
Abstract
Patient safety is one of the main goals of any medical act. Among the various organizational and individual factors that lead to positive medical outcomes, the wellbeing of healthcare professionals is one of the most emphasized in the existing literature. We propose that the concept of work recovery might shed some light on the mechanisms that help health professionals overcome stressful job events and multiple constraints that are daily placed upon their work, thus facilitating wellbeing. The benefits of work recovery on various individual, group and organizational level outcomes were discussed and evidenced in reviews and meta-analyses in samples of employees from various organizational contexts. There is, however, no integration of the research conducted on this topic in medical contexts. In order to understand if and/or how work recovery facilitates wellbeing in healthcare professionals, we need to take into consideration the particular strains of their work context and how they affect individuals’ wellbeing and work outcomes, including patient safety, what are the tools they have to overcome these strains and how do they use them. Hence, the aim of the present chapter is to offer an integrative review of the literature that particularly addresses recovery from work in healthcare professionals. We will consider the multilevel antecedents and consequences of work recovery, and focus on its impact on the wellbeing of healthcare professionals within the complex specificities of medical settings. We then draw on existing literature and suggest potential organizational and individual level interventions on work recovery to enhance health professionals’ wellbeing and ultimately, patient safety.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


1 Introduction
Patient safety pertains to more than just the competent medical act in itself. The World Health Organization defines it as “the prevention of errors and adverse effects to patients associated with health care”. Ever since 1999, when the Institute of Medicine (IOM) released the extensively cited “To Err is Human: Building a Safer Health System”, patient safety has been the focus of numerous studies that have tried to explain both the potential impact of errors in health care on patient safety, and potential ways to counteract their damaging effect (Lawati, Dennis, Short, & Abdulhadi, 2018).
As such, existing literature to date comprises of a large number of studies that discussed antecedents to patient safety. Their focus, however, varies. Most concentrate on individual level factors such as burnout and stress levels (Chuang, Tseng, Lin, Lin, & Chen, 2016), fatigue and recovery (Blasche, Bauböck, & Haluza, 2017), or individual judgments on risk assessment (Chipps et al., 2011; Faye et al., 2010). Other studies, look into team level factors like communication (Botti et al., 2009), implicit and explicit coordination (Kolbe et al., 2014), leadership (Clarke, Lerner, & Marella, 2007), collective vigilance (Jeffs, Lingard, Berta, & Baker, 2012). And finally, an important trend in the existing literature is an investigation of organizational level factors such as safety culture (Lawati et al., 2018; Verbakel, Langelaan, Verheij,Wagner, & Zwart, 2016) and management systems, tools and procedures (Harrison et al., 2015). Because of this variety in research directions, there have been calls in more recent studies to better integrate the existing knowledge and offer a framework that could lead to a better understanding of how patient safety can be reached (Welp & Manser, 2016). In their systematic review on teamwork, clinician wellbeing and patient safety, Welp and Manser (2016) argue that there are inconsistencies in the way that these concepts (especially patient safety) are operationalized and measured, and they propose a framework to help integrate the relationships between them. One of their more important arguments is that the relationship between clinician wellbeing and patient safety is in fact reciprocal, and not just one sided from wellbeing to patient safety. They explain that this particular relationship is studied mostly in terms of negative ties between the two, with two major reasoning lines concerning these ties. First, some of the research they reviewed showed that high levels of strain, stress and burnout lead to a number of increased medical errors, which in turn lead to low patient safety outcomes. On the other hand, committing an error (which means low patient safety) leads to increased emotional distress levels for clinicians. Existing evidence supports both lines of reasoning, which suggests one could enter a vicious cycle where lowered wellbeing consistently leads to lower patient safety, which in turn has further damaging effects on wellbeing.
We propose to develop their argument by introducing the concept of recovery from work as a potential process that can break this cycle.
The cognitive, emotional and physical resources one individual can invest in their work are limited and should be replenished daily, after work, by engaging in activities that require a different set of resources (Sonnentag, Venz, & Casper, 2017). When this does not happen, each subsequent workday drains furthermore on the existing resources and requires additional effort from the individual to deal with work tasks. This, in time, leads to stress, chronic fatigue, and burnout (Elfering, Grebner, Semmer, & Gerber, 2002). Work recovery is exactly about replenishing ones’ resources so that the individual is protected from the adverse effects of occupational stress on ones’ wellbeing. Furthermore, recovering from work not only helps individuals by repairing negative strain effects, but can also catalyze the activation of job resources. In a daily diary study that simultaneously examined the relationship between job resources and recovery on the between-person level and the within-person (day) level, Niks, Gevers, de Jonge, and Houtman (2016) found that detachment from work in the evening is positively related to the state of being recovered at the beginning of the working day, and that the state of being recovered is positively related to the level of job resources. Job resources were considered as the aggregated score of cognitive (i.e., the opportunity to determine a variety of task aspects and to use problem-solving skills), emotional (i.e., emotional support from colleagues or supervisors), and physical (i.e., instrumental support from colleagues and supervisors, or ergonomic aids at work) job resources.
The focus of this chapter is to integrate the literature on work recovery in healthcare settings. However, we keep in mind that by doing this we can better understand the role that recovery from work has in the relationship between clinicians’ wellbeing and the outcome of patient safety.
In the last decade, research interest in recovery and unwinding from work demands has shown a substantial increase (Sonnentag & Fritz, 2018). Several reviews and meta-analyses in samples of employees from various organizational contexts discussed and evidenced the benefits of work recovery on various individual, group and organizational-level outcomes (Bennett, Bakker, & Field, 2018; Sonnentag & Fritz, 2018; Steed, Swider, Keem, & Liu, 2019). There is, however, no integration of the research conducted on the topic of recovery from work in medical contexts, although studies have shown that healthcare professionals report longer working hours, less leisure time, shorter amounts of sleep than average working adults (Cranley, Cunningham, & Pandac, 2015) and high levels of burnout (Alexandrova-Karamanova et al., 2016). There is evidence that work-related variables such as these can hinder recovery from work in healthcare professionals (Fritz & Crain, 2016; Poulsen, Poulsen, Khan, Poulsen, & Khan, 2015). As such, healthcare professionals seem to be more prone to job strain and, at the same time, they may experience fewer opportunities to replenish and activate their job resources through work recovery. We believe a systemic, integrated view of recovery from work in medical settings would benefit both research and practice in a few ways. First of all, there have been calls in the literature, to not just focus independently on either antecedents or consequences of a particular construct but to try and bridge them in order to obtain a clearer picture of the mechanisms behind that construct. For example, in a recent discussion on burnout in healthcare Montgomery and his colleagues stress the importance of researching burnout in a systemic manner, where multiple inputs and outputs are considered, and they span over individual, team and organizational levels (Montgomery, Panagopoulou, Esmail, Richards, & Maslach, 2019). Welp and Manser (2016) also suggest integrating fragmented knowledge in such a way that we can explore more than just one-way effects and look into reciprocal effects between constructs. As we have explained before, in their systematic review of teamwork, clinicians’ wellbeing and patient safety they link team level processes (teamwork processes) with individual level states (wellbeing) and work and organizational outcomes (patient safety). Their framework suggests that there are reciprocal influences between clinicians’ wellbeing and patient safety that are not sufficiently explored. We suggest that recovery from work experiences could help improve wellbeing and hence reduce human errors that negatively impact patient safety. We also argue that work recovery experiences could also help healthcare professionals to overcome instances where their work had a negative impact on patient safety and thus prevent incidents at work from affecting their wellbeing too severely. But to be able to find these linkages we need to understand both antecedents and consequences of work recovery, both the strains of the job and the resources that are available. Finally, we need to have a better understanding of the context where healthcare professional work so that we can identify not just individual level effects, but team level and organizational level effects as well. There is a chain of events here that can only be unfolded when one connects the various pieces of information on work recovery available in the literature. The framework we propose answers these calls by integrating multilevel antecedents and consequences of recovery from work. Another benefit of offering an integrated view of work recovery is that it allows us to identify gaps in the literature that should afford ground for developing the theory on recovery from work. Last, but not least, understanding the complex linkages work recovery has with other individual, team level and organizational processes can help us better inform and pinpoint specific interventions on supporting the development and practice of work recovery experiences that are tailored to the specificities of the medical context.
