
Abstract
There are profound physiological changes in the function of the upper gastrointestinal tract during sleep. These sleep-related changes in both upper and lower esophageal sphincters, and corresponding changes in the salivary production, drive the clearance mechanisms and make sleep emerge as a vulnerable state for patients with Gastroesophageal Reflux Disease (GERD). Given the proximity of the upper airway to the upper gastrointestinal tract, a spectrum of respiratory symptoms that includes apnea, choking, and cyanosis are reported in neonates and young infants with GERD. Furthermore, sleep-related GERD can lead to sleep fragmentation, while Obstructive Sleep Apnea (OSA) and GERD share bidirectional cause and effect relationships. This chapter describes some of the pertinent mechanisms of sleep and GER and reviews the role of sleep in modulation of symptoms of sleep disordered breathing across the pediatric age spectrum.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
- Sleep Related GERD
- Laryngopharyngeal Reflux (LPR)
- Apnea of Prematurity (AOP)
- Brief Resolved Unexplained Events (BRUE)
- Obstructive Sleep Apnea (OSA)
Sleep Related Changes in Upper Gastrointestinal Physiology
Sleep has a profound influence on the physiology of upper gastrointestinal tract and these state-dependent dynamic changes lead to marked alteration of esophageal and gastric function. There is reduction in upper esophageal sphincter pressure, decreasing from 40 mm during wakefulness to 10 mm with sleep onset [1]. The circadian rhythm of basal gastric acid secretion peaks between 8.00 pm and 1.00 am [2]. Sleep disrupts gastroenteric function leading to delayed gastric emptying [3]. There is a marked decrease in swallowing during sleep (an average of 2 swallows per hour during total sleep time) with almost no deglutition during stages 3 and 4 [4, 5]. Along with decreased deglutition frequency during sleep, saliva production was found to be essentially absent [4, 6]. Normal saliva production and deglutition are vital mechanisms in the process of esophageal acid clearance, a pivotal defense mechanism against the development of GERD-related symptoms and inflammation. Thus, sleep hinders the normal clearance mechanisms and leads to prolonged acid clearance time [7]. A summary of these changes is listed below.
Sleep related changes in upper gastrointestinal physiology |
Fall in upper esophageal sphincter tone Reduced swallow frequency Decreased salivary secretion Prolonged acid clearance time Delayed gastric emptying |
Sleep and Gastroesophageal Reflux: Sleep Is a Vulnerable State for GERD
Gastroesophageal reflux (GER), the retrograde passage of gastric contents into the esophagus, is a normal physiologic process that occurs in all age groups. The main protective barrier for GER is the lower esophageal sphincter (LES), which consists of a 2–4 cm high-pressure zone at the level of the gastroesophageal junction. The LES operates as a dual sphincter mechanism consisting of a ring of thickened circular muscle and the diaphragmatic crura. The LES receives cholinergic innervation and the crural diaphragm receives bilateral phrenic nerve innervation. The occurrence of a vagally mediated and transient LES relaxation (TLESR) constitutes the primary mechanism for GER; these TLESRs events are brief, are not related to weak lower esophageal sphincter pressure, and occur independent of swallowing [8]. Esophageal clearance factors are important defensive mechanisms that neutralize the acid refluxate and minimize acid exposure to esophageal and extra-esophageal structures. These include salivation and primary peristaltic contractions triggered by saliva-stimulated swallowing. In addition, salivary bicarbonate also neutralizes the acid refluxate [9]. When awake, GER is most likely to happen in the post prandial period when there is abdominal distention and TLESR. These episodes are short and are rapidly cleared as the acid mucosal contact enhances salivary flow also stimulates a higher frequency of swallowing. However, the swallow frequency and salivary production are almost nonexistent during stable sleep [4, 5], and sleep related reflux events will occur predominantly during arousals and awakenings and, if recurrent in sufficient frequency, can lead to mucosal injury as a result of impaired clearance mechanisms.
