
Abstract
The four-to-one ratio of males to females with autism spectrum disorder (ASD) has remained strikingly stable despite evolving diagnostic criteria. As a result of the higher prevalence of ASD in males, females with a clinical diagnosis of ASD tend to be underrepresented both clinically and in research. Given the underrepresentation of females with ASD, the clarification of the nature of sex/gender-specific differences in ASD carries compelling prospects for understanding this heterogeneous condition. In this chapter, we follow Lai et al. (J Am Acad Child Adolesc Psychiatr 54(1), 11–24, 2015) and use the term ‘sex/gender’ to reflect the awareness that the effects of biological ‘sex’ and socially constructed ‘gender’ cannot be easily separated. The present chapter addresses sex/gender differences in restrictive and repetitive behaviors and interests (RRBI), one of the two domains for establishing a diagnosis of ASD. First, we present a review of sex/gender differences in ASD in general, followed by a survey of the sex/gender differential in RRBI over the lifespan and in co-occurring conditions, highlighting the effect of age and IQ. We continue with a survey of differences between males and females in diagnosis ascertainment in ASD, ending with recommendations for future research in the area of sex/gender differences in ASD and repetitive and restrictive behaviors and interests.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others

Keywords
- Autism spectrum disorder
- Sex/gender differences
- Repetitive and restricted behaviors and areas of interest
- Lifespan
- Diagnosis
Replication of the observation that autism spectrum disorder (ASD) appears four times as often in males as in females has remained strikingly stable despite evolving diagnostic criteria (Baio et al., 2018; Christensen et al., 2016; Fombonne, 2002; Halladay et al., 2015; Lai, Lombardo, Auyeung, Chakrabarti, & Baron-Cohen, 2015). Males are particularly overrepresented among ASD individuals with average to above-average cognitive ability, among whom estimates of the male to female ratio range from 5.7 to 11:1 (Baird et al., 2006; Fombonne, 2005). Conversely, among those individuals with ASD with moderate to severe intellectual disability (ID), the ratio is closer to 2:1 (Fombonne, 1999; Werling & Geschwind, 2013). As a result of the higher prevalence of ASD in males, females with a clinical diagnosis of ASD and average to above-average intellectual ability tend to be underrepresented both clinically and in research (Halladay et al., 2015). Given the underrepresentation of females with ASD, the clarification of the nature of sex/gender-specific differences in ASD carries with it one of the most compelling prospects for understanding this heterogeneous condition. In this chapter, we will be following Lai et al. (2015) by using the term ‘sex/gender’ to reflect the awareness that the effects of biological ‘sex’ and socially constructed ‘gender’ cannot be easily separated. The present chapter addresses sex/gender differences in restrictive and repetitive behaviors and interests (RRBI), one of the two domains for establishing a diagnosis of ASD. First, we present a review of sex/gender differences in ASD in general, followed by a survey of the sex/gender differential in RRBI over the lifespan and in co-occurring conditions, highlighting the effect of age and IQ. We continue with a survey of differences between males and females in diagnosis ascertainment in ASD, ending with recommendations for future research in the area of sex/gender differences in ASD and repetitive and restrictive behaviors and interests.
Sex/Gender Differences in ASD
Since autism emerged as a diagnostic category (Asperger, 1944/1991; Kanner, 1943), the disorder has been mostly observed and depicted in males. Kanner (1943) based his characterization of the disorder on eleven cases, eight of whom were male, while Asperger (1944/1991) based his characterization on four cases all of whom were male. Asperger was fascinated by the male prevalence he observed and tried to explain the sex/gender gap:
“How can this be explained? There is certainly a strong hint at a sex-linked or at least sex-limited mode of inheritance. The autistic personality is an extreme variant of male intelligence. Even within the normal variation, we find typical sex differences in intelligence. In general, girls are the better learners. They are more gifted for the concrete and the practical, and for tidy, methodical work. Boys, on the other hand, tend to have a gift for logical ability, abstraction, precise thinking and formulating, and for independent scientific investigation…. In the autistic individual the male pattern is exaggerated to the extreme…. It may be only chance that there are no autistic girls among our cases, or it could be that autistic traits in the female become evident only after puberty. We just do not know.” (pp. 84–85)
Today, 80 years later, the sex/gender gap in the prevalence of ASD is still not well understood.
Over the years a 4:1 male-to-female ratio has been reported consistently in individuals with ASD (Christensen et al., 2016; Fombonne, 1999, 2005; Halladay et al., 2015; Werling & Geschwind, 2013). Some researchers report a lower ratio of approximately 3:1 males to females (Baio, 2014; Kim et al., 2011; Loomes, Hull, & Mandy, 2017), with a surprising 2.3:1 male-to-female ratio reported in a broad population epidemiological review (Mattila et al., 2011). Others report even higher male-to-female ratios of 5.7:1 (Fombonne, 2002) and 9:1 (Brugha et al., 2016). These discrepancies in the sex/gender gap in the prevalence of ASD, which may be partially explained by sampling differences in clinical and epidemiological studies, have led to research attempting to discover potential reasons for the sex/gender gap in the prevalence of ASD. The main areas of research involve investigating the influence of biological factors, ascertainment bias, diagnostic criteria and the instruments used to measure sex/gender differences, in order to understnad the female phenotype which is not captured in the male-based diagnostic criteria of ASD. It may be that autism traits in females and males are distributed differently, manifest differently and at different ages, are concealed by gender specific cultural expectations and/or are more often behaviorally camouflaged in females than in males. These possibilities and others may contribute to under-referral of females for a clinical diagnosis or a misdiagnosis of females with ASD (Halladay et al., 2015; Lai et al., 2015; Lai, Lombardo, & Baron-Cohen, 2014).
Despite the challenges associated with identifying ASD in females, ongoing research attempts to identify sex/gender differences in ASD symptoms in order to enable clinicians and researchers to diagnose ASD in females. The empirical findings have been equivocal. Some researchers failed to detect sex/gender differences in autism symptomatology (Carter et al., 2007; Holtmann, Bölte, & Poustka, 2007; Mandic-Maravic et al., 2015; Reinhardt, Wetherby, Schatschneider, & Lord, 2015), whereas Hartley and Sikora (2009) and Nicholas et al. (2008) found that females demonstrate fewer repetitive behaviors, while Zwaigenbaum’s et al. (2012) research yielded findings which showed that females exhibit fewer impairments in social communication. It has also been reported that females aged three to eighteen years old (Antezana et al., 2019) and adult females (Cohen et al., 2010) demonstrate higher levels of self-injurious behavior (SIB), which has been conceptualized as reflecting stereotypic movements and as such as a manifestation of RRBI in ASD (Bishop et al., 2013; Boyd, McDonough, & Bodfish, 2012; Georgiades, Papageorgiou, & Anagnostou, 2010). The results from other studies indicate that phenotypic differences which are not present at earlier ages emerge later (Halladay et al., 2015; McFayden, Antezana, Albright, Muskett, & Scarpa, 2019; Schroeder et al., 2014; van Wijngaarden-Cremers et al., 2014).
Different methodologies have been employed in these studies, including quantitative and qualitative paradigms, clinical and epidemiological studies, and methodologies including various informants using different instruments. One example of informant research revealed differences in the descriptions by parents of their male children who were being evaluated for ASD and those of parents of females (Hiller, Young, & Weber, 2014). Parents of girls reported that their daughters were more likely to engage in complex imitation of others, had a strong desire to be liked by peers, and had a more advanced vocabulary than boys, whereas parents of boys reported that their sons tended to have more restricted interests and were more isolated or withdrawn in social settings. These findings suggest that the instruments used to measure autism symptomatology affect the sex/gender differences which emerge (Ratto et al., 2018).
The issues relating to prevalence disproportions between males and females include diverse biological processes which may lead to phenotypic sex/gender differences and an ascertainment bias which may result in an artificially low prevalence in females compared with males. We will also consider sampling bias, which may lead to under-referral and misdiagnosis of females with ASD. Furthermore, because the investigation into sex/gender differences in ASD symptoms has not yielded entirely consistent and clear results, we will address the diagnostic process and the instruments used to identify sex/gender similarities and differences, focusing on repetitive and restricted behaviors and interests.
Biological Factors
Several researchers have examined the genetic, hormonal, and neuro-immune processes which lead to phenotypic sex differences in ASD (see Lai et al., 2015; Werling & Geschwind, 2013, for reviews). A specific attempt to address the differences in the prevalence of ASD between males and females was formulated as the “extreme male brain” theory (Baron-Cohen, 2002). According to this theory, ASD is in fact the radicalization of the normative masculine tendency to systemize. Support for this theory may be found in the findings of genetic research. Zhang et al. (2020) revealed that females diagnosed with ASD have more genetic mutations associated with ASD than males with the equivalent level of autism symptoms. These results, together with those of previous studies, suggest that females who carry a genetic predisposition for ASD need higher environmental impact and/or heredity loading compared to males in order for the disorder to manifest itself (Hallmayer et al., 2011; Lai et al., 2015; Werling & Geschwind, 2013; Zhang et al., 2020).
Diagnostic Ascertainment Bias
Evidence from Shattuck’s et al. (2009) epidemiological study indicates that females are diagnosed later than males, and females with average and above-average IQ are diagnosed significantly later than both females with below-average IQ and males with average and above-average IQ. It is possible that an inherent diagnostic ascertainment bias may lead to an artificially low prevalence of ASD diagnosed in females compared with males. For example, because young boys tend to display more repetitive and restrictive behaviors than girls, they may be referred for a diagnostic evaluation earlier than girls (Solomon, Miller, Taylor, Hinshaw, & Carter, 2012; Werling & Geschwind, 2013). It is possible that some of the differences which are noted between young boys and girls diagnosed with ASD are similar to sex/gender patterns seen in typically developing children. Current diagnostic criteria were developed primarily from male-biased samples and may not address differential developmental patterns that are commonly seen in neurotypical boys and girls (Rivet & Matson, 2011), and this may be one of the underpinnings of the under-diagnosis of ASD in females.
