
Abstract
The aims of this study were to examine speech-language pathologists’ (SLPs) knowledge and consideration of factors found in research when making clinical decisions regarding AAC for children with Autism Spectrum Disorder (ASD), and to reveal additional factors identified based on SLPs’ clinical practice. A 20-question mixed-methods survey was completed internationally by 187 certified SLPs. Overall, SLPs showed some familiarity with the research and considered factors found in research when making clinical decisions. SLPs also identified 20 factors that were not identified in the most recent systematic review that may predict, moderate, and/or mediate outcomes. This information may contribute to advancing clinical services regarding AAC as well as guide future research investigating the mechanisms by which children with ASD respond to AAC interventions.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Autism spectrum disorder (ASD) is a lifelong neurodevelopmental disorder that presents along a continuum with respect to each individual’s strengths and difficulties where some individuals use little to no functional speech, while others do not exhibit spoken language difficulties, resulting in a heterogeneous population (American Psychiatric Association 2013). This variability is also observed in children’s responses to early intervention, with as many as 30% of children with ASD not developing functional speech, even after receiving early intervention (Rose et al. 2016; Tager‐Flusberg and Kasari 2013). The ability to produce multiword combinations spontaneously and regularly before the age of five has been identified to be the strongest prognostic indicator for long-term outcomes, academic achievement, and social functioning (McEachin et al. 1993; Venter et al. 1992). For children who are at risk of not developing functional speech before the age of five, it is critical that they receive early, effective communication intervention.
Speech-language pathologists (SLPs) play a central role in early intervention to support communication development in children who are minimally verbal. This often involves the use of augmentative and alternative communication (AAC) to supplement their speech and facilitate communication development. AAC refers to the use of strategies to supplement communication for individuals with communication disabilities (Beukelman and Mirenda 2005). These strategies can be classified as unaided systems, which do not require external devices (e.g., gestures and sign language), and aided systems, which require the use of devices that are external to the person (e.g., voice output, the Picture Exchange Communication System [PECS], communication boards). There is evidence that, overall, AAC has positive effects for children with ASD with regard to supporting functional communication development (e.g., requests) (Iacono et al. 2016). The National Autism Center (2017), however, completed a systematic review of empirical intervention literature published in peer-reviewed journals from 2007 to 2012, examining the effectiveness of a broad range of interventions for individuals with ASD. The studies included in the review were evaluated based on their (a) research design, (b) measurement of the dependent variable, (c) measurement of the independent variable, (d) participant ascertainment, and (e) generalization and maintenance. The review categorized AAC research as having emerging evidence indicating some support but limited by the quality, quantity, and consistency of research findings. Taking into consideration that AAC interventions are typically designed for individuals with the most complex needs, achieving consistently large effect sizes across participants in multiple studies is a challenge, which may hamper AAC interventions in reaching a higher level of evidence (Iacono et al. 2016). Furthermore, given that the ASD population is highly heterogeneous, with a wide range of abilities and variability in outcomes, a key challenge in research and clinical practice alike is to explain why some children with ASD benefit from a given AAC intervention more than others. Such explanations could ultimately assist in determining which AAC intervention is best to administer to a particular child (Brady et al. 2004; Cafiero 2011).
To better understand the differential response to intervention, a set of terms are used in research to describe what works, for whom, and why. As outlined by Sievers et al. (2018), these factors fall broadly under the categories of predictors, moderators, and mediators. Predictors are baseline characteristics that have an uncorrelated main effect on outcomes, but no interactive effect between treatments (e.g., chronological age, general cognition) while moderators and mediators are factors associated with intervention outcomes. Both moderators and mediators provide an analysis of the possible mechanisms that contribute to therapy outcomes but differ how they associate to intervention outcomes. Moderators are pre-intervention characteristics that indicate a differential response to interventions (e.g., a higher level of a specific skill might be better suited to one form of AAC intervention over another) while mediators are factors measured during intervention that are associated with outcomes (e.g., frequency and duration of therapy, communication partner skills) (Papakostas 2008; Vivanti et al. 2014). Having a greater understanding of these variables will clarify variability and evidence-based decisions regarding the implementation of AAC interventions for children with ASD.
