
Abstract
Diffuse cystic lung diseases (DCLDs) are a heterogeneous group of diseases that need a detailed clinical, radiological, and sometimes pathological evaluation to reach at the underlying diagnosis. Disease-modifying therapies are available for a few diseases such as lymphangioleiomyomatosis (LAM) and pulmonary Langerhans cell histiocytosis (PLCH), and should be considered in patients with progressive or advanced disease. In addition, the management of patients with DCLDs includes prevention and treatment of complications such as spontaneous pneumothorax. This chapter reviews the key aspects of clinical, radiological, and other diagnostic modalities as well as the currently available treatment options that can help physicians in managing DCLD patients.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
- Cyst
- Lymphangioleiomyomatosis (LAM)
- Pulmonary Langerhans cell histiocytosis (PLCH)
- Birt-Hogg-Dubé (BHD) syndrome
- Lymphocytic interstitial pneumonia (LIP)
- Sjögren syndrome
- Amyloidosis
- Light chain deposition disease (LCDD)
- Malignancy
Introduction
Diffuse cystic lung diseases (DCLDs) are a heterogeneous group of diseases that differ significantly with respect to pathogenesis, clinical course, treatment, and prognosis. Underlying DCLD is usually discovered in one of the following scenarios:
-
1.
Patients presenting with chronic respiratory symptoms such as cough and/or dyspnea on exertion.
-
2.
Patients presenting with acute onset symptoms due to complications such as spontaneous pneumothorax.
-
3.
Screening in at-risk populations such as adult women with tuberous sclerosis complex (TSC) or those with personal or family history of other genetic conditions such as Birt-Hogg-Dubé (BHD) syndrome.
-
4.
Incidentally discovered abnormalities on chest or abdomen imaging done for other reasons.
Patients with DCLDs can have respiratory symptoms such as cough and dyspnea, and it is not uncommon to misdiagnose patients as having one of the more prevalent diseases such as chronic obstructive pulmonary disease or asthma. Pneumothorax is another common complication and can be the presenting manifestation of underlying DCLDs, thereby confusing the picture with primary spontaneous pneumothorax [1]. A detailed knowledge about these diseases is thus necessary for proper management of these patients. Chest high-resolution computed tomography (HRCT) remains the single most useful noninvasive diagnostic test for the evaluation of suspected DCLDs. DCLDs often have characteristic imaging findings, which can help narrow the differential diagnoses. Frequently, a confident diagnosis can be made based on CT findings and integration with clinical information. However, confirmatory tests, by either laboratory testing, tissue biopsy, or genetic analysis may be required in some cases, where clinico-radiological information is not sufficient to establish a confident diagnosis.
In this chapter, we summarize the approach toward the proper diagnosis and management of patients presenting with DCLD. In particular, we focus on the major causes of DCLDs that are most likely to be encountered in clinical practice: lymphangioleiomyomatosis (LAM), BHD, pulmonary Langerhans cell histiocytosis (PLCH), lymphocytic interstitial pneumonia (LIP)/follicular bronchiolitis (FB), amyloidosis/light chain deposition disease (LCDD), and malignancy.
Clinical Evaluation
History
A thorough and comprehensive history may provide invaluable information that can help identify the underlying etiology of DCLDs. The development of acute, rapidly progressive cystic change is usually suggestive of an infectious, inflammatory, or traumatic origin, whereas chronic processes are more likely to be secondary to neoplastic, congenital, lymphoproliferative, or other slowly progressive disorders [2].
Patient demographics may make certain diseases more likely than others. Diseases such as congenital pulmonary airway malformation (CPAM), bronchopulmonary dysplasia, and other congenital malformations are seen primarily in childhood but can uncommonly present de novo in the adult [3, 4]. Sporadic LAM is almost exclusively seen in women. While approximately 10–15% of men with TSC can have pulmonary cysts characteristic of LAM, symptomatic LAM in TSC is almost exclusively restricted to women. There is a strong association between cigarette smoking and diseases that can present with cystic changes in the lungs such as PLCH, desquamative interstitial pneumonia (DIP), and respiratory bronchiolitis, such that the presence of these diseases is unlikely in a never-smoker.
Detailed family history is an important component of history taking when evaluating patients with DCLDs. Family history of pulmonary cysts on chest imaging, pneumothoraces, skin lesions, or renal tumors can be suggestive of BHD or TSC-LAM. A history of pneumothorax within the second-degree relatives is much more suggestive of BHD than LAM [5].
Common respiratory symptoms attributable to DCLDs include cough and dyspnea on exertion. Cough is usually nonproductive; however, hemoptysis and chyloptysis can occur in a small proportion of patients with LAM [6]. Dyspnea is rare in patients where cysts or other parenchymal abnormalities are limited such as in BHD. Dyspnea can however develop or worsen acutely due to a spontaneous pneumothorax. Spontaneous pneumothorax is more common in patients with LAM, BHD and PLCH, as opposed to the other DCLDs, and usually presents in the third or fourth decade of life similar to the overall demographic of patients with a primary spontaneous pneumothorax. However, in contrast to primary spontaneous pneumothorax, DCLD patients presenting with a spontaneous pneumothorax have a much higher risk of recurrence if treated conservatively [7]. Pneumothorax can also occur in patients with Pneumocystis jiroveci pneumonia (PJP), connective tissue disorders such as Marfan and Ehlers-Danlos syndrome, and patients with cystic pulmonary metastases especially from underlying sarcomas such as osteogenic sarcoma, angiosarcoma, and synovial cell sarcoma with higher reported rates in patients on chemotherapy [8].
A complete review of systems is essential and often provides helpful diagnostic clues. The presence of sicca symptoms, dental caries, increased thirst, arthritis/synovitis, skin rash, and/or Raynaud’s can suggest autoimmune LIP/FB as the cause of the DCLD. Frequent infections might suggest underlying immune deficiency states such as HIV and common variable immune deficiency (CVID), which are associated with LIP/FB. History of bone pain, skeletal lesions, and/or polydipsia may be a feature of extrapulmonary involvement due to histiocytic disorders such as PLCH and Erdheim-Chester disease. A subset of LAM patients may experience chylous discharge through urine, stool, or vagina. Cyclical variation of symptoms in conjunction with their menstrual cycles and post-coital hemoptysis may also be present in a subset of LAM patients.
Presence of certain diseases or manifestations can help narrow down the differential diagnosis (Table 18.1). Skin lesions and/or renal tumors can be seen in patients with BHD and in patients with TSC-LAM. Presence of DCLD in patients with TSC is highly suggestive of LAM. Similarly, the presence of renal angiomyolipomas or co-existing chylous effusions in women with characteristic cystic change on chest CT is considered diagnostic for LAM. FB/LIP is associated with a wide variety of underlying systemic autoimmune diseases, lymphoproliferative diseases, and immunodeficiency states (e.g., common variable immunodeficiency, HIV). Pulmonary amyloidosis and LCDD are commonly associated with underlying plasma cell dyscrasias or connective-tissue disorders, particularly Sjögren’s, where MALT lymphoma may also be seen [9,10,11]. Common clinical features of systemic amyloidosis include nephrotic syndrome with or without renal insufficiency, congestive cardiomyopathy, sensorimotor and/or autonomic peripheral neuropathy, hepatomegaly, macroglossia, and hemostatic abnormalities [12]. Patients with LCDD often have co-existing renal involvement, usually in conjunction with hematological malignancies such as multiple myeloma or lymphoma [13, 14].
