
Abstract
This chapter discusses the importance of coordinating speech-language services in the community, school, and home settings for youth with autism spectrum disorder (ASD). The role of the speech-language pathologist (SLP) is discussed relative to assessment and treatment of youth with ASD, over the course of development. Practical recommendations are provided for ways that the SLP can work with other community members to build inclusive communities. Interprofessional practice and other models of collaboration are considered, including case scenarios and resources to support successful evidence-based practice collaborations between SLPs and other professionals when supporting individuals with ASD.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
- Pediatrics
- Autism spectrum disorder
- Neurodevelopmental
- Autism
- Management
- Treatment
- Interdisciplinary
- Speech
- Language
- Speech-language pathology
- Youth
Autism spectrum disorder (ASD) is a complex neurodevelopmental disorder (Betancur, 2011; Pelphrey, Shultx, Hudac, & Vander Wyk, 2011). Individuals with ASD meet a defined set of clinically diagnostic criteria (e.g., DSM-5; American Psychiatric Association, 2013), and yet they comprise a heterogeneous and neurodiverse group of individuals. The continuum of language and communication profiles of individuals with ASD is particularly diverse, and can range from nonverbal to minimally verbal to verbally fluent with language impairment to verbally fluent without language impairment (Kasari, Brady, Lord, & Tager-Flusberg, 2013; Kjelgaard & Tager-Flusberg, 2001; McGregor et al., 2012; Tager-Flusberg & Joseph, 2003). Deficits in social communication skills (including pragmatic language) are one of the core features of ASD. Children with ASD may also experience co-occurring deficits in the other domains of language: phonology, semantics, morphology, and syntax. Speech-language pathologists (SLPs) are important members of the service delivery team for youth with ASD and contribute unique knowledge and skills, especially in the areas of language and social communication.
According to the American Speech-Language-Hearing Association (ASHA, 2016), SLPs are professionals who support people with communication disorders and differences across the lifespan. Collaboration is one of eight key service delivery domains for SLPs, along with counseling, prevention and wellness, screening, assessment, treatment, modalities and technology, and populations and systems. “SLPs share a responsibility with other professionals for creating a collaborative culture” (ASHA, 2016, p. 8). A collaborative culture is especially important when coordinating speech-language pathology services for individuals with ASD (see additional resources in Appendix A).
SLPs are not typically the professionals who diagnose ASD (ASHA, n.d.), but may be the professionals who first notice signs and symptoms of ASD in young children, especially those enrolled in early intervention for late language emergence. In a prospective study of young children at risk for ASD, the earliest signs and symptoms of ASD emerge between 6 and 12 months of age (Ozonoff et al., 2010). The earliest signs and symptoms appear in the social communication domain, and include reduced gaze to faces, social smiles, directed vocalizations, and social engagement in children with ASD compared to those without ASD. One of the earliest red flags for ASD that caregivers notice, as a disruption in social communication, is reduced response to name at around 9–12 months of age (e.g., when the child is looking down at a toy and does not turn to look at his mother when she calls his name from behind). Delayed emergence of first words, less frequent canonical babbling (reduplication of consonant and vowel sounds; e.g., baba), and reduced gesture use are additional early signs of concern that many times warrant referral to a team of early intervention professionals, including an SLP. In the early developmental period, it is critical that the SLP know how to differentially diagnose language disorders and know when to collaborate, consult, and/or refer to other developmental specialists if an ASD diagnosis is suspected.
SLPs are the experts who assess language and communication for children who have ASD or who are at risk for ASD. SLPs may work as part of an interdisciplinary or interprofessional autism diagnostic team in healthcare and educational settings. In these models, the SLP is a member of the team along with other service providers (e.g., developmental pediatrician, occupational therapist, physical therapist, and psychologist) and the individual with ASD. Interdisciplinary teams involve professionals assessing the child in their area of expertise and then coming together to discuss the results of each of their individual assessments (Johnson, 2016). In comparison, interprofessional teams are more collaborative, including assessments where members of the team work together to plan and administer the assessment (Johnson, 2016). Communication is regular and ongoing. Families benefit from high-quality communication among team members because the results of the assessment are more likely to be explained the same way by all members of the team.