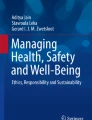
In consequence, the present chapter offers an integrative review of the literature on recovery from work in healthcare professionals by addressing the multilevel antecedents and consequences of work recovery within the complex specificities of medical settings. In developing the model presented in Fig. 11.1, we capitalized on existing frameworks in the field of team effectiveness (e.g., Mathieu, Maynard, Rapp, & Gilson, 2008; Mathieu & Gilson, 2012; Mathieu, Gallagher, Domingo, & Klock, 2019), organizational behavior (e.g., Buchanan & Huczynski, 2017) and the body of research on work recovery highlighting that recovery is influenced by, and influences, both work domain and non–work domain factors (Edwards & Rothbard, 2000; Sonnentag, 2003; Sonnentag & Fritz, 2018). As there are multiple perspectives on work recovery, for the purposes of the present chapter, we consider work recovery only from a process perspective. As such, work recovery refers to leisure activities and non-work experiences that lead to a change in physiological and psychological strain levels (Sonnentag & Fritz, 2018), by facilitating the reduction of strains and replenishment of resources (Sonnentag & Geurts, 2009). Our chapter has a particular focus on work recovery experiences such as psychological detachment, relaxation, mastery experiences, and control.

Work recovery experiences model
1.1 The Construct of Recovery Experiences
Recovery refers to a process in which individual functional systems, that have been called upon during a stressful experience, return to their pre-stressor levels (Meijman & Mulder, 1998). The recovery process can be seen as opposite to strain. It results in the restoration of impaired mood and action prerequisites, and is often also reflected in a decrease in physiological strain indicators. This definition emphasizes two aspects of the process of recovery from work: the process itself (actions) and the results of this process, the outcome. Work recovery can be conceptualized as both (Sonnentag & Fritz, 2018; Sonnentag et al., 2017; Steed et al., 2019). When considered as an outcome, work recovery refers to reduced physiological and psychological strain levels after a recovery period, a state or feeling resulting from engagement in non-work activities. As a process, work recovery refers to leisure activities and non-work experiences that lead to a change in physiological and psychological strain levels (Sonnentag & Fritz, 2018), by facilitating the reduction of strains and the replenishment of resources (Sonnentag & Geurts, 2009). In this process perspective on work recovery, some research has focused on specific activities (i.e., particular behaviors) including replenishing and demanding activities, while others have focused on the psychological experiences (i.e., perceptions and psychological processes underlying those behaviors). Besides recovery activities themselves (i.e., what people are doing), their associated experiences and meanings (i.e., how are people experiencing what they are doing) are those that matter more in order to get recovered (Sonnentag & Fritz, 2007). However, specific activities people may pursue during leisure time have an influence on recovery experiences (Sonnentag & Fritz, 2018). Furthermore, empirical research revealed that not just the time spent on off-work activities but also the subjective experience of such activities (i.e., the level of happiness or pleasure felt when performing these activities) play a pivotal role in the way they are linked to recovery (Oerlemans, Bakker, & Demerouti, 2014; van Hooff, Geurts, Beckers, & Kompier, 2011).
Literature reveals a wide range of recovery experiences that a person can engage in to get recovered from work in different settings such as micro-breaks (e.g., short breaks that are less than 10 min; Bennett, Gabriel, & Calderwood, 2019), work breaks (Bosch, Sonnentag, & Pinck, 2018), after work hours, weekends and holidays. The recovery that occurs within the work settings is termed internal recovery (Geurts & Sonnentag, 2006). It can be achieved through formal and informal breaks during the workday. The recovery that occurs outside of work refers to external recovery (Geurts & Sonnentag, 2006). It may take place after work, on weekends, or for longer periods such as holidays (Colombo & Cifre, 2012). In these recovery settings, the four primary recovery experiences that were most studied are: (1) psychological detachment, (2) relaxation, (3) mastery experiences, and (4) control (Sonnentag & Fritz, 2007). These recovery experiences can occur across a wide variety of activities (Sonnentag, Unger, & Rothe, 2016). They are positively related, but empirically different (Bennett, Bakker, & Field, 2018), as they regard discernibly different elements of the recovery process.
Psychological detachment implies being away from work-related duties and mental disengagement from work (Sonnentag & Fritz, 2007), which means refraining from work-related activities, thoughts, and emotions (Sonnentag & Fritz, 2018). Out of all the recovery experiences, psychological detachment appears as the most salient and, so far, it has received the most interest in the literature (see Sonnentag & Fritz, 2015 for a review; Wendsche & Lohmann-Haislah, 2017). Relaxation is a state characterized by low mental and physical exertion, an experience that can be obtained both through exercises, such as yoga and meditation, as well through other activities that calm the mind and body, such as reading a book, listening to a concert, watching a movie, taking a walk. Mastery experiences refer to off-job activities that distract from the job by providing challenging experiences and learning opportunities in other domains (e.g. philately, apiculture) or broadening one’s horizon (e.g., traveling to a foreign country) (Sonnentag & Geurts, 2009). These challenging activities offer opportunities for experiencing competence and proficiency (Sonnentag & Fritz, 2007), without overtaxing the person’s capabilities (Sonnentag, Binnewies, & Mojza, 2008). Control involves the degree to which a person can decide which activity to pursue during leisure time, as well as when and how to pursue this activity (Sonnentag & Fritz, 2007). Low control of leisure time can be a source of stress and resource consumption. On the other hand, the experience of control during leisure time may satisfy an individual’s desire for control by increasing self-efficacy and feelings of competence, which in turn promote wellbeing. In addition, control during leisure time gives the individual the opportunity to choose those specific leisure activities that he or she prefers and that may be especially supportive for the recovery process (Sonnentag & Fritz, 2007).
Considering this conceptualization of work recovery, we integrated the literature that particularly addresses this concept in healthcare professionals by identifying its multilevel antecedents and consequences and focusing on its impact on the wellbeing of healthcare professionals. The literature we considered for integration consists of the results of a search conducted in the following electronic databases: PubMed, EBSCO—Academic Search and Business Source, SAGE, PsychINFO—PsychARTICLES, and Web of Science. The keywords we used were the following: work recovery, recovery from work, recovery experiences. To narrow our findings for our intended analysis of work recovery in healthcare settings, all three keywords were paired subsequently with: health care, health care professionals, health care workers. We used the model presented in Fig. 11.1 to integrate the results of our search.
2 Antecedents of Work Recovery
Research has spent considerable effort on identifying the processes that lead to recovery (Sonnentag & Fritz, 2018). This is also true for the literature on recovery in medical settings. Hence, most of the studies we analyzed considered work recovery experiences as an output and less as a predictor for various individual, team and organizational level outcomes and, ultimately, for patient safety. In addition, few studies examined work recovery experiences as intervening variables (i.e., moderator and mediator) in the relationship between inputs from various domains and multiple-level outcomes. In the following section, we briefly present the antecedents of work recovery experiences we found in our literature integration approach.