Most children in the United States who receive an ASD diagnosis do so around the age of 4 years and 8 months (Center for Disease Control and Prevention, 2018). Kopp and Gillberg (1992) investigated the later diagnosis of girls by examining the profiles of girls who received an ASD diagnosis around the age of ten despite the fact that they were evaluated before the age of six because of developmental or behavioral concerns. The clinicians who saw these girls before the age of six did not identify the behavioral patterns they saw in the assessment as possible early signs of ASD in the female phenotype. Since these girls then went on to receive an ASD diagnosis by the age of ten, these findings raise the possibility that ASD is not recognized in younger girls referred for neurodevelopmental assessment before the age of six, supporting the hypothesis that some of the differences in prevalence rates of males and females are related to the age of initial diagnosis. Finally, differences in social expectations and requirements of males and females in different cultures may contribute to the diagnostic ascertainment bias between males and females (Nazim & Khalid, 2018). Some of these differences may result in parents and clinicians attributing behavior difficulties of females to shyness more than they do for males (Dean, Harwood, & Kasari, 2017; Hull, Mandy, & Petrides, 2017).
Another factor contributing to differences in diagnostic ascertainment may be the generally greater ability of females to engage in socially appropriate behaviors, as typically developing girls attain early socio-communicative milestones before chronologically age-matched boys (Rose & Rudolph, 2006). This developmental divergence may lead to sex/gender-based differences in the manifestation of ASD and place females at risk for under-diagnosis, particularly among those without co-occurring ID. Recently, this ability to blend in socially has been called the “camouflage effect” (Cage & Burton, 2019; Hull et al., 2017; Lai et al., 2011, 2015), denoting the ability that females may “mask” or “camouflage” their ASD symptoms more successfully than males do (Dworzynski, Ronald, Bolton, & Happé, 2012; Gould & Ashton-Smith, 2011), particularly for the short time frame of a diagnostic session.
Restrictive and Repetitive Behaviors and Interests as a Diagnostic Criterion in ASD
Over the years the criteria for establishing a diagnosis of ASD have changed, but the core symptoms have remained largely the same. The symptoms of ASD have been grouped into two domains (i.e., social communication and repetitive and restrictive behaviors and interests), which are reflected in the fifth edition of the Diagnostic and Statistical Manual for Mental Disorders (DSM-5: APA, 2013). The criteria for restrictive and repetitive behaviors and interests include (1) repetitive or stereotyped motor movements or use of objects (e.g., lining up objects, repetitive interest in parts of objects), and/or speech (e.g., echolalia, idiosyncratic speech); (2) insistence on sameness and difficulties with minor changes in routines or rigid patterns of verbal or nonverbal behavior; (3) fixated, narrow interests that are unusual in intensity (e.g., perseverative interest in dinosaurs or anime) or focus (e.g., strong attachment to or preoccupation with unusual objects); and (4) unusual responses to sensory aspects of the environment, including both unusual interest in and seeking of sensory input (e.g., visual fascination with moving objects, excessive smelling or touching of objects) and being highly sensitive or aversive to sensory input (e.g., unable to tolerate ordinary noises or textures). Co-occurring conditions such as attention deficit/hyperactivity disorder (ADHD), anxiety, sleep disorder, and disruptive behavior are to be indicated in the diagnostic formulation as well.
The two domains incorporated into an ASD diagnosis have been found to be independent in the general population as well as in ASD (Happé & Ronald, 2008), yet the conceptualization of ASD as a social disorder resulted in neglecting the investigation of RRBI as central to the understanding of ASD. Recent data suggest that RRBI can help explain the sex/gender differences in ASD (Duvekot et al., 2017; Frazier, Georgiades, Bishop, & Hardan, 2014; McFayden et al., 2019). The symptom variation in RRBI reflects the heterogeneity of ASD presentation, and by focusing on RRBI it may be possible to understand sex/gender differences in the identification and diagnosis of ASD. For example, Duvekot et al. (2017) and Hiller et al. (2014) found that RRBI are less predictive of a diagnosis for females than for males. In fact, it seems possible that females with ASD demonstrate overall lower RRBI, in terms of both severity and frequency (Rutherford et al., 2016; van Wijngaarden-Cremers et al., 2014). The study of RRBI in the identification and diagnosis of ASD in males and females may illuminate similarities as well as differences in the female ASD phenotype, which may help to address the under-diagnosis of ASD in females.
Gould (2017) studied sex/gender differences in the diagnostic process and found that females received an ASD diagnosis at an older average age and that higher levels of restricted and repetitive behaviors, which is highly correlated with an ASD diagnosis in boys, were not significantly correlated with an ASD diagnosis in girls. Girls were more likely to be diagnosed with ASD when they had higher total levels of behavioral problems. Boys tended to be more active and exhibit more interests in technical hobbies and facts, whereas girls were more passive and collected information about people rather than ‘projects’. The interests of girls with ASD were often similar to those of typically developing girls (e.g., animals, horses and classical literature). It was not the special interests per se that differentiated them from their peers but rather the quality and intensity of their interests and the time spent on them (Gould & Ashton-Smith, 2011). From these findings it is clear that RRBI which are expressed among girls with ASD are different from those which appear in boys and therefore are not adequately captured by most of the current diagnostic instruments which were standardized with male-biased samples. As a result of the differences in the behavioral manifestations of RRBI in girls, clinicians may be less likely to recognize autism characteristics in girls.
Developmental Trajectories of Restrictive and Repetitive Behaviors and Interests
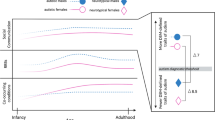
The manifestations of RRBI have been shown to evolve throughout development, so that they may vary in type and intensity at different ages (Seltzer, Shattuck, Abbeduto, & Greenberg, 2004). Longitudinal research has identified common trajectories in the development of children with ASD and sex/gender differences emerge during different developmental time periods. For example, Halladay et al. (2015) revealed no sex/gender differences at early ages, with significant sex/gender differences in repetitive behavior appearing only after age 6 years (van Wijngaarden-Cremers et al., 2014). These findings must be interpreted cautiously, taking into consideration sample size and composition, as well as the diagnostic instruments employed.
One explanation for the finding that RRBI symptoms are less evident in young girls is that some of these behaviors overlap with ordinary, somewhat repetitive play in toddlers (Barton, Robins, Jashar, Brennan, & Fein, 2013). This similarity between typical behavior and repetitive patterns also appears in verbally-skilled older children of average or above-average intelligence, in which more subtle deficits and behaviors may be missed if the only information considered concerns the child’s interactions with a parent, clinician, or other knowledgeable adult, such as a teacher. While a subset of females may in fact evidence symptoms within the first year of life, a more common pattern of symptom expression involves an early course of rather typical development or mild delays followed by the emergence of ASD-related atypical behaviors, including repetitive behaviors and atypical object exploration (Kim & Lord, 2010; Nadig, Vivanti, & Ozonoff, 2009; Paul, Fuerst, Ramsay, Chawarska, & Klin, 2011). Even though toddlers with ASD may demonstrate more severe and/or frequent repetitive actions with objects, motor mannerisms, sensory interests, and non-speech vocalizations compared with children with developmental delays and typically developing children (Kim & Lord, 2010; Schoen, Paul, & Chawarska, 2011; Watt, Wetherby, Barber, & Morgan, 2008), these behaviors are also sometimes observed in other disorders (Lord, Luyster, Guthrie, & Pickles, 2012). Unfortunately, the reduced frequency and quality or complete absence of these behaviors are commonly more challenging for parents and practitioners to identify than the presence of aberrant behaviors that may be seen as more atypical, disruptive, or interfering.
However, more recent findings indicate that high-risk 12-month-olds who are later diagnosed with ASD show more stereotyped motor mannerisms and repetitive manipulation of objects than their low- and high-risk counterparts who do not go on to develop ASD (Elison et al., 2014). Accordingly, more research is needed to better understand the developmental expression of RRBI in children with and without ASD and how this relates to diagnostic criteria and to sex/gender disproportionalities. Whereas social communication skills are more severely impacted in preschool children with significant language and cognitive delays, it appears that the presence of RRBI is relatively independent of developmental level in early childhood. Bishop, Richler, and Lord (2006) found no significant correlations between restricted and repetitive behaviors and interests and nonverbal cognitive skills in children between 2 and 3 years of age, with the exception of sensory interests. A higher percentage of children with moderate impairment in nonverbal IQ showed unusual sensory interests compared to children with nonverbal IQs over 70. However, after age 3 years relations do emerge between nonverbal IQ and several repetitive behaviors. A negative relation with nonverbal IQ was observed for repetitive uses of objects, unusual sensory interests, hand and finger mannerisms, and complex/full-body mannerisms, while a positive relationship was found for fixated interests and insistence on sameness in male-dominant samples (Bishop et al., 2013; Kim, Thurm, Shumway, & Lord, 2013).
No sex/gender differences in RRBI among adolescents with ASD (Bölte, Duketis, Poustka, & Holtmann, 2011; Frazier & Hardan, 2017; Holtmann et al., 2007; Solomon et al., 2012) emerged when measured by RRB domain scores on the ADOS-2 (Lord et al., 2012) and the ADI-R (Rutter, Le Couteur, & Lord, 2003). In a recent multisite study of 282 adolescents and adults with ASD without intellectual disability (68 females), Pugliese et al. (2016) reported that females were rated as less impaired on the following ADOS RRB items: use of immediate echolalia and stereotyped and idiosyncratic words or phrases. In contrast, adult females tend to self-report more ASD behaviors on the SRS-2 (Lai et al., 2015; Lehnhardt et al., 2016), underscoring the importance of using self-report measures to evaluate sex/gender differences in ASD symptomatology in higher functioning adults.