Interprofessional SLP Collaborations Across the Lifespan
Early Intervention
It is important for SLPs and the general population to know the signs of ASD. For children seeking an early intervention evaluation and for those already enrolled in early intervention for speech and language services, the SLP is often the first person to notice the signs and symptoms of ASD. An early diagnosis of ASD comes with the added benefit of early intervention services.
In early intervention, the SLP collaborates with families and caregivers to support wellness and development for the child with ASD. Support includes prevention and wellness activities, such as making appropriate and informed referrals to other healthcare providers and educators. Early intervention is critical to successful long-term language and communication outcomes for children with ASD. As reported by Koegel, Koegel, Ashbaugh, and Bradshaw (2014), fewer than 10% of children with ASD remained nonverbal after early intervention, whereas 50% of children who did not enroll in early intervention remained nonverbal.
Wagner, Wallace, and Rogers (2014) recommend several developmental treatment approaches for young children with ASD (e.g., Early Start Denver Model, Milieu Teaching, and Hanen More than Words). Developmental approaches to treatment meet five criteria: (1) follow the sequence of typical development, (2) reference research on typical development to guide clinical decision-making, (3) focus on child–adult interpersonal relationships, (4) use child-centered approaches, and (5) use play as the context for intervention (Wagner et al., 2014). In developmental approaches to intervention, a speech-language pathologist is often part of an interdisciplinary team of occupational therapists, physical therapists, behavior analysts, child psychologists, special educators, and physicians. The team of professionals works together to conduct assessments and develop treatment plans. Goals may target prelinguistic skills (e.g., gesture or directed eye gaze) or language and social communication skills, depending on the individualized needs of the child.
The Preschool Years
During the preschool years (ages 3–5 years), children with ASD who continue to need intervention transition from home-based early intervention to school and/or center-based services. A child who had an individualized family service plan (IFSP) and continues to qualify for intervention services in the public schools, will likely receive an individualized education plan (IEP). The IFSP and IEP documents are created via collaboration with other rehabilitation and education professionals, since young children with ASD often require intervention services from several different professionals.
During the preschool years, children with ASD often work with an SLP on their language and social-pragmatic communication development. Given the range of language abilities in children with ASD, from nonverbal to verbally fluent, treatment goals will be individualized to address the language and communication needs of the child. For a child who is nonverbal or minimally verbal, augmentative and alternative communication systems may be utilized to support communication. The SLP may consult with other educators regarding ways to facilitate social communication and interaction while using the child’s AAC system. For children with ASD who are verbal communicators, intervention targets may focus on building pragmatic language skills, receptive and expressive vocabulary, increasing comprehension and use of a variety of developmentally appropriate grammatical morphemes and syntactic forms, phonology, preliteracy skills, and/or speech sound intelligibility.
One example of assessment and treatment collaboration among preschool professionals may include the SLP, classroom teacher, and reading intervention specialist. Some children with ASD develop average reading skills, while others demonstrate difficulty learning to read. Preschoolers with ASD who demonstrate poor phonological awareness and emergent literacy skills tend to be at risk for reading impairments, and those with co-occurring spoken language impairments are at even higher risk (Davidson & Ellis Weismer, 2014; Dynia, Bean, Justice, & Kaderavek, 2019). SLPs can work together with classroom teachers, special education teachers, and reading intervention specialists to assess all areas of phonological awareness, plan for treatment and write appropriate literacy goals, and implement the intervention plan for preschoolers with ASD who are at risk for reading impairments (Langer & Watson, 2008). SLPs can provide explicit classroom instruction on phonological awareness.
School-Age and Beyond
Many evidence-based intervention practices are available to target social and communication skills in children with ASD ages 6–14 years; however, fewer evidence-based intervention options are available for individuals with ASD who are high school age or older (Prelock & McCauley, 2012; Wong et al., 2015). Life-long support may be required for many individuals with ASD. Adolescents and adults with ASD struggle with social isolation: fewer than 10% have reciprocal friendships with peers, and nearly half have no peer relationships (Orsmond et al., 2004). It is critical that SLPs work together with other professionals, care providers and the individual with ASD to promote social-pragmatic and communication development during the school-age years. A team approach to transition planning for life beyond high school may also promote optimal social-communication outcomes and reduced social isolation during adolescence and adulthood.