A pediatric based survey has estimated that vomiting, a common symptom GER, occurs in 50% of infants in the first 3 months of life, in 6% of 4-month-old infants, and in 5% of 10–12 month old infants [10, 11]. Most episodes of GER last <3 minutes, occur in the postprandial period, and cause few or no symptoms. However, a subset of children develops pathologic gastroesophageal reflux disease (GERD) which is associated with plethora of gastrointestinal and extra gastrointestinal symptoms. These symptoms include feeding difficulties, failure to thrive, heartburn/chest pain, dystonic posturing, and recurrent respiratory symptoms of coughing, stridor, and wheezing. The estimated prevalence of GERD in infants 0–23 months, children 2–11 years old, and adolescents 12–17 years old is 2.2–12.6%, 0.6–4.1%, and 0.8–7.6%, respectively [12, 13]. It is important to realize that in healthy persons, sleep is relatively free of GER events.
However, given the dynamic changes in sleep as they relate to alteration in clearance mechanisms, it is not surprising that many patients experience frequent nighttime symptoms of regurgitation, heart burn, insomnia, and poor quality of sleep. These symptoms cumulatively grouped as a distinct diagnostic entity as “Sleep Related Gastroesophageal Reflux” in International Classification of Sleep Disorders (ICSD) [14]. Essential features of this diagnosis include heartburn, substernal burning, chest discomfort, coughing, choking, or unexplained excessive day time sleepiness, even in the absence of typical reflux symptoms. Sleep related GER is also associated with sleep onset and sleep maintenance insomnia, early morning awakenings, sleep disturbances, arousals, unrefreshing sleep, daytime dysfunction. A national random sample telephone survey to estimate the prevalence of frequent GERD and nocturnal GERD concluded that over all prevalence of frequent GERD was 14% and nocturnal GERD was 10%. Seventy four percent of those with frequent GERD symptoms reported nocturnal GERD symptoms [15]. Similarly, in a Gallup survey of 100 adults conducted on behalf of the American Gastroenterological association, 79% respondents had nighttime symptoms and 40% reported that these nighttime symptoms diminished their ability to function well the next day [16]. Despite the fact that GERD is common in children of all ages, the exact prevalence of nighttime symptoms and sleep disturbance in children has not been well studied, and there is paucity of information and minimal research on the bidirectional relationships of GERD and sleep in pediatric population. Indeed, the recently published clinical practice guidelines on Pediatric Gastroesophageal reflux did not specify any sleep-related symptoms [17]. A questionnaire-based study identified infants and young children with pathologic reflux, compared with population norms, as having a greater prevalence of nighttime awakenings, delayed onset of sleep during the night, and greater prevalence of daytime sleep [18]. Another large-scale cross-sectional study on Japanese junior high school students found that problem behaviors in adolescents are associated with some sleep problems, including sleep bruxism, as well as several lifestyle and food habits and GERD symptoms [19]. In another study of snoring obese children without evidence of OSA, simultaneously performed polysomnographic and MII-pH studies concluded that acid GER caused increased arousals and awakenings sleep interruptions [20]. Assessing the impact of GERD treatment in improving the sleep quality in adolescents, 8 weeks of esomeprazole improved the sleep dysfunction domains of quality of life in a prospective randomized controlled study [21].
GERD and OSA: Bidirectional Relationship?
In patients with obstructive sleep apnea, the increased collapsibility of the upper airway leads to progressive increases in respiratory effort during periods of heightened upper airway resistance, thereby generating very large intrathoracic pressure swings. Such intrathoracic pressure swings may promote reflux of gastric contents into the distal esophagus. With the impaired clearance mechanisms that characterize the sleep state, such reflux episodes can be prolonged, leading to increased mucosal damage and thus symptoms of esophagitis. Such effects can be compounded by the supine position during sleep, and these effects can be further multiplied by the concurrent presence of obesity, a common co-morbid condition in patients with obstructive sleep apnea. Thus, from a physiological perspective, it is natural to assume that three pathophysiological consequences in the relationship with GERD and OSA are present, namely a) gastroesophageal reflux is estimated to occur with higher degree of prevalence in patients with obstructive sleep apnea, b) there will be temporal relationship between respiratory events and reflux parameters, and c) the severity of OSA will correlate with the severity of GERD.