Currently, there is a small but growing body of research that has focused on examining factors that may predict, moderate, and mediate AAC outcomes for children with ASD. Ganz et al. (2012) completed a meta-analysis that examined potential predictors and their association with the PECS (Bondy and Frost 1994). The authors reported that younger children (i.e., preschool-age) and those who did not have an additional diagnosis (e.g., intellectual disability) demonstrated greater gains in functional communication (with larger effect sizes) following PECS intervention than children who were older and who had additional diagnoses. Flippin et al. (2010) completed a meta-analysis examining potential predicting factors (joint attention, object exploration, and verbal imitation) of PECS outcomes (Bondy and Frost 1994). Children whose initial levels of verbal imitation and object exploration were higher and displayed lower rates of joint attention at baseline demonstrated greater communication gains (i.e., requesting) following PECS. These reviews provide insight into potential predictors but are limited due to concentrating only on PECS, as opposed to the broader range of interventions available. Ganz et al. (2014), however, investigated the moderating effects of chronological age, the presence/absence of an intellectual disability, and the mediating effects of the intervention setting for three AAC interventions: speech-generating devices (SGDs), PECS, and other picture-based communication systems. Children without a comorbid intellectual/developmental disorder were reported to have made larger gains with the SGDs, whereas PECS was more effective for children with ASD and a diagnosis of comorbid intellectual/developmental disorder. A limitation of this review was its reliance on secondary analysis and the focus on broad potential moderators (e.g., children’s cognition, chronological age) versus moderators that may provide insight into the mechanisms underpinning differential response such as joint attention and object exploration. Sievers et al. (2018) completed a systematic review of AAC intervention studies utilizing group-based longitudinal and experimental designs across AAC modalities in which potential predictors, moderators, and mediators of intervention outcomes were examined and reported as part of the original study design. The factors identified to potentially predict responses to AAC interventions were cognitive ability, ASD characteristics, language comprehension, language use, and communication competence, as well as combinations of these factors examined via composite measures. Joint attention, object exploration, and verbal imitation were found to have a potential moderating role, whereas potential mediating factors included frequency of AAC exposure, communication partner knowledge of AAC system, communication partner perception of AAC, and adult input at home.
Even though these research studies provided insight into potential factors that may explain differential responses to treatment, little is understood about the approach taken by SLPs regarding the use of different factors to guide their clinical decisions and their knowledge of the research on these factors. SLPs are trained to make clinical decisions within an evidence-based practice (EBP) framework (American Speech-Language Hearing Association 2007). Within the scope of AAC, EBP is defined by Schlosser and Raghavendra (2004, p. 3) as “…the integration of the best and current research evidence with clinical/educational expertise and relevant stakeholder perspectives, in order to facilitate decision about assessment and interventions that are deemed effective and efficient for a given direct stakeholders.” Whereas the utilization of all three sources of information is recommended, there is little evidence regarding the sources of information accessed by clinicians when making decisions regarding AAC interventions for children with ASD. Furthermore, although research evidence is critical to EBP, so too are the insights clinicians gain through clinical experience. To date, research aimed at identifying predictors, mediators, and moderators of AAC intervention outcomes for children with ASD has focused on evidence derived in research settings. Not only is it not clear to what extent clinicians know of and use this information, it is also not clear what other factors they may identify as relevant based on their own clinical experience.
Given the challenges associated with selecting interventions for children with ASD, it is relevant from both a clinical and research perspective to examine how SLPs make evidence-based decisions regarding the treatments they provide. Thus, the aims of this study were to (a) examine what sources of information SLPs access when making AAC intervention decisions; (b) identify factors that SLPs think predict, moderate, and mediate AAC intervention outcomes; (c) examine SLPs’ level of familiarity with and consideration of the research evidence for factors that may predict, moderate, and mediate communication outcomes for children provided with AAC interventions; and (d) examine SLPs’ views regarding priorities for future research regarding factors that may predict, moderate, and mediate communication outcomes for children with ASD receiving AAC interventions.
Method
Research Design
A 20-question online survey was used to address the research aims regarding SLPs’ knowledge and consideration of factors that may predict, moderate, and mediate AAC outcomes for children with ASD. The study was approved by the Griffith University research ethics committee.
Survey Tool
The survey was developed and hosted on Qualtrics, an online survey software service. Before distribution, the survey was pilot-tested by a certified SLP to obtain feedback regarding flow, interpretability, ambiguous questions, as well as to check the response burden. The survey completion time was estimated to be 15-min based on piloting. The final survey consisted of the following sections: (a) demographics; (b) sources of information that clinicians access when making AAC decisions; (c) factors identified by clinicians that guide decisions regarding AAC intervention; (d) SLPs’ level of familiarity with the factors identified in research; (e) SLPs’ consideration of the factors found in research when making AAC decisions; and (f) priority areas for future research as identified by clinicians.
Each section of the survey related to one study aim. If a participant did not complete a question, s/he was unable to continue with the next section of the survey. The first section comprised multiple-choice and open-ended questions to obtain information regarding (a) years of experience, (b) professional affiliations [e.g., American Speech-Language-Hearing Association (ASHA); Speech-Language & Audiology Canada (SAC); Speech Pathology Australia (SPA)], (c) academic degrees completed (e.g., bachelors, masters), and (d) the sources of information (e.g., other SLPs, AAC blogs, coursework, or assessments used) that guide SLPs’ clinical decision-making regarding AAC.