Co-Occurring Conditions and Differential Diagnosis in RRBI in ASD
The co-occurrence of two or more clinical diagnoses, known as “comorbidity,” is particularly salient in individuals with ASD, since an ASD diagnosis can co-exist with a number of other conditions. These additional problems have a substantial negative impact on functioning (Lecavalier, Leone, & Wiltz, 2006) and must be addressed as a crucial part of the diagnostic evaluation. Several large studies, most based on clinically referred samples, have reported that over 70% of children with ASD were above diagnostic thresholds for another developmental, emotional or behavioral disorder and that over 40% may have two or more comorbid mental health conditions (Gjevik, Eldevik, Fjæran-Granum, & Sponheim, 2011; Joshi et al., 2013; Kaat, Gadow, & Lecavalier, 2013; Simonoff et al., 2008), including intellectual impairment (Rydzewska et al., 2019). In the Repetitive Behavior domain, the child with low IQ may present with multiple motor stereotypies and unusual visual behaviors, while the child with higher IQ may manifest this characteristic more in resistance to changes in routines and preoccupations with unusual topics. Specifically, RRBI overlap with other conditions which must be addressed in order to understand their expression in males and females. Individuals with intellectual disabilities, even those without co-occurring ASD, exhibit motor stereotypies as well as repetitive behavior and sometimes echolalia, all of which are included in the diagnostic criteria of RRBI for ASD. In addition, the insistence on sameness, one of the RRBI in ASD, is a central manifestation of obsessive-compulsive disorder (OCD) as well as a manifestation of anxiety. These three conditions will be addressed in order to emphasize the need for multiple diagnoses as well as the need for differential diagnosis.
Most very young children who undergo an ASD assessment also have some general developmental delay (DD). The complexity of understanding the overlap between ASD and DD is more pronounced in younger children, among whom distinguishing social-communication limitations above and beyond the global developmental delays is difficult even for the most experienced clinicians (Thurm, Farmer, Salzman, Lord, & Bishop, 2019). The common features of individuals with DD and those with both DD and ASD, above and beyond cognitive and language delays, include difficulties in behavioral regulation, aggressive outbursts, and/or self-injurious behavior, considered to be RRBI. Some children may demonstrate overall delays in reaching play milestones. If play appears developmentally appropriate given age and developmental functioning, the presence of nonfunctional use of objects, repetitive play schemes, and inflexibility in play, all expressions of RRBI, may signify ASD.
Differential diagnosis among school-age children is complicated, as many of the conditions that commonly co-occur with ASD at this age also have substantial symptom overlap. Teasing out the individual’s interaction style from shyness to phobia to ASD can often be difficult without assessing all environments in which he or she interacts with others. Generalized anxiety disorder (GAD), social phobia, obsessive-compulsive disorder (OCD), depression, and eating disorders have all been found to be related to ASD (Oldershaw, Treasure, Hambrook, Tchanturia, & Schmidt, 2011; Westwood et al., 2016; Westwood, Mandy, & Tchanturia, 2017), although all these have been reported with higher prevalence in females than in males (Solomon et al., 2012). Research has shown that throughout adolescence anxiety problems increase, especially in females with ASD, whereas males tend to have increased levels of depression (Gotham, Brunwasser, & Lord, 2015). A significant proportion of individuals with ASD will develop an anxiety disorder during adolescence. This is more frequently observed in females than in males (Solomon et al., 2012). Restricted and repetitive behavior severity in ASD correlates positively with anxiety severity in cross-sectional surveys (Baribeau et al., 2019). Someone with ASD and anxiety may develop routines that seem rigid; however, it is often in order to gain a sense of control and/or to avoid triggers. Alternatively, the anxiety may manifest itself as obsessive questioning or insistence on sameness rather than in rumination or somatic complaints (Kerns et al., 2016), and this may be misinterpreted by professionals who are unfamiliar with ASD presentation, particularly in higher functioning, more capable individuals with ASD. Like older children, adults with ASD have been found to have co-occurring psychiatric conditions at higher rates than the non-ASD population (Deprey & Ozonoff, 2018). Although males and females with ASD reveal a similar pattern of behavior problems to that of typically developing males and females in childhood, with the boys exhibiting more externalizing behaviors and the girls more internalizing behaviors, by adolescence the sex/gender difference no longer exists, with both males and females with ASD manifesting more internalizing behavior problems, specifically anxiety and depression (Solomon et al., 2012; Werling & Geschwind, 2013).
Behaviors necessary for an ASD diagnosis may overlap with characteristics of other developmental and behavioral conditions and it is imperative to address the issue of differential diagnosis in order to understand whether an ASD diagnosis is appropriate or whether another condition better accounts for the profile revealed during the diagnostic evaluation. The first step in understanding the overlap among symptoms is to obtain an extensive developmental history in order to examine the consistency of symptoms over time and their pervasiveness over contexts (for a review see Mazefsky, Pelphrey, & Dahl, 2012). If ASD is indeed the primary diagnosis, the core challenges in social communication and interaction and the presence of restricted, repetitive, or unusual behaviors would appear to be the major issues to be addressed. This is particularly important for females, for whom the expression of ASD symptomatology may suggest another disorder.
Lidstone et al. (2014) explored the manner in which atypical reactions to sensory stimuli contribute to the association between restricted and repetitive behaviors and anxiety in children with ASD and found that insistence on sameness was significantly associated with anxiety whereas repetitive motor behaviors were not. The relation between anxiety and insistence on sameness was mediated by sensory aversion. No sex/gender differences were found, possibly as a result of sampling bias, as 110 boys and only ten girls were included in this study.
Interest in a potential link between ASD and eating disorders (ED) has increased recently as eating disturbances and/or abnormal eating behaviors such as eating non-foods, selective eating, avoiding new foods, feeding problems, overeating, and polydipsia are commonly noted among individuals with ASD and they are among the diagnostic criteria for some ED (Kahathuduwa et al., 2019; Keen, 2008; Marshall, Hill, Ziviani, & Dodrill, 2014; Råstam, 2008; Williams, Darlymple, & Neal, 2000; Zucker et al., 2007). High levels of autism traits among women with ED have been reported (Courty et al., 2013; Dell’Osso et al., 2018; Gesi et al., 2017), with more cases of ED co-occurring among females with ASD than in males (Courty et al., 2013; Westwood et al., 2016, 2017). Furthermore, a significant proportion of individuals with a clinical ED diagnosis, with no previous diagnosis of ASD, met diagnostic criteria for ASD on the ADOS-2 when tested (Mandy & Tchanturia, 2015; Westwood & Tchanturia, 2017).
The investigation of the overlap between the behavioral phenotypes observed in eating patterns as expressed in ASD and in ED can shed light on the sex/gender differences in RRBI (Råstam, 2008; Zucker et al., 2007). Wallace, Llewellyn, Fildes, and Ronald (2018) found that higher RRBI scores in individuals in the general population were associated with higher rates of eating disturbances. In another population study Van’t Hof et al. (2020) documented that autism traits were associated with different types of eating disturbances in males and in females. These findings suggest the possibility of an underlying mechanism for eating disturbances among people with ASD which involve unusual responses to sensory input, fixated interests and insistence on routines, all expressions of RRBI (Bitsika & Sharpley, 2018; Chistol et al., 2018; Marshall et al., 2014; Råstam, 2008). For example, both avoidance of the sensory stimulation associated with certain foods and insistence on sameness may elicit selective eating.
Since ED are much more common among females than among males (National Institute of Mental Health [NIH], n.d.; Kjelsås, Bjørnstrøm, & Götestam, 2004; Makino, Tsuboi, & Dennerstein, 2004), an ascertainment bias may exist. As previously stated, parents and clinicians may attribute difficulties associated with ASD for females to personality traits or to other disorders more than they do for males (Dean et al., 2017; Hull, Petrides, et al., 2017). Parallel to the under-diagnosis and misdiagnosis of ASD in females, it may be that males suffering from ED are less likely to be diagnosed as a result of significant differences in the way ED expresses itself in males and females, and the fact that ED are most commonly attributed to females (Recio-Barbero et al., 2019; Strother, Lemberg, Stanford, & Turberville, 2012). In order to understand the striking over-representation of ASD symptomatology in individuals with ED, female-specific diagnostic tools must be developed because, at this point, it is not clear whether ASD and ED are co-occurring conditions or whether a differential diagnosis is necessary. Investigating eating disorders as a possible RRBI in females with ASD may help elucidate specific aspects of the female ASD behavioral phenotype.
Evaluation of RRBI
Assessing RRBI as part of the comprehensive evaluation for diagnostic ascertainment of ASD is complex. It is essential to collect information from parents, caregivers, service providers, teachers and physicians, as RRBI may not express themselves in a clinical evaluation although they may be present in other contexts (Adamou, Johnson, & Alty, 2018). Since RRBI may cause significant impairment to individuals with ASD, this information is crucial. Rituals can consume the majority of the waking hours of an individual and interfere with daily family activities. Affected individuals may become anxious, agitated, or disruptive if such behaviors are interrupted (Gordon, 2000). These behaviors can be socially inappropriate and stigmatizing. RRBI have also been shown to interfere with observational learning (Varni, Lovaas, Koegel, & Everett, 1979), attempts to teach play skills (Koegel, Firestone, Kramme, & Dunlap, 1974), responses to auditory stimuli (Lovaas, Litrownik, & Mann, 1971), performance of discrimination tasks (Koegel & Covert, 1972), and environmental exploration (Fornasari et al., 2013; Pierce & Courchesne, 2001). RRBI are most commonly measured by parent report and/or clinician-informed ratings, but can also be measured by self-report in older adolescents and adults. The findings regarding sex/gender differences in RRBI which have emerged from clinical practice and research are presented next.
