
Abstract
Purpose
Adequate recovery opportunities are crucial for preventing long-term health effects of acute load reactions in response to stressful work. However, little is known about the time course of recovery from work during non-working days. Thus, the present study assessed recovery from two consecutive 12-hours day shifts during a period of three rest days among nurses.
Methods
In total, 48 nurses (89.6% females) working in three public Austrian nursing homes completed 5-day self-reporting diaries prior to a work phase consisting of two consecutive 12-hours day shifts followed by three consecutive rest days. Therefore, morning and evening fatigue, distress, vigor and sleep were self-assessed by standardized questionnaires. We analyzed the data using multivariate analysis of variance for repeated measures.
Results
Study participants experienced worse well-being and a greater decline in well-being on working days compared to rest days. Well-being increased from rest day 1 to rest day 2 in fatigue, vigor and distress. Rest day 2 to rest day 3 showed a further improvement in fatigue and vigor.
Conclusions
Understanding the concepts of allostatic load, need for recovery and fatigue is essential to develop personalized working schedules. The results suggest that at least three rest days are necessary for full recovery after two consecutive 12-hours day shifts. Thus, adequate time for recovery enables nurses to maintain caring attitudes with patients, thus contributing to patient safety.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
In presently aging societies, the amount of chronic and geriatric patients entering the long-time care system continues to grow (Sander et al. 2015). At the same time, financial resources are constrained, while reimbursement and reputation increasingly depend on measures of patient satisfaction (Martin et al. 2015). Nursing professionals provide quality and safe care customized to patients’ needs and preferences. Thus, nursing is a physically, emotionally and mentally demanding work that potentially leads to fatigue and a decrease in well-being (Chen et al. 2010, 2014a; Josten et al. 2003; Smith-Miller et al. 2014; Steege et al. 2015). Symptoms of burnout including emotional exhaustion, compassion fatigue and reduced personal accomplishment are disproportionately often found in nurses (Bakker et al. 2005). Wróbel (2013) showed a strong correlation between emotional labor, negative mood induction and emotional exhaustion. Additionally, mandatory long work, shift work and night shifts typical for nursing contribute to prolonged fatigue due to impaired recovery from work (Josten et al. 2003; Sheppard 2015; Silva-Costa et al. 2011).
Intensive workload hampers physiological relaxation through elevated adrenaline levels indicating incomplete recovery (Sluiter et al. 2000). Moreover, elevated salivary cortisol levels as an objective measure of job demands predict the cumulative healthcare costs over the following 5-year period (Ganster et al. 2001). Especially long-term work-related strain leads to health complaints due to inadequate restoration (Stimpfel et al. 2012; van Hooff et al. 2005). According to the effort-recovery model, recovery plays a central role in the transition from acute to chronic load reactions. Thus, workers experiencing incomplete recovery have to activate additional performance capacities. In the long run, the resulting accumulation of load effects, also known as “allostatic load,” triggers chronic disease (McEwen 1998). Hence, adequate recovery opportunities are crucial for preventing long-term health effects of acute load reactions in response to stressful working conditions. Understanding the concepts of allostatic load, need for recovery, fatigue and associated symptoms enables nursing facilities to develop best practice settings helping nurses to maintain caring attitudes with patients and contribute to patient satisfaction.
Regulations on work hours usually include a minimum weekly rest period (Totterdell et al. 1995). Twelve-hour shifts are a common staffing solution in hospitals and nursing homes in most countries (Estryn-Behar and Van der Heijden 2012). Nevertheless, evidence suggests impaired fatigue-recovery processes in nurses working a 12-hours shift during the day, potentially resulting in poor quality of care and high nursing turnover rates (Chen et al. 2014b). In the USA, where work shifts of nurses often exceed 12 h, greatly increased rates of serious medical errors and occupational injuries as a consequence of sleep deprivation and fatigue have been reported (Landrigan et al. 2007; Lockley et al. 2007). Increasing concerns regarding quality of patient care provided by fatigued healthcare workers demand empirical research on how effects of long hours of work affect nurses’ health and well-being.
