
Abstract
Diagnostic imaging has been using ionizing radiation techniques since 1896. An image is obtained as X-rays having been attenuated differently by different tissues in the patient’s body, will reach the image detector or not. This variation in attenuation causes a gradation of grey values in the image, which can subsequently be interpreted. In dentistry several techniques have been developed in intraoral (e.g. periapical and occlusal radiography) and extraoral imaging (e.g. panoramic and cephalometric radiography). Two dimensional images are still the standard, whereas three dimensional imaging should be considered an adjunct in those cases where the former is lacking in diagnostic information. Three dimensional imaging with ionizing radiation is known as computed tomography and is available in two variations: multi-slice computed tomography and cone beam computed tomography. Magnetic resonance imaging and ultrasonography are two diagnostic imaging techniques that do not use ionizing radiation. The former computes a diagnostic image by using magnetic fields to influence the hydrogen atoms’ spins in the tissues, whereas the latter computes an image by detecting the reflexion of ultrasonic waves from the tissues. Differences in water content and impedance of the tissues, respectively, will provide the possibility to distinguish between tissues in both these techniques. Choosing the correct imaging modality for the right purpose is the challenge in diagnostic imaging. Some techniques are more useful to investigate hard tissues (e.g. cone beam computed tomography), whereas others are more useful to investigate soft tissues (e.g. ultrasonography).
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
2.1 Introduction
The famous picture of the radiograph taken of Roentgen’s wife’s hand, was the start of a new era. On 12 January 1896, merely two weeks after Roentgen’s discovery of X-rays was published, Dr. Otto Walkhoff probably took the first dental radiograph which initiated the birth of dental radiography. In Fig. 2.1, a timeline shows what the images looked like back then and how long the exposures had to be. It also shows important events and discoveries that changed the field of medicine and dentistry. The author is pretty sure that this is not the end of that timeline, as new technologies and improvements of current technologies will be explored and applied.

Timeline showing introductions of innovation in diagnostic imaging from 1895 until 2019
Since 1896, a new era was born and ever since, dental radiographs have proven their significant value in dental and maxillofacial diagnosis. For many years two-dimensional intraoral radiography and extraoral radiography was the only radiographic modality, but in recent years, three-dimensional imaging in dentistry (CBCT, i.e. Cone Beam Computed Tomography) has become common ground. Challenges regarding tomography of the skull were battled by the Finish Professor Paatero, who developed the first panoramic machine. Many of us refer to the panoramic radiograph as ‘pan’, ‘pano’, ‘panorex’, ‘DPT’, ‘OPT’ or ‘OPG’. Other advanced imaging modalities such as Multi-Slice Computed Tomography (MSCT), Magnetic Resonance Imaging (MRI) and ultrasound imaging are also available to the clinician. Both MSCT and MRI are too expensive to be used in a dental environment, but they have their applications in dentistry. Ultrasonography is in some countries around the world better accepted than in others for diagnostic purposes in the dental and maxillofacial region. Without a doubt ultrasonography or echography, as it is also called, has definitely a place in our armamentarium. In contrast to MSCT and CBCT and plain radiography, MRI and ultrasonography do not use ionizing radiation, and can therefore be considered ‘safer’ than the other imaging modalities. Infrared thermography, near-infrared transillumination and laser fluorescence are gaining more ground in dentistry too. The first one is used for soft tissue pathology (e.g. cancer) and the two latter rather for caries diagnosis. Further research will show how reliable these two latter techniques are and if they can replace ionizing radiation (e.g. bitewing radiographs). Figure 2.1 also shows the introduction of ultrasonography in 1939 by Dr. Sokolow, who managed to image soft tissues when patients were submerged in water or when a bag of water was placed over the patient to allow ultrasound waves to penetrate the patient’s tissues. The principle of and need for a watery medium will be discussed elsewhere in this book. As is clear from the timeline in Fig. 2.1, the introduction of magnetic resonance imaging (MRI) took place around the same time as the introduction of multi-slice computed tomography (MSCT). Drs. Hounsfield and Cormack, the inventors of MSCT, stuck to the use of ionizing radiation, while Dr. Lauterbur suggested the future lie in magnetic resonance imaging, or nuclear magnetic resonance imaging (NMR), as it was first called. In the last decade of the twentieth century, cone beam computed tomography (CBCT) was introduced into dentistry in particular. This technology has rushed like a tsunami over dental imaging and it seems, assessing the literature published about dental imaging in the last 20 years, that there is more than plenty written and researched