
Abstract
Total gastrectomy is a surgery with significant perioperative morbidity and mortality, being considered the treatment of choice in proximal gastric cancer.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others



Keywords
- Gastric cancer
- 95% gastrectomy
- Total gastrectomy
- Manual anastomosis
- Esophagojejunostomy
- Gastrojejunostomy
- Thoracoscopic esophagojejunostomy
40.1 Introduction
Total gastrectomy is a surgery with significant perioperative morbidity and mortality, being considered the treatment of choice in proximal gastric cancer. First described in 1980, our group reported and standardized totally laparoscopic 95% gastrectomy in 2014 [1, 2]. This technique aims to reduce the complications of total gastrectomy while maintaining oncological radicality. In these patients, a standard hand-sewn anastomosis was performed.
A prospective observational study was carried out in 67 patients with laparoscopic 95% gastrectomy between 2014 and 2017. The main objective has been to detect complications (Clavien Dindo > IIIa), focusing on anastomotic leaks. The secondary objective was to assess the quality of oncological surgery.
Sixty-seven consecutive patients were included, in whom 95% totally laparoscopic gastrectomy was performed. There was no case of anastomotic leak. Two patients (2.98%) had one or more Clavien Dindo complications equal to or greater than IIIa. The total hospital stay was six (3–13) days. R0 radical resection was performed in all patients.
95% gastrectomy allows selected patients to meet the oncological standards of resection in proximal gastric cancer in a reproducible and safe manner, reducing perioperative risks such as anastomotic leakage.
Sometimes, in high localized cancers, a standard total gastrectomy should be performed with proximal resection at the distal esophagus. Moreover, in patients with Siewert II, a distal esophagectomy should be added to be radical, and this implies to perform an esophagojejunal anastomosis, transhiatal or by thoracoscopy in prone using a long jejunal loop.
Furthermore, Robot-assisted gastrectomy is being used increasingly in daily practice [3, 4]. After a near total, and total gastrectomy, anastomosis can be performed as described above.
40.2 Description of the Operative Technique (See Videos 40.1–40.4)
We described the same type of anastomosis in four different types of interventions:
-
1.
Laparoscopic end-to-side Roux-en-Y Gastrojejunostomy after 95% Gastrectomy
-
2.
Laparoscopic side-to-side Roux-en-Y Esophagojejunostomy after Total Gastrectomy
-
3.
Laparoscopic or Robotic end-to-side Roux-en-Y Esophagojejunostomyafter Total Gastrectomy
-
4.
Right Thoracoscopic end-to-sideesophagojejunostomy in Prone Position
The key steps to perform a hand-sewn end-to-side Roux-en-Y gastrojejunostomy reconstruction after laparoscopic 95% gastrectomy are
-
1.
Patient position, surgical team, and trocars have been placed in the upper abdomen (Fig. 40.1)
Fig. 40.1 
Patient, surgical team, and trocar placement (1–10 mm: 0° telescope, 2–10 mm: stapler, 5 mm: sealer, clips, etc.). Abbreviations: S1: First surgeon, S2: Second surgeon, S3: nurse
-
2.
After inspection of the abdominal cavity and local inspection, dissection of the stomach is performed according to the oncological rules (dissection and extension of the lymphadenectomy according to Japanese Gastric Cancer Society)
-
3.
With enough radical margin (at least 5 cm), the proximal stomach is divided by means of staplers, leaving a small pouch of 5% (Fig. 40.2a–c)
Fig. 40.2 
95% gastrectomy by staplers (a, b). Schematic view of the resection (c)
-
4.
After resection, retrocolic jejunal loop is ascended into the rest stomach (Fig. 40.3a)
Fig. 40.3 
Posterior outer layer by continuous suturing with V-Loc™ (a, b, c, d)
Fig. 40.4 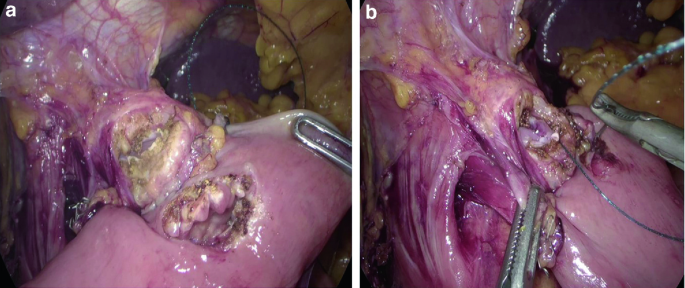
Stomach and jejunum are open by diathermia and a stitch od V Loc® set in the far corner (a, b)
Fig. 40.5 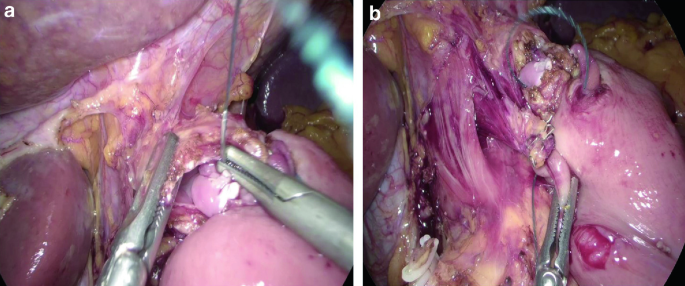
The inner posterior layer is done (a, b)
-
5.
A V-Loc™ 3.0 wound closure device is used to aproximate the seromuscular layer of the jejunum to the rest stomach through and through the stapler line (outer posterior layer) (Fig. 40.3b–d)
-
6.
Another V-Loc is passed through the corner and placed there for traction.
-
7.
The stomach and the jejunal loop are opened by diathermia (Fig. 40.4a, b)
-
8.
With the last V-Loc™ placed in the corner, the inner posterior layer is sutured in a continuos fashion (Fig. 40.5a, b)
-
9.
The anterior layer is now sutured in a continuous fashion by means of a V-Loc™ (Fig. 40.6a–e)
Fig. 40.6 
The anterior layer is sutured (a, b, c, d). Schematic view of the anastomosis (e)
Fig. 40.7 
The jejunal loop is divided by stapler (a, b)
Fig. 40.8 
Jejunojejunal anastomosis and closure of the defect (a, b)
-
10.
The jejunal loop is divided by means of staplers (Fig. 40.7a, b)
-
11.
Jejunojejunal side-to-side anastomosis is now performed by linear stapler (Fig. 40.8a, b)