Full recovery requires sufficient time for recovery. However, scientific knowledge on the time course of recovery after demanding work shifts is still poor. So far, only few authors have investigated best modes of recovery from work load of 12-hours shifts in nurses, with the crucial question being the number of days necessary for recovery (Chen et al. 2010, 2014b; Drach-Zahavy and Marzuq 2013; Totterdell et al. 1995). In their longitudinal panel survey among nurses, Drach-Zahavy and Marzuq (2013) found that relaxation and vigor were higher after a short weekend respite compared to two midweek rest days. Also, individual preferences regarding weekend on midweek respites were crucial for experienced recovery, but could possibly interfere with pre-fixed work schedules and staff shortage.
In the light of high workload associated with nursing, we studied recovery from two consecutive 12-hours day shifts during a period of three rest days in a sample of Austrian nurses. The study protocol incorporated the use of a 5-day diary to obtain reliable and valid real-world data about nurses` behavior and well-being (Bolger et al. 2003). In this article, we referred to the two consecutive workings days as W1 and W2 and to the three consecutive rest days as R1, R2 and R3. We assume that the outcome variables will reflect greater recovery on the rest days compared to the working days, indicated by a significant difference between the R2 and W1-2 (hypothesis 1); that the time for recovery will encompass three days, indicated by significant differences between R1 and R2 as well as R2 and R3 (hypothesis 2); and that well-being will deteriorate to a greater extent on working days than on rest days, indicated by a significant difference between the morning to evening differences of W1–2 compared to the morning and evening differences of R2 (hypothesis 3).
Methods
Study design
The current study aimed at examining recovery conceptualized by measures of fatigue, vigor, distress and sleep from two consecutive 12-h day shifts during a period of three rest days in nurses. A 5-day paper and pencil-based diary study assessed morning and evening measures on work and rest days to analyze within-subjects differences. The current study collected data in three public nursing homes in different geographic Austrian regions with predominantly permanent residents (n = 75–109) from September 2011 to December 2013. Informed consent was obtained from all individual participants included in the study. Prior to participation, we informed participants that their involvement in the study was completely voluntary and anonymous and could be discontinued at any time.
Participants
After receiving permission from the administration of the nursing homes, all employed nurses were invited to participate in this study. Exclusion criteria were (1) current consumption of sleeping pills or antidepressants, (2) having been on a vacation within the last three weeks, as these factors are likely to adulterate test results on fatigue, sleep and recovery, and (3) having only two instead of three rest days after two working days (de Bloom et al. 2009). Thus, of the 148 diaries handed out, 103 were returned (response rate of 69.6%). Of these, 48 nurses who had three consecutive rest days were included in the current analysis. The remaining 55 individuals with only two rest days were excluded. We did not find differences between these two groups regarding age, the presence of a partner or dependent children, working hours and night shifts per week (p > 0.25, unpaired t test, data not shown).
Data collection
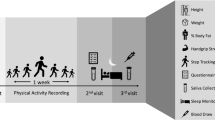
For pilot testing, eight employees from various occupations including nurses analyzed feasibility of the study and comprehension of the study questionnaire. We adapted the questionnaire based on their feedback and remarks. The study questionnaire was comprised of two parts. The first part collected socio-demographic and family characteristics (age, sex, years of education, having a partner/dependent children) as well as work schedule-related data (work hours/week, night shifts/month, leisure-time exercise/week and weeks since the last vacation). The second part was designed as a 5-day diary for scaling present moment well-being both in the morning and in the evening. Participants received this diary prior to a work phase consisting of two consecutive 12-hours day shifts from 7 am to 7 pm (W1–2) followed by three consecutive rest days (R1–3). The day shifts incorporated a 60-min lunch break taken between 11:30 am and 1:30 pm, a 15-min morning at 10 am as well as a 15-min afternoon break at 3 pm. Study subjects were instructed to fill out the diary in the morning when starting work and in the evening when finishing work, thus at 7 am and 7 pm on W1–2 and R1–3. We advised participants to avoid consuming caffeine, alcohol or tobacco directly prior to filling out the study questionnaire. At the end of the study phase, the study participants mailed the diaries directly to the study administrator using stamped self-addressed envelopes, thus establishing anonymity for both participants and nursing homes.