Intervention for language, literacy, and communication during the school-age years may take place in an educational or outpatient setting. SLPs in the public schools are part of individualized education plan (IEP) teams, help with planning multitiered systems of support (MTSS) and response to intervention (RTI), consistent with the individuals with disabilities education improvement act (IDEA, 2004; Hollenbeck 2007; Leach, 2018). SLPs who work in outpatient hospital or community clinics may run social skills groups or work with individuals one-on-one to target social communication, language, and/or literacy.
During the school years, SLPs must work together with other school personnel to ensure that assessments and treatments are curriculum-based and educationally relevant. In a systematic review, compelling evidence was found to support SLPs and classroom educators in collaboration around curriculum-based target vocabulary and phonological awareness preliteracy activities in early elementary school (Archibald, 2017). The development of literacy skills is as important for children with ASD as they are for any other school-age child. Literacy skill development includes a progression from learning to decode and read to the establishment of good reading fluency and reading comprehension skills (Lanter & Watson, 2008). Fluent readers with ASD may experience less difficulty with fact-finding literacy tasks, but more difficulty with reading questions that require taking the perspective of characters in the story, making inferences from the story, and considering the beliefs and perspectives of characters in a story (Lanter & Watson, 2008).
SLPs collaborate and consult with families to support the child’s communication development at school and home. Alli, Abdoola, and Mupawsoe (2015) surveyed nine parents of children with ASD (average age 11.8 years), who described that the communication challenges that existed within their families impacted their ability to participate in activities outside of the home. Alli and colleagues encouraged SLPs to work together with families to support improved understanding when new modes of communication are introduced in therapy (e.g., picture exchange communication system [PECS]), and to educate families on effective communication strategies. In-service events for caregivers of children with ASD provide an excellent opportunity for SLPs to partner with teachers and other school professionals around teaching effective communication strategies to use at home and school (e.g., teaching caregivers to repeat and explain new vocabulary, or to increase wait time before expecting a response to aid comprehension).
When working with youth with ASD who have severe disabilities, Bruce and Bashinski (2017) encourage an interprofessional practice approach that includes the learner, the communication partner, and the environment. A collaborative team approach is especially important with children with severe disabilities because each child is likely to have a unique set of co-occurring medical, educational, and communicative needs. No one professional is likely to be expert in all of the child’s areas of need; yet when working collaboratively, each professional, the learner and the communication partners can all contribute their expert knowledge in order to optimize outcomes. The SLP, for example, can recommend ways to augment and enhance communication but the communication partners (e.g., parents, teachers, and paraprofessionals) are likely to be the experts on the everyday communication routines within the child’s environment and can suggest communication situations that require augmentation. Additional examples of interprofessional practice collaborations when working with children with ASD are provided in Appendix B.
Building Inclusive Communities
Community Connections
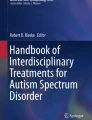
When communities actively work to include children with ASD, stronger communities are created. SLPs can work to build inclusive communities for children with ASD via advocacy and outreach activities. These activities can include work to build relationships between children with ASD, neurotypical peers, and their families. Inclusion of children with ASD in community activities provides all community members with more experiences with neurodiversity. A focus on relationship building can create communities with greater acceptance and understanding of similarities and differences, and stronger community support systems as a result of intentional peer and family relationship building. For example, communities may come together around autism awareness day (see Fig. 1) to support increased public awareness of ASD and community inclusion.

Example of collaboration with parents of children with autism spectrum disorder in a school district to celebrate World Autism Awareness Day. Parents were asked, “what important messages do you want to be heard in a handout to celebrate world autism awareness day?” spokes of the wheel were filled with messages contributed by parents of children with autism
Play Dates
Positive relationships between peers with and without ASD enhance social and academic outcomes for all children. For children with ASD, play dates with peers, including neurotypical peers, can enhance positive peer relationships, friendship building, and social outcomes (Koegel, Werner, Vismara, & Koegel, 2005). SLPs can work together with classroom teachers and paraprofessionals, to facilitate positive peer relationships and friendship building at school, and can provide caregivers with training and suggestions for play dates and socializing outside of school time. In a multiple-baseline case study, Koegel et al. (2005) found improved reciprocal social interactions (verbal initiations, verbal responses, nonverbal eye contact, and joint engagement) during play dates that included contextual support: mutually reinforcing activities and adult-facilitated cooperative arrangements. Activities and locations that are likely to be mutually reinforcing for school-age children might include making crafts, baking and decorating cookies, playing a game, or structured play outside. In order to facilitate a cooperative arrangement between the children, ensure that both children have important roles to play in the activity and scaffold and support their back-and-forth interactions, as needed (e.g., when making cookies together, the adult can give each child a role, like having one child use the cookie cutters and the other child use the spatula to put the cookies on a pan).