Physical Examination
Pulmonary exam is usually not specific enough to help ascertain a diagnosis in patients with DCLDs. Wheezing is rare in DCLDs and if present usually suggests underlying COPD or asthma. Bibasilar rales can be heard in patients with LIP or other ILDs with interstitial infiltrates or fibrosis. A high-pitched blowing sound termed “amphoric breathing” can sometimes be heard in cases of large cysts communicating with the bronchus due to turbulent airflow [15]. Diminished breath sounds on one side compared to the contralateral side might suggest the presence of a pneumothorax.
In contrast to the limited utility of pulmonary examination in patients with suspected DCLDs, extrapulmonary findings can often provide clinically useful diagnostic clues. Clubbing is rare and, if present, can be suggestive of underlying malignancy. Particular attention must be paid to the signs of underlying connective tissue disease or skin findings suggestive of BHD or TSC. Patients with BHD often have characteristic skin fibrofolliculomas, which are white to flesh-colored papules, 2–4 mm in size, on the face, neck, ear lobes, and upper trunk, and are not painful or pruritic. These lesions can be difficult to differentiate from perifollicular fibroma and angiofibromas, which are more commonly seen in TSC [16, 17]. Uncommonly, skin lesions presenting as brown to purplish papules and eczematoid or seborrhea-like lesions can be seen in patients with PLCH [18]. Petechiae, purpura, and nail dystrophy can be seen in patients with systemic amyloidosis [19]. Presence of connective tissue disorders such as skeletal anomalies, hyperextensibility, and distinct facial features could suggest a genetic syndrome such as Marfan or Ehlers-Danlos syndrome.
Diagnostic Evaluation
Laboratory testing can be a useful adjunct to aid in establishing the diagnosis of DCLDs (Table 18.2). Serum vascular endothelial growth factor-D (VEGF-D) levels are elevated in women with sporadic LAM compared to healthy controls and patients with other DCLDs, and serum VEGF-D levels ≥800 pg/mL are considered diagnostic in patients with typical CT features [20, 21]. A probable diagnosis of LAM based on serum VEGF-D levels ≥600 pg/mL may be sufficient in some situations, such as for patients who have a low burden of disease that would not justify treatment, or those who are not interested in therapies or interventions [21]. It is critical to not confuse VEGF-D quantification with the more commonly commercially available VEGF quantification. In the United States, serum VEGF-D testing performed in a manner meeting College of American Pathologists (CAP)/Clinical Laboratory Improvements Amendments (CLIA) standards is only available at the Translational Trial Development and Support Laboratory based at Cincinnati Children’s Hospital Medical Center. Directions for test requisition, sample processing, and shipment are available here: https://www.testmenu.com/cincinnatichildrens/Tests/665748.
Autoimmune panel can suggest underlying rheumatological disease, particularly Sjögren’s, which can be associated with FB/LIP. Approximately 80% of patients with FB/LIP also have serum dysproteinemias; most commonly hypergammaglobulinemia, but hypogammaglobulinemia can occur in the setting of CVID [22]. Screening for monoclonal proteins should be pursued in patients suspected to have amyloidosis or LCDD. A comprehensive panel that includes serum immunofixation (IFE), serum protein electrophoresis (SPEP), and serum free light chain (FLC) should be ordered to ensure adequate sensitivity [23, 24]. Addition of urine IFE and UPEP can further increase sensitivity particularly in LCDD [24]. Attention should be paid to the free light chain ratio as this may be the only abnormality present on screening in some patients [25].
Besides the abovementioned labs, genetic analyses can be useful in certain patients. For instance, FLCN mutation analysis is available as a diagnostic test and detects mutations in ~90% of patients with BHD and should be considered in patients with family history of pneumothorax, renal tumors, skin lesions, or patients with feature, suggestive of BHD in the absence of a positive family history [26]. Similarly, detection of TSC1/TSC2 mutations can help confirm the presence of underlying TSC in cases where the clinical criteria for TSC have not been met and there is high clinical suspicion [27].
Pulmonary Function Testing
Pulmonary function testing (PFT) in patients with DCLDs can be normal, or demonstrate obstructive, restrictive, or mixed abnormalities depending on cause and extent of disease. Patients with LAM, PLCH and FB most often have obstructive defects. PFTs are often normal in patients with BHD. While PFTs do not have diagnostic value, they have been shown to correlate with extent of disease on CT and serve as the primary modality used to monitor disease course and response to therapy in patients with DCLDs [28, 29]. In addition, the rate of change in PFTs is a commonly utilized end point in clinical trials aiming to develop novel therapeutic options for DCLD patients.
Radiological Assessment
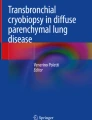
Chest X-rays are usually not helpful in detailed evaluation of pulmonary cysts but can reveal the presence of pneumothorax or pleural effusions, which can sometimes be seen in patients with DCLDs and may warrant intervention. HRCT scanning is crucial in the evaluation of patients with DCLD. Critical review of the HRCT for cyst characteristics such as shape, size, wall thickness, and distribution, as well as other co-existing findings can reveal patterns that can help accurately diagnose the underlying condition in greater than two-thirds of patients [30,31,32], and substantially narrow the differential in the rest. The CT features of various DCLDs have been discussed in detail in Chap. 3, and key features are summarized in Tables 18.3 and 18.4, and Fig. 18.1.

Chest computed tomography images of common diffuse cystic lung diseases. (a) Axial and (b) coronal cuts on high-resolution chest computed tomography (HRCT) of a patient with lymphangioleiomyomatosis showing multiple smooth, round, thin-walled parenchymal cysts. (c) Axial and (d) coronal cuts on HRCT chest of a patient with pulmonary Langerhans cell histiocytosis showing multiple nodules and cysts. (e) Axial and (f) coronal cuts on HRCT chest of a patient with Birt-Hogg-Dubé syndrome showing lentiform cysts in a basilar distribution. (g) Axial and (h) coronal cuts on HRCT chest of a patient with lymphocytic interstitial pneumonia in a patient with showing multiple cysts of varying sizes and ground-glass opacities
Evaluation of cystic lung disease begins with ascertaining that the lesions on HRCT scan are true cysts and not mimics such as cavities, emphysema, and cystic bronchiectasis as discussed in Chap. 14. However, occasionally true cysts and cyst mimics may co-exist in the same patient. Solitary cysts are usually congenital, age-related phenomenon or may be a remnant of prior trauma or infection. Age-related cysts are mostly 1–5 in number, in the peripheral area of the lower lobes and remain unchanged or slightly increase in size over time [33]. These can be seen in people above 40 years old, and the prevalence increases with age. However, all solitary cysts should not be ignored, as malignancy can also present as a solitary cyst. One helpful clue to distinguish between age-related benign solitary/few cysts from malignancy associated-cysts can be the wall thickness; increased wall thickness has been associated with increasing chances of malignancy. However, the reliance on wall thickness is not 100% sensitive or specific as early cancers can present with cystic airspaces that are initially thin but became thicker overtime. Lesions can also develop nodules (endophytic or exophytic) or increase in nodule size or density over time with a consequent decrease in airspace size; however, this is not a consistent feature [34]. Other features suggestive of malignancy are nonuniform cystic walls, cyst septations, ground-glass opacity around the cyst and irregular margins, lymphadenopathy, and presence of solid or nonsolid tissue intermixed with cysts [35,36,37].