The frequency of nocturnal GER in adult patients with obstructive sleep apnea ranges from 54% to 76%, and application of nasal CPAP resulted in marked improvement of nocturnal GER [22]. One study found that five of six patients with OSA who underwent pH monitoring had markedly abnormal nocturnal GER, and that application of CPAP reduced GER frequency [23]. Graf and coworkers found that 11 of 17 patients with OSA had abnormal GER but failed to establish a temporal relationship, as well as any other relation between GER and the severity of OSA [24]. In addition to these small studies, Ing and colleagues compared nighttime pH monitoring results in patients with AHI <5/ hrTST (n = 41) to those with and AHI index >15 /hrTST (n = 63). Patients with AHI >15 /hrTST experienced more GER events, and nasal CPAP reduced GER in both groups suggesting a nonspecific effect [25]. Additionally, CPAP reduced the mean duration of reflux episodes, as well as the total percentage time of reflux in six non OSA patients with GER, further confirming the non-specific effect of CPAP in reducing nocturnal GER [26]. Unfortunately, few studies are available in children on this specific issue. In a small sample of otherwise healthy children referred to sleep laboratory to rule out OSA, a high prevalence of GER was observed in children with OSA [27]. In addition, and similar to the aforementioned studies in adult patients, no time-based or severity-based relationships emerged between OSA events and reflux episodes [27]. In another small series of 18 children with obstructive sleep apnea, gastroesophageal reflux was frequent and occurred in 41% children. However, no temporal relationship was observed between the respiratory events and reflux events and furthermore, there was no correlation between the severity of OSA and the presence and severity of GERD [28].
Laryngopharyngeal Reflux: LPR
Extraesophageal symptoms are common in patients with GERD. The principal protective barrier for the prevention of extraesophageal reflux is the Upper Esophageal Sphincter (UES), a zone of high pressure that includes the cricopharyngeus muscle. Due to sleep related changes in the decrease of upper esophageal sphincter tone in combination with prolonged clearance time, sleep state may promote proximal retrograde migration of gastric contents breaching the UES with the resultant pharyngolaryngeal injury. Recent studies in adults have identified that the etiology, pathogenesis, clinical manifestations, and the treatment of these symptoms are indeed unique, and significantly differs from conventional GERD, being actually viewed as a variant. Thus, the term LPR (laryngopharyngeal reflux) has been coined to describe this separate entity, and the abundance of publications in the recent literature justifies its consideration and discussion [29]. Indeed, while GERD represents the digestive manifestations of the disease, LPR represents the upper airway manifestations of this disease process. Hoarseness, dysphonia, sore throat, and dysphagia are common symptoms. Although GERD symptoms can be present in patients with LPR, symptoms related to LPR are exclusively extraesophageal, predominantly laryngopharyngeal in majority of cases, with no associated GI symptoms [30].
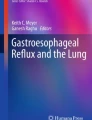
Although extraesophageal reflux and its associated laryngopharyngeal symptoms are well characterized in adults, recent reports seem to indicate that a similar presentation spectrum also occurs in children. Indeed, chronic rhinitis and rhinosinusitis and laryngeal disorders have been reported in children associated with laryngopharyngeal reflux [31]. Furthermore, an increased prevalence of GER has been associated with the presence of increased risk for adenoidal hypertrophy in young children [32]. This association strongly supports the role of chronic chemical irritation and ensuing inflammation resulting from GERD and promoting lymphoid hyperplasia in the upper airway, thus contributing to adenotonsillar hypertrophy. The putative role of extraesophageal reflux as a cause of adenotonsillar hypertrophy leading to OSA has been highlighted by a recent publication of a case report. A 7-year-old child with adenotonsillar hypertrophy and OSA had severe GERD confirmed by 24 hr. pH probe monitoring. This patient also had an endoscopically confirmed diagnosis of laryngopharyngeal reflux (Fig. 8.1). The adenotonsillar hypertrophy and laryngeal changes improved significantly with acid suppression therapy, and such changes were also associated with ameliorations in overnight polysomnographic findings [33]. Intuitively, one can propose that a subset of patients with OSA is likely to present with LPR, and that appropriate treatment of LPR may decrease the severity of OSA. Given that the treatment for OSA in children is surgical, it is imperative to look for evidence of GERD in general, and LPR in particular, in an effort to minimize the need for invasive surgical treatments.