Section two included questions regarding factors that may explain the differential response to AAC intervention, specifically (a) open-ended questions about SLP’s insights around predictors, moderators, and mediators, and (b) closed-ended questions regarding their knowledge of, familiarity with, and consideration of the available research around these concepts. As the terms predictor, moderator, and mediator might not have been familiar to the participants; the researcher rephrased these terms in ways that may reflect the way they are applied in clinical settings. Predictors were operationalized as “things about the child, family, or environment that impact intervention outcomes, irrespective of which AAC intervention is used;” moderators as “things about the child, family, or environment that impact outcomes for one AAC intervention (e.g., PECS) more so than for another (e.g., communication board);” and mediators as “things about the child, family, or environment that are happening during an intervention that impact AAC outcomes.” The participating SLPs were first presented with open-ended questions regarding factors identified through their own practice so as to not to prime them to possible factors found in research (i.e., the focus of subsequent questions). Likert scales were used to assess SLPs’ familiarity, from 1 (very familiar) to 4 (no familiarity), and consideration, from 1 (frequently consider) to 4 (never consider), of factors found in research. In the final section, SLPs were asked to identify priorities for future research by way of multiple-choice questions. These factors were based on a systematic review by Sievers et al. (2018). To obtain a copy of the survey, please contact the first author.
Participants
To be included in this study, participants were required to be certified SLPs who had experience working with children with ASD and AAC interventions, based on self-report. Responses to survey questions regarding experience as an SLP working with AAC were used to automatically exclude participants who did not meet the study’s inclusion criterion at the start of the survey. A total of 237 people accessed the survey, of whom 203 met eligibility criteria as indicated by their responses with 187 SLPs continuing past the inclusion criteria questions. Participants were recruited through emails distributed via professional organizations in Australia, the United States, Canada, the United Kingdom, Ireland, and New Zealand. No forms of compensation or incentives were provided. Participant experience in working with children with ASD ranged from < 1 year to 40 years, and 79% held post-graduate qualifications (e.g., Masters, Ph.D.), with those with bachelor’s degrees reflecting different requirements for certification across countries. The average amount of experience was 12.64 years. Demographic information is presented in Table 1.
Procedure
An advertisement was distributed with the assistance of speech-language pathology professional organizations (i.e., ASHA, SAC, SPA) through their respective networks, online community message boards for SLPs (e.g., AAC for SLPs), and through the research team’s professional networks. Through these channels, participants accessed a secure web-link that directed them to a participant information statement explaining the study, the inclusion criteria for participation, and what would be asked of them as participants. Informed consent was obtained from all individual participants included in the study via an online consent form. The survey was active for 6 weeks.
Data Analysis
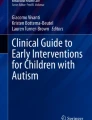
Data from the surveys was first exported to Microsoft Excel and was analyzed using both qualitative and quantitative approaches. The qualitative data from the open-ended questions regarding factors SLPs believed to predict, moderate, and mediate AAC outcomes for children with ASD were read, categorized, and analyzed using a general inductive analysis approach (Thomas 2006). Categories were developed by the systematic reading and interpretations of the open-ended responses. The first author grouped responses into 45 meaning units (e.g., vocabulary, vision) according to related words, phrases, and previous factors found in the research (Hsieh and Shannon 2005; Thomas 2006). The meaning units were then reduced into larger categories (e.g., AAC display design, comorbidities) by combining units that shared concepts for readability and usability (Graneheim and Lundman 2004). The process resulted in a total of 27 categories (Fig. 1).

General inductive analysis approach: coding example
To assess the reliability of the data analysis, a doctoral SLP candidate who had experience with AAC independently coded the data. The SLP was given the list of the 45 meaning units and then asked to code the first 20% of the responses from an Excel spreadsheet, resulting in the agreement of 80.5%. The discrepancies between the first author and the coder were primarily due to the coder assigning multiple-meaning units to one data set, while the first author assigned only one, and vice versa. The independent coder was given a condensed list of the 27 categories with corresponding meaning units and reported 100% agreement with the categorization.
Quantitative data analysis, involving the use of descriptive statistics, was used to identify means, ranges, and percentages for questions related to responses regarding demographics, resources accessed, level of knowledge and consideration of factors, and future research priorities.
Results
A total of 187 SLPs met the inclusion criteria and completed the demographics section. Out of the 187 participating SLPs, a total of 49.73% completed the main components of the survey (knowledge and consideration of factors that may predict, moderate, and mediate outcomes) and 38.50% completed the entire survey, which included questions on priorities for future research. For each survey question, all responses were analyzed, and percentages were calculated based on the mean number of participants who had completed that section.