Recreational Activities
Community-based unified sports teams provide opportunities for SLPs to collaborate with physical therapists, physical education teachers, applied behavioral analysis professionals, coaches, and families to support successful participation by youth with ASD. In an adapted soccer program for youth ages 5–19 years, children with ASD were partnered with neurotypical high school “buddies”, who volunteered to support full participation of the children with ASD in the soccer practices and games (Hayward et al., 2016). Youth with ASD utilized individualized picture schedules and/or picture exchange communication systems (PECS) and token reinforcements to support communication and participation. After participating in the adapted soccer program, participants improved their physical fitness and soccer skills, and they built positive relationships with their “buddy” (Hayward et al., 2016).
In a survey of parents of children with ASD, 91% of the parents surveyed reported that “development of social skills” (p. 22) was their top goal for a sports program for their child (Alexander & Leather, 2013). The parents also tended to prefer a unified sports setting (59%; one with children with and without disabilities paired together for participation), rather than segregated settings (22%; one where all of the children have a disability) or inclusive settings (20%; one where most children do not have a disability but those with disabilities may participate).
In a study examining the impact of unified sports programs for individuals with intellectual disability, across five different countries (Germany, Hungary, Poland, Serbia, and Ukraine), the athletes with ongoing participation reported improved social inclusion (McConkey, Dowling, Hassan, & Menke, 2013). In particular, the athletes with intellectual disabilities and the partners without intellectual disabilities reported benefits to interpersonal communication skills, especially confidence in talking with one another and building friendships (McConkey et al., 2013). For individuals with ASD and co-occurring intellectual disability, these results may be suggestive of similar gains in social inclusion during participation in unified sports programs. While this study has not been replicated with individuals with ASD, the benefits to improved social communication skills of the athletes with intellectual disability are noteworthy.
SLPs can encourage participation in community recreational athletic events for children with ASD. SLPs may also play a critical role in supporting communication to allow for participation in recreational activities, including adapting AAC equipment to include relevant functional communication messages for athletes with ASD. Key benefits of athletic programs that include youth with and without disabilities playing together, include improved social communication skills, social inclusion, and relationship building among community members.
Interprofessional Education and Interprofessional Practice (IPE/IPP)
Intersectionality: Interprofessional Practice and “Best-Practice”
In the school setting, students benefit when SLPs work collaboratively with other educators, using co-teaching models (Heisler & Thousand, 2019; Justice, McGinty, Guy, & Moore, 2009). Heisler and Thousand (2019) describe four approaches to co-teaching: supportive, parallel, complementary, and team. Co-teaching methods are appropriate for children in preschool through high school.
In a supportive co-teaching model, one professional teaches a lesson while the other circulates to support student learning (Heisler & Thousand, 2019). For example, the SLP may provide a whole-class lesson on social communication skills in an inclusion classroom with children who have ASD and those without ASD. During the lesson, the general education teacher may circulate to support all of the students’ learning during the lesson.
In a parallel co-teaching model, one professional works with a group of children while the other professional works with the remaining children simultaneously (Heisler & Thousand, 2019). If the lesson is about social communication skills, children may circulate around stations in the room that each focus on different components of social communication. The stations could focus on areas of social communication difficulty for both children with ASD and for children with language impairments (see Gerber, Brice, Capone, Fujiki, & Timler, 2012), who are likely to be in inclusion classrooms together. The SLP and classroom teacher should work together to identify areas of social communication to target based on the cohort of children in the classroom. Areas of focus may include verbal and nonverbal pragmatic skills (e.g., reading body language and facial expressions, making polite requests, taking turns when making comments, and providing polite feedback) and social communication situations (e.g., joining a conversation, working cooperatively, and resolving conflicts).
Complementary co-teaching involves one professional supporting differentiated instruction while the other provides the general classroom lesson (Heisler & Thousand, 2019). For example, the classroom teacher may be teaching the students a science lesson and the SLP may serve as the complementary co-teacher to explain figurative language, identify new or difficult vocabulary words, help the students to stop and think about what they are learning, and model ways for students to self-advocate when repeated instruction or further explanation is required (Heisler & Thousand, 2019).