2.1 Job Specific Antecedents
We only identified a small body of research that examined the influence of various aspects of the job on work recovery experiences. In particular, the relationship between job specific variables and work recovery experiences was highlighted in two studies. In the first one, job specific variables such as shift work, hours worked per week, hours of direct patient care, public versus private work sector, metropolitan versus regional location of main practice, and professional stream were investigated as antecedents of work recovery experiences (Poulsen, Poulsen, Khan, Poulsen, & Khan, 2015). Findings based on multiple regression revealed no relationships between these factors and work recovery experiences. In contrast, another study using rich qualitative and quantitative data found that early career physicians report longer working hours, less leisure time and shorter amounts of sleep than average working adults (Cranley, Cunningham, & Panda, 2015). In addition, other findings of this study indicated that early career physicians do not participate in many resource-replenishing activities while at work, and when out of work, they tend to participate in more passive than active forms of recovery. More than half of the early career physicians surveyed indicated not psychologically detaching from work during their last recovery period and in general from work. Resource-draining activities were identified as requiring much of the early career physicians’ non-work time, further limiting recovery. Although these two studies report contradictory findings on the relation between the number of working hours and recovery experiences, they reflect the existing incipient stage of the research on the relationship between job-related variables and recovery experiences in medical settings compared to other organizational settings.
2.2 Individual Level Antecedents
The individual level antecedents to work recovery experiences examined in the existing literature are various demographic characteristics, self-reported physical and mental health, and work attitudes.
In one cross-sectional study that involved 573 oncology workers, Poulsen, Poulsen, Khan, Poulsen, and Khan (2015) investigated demographic variables (e.g., gender, age, years of experience, post-graduate qualifications, marital status, having children, income, other-career commitments, participating in strenuous exercise), and self-reported physical and mental health variables including psychological distress, burnout, and work engagement. They found that low recovery experiences were associated with an increase in age, having a postgraduate qualification, being married in contrast to being single or never married, and having career commitments, while participating in strenuous exercise was associated with high recovery. They also showed in their research that there was a negative association between recovery experiences and burnout, as well as psychological distress.
The relationship between work attitudes, in particular passion for work, and recovery experiences outside of regular work hours was investigated by Donahue and colleagues (2012). Passion for work was defined in terms of a strong inclination toward a self-defining activity that one likes (or even loves), finds important (or highly values), and in which one invests time and energy. Two types of passion for work were considered in this study: obsessive and harmonious passion. Obsessive passion refers to a controlled internalization of an activity in one’s identity that creates an internal pressure to engage in an activity that the person likes. Harmonious passion refers to an autonomous internalization that leads individuals to choose to engage in an activity that they like (Vallerand et al., 2003). Specifically, data from 118 French-Canadian nurses collected through a prospective design has shown that obsessive passion undermined recovery experiences, while harmonious passion positively predicted recovery experiences.
2.3 Non-work Antecedents
Non-work factors (i.e., non-work life and leisure activities) are related to employees’ work recovery experiences (Sonnentag & Fritz, 2018). In fact, both foundational and more recent works emphasizing work recovery as a process focused on individual engagement in specific non-work activities to determine whether these activities might replenish resources and curtail demands (Steed et al., 2019). In our search, we found few studies conducted on healthcare professionals that considered individual engagement in off-job recovery activities, including work-related off-job activities, low-effort off-job activities, and cultural activities. One study highlighted the importance of work-related off-job activities and low-effort off-job activities for healthcare employees’ detachment from work. In a two-wave panel study of 230 healthcare employees, de Jonge, Shimazu, and Dollard (2018) examined whether particular recovery activities after-work have an effect on recovery from work (i.e., cognitive, emotional, and physical detachment) and sleep quality. Results of the hierarchical multiple regression analyses revealed that work-related off-job activities were negatively associated with a cognitive and emotional detachment in both the short and long run, whereas low-effort off-job activities were positively related to cognitive detachment in the short run. The long-term findings existed beyond the strong effects of baseline detachment.
Similarly, while looking into individual involvement in off-job cultural activities, Tuisku, Virtanen, Bloom, and Kinnunen (2016) found that employees who reported both receptive (i.e., passive consumption of culture) and creative (i.e., active art-making) cultural activities on a weekly basis had the highest relaxation, mastery and control experiences during time after work. In addition, those with weekly creative activities had beneficial mastery experiences.
The antecedents briefly depicted in this section reveal that the focus of the past research on antecedents of work recovery experiences in healthcare professionals was rather on individual level, job specific and non-work domain factors and less so on team, organizational, and contextual factors. Even so, the body of research that investigated the antecedents of work recovery experiences specifically in healthcare professionals is rather small compared to research that included samples of employees from other professions. Moreover, these studies examined the effects of antecedents alone and not of the interaction between factors from work, non-work and individual domains.
These studies only outline a fragmented and incomplete picture of the work, individual and non-work domains we can capitalize on to facilitate work recovery experiences and, subsequently, the growth of healthcare professionals’ wellbeing that will ultimately lead to an increased patient safety. But, of course, this picture can be enhanced, on one side, by using findings from research on work recovery experiences conducted with employees from other professions (e.g., Parker, Sonnentag, Jimmieson, & Newton, 2019; Steed et al., 2019) and, on the other side, by continuing to explore in depth the particularities of work recovery conceptualized either as experiences, activities (e.g., Manomenidis, Panagopoulou, & Montgomery, 2016), and state and its antecedents in healthcare settings.
3 Consequences of Work Recovery
Recovery from work experiences, considered individually and together as aggregated score, have been documented to influence a wide variety of outcomes for employees (Colombo & Cifre, 2012; Ouyang, Cheng, Lam, & Parker, 2019; Sonnentag & Fritz, 2018; Steed et al., 2019; Taylor, Snyder, & Lin, 2019; Wendsche & Lohmann-Haislah, 2017), their teams and organizations (Fritz & Sonnentag, 2005). However, the body of research investigating the benefits and pitfalls of work recovery experiences in healthcare professionals is very small. All the studies that we analyzed have only looked into the individual or employee-related outcomes. None of the studies conducted in medical settings documented the influence of work recovery experiences on team and organizational level outcomes. This situation can also be found in the empirical research on work recovery that involved other professions or organizations from other industries. Thus, in the following paragraphs, we will present the range of the individual level outcomes of work recovery experiences in healthcare professionals.
3.1 Individual Level Consequences
In healthcare professionals, work recovery experiences have been studied only in relation to individual level outcomes including behavioral and wellbeing outcomes. Also, we found one study that conceptually discussed the impact of job engagement and recovery on dentists’ wellbeing (Montasem, 2017).
In terms of behavioral outcomes, work recovery experiences were linked to creative performance. In a day-level study, Niks, de Jonge, Gevers and Houtman (2017) used a within-person design to investigate the role of cognitive and emotional detachment from work during non-work time in relation to equivalent types of job demands and job resources, in the prediction of self-rated employee creativity (e.g., generation of new and useful ideas about work by employees). Survey data were gathered over the course of eight consecutive days from 151 health care employees. Findings from multilevel analyses showed that cognitive detachment was positively related to creativity, irrespective of the level of cognitive job demands and resources, but it did not interact with cognitive demands and/or resources to predict creativity. Furthermore, high emotional job demands in combination with either high levels of emotional job resources or low levels of emotional detachment were positively related to creativity. Thus, these findings indicate that different types of psychological detachment have different effects on producing new (problem solving) ideas about work, sketching the divergent effects of detachment from work, as a recovery experience, on employee creativity.