An independent samples T test and Chi square test were conducted to determine if there were differences in those SLPs who completed the main survey section (SLP insights) and those who did not based on years of experience and highest level of education. There was no significant difference in years of experience between those who completed the open-end survey questions regarding clinical insights (M = 12.275 years, SD = 10.72) and those who did not (M = 12.88 years, SD = 11.79), t(157) = − 0.373, p = 0.71, nor was there an association with respect to highest level of education and completion of the survey, χ2(2) = 0.95, p = 0.68.
Sources of Information
SLPs were asked to identify sources of information they typically accessed to inform clinical decisions about AAC for children with ASD. As indicated in Table 2, the most prevalent sources reported were information from their own clinical experiences, AAC training/workshops, and other clinicians/colleagues. Research journals and university coursework were accessed less commonly than the other sources.
SLPs indicated that they assessed a variety of skills in children when making AAC decisions. The skills SLPs reportedly assessed the most were language [e.g., assessed using tools such as the Preschool Language Scales-5, (PLS-5); Zimmerman et al. 1997] (75.86%), AAC/functional language [e.g. assessed using tools such as the Functional Communication Profile, (FCP-R); Kleiman 2003] (68.70%) and play skills (53.91%), whereas fine/gross motor (24.14%), literacy (19.83%), and cognitive skills (12.07%) were assessed less often. They were also provided the opportunity to expand on these responses and added that they used informal observations, pragmatic checklists, and The Communication Matrix (Rowland 2011) to guide their practices (see Table 3).
Factors SLPs Identified That May Predict, Moderate, and Mediate AAC Outcomes
SLPs were asked to list factors they considered predict, moderate, and mediate AAC outcomes. A total of 31 factors were identified, 11 of which were related to potential factors found previously in research (e.g., general cognition, joint attention, frequency of AAC exposure) (Sievers et al. 2018). Additional factors that were revealed through analysis were communicative intent, having peers as AAC communicators, availability of clinical resources, motivation of child to use the AAC system, understanding the function of communication, pragmatics/social skills, SLP knowledge and skills related to AAC, access to a multidisciplinary team, and AAC display/features (see Table 4). The most frequently mentioned factors by SLPs were communication partner’s AAC skills (147), SLP’s AAC skills (72), access to an AAC system (78), and communication partner’s perception of AAC outcomes (57). In contrast, the following factors were mentioned fewer than five times: prelinguistic skills (3), imitation (3), pragmatics/social skills (3), function of communication (1), and peers as communication partners (4). It should be noted that we opted to keep the term prelinguistic as a separate category so as not to make inferences regarding which specific skills the SLPs were referring (e.g., joint attention, imitation). A total of 132 responses from 68 SLPs were classified as ambiguous due to the responses being vague or off-topic including stating their frustration with the AAC clinical decision-making process.
SLPs’ Level of Familiarity with the Research on Factors That May Predict, Moderate, and Mediate AAC Outcomes
SLPs rated their level of familiarity with the research (4-point Likert scale, from 1 = very familiar to 4 = no familiarity) regarding 13 factors identified by (Severs et al. (2018), that may predict, moderate, and mediate responses to AAC intervention. As presented in Table 5, 37.93% of the total responses indicated they were very familiar, 42.69% some familiarity, 15.19% very little familiarity, and 4.19% no familiarity with the research when summed across the 13 factors. The factors for which SLPs reported they had the greatest familiarity with the research were joint attention (M = 1.60), communication competence/complexity (M = 1.61), and frequency of AAC exposure (M = 1.61). By contrast, the factors with lower levels of familiarity were motor skills (M = 2.28), communication partner’s knowledge of AAC (M = 1.91), general cognitive ability (M = 2.13), and play skills/object exploration (M = 2.01).
SLPs’ Level of Consideration of Factors Found in Research That Predict, Moderate, and Mediate AAC Outcomes
To gain insight into the extent to which SLPs considered information from previous research in their practice, SLPs were asked to rank to what the extent they consider research pertaining to each factor when making clinical decisions, using a Likert scale from 1 = frequently consider to 4 = never consider. Out of the total SLP responses, 66.14% indicated they frequently considered, 23.57% sometimes considered, 8.05% rarely considered, and 2.24% never considered the research when summed across all 13 factors. Motor skills (M = 1.20) and communication competence/complexity (M = 1.25) had the highest ratings for consideration, while factors with lower average scores were play skills/object exploration (M = 1.96) and imitation (verbal) (M = 1.90) (see Table 6).
Priority for Future Research as Indicated by SLPs
To gain insight into what factors the SLPs believed warrant further research, they were again presented with a list of factors reported in previous research and asked to indicate the extent to which each was a priority for further research, using Likert scales (1 = high priority to 5 = not sure). The factors AAC input at home (M = 1.49) and frequency of AAC exposure (M = 1.55) were indicated to have higher levels of priority. Lower average priority ratings, albeit still relevant to practice, were imitation (verbal) (M = 2.67) and cognitive ability (M = 2.61) (see Table 7).