Team co-teaching involves co-responsibility for teaching a class of students together (Heisler & Thousand, 2019). In the team co-teaching model, both professionals take responsibility for teaching all of the students in the classroom, not just the students on IEPs. SLPs involved in co-teaching would plan all lessons together with the co-teacher and may use supportive, parallel, or complementary co-teaching methods when teaching the students. In particular, the SLP can contribute to the lesson planning by recommending specific ways to target the goals of the children on IEPs while planning the lesson for the entire class together with the co-teacher (Heisler & Thousand, 2019).
Limitations and Conclusions
Interprofessional and interdisciplinary practice requires many resources (time and money related to service delivery and continuing education) in order to provide comprehensive and collaborative assessment and treatment (Archibald, 2017; Bauer et al., 2010; Gotham, Bishop, & Lord, 2011). Baker, Egan-Lee, Martimianakis, & Reeves (2011) interviewed nurses, OTs, pharmacists, PTs, SLPs, and social workers regarding the collaboration of health care. Results indicated that “inappropriate consultations” may result from professionals who do not understand each other’s roles and scopes of practice.
Research investigating the clinical effectiveness of interprofessional practice compared to other models of collaboration (e.g., multidisciplinary and interdisciplinary) is limited (Archibald, 2017; Cirrin et al., 2010). Available studies tend to focus on the explanation of service delivery approaches rather than fidelity measures and effectiveness outcomes (Bruce & Bashinski, 2017; Ogletree, 2017; Pfeiffer et al., 2019). Professionals who practice collaboratively need to demonstrate clinical competence in their professional area of expertise, knowledge of the professional scope of practice of their team members, openness to inquiry and collaborative problem-solving, frequent communication among team members, and a focus on caring for optimal client/patient/student outcomes (Ogletree, 2017). Clinical SLPs are encouraged to use reason-based practice and local outcomes data to inform clinical decision-making, in the absence of available evidence to inform best practice regarding models of collaboration (Archibald, 2017; Cirrin et al., 2010).
Interprofessional practice and best practice are likely to become more synonymous in the coming decade. ASHA has created a 2018–2025 initiative to increase interprofessional education, practice, and research in the fields of speech-language pathology and audiology. ASHA has adopted the World Health Organization definition of interprofessional collaborative practice (IPP; WHO, 2010). ASHA’s definition of IPP is “when multiple service providers from different professional backgrounds provide comprehensive healthcare or educational services by working with individuals and their families, caregivers, and communities- to deliver the highest quality of care across settings” (ASHA practice portal, n.d.). The focus of IPP is not on one professional field but on collaboration across disciplines, in all settings. Clinicians and researchers working in the field of ASD are well suited for excellence in interprofessional practice and with further research, current effective collaborative clinical practice models for youth with ASD are likely to inform future best practice in the fields of speech-language pathology, occupational therapy, physical therapy, education, psychology, and more.
References
Alexander, M. G. F., & Leather, R. C. (2013). Parents' perspectives on appropriate sports programs for children with autism spectrum disorders. Palestra, 27(4), 20–24.
Alli, A., Abdoola, S., & Mupawose, A. (2015). Parents’ journey into the world of autism. South African Journal of Child Health, 9(3), 81–84.
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.). Washington, DC: Author.
American Speech-Language-Hearing Association. (2016). Scope of practice in speech-language pathology [Scope of Practice]. www.asha.org/policy.
American Speech-Language-Hearing Association. (n.d.). Interprofessional education/interprofessional practice. https://www.asha.org/Practice/Interprofessional-Education-Practice/
Archibald, L. M. (2017). SLP-educator classroom collaboration: A review to inform reason-based practice. Autism & Developmental Language Impairments, 2, 1–17.
Baker, L., Egan-Lee, E., Martimianakis, M. A., & Reeves, S. (2011). Relationships of power: implications for interprofessional education. Journal of Interprofessional Care, 25(2), 98–104.
Bauer, K. L., Iyer, S. N., Boon, R. T., & Fore, C. (2010). 20 ways for classroom teachers to collaborate with Speech-Language Pathologists. Intervention in School and Clinic, 45, 333–337.
Betancur, C. (2011). Etiological heterogeneity in autism spectrum disorders: More than 100 genetic and genomic disorders and still counting. Brain Research, 1380, 42–77.