Work recovery experiences were linked to various aspects of healthcare professionals’ wellbeing, including psychosomatic wellbeing (i.e., fatigue at home, state of being recovered) and mental wellbeing (i.e., affect spillover, negative affect at home, emotional exhaustion at work).
Specifically, in a daily diary study in which 96 health-care workers completed surveys three times a day, over the period of one work-week, Sonnentag and Binnewies (2013) tested if psychological detachment from work during evening hours and sleep quality moderate the spillover of positive and negative affect from work to home and, whether affect spillover persists until the next morning. Findings based on the results of hierarchical linear modeling suggested that detachment can impact on spillover processes. While detachment is beneficial in interrupting the spillover of negative affect, it neutralizes potential gains that could be derived from positive affect experienced at work. Again, these findings reveal the divergent effect of psychological detachment on healthcare workers’ mental wellbeing.
Donahue and colleagues (2012) found that work recovery experiences and rumination mediated the relationship between passion for work and workers’ emotional exhaustion. In turn, recovery experiences protected workers from emotional exhaustion. In another study, Blanco-Donoso, Garrosa, Demerouti and Moreno-Jiménez (2017), using a diary approach and a multilevel design, found that nurses’ daily difficulties in emotion regulation have a direct effect on daily emotional exhaustion at work, and on fatigue and negative affect at home at night. They also found that coworker support, psychological detachment and relaxation minimize the unfavorable effects on the wellbeing of difficulties in emotion regulation. These findings were drawn from multilevel analyses conducted on data provided by 74 nurses from various Spanish hospitals and primary health care centers that completed a general questionnaire and a diary booklet over five consecutive workdays at two different moments, after work and at night (N = 370 observations).
As in the case of the antecedents of work recovery, our integration reveals that the focus of the past research on consequences of work recovery experiences in healthcare professionals was rather on individual level outcomes and not on team and organizational outcomes and patient safety. Previous work generally looks into the consequences of work recovery experiences at one level of analysis, neglecting to study the impact that work recovery experiences might have on other levels of analysis such as teams and organizations or, why not, the cross-levels. Furthermore, the types of the consequences we identified in our search efforts emphasize the lack of connecting in a consistent manner work recovery experiences with different dimensions of various concepts relevant for patient safety, such as wellbeing. In addition, we found no studies investigating the role of political, economic, social, technological, legal, and environmental context on work recovery experiences. Focus on this topic might be useful, as recent studies revealed the existence of cultural variability in the association between age and wellbeing (Lawrie, Eom, Moza, Gavreliuc, & Kim, 2019). Using a multilevel approach with an international database (Study 1, N = 64,228), Lawrie and colleagues (2019) found that older age was associated with lower wellbeing in countries higher in uncertainty avoidance but not in countries lower in uncertainty avoidance. Further, this cultural variation was mediated by a sense of control. When, in a second study (Study 2, N = 1025), they focused on the comparison between a culture with low uncertainty avoidance (the United States) and a culture with high uncertainty avoidance (Romania), they found that age was negatively associated with wellbeing in Romania but not in the United States. This cultural difference was mediated by the use of contrasting coping strategies associated with different levels of a sense of control.
In view of these findings, we believe more research is needed in order to identify how work recovery experiences in healthcare settings, via different mechanisms, can lead to patient safety, as well as how interventions dedicated to increase work recovery experiences should be tailored to facilitate it.
4 Work Recovery Interventions
In this section, we draw on existing literature and suggest potential organizational and individual level interventions on work recovery to ensure the wellbeing of healthcare professionals and ultimately, patient safety.
4.1 Organization Level Interventions
Many work and hospital-specific factors that have an impact on the recovery process are hard to change (Smith, Folkard, Tucker & Evans, 2011). Specifically, a high volume of work, time pressure, or the need for overtime hours are amongst the most common factors that can impair the recovery experiences (Sonnentag & Fritz, 2015). As such, while we would have a hard time trying to build interventions where the aim is to reduce these stressors, we posit that interventions should rather target specific activities to help medical personnel recuperate from working under these conditions. Some of these possible interventions and solutions are straightforward. Micro-breaks during the working day, characterized by social activities (e.g., phoning friends or family members) and relaxation activities (e.g., stretching), but not by cognitive activities, have the potential to reduce the negative effects of work demands such as end-of-workday negative affect (Kim, Park, & Niu, 2017). In addition, the availability of opportunities to relax and recover during the working day is associated with less work–home conflict and indirectly with less emotional exhaustion (Nitzsche et al., 2016). Together, these studies support internal recovery through micro-breaks, daily breaks and ‘switching off during work’. They can be regarded as small steps toward enhancing healthcare professionals’ wellbeing by preventing states of exhaustion and end-of-workday negative affect. Medical practices should consider including micro-breaks and breaks during a working day of a shift. Daily micro-breaks including social, relaxation, and cognitive activities also have the potential to generate positive affect that leads to a greater job performance for workers with lower general work engagement (Kim, Park, & Headrick, 2018). In parallel, it is also important to create free space and time out at weekends in a targeted way. This can contribute to reduce negative affect, improve the work–home interplay, and to prevent exhaustion and potential burnout.
Also, a high volume of work brings about a number of tasks that remain unfinished at the end of the day. A solution is to establish, at the end of the working day, the way in which the tasks will be solved through the most specific objectives. This method helps to reduce associated negative activation, increases control over tasks, and promotes recovery experiences (Smit & Barber, 2015).
Given the fact that organizational stressors are sometimes difficult to change, a strong emphasis must be put on the medical staff’s reactions to stress. In this respect, many cognitive-behavioral programs and relaxation techniques were used in the organizational environment (Richardson & Rothstein, 2008), but recovery experiences were much less used in these programs. In a quasi-experimental study, Hahn et al. (2011) highlighted the benefits of a recovery training program that covered all four recovery experiences in two theoretical and practical sessions. The results of the intervention revealed an increase in mastery experiences, sleep quality and recovery self-efficacy experience. These studies show that recovery experiences can be learned. Furthermore, based on these results, a 1-day workshop intervention conducted on radiation therapists and oncology nurses was developed (Poulsen, Sharpley, Baumann, Henderson & Poulsen 2015). It was found that their intervention had a positive effect on the total recovery experiences and perceived sleep quality, an important component of the recovery process in comparison to the control group.
Sleep, is an important component of the recovery process, and the development of a sleep routine during the daytime and keeping sleep debt to a minimum, is one of the recommendations in guidelines on recovery from the night shifts, for junior doctors. In an intervention to increase work recovery (Hahn et al., 2011), the participants were taught what sleep-hygiene means and rules about sleeping times. After this intervention participants reported a better perceived sleep quality.
The promotion of recovery experiences can start from leaders, primarily through the expectations they have from subordinates. Also, supervisors can discuss with employees about the importance of post-work recovery or draw clear expectations about work-related behaviors (e.g., expectations that employees will respond or not to emails in their spare time). Work-home segmentation expectations are positively associated with psychological detachment after work (Park et al., 2011). More specifically, the perception of work-home segmentation promoted between colleagues or supervisors could influence recovery experiences.
Given the schedule of medical personnel, there are few studies that analyze how many days of recovery it takes to accomplish recovery after work shifts. A study on nurses, suggests that three rest days are necessary to recover after two 12-h day shifts for the full restoration of fatigue and to promote wellbeing (Blasche et al., 2017). When setting up the 12-h work schedule for medical staff, it is important to consider the work-recovery balance, in order to enhance nurses’ wellbeing and patient safety.