Discussion
Decision making regarding AAC interventions for children with ASD is a complex process due to the heterogeneity of the ASD population and the abundant array of AAC options. SLPs must integrate various information from skill assessments and parent reports as well as research evidence to make decisions, despite a general lack of evidence to inform SLPs on what works best for whom and why. Given SLPs are highly involved in the early intervention process and can provide insights that impact the provision of clinical service, both the previous research and clinical perspectives need to be considered. The results from this international online survey provide preliminary insights into the clinical applicability of factors found in research while capturing additional factors identified by SLPs that may influence AAC outcomes. Exploring insights from both perspectives has the potential to further enable SLPs to develop AAC interventions that are tailored and increasingly effective for children with ASD.
Sources of Information Accessed to Inform AAC Decisions
The SLPs in the study were asked to indicate the sources of information they accessed and children’s skills they assessed when making AAC intervention decisions. As expected, SLPs reportedly accessed various sources of information, across multiple domains, when making decisions regarding AAC interventions (Iacono and Cameron 2009). The most frequently accessed sources were SLPs’ own clinical experience, resources available in their clinics, and other clinicians/colleagues, whereas university coursework and research journals were indicated to be accessed relatively less. The finding of a tendency to rely on informal (e.g., other colleagues, own clinical experience) more so than research literature when making clinical decisions is consistent with longstanding previous research findings (McAlister et al. 1999; Nail-Chiwetalu and Ratner 2007). For example, Zipoli and Kennedy (2005) surveyed SLPs’ attitudes and utilization of EBP and found that SLPs predominantly relied on their own clinical experience and the opinions of colleagues over data from previous research when making clinical decisions.
Assessing children who may need AAC is not a straightforward process due to the complex nature of how children with ASD acquire language and the multitude of factors that could influence intervention outcomes including child-specific skills (e.g., levels of joint attention) and communication partner skills (e.g., amount of training). Currently, there is not a consistent AAC assessment framework that is used in practice to direct clinicians on what to specifically assess and how these results should dictate clinical decisions. The findings in this study regarding the skills SLPs assess provide insights into factors that may be relevant to assess and that may also influence AAC intervention outcomes. The skills that SLPs reported assessing most frequently to guide AAC decisions were children’s language, functional language using AAC, and play skills, with literacy and cognitive assessments reported as being assessed less often. The emphasis on assessing language was also highlighted in previous survey studies (Dietz et al. 2012). Dietz et al. (2012) reported that SLPs assessed specific skills (e.g., communication competence, auditory comprehension, motor skills, attention), and the SLPs in Lund’s (2017) study frequently discussed focusing on subthemes regarding communicative intent and pragmatic aspects of language when assessing language. Similar to the SLPs in the Dietz et al. (2012), the SLPs in this survey study indicated they also assessed language (75.65%) and AAC/Functional language (68.70%). However, direct comparisons between the current study and previous research regarding what specific communication skills assessed was not possible due to the survey design which did not enable researchers to ask follow-up questions. The opportunity for further inquiry could have provided clarity in relation to the responses of those SLPs who indicated they used “other assessments” (4.35%) or who noted assessing specific skills was “not applicable” (3.48%) to their clinical decision process.
Factors Explored in Research and SLP Identified Factors That May Predict, Moderate, and Mediate AAC Communication Outcomes
The SLPs in this survey were asked to list factors they thought contributed to how a child with ASD responded to AAC intervention and were then provided a list of factors found in previous research that have the potential to explain the differential responses. Overall, the SLPs self-reported having knowledge of, and considering, factors found in research that may influence differential responses to AAC interventions, which could indicate the positive transfer of research to a clinical context. SLPs also contributed numerous factors from their practice, many of which are currently being investigated in research.
Exploring SLPs’ perspectives illustrated the complexity of AAC and the multitude of factors that must be considered during design and implementation, as well as the child factors that must be considered. When SLPs were asked to offer their perspectives on factors that may help to explain outcomes from an AAC intervention, factors such as communication partners’ skills, SLP’s AAC skills, and communication partners’ perceptions of AAC outcomes received the most mentions. These factors, if adopting the definitions used by Sievers et al. (2018), would be classified as mediators. The attention SLPs placed on mediating factors was also a focus in the Likert Scale section, where, overall, a greater percentage of SLPs indicated they frequently considered mediators, as well as placing a high priority on mediating factors over predictor and moderating factors. Improving communication aims through everyday interaction is a goal of AAC, so the emphasis SLPs placed on mediating factors could explain the SLPs’ prioritizing of these factors. Numerous studies have investigated how to enhance meaningful participation and use of AAC systems (McNaughton et al. 2008), which could also contribute to the observation of higher levels of considering these factors, as well as the concentration of these factors in open-ended responses.