Autism Diagnostic Observation Schedule – Second Edition (ADOS-2)
The ADOS-2 (Lord, Rutter, et al., 2012) is a semi-structured, standardized assessment in which the quality of social interaction and communication are evaluated in set “presses”, activities which encourage interaction and communication to observe those behaviors associated with an ASD diagnosis. In addition, the presence of repetitive and restrictive behaviors and interests including insistence on sameness is assessed during these tasks. The repetitive and restrictive behavior domain on the diagnostic algorithm is comprised of clinician codes from restrictive interests, sensory behaviors, verbal rituals, compulsions, repetitive behaviors, finger and hand mannerisms, and stereotyped speech that are observed during the 30–75-minute interactive session. When investigating RRBI empirically, the repetitive and restrictive behavior domain scale of the ADOS is commonly used.
Different RRBI items were most sensitive at identifying ASD in each of the five modules. For example, for younger, lower functioning, less verbal children, “unusually repetitive interests or stereotyped behaviors” and “unusual sensory interest in play material/person” were most indicative of an ASD diagnosis. These are exactly the items in which girls have been found to be less impaired than boys (Hiller et al., 2014). For children and young adolescents, “stereotyped/idiosyncratic use of words or phrases” was more sensitive, again an area in which females were found to be less impaired than males. Finally “excessive interest in or references to unusual or highly specific topics or objects or repetitive behavior” was the most sensitive of the RRBI items for older adolescents and adults, and as reported above the areas of interest of females with ASD have been found to be similar to the areas of interest of females without ASD, with the intensity and quality of the interest diagnostically salient, whereas for males the actual area of interest is often different for males with ASD and for those without. When the ADOS-2 was used to investigate sex/gender differences in ASD, females showed significantly fewer ASD symptoms in the repetitive behavior domain (Frazier et al., 2014; Lai et al., 2011). Only a handful of researchers have examined autism symptomatology using the ADOS-2 in female adults with average cognitive abilities. Whereas Wilson et al. (2016) reported no differences between males and females on the restricted and repetitive behavior domain on the ADOS, Pugliese et al. (2016) found that females had fewer RRBI than males when assessed using the ADOS-2.
Autism Diagnostic Interview – Revised (ADI-R)
The ADI-R (Rutter et al., 2003) is a standardized, semi-structured clinical interview for caregivers of children and adults, which contains 93 items and focuses on behaviors associated with ASD. RRBI have been investigated using the ADI-R either by using the RRBI domain of the algorithm or by analyzing specific items to identify specific sex/gender differences. The algorithm items in RRBI include restricted interest, compulsive adherence to routine and rituals, stereotypes/repetitive motor mannerisms, preoccupation with non-functional manipulation of objects and abnormal sensory interest or aversion. ADI-R item analyses revealed that females with ASD showed fewer autism symptoms related to imaginary play, limited interests, and unusual occupations, all of which are associated with RRBI (Beggiato et al., 2017). Despite the finding that in childhood boys had significantly more RRBI on the ADI-R than did girls (Wilson et al., 2016), no significant sex/gender differences in RRBI were revealed in older adolescents and adults with average or above-average cognitive abilities on the ADI-R items (Lai et al., 2011; Park et al., 2012), which may be the result of the retrospective nature of the interview.
The Social Responsiveness Scale, Second Edition (SRS-2)
The SRS-2 (Constantino & Gruber, 2012) is divided by age and by informant and is comprised of four forms that allow for evaluation from age 2 years, 5 months, through adulthood (i.e., preschool form, school-age form, adult self-report and adult other report). The SRS-2 yields five treatment subscales, only one of which specifically addresses RRBI. The SRS-2 RRBI subscale has been used to investigate sex/gender differences in ASD. Specifically, Ratto et al. (2018) reported that females 6–16 years old with ASD received higher scores on the RRBI subscale of the SRS-2 than males. Similarly, Torske, Nærland, Øie, Stenberg, and Andreassen (2018) reported a tendency for higher RRBI scores on the SRS-2 for females but the differences were not significant, which may have been due to the smaller sample size in their study. Lai et al. (2015) and Lehnhardt et al. (2016) found that adult females tended to report more RRBI than males. These results reveal the utility of the SRS-2 in distinguishing between gender/sex differences in RRBI’s and the importance of employing self-report measures alongside other sources of information when investigating sex/gender differences in ASD.
Autism Spectrum Rating Scale (ASRS)
The Autism Spectrum Rating Scale (ASRS; Goldstein & Naglieri, 2009) is an observer-rated scale completed by parents (or similar caregivers) or teachers (or similar professionals) who rate behavioral characteristics of children aged 2–5 years (early childhood form) and older children aged 7–18 years (school-age form). Both forms require the rater to consider behaviors during the past month. The items measure behaviors characteristic of ASD, which are delineated into eleven scales relating to self-regulation, social/communication, adult socialization, attention, emotionality, peer socialization, language, sensory sensitivity, behavioral rigidity, unusual behaviors, and unusual interests. In addition, a short screening version of the ASRS is provided, consisting of 15 items. Scores on the ASRS are particularly salient when examining sex/gender differences in ASD as it is one of the only questionnaires which was standardized on the same numbers of males and females. Empirical findings from the ASRS indicate that ASD repetitive behaviors are significantly more prevalent among males than females throughout childhood. Comparisons of scores on the ASRS indicate that males have significantly higher scores in stereotypical behavior and sensory sensitivity than females (Camodeca, 2019). Surprisingly, the Chinese version of the ASRS revealed significantly higher scores for males on all RRBI subscales, despite having representative sex/gender standardization samples (Zhou et al., 2017, 2019), reflecting the importance of taking social norms into account when examining RRBI.
Repetitive Behavior Questionnaire 2 (RBQ-2)
The RBQ-2 (Leekam et al., 2007) is a 20-item questionnaire which provides a list of many specific repetitive behaviors observed in the last month. It can be self- or informant-reported, which has the added benefit of providing information from several perspectives. May (2012, 2014) has used this measure to show that significantly fewer RRBI appear in female children and adults than in males matched by chronological and mental ages.
Repetitive Behavior Survey-R (RBS-R)
The RBS-R was developed to assess complex behaviors (Bodfish, Symons, Parker, & Lewis, 2000; Lam & Aman, 2007). The 43 items of the RBS-R are grouped into six subscales, which include (1) stereotyped behavior (apparently purposeless movements or actions that are repeated in a similar manner); (2) self-injurious behavior (movements or actions that cause or have the potential to cause redness, bruising, or other injury to the body, and that are repeated in a similar manner); (3) compulsive behavior (behavior that is repeated and performed according to a rule or involves things being done “just so”); (4) ritualistic behavior (performing activities of daily living in a particular order or manner); (5) sameness behavior (resistance to change, insisting that things stay the same); and (6) restricted behavior (limited range of focus, interest, or activity). The RBS-R is unique in its ability to assess such a variety of RRBI, providing the most detailed information about specific RRBI, and has been used in many studies to evaluate RRBI (Bishop et al., 2013; Lam & Aman, 2007; Mirenda et al., 2010; Schertz, Odom, Baggett, & Sideris, 2016). Solomon et al. (2012) included typically developing boys and girls matched with boys and girls with ASD in their study, and found that boys and girls with ASD scored higher on all subscales of the RBS-R than typically developing children except for the compulsive behavior scale, in which no differences emerged between girls with and without ASD. The results from this study did not reveal any significant sex/gender differences on any of the subscales of the RBS-R, although the boys tended to show higher scores on the restrictive interests scale. In contrast, Antezana et al. (2019) investigated sex/gender differences in RRBI among males and females 3–18 years old and found that females with ASD manifested more RRBI related to insistence on sameness and restricted, compulsive, and self-injurious behaviors, and fewer stereotyped, restricted behaviors, and circumscribed interests than males.
Summary and Directions for Future Research
As presented in this chapter, clear sex/gender differences emerge in RRBI, revealing that females exhibit fewer of the diagnostic RRBI criteria than males do, and yet may show more self-injurious behaviors, compulsive behaviors and insistence on sameness than males. These differences emerged from self- and parent-report measures of RRBI. Identifying sex/gender differences in RRBI depends on the measures used and it is critical to be aware of the biases inherent in different instruments. ASD presentation is evaluated based on a male-dominated clinical phenotype which may lead to a diagnostic bias, resulting in under-diagnosis of females (e.g., Lidstone et al., 2014). Until the female presentation is better appreciated and better reflected by diagnostic measures, this bias may continue. Therefore, when considering sex/gender differences in RRBI it is important to consider the normed sample used in the development of the specific measure.
Nesting research into sex/gender differences in ASD in a developmental perspective can help to understand similarities and differences among males and females with ASD as they develop, as well as comparing the manifestation of RRBI in ASD and in typically developing males and females, as RRBI are mediated by age. The sex/gender differences in RRBI expression reported in this chapter change over the course of development, with relatively few differences appearing in toddlerhood, more significant differences emerging in early childhood, school-age and early adolescence, with changes again occurring in later adolescence and adulthood, when there seems to be a reduction in the sex/gender differences of RRBI. These findings suggest the importance of comparing sex/gender differences across all ages, as there may be age-related variation in the similarities and/or differences among ASD and typical development groups which need further study. Many of these changes are associated with co-occurring conditions which affect the manifestation of RRBI in males and females with ASD.
Diagnosing ASD among females in a timely manner in order to provide them with the understanding and support that can stem from receiving an autism diagnosis is crucial, but it may not happen until widely used diagnostic and screening tools include female normative and clinical samples. Existing instruments for capturing the sex/gender differences in RRBI have not been sex/gender-normed or evaluated with respect to their sex/gender bias and thus may not be adequately evaluating the presentation of autism in females. This is particularly important in the assessment of RRBI, in that both quantitative and qualitative differences have emerged. To better understand the unique profile of RRBI in females, it will be necessary to identify potential diagnostic markers that clinicians and researchers may not be currently assessing. This could be achieved through cognitive interviewing of affected females and their families to determine whether current measures adequately capture symptom presentation. Based on the literature presented in this chapter, it is imperative that clinicians not rely solely on standardized measures when evaluating females, but obtain a thorough and nuanced developmental history addressing the development and expression of RRBI across the lifespan.