about CBCT. However, CBCT uses ionizing radiation and therefore carries a potential risk to patients, which is something, especially in paediatric dentistry, of great concern, as this technique is proposed to be used in orthodontic planning and follow-up. Though it is not the scope of this book to address this issue, the author wishes, nevertheless, to draw the reader’s attention to this issue, as the main technique this book is emphasizing on is not using ionizing radiation at all. This chapter will further focus on the different imaging modalities that are available within the dental field. Table 2.1 shows an overview of intraoral and extraoral techniques, two- and three-dimensional imaging and ionizing versus non-ionizing diagnostic imaging. Table 2.1 is further explained in the following paragraphs, each describing the particular diagnostic imaging techniques. The reader who is interested in more detailed information is kindly referred to the textbooks mentioned in the reference list of this chapter.
2.2 Ionizing Radiation or X-rays
All X-ray machines consist, generally speaking, of the same components [1,2,3,4]. A vacuum glass tube contains the negatively charged cathode, which looks like an incandescent light bulb’s filament, and the anode, which is a flat surface allowing for electron collisions, which will subsequently cause production of X-rays if the energy of the incoming colliding electrons from the cathode is high enough. The number of electrons is determined by the Amperage (usually milli-Ampere or mA) and is proportionate to the number of X-rays and hence to the X-ray dose. Both anode and cathode are usually made of Tungsten (W) or Molybdenum (Mo). The electrons are attracted to the anode due to a high voltage across both. That (kilo-)voltage determines the penetration power (energy) of the X-rays that are produced. Most medical X-ray machines have a rotating anode to dissipate the heat better, as they use longer exposure times, higher kV and mA settings. Approximately 99% of all electron collisions are after all only causing heat and no X-rays. The vacuum glass tube is therefore surrounded by oil, in order to cool down the machine. Lead lining around the machine is essential, as X-rays should only be exiting the machine through the collimator, which is aimed at the patient and the image detector. Before the X-rays exit the machine, they pass through an aluminium filter, which ensures only high enough X-rays will exit the machine. Lower energy X-rays would only add to the patient’s absorbed dose and not benefit the image. Therefore filtering out the low energy X-rays is essential. The latter will benefit image quality (less scattered radiation) and will also decrease the patient’s absorbed radiation dose. In medical diagnostic X-ray machines, the collimation can easily be changed and the machines are manufactured with a diaphragm light bundle to visualize the surface that will be irradiated. This is not the case in dental radiography equipment.
2.3 Intraoral Imaging
2.3.1 Bitewing and Periapical Radiography
In intraoral radiography the image detector is placed inside the patient’s mouth and the X-ray machine is positioned extraorally, and stationary, aiming at the image detector. There are three ways of obtaining intraoral radiographs: parallel technique, bisecting angle technique and occlusal technique. The latter two techniques are somewhat different, as the X-rays are not aimed perpendicular at the image detector, but perpendicular at the imaginary bisecting angle between the long axis of the tooth and the long axis of the image detector [1,2,3,4]. Under ideal circumstances, a periapical and bitewing radiograph requires the image detector to be as parallel and close as possible to the teeth, with the X-ray beam aligned perpendicular to the image detector. This is the so-called parallel technique. This creates geometrically accurate images of teeth and alveolar bone levels. To obtain proper alignment one should use image detector holders (e.g. Rinn® and Hawe Neos®) with extraorally placed guidance rods and rings, which definitely help properly aligning the X-ray machine with the image detector. Unfortunately the image detector cannot always be placed ideally inside the patient’s mouth due to anatomical restrictions (e.g. shape of the palate, the level of the floor of the mouth or a mandibular torus), or due to the patient not tolerating the intraoral placement of the image detector. In some cases, the parallel technique cannot be performed as the patient does not tolerate the image detector placement parallel to the teeth. In that case, one can attempt the bisecting angle technique. This technique requires one to aim the X-ray beam perpendicular at an imaginary bisecting line between the long axis of the tooth and the long axis of the image detector as mentioned above. This is a more difficult technique as there is usually no image detector holder involved with an extraoral guide to aid with the X-ray machine alignment. There is, however, an image detector holder on the market that allows for proper alignment using the bisecting angle technique: the Rinn® BAI (bisecting angle instrument). Unfortunately it is usually the image detector holder that causes issues for patients and as a consequence this holder is less frequently used.