Cysts in LAM are numerous and are uniformly round or oval and diffusely distributed throughout the pulmonary parenchyma. BHD cysts have a lower lung zone predominance, and frequently abut the pleural surface and proximal segments of the lower lobe pulmonary artery or veins. The larger cysts are often irregular or lentiform in shape and can be multiseptated. Another key feature of BHD is the elliptical (floppy) paramediastinal cysts; the presence of three or more elliptical paramediastinal cysts or disproportionate paramediastinal cysts is considered to be pathognomonic of BHD [38]. Recently, a quantitative analysis using paired inspiratory and expiratory CTs for estimating the extent of cyst-airway communication has been found to be useful in distinguishing BHD from other DCLDs [39].
The cysts in PLCH have varying sizes and shapes, with a predominance in the mid and upper lung fields and relative sparing of the lung bases and costophrenic angles. FB/LIP cysts vary in size and can be >50–70 mm in diameter and often have eccentric vessels at the periphery. The cysts in LIP are randomly distributed with a slight basal predominance. Lymphoma can complicate cystic lung disease in LIP and should be considered if there is associated nodularity especially large nodules, consolidation, and/or effusions [40]. Cysts in amyloidosis and LCDD are thin-walled, multiple, bilateral, small to medium in size, and often in a peri-bronchovascular distribution with lower lobe predominance [9, 10, 41].
Besides detailed evaluation of cysts, attention should also be paid to ancillary findings such as nodules, ground-glass opacities, lymphadenopathy, and pleural effusions. Nodules can be seen in PLCH, cystic metastases, LIP, amyloidosis, and LCDD. The presence of calcified nodules is a fairly characteristic finding seen in amyloidosis but not in LCDD and can be used to differentiate between the two conditions [9, 10]. Nodules in LIP are generally small and centrilobular. Ground-glass opacities are often seen in patients with PJP, DIP, and LIP. Due to the presence of smoking exposure in the vast majority of patients with PLCH, co-existing RB/DIP-like changes are commonly seen in PLCH and can cause the appearance of ground-glass attenuation on HRCT [42]. Mediastinal and hilar lymphadenopathy can be seen in LIP, amyloidosis, and cystic metastases. Lymphadenopathy can be bulky and associated with calcification in amyloidosis [43]. Lymphadenopathy can also be seen in patients with LAM; however, the lymphadenopathy in LAM generally tends to follow a reverse cranio-caudal gradient such that the biggest lymph nodes are in the pelvic region and tend to get progressively less bulky along the thoracic duct. Intervening lung parenchyma between cysts appears grossly normal in LAM and BHD. This is especially true for patients with sporadic LAM. Patients with TSC-LAM, however, can have multiple bland appearing nodules in addition to the cystic change. These micronodular changes most commonly represent a benign condition known as multifocal micronodular pneumocyte hyperplasia (MMPH). MMPH does not tend to progress or cause physiological impairment in these subjects [44]. It must be noted that cystic metastasis particularly from endometrial stromal sarcomas can also present exclusively as pulmonary cysts without any other radiographic abnormality [45].
Other radiological imaging may also help in clinching the diagnosis in DCLDs. Abdominal imaging can show renal tumors, which can be suggestive of LAM or BHD. AMLs are pathognomonic of LAM [46], and majority can be easily identified on CT scan and MRI due to their high fat content [47]. Identification of extrapulmonary neoplasms can be suggestive of cystic metastasis. The renal tumors in BHD can be bilateral and multifocal and provide a clue to the underlying diagnosis [48].
18-Fluoro deoxy (FDG) positron emission tomography (PET) scan can sometimes be useful in evaluation of cystic lung lesions. FDG-PET is often positive in lung cancers and metastases but given that lesions smaller than 1 cm may fall below the sensitivity threshold for FDG-PET, it can yield false-negative results when solid components, such as wall thickness or nodule size, are below this threshold [49, 50]. Moreover, FDG-PET is often negative in tumors with low metabolic activity such as low-grade adenocarcinomas and in situ pulmonary adenocarcinomas. FDG-PET may be helpful in assessing extrapulmonary disease activity in patients with PLCH and amyloidosis [51,52,53]. Within the lungs, a positive FDG-PET scan in PLCH is more likely in patients with early disease associated with predominantly nodular chest CT scan findings and can at times be difficult to differentiate from malignancy [51, 52]. Results for PET-CT in amyloidosis are also variable but a standardized uptake value (SUV) uptake greater than 3.0 should raise suspicion for malignancies or associated lymphoma or plasmacytoma [53]. PET-CT can also be helpful in evaluation for malignancy in patients with Sjögren’s where a SUV max in the parotid gland of ≥4.7 and/or the presence of focal pulmonary lesions can be highly suggestive of lymphoma [54].
Pathological Evaluation
Pathologic evaluation may be required in patients where diagnosis remains uncertain after a thorough review of the clinical and radiological data. Bronchoalveolar lavage (BAL) has limited diagnostic utility and is primarily useful to rule out infectious etiologies such as PJP. The presence of more than 5% CD1a cells on BAL has been proposed as a confirmatory diagnostic finding in patients with suspected PLCH but is limited by its lack of sensitivity and is not clinically useful in most patients [55]. Bronchoscopy with transbronchial lung biopsy can be helpful in establishing the diagnosis in cases of LAM and PLCH with the diagnostic yield being more than 50% in patients with LAM and 30–50% in patients with PLCH [2]. Transbronchial lung cryobiopsy is a relatively new technique that involves freezing the lung tissue with compressed cold gas and allows the extraction of larger pieces of tissue than the traditional forceps-guided transbronchial lung biopsy. The safety and diagnostic yield of transbronchial lung cryobiopsy in patients with DCLD has not been systematically evaluated. As such, its use is perhaps best reserved in centers with expertise in the technique. Anecdotal evidence suggests that transbronchial lung cryobiopsy may be a potentially useful modality to obtain tissue in DCLD patients and is likely to have better diagnostic yield than conventional transbronchial lung biopsy [56, 57]. Video-assisted thoracoscopic surgery (VATS)-guided surgical lung biopsy remains the gold standard modality to obtain tissue for histopathological confirmation.
On pathology, true cysts have an epithelial cell lining compared to discontinuous epithelial lining resulting from parenchymal loss as seen in emphysema or post-traumatic pseudocysts. Histological features of BHD cysts are generally not distinctive and may be indistinguishable from those of emphysema, but can include hyperplastic type II pneumocyte-like cells and positive staining for PCNA and p-S6 [58]. LAM, PLCH, amyloidosis, LCDD, and metastatic disease may show diagnostic cellular proliferations or material deposition. Proliferation of spindle cells that stain positive for HMB-45, smooth muscle actin, and estrogen and progesterone receptors is characteristic of LAM, while infiltration with Langerhans cells positive for CD1a, Langerin, and S100 is seen in PLCH [59]. Amorphous eosinophilic material is seen in amyloidosis and LCDD, and distinction can be made based on Congo red staining or material deposition seen on electron microscopy [59]. Cellular interstitial infiltrates are seen in patients with FB/LIP. Immunohistochemical studies and flow cytometry should be performed in order to distinguish between the polyclonal populations of lymphocytes seen in LIP and a monotypic cell population seen in malignant lymphoproliferative disorders.
Occasionally, the diagnosis may be established by biopsy of an involved site outside the thorax. Biopsy of skin fibrofolliculomas can establish the diagnosis of BHD and is particularly important as lung biopsy in patients with BHD is not pathognomonic. Bone biopsy can be pursued for suspected lesions in PLCH. Lip biopsy is usually the procedure of choice in the diagnosis of suspected Sjögren’s. Subcutaneous abdominal fat aspirate and bone marrow biopsy may be examined for suspected amyloid, but a negative result does not necessarily exclude pulmonary amyloidosis [12].