The association between sex/gender and ASD raises many questions that still need to be answered. Further research into sex/gender differences in RRBI has the potential to improve understanding of the sex/gender prevalence differential and may grant new insight into the female phenotype. Most of the studies reviewed in this chapter based their findings on research focusing on people clinically diagnosed with ASD. As discussed above, factors such as the variance in ASD prevalence between males and females across different cognitive abilities, ages, ascertainment bias and diagnostic bias may result in many females (especially those with average and above-average cognitive abilities) being overlooked (McFayden et al., 2019; van Wijngaarden-Cremers et al., 2014). Co-occurring conditions such as anxiety, depression, intellectual disability, and more recently eating disorders may also affect our understanding of female RRBI presentation. Until such time as more female-specific instruments are developed, the RRBI female and male profiles may be suffering from confounding information.
Some of the studies reviewed in this chapter had a majority of male participants, and although a male majority is representative of the ASD epidemiology, such sampling reduces the applicability of the results to females (Antezana et al., 2019; Fulceri et al., 2016; Kim & Lord, 2010; Lidstone et al., 2014). Therefore, future research should include large-scale community based and/or epidemiological studies which are comprised of large samples of females with ASD. The research should also include comparison groups of males and females with typical development and comparison groups of people with other disorders, specifically focusing on anxiety, eating disorders and obsessive-compulsive disorders. Such research may shed light on sex/gender differences in ASD in general and specifically in RRBI presentation.
Some researchers (e.g., Matheis, Matson, Hong, & Cervantes, 2019; Rubenstein et al., 2017; Ventola et al., 2006) have pointed out discrepancies between information obtained from parent- and self-reports and information obtained from clinical, observational measures when evaluating differences in RRBI among males and females. Although these discrepancies may be due to parental biases, they may also stem from an inherent bias in the observational procedures, instruments and scoring when assessing RRBI. Furthermore, when measured globally RRBI have been shown to be inadequate in predicting an ASD diagnosis in males and females, but on a phenomenological level, some RRBI sub-domains highlight key phenotypic differences between males and females with ASD (McFayden et al., 2019). This chapter highlighted the differences in assessment of RRBI using measures designed for autism symptomatology (e.g., ADOS-2, ADI-R) and measures specifically designed to assess RRBI (e.g., RBS-R, RBQ-2). It appears that measures that target a broad range of RRBI are better at distinguishing between males and females with ASD. Therefore, future research should examine sex/gender differences in RRBI using informant- and self-report measures, clinical observation and comprehensive RRBI measures.
It is important to note that sex/gender differences with respect to RRBI presentation can be attributed in part to genetic liability (Szatmari et al., 2012) and to neurological and hormonal variations (Antezana et al., 2019). The relations between certain RRB subtypes and biological disparities in males and females must be investigated more precisely, by including neurological and hormonal measurements in future research. Advances in understanding the biological mechanisms involved in the presentation of RRBI and the sex/gender differences in RRBI will advance diagnostic precision and will help to develop more specific and reliable treatments.
References
Adamou, M., Johnson, M., & Alty, B. (2018). Autism Diagnostic Observation Schedule (ADOS) scores in males and females diagnosed with autism: A naturalistic study. Advances in Autism, 4(2), 49–55.
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.). Washington, DC: Author.
Antezana, L., Factor, R. S., Condy, E. E., Strege, M. V., Scarpa, A., & Richey, J. A. (2019). Gender differences in restricted and repetitive behaviors and interests in youth with autism. Autism Research, 12(2), 274–283.
Asperger, H. (1944/1991). ‘Autistic psychopathy’ in childhood (U. Frith, Trans.). In U. Frith (Ed.), Autism and Asperger syndrome (pp. 37–92). (This chapter is an annotated translation of a German article by Hans Asperger that was published in “Archiv für Psychiatrie und Nervenkrankenheiten,” 1944, 117, 76–136. The original also appeared in “Heilpädagogik,” Vienna: Springer-Verlag, 1952) Cambridge, MA: Cambridge University Press. https://doi.org/10.1017/CBO9780511526770.002.
Baio, J. (2014). Prevalence of autism spectrum disorder among children aged 8 years—Autism and developmental disabilities monitoring network, 11 Sites, United States, 2010. CDC MMWR Surveillance Summaries, 63, 1–21. https://www.cdc.gov/mmwr/preview/mmwrhtml/ss6302a1.htm.
Baio, J., Wiggins, L., Christensen, D. L., Maenner, M. J., Daniels, J., Warren, Z., et al. (2018). Prevalence of autism spectrum disorder among children aged 8 years—autism and developmental disabilities monitoring network, 11 sites, United States, 2014. MMWR Surveillance Summaries, 67(6), 1–23.
Baird, G., Simonoff, E., Pickles, A., Chandler, S., Loucas, T., Meldrum, D., & Charman, T. (2006). Prevalence of disorders of the autism spectrum in a population cohort of children in South Thames: The Special Needs and Autism Project (SNAP). The Lancet, 368(9531), 210–215.
Baribeau, D. A., Dupuis, A., Paton, T. A., Hammill, C., Scherer, S. W., Schachar, R. J., et al. (2019). Structural neuroimaging correlates of social deficits are similar in autism spectrum disorder and attention-deficit/hyperactivity disorder: Analysis from the POND Network. Translational Psychiatry, 9(1), 1–14.
Baron-Cohen, S. (2002). The extreme male brain theory of autism. Trends in Cognitive Sciences, 6(6), 248–254. https://doi.org/10.1016/S1364-6613(02)01904-6.
Barton, M. L., Robins, D. L., Jashar, D., Brennan, L., & Fein, D. (2013). Sensitivity and specificity of proposed DSM-5 criteria for autism spectrum disorder in toddlers. Journal of Autism and Developmental Disorders, 43(5), 1184–1195.
Beggiato, A., Peyre, H., Maruani, A., Scheid, I., Råstam, M., Amsellem, F., & Delorme, R. (2017). Gender differences in autism spectrum disorders: Divergence among specific core symptoms. Autism Research, 10(4), 680–689. https://doi.org/10.1002/aur.1715.
Bishop, S. L., Hus, V., Duncan, A., Huerta, M., Gotham, K., Pickles, A., et al. (2013). Subcategories of restricted and repetitive behaviors in children with autism spectrum disorders. Journal of Autism and Developmental Disorders, 43(6), 1287–1297.
Bishop, S. L., Richler, J., & Lord, C. (2006). Association between restricted and repetitive behaviors and nonverbal IQ in children with autism spectrum disorders. Child Neuropsychology, 12(4–5), 247–267.
Bitsika, V., & Sharpley, C. F. (2018). Using parent-and self-reports to evaluate eating disturbances in young girls with Autism Spectrum Disorder. International Journal of Developmental Neuroscience, 65, 91–98.
Bodfish, J. W., Symons, F. J., Parker, D. E., & Lewis, M. H. (2000). Varieties of repetitive behavior in autism: Comparisons to mental retardation. Journal of Autism and Developmental Disorders, 30(3), 237–243.
Bölte, S., Duketis, E., Poustka, F., & Holtmann, M. (2011). Sex differences in cognitive domains and their clinical correlates in higher-functioning autism spectrum disorders. Autism, 15(4), 497–511.
Boyd, B. A., McDonough, S. G., & Bodfish, J. W. (2012). Evidence-based behavioral interventions for repetitive behaviors in autism. Journal of Autism and Developmental Disorders, 42(6), 1236–1248.
Brugha, T. S., Spiers, N., Bankart, J., Cooper, S. A., McManus, S., Scott, F. J., et al. (2016). Epidemiology of autism in adults across age groups and ability levels. The British Journal of Psychiatry, 209(6), 498–503.
Cage, E., & Burton, H. (2019). Gender differences in the first impressions of autistic adults. Autism Research, 12(10), 1495–1504.
Camodeca, A. (2019). Description of criterion validity of the Autism Spectrum Rating Scales 6–18 Parent Report: Initial exploration in a large community sample. Child Psychiatry and Human Development, 50(6), 987–1001.
Carter, A. S., Black, D. O., Tewani, S., Connolly, C. E., Kadlec, M. B., & Tager-Flusberg, H. (2007). Sex differences in toddlers with autism spectrum disorders. Journal of Autism and Developmental Disorders, 37(1), 86–97.
Center for Disease Control and Prevention. (2018). Autism spectrum disorder (ASD), identified prevalence of autism spectrum disorder ADDM Network 2000–2014 combining data from all sites. Retrieved December 17, 2018, from https://www.cdc.gov/ncbddd/autism/data.html
Chistol, L. T., Bandini, L. G., Must, A., Phillips, S., Cermak, S. A., & Curtin, C. (2018). Sensory sensitivity and food selectivity in children with autism spectrum disorder. Journal of Autism and Developmental Disorders, 48(2), 583–591.
Christensen, D. L., Baio, J., Braun, K. V., Bilder, D., Charles, J., Constantino, J. N., & Yeargin-Allsopp, M. (2016). Prevalence and characteristics of autism spectrum disorder among 4-year-old children in the autism and developmental disabilities monitoring network, 11 Sites, United States, 2012. MMWR Surveillance Summaries, 65(3), 1–23. https://doi.org/10.15585/mmwr.ss6503a1.