Factors that have the potential to predict differential responses to interventions (moderators) were regarded as contributing less. There is a growing emphasis in research on the potential value of on identifying fine-grain factors (e.g., joint attention, object exploration) that can predict differential responses to interventions (Sievers et al. 2018; Vivanti et al. 2014). Joint attention, a factor reported to moderate communication outcomes by Sievers et al. was in the top five factors that were indicated to be frequently considered, whereas, in the open-ended responses, it was only mentioned a total of ten times, one of the lowest rates. The discrepancy between higher levels of self-reported knowledge and consideration of factors versus what was reported in open-ended questions is consistent with findings in other studies. Sackett et al. (1991), for example, found that clinicians have knowledge of research, but, when questioned about their decision process, it was often not based on the best evidence. In specialist areas with emerging research, such as AAC, clinicians access the research but tend to rely on their own clinical experience (Meline and Paradiso 2003). While observations from SLPs may be significant, without evidence from research, it is challenging to develop theories to explain the mechanisms that explain how and why intervention had a positive effect (Meline and Paradiso 2003). Other contributing factors to higher levels of knowledge and consideration, but lower levels of utilization, could include (a) workplace restrictions (e.g., time to analyze research results, obstructions to alter existing practices, employers), (b) lack of skills to apply research directly to practice, and/or (c) a nominal level of clinical utility for these factors found in research (Cheung et al. 2013; Metcalfe et al. 2001; Reilly 2004; Schlosser and Sigafoos 2009; Upton and Upton 2006).
Limitations
This survey provides clinical insights regarding SLPs’ approach to AAC intervention on an international scale. However, this analysis comes with limitations. Completion rate of the full survey was relatively low, with only 49.73% completing questions regarding knowledge and consideration of factors and 38.50% of SLPs completing the entire survey. Most notably, this survey represents only a small percentage of practicing SLPs. Since the actual response rate is unknown, it may not be representative of SLPs’ views and experience across the board. Another limitation relates to the analysis of open-ended questions regarding participants’ acumen of factors that may predict, moderate, and mediate outcomes. Although AAC outcome variability is acknowledged, it is unlikely to be considered in the clinic using these terms. Despite providing plain-language definitions in the survey, these are complex concepts, and there is a potential for participant confusion. This could have been remedied through follow-up interviews and/or surveys to clarify the interpretation of the coding. Accordingly, our findings should be interpreted as a clinical inquiry as to provide direction for future research rather than taken as definitive.
Conclusion
The research around AAC intervention for children with ASD has grown over the past 30 years (Romski et al. 2015), with emphasis increasingly placed on the importance of identifying factors that help to account for differential response to intervention. Until now, there was little information regarding what SLPs know of this research, how it is utilized in practice, or which factors SLPs consider to be relevant from their own experience (Schlosser and Raghavendra 2004). The results of this survey provide an international perspective on SLPs’ knowledge and consideration of factors found in the research that may predict, moderate, and mediate responses to AAC interventions, as well highlighting factors that arise from their clinical practice. However, despite these developments, there still exists an overall lack of information to inform SLPs’ assessment and intervention for children with ASD using AAC, with respect to potential moderating and mediating factors.
Moving forward, identifying the mechanisms at play and how these factors can be applied to make decisions regarding which AAC interventions are more suitable for a specific child will take a concerted effort from both researchers and clinicians. SLPs, despite the paucity of the available evidence, should be encouraged to frame their AAC decision making, and share insights about factors that may influence outcomes, in terms of potential predictors, moderators, and mediators of outcomes. Framing factors such as skills, opportunities, and barriers using these terms will help to increase sharing and discussion in clinical contexts, with the potential to direct future research. Notably, the SLPs in this study placed an onus on mediating factors, highlighting factors such as communication partner AAC training and the benefits of having AAC support networks. Future research should utilize the insights drawn from SLPs’ own clinical experiences in conjunction with emerging research to produce clinically actionable results that could lead to positive communication gains.
References
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders: DSM-5 (Vol. 5). Washington, D.C: American Psychiatric Association.
American Speech-Language Hearing Association. (2007). Scope of practice in speech-language pathology. Retrieved 3 October, 2019 from www.asha.org/policy (Index terms: Scope of practice).
Beukelman, D. R., & Mirenda, P. (2005). Augmentative & alternative communication: Supporting children & adults with complex communication needs (Vol. 3). Baltimore: Paul H. Brookes Pub. Co.
Bondy, A., & Frost, L. (1994). PECS: The picture exchange communication system training manual. Cherry Hill, NY: Pyramid Educational Consultants.