Laryngopharyngeal Reflux. Endoscopic view of Laryngopharyngeal reflux reveals thickened epiglottis, posterior glottic swelling, and almost complete obstruction of the larynx with grade 3 subglottic stenosis. (From Stapleton and Brodsky [33]. Reprinted with permission from Elsevier)
While the diagnosis of GERD is based on well-established criteria based on 24 hr. pH probe monitoring, similar criteria are not present for defining LPR, and the diagnosis is often challenging and based on empirical assumptions, usually by incorporating the symptoms and upper airway endoscopic findings. Endoscopic abnormalities are often localized in regions of the larynx, particularly involving the posterior laryngeal wall, the arytenoid cartilages, interarytenoid areas, and the posterior third of the vocal cords. Although adding a hypopharyngeal sensor in the context of the conventional dual pH probe recording may increase the diagnostic yield of LPR, demonstration of reflux events can be best achieved by multichannel intraluminal impedance (MII) studies. Symptom-based diagnosis has low diagnostic specificity and laryngoscopic findings have low sensitivity. In addition, only 40% of patients with laryngeal findings attributed to LPR have objectively confirmed reflux events measured by MII pH [34]. Treatment is often lengthy, usually requiring 2–6 months administration of high dose, twice daily, acid suppression therapy [35].
Many of the published studies have investigated relationships between OSA and GERD, but very few studies have explored the relationship between LPR and OSA. It has been hypothesized that the causal relationship between LPR and OSA is actually bidirectional. The swings in negative intrathoracic pressure related to repetitive obstructive apneas promote reflux of gastric contents into the esophagus. Proximal migration of the refluxate into the laryngopharyngeal structures is promoted by sleep-related decrease in the clearance mechanisms, as well as by the sleep-associated decrease in upper esophageal sphincter tone, Over time, the pharyngeal inflammation related to LPR may then contribute to the progression of OSA by enhancing the collapsibility of the upper airway, likely mediated by the activation and propagation of local inflammatory and sensory neuropathic mechanisms [36] (Fig. 8.2). Indeed, significant improvement s in the severity of OSA have been reported in adults by implementation of an aggressive anti-reflux therapy regimen [37].

Schematic drawing of the relationship between OSA and LPR disease. (From Eskiizmir and Kezirian [36]. Reprinted with permission from Elsevier)
Modulation of Cardiorespiratory Events in Neonates and Infants: Role of Sleep and GER
Protective Airway Reflexes
For better understanding of the interrelationship between GER and cardiorespiratory events in neonates and infants, it is important to recognize two important airway protective reflexes, namely the laryngeal chemoreflex and the esophago-glottal closure reflex. Active glottic closure is involved in both reflexes, and plays an important role in preventing aspiration, but can potentially promote apnea. The laryngeal chemoreflex is elicited by stimulation of laryngeal mucosal receptors by various liquids and the esophago-glottal closure reflux is elicited by distension of the proximal esophagus [38,39,40].