In a study conducted with medical practitioners, they were asked to write about three good things that happened during the working day (personal or work-related) and to explain why they think those events took place (Bono et al., 2013). The level of stress and wellbeing was assessed before and after the positive reflection intervention, and results demonstrate that participants experienced reduced stress and reported fewer physical and mental health complaints, in comparison with days when they didn’t reflect on the positive moments occurring during their day. At the organizational level, the focus should not only be on controlling negative events, but also on reinforcing and revealing positive events. According to the study mentioned above, a brief end-of-workday positive reflection can lead to a decrease in stress levels and improve health in the evening. This practice can be used by supervisors at the beginning of a workday, or at the end, in a meeting. For example, the meeting after the night shifts, aside from discussing the negative events that took place, could also celebrate the colleagues’ success or the aspects that went well, and to express gratitude for the effort invested and their engagement in saving people’s lives.
More than that, at the organizational level, the focus can be placed on promoting strengths in the working environment, on positive feedback and encouraging productive behaviors, and not on criticisms brought to medical staff. In addition, Schwartz Centre Rounds® can be used to foster healthcare professionals’ mastery and reflection with regard to the application of human connection patient-caregiver principle in their practice to improve the quality of caregiving. Rounds are organization-wide forums that prompt reflection and evidence-based interdisciplinary discussion of the emotional, social and ethical challenges of health-care work, with the aim of improving staff wellbeing and patient care (Farr & Barker, 2017; Maben et al., 2018). These rounds provide healthcare professionals with the opportunity to come together in a safe but open environment, to explore the human and emotional impact of their everyday work by sharing their expertise, experience, and a passion for what they do. These rounds last 1 h, typically co-facilitated by a senior doctor and psychosocial practitioner with a panel of up to four presenters and an open audience. Each round begins with short presentations by the panel, on a key theme, scenario or patient case, after which the round is opened for general discussion (Reed, Cullen, Gannon, Knight, & Todd, 2015). Recent empirical studies and scoping reviews highlighted the beneficial role of these rounds among other techniques in the process of team-based reflection (Anderson, Sandars, & Kinnair, 2019; Angelopoulou & Panagopoulou, 2019; Maben et al., 2018). They can lead to improved emotional wellbeing and learning for quality improvement and patient safety. Also, a series of socializing events can be organized according to the work schedule, or during work breaks, meant to increase the wellbeing and the positive emotions between the employees.
4.2 Individual Level
While the focus on recovery as an experience aims at better understanding the psychological process underlying recovery from work, a focus on specific recovery activities may provide more focused opportunities for developing interventions. At the individual level, a number of activities have been studied as influencing recovery experiences. Among the activities studied are physical, household activities, such as taking care of children, social activities and also work-related activities. Physical activities have a high ability to distract attention from work problems (Sonnentag, 2001). Social activities also help the recovery process, especially if work-related thoughts are left aside. In a longitudinal study conducted on emergency medical service workers (Fritz & Sonnentag, 2005), social activity during the weekends was negatively associated with the disengagement component of burnout and poor general wellbeing after the weekend. Social activities usually require a lower level of emotional regulation compared to the social interactions at the workplace (Grandey, 2000), helping to restore the invested resources and build new ones. More than that, spending time with others during the weekend was associated with task performance when returning to the workplace.
At the same time, activities that develop new skills, such as various hobbies, have the ability to promote work recovery and also to acquire new resources. In a study that evaluated short and long-term effects of off-job activities on recovery and sleep among healthcare workers (de Jonge, Shimazu, & Dollard, 2018) it has been shown that time spent on high-duty activities like work-related activities has a negative impact on work recovery. On the other hand, activities such as social, creative, physical, and low-effort activities facilitate recovery experiences. Also, cultural activities like going to a concert or performing creative activities like writing or playing an instrument were associated with mastery experiences and control among hospital personnel (Tuisku et al., 2016). These recovery experiences have the potential to create new resources, like feelings of personal accomplishment when acquiring new skills and knowledge, which can then lead to better wellbeing and positive emotions.
Hülsheger, Feinholdt, and Nübold (2015) investigated in a randomized field experiment (with a self-training and a wait-list control group) the effectiveness of a low-dose mindfulness intervention for recovery from work. They also examined the different responses to the treatment in terms of treatment-by-baseline interactions. Recovery from work was conceptualized as psychological detachment, sleep quality, sleep duration, and it was assessed with an event-sampling methodology involving daily measurements over 10 workdays. While growth curve analyses revealed intervention effects on sleep quality and sleep duration, no effects were found for psychological detachment after work. Also, gains in recovery processes, including psychological detachment, due to the intervention were not stronger for participants with low baseline levels.
Poulsen, Sharpley, Baumann, Henderson, and Poulsen (2015) however found, using a sample of 70 oncology care workers, that work recovery experiences can be increased significantly after a one-day educational intervention (workshop) designed to build the recovery-related self-care resources. Workshop participants reported greater mean changes 6 weeks post-workshop for total recovery experiences, self-care satisfaction, and perceived sleep quality. There was a decline in the scores of the control group (that only used written educational materials) over the 6-week period for all measures. Workshop participants not only avoided this decline but also demonstrated increased mean scores, with a significant main effect 6 weeks post-workshop, compared with the control group.
Beyond all of the suggestions offered by literature on setting clear limits on personal and professional life, there are individuals who prefer to dedicate themselves to work even in leisure time. Control over leisure time is an important factor in recovery processes (Sonnentag & Fritz, 2007). An alternative to dropping out of work is to engage in activities that are considered pleasant to reduce the negative effects associated with less pleasant daytime tasks and to orientate cognitive resources to resolve problems at the expense of emotional rumination.
A recent meta-analysis has shown that demands (overload, cognitive, emotional, and physical) were negatively related to work recovery experiences, while resources (contextual-work, contextual-home and personal) were positively related to these experiences (Steed et al., 2019). Thus, interventions dedicated to increase work recovery experiences could target simultaneously reducing the demands of both work and non-work domains and increasing the resources that an employee can access in these domains. These interventions can in particular address recovery that occurs within the work settings through formal and informal breaks during the workday or recovery that takes place after work, on weekends, or for longer periods such as holidays or both.
5 Conclusions
It is time to create an organizational culture that encourages healthcare professionals to keep a balance between taking care of others and taking care of themselves, and their personal wellbeing. Focusing attention on how medical personnel manages to restore their work resources will have an impact on both their wellbeing and patient safety. Contrary to first impressions, in order to reduce the overall stress levels, it is not enough to reduce the stress factors associated with the job, but it also requires to highlight the importance of the medical staff’s free time. Interventions at the individual level should encourage healthcare professionals to take time after work to engage in low demanding, replenishing or creative cultural off-job activities. These habits can be promoted from leaders to team members.
Taking into account that the medical setting has its particularities, more focused research is needed with regard to the role of recovery from work on health professionals’ wellbeing and, subsequently, on patient safety. At the same time, this research should take into account and unpack the various potential individual, team, and organizational factors that can intensify or buffer recovery from work experiences in healthcare professionals. Finally, considering that medical organizations are embedded in the wider society and that they are a critical part of it, it is important to also understand the influence of the political, economic, social, technological, legal and environmental context in intensifying or buffering work recovery experiences.