2.3.2 Occlusal Radiography
If neither the parallel nor the bisecting angle technique is possible, then one more alternative is still possible: the occlusal radiograph. For this technique, one uses best a photo stimulable phosphor storage plate, as these come in different sizes and allow for proper placement in the patient’s mouth. For primary teeth, a size 2 will suffice, while for permanent teeth, a more useful size would be size 4. These images will not always produce the perfect geometrically aligned images as is the case with the parallel technique, but can still provide sufficient diagnostic yield. Intraoral radiography is the standard diagnostic imaging technique to assess interproximal caries, and also interproximal periodontal bone levels. Bitewing radiographs are good examples of the latter, whereas periapical radiography and occlusal radiography are better for evaluation and assessment of the periapical regions of the jaws. The major limitation of intraoral radiography is that it is only a two-dimensional imaging modality which is not very good at differentiating between soft tissues (see Table 2.1). That being said, it should be emphasized that occlusal radiographs can be useful in identifying radiopaque sialoliths in the floor of the mouth, despite the fact that the musculature and glandular tissue cannot be differentiated.
2.4 Extraoral Imaging with Stationary X-ray Tube
2.4.1 Cephalometric Radiography
The cephalometric radiograph [4] is very often used in orthodontic and orthognathic surgery planning. The technique requires a specialized X-ray machine which provides a reproducible lateral skull view. That reproducibility is important as certain structures in the skull, and especially the sella turcica, have to be used as reference to verify growth or the impact of disease or surgery. A dental cephalometric radiograph is therefore unique and that is exactly why the machine is equipped with a so-called cephalostat. This device helps position the patient with the midsagittal plane of the skull perpendicular to the floor, by putting an ear rod in each external acoustic meatus, while a support on the bridge of the nose reassures the patient’s head is in a natural position. The patient should have the teeth in occlusion during the exposure. Some manufacturers use a one-shot approach, which implies a 1 s X-ray exposure and hence very little chance for motion artifacts. Other manufacturers use an anterior to posterior or vice versa scan of the skull, which takes several seconds, hence a higher chance for motion artifacts during the exposure. Technically the latter machines are therefore not stationary X-ray tube machines. Cephalometric images should always show the soft tissues overlying the face and neck, as these outlines are also used for planning purposes in several orthodontic and orthognathic analyses. By convention, the image is supposed to be viewed with the patient facing to the right-hand side. It needs to be emphasized that one cannot distinguish between the different soft tissues (e.g. salivary glands from muscular tissue) on a cephalometric radiograph. The medical lateral skull radiograph differs significantly from a dental cephalometric image, as the first one does not use a cephalostat, and therefore reproducibility is impossible. Medical lateral skull radiographs are rarely used in dentistry. Many clinicians do not realize that the cephalostat can also be rotated and allows one to take other skull radiographic projections, which are more common in medicine: anterior-posterior skull, posterior-anterior-skull, submento-vertex skull and any deviation or variation of the former positions. Since the use and availability of cone beam computed tomography (CBCT) have increased, most of these techniques have become obsolete, as these views of the skull can be easily regenerated from a CBCT scan, while providing more information as the latter technique offers three-dimensional images.