Binns, A. V., & Oram Cardy, J. (2019). Developmental social pragmatic interventions for preschoolers with autism spectrum disorder: A systematic review. Autism & Developmental Language Impairments, 4(1), 1–18.
Bruce, S. M., & Bashinski, S. M. (2017). The trifocus framework and interprofessional collaborative practice in severe disabilities. American Journal of Speech-Language Pathology, 26(2), 162–180.
Cirrin, F. M., Schooling, T. L., Nelson, N. W., Diehl, S. F., Flynn, P. F., Staskowski, M., et al. (2010). Evidence-based systematic review: Effects of different service delivery models on communication outcomes for elementary school-age children. Language, Speech, and Hearing Services in Schools, 41, 223–264.
Davidson, M. M., & Ellis Weismer, S. (2014). Characterization and prediction of early reading abilities in children on the autism spectrum. Journal of Autism and Developmental Disorders, 44(4), 828–845.
Dynia, J. M., Bean, A., Justice, L. M., & Kaderavek, J. N. (2019). Phonological awareness emergence in preschool children with autism spectrum disorder. Autism & Developmental Language Impairments, 4, 1–15.
Gerber, S., Brice, A., Capone, N., Fujiki, M., & Timler, G. (2012). Language use in social interactions of school-age children with language impairments: An evidence-based systematic review of treatment. Language, Speech, and Hearing Services in Schools, 43, 235–249.
Gotham, K., Bishop, S. L., & Lord, C. (2011). Diagnosis of autism spectrum disorders. In D. Amaral, D. Geshwind, & G. Dawson (Eds.), autism spectrum disorders (pp. 30–43). New York: Oxford University Press.
Hayward, L. M., Fragala-Pinkham, M., Johnson, K., & Torres, A. (2016). A community-based, adaptive soccer program for children with autism: Design, implementation, and evaluation. Palaestra, 30(4), 44–50.
Heisler, L. A., & Thousand, J. S. (2019). A guide to co-teaching for the SLP: A tutorial. Communication Disorders Quarterly, 1–6.
Hollenbeck, A. F. (2007). From IDEA to implementation: A discussion of foundational and future responsiveness-to-intervention research. Learning Disabilities Research & Practice 22(2), 137–146.
Individuals with Disabilities Education Improvement Act (IDEA) of 2004, PL 108–446, 20 USC §§ 1400 et seq.
Johnson, A. (2016). Interprofessional education and interprofessional practice in communication sciences and disorders: An introduction and case-based examples of implementation in education and health care settings. Rockville, MD: American Speech-Language-Hearing Association. Retrieved from https://www.asha.org/uploadedFiles/IPE-IPP-Reader-eBook.pdf.
Justice, L. M., McGinty, A., Guo, Y., & Moore, D. (2009). Implementation of responsiveness to intervention in early education settings. Seminar in Speech Language Pathology, 30, 59–74.
Kasari, C., Brady, N., Lord, C., & Tager-Flusberg, H. (2013). Assessing the minimally verbal school-aged child with autism spectrum disorder. Autism Research, 6(6), 479–493.
Kjelgaard, M. M., & Tager-Flusberg, H. (2001). An investigation of language impairment in autism: Implications for genetic subgroups. Language and Cognitive Processes, 16(2–3), 287–308.
Koegel, R. L., Werner, G. A., Vismara, L. A., & Koegel, L. K. (2005). The effectiveness of contextually supported play date interactions between children with autism and typically developing peers. Research and Practice for Persons with Severe Disabilities, 30(2), 93–102.
Koegel, L. K., Koegel, R. L., Ashbaugh, K., & Bradshaw, J. (2014). The importance of early identification and intervention for children with or at risk for autism spectrum disorders. International Journal of Speech-Language Pathology, 16(1), 50–56.
Lanter, E., & Watson, L. R. (2008). Promoting literacy in students with ASD: The basics for the SLP. Language, Speech, and Hearing Services in Schools., 39(1), 33–43.
Leach, D. (2018). Using multi-tiered systems of support for students with autism spectrum disorders in inclusive classrooms. Journal of the Division on Autism and Developmental Disabilities, 5(1), 6–17.
McConkey, R., Dowling, S., Hassan, D., & Menke, S. (2013). Promoting social inclusion through Unified Sports for youth with intellectual disabilities: A five-nation study. Journal of Intellectual Disability Research, 57(10), 923–935.