Cohen, I. L., Tsiouris, J. A., Flory, M. J., Kim, S. Y., Freedland, R., Heaney, G., et al. (2010). A large scale study of the psychometric characteristics of the IBR modified overt aggression scale: Findings and evidence for increased self-destructive behaviors in adult females with autism spectrum disorder. Journal of Autism and Developmental Disorders, 40(5), 599–609.
Constantino, J. N., & Gruber, C. P. (2012). Social responsiveness scale: SRS-2. Torrance, CA: Western Psychological Services.
Courty, A., Maria, A. S., Lalanne, C., Ringuenet, D., Vindreau, C., Chevallier, C., et al. (2013). Levels of autistic traits in anorexia nervosa: A comparative psychometric study. BMC Psychiatry, 13(1), 222–231.
Dean, M., Harwood, R., & Kasari, C. (2017). The art of camouflage: Gender differences in the social behaviors of girls and boys with autism spectrum disorder. Autism, 21(6), 678–689. https://doi.org/10.1177/1362361316671845.
Dell’Osso, L., Carpita, B., Gesi, C., Cremone, I. M., Corsi, M., Massimetti, E., et al. (2018). Subthreshold autism spectrum disorder in patients with eating disorders. Comprehensive Psychiatry, 81, 66–72.
Deprey, L., & Ozonoff, S. (2018). Assessment of comorbid psychiatric conditions in autism spectrum disorder. In S. Goldstein, J. A. Naglieri, & S. Ozonoff (Eds.), Assessment of autism spectrum disorders (pp. 290–317). New York, NY: Guilford Press.
Duvekot, J., van der Ende, J., Verhulst, F. C., Slappendel, G., van Daalen, E., Maras, A., & Greaves-Lord, K. (2017). Factors influencing the probability of a diagnosis of autism spectrum disorder in girls versus boys. Autism, 21(6), 646–658. https://doi.org/10.1177/1362361316672178.
Dworzynski, K., Ronald, A., Bolton, P., & Happé, F. (2012). How different are girls and boys above and below the diagnostic threshold for autism spectrum disorders? Journal of the American Academy of Child & Adolescent Psychiatry, 51(8), 788–797.
Elison, J. T., Wolff, J. J., Reznick, J. S., Botteron, K. N., Estes, A. M., Gu, H., et al. (2014). Repetitive behavior in 12-month-olds later classified with autism spectrum disorder. Journal of the American Academy of Child & Adolescent Psychiatry, 53(11), 1216–1224.
Fombonne, E. (1999). The epidemiology of autism: A review. Psychological Medicine, 29(4), 769–786.
Fombonne, E. (2002). Epidemiological trends in rates of autism. Molecular Psychiatry, 7(2), S4–S6.
Fombonne, E. (2005). The changing epidemiology of autism. Journal of Applied Research in Intellectual Disabilities, 18(4), 281–294.
Fornasari, L., Chittaro, L., Ieronutti, L., Cottini, L., Dassi, S., Cremaschi, S., et al. (2013). Navigation and exploration of an urban virtual environment by children with autism spectrum disorder compared to children with typical development. Research in Autism Spectrum Disorders, 7(8), 956–965.
Frazier, T. W., Georgiades, S., Bishop, S. L., & Hardan, A. Y. (2014). Behavioral and cognitive characteristics of females and males with autism in the Simons Simplex Collection. Journal of the American Academy of Child & Adolescent Psychiatry, 53(3), 329–340. https://doi.org/10.1016/j.jaac.2013.12.004.
Frazier, T. W., & Hardan, A. Y. (2017). Equivalence of symptom dimensions in females and males with autism. Autism, 21(6), 749–759.
Fulceri, F., Narzisi, A., Apicella, F., Balboni, G., Baldini, S., Brocchini, J., et al. (2016). Application of the Repetitive Behavior Scale-Revised–Italian version–in preschoolers with autism spectrum disorder. Research in Developmental Disabilities, 48, 43–52.
Georgiades, S., Papageorgiou, V., & Anagnostou, E. (2010). Brief report: Repetitive behaviours in Greek individuals with autism spectrum disorder. Journal of Autism and Developmental Disorders, 40(7), 903–906.
Gesi, C., Carmassi, C., Luciano, M., Bossini, L., Ricca, V., Fagiolini, A., & Dell’Osso, L. (2017). Autistic traits in patients with anorexia nervosa, bulimia nervosa or binge eating disorder: A pilot study. European Psychiatry, 41(S1), S100–S100.
Gjevik, E., Eldevik, S., Fjæran-Granum, T., & Sponheim, E. (2011). Kiddie-SADS reveals high rates of DSM-IV disorders in children and adolescents with autism spectrum disorders. Journal of Autism and Developmental Disorders, 41(6), 761–769.
Goldstein, S., & Naglieri, J. A. (2009). Autism spectrum rating scales (ASRS). North Tonawanda, NY: Multi-Health System.
Gordon, C. T. (2000). Commentary: Considerations on the pharmacological treatment of compulsions and stereotypies with serotonin reuptake inhibitors in pervasive developmental disorders. Journal of Autism and Developmental Disorders, 30(5), 437–438.
Gotham, K., Brunwasser, S. M., & Lord, C. (2015). Depressive and anxiety symptom trajectories from school age through young adulthood in samples with autism spectrum disorder and developmental delay. Journal of the Academy of Child & Adolescent Psychiatry, 54(5), 369–376.
Gould, J. (2017). Towards understanding the under-recognition of girls and women on the autism spectrum. Autism, 21(6), 703–705.
Gould, J., & Ashton-Smith, J. (2011). Missed diagnosis or misdiagnosis? Girls and women on the autism spectrum. Good Autism Practice (GAP), 12(1), 34–41.
Halladay, A. K., Bishop, S., Constantino, J. N., Daniels, A. M., Koenig, K., Palmer, K., & Taylor, J. L. (2015). Sex and gender differences in autism spectrum disorder: Summarizing evidence gaps and identifying emerging areas of priority. Molecular Autism, 6(1), 36.1–36.5. https://doi.org/10.1186/s13229-015-0019-y.
Hallmayer, J., Cleveland, S., Torres, A., Phillips, J., Cohen, B., Torigoe, T., & Lotspeich, L. (2011). Genetic heritability and shared environmental factors among twin pairs with autism. Archives of General Psychiatry, 68(11), 1095–1102. https://doi.org/10.1001/archgenpsychiatry.2011.76.
Happé, F., & Ronald, A. (2008). The ‘fractionable autism triad’: A review of evidence from behavioural, genetic, cognitive and neural research. Neuropsychology Review, 18(4), 287–304.
Hartley, S. L., & Sikora, D. M. (2009). Sex differences in autism spectrum disorder: An examination of developmental functioning, autistic symptoms, and coexisting behavior problems in toddlers. Journal of Autism and Developmental Disorders, 39(12), 1715–1722. https://doi.org/10.1007/s10803-009-0810-8.
Hiller, R. M., Young, R. L., & Weber, N. (2014). Sex differences in autism spectrum disorder based on DSM-5 criteria: Evidence from clinician and teacher reporting. Journal of Abnormal Child Psychology, 42(8), 1381–1393.
Holtmann, M., Bölte, S., & Poustka, F. (2007). Autism spectrum disorders: Sex differences in autistic behavior domains and coexisting psychopathology. Developmental Medicine & Child Neurology, 49(5), 361–366. https://doi.org/10.1111/j.1469-8749.2007.00361.x.
Hull, L., Mandy, W., & Petrides, K. V. (2017). Behavioural and cognitive sex/gender differences in autism spectrum condition and typically developing males and females. Autism, 21(6), 706–727.
Hull, L., Petrides, K. V., Allison, C., Smith, P., Baron-Cohen, S., Lai, M. C., & Mandy, W. (2017). “Putting on my best normal”: Social camouflaging in adults with autism spectrum conditions. Journal of Autism and Developmental Disorders, 47, 1–16. https://doi.org/10.1007/s10803-017-3166-5.
Joshi, G., Wozniak, J., Petty, C., Martelon, M. K., Fried, R., Bolfek, A., et al. (2013). Psychiatric comorbidity and functioning in a clinically referred population of adults with autism spectrum disorders: A comparative study. Journal of Autism and Developmental Disorders, 43(6), 1314–1325.
Kaat, A. J., Gadow, K. D., & Lecavalier, L. (2013). Psychiatric symptom impairment in children with autism spectrum disorders. Journal of Abnormal Child Psychology, 41(6), 959–969.
Kahathuduwa, C. N., West, B. D., Blume, J., Dharavath, N., Moustaid-Moussa, N., & Mastergeorge, A. (2019). The risk of overweight and obesity in children with autism spectrum disorders: A systematic review and meta-analysis. Obesity Reviews, 20(12), 1667–1679.
Kanner, L. (1943). Autistic disturbances of affective contact. Nervous Child, 2(3), 217–250. Retrieved December 11, 2018, from https://www.rescuepost.com/files/library_kanner_1943.pdf.
Keen, D. V. (2008). Childhood autism, feeding problems and failure to thrive in early infancy. European Child & Adolescent Psychiatry, 17(4), 209–216.
Kerns, C. M., Rump, K., Worley, J., Kratz, H., McVey, A., Herrington, J., & Miller, J. (2016). The differential diagnosis of anxiety disorders in cognitively-able youth with autism. Cognitive and Behavioral Practice, 23(4), 530–547.
Kim, S. H., & Lord, C. (2010). Restricted and repetitive behaviors in toddlers and preschoolers with autism spectrum disorders based on the Autism Diagnostic Observation Schedule (ADOS). Autism Research, 3(4), 162–173.
Kim, S. H., Thurm, A., Shumway, S., & Lord, C. (2013). Multisite study of new autism diagnostic interview-revised (ADI-R) algorithms for toddlers and young preschoolers. Journal of Autism and Developmental Disorders, 43(7), 1527–1538.