Diagnostic Approach
While a large proportion of patients may present with symptoms secondary to DCLDs, it is not uncommon for patients to present with mild or no symptoms. A considerable subgroup of patients with DCLDs, especially those without underlying high-grade malignancies, may remain stable and not warrant any therapy. Moreover, pulmonary cysts can develop normally in some individuals, as an age-related phenomenon, and do not always represent a true pathology. Thus, the diagnostic algorithm and management must be tailored according to the individual patient’s presentation, risks and preferences. For instance, it may be reasonable to pursue serial longitudinal monitoring of the clinical course in a patient with mild DCLD due to uncertain cause as long as there are minimal or no symptoms, and pursue invasive diagnostic testing if and when patient is at risk of morbidity or mortality due to disease. On the other hand, if there is a suspicion for high-grade malignancy – further evaluation with biopsy, FGD-PET, and/or serial CT scans should be pursued regardless of symptoms. We usually tend to follow the clinical course in asymptomatic or minimally symptomatic patients who do not have substantial physiological (normal PFTs) or radiological disease burden (≤10 cysts on CT).
We tend to approach evaluation of DCLDs in a stepwise manner where the first step is to decipher whether the parenchymal lucencies represent true cysts or other noncystic parenchymal opacities. Once we identify true cysts, we categorize the patients on the basis of underlying cyst profusion into pauci-cystic (≤10 cysts) or multi-cystic (>10 cysts) (Fig. 18.2). Age-related cysts and a variety of diseases such as parasitic infections, traumatic pneumatoceles, primary lung cancers, and congenital cysts generally present with pauci-cystic disease. It is worth mentioning, however, that occasionally the diseases typically associated with multi-cystic chest radiology may be detected very early in the disease course at a pauci-cystic stage, highlighting the importance of continued longitudinal monitoring of patients with cystic lung disease. A proposed algorithm for work-up of patients with pauci-cystic and multi-cystic DCLDs is shown in Figs. 18.3 and 18.4.

Algorithm to classify cystic lung diseases based on chest computed tomography. BHD Birt-Hogg-Dubé syndrome, DIP desquamative interstitial pneumonia, FB follicular bronchiolitis, LAM lymphangioleiomyomatosis, LCDD light chain deposition disease, LIP lymphocytic interstitial pneumonia, PLCH pulmonary Langerhans cell histiocytosis, PJP pneumocystis jiroveci pneumonia, RB respiratory bronchiolitis

Algorithm to guide approach to the diagnosis of pauci-cystic lung diseases. GGOs ground-glass opacities

Algorithm to guide approach to the diagnosis of diffuse multi-cystic lung diseases. AML angiomyolipoma, BAL broncheoalveolar lavage, BHD Birt-Hogg-Dubé syndrome, BRAF v-Raf murine sarcoma viral oncogene homolog B, CT computed tomography, CTD connective tissue diseases, DCLD diffuse cystic lung disease, DI diabetes insipidus, DIP desquamative interstitial pneumonia, FB follicular bronchiolitis, FDG-PET 18-Fluoro deoxy positron emission tomography, FLCN folliculin, GGOs ground-glass opacities, HRCT high-resolution computed tomography, HP hypersensitivity pneumonitis, ILD interstitial lung disease, LAM lymphangioleiomyomatosis, LCDD light chain deposition disease, LIP lymphoid interstitial pneumonia, MAPK mitogen-activated protein kinase, PLCH pulmonary Langerhans cell histiocytosis, SS Sjögren syndrome, Tbbx transbronchial biopsy, TSC tuberous sclerosis complex, VATS video-assisted thoracoscopic surgery, VEGF-D vascular endothelial growth factor-D. (Modified from Gupta et al. [2])
Diagnosis of DCLD involves a detailed clinical and radiological assessment as discussed previously, with the need for invasive biopsies considered on a case-by-case basis depending upon the disease and symptom burden and the patient/physician’s desire to establish a certain diagnosis. Key clinical, radiological, and pathological features of common causes of DCLDs are summarized in Table 18.4. Disease-specific diagnostic guidelines are available for a few diseases such as LAM and BHD and also for diseases associated with DCLDs such as TSC (associated with LAM) and Sjögren’s (associated with LIP, amyloidosis, and/or LCDD), and are summarized in Table 18.5.
Management
Screening for DCLDs
Screening for DCLDs with CT scan of chest should be pursued in certain situations. While all cases of recurrent spontaneous pneumothorax should undergo evaluation by CT scan, preferably after re-expansion of the lung, the role of CT scan after the first episode of spontaneous pneumothorax remains unclear. It is advisable to consider chest CT imaging in first-time spontaneous pneumothorax if there is a positive family history or if the patient is female, because the discovery of either BHD or LAM, respectively, has important management implications [26]. We follow the approach of performing CT scan after first episode of an apparent primary spontaneous pneumothorax in all patients as this approach can lead to timely diagnosis of underlying conditions and allow the pursuit of appropriately aggressive interventions to reduce the pneumothorax recurrence risk. The strategy to pursue screening chest CT scan to evaluate for DCLDs in patients presenting with an apparent primary spontaneous pneumothorax has been demonstrated to be cost-effective in a recent analysis [1, 60].
Certain high-risk patient groups warrant screening CT scans to evaluate for underlying DCLDs. Given the high prevalence of LAM in women with TSC, all women with TSC should undergo a baseline chest HRCT starting at the age of 18 years, regardless of pulmonary symptoms. In cases where the screening CT is negative, repeat imaging can be performed every 5 years, or sooner as dictated by pulmonary symptoms [61]. For TSC women with documented evidence of LAM on chest CT, the repeat HRCT interval can be reduced to every 2–3 years in order to gauge the trajectory of disease progression. These follow-up CT scans can be done using low-dose radiation protocols. In addition, these patients should undergo periodic (at least annual) pulmonary function testing. Sporadic renal AMLs (without TSC) can be associated with LAM in approximately 10% of the patients and discovery of renal AMLs should prompt consideration of screening for LAM with chest CT [62].
General Management
As with any other chronic lung disease, it advisable to quit smoking and inhalation of any potentially harmful agents such as vaping and marijuana. Smoking (and marijuana) cessation is the cornerstone of treatment in patients with PLCH and can lead to disease regression or stabilization in a substantial proportion of patients. Patients should be advised to stay up to date with influenza and pneumococcal vaccines. Pulmonary rehabilitation could be an effective intervention to improve symptoms, health-related quality of life, and functional status in patients with impaired exercise tolerance [63, 64]. General recommendations applicable to all DCLD patients are highlighted in Table 18.6.
Spontaneous pneumothorax is common in DCLD patients, particularly in patients with LAM, BHD and PLCH, and carries a very high risk of recurrence [7]. Patients should be made aware of symptoms suggestive of pneumothorax, and an action plan should be formulated in case of emergency. In contrast to patients with primary spontaneous pneumothorax, given the high risk of recurrence, patients with DCLDs (especially LAM, BHD, and PLCH) presenting with a spontaneous pneumothorax should undergo pleurodesis to reduce the recurrence risk following the first episode of spontaneous pneumothorax rather than waiting for a recurrent event [20, 65, 66]. We prefer VATS-guided mechanical pleurodesis as the initial modality. It is worth mentioning that prior pleurodesis is not a contraindication for future lung transplantation [67] and that when making the decision whether to pursue pleurodesis or not, generally more weight should be assigned to the reduction in morbidity arising from recurrent spontaneous pneumothoraces as opposed to the possibility of future technical difficulties in case there is need for lung transplantation.