Brady, N. C., Marquis, J., Fleming, K., & McLean, L. (2004). Prelinguistic predictors of language growth in children with developmental disabilities. Journal of Speech, Language, and Hearing Research,47(3), 663–677. https://doi.org/10.1044/1092-4388(2004/051).
Cafiero, J. M. (2011). Autism spectrum disorders and AAC. Focus on Autism and Other Developmental Disabilities,26(3), 184–186. https://doi.org/10.1177/1088357610394653.
Cheung, G., Trembath, D., Arciuli, J., & Togher, L. (2013). The impact of workplace factors on evidence-based speech-language pathology practice for children with autism spectrum disorders. International Journal of Speech-Language Pathology,15(4), 396–406. https://doi.org/10.3109/17549507.2012.714797.
Dietz, A., Quach, W., Lund, S. K., & McKelvey, M. (2012). AAC Assessment and clinical-decision making: The impact of experience. Augmentative and Alternative Communication,28(3), 148–159. https://doi.org/10.3109/07434618.2012.704521.
Flippin, M., Reszka, S., & Watson, L. R. (2010). Effectiveness of the picture exchange communication system (PECS) on communication and speech for children with autism spectrum disorders: A meta-analysis. American Journal of Speech-language Pathology/American Speech-Language-Hearing Association,19(2), 178–195. https://doi.org/10.1044/1058-0360(2010/09-0022).
Ganz, J., Davis, J., Lund, E., Goodwyn, F., & Simpson, R. (2012). Meta-analysis of PECS with individuals with ASD: Investigation of targeted versus non-targeted outcomes, participant characteristics, and implementation phase. Research in Developmental Disabilities,33(2), 406–418.
Ganz, J., Mason, R., Goodwyn, F., Boles, M., Heath, A., & Davis, J. (2014). Interaction of participant characteristics and type of AAC with individuals with ASD: A meta-analysis. American Journal on Intellectual and Developmental Disabilities,119(6), 516–535. https://doi.org/10.1352/1944-7558-119.6.516.
Graneheim, U. H., & Lundman, B. (2004). Qualitative content analysis in nursing research: Concepts, procedures and measures to achieve trustworthiness. Nurse Education Today,24(2), 105–112. https://doi.org/10.1016/j.nedt.2003.10.001.
Hsieh, H.-F., & Shannon, S. E. (2005). Three approaches to qualitative content analysis. Qualitative Health Research,15(9), 1277–1288. https://doi.org/10.1177/1049732305276687.
Iacono, T., & Cameron, M. (2009). Australian speech-language pathologists’ perceptions and experiences of augmentative and alternative communication in early childhood intervention. Augmentative and Alternative Communication,25(4), 236–249. https://doi.org/10.3109/07434610903322151.
Iacono, T., Trembath, D., & Erickson, S. (2016). The role of augmentative and alternative communication for children with autism: Current status and future trends. Neuropsychiatric Disease and Treatment,12, 2349–2361. https://doi.org/10.2147/NDT.S95967.
Kleiman, L. I. (2003). Functional communication profile-revised. East Moline, IL: LinguiSystems Inc.
Lund, S. K., Quach, W., Weissling, K., McKelvey, M., & Dietz, A. (2017). Assessment with children who need augmentative and alternative communication (AAC): Clinical decisions of AAC specialists. Language, Speech, and Hearing Services in Schools, 48(1), 56–68.
McAlister, F. A., Graham, I., Karr, G. W., & Laupacis, A. (1999). Evidence-based medicine and the practicing clinician. Journal of General Internal Medicine,14(4), 236–242. https://doi.org/10.1046/j.1525-1497.1999.00323.x.
McEachin, J. J., Smith, T., & Lovaas, O. I. (1993). Long-term outcome for children with autism who received early intensive behavioral treatment. American Journal of Mental Retardation,97(4), 359–372 (discussion 373–391).
McNaughton, D., Rackensperger, T., Benedek-Wood, E., Krezman, C., Williams, M. B., & Light, J. (2008). “A child needs to be given a chance to succeed”: Parents of individuals who use AAC describe the benefits and challenges of learning AAC technologies. Augmentative and Alternative Communication,24(1), 43–55. https://doi.org/10.1080/07434610701421007.
Meline, T., & Paradiso, T. (2003). Evidence-based practice in schools: Evaluating research and reducing barriers. Language, Speech, and Hearing Services in Schools,34(4), 273–283. https://doi.org/10.1044/0161-1461(2003/023).
Metcalfe, C., Lewin, R., Wisher, S., Perry, S., Bannigan, K., & Moffett, J. K. (2001). Barriers to implementing the evidence base in four NHS therapies. Physiotherapy,87(8), 433–441. https://doi.org/10.1016/S0031-9406(05)65462-4.