Measures
By measuring various aspects of present moment well-being, the standardized German questionnaire “Eigenzustandsskala” assessed perceived levels of fatigue, distress and vigor (Nitsch 1976). In total, these three variables were assessed with 27 adjectives describing current well-being. Individuals responded to the statement “At the moment I feel …” using six-point Likert scales. Fatigue was assessed with the eight items “rested,” “in need of recovery,” “exhausted,” “recovered,” “spent,” “drowsy,” “tired” and “weary” (scale range 0–40), showing a high internal consistency of Cronbach’s alpha (α) = 0.85. Distress was assessed with the five items “tense,” “unselfconscious,” “calm,” “nervous” and “relaxed,” resulting in an acceptable internal consistency of α = 0.66 (scale range 0–25). Vigor was assessed with the seven items “vigorous,” “zealous,” “energetic,” “persistent,” “able to concentrate,” “active” and “eager to work” (scale range 0–35), showing a high internal consistency of α = 0.92. Sleep was assessed with the standardized German questionnaire “Erholungs–Belastungs–Fragebogen” for evaluating stress and recovery (Kallus 1995). Items relating to last night’s sleep were presented on six-point Likert scales (scale range 0–20). The scale incorporated four items (“I fell asleep peacefully”; “My sleep was restful”; “I woke without an external cause”; “I slept restlessly”) resulting in a high internal consistency of α = 0.88. The quality of sleep was assessed during the morning entry in the diary.
Data analyses
We processed and analyzed the collected data using Excel (Microsoft Corp., Redmond, USA) and SPSS 20 (SPSS Inc., Chicago, IL, USA). We set the two-sided significance level at p < 0.05. The sample size was adequate to detect differences of medium magnitude (effect size d = .45) in same-group comparison with a statistical power of 80% and significance level of p = .05, as calculated by G*Power version 3.1 (University of Kiel, Germany). Thus, the sample size was suitable to detect differences that can be considered relevant. We used multivariate analysis of variance for repeated measures to test the research hypotheses. As for, we defined two repeated measures factors: the first one indicated the day (one of five days, i.e., W1–2 and R1–3), whereas the second one indicated the time of measurement (morning or evening). For the first repeated measures factor, simple contrasts were calculated comparing each day with R2 (i.e., the second rest day) as reference day. We used the second rest day as reference so as to be able to determine day-to-day changes in well-being over the three rest days by comparing rest day 1 with rest day 2 and rest day 2 with rest day 3 as well as to be able to determine whether the rest period statistically significantly differed from the work period. Contrasts were also determined for the second repeated measures factor (time of measurement). The following effects were determined: the effect of day (does the average values of R2 differ from the average value of each of the other days?), the effect of time of measurement (does the morning value differ from the evening value over all days?) and the interaction between day and time of measurement expressed by the interaction term day × time of day (i.e., the difference between morning versus evening vales on R2 different from the difference of morning versus evening values of the other days?). We analyzed the variables fatigue, distress and vigor accordingly. An analysis of variance for repeated measures also assessed the change in quality of sleep using simple contrasts, however, with just one repeated measures factor (days). Again, the reference day was R2. For graphical illustration of the data, we plotted the time course of the outcome variables fatigue, vigor, distress and sleep (means and standard deviations) on morning and evening across work and rest days.
Results
Table 1 presents the socio-demographic characteristics of the study sample. The final study sample consisted of 48 nurses (89.6% women) of three nursing homes. Their mean age was 39.0 years (SD 10.3, range 19–58 years). Four nurses (8%) worked for 20 h/week or less, 16 nurses (33%) for 21–30 h/week and 28 nurses (58%) for 31–40 h/week. Seven nurses had no night shifts (15%), 23 (48%) had one to two night shifts per month and 18 (38%) had three to four night shifts per month. Thirty-four of the study subjects were living with a partner (71%), and nine (19%) had dependent children.
The time course of self-assessed fatigue, vigor, distress and sleep during W1–2 and R1–3 is displayed in Fig. 1. As illustrated, fatigue increased over the working days and decreased during the rest days, the other measures showing corresponding changes. Generally, fatigue was lower and vigor was higher in the morning than in the evening.

Time course of a fatigue, b vigor, c distress (scale range 0–25) and d sleep (scale range 0–20) across work and rest days; means and standard deviations for the morning (dashed line) and evening (solid line) are shown
Table 2 provides effect sizes (partial eta 2) and levels of statistical significance to illustrate the differences between the reference day R2 and the other days regarding the daily average (average of morning and evening values) as well as the daily change (difference between the morning and evening values). A partial eta 2 of ≥.13 represents a medium effect size and is viewed as indicating relevant differences. The average level of perceived fatigue, vigor, distress and sleep during W1–2 differed significantly from that of R2. On working days, study subjects were more fatigued, less vigorous and more distressed and had a lower quality of sleep than on R2. Also, the deterioration of well-being was greater on working days. On W1–2, nurses showed a 34% greater increase in fatigue, a 30% greater decrease in vigor and a 10% greater increase in distress compared to R2.