2.4.2 Oblique Lateral Radiography
A technique which is often forgotten is the oblique lateral radiograph [1, 4]. This technique is overlooked by many, but definitely has a place in paediatric dentistry imaging and imaging in patients with special needs. In the hands of an experienced clinician/radiographer this technique can provide very good diagnostic information. This being said, it needs to be emphasized that there is a learning curve to produce good oblique lateral radiographs. This technique requires a stiff cassette with a phosphor storage plate inside and an X-ray machine that is used for intraoral radiography. The exposure time is only 0.16 s at 65 or 70 kV. The image detector should not bend as that would cause significant distortion in the image. The cassette should be held against the side one wishes to image, and should be in contact with the tip of the nose and the cheek. Part of the cassette should be inferior to the inferior border of the mandible. Subsequently the patient has to turn the head towards the side the cassette is leaning against. This creates a radiographic key-hole on the opposite side between the cervical spine and the posterior border of the ramus of the mandible. The X-ray machine, with circular collimator, is now aimed perpendicular at the cassette, with the central X-ray beam following the occlusal plane. For the latter one can use the lips as a guide. If the geometry was correct, the image should be a perfect circle. If one sees an oval, it means the X-rays were not aimed perpendicular at the cassette. It is obvious that this technique is only to be considered an alternative for a panoramic radiograph or a periapical or bitewing radiograph in cases where patients are not able to cope with the procedure. Oblique lateral radiographs have the same limitations as intraoral radiographs and cephalometric radiographs regarding soft tissue diagnosis.
2.5 Extraoral Imaging with Revolving X-ray Tube
2.5.1 Panoramic Radiography
Dental panoramic tomography is often called, depending on the region in the world, a panorex, a pan, an OPG, an OPT, a DPT, just to name a few. They all refer to the same technique and the same image that is generated [1,2,3,4]. This technique implies that the X-ray source and the image detector, placed opposite of each other, rotate synchronous around the patient’s head, with the image detector passing as close as possible to the patient’s face. By doing so, one creates a focal trough, or a slice with a particular thickness. The shape of the focal through is a three-dimensional horse shoe, which, ideally, follows the shape of the dental arches as good as possible. The thickness of the slice depends on the width of the X-ray beam. The narrower the beam, the thinner the slice. The latter means a more sharp image, but there is a threshold of course, below which one should not go, as the image would become non-diagnostic. Some machines allow for adjustments to the shape and size of the focal trough, while others do not. The latter are usually cheaper and assume one size fits all. It is evident that this is incorrect and that if the shape of the jaw can be followed more accurately, the image will be better as well. The most recent machines use technology that collects information from different image layers, without radiation dose increase, but with image quality improvement. The X-ray beam used in panoramic radiography is collimated as a vertical narrow slit beam, which can be adjusted in height to accommodate for adult or paediatric settings. This collimation is essential when imaging children as it will reduce the radiation burden and avoid unnecessary parts of the head to be exposed. The X-ray beam is also angled slightly upwards (8–12∘), which explains why structures in the neck, like, for instance, a forgotten necklace or a lead (equivalent) apron over the shoulders and neck, will be projected on the patient’s chin in the final image. It also deserves to be emphasized that the upward angulation of the X-ray beam causes distortion and magnification in a panoramic image, which is about 1.3 in magnitude. Therefore measuring tooth length or bone height, for instance, on a panoramic radiograph is not accurate at all, as differences in patient positioning may cause additional distortion in the final image. Due to the technique there are always ghost or phantom images in panoramic radiography, which makes interpretation of the image sometimes challenging. Just like the previous techniques, also this radiographic imaging technique is not good at differentiating between soft tissues.