Situations leading to increase in cyst size or pressure can predispose patients to develop pneumothorax. In accordance with the Boyle’s law of inverse relationship between pressure and volume, lung cysts have the potential to expand in size when exposed to atmospheric pressure changes such as during air travel or deep-sea diving. It is usually advised to avoid deep-sea diving as development of pneumothorax in these situations can potentially become life-threatening [68]. Air travel has been shown to have a low risk (~1 episode of spontaneous pneumothorax per 100 flights) particularly in patients with LAM, BHD, and PLCH. This risk of pneumothorax with air travel is usually not considered prohibitive unless the patient has severely reduced cardiopulmonary reserve and cannot tolerate a pneumothorax. Patients should be counselled about this risk and educated about concerning symptoms that might prompt appropriate medical evaluation prior to undertaking air travel. In addition to the risk of pneumothorax associated with air travel, DCLD patients should also undergo evaluation for the need of supplemental oxygen during air travel. These issues have been covered in detail in Chap. 17 of this textbook.
Specific Treatment
Inhaled bronchodilators can be tried, especially in patients with reversible airflow obstruction on pulmonary function testing and in patients who report symptomatic benefit from a bronchodilator trial [55, 69, 70]. Concomitant asthma may be present in some patients, and inhaled corticosteroids may be beneficial in this subset.
Disease -modifying therapies for LAM, PLCH, FB/LIP, and amyloidosis are available and should be considered if patients develop significant symptoms or exhibit a progressive decline in pulmonary function (Table 18.7). Use of the mechanistic target of rapamycin (mTOR) inhibitor, sirolimus, has been shown to stabilize lung function decline and improve the quality of life in patients with LAM, and is recommend for patients with abnormal lung function as defined by forced expiratory volume in one-second (FEV1) less than or equal to 70% predicted [46]. Sirolimus has also been shown to be effective in LAM patients with chylous complications such as chylous effusions, lymphangioleiomyomas, and in patients with rapidly declining lung function. mTOR inhibitors are efficacious and safe in controlling AML burden in patients with TSC, while preserving the renal parenchyma [71, 72]. Cladribine (2-chlorodeoxyadenosine) has been shown to be helpful in refractory systemic LCH and has also been used in isolated PLCH with reported improvement [73,74,75]. Multiple other chemotherapeutic regimens have been tried in patients with PLCH with limited success. Targeted treatment of PLCH with BRAF or MEK inhibition may be a promising therapeutic approach in the near future [76]. Treatment of FB/LIP relies on managing the underlying cause. Immunosuppression can be helpful in idiopathic LIP and LIP associated with autoimmune disease [77]. Clinical and radiological resolution of LIP has been reported with the use of antiretroviral drugs in cases of LIP secondary to HIV [78]. Treatment of amyloidosis and LCDD depends on the extent of organ involvement and options include autologous stem cell transplantation and a variety of chemotherapeutic drugs [79]. Solitary malignancy and some congenital lesions such as CPAM and bronchogenic cysts may be amenable to surgical resection because of their propensity to enlarge and to become infected as well as the potential risk for transformation into malignancy [80]. Lung transplantation remains a viable management option for patients with advanced DCLDs with patients having post-transplant survival either similar to (in case of PLCH) or better than (in case of LAM) the patients undergoing lung transplantation for other pulmonary disorders [81,82,83,84,85]; however, recurrence of disease in allograft can occur in some patients with LAM and PLCH [86].
Active surveillance and management for co-existing conditions or complications is warranted for certain DCLDs. Patients with LAM should be evaluated for presence of TSC and AMLs [61]. Serial screening of renal tumors in BHD is recommended [48]. Development of lymphoma is the most dreaded complications of Sjögren’s and can occur in ~5% of patients [77]. Although guidance on appropriate screening of lymphoma in these patients is lacking, development of three or more risk factors such as salivary gland enlargement, lymphadenopathy, Raynaud phenomenon, anti-Ro/SSA or/and anti-La/SSB autoantibodies, rheumatoid factor positivity, monoclonal gammopathy, and C4 hypocomplementemia have been associated with development of lymphoma [87]. Pulmonary hypertension is known to occur in patients with DCLDs, particularly LAM and PLCH [88,89,90], which may need further evaluation.
Conclusion
The combined synergy between scientists, clinicians, and patient advocacy organizations (Table 18.8) has enabled transformative progress in our understanding of the molecular pathogenesis and the development of novel therapeutic options in patients with DCLDs. The recent progress in LAM is perhaps the best exemplar of the abovementioned synergy driving meaningful progress. In a relatively short time span of approximately two decades, the collaborative effort between patients and scientists has led to major scientific breakthroughs in LAM, including identification of the causative gene, clear understanding of the disease pathogenesis, discovery of a blood-based biomarker that aids noninvasive diagnosis, and the development of FDA-approved treatment. Active efforts are underway to emulate the example of LAM and apply similar approaches to drive progress in other DCLDs. In conclusion, we submit that the DCLDs represent a unique set of disorders that are fundamentally distinct from the typical interstitial lung diseases in almost every aspect including the pathophysiology, radiological features, clinical phenotypes, natural history, and management strategies. Although rare individually, collectively DCLDs represent a substantial minority of the pulmonary practice and are being increasingly identified due to widespread use of CT scans and increased awareness. Knowledge regarding the nuances of appropriately diagnosing and treating DCLDs for clinicians is critical in order to provide optimal care to these patients. Finally, the discoveries made in this field are not only impacting the lives of patients with DCLDs but are also providing crucial insights into the pathobiology of more common conditions.
Key Learning Points
-
When evaluating a patient with cystic change on chest imaging, a detailed history with particular attention to demographics, inhaled exposures such as smoking, family history, and search for extrapulmonary features, including cutaneous, pleural, and intra-abdominal manifestations, can provide crucial insight into the underlying diagnosis.
-
High-resolution computed tomography is an essential component of the evaluation process, and careful evaluation of the cyst characteristics, such as profusion, distribution, and morphology, combined with ancillary pulmonary and extra-pulmonary findings, can help differentiate between the various causes of cystic lung diseases in a large proportion of patients.
-
Laboratory analysis can provide valuable information in patients with suspected DCLDs, and can sometimes be diagnostic such as elevated VEGF-D in LAM or establishment of diagnosis of Sjögren’s in a patient suspected to have FB/LIP.
-
Invasive procedures such as lung biopsy may be needed in some patients after exhausting the noninvasive diagnostic work-up. The decision to pursue invasive diagnostic procedures should be taken with careful consideration of future management implications and the knowledge that the diagnosis of DCLDs can generally be established by noninvasive means in over two-thirds of the patients.
-
Management of patients with DCLDs includes attention to the prevention and management of complications such as spontaneous pneumothorax. There is a high risk of recurrence of pneumothorax in these patients, and pleurodesis should be considered following the initial episode of spontaneous pneumothorax rather than waiting for a recurrent episode.
-
Disease-modifying therapies are available for certain DCLDs, such as mTOR inhibitors for LAM, with lung transplantation reserved for patients with advanced disease.
References
Gupta N. Primary spontaneous pneumothorax: looking beyond the usual. Acad Emerg Med. 2018;25(4):470–2.
Gupta N, Vassallo R, Wikenheiser-Brokamp KA, McCormack FX. Diffuse cystic lung disease. Part II. Am J Respir Crit Care Med. 2015;192(1):17–29.
Shanmugam G. Adult congenital lung disease. Eur J Cardiothorac Surg. 2005;28(3):483–9.
Hamanaka R, Yagasaki H, Kohno M, Masuda R, Iwazaki M. Congenital cystic adenomatoid malformation in adults: report of a case presenting with a recurrent pneumothorax and a literature review of 60 cases. Respir Med Case Rep. 2019;26:328–32.