In regard to the time course of recovery, average fatigue and distress significantly decreased and vigor increased from R1 to R2. However, there was no change in the quality of sleep. Average fatigue and vigor continued to improve from R2 to R3. This continued improvement, however, was not observed in distress and the quality of sleep. As for the relative improvement over the consecutive rest days, fatigue improved 47% on R1, 37% on R2 and 16% on R3, vigor improved 33, 45 and 22% and distress improved 48, 37 and 15%, respectively.
Discussion
The current diary study examined the recovery from two 12-hours day shifts during a period of three consecutive rest days in Austrian nurses based on self-assessed levels of fatigue, vigor, distress and the quality of sleep. In support of our research hypotheses, perceived fatigue was lower and perceived well-being higher on rest days compared to working days and study subjects experienced a greater decline in well-being on working days compared to rest days. The time to recovery was one day for sleep, two days for distress and three days for fatigue and vigor, thus suggesting that three rest days are necessary for the full restoration of fatigue and well-being.
National working time regulations determine the maximum weekly working hours, patterns of work and holidays as well as the daily and weekly rest periods (Totterdell et al. 1995). Nevertheless, chronic understaffing due to shortage of nursing staff could lead to nurses’ working longer shifts or overtime (Stimpfel et al. 2012). Nurses working 12-hours shifts experience physiological strain as shown by elevated cardiac stress levels (Chen et al. 2010). So far, there is little empirical evidence concerning recovery from work and the respective number of days off needed to accomplish recovery from work-related exhaustion. As for nurses, several authors investigated best modes of recovery from and aftereffects of work load (Chen et al. 2010, 2014b; Drach-Zahavy and Marzuq 2013; Totterdell et al. 1995). In this vein, the present study investigated the perceived extent of strain nurses experienced in the mornings and evenings of working days and on the subsequent rest days. Thus, the current study complements preexisting literature in the area of recovery research and the underlying effort-recovery model by providing empirical support for the critical role of recovery in the transition between acute work-related load reactions and chronic ill health (McEwen 1998; van Hooff et al. 2005).
In our study, evening well-being showed the greatest improvement from W2 to R1, morning well-being improved at a faster rate from R1 to R3, as reflected by the significant interaction day × time of day, with the exception of distress. The latter showed no further increase on R2 compared to R1. Thus, we found higher levels of perceived fatigue and distress and lower levels of perceived vigor and quality of sleep on W1–2 compared to R1–3, thus fully supporting hypothesis 1. Also, we found a greater increase in strain over the work day as indicated by an increase in fatigue and distress and a decrease in vigor compared to R1–3, thus fully supporting hypothesis 3. These results are in line with the well-known effects of work, especially demanding work, on well-being, with working days or periods being associated with higher levels of fatigue than with non-working days or periods (Akerstedt et al. 2002; Meijman 1997; Westman and Eden 1997).
In nurses, work encompasses a variety of demands drawing on physical, emotional and mental resources all of which contribute to fatigue. In addition to the type of work, also the duration of work increases levels of fatigue. Though fatigue may not increase linearly over a work day, the risk for accidents is markedly higher after the ninth hour on the job, suggesting an accumulation of fatigue at the end of long work shifts (Folkard and Lombardi 2006). Working two consecutive 12-hours shifts may further increase this accumulation of fatigue on the second work day, as inter-shift recovery time is limited and presumably insufficient for full recovery, according to related research on overtime and long work hours (Blasche et al. 2014; Chen et al. 2014b; Rau and Triemer 2004). From a theoretical perspective, the accumulation of fatigue is due to the need to compensate for fatigue at work by increasing effort to maintain performance, thus increasing physiological stress and contributing to fatigue (Robert and Hockey 1997; Wright et al. 2013).