Apnea of Prematurity (AOP)
The estimated prevalence of GERD is about 10% in sick infants in the Neonatal Intensive Care Unit (NICU) [41]. Pre-term infants are at increased risk for GER partly because of their large fluid intake in addition to the age-specific supine position. A causal relationship between AOP and GER has long been suspected due to the observations that AOP occurs more frequently in the immediate post-prandial period and that the apneic episodes are more likely to occur after episodes of regurgitation, Consequently, the laryngeal chemoreflex has been suggested as the possible mechanism. These observations have been supported by animal studies wherein stimulation of laryngeal chemoreceptors with various liquids, milk formula, and acidic fluids can provoke a prolonged and fatal apnea [42]. The hypothesis on this causative linkage has been also been confirmed in human preterm infants [38]. Such assumptions led to widespread use of anti-GER medications in the newborn nursery with an expectation that this will reduce the frequency and severity of the apneic episodes. Few earlier studies have shown an association between regurgitation and apnea. Nine pre-term infants and one term infant showed a 14-fold increase in prolonged apnea frequency immediately following regurgitation [43]. However, in a subsequent study, no relationship between the occurrence of GER and apneas was identified in a study of 20 premature infants with a concurrent history of persistent AOP [44]. Furthermore, GER treatment did not reduce the frequency of apnea in 132 premature infants <36 weeks of gestational age [45]. A proposed explanation for the lack of such association between apneas and reflux events was that it was nonacid reflux, undetectable by conventional pH monitoring, that operated as the culprit for AOP causation. This led to implementation of novel diagnostic MII techniques for detection of both acid and non-acid reflux events [46]. However, in a study of 19 preterm infants, using MII technology in conjunction with cardiorespiratory monitoring, Poets et al. concluded that both reflux and apneic events are common, but that no temporal relationships can be identified between cardiorespiratory events and GER [47]. As neonates sleep 80% of the time, it is likely that sleep state might modulate the frequency and severity of these events. To identify the role of sleep in the modulation of GER and to define the spatio-temporal characteristics of GER, respiratory events, and sleep state, Jadcherla et al. have performed concurrent polysomnography with pH impedance study in a group of neonates who are hospitalized in NICU. There were 18 neonates who were hospitalized with apparent life-threatening events, apnea, desaturations, bradycardia, cyanosis, and stridor, with mean post menstrual age of 41 weeks at the time of study. A total of 317 GER events during 16 hours of polysomnography were analyzed. The study concluded that (1) frequency of impedance positive events were significantly less during sleep, (2) proximal migration of refluxate is also significantly less during sleep, and (3) frequency of respiratory symptoms were significantly decreased during sleep [48].
Brief Resolved Unexplained Event (BRUE) (Apparent Life-Threatening Event: ALTE)
Apparent Life-Threatening Events are frightening episodes in infants characterized by a combination of apnea, color change, abnormal muscle tone, choking, and gagging that require an intervention by the observer [49]. In 2016, the American Academy of Pediatrics (AAP) released a clinical guideline for practitioners recommending that the term ALTE be replaced by Brief Resolved Unexplained Event (BRUE) [50]. The aim was to allay the anxiety to the caregivers brought about by the use of the term ALTE, as well as to give practitioners clear management guidance by stratifying such infants into high- and low-risk groups. In patients with ALTE, apnea is the most frequently reported symptom, and 60–70% of patients with ALTE will also manifest the presence of recurrent regurgitation or emesis. Thus, GER has been suspected as a causative factor for ALTE. Indeed, up to 40–80% of patients with ALTE have abnormal pH monitoring studies. However, despite such associations, efforts to document a temporal relationship between ALTE and GER by simultaneous polysomnographic and pH probe studies have failed to convincingly demonstrate the occurrence of this process. Indeed, 14 infants with abnormal GER scores and a history of apnea did not show a temporal relationship between reflux and apneic events, the latter being considered as a manifestation of more general developmental delay [51] (Figs. 8.3 and 8.4). In another study of 20 infants with ALTE with no clinical symptoms of emesis, no correlations between duration, lowest value of esophageal pH, and the number of apneas or duration of apneas could be found [52]. Even in patients with proven GER and ALTE, no relationship between GER and obstructive episodes in terms of frequency, duration, or temporal occurrence was detected [53]. Although it is often stated that gastroesophageal reflux is the most common cause of a brief resolved unexplained event or apparent life-threatening event, a recent literature search of multiple cross-sectional observational studies concluded that there are very few data to support the hypothesis of cause and effect [54]. Thus, based on the current evidence, in the majority of infants, GER is not related to ALTE, although a clear temporal relation based on history, observation or testing may occur in individual infants.