Nail-Chiwetalu, B., & Ratner, N. B. (2007). An assessment of the information-seeking abilities and needs of practicing speech-language pathologists. Journal of the Medical Library Association,95(2), 182-e157. https://doi.org/10.3163/1536-5050.95.2.182.
National Autism Center. (2017). National Standards Project, Phase 2. Retrieved from http://www.nationalautismcenter.org/national-standards-project/
Papakostas, G. I., & Fava, M. (2008). Predictors, moderators, and mediators (correlates) of treatment outcome in major depressive disorder. Dialogues in Clinical Neuroscience, 10(4), 439–451.
Reilly, S. (2004). The challenges in making speech pathology practice evidence based. Advances in Speech-Language Pathology,6(2), 113–124. https://doi.org/10.1080/14417040410001708549.
Romski, M., Sevcik, R. A., Barton-Hulsey, A., & Whitmore, A. S. (2015). Early intervention and AAC: What a difference 30 years makes. Augmentative and Alternative Communication,31(3), 181–202. https://doi.org/10.3109/07434618.2015.1064163.
Rose, V., Trembath, D., Keen, D., & Paynter, J. (2016). The proportion of minimally verbal children with autism spectrum disorder in a community-based early intervention programme. Journal of Intellectual Disability Research,60(5), 464–477. https://doi.org/10.1111/jir.12284.
Rowland, C. (2011). Using the communication matrix to assess expressive skills in early communicators. Communication Disorders Quarterly,32(3), 190–201. https://doi.org/10.1177/1525740110394651.
Sackett, D. L., Haynes, B., Guyatt, G. H., & Tugwell, P. (1991). Clinical epidemiology a basic science for clinical medicine (Vol. 12). London: Little & Brown.
Schlosser, R. W., & Raghavendra, P. (2004). Evidence-based practice in augmentative and alternative communication. Augmentative and Alternative Communication,20(1), 1–21. https://doi.org/10.1080/07434610310001621083.
Schlosser, R. W., & Sigafoos, J. (2009). Navigating evidence-based information sources in augmentative and alternative communication. Augmentative and Alternative Communication,25(4), 225–235. https://doi.org/10.3109/07434610903360649.
Sievers, S. B., Trembath, D., & Westerveld, M. (2018). A systematic review of predictors, moderators, and mediators of augmentative and alternative communication (AAC) outcomes for children with autism spectrum disorder. Augmentative and Alternative Communication, 34(3), 219–229.
Tager-Flusberg, H., & Kasari, C. (2013). Minimally verbal school-aged children with autism spectrum disorder: The neglected end of the spectrum. Autism Research,6(6), 468–478. https://doi.org/10.1002/aur.1329.
Thomas, D. R. (2006). A general inductive approach for analyzing qualitative evaluation data. American Journal of Evaluation,27(2), 237–246. https://doi.org/10.1177/1098214005283748.
Upton, D., & Upton, P. (2006). Knowledge and use of evidence-based practice by allied health and health science professionals in the United Kingdom. Journal of Allied Health,35(3), 127–133.
Venter, A., Lord, C., & Schopler, E. (1992). A follow-up study of high-functioning autistic children. Journal of Child Psychology and Psychiatry,33(3), 489–597. https://doi.org/10.1111/j.1469-7610.1992.tb00887.x.
Vivanti, G., Prior, M., Williams, K., & Dissanayake, C. (2014). Predictors of outcomes in autism early intervention: Why don’t we know more? Frontiers in Pediatrics,2, 58.
Zimmerman, I. L., Steiner, V., & Pond, R. E. (1997). Preschool language scales (3rd ed., UK end adapted by J. Boucher & V. Lewis ed.). London: Psychological Corporation.
Zipoli, R. P., Jr., & Kennedy, M. (2005). Evidence-based practice among speech-language pathologists: Attitudes, utilization, and barriers. American Journal of Speech-Language Pathology,14(3), 208–220. https://doi.org/10.1044/1058-0360(2005/021).
Acknowledgments
The authors thank the participants who shared their experience and expertise in this research. This study will form part of Stephanie Sievers doctoral dissertation.
Funding
David Trembath was supported by a National Health and Medical Research Council ECR Fellowship (GNT1071811).
Author information
Authors and Affiliations
Contributions
SBS, DT and MFW contributed to the study conception and design. Material preparation, data collection and analysis were performed by SBS under the supervision of DT and MFW. The first draft of the manuscript was written by SBS and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare no conflict of interest.
Ethical Approval
This study was approved by the Griffith University Human Ethics Committee (Ref: 2017/758).
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Sievers, S.B., Trembath, D. & Westerveld, M.F. Speech-Language Pathologists’ Knowledge and Consideration of Factors That May Predict, Moderate, and Mediate AAC Outcomes. J Autism Dev Disord 50, 238–249 (2020). https://doi.org/10.1007/s10803-019-04217-4
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10803-019-04217-4