Further, the present study showed that working days were associated with worse well-being and a greater decline in well-being compared to the rest days and that well-being increased over all three rest days in fatigue and vigor, but not in distress and sleep. These findings thus fully support hypotheses 1 and 2 and partly support hypothesis 3, suggesting that recovery after two consecutive 12-hours shifts required at least three free days for complete recovery to occur. As irregular work hours accumulate fatigue, the literature suggests that one day of recovery is insufficient, two days are usually sufficient, whereas three to four days are necessary after periods of severely disturbed circadian rhythmicity (Åkerstedt et al. 2000; van Hooff et al. 2005). Thus, our findings support less recent investigations by Totterdell et al., stating higher levels of social satisfaction, cheerfulness, calmness and alertness on workdays preceded by two compared to one rest day (Totterdell et al. 1995). Also, these authors suggested that perceived workload increased over consecutive shifts due to the inherent adaptive costs of fatigue.
Our observation that perceived distress did not improve from R2 to R3 might root in the anticipation of the next work day reflected in an increase in distress in the evening of R3. However, in a previous study, distress recovered faster than fatigue or vigor (Blasche et al. 2016b). This faster recovery of distress may reflect the increasing mental detachment from work which is a precondition for successful recovery from work (Sonnentag and Fritz 2015). Thus, one would expect distress to recover prior to fatigue. Similarly, the quality of sleep improved faster than fatigue.
Getting enough quality sleep at the right time is critical in promoting health and well-being. Conversely, sleep disturbance increases the risk of infectious disease, cardiovascular disease and cancer as well as the incidence of depression (Irwin 2015; Prather et al. 2015; Virtanen et al. 2009). As long working hours disturb the circadian rhythm, nurses might accumulate a significant sleep debt while working successive 12-hours shifts with associated fatigue and sleepiness (Geiger-Brown et al. 2012; Virtanen et al. 2009). Akerstedt et al. (2002) reported that the extent of work stress and workload deteriorate sleep quality and related fatigue with highest levels during the first rest day, not the last work day in employees. In our study, we did not find changes in the quality of sleep from R1 to R2 as well as R2 to R3. Assuming the presence of a healthy worker effect in nurses, explanations for this observation could additionally include that the current diary study evaluated the time course of recovery during a regular, work schedule-based employment, thus reflecting routine recovery in the context of work–life balance (Burdelak et al. 2012). Additionally, individual leisure-time behaviors such as exercise and social interactions mediate maladaptive fatigue symptomology and significantly enhance sleep quality and recovery between work periods (Winwood et al. 2007). However, it is also conceivable that the chosen sleep measure was not adequately sensitive to change.
Physically demanding patient care tasks and mentally fatiguing demands such as organization, management and logistics tasks are the most frequently mentioned fatiguing work demands among nurses (Steege et al. 2015). Controversially, job satisfaction predicts vigor and dedication (Jenaro et al. 2011). Thus, the design of work schedules contributes substantially to the health and well-being of nurses (Peters et al. 2016). However, nurses have been shown to prefer 12-hours shift over shorter shifts to reduce their work/family conflicts, irrespective of the patient’s safety and their own health (Estryn-Behar and Van der Heijden 2012; Josten et al. 2003).
As energy expenditure accumulates during 12-hours shifts, nurses experience physiological strain as shown by elevated cardiac stress levels (Chen et al. 2010, 2014b). To reduce allostatic load, two rest days or a typical two-day weekend might be insufficient to ensure a full fatigue-recovery process (Åkerstedt et al. 2000; McEwen 1998). This is especially obvious when considering the high workload and long working hours experienced in nursing professions. In line with the literature, our results suggest revisiting traditional work schedules in nursing homes and develop additional solutions to the issue of nurse fatigue (Estryn-Behar and Van der Heijden 2012; Landrigan et al. 2007; Lockley et al. 2007; Martin 2015). As such, personalized work schedules ensuring sufficient rest breaks and leisure opportunities should stipulate adequate weekly rest periods of at least two, but preferably three rest days (Blasche et al. 2016a; Haluza and Blasche 2016). Recommendations for organizations could include to increase the number of registered nurses, define a minimum nurse-to-patient ratio and provide tailored continuous education programs (Park and Han 2010). Based on their findings on prevalent acute and chronic fatigue, Chen et al. (2014b) suggested establishing fatigue intervention programs for nurses working 12-hours shifts in hospitals. When implementing 12-hours shifts, hospital administration, unit managers and nurses need to collaborate for achieving an adequate fatigue-recovery balance. Also, changing shifts with short notice and lack of time for shift handover should be reduced. Moreover, Gangster et al. argue to encourage control-enhancing job design interventions for sustained stress reduction in nurses experiencing high workload demands (Ganster et al. 2001).