Tobino K, Hirai T, Johkoh T, Kurihara M, Fujimoto K, Tomiyama N, et al. Differentiation between Birt–Hogg–Dubé syndrome and lymphangioleiomyomatosis: quantitative analysis of pulmonary cysts on computed tomography of the chest in 66 females. Eur J Radiol. 2012;81(6):1340–6.
Ryu JH, Moss J, Beck GJ, Lee J-C, Brown KK, Chapman JT, et al. The NHLBI lymphangioleiomyomatosis registry: characteristics of 230 patients at enrollment. Am J Respir Crit Care Med. 2006;173(1):105–11.
Cooley J, Lee YG, Gupta N. Spontaneous pneumothorax in diffuse cystic lung diseases. Curr Opin Pulm Med. 2017;23(4):323.
Hoag JB, Sherman M, Fasihuddin Q, Lund ME. A comprehensive review of spontaneous pneumothorax complicating sarcoma. Chest. 2010;138(3):510–8.
Zamora AC, White DB, Sykes A-MG, Hoskote SS, Moua T, Eunhee SY, et al. Amyloid-associated cystic lung disease. Chest. 2016;149(5):1223–33.
Baqir M, Moua T, White D, Eunhee SY, Ryu JH. Pulmonary nodular and cystic light chain deposition disease: a retrospective review of 10 cases. Respir Med. 2020;164:105896.
Jeong YJ, Lee KS, Chung MP, Han J, Chung MJ, Kim K-I, et al. Amyloidosis and lymphoproliferative disease in Sjögren syndrome: thin-section computed tomography findings and histopathologic comparisons. J Comput Assist Tomogr. 2004;28(6):776–81.
Gillmore JD, Wechalekar A, Bird J, Cavenagh J, Hawkins S, Kazmi M, et al. Guidelines on the diagnosis and investigation of AL amyloidosis. Br J Haematol. 2015;168(2):207–18.
Rho L, Qiu L, Strauchen JA, Gordon RE, Teirstein AS. Pulmonary manifestations of light chain deposition disease. Respirology. 2009;14(5):767–70.
Colombat M, Stern M, Groussard O, Droz D, Brauner M, Valeyre D, et al. Pulmonary cystic disorder related to light chain deposition disease. Am J Respir Crit Care Med. 2006;173(7):777–80.
Saraya T, Fujiwara M, Mikura S, Fukuda N, Ishii H, Takizawa H. Answer found in a blowing sound: Amphoric breathing due to cyst formation in pulmonary adenocarcinoma. Intern Med. 2019;58(3):423–5.
Misago N, Kimura T, Narisawa Y. Fibrofolliculoma/trichodiscoma and fibrous papule (perifollicular fibroma/angiofibroma): a revaluation of the histopathological and immunohistochemical features. J Cutan Pathol. 2009;36(9):943–51.
Nathan N, Burke K, Moss J, Darling T. A diagnostic and management algorithm for individuals with an isolated skin finding suggestive of tuberous sclerosis complex. Br J Dermatol. 2017;176(1):220–3.
Vassallo R, Ryu JH, Schroeder DR, Decker PA, Limper AH. Clinical outcomes of pulmonary Langerhans’-cell histiocytosis in adults. N Engl J Med. 2002;346(7):484–90.
Schreml S, Szeimies R-M, Vogt T, Landthaler M, Schroeder J, Babilas P. Cutaneous amyloidoses and systemic amyloidoses with cutaneous involvement. Eur J Dermatol. 2010;20(2):152–60.
Gupta N, Finlay GA, Kotloff RM, Strange C, Wilson KC, Young LR, et al. Lymphangioleiomyomatosis diagnosis and management: high-resolution chest computed tomography, Transbronchial lung biopsy, and pleural disease management. An official American Thoracic Society/Japanese respiratory society clinical practice guideline. Am J Respir Crit Care Med. 2017;196(10):1337–48.
Young LR, VanDyke R, Gulleman PM, Inoue Y, Brown KK, Schmidt LS, et al. Serum vascular endothelial growth factor-D prospectively distinguishes lymphangioleiomyomatosis from other diseases. Chest. 2010;138(3):674–81.
Strimlan CV, Rosenow EC III, Weiland LH, Brown L. Lymphocytic interstitial pneumonitis: review of 13 cases. Ann Intern Med. 1978;88(5):616–21.
Dispenzieri A, Kyle R, Merlini G, Miguel J, Ludwig H, Hajek R, et al. International myeloma working group guidelines for serum-free light chain analysis in multiple myeloma and related disorders. Leukemia. 2009;23(2):215–24.
Katzmann JA. Screening panels for monoclonal gammopathies: time to change. Clin Biochem Rev. 2009;30(3):105.
Nasr SH, Valeri AM, Cornell LD, Fidler ME, Sethi S, D’Agati VD, et al. Renal monoclonal immunoglobulin deposition disease: a report of 64 patients from a single institution. Clin J Am Soc Nephrol. 2012;7(2):231–9.
Boone PM, Scott RM, Marciniak SJ, Henske EP, Raby BA. The genetics of pneumothorax. Am J Respir Crit Care Med. 2019;199(11):1344–57.
Northrup H, Krueger DA, Roberds S, Smith K, Sampson J, Korf B, et al. Tuberous sclerosis complex diagnostic criteria update: recommendations of the 2012 international tuberous sclerosis complex consensus conference. Pediatr Neurol. 2013;49(4):243–54.
Paciocco G, Uslenghi E, Bianchi A, Mazzarella G, Roviaro GC, Vecchi G, et al. Diffuse cystic lung diseases: correlation between radiologic and functional status. Chest. 2004;125(1):135–42.
Avila NA, Chen CC, Chu SC, Wu M, Jones EC, Neumann RD, et al. Pulmonary lymphangioleiomyomatosis: correlation of ventilation-perfusion scintigraphy, chest radiography, and CT with pulmonary function tests. Radiology. 2000;214(2):441–6.
Koyama M, Johkoh T, Honda O, Tsubamoto M, Kozuka T, Tomiyama N, et al. Chronic cystic lung disease: diagnostic accuracy of high-resolution CT in 92 patients. Am J Roentgenol. 2003;180(3):827–35.
Sundaram B, Gross BH, Martinez FJ, Oh E, Müller NL, Schipper M, et al. Accuracy of high-resolution CT in the diagnosis of diffuse lung disease: effect of predominance and distribution of findings. Am J Roentgenol. 2008;191(4):1032–9.
Gupta N, Meraj R, Tanase D, James LE, Seyama K, Lynch DA, et al. Accuracy of chest high-resolution computed tomography in diagnosing diffuse cystic lung diseases. Eur Respir J. 2015;46(4):1196–9.
Araki T, Nishino M, Gao W, Dupuis J, Putman RK, Washko GR, et al. Pulmonary cysts identified on chest CT: are they part of aging change or of clinical significance? Thorax. 2015;70(12):1156–62.
Farooqi AO, Cham M, Zhang L, Beasley MB, Austin JH, Miller A, et al. Lung cancer associated with cystic airspaces. Am J Roentgenol. 2012;199(4):781–6.
Tan Y, Gao J, Wu C, Zhao S, Yu J, Zhu R, et al. CT characteristics and pathologic basis of solitary cystic lung cancer. Radiology. 2019;291(2):495–501.
Mascalchi M, Attinà D, Bertelli E, Falchini M, Vella A, Pegna AL, et al. Lung cancer associated with cystic airspaces. J Comput Assist Tomogr. 2015;39(1):102–8.