Temporal relationship between obstructive events and reflux events

Possible mechanisms for the relationship between obstructive sleep apnea syndrome (OSAS) and gastroesophageal reflux disease (GERD). The mechanisms of the specific linkage between OSAS and GER are not fully elucidated, but possible explanations include the generation of large negative intrathoracic pressures, insufficient lower esophageal sphincter (LES) function, increased arousals, autonomic neural unbalance, and obesity predisposing to both conditions. TLESR transient lower esophageal sphincter relaxations. (From: Mizuta et al. [55])
Thus, both GER and apneic episodes (central/obstructive) are common in vulnerable infants in specific age groups, but there is an apparent lack of temporal relationships between the apneic events and GER. Several plausible reasons for the lack of such relationship could include (1) methodological issues such as small cohort size, selection bias, different methods for the diagnosis of apnea and GER, (2) the two conditions may share a common causative mechanism, and (3) different mechanisms for airway obstruction other than laryngeal closure with regurgitation may be operational.
References
Kahrilas PJ, Dodds WJ, Dent J, et al. Effect of sleep, spontaneous gastroesophageal reflux, and a meal on upper esophageal sphincter pressure in normal human volunteers. Gastroenterology. 1987;92(2):466–71.
Moore JG, Englert E. Circadian rhythm of gastric acid secretion in man. Nature. 1970;226:1261–2.
Orr WC, Dubois A, Stahl ML, et al. Gastric function during sleep. Sleep Res. 1978;7:72.
Schneyer LH, Pigman W, Hanahan L, et al. Rate of flow of human parotid, sublingual and sub maxillary secretions during sleep. J Dent Res. 1956;35:109–14.
Lichter J, Muir RC. The pattern of swallowing during sleep during sleep. Electroencephalogr Clin Neurophysiol. 1975;38:427–32.
Lichter J, Muir RC. The pattern of swallowing during sleep. Electroencephalogr Clin Neurophysiol. 1975;38:427–32.
Sondheimer JM. Clearance of spontaneous gastroesophageal reflux in awake and sleeping infants. Gastroenterol. 1989;97:821–6.
Kawahara H, Dent J, Davidson G. Mechanisms responsible for gastroesophageal reflux in children. Gasteroenterol. 1997;113(2):399–408.
Helm JF, Reidel DR, Teeter BC, et al. Determinants of esophageal acid clearance in normal subjects. Gastroenterol. 1983;85:807–12.
Nelson SP, Chen EH, Syniar GM, Christoffel KK. Prevalence of symptoms of gastroesophageal reflux during childhood: a pediatric practice-based survey. Pediatric Practice Research Group. Arch Pediatr Adolesc Med. 2000 Feb;154(2):150–4.
Nelson SP, Chen EH, Syniar GM, Christoffel KK. One-year follow-up of symptoms of gastroesophageal reflux during infancy. Pediatric Practice Research Group. Pediatrics. 1998 Dec;102(6):E67.
Martigne L, et al. Prevalence and management of gastroesophageal reflux disease in children and adolescents: a nationwide cross-sectional observational study. Eur J Pediatr. 2012;171(12):1767–73.
Hegar B, et al. Natural evolution of regurgitation in healthy infants. Acta Paediatr. 2009;98(7):1189.
American Academy of Sleep Medicine. International classification of sleep disorders. 3rd ed. Darien, IL: American Academy of Sleep Medicine; 2014.
Farup C, Kleinman L, Sloan S, et al. The impact of nocturnal symptoms associated with gastroesophageal reflux disease on health related quality life. Arch Intern Med. 2001;161(1):45–52.
Shaker R, Castell DO, Schoenfeld PS, et al. Nighttime heart burn is an underappreciated clinical problem that impacts sleep and day time function: the results of a Gallup survey conducted on behalf of American Gastroenterological Association. Am J Gastroenterol. 2003;98(7):487–93.