Study limitations
The results of the present study should be viewed with caution due to limitations inherent in the study design. Diary studies have been shown to serve as useful research tools to assess recovery activities and individual well-being (Sonnentag 2000). However, self-reported data could introduce reporting bias. Also, self-assessment reflected perceived levels of the main outcome variables fatigue and recovery, no objective measures. In the present study, we did not evaluate whether the employees had an additional occupation. In Austria, unlike to other countries, e.g., the USA, having more than one job is very unusual in general and especially for women. Thus, we assumed that all the non-working time could be considered as rest time free of work. Nevertheless, this potentially undermines our assumption that the three rest days following the double shift were indeed non-working time. Future study on recovery could provide further insight into activities pursued by the employees on their free days. We were not able to account for potential effects of gender (hormonal status, menstrual cycle, etc.) on the study results, as only a limited number of male nurses participated in the study. Noteworthy, the male/female ratio reflected the actual gender distribution with nurses being predominantly females. As no information was available on characteristics of non-respondents, we could not discuss the influence of their absence quantitatively. However, the high response rate and the absence of differences between nurses with two versus three days off indicate that the results of the present study can be generalized. To achieve regional stratification, we used data derived from three nursing homes in different geographic regions, similar to other publications (Chen et al. 2014b). We only studied recovery in Austrian nurses working in nursing homes which limits generalization to other nursing professions.
The sample size of the present study was adequate to detect changes in medium, but not of small magnitude between longitudinal measurements. Therefore, the results of our study regarding the time necessary for full recovery can be viewed as conservative, though relevant changes were detected. It is likely that a replication of the study with a larger sample size would result in the detection of significant differences in more variables. We did not modify the existing work schedule of the nurses, so the respite period was situated either midweek or on weekends. However, there is evidence that weekends might provide a greater potential for recovery compared to weekdays, potentially due to favorable leisure experiences (Drach-Zahavy and Marzuq 2013).
Conclusion
This study provides new insights into the course of recovery after two consecutive 12-hours day shifts in nurses. The results suggest that at least three rest days are necessary for full recovery. In a physically and psychologically demanding occupation like nursing, where performance is critical, employees’ health and well-being should not be unnecessarily affected by lack of recovery and sleep deprivation. In view of these results, we would advise decisions makers and nursing home administrations to alleviate allostatic load in nurses. This could be facilitated by providing an adequate number of rest days and avoiding extended shifts for nurses.
References
Akerstedt T, Fredlund P, Gillberg M, Jansson B (2002) Work load and work hours in relation to disturbed sleep and fatigue in a large representative sample. J Psychosom Res 53(1):585–588
Åkerstedt T, Kecklund G, Gillberg M, Lowden A, Axelsson J (2000) Sleepiness and days of recovery. Transp Res Part F: Traffic Psychol Behav 3(4):251–261. doi:10.1016/S1369-8478(01)00009-2
Bakker AB, Le Blanc PM, Schaufeli WB (2005) Burnout contagion among intensive care nurses. J Adv Nurs 51(3):276–287. doi:10.1111/j.1365-2648.2005.03494.x
Blasche G, Arlinghaus A, Dorner TE (2014) Leisure opportunities and fatigue in employees: a large cross-sectional study. Leis Sci 36(3):235–250. doi:10.1080/01490400.2014.886981