Fintelmann FJ, Brinkmann JK, Jeck WR, Troschel FM, Digumarthy SR, Mino-Kenudson M, et al. Lung cancers associated with cystic airspaces: natural history, pathologic correlation, and mutational analysis. J Thorac Imaging. 2017;32(3):176–88.
Escalon JG, Richards JC, Koelsch T, Downey GP, Lynch DA. Isolated cystic lung disease: an algorithmic approach to distinguishing Birt-Hogg-Dubé syndrome, Lymphangioleiomyomatosis, and lymphocytic interstitial pneumonia. Am J Roentgenol. 2019;212(6):1260–4.
Suzuki K, Seyama K, Ebana H, Kumasaka T, Kuwatsuru R. Quantitative analysis of cystic lung diseases by use of paired inspiratory and expiratory CT: estimation of the extent of cyst-airway communication and evaluation of diagnostic utility. Radiology: Cardiothorac Imag. 2020;2(2):e190097.
Hare S, Souza C, Bain G, Seely J, Frcpc, Gomes M, et al. The radiological spectrum of pulmonary lymphoproliferative disease. Br J Radiol. 2012;85(1015):848–64.
Sheard S, Nicholson A, Edmunds L, Wotherspoon A, Hansell D. Pulmonary light-chain deposition disease: CT and pathology findings in nine patients. Clin Radiol. 2015;70(5):515–22.
Vassallo R, Jensen EA, Colby TV, Ryu JH, Douglas WW, Hartman TE, et al. The overlap between respiratory bronchiolitis and desquamative interstitial pneumonia in pulmonary Langerhans cell histiocytosis: high-resolution CT, histologic, and functional correlations. Chest. 2003;124(4):1199–205.
Czeyda-Pommersheim F, Hwang M, Chen SS, Strollo D, Fuhrman C, Bhalla S. Amyloidosis: modern cross-sectional imaging. Radiographics. 2015;35(5):1381–92.
Konno S, Shigemura M, Ogi T, Shimizu K, Suzuki M, Kaga K, et al. Clinical course of histologically proven multifocal micronodular pneumocyte hyperplasia in tuberous sclerosis complex: a case series and comparison with lymphangiomyomatosis. Respiration. 2018;95(5):310–6.
Aubry M-C, Myers JL, Colby TV, Leslie KO, Tazelaar HD. Endometrial stromal sarcoma metastatic to the lung: a detailed analysis of 16 patients. Am J Surg Pathol. 2002;26(4):440–9.
McCormack FX, Gupta N, Finlay GR, Young LR, Taveira-DaSilva AM, Glasgow CG, et al. Official American Thoracic Society/Japanese respiratory society clinical practice guidelines: lymphangioleiomyomatosis diagnosis and management. Am J Respir Crit Care Med. 2016;194(6):748–61.
Campbell S, Uzzo RG, Allaf ME, Bass EB, Cadeddu JA, Chang A, et al. Renal mass and localized renal cancer: AUA guideline. J Urol. 2017;198(3):520–9.
Stamatakis L, Metwalli AR, Middelton LA, Linehan WM. Diagnosis and management of BHD-associated kidney cancer. Familial Cancer. 2013;12(3):397–402.
Sheard S, Moser J, Sayer C, Stefanidis K, Devaraj A, Vlahos I. Lung cancers associated with cystic airspaces: underrecognized features of early disease. Radiographics. 2018;38(3):704–17.
Gottumukkala RV, Fintelmann FJ, Keane FK, Shepard J-AO. Cystic lesions on lung Cancer screening chest computed tomography: when should we be concerned? Ann Am Thorac Soc. 2018;15(2):263–5.
Lee HJ, Ahn B-C, Lee S-W, Lee J. The usefulness of F-18 fluorodeoxyglucose positron emission tomography/computed tomography in patients with Langerhans cell histiocytosis. Ann Nucl Med. 2012;26(9):730–7.
Krajicek BJ, Ryu JH, Hartman TE, Lowe VJ, Vassallo R. Abnormal fluorodeoxyglucose PET in pulmonary Langerhans cell histiocytosis. Chest. 2009;135(6):1542–9.
Baqir M, Lowe V, Eunhee SY, Ryu JH. 18F-FDG PET scanning in pulmonary amyloidosis. J Nucl Med. 2014;55(4):565–8.
Keraen J, Blanc E, Besson FL, Leguern V, Meyer C, Henry J, et al. Usefulness of 18F-labeled Fluorodeoxyglucose–positron emission tomography for the diagnosis of lymphoma in primary Sjögren’s syndrome. Arthritis Rheumatol. 2019;71(7):1147–57.
Tazi A. Adult pulmonary Langerhans’ cell histiocytosis. Eur Respir J. 2006;27(6):1272–85.
Fruchter O, Fridel L, El Raouf BA, Abdel-Rahman N, Rosengarten D, Kramer MR. Histological diagnosis of interstitial lung diseases by cryo-transbronchial biopsy. Respirology. 2014;19(5):683–8.
Babiak A, Hetzel J, Krishna G, Fritz P, Moeller P, Balli T, et al. Transbronchial cryobiopsy: a new tool for lung biopsies. Respiration. 2009;78(2):203–8.
Furuya M, Tanaka R, Koga S, Yatabe Y, Gotoda H, Takagi S, et al. Pulmonary cysts of Birt-Hogg-Dubé syndrome: a clinicopathologic and immunohistochemical study of 9 families. Am J Surg Pathol. 2012;36(4):589–600.
Smith ML, Gotway MB, Larsen BT, Colby TV, Tazelaar HD, Leslie KO. Pathologic approach to cystic lung disease. AJSP Rev Rep. 2017;22(1):36–45.
Gupta N, Langenderfer D, McCormack FX, Schauer DP, Eckman MH. Chest computed tomographic image screening for cystic lung diseases in patients with spontaneous pneumothorax is cost effective. Ann Am Thorac Soc. 2017;14(1):17–25.
Krueger DA, Northrup H, Roberds S, Smith K, Sampson J, Korf B, et al. Tuberous sclerosis complex surveillance and management: recommendations of the 2012 international tuberous sclerosis complex consensus conference. Pediatr Neurol. 2013;49(4):255–65.
Ryu JH, Hartman TE, Torres VE, Decker PA. Frequency of undiagnosed cystic lung disease in patients with sporadic renal angiomyolipomas. Chest. 2012;141(1):163–8.
Nakazawa A, Cox NS, Holland AE. Current best practice in rehabilitation in interstitial lung disease. Therapeut Adv Respir Dis. 2017;11(2):115–28.
Araujo MS, Baldi BG, Freitas CS, Albuquerque AL, da Silva CCM, Kairalla RA, et al. Pulmonary rehabilitation in lymphangioleiomyomatosis: a controlled clinical trial. Eur Respir J. 2016;47(5):1452–60.
Gupta N, Kopras EJ, Henske EP, James LE, El-Chemaly S, Veeraraghavan S, et al. Spontaneous pneumothoraces in patients with Birt–Hogg–Dubé syndrome. Ann Am Thorac Soc. 2017;14(5):706–13.
Singla A, Kopras EJ, Gupta N. Spontaneous pneumothorax and air travel in pulmonary Langerhans cell histiocytosis: a patient survey. Respir Investig. 2019;57(6):582–9.
Weill D, Benden C, Corris PA, Dark JH, Davis RD, Keshavjee S, et al. A consensus document for the selection of lung transplant candidates: 2014 – an update from the pulmonary transplantation Council of the International Society for heart and lung transplantation. J Heart Lung Transplant. 2015;34(1):1–15.