Rosen R, Vandenplas Y, Singendonk M, et al. Pediatric Gastroesophageal Reflux Clinical Practice Guidelines: Joint Recommendations of the North American Society for Pediatric Gastroenterology, Hepatology, and Nutrition and the European Society for Pediatric Gastroenterology, Hepatology, and Nutrition. J Pediatr Gastroenterol Nutr. 2018;66:516–54.
Ghaem M, Armstrong KL, Trocki O, et al. The sleep patterns of infants and young children with gastroesophageal reflux. J Pediatr Child Health. 1998;34:160–3.
Sakaguchi K, Yagi T, Maeda A, et al. Association of problem behavior with sleep problems and gastroesophageal reflux symptoms. Ped Int. 2014;56:24–30.
Strehl Machado R, Woodley F, Mlusa H, et al. Gastroesophageal reflux affects sleep quality in snoring obese children. Pediatr Gastroenterol Hepatol Nutr. 2016 Mar;19(1):12–9.
Gunasekaran T, Tolia V, Collen RB, et al. Effects of esomeprazole treatment for gastroesophageal reflux disease on quality of life in 12–17 yr old adolescents: An international health outcomes study. BMC Gasroenterol. 2009;9:84.
Zanation AM, Senior BA. The relationship between extraesophageal reflux and obstructive sleep apnea. Sleep Med Rev. 2005;9:453–8.
Kerr P, Shoenut JP, Milar T, et al. Nasal CPAP reduces gastroesophageal reflux in obstructive sleep apnea syndrome. Chest. 1992;101:1539–44.
Graf KI, Karaus M, Hieneman S, et al. Gastroesophageal reflux in patients with sleep apnea syndrome. Z Gastroenterol. 1995;33:889–93.
Ing AJ, Ngu MC, Breslin AB. Obstructive Sleep Apnea and gastroesophageal reflux. Am J Med. 2000;108:120s–5s.
Kerr P, Shoenut JP, Steens RD, et al. Nasal continuous positive airway pressure. A new treatment for nocturnal gastroesophageal reflux? J Clin Gastroenterol. 1993;17:276–80.
Bandla H, Statza T, Rice T. Gastroesophageal reflux in children with obstructive sleep apnea syndrome. Am J Resp Crit Care Med. 2002;A263
Noronha AC, de Bruin VM, Nobree Souza MA, et al. Gastroesophageal reflux and obstructive sleep apnea in childhood. Int J Pediatric Otorhinolaryngol. 2009;73:383–9.
Koulman J, Sataloff RT, Toohill R. Laryngopharyngeal reflux: consensus conference report. J Voice. 1996;10:215–6.
Celik M, Ercan I. Diagnosis and management of laryngopharyngeal reflux disease. Curr Opin Otolaryngol Head Neck Surg. 2006 Jun;14(3):150–5.
Bothwell MR, Parson DS, Talbot A, et al. Outcome of reflux therapy on pediatric chronic sinusitis. Otolaryngol Head Neck Surg. 1999;121:255–62.
Carr MM, Pole CP, Ehrig D, et al. Incidence of reflux in young children undergoing adenoidectomy. Laryngoscope. 2001;111:2170–2.
Stapleton A, Brodsky L. Extraesophageal acid reflux induced adenotonsillar hyperplasia. Case report and literature review. Int J Pediatr Otorhinolaryngol. 2008;72:409–13.
de Bortoli N, Savarinno NA, et al. How many cases of laryngopharyngeal reflux suspected by laryngoscopy are gastroesophageal reflux disease related? World J Gastroenterol. 2012;18(32):4364–70.
Ford CN. Evaluation and management of laryngopharyngeal reflux. JAMA. 2005;294:1534–40.
Eskiizmir G, Kezirian E. Is there a vicious cycle between obstructive sleep apnea and laryngopharyngeal reflux disease? Med Hypotheses. 2009 Nov;73(5):706–8.
Steward DL. Pantoprazole for sleepiness associated with acid reflux and obstructive sleep disordered breathing. Laryngoscope. 2004;114:1525–8.