Blasche G, Pasalic S, Baubock VM, Haluza D, Schoberberger R (2016a) Effects of rest-break intention on rest-break frequency and work-related fatigue. Hum Factors. doi:10.1177/0018720816671605
Blasche G, Zilic J, Frischenschlager O (2016b) Task-related increases in fatigue predict recovery time after academic stress. J Occup Health 58(1):89–95
Bolger N, Davis A, Rafaeli E (2003) Diary methods: capturing life as it is lived. Annu Rev Psychol 54:579–616
Burdelak W, Bukowska A, Krysicka J, Peplonska B (2012) Night work and health status of nurses and midwives. cross-sectional study. Med Pr 63(5):517–529
Chen J, Davis LS, Davis KG, Pan W, Daraiseh NM (2010) Physiological and behavioural response patterns at work among hospital nurses. J Nurs Manag 19(1):57–68. doi:10.1111/j.1365-2834.2010.01210.x
Chen J, Daraiseh NM, Davis KG, Pan W (2014a) Sources of work-related acute fatigue in United States hospital nurses. Nurs Health Sci 16(1):19–25. doi:10.1111/nhs.12104
Chen J, Davis KG, Daraiseh NM, Pan W, Davis LS (2014b) Fatigue and recovery in 12-hour dayshift hospital nurses. J Nurs Manag 22(5):593–603. doi:10.1111/jonm.12062
de Bloom J, Kompier M, Geurts S, de Weerth C, Taris T, Sonnentag S (2009) Do we recover from vacation? Meta-analysis of vacation effects on health and well-being. J Occup Health 51(1):13–25
Drach-Zahavy A, Marzuq N (2013) The weekend matters: exploring when and how nurses best recover from work stress. J Adv Nurs 69(3):578–589. doi:10.1111/j.1365-2648.2012.06033.x
Estryn-Behar M, Van der Heijden BI (2012) Effects of extended work shifts on employee fatigue, health, satisfaction, work/family balance, and patient safety. Work 1:4283–4290
Folkard S, Lombardi DA (2006) Modeling the impact of the components of long work hours on injuries and “accidents”. Am J Ind Med 49(11):953–963
Ganster DC, Fox ML, Dwyer DJ (2001) Explaining employees’ health care costs: a prospective examination of stressful job demands, personal control, and physiological reactivity. J Appl Psychol 86(5):954–964. doi:10.1037/0021-9010.86.5.954
Geiger-Brown J, Rogers VE, Trinkoff AM, Kane RL, Bausell RB, Scharf SM (2012) Sleep, Sleepiness, Fatigue, and Performance of 12-Hour-Shift Nurses. Chronobiol Int 29(2):211–219. doi:10.3109/07420528.2011.645752
Haluza D, Blasche G (2016) Fatigue and insufficient leisure opportunities in older employees. J Occup Environ Med 58(7):0000000000000794
Irwin MR (2015) Why sleep is important for health: a psychoneuroimmunology perspective. Annu Rev Psychol 66:143–172
Jenaro C, Flores N, Orgaz MB, Cruz M (2011) Vigour and dedication in nursing professionals: towards a better understanding of work engagement. J Adv Nurs 67(4):865–875. doi:10.1111/j.1365-2648.2010.05526.x
Josten EJC, Ng-A-Tham JEE, Thierry H (2003) The effects of extended workdays on fatigue, health, performance and satisfaction in nursing. J Adv Nurs 44(6):643–652
Kallus KW (1995) Erholungs–Belastungs–Fragebogen (EBF) [Recovery Stress Questionnaire (RESTQ)]. Swets, Frankfurt
Landrigan CP, Czeisler CA, Barger LK, Ayas NT, Rothschild JM, Lockley SW (2007) Effective implementation of work-hour limits and systemic improvements. Jt Comm J Qual Patient Saf 33(11 Suppl):19–29
Lockley SW, Barger LK, Ayas NT, Rothschild JM, Czeisler CA, Landrigan CP (2007) Effects of health care provider work hours and sleep deprivation on safety and performance. Jt Comm J Qual Patient Saf 33(11 Suppl):7–18
Martin DM (2015) Nurse fatigue and shift length: a pilot study. Nurs Econ 33(2):81–87
Martin LC, Arenas-Montoya NM, Barnett TO (2015) Impact of nurse certification rates on patient satisfaction and outcomes: a literature review. J Contin Educ Nurs 46(12):549–554
McEwen BS (1998) Stress, adaptation, and disease—allostasis and allostatic load. Ann NY Acad Sci 840:33–44. doi:10.1111/j.1749-6632.1998.tb09546.x
Meijman TF (1997) Mental fatigue and the efficiency of information processing in relation to work times. Int J Ind Ergonom 20(1):31–38. doi:10.1016/S0169-8141(96)00029-7
Nitsch J (1976) Die Eigenzustandsskala (EZ-Skalal)-Ein Verfahren zur hierarchisch-mehrdimensionalen Befindlichkeitsskalierung. In: Nitsch JR, Udris I (eds) Beanspruchung im Sport. Limpert, Bad Hombug v.d.H., pp 81–102