McGregor, K. K., Berns, A. J., Owen, A. J., Michels, S. A., Duff, D., Bahnsen, A. J., et al. (2012). Associations between syntax and the lexicon among children with or without ASD and language impairment. Journal of Autism and Developmental Disorders, 42(1), 35–47.
Ogletree, B. T. (2017). Addressing the communication and other needs of persons with severe disabilities through engaged interprofessional teams: Introduction to a clinical forum. American Journal of Speech-Language Pathology, 26(2), 157–161.
Orsmond, G. I., Krauss, M. W., & Seltzer, M. M. (2004). Peer relationships and social and recreational activities among adolescents and adults with autism. Journal of Autism and Developmental Disorders, 34(3), 245–256.
Ozonoff, S., Iosif, A. M., Baguio, F., Cook, I. C., Hill, M. M., Hutman, T., … & Steinfeld, M. B. (2010). A prospective study of the emergence of early behavioral signs of autism. Journal of the American Academy of Child & Adolescent Psychiatry, 49(3), 256–266.
Pelphrey, K. A., Shultz, S., Hudac, C. M., & Vander Wyk, B. C. (2011). Research review: Constraining heterogeneity: The social brain and its development in autism spectrum disorder. Journal of Child Psychology and Psychiatry, 52(6), 631–644.
Pfeiffer, D. L., Pavelko, S. L., Hahs-Vaughn, D. L., & Dudding, C. C. (2019). A national survey of speech-language pathologists’ engagement in interprofessional collaborative practice in schools: Identifying predictive factors and barriers to implementation. Language, Speech, and Hearing Services in Schools, 50(4), 639–655.
Prelock, P. A., & McCauley, R. J. (2012). Treatment of Autism Spectrum Disorders. Baltimore: Brooks Publishing.
Tager-Flusberg, H., & Joseph, R. M. (2003). Identifying neurocognitive phenotypes in autism. Philosophical Transactions of the Royal Society of London. Series B: Biological Sciences, 358(1430), 303–314.
Tracy-Bronson, C. P., Causton, J. N., & MacLeod, K. M. (2019). Everybody has the right to be here: Perspectives of related service therapists. International Journal of Whole Schooling, 15(1), 132–174.
Wagner, A. L., Wallace, K. S., & Rogers, S. J. (2014). Developmental approaches to treatment of young children with autism spectrum disorder. Handbook of Early Intervention for Autism Spectrum Disorders (pp. 393–427). New York, NY: Springer.
Wilkinson, K. M. (Ed.). (2017) Clinical forum: Interprofessional collaborative practices in service delivery for individuals with severe disabilities [Special issue]. American Journal of Speech Language Pathology, 26(2).
Wong, C., Odom, S. L., Hume, K. A., Cox, A. W., Fettig, A., Kucharczyk, S., … & Schultz, T. R. (2015). Evidence-based practices for children, youth, and young adults with autism spectrum disorder: A comprehensive review. Journal of autism and developmental disorders, 45(7), 1951–1966.
World Health Organization. (2010). Framework for action on interprofessional education and collaborative practice. World Health Organization.
World Health Organization. (2013). Interprofessional collaborative practice in primary health care: nursing and midwifery perspectives: six case studies. Human Resources for Health Observer, 13, 1–24.
Acknowledgement
Thank you to Kristine Philbin, OT, OTR, MS for contributing examples of clinical collaborations including occupational therapy and speech-language pathology services.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Appendices
Appendix A
Resources to further your study of speech-language pathology interprofessional practice service coordination for individuals with autism spectrum disorder:
ASHA Interprofessional Practice Resources
-
Video about interprofessional practice service coordination for students with autism spectrum disorders: https://www.scsha.net/asha-ipp-autism-spectrum-disorders
-
Interprofessional practice case vignette of a kindergartener with autism spectrum disorder: https://www.asha.org/uploadedFiles/Kindergarten-ASD-Vignette.pdf
-
Interprofessional practice case rubric for a kindergartener with autism spectrum disorder: https://www.asha.org/uploadedFiles/Kindergarten-ASD-Rubric.pdf
-
American Journal of Speech-Language Pathology (Wilkinson, 2017) clinical forum on interprofessional collaborative practice for individuals with severe disabilities, including those with ASD and co-occurring conditions (e.g., intellectual disability): https://pubs.asha.org/toc/ajslp/26/2.