2.5.2 Cone Beam Computed Tomography
Cone beam computed tomography (CBCT), as the name of the technique implies, uses a conical (actually pyramidal) shaped X-ray beam, which revolves in a single rotation arc around the patient’s head, while the image detector (flat panel) moves in synchronicity on the opposite side of the skull [1,2,3,4]. The image that is obtained is therefore a cylinder, providing three-dimensional images, and is captured as a whole and not in segments as is the case in multi-slice computed tomography. The latter technique, also called medical CT, uses a fan shaped beam which revolves multiple times around the patient (see further), hence causing a higher radiation dose. In CBCT, one can decide where the pivoting point or rotation axis has to be positioned, in order to get the region of interest in the centre of the scan volume. Some CBCT manufacturers allow for the field of view, or the size of the volume that is scanned, to be changed. Ideally the field of view should be as close as possible to the area of interest, in order to keep the radiation dose as low as possible to the patient. The latter implies that some machines, due to their design, do not allow the field of view to be altered, and therefore might be covering much more volume than they should. Besides the field of view, CBCT manufacturers have autonomy regarding the design of the machine. There are machines that have a chair fixed to the machine (e.g. Morita® Accuitomo 170) and there are machines that have no chair (e.g. Planmeca® 3D Max). The latter usually allows for patients to either stand, or sit on a stool, or sit in a wheelchair for the exposure. It is obvious that the wheelchair should not interfere with the machine. In machines with a chair, the patient will be moved to the correct position for the axis of rotation to fall through the centre of the region of interest. In machines that have no chair attached to their frame, the C-arm manoeuvres around the patient’s head to ensure the correct position of the rotation axis. The resulting images from both machines are similar though. The image resolution has to be decided before the patient is exposed and has to be justified for the purpose. One has to bear in mind that the higher the resolution, the higher the radiation dose will be, as the exposure time will increase. This has to be balanced with the goal of the study. A high resolution (e.g. 76 μm) is indicated for endodontic purposes, while a lower resolution (e.g. 200 μm) would suffice for root resorptions or eruption issue cases. With regard to the rotation arc, it deserves to be mentioned that some manufacturers allow it to be altered, for instance from 360∘ to 180∘ rotation. This reduces the radiation dose with approximately 50%, without affecting the image quality significantly [5, 6]. The latter should definitely be considered when imaging children. Unfortunately the soft tissue resolution of CBCT is low, and as such for soft tissue imaging this technique is not really suited, if one is interested in differentiating between soft tissue layers.
2.5.3 Multi-Slice Computed Tomography
Sir Godfrey Hounsfield invented computed tomography in 1973 and together with Dr. Cormack worked on the development of the first scanner [1, 4, 7,8,9,10,11]. Since then many improvements have been realized to increase image quality of these three-dimensional images, as well as patient comfort. Professor Willi Kalender is credited for his significant contributions to develop helical computed tomography. Commonly this technique is called ‘CT’. It is, however, very different from the cone beam computed tomography (CBCT) that was discussed above. Multi-slice CT uses a collimated narrow fan shaped beam, which revolves several times around the patient, while on the opposite side of the patient, image detectors capture the image. The patient is simultaneously moved slow or fast through that revolving X-ray field. If done fast, the resolution will be low, as the slices will be thicker (large pitch), whereas if done slowly, the slice thickness is thinner (smaller pitch) and hence the resolution is higher (maximum 350 μm, compared to CBCT where the highest resolution today is 70 μm). However, one has to keep in mind that the higher the resolution, the higher the radiation dose will be. As these machines require the patient to lie on a table, while the table is moved into the machine’s gantry, their footprint is considerable and therefore they will not be found in a dental setting. Because of the radiation dose and the need for a radiographer to obtain the images, these machines belong in hospital environments. At the writing of this chapter, the fourth generation CT scanners have been developed and are referred to as stationary-rotate geometry scanners as the X-ray tube rotates within a stationary circle of detectors. Technology allows the detectors to be arranged in a continuous circular array containing as many as forty thousand individual detectors. Whereas in the past scanning time could be substantially long (minutes), today that scanning time is merely a few seconds anymore. The latter causes less movement artefacts to be present in the image, which is a great advantage. However, the resolution of the image can be affected negatively by this fast scanning, as the patient is moved faster through the gantry. Reducing the speed would increase the resolution, but also the radiation dose. It is obvious that this is a trade-off that needs to be made for the pathology one is investigating. That decision lies with the radiologist/radiographer team and the purpose of the diagnostic investigation. MSCT is ideal for hard and soft tissue imaging and as its exposure settings and algorithms are standardized, one can obtain information about the type of tissue one is assessing. The soft tissue resolution is much better than that of CBCT and one can distinguish several tissues from one another (e.g. salivary gland versus muscle), as for the use of the so-called Hounsfield units, which allow for finer diagnosis in assessing the nature of a lesion or a tissue (e.g. haemorrhage in the brain). It is obvious that MSCT, because of its high radiation dose associated, is not an imaging modality one would order for common dental pathology, such as dentigerous cyst or radicular cyst. However, patients who suffered a severe trauma with risk of intracranial haemorrhage would benefit from being submitted for MSCT immediately after the accident, as it could save their lives. This technique is also indicated for pathology involving the jaws which invades the surrounding soft tissues (e.g. squamous cell carcinoma, osteosarcoma).
