperative Care in the 21st Century. Springer, Cham. https://doi.org/10.1007/978-3-030-79721-8_4
Download citation
DOI: https://doi.org/10.1007/978-3-030-79721-8_4
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-79720-1
Online ISBN: 978-3-030-79721-8
eBook Packages: MedicineMedicine (R0)