Kim, Y. S., Leventhal, B. L., Koh, Y. J., Fombonne, E., Laska, E., Lim, E. C., & Song, D. H. (2011). Prevalence of autism spectrum disorders in a total population sample. American Journal of Psychiatry, 168(9), 904–912. https://doi.org/10.1176/appi.ajp.2011.10101532.
Kjelsås, E., Bjørnstrøm, C., & Götestam, K. G. (2004). Prevalence of eating disorders in female and male adolescents (14–15 years). Eating Behaviors, 5(1), 13–25.
Koegel, R. L., & Covert, A. (1972). The relationship pf self-stimulation to learning in autistic children. Journal of Applied Behavior Analysis, 5(4), 381–387.
Koegel, R. L., Firestone, P. B., Kramme, K. W., & Dunlap, G. (1974). Increasing spontaneous play by suppressing self-stimulation in autistic children. Journal of Applied Behavior Analysis, 7(4), 521–528.
Kopp, S., & Gillberg, C. (1992). Girls with social deficits and learning problems: Autism, atypical Asperger syndrome or a variant of these conditions. European Child and Adolescent Psychiatry, 1(2), 89–99.
Lai, M. C., Lombardo, M. V., Auyeung, B., Chakrabarti, B., & Baron-Cohen, S. (2015). Sex/gender differences and autism: Setting the scene for future research. Journal of the American Academy of Child and Adolescent Psychiatry, 54(1), 11–24. https://doi.org/10.1016/j.jaac.2014.10.003.
Lai, M. C., Lombardo, M. V., & Baron-Cohen, S. (2014). Autism. The Lancet, 383(9920), 896–910.
Lai, M. C., Lombardo, M. V., Pasco, G., Ruigrok, A. N., Wheelwright, S. J., Sadek, S. A., & MRC AIMS Consortium. (2011). A behavioural comparison of male and female adults with high functioning autism spectrum conditions. PLoS One, 6(6), e20835. https://doi.org/10.1371/journal.pone.0020835.
Lam, K. S., & Aman, M. G. (2007). The Repetitive Behavior Scale-Revised: Independent validation in individuals with autism spectrum disorders. Journal of Autism and Developmental Disorders, 37(5), 855–866.
Lecavalier, L., Leone, S., & Wiltz, J. (2006). The impact of behaviour problems on caregiver stress in young people with autism spectrum disorders. Journal of Intellectual Disability Research, 50(3), 172–183.
Leekam, S., Tandos, J., McConachie, H., Meins, E., Parkinson, K., Wright, C., et al. (2007). Repetitive behaviours in typically developing 2-year-olds. Journal of Child Psychology and Psychiatry, 48(11), 1131–1138.
Lehnhardt, F. G., Falter, C. M., Gawronski, A., Pfeiffer, K., Tepest, R., Franklin, J., & Vogeley, K. (2016). Sex-related cognitive profile in autism spectrum disorders diagnosed late in life: Implications for the female autistic phenotype. Journal of Autism and Developmental Disorders, 46(1), 139–154.
Lidstone, J., Uljarević, M., Sullivan, J., Rodgers, J., McConachie, H., Freeston, M., et al. (2014). Relations among restricted and repetitive behaviors, anxiety and sensory features in children with autism spectrum disorders. Research in Autism Spectrum Disorders, 8(2), 82–92.
Loomes, R., Hull, L., & Mandy, W. P. L. (2017). What is the male-to-female ratio in autism spectrum disorder? A systematic review and meta-analysis. Journal of the American Academy of Child and Adolescent Psychiatry, 56(6), 466–474. https://doi.org/10.1016/j.jaac.2017.03.013.
Lord, C., Luyster, R., Guthrie, W., & Pickles, A. (2012). Patterns of developmental trajectories in toddlers with autism spectrum disorder. Journal of Consulting and Clinical Psychology, 80(3), 477–489.
Lord, C., Rutter, M., DiLavore, P., Risi, S., Gotham, K., & Bishop, S. (2012). Autism diagnostic observation schedule–2nd edition (ADOS-2). Los Angeles, CA: Western Psychological Corporation.
Lovaas, O. I., Litrownik, A., & Mann, R. (1971). Response latencies to auditory stimuli in autistic children engaged in self-stimulatory behavior. Behaviour Research and Therapy, 9(1), 39–49.
Makino, M., Tsuboi, K., & Dennerstein, L. (2004). Prevalence of eating disorders: A comparison of Western and non-Western countries. Medscape General Medicine, 6(3), 49–73.
Mandic-Maravic, V., Pejovic-Milovancevic, M., Mitkovic-Voncina, M., Kostic, M., Aleksic-Hil, O., Radosavljev-Kircanski, J., et al. (2015). Sex differences in autism spectrum disorders: Does sex moderate the pathway from clinical symptoms to adaptive behavior? Scientific Reports, 5(1), 1–8.
Mandy, W., & Tchanturia, K. (2015). Do women with eating disorders who have social and flexibility difficulties really have autism? A case series. Molecular Autism, 6(1), 6–16.
Marshall, J., Hill, R. J., Ziviani, J., & Dodrill, P. (2014). Features of feeding difficulty in children with Autism Spectrum Disorder. International Journal of Speech-Language Pathology, 16(2), 151–158.
Matheis, M., Matson, J. L., Hong, E., & Cervantes, P. E. (2019). Gender differences and similarities: Autism symptomatology and developmental functioning in young children. Journal of Autism and Developmental Disorders, 49(3), 1219–1231.
Mattila, M. L., Kielinen, M., Linna, S. L., Jussila, K., Ebeling, H., Bloigu, R., & Moilanen, I. (2011). Autism spectrum disorders according to DSM-IV-TR and comparison with DSM-5 draft criteria: An epidemiological study. Journal of the American Academy of Child and Adolescent Psychiatry, 50(6), 583–592. https://doi.org/10.1016/j.jaac.2011.04.001.
Mazefsky, C. A., Pelphrey, K. A., & Dahl, R. E. (2012). The need for a broader approach to emotion regulation research in autism. Child Development Perspectives, 6(1), 92–97.
McFayden, T. C., Antezana, L., Albright, J., Muskett, A., & Scarpa, A. (2019). Sex differences in an autism spectrum disorder diagnosis: Are restricted repetitive behaviors and interests the key? Review Journal of Autism and Developmental Disorders, 23(4), 858–868. https://doi.org/10.1007/s40489-019-00183-w.
Mirenda, P., Smith, I. M., Vaillancourt, T., Georgiades, S., Duku, E., Szatmari, P., et al. (2010). Validating the repetitive behavior scale-revised in young children with autism spectrum disorder. Journal of Autism and Developmental Disorders, 40(12), 1521–1530.
Nadig, A., Vivanti, G., & Ozonoff, S. (2009). Adaptation of object descriptions to a partner under increasing communicative demands: A comparison of children with and without autism. Autism Research, 2(6), 334–347.
National Institute of Mental Health [NIH]. (n.d.). Eating disorders. Retrieved April 19, 2020, from https://www.nimh.nih.gov/health/statistics/eating-disorders.shtml
Nazim, A., & Khalid, R. (2018). Assessment of adaptive functioning of children with typical development attending primary schools in Lahore. International Journal of Social Sciences & Educational Studies, 4(4), 124–134. https://doi.org/10.23918/ijsses.v4i4p124.
Nicholas, J. S., Charles, J. M., Carpenter, L. A., King, L. B., Jenner, W., & Spratt, E. G. (2008). Prevalence and characteristics of children with autism-spectrum disorders. Annals of Epidemiology, 18(2), 130–136.
Oldershaw, A., Treasure, J., Hambrook, D., Tchanturia, K., & Schmidt, U. (2011). Is anorexia nervosa a version of autism spectrum disorders? European Eating Disorders Review, 19(6), 462–474.
Park, S., Cho, S. C., Cho, I. H., Kim, B. N., Kim, J. W., Shin, M. S., et al. (2012). Sex differences in children with autism spectrum disorders compared with their unaffected siblings and typically developing children. Research in Autism Spectrum Disorders, 6(2), 861–870.
Paul, R., Fuerst, Y., Ramsay, G., Chawarska, K., & Klin, A. (2011). Out of the mouths of babes: Vocal production in infant siblings of children with ASD. Journal of Child Psychology and Psychiatry, 52(5), 588–598.
Pierce, K., & Courchesne, E. (2001). Evidence for a cerebellar role in reduced exploration and stereotyped behavior in autism. Biological Psychiatry, 49(8), 655–664.
Pugliese, C. E., Anthony, L. G., Strang, J. F., Dudley, K., Wallace, G. L., Naiman, D. Q., & Kenworthy, L. (2016). Longitudinal examination of adaptive behavior in autism spectrum disorders: Influence of executive function. Journal of Autism and Developmental Disorders, 46(2), 467–477. https://doi.org/10.1007/s10803-015-2584-5.
Råstam, M. (2008). Eating disturbances in autism spectrum disorders with focus on adolescent and adult years. Clinical Neuropsychiatry: Journal of Treatment Evaluation, 5, 31–42.
Ratto, A. B., Kenworthy, L., Yerys, B. E., Bascom, J., Wieckowski, A. T., White, S. W., & Scarpa, A. (2018). What about the girls? Sex-based differences in autistic traits and adaptive skills. Journal of Autism and Developmental Disorders, 48(5), 1698–1711.
Recio-Barbero, M., Fuertes-Soriano, S., Cabezas-Garduño, J., López-Atanes, M., Peña-Rotella, A., & Sáenz-Herrero, M. (2019). Delayed diagnosis of an eating disorder in a male patient with superior mesenteric artery syndrome: Results from a case study. Frontiers in Psychiatry, 10, 731–749.
Reinhardt, V. P., Wetherby, A. M., Schatschneider, C., & Lord, C. (2015). Examination of sex differences in a large sample of young children with autism spectrum disorder and typical development. Journal of Autism and Developmental Disorders, 45(3), 697–706.