2.6 Non-ionizing Radiation Techniques
2.6.1 Magnetic Resonance Imaging
Magnetic resonance imaging (MRI) was initially called nuclear magnetic resonance (NMR), but because the public’s erroneous perception that there was a connotation with nuclear energy made the medical profession change the name to MRI [1,2,3,4, 8, 9, 11]. This technique does not use ionizing radiation, but magnetism and the fact that hydrogen atoms, hence the original name nuclear imaging, can be influenced in their precession when a high magnetic field is applied. The principle is to place the patient in a very strong magnetic field (1.5 or 3.0 T), several times higher than the Earth’s magnetic field (approximately 0.5 μT). This will have an effect on the hydrogen atoms (protons) in the human body, which can be considered as positively charged randomly spinning tops. These hydrogen atoms will respond to the high magnetic field and will start spinning in a particular direction and at a specific speed and with a particular magnitude. Since the hydrogen content is different per type of tissue in the body, every type of tissue will emit a different signal when the magnetic field is switched on and off. When the magnetic field is turned off, the hydrogen atoms return to their resting state. The speed of this, as just mentioned, depends on the tissue (amount of hydrogen atoms and their chemical bonds). The software translates these returns into an image of grey values, which allows for differentiation between soft tissues very well. Therefore MRI is the preferred technology to image soft tissue and soft tissue pathology. Tissues with a lot of hydrogen atoms will give a strong signal (e.g. salivary glands are bright white) and tissues with a low amount of hydrogen will result in a low signal (e.g. cortical bone is black). Both hard and soft tissue diagnosis is possible, however, the technique gets more credit for imaging soft tissues. In order to obtain the best image, several so-called sequences can be used, which result in images with differences in appearance of the tissues. In a T1 sequence, fat will give a high signal (white), while water will give a low signal (dark), whereas in a T2 sequence, water will give a high signal (white) as will fat. Some other examples of particular sequences that are used are: spin echo, fluid attenuated inversion recovery or FLAIR, short time inversion recovery or STIR and turbo spin echo or TSE. In its physical appearance the MRI machine shows some resemblance with the MSCT machine, but as explained, the technology is completely different. Caution is required when entering the MRI area in the hospital. All ferro-magnetic materials need to be banned from the room and its immediate surroundings as it would cause harm to the patients and damage the machine. Since the magnetic field in the MRI is several hundred times stronger than the earth’s magnetic field (30 μT near the equator and 70 μT at the poles), objects like scissors, oxygen tanks, metal carts, for instance, would be attracted into the magnet with great force. Accidents have happened and as such precaution is key when entering the zone around an MRI machine. Audible and visual warning signs are always in place to announce visitors of potential risks entering the zone. MRI in dentistry is indicated if the patient has soft tissue pathology that requires imaging (e.g. ranula, salivary gland tumour) or a temporomandibular joint disorder that affects the muscles and/or condylar disc. In the latter case MRI will enable one to visualize the disc clearly (low signal as the disc does not contain as much hydrogen atoms as muscle, for instance) in the joint space. One also has to keep in mind that MRI machines produce a banging sound (sometimes more than 95 dB, which requires ear plugs or head phones to be worn by the patient), which might be frightening and which may require some patients to be sedated. Claustrophobia is another issue as often a mask (magnetic coils) is placed over the patient’s face, which again may be another reason for patients to be sedated. The high cost of the machine, the large footprint, the specialized technical support and the special requirements for the room make this piece of equipment unique and therefore highly unsuited for a dental office environment.