Key messages for researchers (2–3 points) | Key messages for healthcare delivery (2–3 points) |
|---|---|
Considering the role of context in shaping organizational outcomes and the lack of studies on the role of context in work recovery, it is important to investigate the role of political, economic, social, technological, legal and environmental context in intensifying or buffering work recovery experiences. | Teach healthcare professionals to identify the signs of stress and recovery needs, and how to effectively address these needs by recognizing when engaging in different work recovery experiences is needed and when not (e.g., psychological detachment from work should be encouraged on days with high levels of negative affect, but not on days with high levels of positive affect). |
As there is only a relatively small body of research on recovery experiences of healthcare professionals, in comparison to other domains, it would worth to highlight the particularities of work recovery experiences in healthcare professionals and to further investigate the impact of the individual, team, and organizational factors that can intensify or buffer recovery from work experiences in healthcare professionals. Furthermore, as most of the studies on work recovery experiences in healthcare professionals used cross-sectional and diary studies, it is important to examine longitudinally and from a multilevel perspective how different work recovery experiences are linked to various antecedents from work and non-work domains and consequences, in particular wellbeing and patient safety, and how these variables are reciprocally linked in healthcare settings. | In order to facilitate the occurrence of work recovery experiences during and after work and to achieve the state of feeling and being recovered from work, provide healthcare professionals with: • Opportunities for recovery that takes place during work (e.g., possibility of deciding working hours, the work pace, taking short breaks, deciding when to perform a work task, and having mostly varied work). • Activities to formally and informally share expertise, experience and passion for what they do (e.g., Schwartz Centre rounds®). • Support to engage in replenishing activities during work time (e.g., eating lunch, short time off for relaxation rituals). |
Considering that the same daily activities can be either resource replenishing or resource draining, depending on the contexts in which they are experienced (i.e., work and home; Cranley et al., 2015), it is important to examine when (i.e., during work and after work) and how (i.e., the mechanisms) different work recovery experiences lead to individual, team and organizational positive outcomes and reduce the negative ones in healthcare settings. | Support healthcare professionals: • To take time after work to engage in low demanding, replenishing and creative cultural off-job activities. • To build a positive daily cycle of resource replenishment that runs parallel to resource depletion. • To understand how involving in work recovery experiences can be beneficial for them, their units and organizations, and ultimately for patient safety. |
References
Alexandrova-Karamanova, A., Todorova, I., Montgomery, A., Panagopoulou, E., Costa, P., Baban, A., et al. (2016). Burnout and health behaviors in health professionals from seven European countries. International Archives of Occupational and Environmental Health, 89(7), 1059–1075. https://doi.org/10.1007/s00420-016-1143-5
Anderson, E., Sandars, J., & Kinnair, D. (2019). The nature and benefits of team-based reflection on a patient death by healthcare professionals: A scoping review. Journal of Interprofessional Care, 33(1), 15–25. https://doi.org/10.1080/13561820.2018.1513462
Angelopoulou, P., & Panagopoulou, E. (2019). Non-clinical rounds in hospital settings: A scoping review. Journal of Health Organization and Management, 33(5), 605–616. https://doi.org/10.1108/jhom-09-2018-0244
Bennett, A. A., Bakker, A. B., & Field, J. G. (2018). Recovery from work-related effort: A meta-analysis. Journal of Organizational Behavior, 39, 262–275. https://doi.org/10.1002/job.2217
Bennett, A. A., Gabriel, A. S., & Calderwood, C. (2019). Examining the interplay of micro-break durations and activities for employee recovery: A mixed-methods investigation. Journal of Occupational Health Psychology, 25, 126–142. https://doi.org/10.1037/ocp0000168
Blanco-Donoso, L. M., Garrosa, E., Demerouti, E., & Moreno-Jimenez, B. (2017). Job resources and recovery experiences to face difficulties in emotion regulation at work: A diary study among nurses. International Journal of Stress Management, 24(2), 107–134. https://doi.org/10.1037/str0000023
Blasche, G., Bauböck, V. M., & Haluza, D. (2017). Work-related self-assessed fatigue and recovery among nurses. International Archives of Occupational and Environmental Health, 90(2), 197–205. https://doi.org/10.1007/s00420-016-1187-6
Bono, J. E., Glomb, T. M., Shen, W., Kim, E., & Koch, A. J. (2013). Building positive resources: Effects of positive events and positive reflection on work stress and health. Academy of Management Journal, 56(6), 1601–1627. https://doi.org/10.5465/amj.2011.0272
Bosch, C., Sonnentag, S., & Pinck, A. S. (2018). What makes for a good break? A diary study on recovery experiences during lunch break. Journal of Occupational and Organizational Psychology, 91(1), 134–157. https://doi.org/10.1111/joop.12195
Botti, M., Bucknall, T., Cameron, P., Johnstone, M. J., Redley, B., Evans, S., et al. (2009). Examining communication and team performance during clinical handover in a complex environment: The private sector post-anaesthetic care unit. The Medical Journal of Australia, 190(S11), S157–S160.
Buchanan, D. A., & Huczynski, A. A. (2017). Organizational behavior (9th ed.). Harlow: Pearson Education Limited.
Chipps, E., Wills, C. E., Tanda, R., Patterson, E. S., Elfrink, V., Brodnik, M., et al. (2011). Registered nurses’ judgments of the classification and risk level of patient care errors. Journal of Nursing Care Quality, 26(4), 302–310. https://doi.org/10.1097/NCQ.0b013e31820f4c57
Chuang, C. H., Tseng, P. C., Lin, C. Y., Lin, K. H., & Chen, Y. Y. (2016). Burnout in the intensive care unit professionals: A systematic review. Medicine (Baltimore), 95(50), e5629. https://doi.org/10.1097/md.0000000000005629
Colombo, V., & Cifre, E. (2012). The importance of recovering from work: A review of where, how and why. Papers of the Psychologist, 33(2), 129–137.