Park YH, Han HR (2010) Nurses’ perceptions and experiences at daycare for elderly with stroke. J Nurs Scholarsh 42(3):262–269
Peters V, de Rijk A, Engels J, Heerkens Y, Nijhuis F (2016) A new typology of work schedules: evidence from a cross-sectional study among nurses working in residential elder care. Work 7:7
Prather AA, Janicki-Deverts D, Hall MH, Cohen S (2015) Behaviorally assessed sleep and susceptibility to the common cold. Sleep 38(9):1353–1359
Rau R, Triemer A (2004) Overtime in relation to blood pressure and mood during work, leisure, and night time. Soc Indic Res 67(1–2):51–73
Robert G, Hockey J (1997) Compensatory control in the regulation of human performance under stress and high workload: a cognitive-energetical framework. Biol Psychol 45(1):73–93
Sander M et al (2015) The challenges of human population ageing. Age Ageing 44(2):185–187. doi:10.1093/ageing/afu189
Sheppard K (2015) Compassion fatigue among registered nurses: connecting theory and research. Appl Nurs Res 28(1):57–59. doi:10.1016/j.apnr.2014.10.007
Silva-Costa A, Rotenberg L, Griep RH, Fischer FM (2011) Relationship between sleeping on the night shift and recovery from work among nursing worker—the influence of domestic work. J Adv Nurs 67(5):972–981. doi:10.1111/j.1365-2648.2010.05552.x
Sluiter JK, Frings-Dresen MHW, Meijman TF, van der Beek AJ (2000) Reactivity and recovery from different types of work measured by catecholamines and cortisol: a systematic literature overview. Occup Environ Med 57(5):298–315. doi:10.1136/Oem.57.5.298
Smith-Miller CA, Shaw-Kokot J, Curro B, Jones CB (2014) An integrative review: fatigue among nurses in acute care settings. J Nurs Adm 44(9):487–494. doi:10.1097/nna.0000000000000104
Sonnentag S (2000) Work, recovery activities, and individual well-being: a diary study. Int J Psychol 35(3–4):399–399
Sonnentag S, Fritz C (2015) Recovery from job stress: the stressor-detachment model as an integrative framework. J Organ Behav 36:S72–S103. doi:10.1002/job.1924
Steege LM, Drake DA, Olivas M, Mazza G (2015) Evaluation of physically and mentally fatiguing tasks and sources of fatigue as reported by registered nurses. J Nurs Manag 23(2):179–189. doi:10.1111/jonm.12112
Stimpfel AW, Sloane DM, Aiken LH (2012) The longer the shifts for hospital nurses, the higher the levels of burnout and patient dissatisfaction. Health Aff 31(11):2501–2509
Totterdell P, Spelten E, Smith L, Barton J, Folkard S (1995) Recovery from work shifts: how long does it take? J Appl Psychol 80(1):43–57
van Hooff ML et al (2005) Disentangling the causal relationships between work-home interference and employee health. Scand J Work Env Hea 31(1):15–29
Virtanen M et al (2009) Long working hours and sleep disturbances: the Whitehall II prospective cohort study. Sleep 32(6):737–745
Westman M, Eden D (1997) Effects of a respite from work on burnout: vacation relief and fade-out. J Appl Psychol 82(4):516
Winwood PC, Bakker AB, Winefield AH (2007) An investigation of the role of non-work-time behavior in buffering the effects of work strain. J Occup Environ Med 49(8):862–871. doi:10.1097/JOM.0b013e318124a8dc
Wright RA, Patrick BM, Thomas C, Barreto P (2013) When fatigue promotes striving: confirmation that success importance moderates resource depletion influence on effort-related cardiovascular response. Biol Psychol 93(2):316–324
Wróbel M (2013) Can empathy lead to emotional exhaustion in teachers? the mediating role of emotional labor. Int J Occup Med Environ Health 26(4):581–592. doi:10.2478/s13382-013-0123-1
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
All procedures performed in this study were in accordance with the ethical standards of the institutional and national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Rights and permissions
About this article

Cite this article
Blasche, G., Bauböck, VM. & Haluza, D. Work-related self-assessed fatigue and recovery among nurses. Int Arch Occup Environ Health 90, 197–205 (2017). https://doi.org/10.1007/s00420-016-1187-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00420-016-1187-6