Godden DJ, Currie G, Denison D, Farrell P, Ross JA, Stephenson R, et al. British Thoracic Society guidelines on respiratory aspects of fitness for diving. Thorax. 2003;58(1):3–13.
Taveira-DaSilva AM, Steagall WK, Rabel A, Hathaway O, Harari S, Cassandro R, et al. Reversible airflow obstruction in lymphangioleiomyomatosis. Chest. 2009;136(6):1596–603.
Tazi A, De Margerie C, Naccache JM, Fry S, Dominique S, Jouneau S, et al. The natural history of adult pulmonary Langerhans cell histiocytosis: a prospective multicentre study. Orphanet J Rare Dis. 2015;10(1):30.
Bissler JJ, McCormack FX, Young LR, Elwing JM, Chuck G, Leonard JM, et al. Sirolimus for angiomyolipoma in tuberous sclerosis complex or lymphangioleiomyomatosis. N Engl J Med. 2008;358(2):140–51.
Bissler JJ, Kingswood JC, Radzikowska E, Zonnenberg BA, Frost M, Belousova E, et al. Everolimus for angiomyolipoma associated with tuberous sclerosis complex or sporadic lymphangioleiomyomatosis (EXIST-2): a multicentre, randomised, double-blind, placebo-controlled trial. Lancet. 2013;381(9869):817–24.
Grobost V, Khouatra C, Lazor R, Cordier J-F, Cottin V. Effectiveness of cladribine therapy in patients with pulmonary Langerhans cell histiocytosis. Orphanet J Rare Dis. 2014;9(1):191.
Epaud R, Le Pointe HD, Fasola S, Ploussard S, Delestrain C, Sileo C, et al. Cladribine improves lung cysts and pulmonary function in a child with histiocytosis. Eur Respir J. 2015;45(3):831–3.
Lorillon G, Bergeron A, Detourmignies L, Jouneau S, Wallaert B, Frija J, et al. Cladribine is effective against cystic pulmonary Langerhans cell histiocytosis. Am J Respir Crit Care Med. 2012;186(9):930–2.
Haroche J, Cohen-Aubart F, Emile J-F, Arnaud L, Maksud P, Charlotte F, et al. Dramatic efficacy of vemurafenib in both multisystemic and refractory Erdheim-Chester disease and Langerhans cell histiocytosis harboring the BRAF V600E mutation. Blood. 2013;121(9):1495–500.
Swigris JJ, Berry GJ, Raffin TA, Kuschner WG. Lymphoid interstitial pneumonia: a narrative review. Chest. 2002;122(6):2150–64.
Dufour V, Wislez M, Bergot E, Mayaud C, Cadranel J. Improvement of symptomatic human immunodeficiency virus-related lymphoid interstitial pneumonia in patients receiving highly active antiretroviral therapy. Clin Infect Dis. 2003;36(10):e127–e30.
Palladini G, Merlini G. What is new in diagnosis and management of light chain amyloidosis? Blood. 2016;128(2):159–68.
Trotman-Dickenson B. Congenital lung disease in the adult: guide to the evaluation and management. J Thorac Imaging. 2015;30(1):46–59.
Khawar MU, Yazdani D, Zhu Z, Jandarov R, Dilling DF, Gupta N. Clinical outcomes and survival following lung transplantation in patients with lymphangioleiomyomatosis. J Heart Lung Transplant. 2019;38(9):949–55.
Wajda N, Zhu Z, Jandarov R, Dilling DF, Gupta N. Clinical outcomes and survival following lung transplantation in patients with pulmonary Langerhans cell histiocytosis. Respirology. 2019 Jun;25(6):644–50.
Hirschi S, Colombat M, Kessler R, Reynaud-Gaubert M, Stern M, Chenard MP, et al. Lung transplantation for advanced cystic lung disease due to nonamyloid kappa light chain deposits. Ann Am Thorac Soc. 2014;11(7):1025–31.
Boehler A. Editor lung transplantation for cystic lung diseases: lymphangioleiomyomatosis, histiocytosis x, and sarcoidosis. Semin Respir Crit Care Med. 2001;22(5):509–16.
Benden C, Rea F, Behr J, Corris PA, Reynaud-Gaubert M, Stern M, et al. Lung transplantation for lymphangioleiomyomatosis: the European experience. J Heart Lung Transplant. 2009;28(1):1–7.
Collins J, Hartman MJ, Warner TF, Muller NL, Kazerooni EA, McAdams HP, et al. Frequency and CT findings of recurrent disease after lung transplantation. Radiology. 2001;219(2):503–9.
Fragkioudaki S, Mavragani CP, Moutsopoulos HM. Predicting the risk for lymphoma development in Sjogren syndrome: an easy tool for clinical use. Medicine. 2016;95(25):e3766.
Cottin V, Harari S, Humbert M, Mal H, Dorfmüller P, Jaïs X, et al. Pulmonary hypertension in lymphangioleiomyomatosis: characteristics in 20 patients. Eur Respir J. 2012;40(3):630–40.
Le Pavec J, Lorillon G, Jaïs X, Tcherakian C, Feuillet S, Dorfmüller P, et al. Pulmonary Langerhans cell histiocytosis-associated pulmonary hypertension: clinical characteristics and impact of pulmonary arterial hypertension therapies. Chest. 2012;142(5):1150–7.
Wu X, Xu W, Wang J, Tian X, Tian Z, Xu K. Clinical characteristics in lymphangioleiomyomatosis-related pulmonary hypertension: an observation on 50 patients. Front Med. 2019;13(2):259–66.
Menko FH, Van Steensel MA, Giraud S, Friis-Hansen L, Richard S, Ungari S, et al. Birt-Hogg-Dubé syndrome: diagnosis and management. Lancet Oncol. 2009;10(12):1199–206.
Gupta N, Seyama K, McCormack FX. Pulmonary manifestations of Birt-Hogg-Dubé syndrome. Familial Cancer. 2013;12(3):387–96.
Shiboski CH, Shiboski SC, Seror R, Criswell LA, Labetoulle M, Lietman TM, et al. 2016 American College of Rheumatology/European league against rheumatism classification criteria for primary Sjögren’s syndrome: a consensus and data-driven methodology involving three international patient cohorts. Ann Rheum Dis. 2017;76(1):9–16.
Travis WD, Costabel U, Hansell DM, King TE Jr, Lynch DA, Nicholson AG, et al. An official American Thoracic Society/European Respiratory Society statement: update of the international multidisciplinary classification of the idiopathic interstitial pneumonias. Am J Respir Crit Care Med. 2013;188(6):733–48.
Obaidat B, Yazdani D, Wikenheiser-Brokamp KA, Gupta N. Diffuse cystic lung diseases. Respir Care. 2020;65(1):111–26.
Conflicts of Interest
The authors declare no conflicts of interest.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2021 Springer Nature Switzerland AG
About this chapter

Cite this chapter
Singla, A., Gupta, N. (2021). Approach to the Diagnosis and Management of Diffuse Cystic Lung Diseases. In: Gupta, N., Wikenheiser-Brokamp, K.A., McCormack, F.X. (eds) Diffuse Cystic Lung Diseases. Respiratory Medicine. Humana, Cham. https://doi.org/10.1007/978-3-030-63365-3_18
Download citation
DOI: https://doi.org/10.1007/978-3-030-63365-3_18
Published:
Publisher Name: Humana, Cham
Print ISBN: 978-3-030-63364-6
Online ISBN: 978-3-030-63365-3
eBook Packages: MedicineMedicine (R0)