Perkett EA, Vaughan RL. Evidence for a laryngeal chemoreflex in some human preterm infants. Acta Paediatr Scand. 1982;71(6):969–72.
Thach BT. Maturation and transformation of reflexes that protect the laryngeal airway from liquid aspiration from fetal to adult life. Am J Med. 2001;111 Suppl 8A:69S–77S.
Jadcherla SR. Upstream effect of esophageal distention: effect on airway. Curr Gastroenterol Rep. 2006;8(3):190–4.
Jadcherla SR, Peng J, Chan CY, et al. Significance of gastroesophageal refluxate in relation to physical, chemical and spatiotemporal characteristics in symptomatic intensive care unit neonates. Pediatr Res. 2011;70:192–8.
Storey AT, Johnson P. Laryngeal water receptors initiating apnea in the lamb. Exp Neurol. 1975;47(1):42–55.
Menon AP, Schefft GL, Thatch BT. Apnea associated with regurgitation in infants. J Pediatr. 1985;106:625–9.
de Ajuriaguerra M, Radvanyi-Bouvet MF, Huon C, et al. Gastroesophageal reflux and apnea in prematurely born infants during wakefulness and sleep. Am J Dis Child. 1991;145:1132–6.
Kimball AL, Carlton DP. Gastroesophageal reflux medications in the treatment of apnea in premature infants. J Pediatr. 2001;138:355–60.
Wenzl TG, Silny J, Schenke S, et al. Gastroesophageal reflux and respiratory phenomena in infants: status of the intraluminal impedance technique. J Pediatr Gastroenterol Nutr. 1999;28:423–8.
Peter CS, Sprodowski N, Bohnhorst B, et al. Gastroesophageal reflux and apnea of prematurity. No temporal relationship. Pediatrics. 2002;109:8–11.
Qureshi A, Malkar M, Splaingard M, Khuhro A, Jadcherla S. The role of sleep in the modulation of gastroesophageal reflux and symptoms in NICU neonates. Pediatr Neurol. 2015;53(3):226–32.
National Institutes of Health Consensus Development Conference on Infantile Apnea and Home Monitoring, Sept 29 to Oct 1, 1986. Pediatrics. 1987;79(2):292–9.
Tieder JS, Bonkowsky JL, Etzel RA, et al. Brief resolved unexplained events (formerly apparent life-threatening events) and evaluation of lower-risk infants. Pediatrics. 2016;137:e20160590.
Walsh JK, Farell MK, Lucas M, et al. Gastroesophageal reflux in infants: relation to apnea. J Pediatr. 1981;99:197–201.
Kahn A, Rebuffat E, Sottiaux M, et al. Lack of temporal relation between acid reflux in the proximal oesophagus and cardiorespiratory events in sleeping infants. Eur J Pediatr. 1992;151:208–12.
Payton JY, Macfayden U, Williams A, et al. Gastro-oesophageal reflux and apnoeic pauses during sleep in infancy–no direct relationship. Eur J Pediatr. 1990;149:680–6.
Jilani NZ, Hussain A, Al Ansari K, et al. Gastrooesophageal reflux is not a major cause of brief resolved unexplained events in infants. Breathe. 2019;15:e32–9.
Mizuta Y, Takeshima F, Shikuwa Y. Is there a specific linkage between obstructive sleep apnea syndrome and gastroesophageal reflux disease? Digest Endosc. 2006;18:88–97.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2021 Springer Nature Switzerland AG
About this chapter

Cite this chapter
Bandla, H.P.R. (2021). Sleep and the Gastrointestinal System. In: Gozal, D., Kheirandish-Gozal, L. (eds) Pediatric Sleep Medicine. Springer, Cham. https://doi.org/10.1007/978-3-030-65574-7_8
Download citation
DOI: https://doi.org/10.1007/978-3-030-65574-7_8
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-65573-0
Online ISBN: 978-3-030-65574-7
eBook Packages: MedicineMedicine (R0)