2.6.2 Ultrasonography
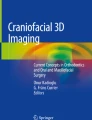
Ultrasonography or echography is another imaging modality that does not use ionizing radiation [1,2,3,4, 8, 9, 11]. However, compared to MRI, this machine is very cheap (thousands of dollars versus millions). This technique is probably best known for its application in OB/GYN medicine to visualize the unborn child in the womb. The technique uses ultrasonic waves which are generated in a piezoelectric crystal inside the so-called transducer, which not only emits but also receives the ultrasonic waves. An example of a linear and hockey stick type transducer is shown in Fig. 2.2. The speed of sound is affected by the compressibility of the medium (acoustic impedance), therefore it travels faster in rigid materials which are more resistant to compression and it travels slower in fluids and gases as these are more susceptible to compression. Reflection of the sound is paramount in this technique as the sound will be reflected at boundaries of tissues. Tissues or pathology that reflect little to no sound waves will produce no ‘echo’, hence the typical jargon hypoechoic or anechoic, respectively, whereas tissues or pathology that do reflect the sound waves will return an echo and will be identified as echoic or hyperechoic (high signal or white shadow). The particular characteristics of each of the soft tissues will enable one to distinguish between them (e.g. healthy salivary gland tissue shows a homogenously grey echo, whereas muscular tissue is hypoechoic). When the ultrasound beam hits a boundary between two materials with different acoustic impedance, some of the beam will be reflected and the remainder will be transmitted. For diagnostic imaging, an ultrasound frequency between 2 and 20 MHz (mega Hertz) is required. This is initiated inside the transducer, which is held in contact with the soft tissues. However, since air is a bad medium for sound, a so-called coupling agent (a gel or a gel pad) is required to ensure a good contact. If ultrasound is used intraorally, saliva or a gel pad will be the coupling agent. This is the principle earlier described by Sokolow in 1939, who used a water bath as coupling agent or medium. The frequency affects the travel depth or penetration of the ultrasound waves. The lower the frequency, the deeper the ultrasound will travel, while the higher the frequency, the more superficial the penetration will be. The images from the latter will, however, have a higher resolution than the former. Colour Doppler is a feature in ultrasound that allows for visualization of vascularization. That is a feature that will be useful in live image identifying pathology (e.g. hypervascularisation in a tumour) or to assess healing tissue (e.g. check blood flow after a flap or major orthognathic surgery). Variation in operators, in terms of application of amount of pressure on the patient’s tissues with the transducer, will result in different images. But then again, ultrasonography does not pose any danger for the patients and can be repeated as often as needed, if one requires to check the patient again. In the field of dentistry, ultrasonography is useful in patients with, for instance, salivary gland problems (e.g. sialolith, mumps), muscular issues and hypertrophy of lymph nodes (lymphadenopathy). Since it requires special training and is not yet often used in the dental setting, this imaging modality will usually be available in specific hospital settings or private specialty clinics. The harmless character of ultrasonography and the small footprint of the modern machines (some can be plugged into a mobile phone or a tablet) and the fact that this technique allows for quick and live image assessment of soft tissues inside and outside the oral cavity make this a very promising diagnostic technique in modern oro-dental medicine.