Rivet, T. T., & Matson, J. L. (2011). Review of gender differences in core symptomatology in autism spectrum disorders. Research in Autism Spectrum Disorders, 5(3), 957–976.
Rose, A. J., & Rudolph, K. D. (2006). A review of sex differences in peer relationship processes: Potential trade-offs for the emotional and behavioral development of girls and boys. Psychological Bulletin, 132(1), 98–131.
Rubenstein, E., Pretzel, R. E., Windham, G. C., Schieve, L. A., Wiggins, L. D., DiGuiseppi, C., et al. (2017). The broader autism phenotype in mothers is associated with increased discordance between maternal-reported and clinician-observed instruments that measure child autism spectrum disorder. Journal of Autism and Developmental Disorders, 47(10), 3253–3266.
Rutherford, M., McKenzie, K., Johnson, T., Catchpole, C., O’Hare, A., McClure, I., & Murray, A. (2016). Gender ratio in a clinical population sample, age of diagnosis and duration of assessment in children and adults with autism spectrum disorder. Autism, 20(5), 628–634. https://doi.org/10.1177/1362361315617879.
Rutter, M., Le Couteur, A., & Lord, C. (2003). Autism diagnostic interview-revised. Los Angeles, CA: Western Psychological Services.
Rydzewska, E., Hughes-McCormack, L. A., Gillberg, C., Henderson, A., MacIntyre, C., Rintoul, J., & Cooper, S. A. (2019). Prevalence of sensory impairments, physical and intellectual disabilities, and mental health in children and young people with self/proxy-reported autism: Observational study of a whole country population. Autism, 23(5), 1201–1209.
Schertz, H. H., Odom, S. L., Baggett, K. M., & Sideris, J. H. (2016). Parent-reported repetitive behavior in toddlers on the autism spectrum. Journal of Autism and Developmental Disorders, 46(10), 3308–3316.
Schoen, E., Paul, R., & Chawarska, K. (2011). Phonology and vocal behavior in toddlers with autism spectrum disorders. Autism Research, 4(3), 177–188.
Schroeder, S. R., Marquis, J. G., Reese, R. M., Richman, D. M., Mayo-Ortega, L., Oyama-Ganiko, R., et al. (2014). Risk factors for self-injury, aggression, and stereotyped behavior among young children at risk for intellectual and developmental disabilities. American Journal on Intellectual and Developmental Disabilities, 119, 351–370. https://doi.org/10.1352/1944-7558-119.4.351.
Seltzer, M. M., Shattuck, P., Abbeduto, L., & Greenberg, J. S. (2004). Trajectory of development in adolescents and adults with autism. Mental Retardation and Developmental Disabilities Research Reviews, 10(4), 234–247.
Shattuck, P. T., Durkin, M., Maenner, M., Newschaffer, C., Mandell, D. S., Wiggins, L., et al. (2009). Timing of identification among children with an autism spectrum disorder: Findings from a population-based surveillance study. Journal of the American Academy of Child & Adolescent Psychiatry, 48(5), 474–483.
Simonoff, E., Pickles, A., Charman, T., Chandler, S., Loucas, T., & Baird, G. (2008). Psychiatric disorders in children with autism spectrum disorders: Prevalence, co-morbidity, and associated factors in a population-derived sample. Journal of the American Academy of Child and Adolescent Psychiatry, 47(8), 921–929.
Solomon, M., Miller, M., Taylor, S. L., Hinshaw, S. P., & Carter, C. S. (2012). Autism symptoms and internalizing psychopathology in girls and boys with autism spectrum disorders. Journal of Autism and Developmental Disorders, 42(1), 48–59.
Strother, E., Lemberg, R., Stanford, S. C., & Turberville, D. (2012). Eating disorders in men: Underdiagnosed, undertreated, and misunderstood. Eating Disorders, 20(5), 346–355.
Szatmari, P., Liu, X. Q., Goldberg, J., Zwaigenbaum, L., Paterson, A. D., Woodbury-Smith, M., et al. (2012). Sex differences in repetitive stereotyped behaviors in autism: Implications for genetic liability. American Journal of Medical Genetics Part B: Neuropsychiatric Genetics, 159(1), 5–12.
Thurm, A., Farmer, C., Salzman, E., Lord, C., & Bishop, S. (2019). State of the field: Autism versus Intellectual Disability. Frontiers in Psychiatry, 10, 526–536.
Torske, T., Nærland, T., Øie, M. G., Stenberg, N., & Andreassen, O. A. (2018). Meta-cognitive aspects of executive function are highly associated with social functioning on parent-rated measures in children with autism spectrum disorder. Frontiers in Behavioral Neuroscience, 11, 258. https://doi.org/10.3389/fnbeh.2017.00258.
van Wijngaarden-Cremers, P. J., van Eeten, E., Groen, W. B., van Deurzen, P. A., Oosterling, I. J., & van der Gaag, R. J. (2014). Gender and age differences in the core triad of impairments in autism spectrum disorders: A systematic review and meta-analysis. Journal of Autism and Developmental Disorders, 44(3), 627–635. https://doi.org/10.1007/s10803-013-1913-9.
Van’t Hof, M., Ester, W. A., Serdarevic, F., van Berckelaer-Onnes, I., Hillegers, M. H., Tiemeier, H., & Jansen, P. W. (2020). The sex-specific association between autistic traits and eating behavior in childhood: An exploratory study in the general population. Appetite, 147(147), 104519. https://doi.org/10.1016/j.appet.2019.104519.
Varni, J. W., Lovaas, O. I., Koegel, R. L., & Everett, N. L. (1979). An analysis of observational learning in autistic and normal children. Journal of Abnormal Child Psychology, 7(1), 31–43.
Ventola, P. E., Kleinman, J., Pandey, J., Barton, M., Allen, S., Green, J., & Fein, D. (2006). Agreement among four diagnostic instruments for autism spectrum disorders in toddlers. Journal of Autism and Developmental Disorders, 36(7), 839–847.
Wallace, G. L., Llewellyn, C., Fildes, A., & Ronald, A. (2018). Autism spectrum disorder and food neophobia: Clinical and subclinical links. The American Journal of Clinical Nutrition, 108(4), 701–707.
Watt, N., Wetherby, A. M., Barber, A., & Morgan, L. (2008). Repetitive and stereotyped behaviors in children with autism spectrum disorders in the second year of life. Journal of Autism and Developmental Disorders, 38(8), 1518–1533.
Werling, D. M., & Geschwind, D. H. (2013). Sex differences in autism spectrum disorders. Current Opinion in Neurology, 26(2), 146–153. https://doi.org/10.1097/WCO.0b013e32835ee548.
Westwood, H., Eisler, I., Mandy, W., Leppanen, J., Treasure, J., & Tchanturia, K. (2016). Using the autism-spectrum quotient to measure autistic traits in anorexia nervosa: A systematic review and meta-analysis. Journal of Autism and Developmental Disorders, 46(3), 964–977.
Westwood, H., Mandy, W., & Tchanturia, K. (2017). Clinical evaluation of autistic symptoms in women with anorexia nervosa. Molecular Autism, 8(1), 12–21.
Westwood, H., & Tchanturia, K. (2017). Autism spectrum disorder in anorexia nervosa: An updated literature review. Current Psychiatry Reports, 19(7), 41–51.
Williams, P. G., Darlymple, N., & Neal, J. (2000). Eating habits of children with autism. Pediatric Nursing, 26, 259–264.
Wilson, C. E., Murphy, C. M., McAlonan, G., Robertson, D. M., Spain, D., Hayward, H., et al. (2016). Does sex influence the diagnostic evaluation of autism spectrum disorder in adults? Autism, 20(7), 808–819.
Zhang, Y., Li, N., Li, C., Zhang, Z., Teng, H., Wang, Y.,... & Sun, Z. (2020). Genetic evidence of gender difference in autism spectrum disorder supports the female-protective effect. Translational Psychiatry, 10(1), 1–10.
Zhou, H., Zhang, L., Zou, X., Luo, X., Xia, K., Wu, L., & Fombonne, E. (2017). Chinese norms for the Autism Spectrum Rating Scale. Neuroscience Bulletin, 33(2), 161–167.
Zhou, H., Li, C. P., Huang, Y., Zou, X. B., Luo, X. R., Wu, L. J.,... & Wang, Y. (2019). Reliability and validity of the translated Chinese version of Autism Spectrum Rating Scale (2–5 years). World Journal of Pediatrics, 15(1), 49–56.
Zucker, N. L., Losh, M., Bulik, C. M., LaBar, K. S., Piven, J., & Pelphrey, K. A. (2007). Anorexia nervosa and autism spectrum disorders: guided investigation of social cognitive endophenotypes. Psychological Bulletin, 133(6), 976–1006.
Zwaigenbaum, L., Bryson, S. E., Szatmari, P., Brian, J., Smith, I. M., Roberts, W.,... & Roncadin, C. (2012). Sex differences in children with autism spectrum disorder identified within a high-risk infant cohort. Journal of Autism and Developmental Disorders, 42(12), 2585–2596.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2021 Springer Nature Switzerland AG
About this chapter

Cite this chapter
Shulman, C., Bing, O. (2021). Sex/Gender and Repetitive and Restrictive Behaviors in Autism Spectrum Disorder. In: Gal, E., Yirmiya, N. (eds) Repetitive and Restricted Behaviors and Interests in Autism Spectrum Disorders. Autism and Child Psychopathology Series. Springer, Cham. https://doi.org/10.1007/978-3-030-66445-9_7
Download citation
DOI: https://doi.org/10.1007/978-3-030-66445-9_7
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-66444-2
Online ISBN: 978-3-030-66445-9
eBook Packages: Behavioral Science and PsychologyBehavioral Science and Psychology (R0)