Clarke, J. R., Lerner, J. C., & Marella, W. (2007). The role for leaders of health care organizations in patient safety. American Journal of Medical Quality, 22(5), 311–318. https://doi.org/10.1177/1062860607304743
Cranley, N. M., Cunningham, C. L., & Panda, M. (2015). Understanding time use, stress and recovery practices among early career physicians: An exploratory study. Psychology, Health & Medicine, 21, 1–6. https://doi.org/10.1080/13548506.2015.1061675
de Jonge, J. D., Shimazu, A., & Dollard, M. (2018). Short-term and long-term effects of off-job activities on recovery and sleep: A two-wave panel study among health care employees. International Journal of Environmental Research and Public Health, 15(9), 2044. https://doi.org/10.3390/ijerph15092044
Donahue, E. G., Forest, J., Vallerand, R. J., Lemyre, P. N., Crevier-Braud, L., & Bergeron, E. (2012). Passion for work and emotional exhaustion: the mediating role of rumination and recovery. Applied Psychology. Health and Well-Being, 4(3), 341–368. https://doi.org/10.1111/j.1758-0854.2012.01078.x
Edwards, J. R., & Rothbard, N. P. (2000). Mechanisms linking work and family: clarifying the relationship Between work and family constructs. Academy of Management Review, 25(1), 178–199. https://doi.org/10.5465/amr.2000.2791609
Elfering, A., Grebner, S., Semmer, N., & Gerber, H. (2002). Time control, catecholamines and back pain among young nurses. Scandinavian Journal of Work, Environment & Health, 28(6), 386–393. Retrieved October 25, 2020, from http://www.jstor.org/stable/40967229
Farr, M., & Barker, R. (2017). Can staff be supported to deliver compassionate care through implementing Schwartz Rounds in community and mental health services? Qualitative Health Research, 27(11), 1652–1663. https://doi.org/10.1177/1049732317702101
Faye, H., Rivera-Rodriguez, A. J., Karsh, B. T., Hundt, A. S., Baker, C., & Carayon, P. (2010). Involving intensive care unit nurses in a proactive risk assessment of the medication management process. Joint Commission Journal on Quality and Patient Safety, 36(8), 376–384. https://doi.org/10.1016/s1553-7250(10)36056-9
Fritz, C., & Crain, T. (2016). Recovery from work and employee sleep: Understanding the role of experiences and activities outside of work. In J. Barling, C. M. Barnes, E. L. Carleton, & D. T. Wagner (Eds.), Work and sleep: Research insights for the workplace (pp. 55–76). Oxford: Oxford University Press. https://doi.org/10.1093/acprof:oso/9780190217662.003.0004
Fritz, C., & Sonnentag, S. (2005). Recovery, health, and job performance: Effects of weekend experiences. Journal of Occupational Health Psychology, 10(3), 187–199. https://doi.org/10.1037/1076-8998.10.3.187
Geurts, S. A. E., & Sonnentag, S. (2006). Recovery as an explanatory mechanism in the relation between acute stress reactions and chronic health impairment. Scandinavian Journal of Work, Environment and Health, 32(6), 482–492. https://doi.org/10.5271/sjweh.1053
Grandey, A. A. (2000). Emotional regulation in the workplace: A new way to conceptualize emotional labor. Journal of Occupational Health Psychology, 5(1), 95–110. https://doi.org/10.1037/1076-8998.5.1.95
Hahn, V. C., Binnewies, C., Sonnentag, S., & Mojza, E. J. (2011). Learning how to recover from job stress: Effects of a recovery training program on recovery, recovery-related self-efficacy, and wellbeing. Journal of Occupational Health Psychology, 16(2), 202–216. https://doi.org/10.1037/a0022169
Harrison, R., Lawton, R., Perlo, J., Gardner, P., Armitage, G., & Shapiro, J. (2015). Emotion and coping in the aftermath of medical error: A cross-country exploration. Journal of Patient Safety, 11(1), 28–35. https://doi.org/10.1097/PTS.0b013e3182979b6f
Hülsheger, U. R., Feinholdt, A., & Nübold, A. (2015). A low-dose mindfulness intervention and recovery from work: effects on psychological detachment, sleep quality, and sleep duration. Journal of Occupational and Organizational Psychology, 88(3), 464–489. https://doi.org/10.1111/joop.12115
Jeffs, L. P., Lingard, L., Berta, W., & Baker, G. R. (2012). Catching and correcting near misses: The collective vigilance and individual accountability trade-off. Journal of Interprofessional Care, 26(2), 121–126. https://doi.org/10.3109/13561820.2011.642424
Kim, S., Park, Y., & Headrick, L. (2018). Daily micro-breaks and job performance: General work engagement as a cross-level moderator. Journal of Applied Psychology, 103(7), 772–786. https://doi.org/10.1037/apl0000308
Kim, S., Park, Y., & Niu, Q. (2017). Micro-break activities at work to recover from daily work demands. Journal of Organizational Behavior, 38(1), 28–44. https://doi.org/10.1002/job.2109
Kolbe, M., Grote, G., Waller, M. J., Wacker, J., Grande, B., Burtscher, M. J., et al. (2014). Monitoring and talking to the room: Autochthonous coordination patterns in team interaction and performance. Journal of Applied Psychology, 99(6), 1254–1267. https://doi.org/10.1037/a0037877
Lawati, M., Dennis, S., Short, S. D., & Abdulhadi, N. N. (2018). Patient safety and safety culture in primary health care: A systematic review. BMC Family Practice, 19(1), 104. https://doi.org/10.1186/s12875-018-0793-7
Lawrie, S. I., Eom, K., Moza, D., Gavreliuc, A., & Kim, H. S. (2019). Cultural variability in the association between age and wellbeing: The role of uncertainty avoidance. Psychological Science, 31, 51–64. https://doi.org/10.1177/0956797619887348
Maben, J., Taylor, C., Dawson, J., Leamy, M., McCarthy, I., Reynolds, E., et al. (2018). A realist informed mixed methods evaluation of Schwartz center rounds® in England. Health Services and Delivery Research, 6(37), 1–260.
Manomenidis, G., Panagopoulou, E., & Montgomery, A. (2016). The ‘switch on-switch off model’: Strategies used by nurses to mentally prepare and disengage from work. International Journal of Nursing Practice, 22(4), 356–363. https://doi.org/10.1111/ijn.12443
Mathieu, J. E., Gallagher, P. T., Domingo, M. A., & Klock, E. A. (2019). Embracing complexity: reviewing the past decade of team effectiveness research. Annual Review of Organizational Psychology and Organizational Behavior, 6(1), 17–46. https://doi.org/10.1146/annurev-orgpsych-012218-015106
Mathieu, J. E., & Gilson, L. L. (2012). Criteria issues and team effectiveness. In S. W. Kozlowski (Ed.), The Oxford handbook of organizational psychology (Vol. 2, pp. 910–930). New York: Oxford University Press.
Mathieu, J. E., Maynard, M. T., Rapp, T., & Gilson, L. (2008). Team effectiveness 1997-2007: A review of recent advancements and a glimpse into the future. Journal of Management, 34(3), 410–476. doi: 0.1177/0149206308316061.
Meijman, T. F., & Mulder, G. (1998). Psychological aspects of workload. In Handbook of work and organizational: Work psychology (Vol. 2, 2nd ed., pp. 5–33). Hove, England: Psychology Press/Erlbaum (UK) Taylor & Francis.
Montasem, A. (2017). The impact of job engagement and recovery on dentists’ wellbeing. Journal of the Massachusetts Dental Society, 66(1), 14–17.