In the rest of the four procedures mentioned above, the procedures are different but the hand-sewn anastomosis is performed in the same way as previously described.
Some details about the different procedures are given below:
-
1.
In total gastrectomy, position of patient, surgical team, and trocar placement are done in the same way as in the 95% gastrectomy. Laparoscopic end-to-side Roux en Y esophago-jejunostomy (Figs. 40.1, 40.9a–c, 40.10 and 40.11a–c).
Fig. 40.9 
After total gastrectomy. Esophagojejunostomy anastomosis. Outer post layer (a, b, c)
Fig. 40.10 
Esophagus and jejunum are open
Fig. 40.11 
Anterior layer with continuous suturing is performed (a, b, c)
-
2.
In a Robotic-assisted 95% or total gastrectomy, position of the patient, surgical team, and trocar placement are given in Fig. 40.12. Anastomosis is performed in the same hand-sewn fashion as described above.
Fig. 40.12 
Position of the patient, surgical team, and trocar placement for Robotic-Assisted Gastrectomy (A: bipolar robotic grasper and robotic 4 or 6 cm stapler, B: 30° robotic optique, C: monopolar scissors and robotic 4 or 6 cm stapler, and D: Cadiere grasper). Distance between robotic trocars: 8 cm, and between optique and target: 20 cm. Abbreviations: RAS: robotic assistant surgeon
-
3.
In the specific patients with a Siewert II, the total gastrectomy should be extended to the distal esophagus in order to get an R0resection.




There are two possibilities to perform the anastomosis:
-
1.
Transhiatal anastomosis using the linearstapler followed by closure of the defect with barbed V-Loc™ suture, (Fig. 40.13a–i)
Fig. 40.13 
Mediastinal esophagojejunal anastomosis by means of linear stapler (a, b, c, d, e, f, g, h, i)
-
2.
After completion of the resection, if the anastomosis can not be performedtechnicallytranshiatally, esophagus is stapled and jejunal loop is introduced through the hiatus into mediastinum and there fixed. Patient is placed in prone position for thoracoscopy. Placement of trocars are given in Fig. 40.14. The jejunal loop is anastomosed to the esophagus in the same fashion as described above (Figs. 40.15, 40.16a, b, 40.17a, b, 40.18 and 40.19).
Fig. 40.14 
Thoracoscopy in prone position. Trocar placement. Abbreviations: S1: First surgeon, S2: assistant, A: sealer, clips, needle holder, B: 30° telescope, C: grasper
Fig. 40.15 
By thoracoscopy, the first stitch is done to approximate the two ends
Fig. 40.16 
The first outer layer is sutured by V-Loc™ suturing device (a, b)
Fig. 40.17 
Jejunum and esophagus are open. First stitches of the inner posterior layer (a, b)
Fig. 40.18 
Anterior layer is sutured (a). Schematic view of esophagojejunostomy anastomosis (b)
Fig. 40.19 
Final aspect of the intrathoracic anastomosis







References
Arru L, Azagra JS, Facy O, et al. Totally laparoscopic 95% gastrectomy for cancer: technical considerations. Langenbecks Arch Surg. 2015;400(3):387–93.
Sarriugarte A, Arru L, Makai-Popa S, et al. Short-term results of near-total (95%) laparoscopic gastrectomy. Cir Esp. 2018;96(10):634–9.
Parisi A, Nguyen NT, Reim D, et al. Current status of minimally invasive surgery for gastric cancer: A literature review to highlight studies limits. Int J Surg. 2015;17:34–40.
Desiderio J, Jiang ZW, Nguyen NT, et al. Robotic, laparoscopic and open surgery for gastric cancer compared on surgical, clinical and oncological outcomes: a multi-institutional chart review. A study protocol of the International study group on Minimally Invasive surgery for GASTRIc Cancer-IMIGASTRIC. BMJ Open. 2015;19;5(10):e008198.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
40.1 Electronic supplementary material
Below is the link to the electronic supplementary material.
Laparoscopic 95% gastric resection manual anastomosis
Laparoscopic total gastrectomy. Manual esophagojejunostomy anastomosis
Robot-assisted manual esophagojejunal anastomosis
Thoracoscopic esophagojejunostomy
Rights and permissions
Copyright information
© 2021 Springer Nature Switzerland AG
About this chapter

Cite this chapter
Azagra, J.S., Pascotto, B., Arru, L., Ibañez, F., Makkai-Popa, S.T., Goergen, M. (2021). Hand-Sewn Anastomosis After 95% Gastrectomy, Total Gastrectomy, and Total Gastrectomy Extended to the Distal Esophagus for Gastric Cancer. In: Asunción Acosta, M., Cuesta, M.A., Bruna, M. (eds) Atlas of Minimally Invasive Techniques in Upper Gastrointestinal Surgery. Springer, Cham. https://doi.org/10.1007/978-3-030-55176-6_40
Download citation
DOI: https://doi.org/10.1007/978-3-030-55176-6_40
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-55175-9
Online ISBN: 978-3-030-55176-6
eBook Packages: MedicineMedicine (R0)