Example of linear Philips® transducers (left-hand side is a traditional linear transducer and right-hand side is a hockey stick type transducer, which can be used intraorally on the cheek or tongue, for instance)
2.7 Conclusion
The majority of imaging in dentistry is mostly covered by intraoral radiography, as this technique often provides sufficient diagnostic yield. However, in other cases where there is substantial involvement of pathology spreading within the jaws, additional imaging modalities should be used. Panoramic radiography provides a large overview of the maxillofacial complex and can provide adequate diagnostic information in several cases, though this two-dimensional imaging modality with its distortions is sometimes simply not good enough. For the latter, cone beam computed tomography, which provides three-dimensional images, may be the solution, especially if the information one is after is to be found in hard tissues, such as teeth and bone. However, if one suspects the pathology involves hard and soft tissues, a multi slice computed tomography scan is the best choice. After all, one has to balance which technique is beneficial in each individual clinical case: two-dimensional versus three-dimensional and ionizing radiation versus non-ionizing radiation. These latter techniques all use ionizing radiation, which hold potential risk for the patient to develop a fatal cancer over time (stochastic effects of ionizing radiation). At the other end of the diagnostic imaging spectrum, there are magnetic resonance imaging and ultrasonography, both techniques which are not using ionizing radiation and which also can provide three-dimensional images. However, the applicability of these techniques is quite different. While magnetic resonance imaging can also provide important information about hard tissue (e.g. bone) involvement in the pathology that is mainly occupying soft tissue, ultrasonography is a more affordable imaging modality, compared to magnetic resonance imaging, and can be used in a chairside setting in a dental office to investigate soft tissues in the head and neck region (e.g. salivary glands, tongue). Even intraoral use of ultrasonography is possible (e.g. gingiva measurements, apical bone lesions). Other imaging modalities, such as thermography and near-infrared light, certainly deserve our attention, as they may be playing a role in the future, once their accuracy has been proven for diagnosis in the head and neck region. This chapter has not addressed the cost of the equipment in detail, but it is obvious that multi slice computed tomography and magnetic resonance imaging are too expensive to be used in a dental setting, let alone their foot print which would not suite a dental office anyway.
References
Whaites E, Drage N. Essentials of dental radiography and radiology. Amsterdam: Elsevier; 2013. ISBN: 0702045993.
White SC, Pharoah MJ: Oral radiology-E-Book: principles and interpretation. Amsterdam: Elsevier; 2014. ISBN: 0323096344.
Haring JI, Jansen L. Dental radiography: principles and techniques London: WB Saunders; 2000. ISBN: 0721685455.
Aps J. Imaging in pediatric dental practice. Berlin: Springer; 2019.
Hoff MN, et al. Can cephalometric parameters be measured reproducibly using reduced-dose cone-beam computed tomography? J World Fed Orthod. 2019;8(2):43–50. ISSN: 2212-4438.
Yeung AWK, Jacobs R, Bornstein MM. Novel low-dose protocols using cone beam computed tomography in dental medicine: a review focusing on indications, limitations, and future possibilities. Clin Oral Investig. 2019;23(6):2573–81. ISSN: 1432-6981.
Mahesh M. MDCT physics: the basics-technology. In: Image quality and radiation dose, vol. 62. Philadelphia: Lippincott Williams & Wilkins; 2009.
Graham D, Cloke P, Vosper, M. Principles and applications of radiological physics. London: Churchill Livingstone; 2011. ISBN: 0702043095.
Armstrong P, Wastie M, Rockall AG. Diagnostic imaging. London: Wiley; 2010. ISBN: 1444391232.
Upton AC, Mettler FA Jr. Medical effects of ionizing radiation. Philadelphia: WB Saunders; 1995.
Hendee WR, Ritenour ER. MyiLibrary medical imaging physics. London: Wiley; 2002.
Author information
Authors and Affiliations
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2021 Springer Nature Switzerland AG
About this chapter

Cite this chapter
Aps, J. (2021). Ultrasonic Imaging in Comparison to Other Imaging Modalities. In: Chan, HL.(., Kripfgans, O.D. (eds) Dental Ultrasound in Periodontology and Implantology. Springer, Cham. https://doi.org/10.1007/978-3-030-51288-0_2
Download citation
DOI: https://doi.org/10.1007/978-3-030-51288-0_2
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-51287-3
Online ISBN: 978-3-030-51288-0
eBook Packages: MedicineMedicine (R0)