Montgomery, A., Panagopoulou, E., Esmail, A., Richards, T., & Maslach, C. (2019). Burnout in healthcare: The case for organisational change. BMJ, 366, l4774. https://doi.org/10.1136/bmj.l4774
Niks, I. M. V., de Jonge, J., Gevers, M. P., & Houtman, I. L. D. (2017). Divergent effects of detachment from work: A day-level study on employee creativity. European Journal of Work and Organizational Psychology, 26(2), 183–194. https://doi.org/10.1080/1359432X.2016.1241767
Niks, I. M. V., Gevers, J. M. P., de Jonge, J., & Houtman, I. L. D. (2016). The relation between off-job recovery and job resources: Person-level differences and day-level dynamics. European Journal of Work and Organizational Psychology, 25(2), 226–238. https://doi.org/10.1080/1359432X.2015.1042459
Nitzsche, A., Neumann, M., Groß, S. E., Ansmann, L., Pfaff, H., Baumann, W., et al. (2016). Recovery opportunities, work–home conflict, and emotional exhaustion among hematologists and oncologists in private practice. Psychology, Health & Medicine, 22(4), 462–473. https://doi.org/10.1080/13548506.2016.1237666
Oerlemans, W. G. M., Bakker, A. B., & Demerouti, E. (2014). How feeling happy during off-job activities helps successful recovery from work: A day reconstruction study. Work and Stress, 28(2), 198–216. https://doi.org/10.1080/02678373.2014.901993
Ouyang, K., Cheng, B. H., Lam, W., & Parker, S. K. (2019). Enjoy your evening, be proactive tomorrow: How off-job experiences shape daily proactivity. Journal of Applied Psychology, 104(8), 1003–1019. https://doi.org/10.1037/apl0000391
Park, Y., Fritz, C., & Jex, S. M. (2011). Relationships between work-home segmentation and psychological detachment from work: The role of communication technology use at home. Journal of Occupational Health Psychology, 16(4), 457–467. https://doi.org/10.1037/a0023594
Parker, S. L., Sonnentag, S., Jimmieson, N. L., & Newton, C. J. (2019). Relaxation during the evening and next-morning energy: The role of hassles, uplifts, and heart rate variability during work. Journal of Occupational Health Psychology, 25, 83–98. https://doi.org/10.1037/ocp0000155
Poulsen, M. G., Poulsen, A. A., Khan, A., Poulsen, E. E., & Khan, S. R. (2015). Recovery experience and burnout in cancer workers in Queensland. European Journal of Oncology Nursing, 19(1), 23–28. https://doi.org/10.1016/j.ejon.2014.08.003
Poulsen, A. A., Sharpley, C. F., Baumann, K. C., Henderson, J., & Poulsen, M. G. (2015). Evaluation of the effect of a 1-day interventional workshop on recovery from job stress for radiation therapists and oncology nurses: A randomised trial. Journal of Medical Imaging and Radiation Oncology, 59(4), 491–498. https://doi.org/10.1111/1754-9485.12322
Reed, E., Cullen, A., Gannon, C., Knight, A., & Todd, J. (2015). Use of Schwartz Centre rounds in a UK hospice: Findings from a longitudinal evaluation. Journal of Interprofessional Care, 29(4), 365–366. https://doi.org/10.3109/13561820.2014.983594
Richardson, K. M., & Rothstein, H. R. (2008). Effects of occupational stress management intervention programs: A meta-analysis. Journal of Occupational Health Psychology, 13(1), 69–93. https://doi.org/10.1037/1076-8998.13.1.69
Smith, C. S., Folkard, S., Tucker, P., & Evans, M. S. (2011). Work schedules, health, and safety. In J. C. Quick & L. E. Tetrick (Eds.), Handbook of occupational health psychology (p. 185–204). Washington: American Psychological Association.
Sonnentag, S. (2001). Work, recovery activities, and individual wellbeing: A diary study. Journal of Occupational Health Psychology, 6(3), 196–210. https://doi.org/10.1037/1076-8998.6.3.196
Sonnentag, S. (2003). Recovery, work engagement, and proactive behavior: A new look at the interface between nonwork and work. Journal of Applied Psychology, 88(3), 518–528. https://doi.org/10.1037/0021-9010.88.3.518
Sonnentag, S., & Binnewies, C. (2013). Daily affect spillover from work to home: Detachment from work and sleep as moderators. Journal of Vocational Behavior, 83(2), 198–208. https://doi.org/10.1016/j.jvb.2013.03.008
Sonnentag, S., Binnewies, C., & Mojza, E. J. (2008). “Did you have a nice evening?” A day-level study on recovery experiences, sleep, and affect. Journal of Applied Psychology, 93(3), 674–684. https://doi.org/10.1037/0021-9010.93.3.674
Sonnentag, S., & Fritz, C. (2007). The recovery experience questionnaire: Development and validation of a measure for assessing recuperation and unwinding from work. Journal of Occupational Health Psychology, 12(3), 204–221. https://doi.org/10.1037/1076-8998.12.3.204
Sonnentag, S., & Fritz, C. (2015). Recovery from job stress: The stressor-detachment model as an integrative framework. Journal of Organizational Behavior, 36(S1), S72–S103. https://doi.org/10.1002/job.1924
Sonnentag, S., & Fritz, C. (2018). Recovery from work. In D. S. Ones, N. Anderson, & H. K. Sinangil (Eds.), The SAGE handbook of industrial, work and organizational psychology (Chapter 20) (pp. 471–482). London: SAGE. https://doi.org/10.4135/9781473914964.n21
Sonnentag, S., & Geurts, S. A. E. (2009). Methodological issues in recovery research. In S. Sonnentag, P. Perrewé, & D. Ganster (Eds.), Currents perspectives on job-stress recovery (pp. 1–36). Bingley: Emerald.
Sonnentag, S., Unger, D., & Rothe, E. (2016). Recovery and the work-family interface. In T. D. Allen & L. T. Eby (Eds.), Oxford library of psychology. The Oxford handbook of work and family (p. 95–108). England: Oxford University Press.
Sonnentag, S., Venz, L., & Casper, A. (2017). Advances in recovery research: What have we learned? What should be done next? Journal of Occupational Health Psychology, 22(3), 365–380. https://doi.org/10.1037/ocp0000079
Smit, B. W., & Barber, L. K. (2015) Psychologically detaching despite high workloads: The role of attentional processes. Journal of Occupational Health Psychology. Advance online publication. https://doi.org/10.1037/ocp0000019
Steed, L. B., Swider, B. W., Keem, S., & Liu, J. T. (2019). Leaving work at work: A meta-analysis on employee recovery from work. Journal of Management, XX(X), 1–31. https://doi.org/10.1177/0149206319864153
Taylor, W. D., Snyder, L. A., & Lin, L. (2019). What free time? A daily study of work recovery and wellbeing among working students. Journal of Occupational Health Psychology, XX(X), xxx–xxx. https://doi.org/10.1037/ocp0000160
Tuisku, K., Virtanen, M., De Bloom, J. D., & Kinnunen, U. (2016). Cultural leisure activities, recovery and work engagement among hospital employees. Industrial Health, 54(3), 254–262. https://doi.org/10.2486/indhealth.2015-0124
Vallerand, R. J., Blanchard, C., Mageau, G. A., Koestner, R., Ratelle, C., Léonard, M., et al. (2003). Les Passions de l’Âme: On obsessive and harmonious passion. Journal of Personality and Social Psychology, 85, 756–767. https://doi.org/10.1037/0022-3514.85.4.756
van Hooff, M. L. M., Geurts, S. A. E., Beckers, D. G. J., & Kompier, M. A. J. (2011). Daily recovery from work: The role of activities, effort and pleasure. Work & Stress, 25(1), 55–74. https://doi.org/10.1080/02678373.2011.570941
Verbakel, N. J., Langelaan, M., Verheij, T. J. M., Wagner, C., & Zwart, D. L. M. (2016). Improving patient safety culture in primary care: A systematic review. Journal of Patient Safety, 12(3), 152–158. https://doi.org/10.1097/pts.0000000000000075
Welp, A., & Manser, T. (2016). Integrating teamwork, clinician occupational wellbeing and patient safety–development of a conceptual framework based on a systematic review. BMC Health Services Research, 16, 281. https://doi.org/10.1186/s12913-016-1535-y
Wendsche, J., & Lohmann-Haislah, A. (2017). A meta-analysis on antecedents and outcomes of detachment from work. Frontiers in Psychology, 7, 2072. https://doi.org/10.3389/fpsyg.2016.02072
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2020 Springer Nature Switzerland AG
About this chapter

Cite this chapter
Rus, C.L., Vâjâean, C.C., Oţoiu, C., Băban, A. (2020). Between Taking Care of Others and Yourself: The Role of Work Recovery in Health Professionals. In: Montgomery, A., van der Doef, M., Panagopoulou, E., Leiter, M.P. (eds) Connecting Healthcare Worker Well-Being, Patient Safety and Organisational Change. Aligning Perspectives on Health, Safety and Well-Being. Springer, Cham. https://doi.org/10.1007/978-3-030-60998-6_11
Download citation
DOI: https://doi.org/10.1007/978-3-030-60998-6_11
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-60997-9
Online ISBN: 978-3-030-60998-6
eBook Packages: Behavioral Science and PsychologyBehavioral Science and Psychology (R0)