Appendix B
Case Examples
Case Collaboration Example 1: Cooking Group
Once a week, three middle-school-age boys with autism participated in a cooking group. The boys attended their local public middle school with IEPs and were learning in a sub-separate classroom with minimal to no inclusion time with peers learning in general education classrooms. The speech-language pathologist, occupational therapist, and special education teacher joined the three boys weekly for a cooking group, to work collaboratively on communication, activities of daily living, and academic goals. The cooking supplies and materials were set up in order to facilitate communication, fine motor development, sensory regulation, and learning of mathematical concepts. One set of measuring cups was shared so that the students had opportunities to practice making verbal requests to peers and teachers. A variety of ingredients were measured, poured, and stirred to encourage bilateral hand skills, tolerance to sensory experiences, and self-regulation during the group. Ingredients were measured and counted to encourage mathematical practices. The SLP, OT, and special education teacher were all responsible for supporting the students and collaborated to ensure that each goal area was addressed during each cooking group session.
Case Collaboration Example 2: Executive Summary Cards
In a public school with a specialized unit for children on the autism spectrum, maladaptive behaviors increased when regular staff members were absent and substitutes were in the classroom. The substitute teachers often felt overwhelmed, and complained that they could not easily find the information needed to follow the behavior plans on the students’ IEPs because it was buried in password-protected online systems and/or lengthy printed IEP documents. The special education teachers, occupational therapist, speech language pathologist, and behavioral specialist collaborated to create an “Executive Summary” for each student, formatted in an easy to follow bulleted list, including pictures of the students, successful behavior strategies with specific phrasing, triggers, and behaviors to watch for (e.g., running away or hair-pulling). Each student’s individual schedule was also included in the one-page executive summary. The executive summary was then kept in a special folder for substitutes, which they could access and take with them for the day. The executive summary also facilitated increased communication and collaboration among team members after the team came together to create cards for each child.
Appendix C
Once a week, three middle-school-age boys with autism participated in a cooking group. The boys attended their local public middle school with IEPs and were learning in a sub-separate classroom with minimal to no inclusion time with peers learning in general education classrooms. The speech-language pathologist, occupational therapist, and special education teacher joined the three boys weekly for a cooking group, to work collaboratively on communication, activities of daily living, and academic goals. The cooking supplies and materials were set up in order to facilitate communication, fine motor development, sensory regulation, and learning of mathematical concepts. One set of measuring cups was shared so that the students had opportunities to practice making verbal requests to peers and teachers. A variety of ingredients were measured, poured, and stirred to encourage bilateral hand skills, tolerance to sensory experiences, and self-regulation during the group. Ingredients were measured and counted to encourage mathematical practices. The SLP, OT, and special education teacher were all responsible for supporting the students and collaborated to ensure that each goal area was addressed during each cooking group session.
In a public school with a specialized unit for children on the autism spectrum, maladaptive behaviors increased when regular staff members were absent and substitutes were in the classroom. The substitute teachers often felt overwhelmed, and complained that they could not easily find the information needed to follow the behavior plans on the students’ IEPs because it was buried in password-protected online systems and/or lengthy printed IEP documents. The special education teachers, occupational therapist, speech language pathologist, and behavioral specialist collaborated to create an “Executive Summary” for each student, formatted in an easy to follow bulleted list, including pictures of the students, successful behavior strategies with specific phrasing, triggers, and behaviors to watch for (e.g., running away or hair-pulling). Each student’s individual schedule was also included in the one-page.
Rights and permissions
Copyright information
© 2020 Springer Nature Switzerland AG
About this chapter

Cite this chapter
Wisman Weil, L. (2020). Coordinating Speech-Language Pathology Services for Youth with Autism Spectrum Disorder. In: McClain, M., Shahidullah, J., Mezher, K. (eds) Interprofessional Care Coordination for Pediatric Autism Spectrum Disorder. Springer, Cham. https://doi.org/10.1007/978-3-030-46295-6_16
Download citation
DOI: https://doi.org/10.1007/978-3-030-46295-6_16
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-46294-9
Online ISBN: 978-3-030-46295-6
eBook Packages: Behavioral Science and PsychologyBehavioral Science and Psychology (R0)