
Abstract
Single Nucleotide Polymorphisms (SNPs) is the substitution of a single nucleotide, stably inherited, highly abundant, and distributed throughout the genome. Up today 9746 SNPs were found in the HPSE gene. During 12 years 21 SNPs were analyzed in normal and pathological samples. The most prominent SNPs are rs4693608, rs11099592, rs4693084, and rs4364254. These SNPs were found in correlation with heparanase mRNA and protein expression among healthy persons. Moreover, an association of the HPSE gene SNPs with inflammatory processes, cancer development and progression was detected. SNP investigation allowed the identification of strong HPSE gene enhancer in the intron 2. In normal leukocytes, heparanase binds to the enhancer region and regulates HPSE gene expression via negative feedback in rs4693608 SNP-dependent manner. In malignant cells, heparanase halted self-regulation of the enhancer region. Instead of heparanase, the helicase-like transcription factor (HLTF) binds to the regulatory region. These and subsequent studies will elucidate how modification in the HPSE enhancer region could be applied to develop new approaches for cancer treatment.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others
Keywords
1 The HPSE Gene SNPs Characterization, Distribution, and Linkage Disequilibrium
According to the definition of SNP, the frequency of such polymorphism is greater than 1%, in at least one population. SNPs are located in different regions of genes such as promoters, exons, introns, and 5′ and 3′ untranslated regions (UTR) and may affect gene expression and regulation. Thereby, SNPs contribute to disease susceptibility, various responses to medication treatment and differences in outcomes within a disease population [8, 9].
Ninety percent of all human variations are SNPs, which appear every 300 bp. Majority of nucleotide substitutions are C to T as a result of easy deamination of C nucleotide. SNPs are useful tools in various aspects of molecular biology, anthropology, and history. Polymorphisms may help to investigate population genetics, tracing of migration, human evolution, and tolerance to different enzymes. SNPs are good genetic markers when correlated with disease phenotype, are located in known genes and are linked to the disease-caused mutations [8, 16]. In common complex diseases, SNPs may help to identify genes or loci that contribute to disease susceptibility. Genetic association studies are the primary method for analysis of the effect of SNPs on disease outcomes [9, 52].
Identification of functional SNPs, including those of heparanase, among healthy persons, allows elucidating the normal functions of a gene in various activated and non-activated cells and involvement of the protein encoded by this gene in normal processes [2]. Functional SNPs take part in pathological processes such as cancer development and progression, acute and chronic inflammation, resistance to treatments, and elevated risk of treatment complications [3]. Functional SNPs, which lead to high or low gene expression among healthy populations help to identify actual biological processes in comparison to studies performed with cell lines. Each cell line has a different cell and disease origin (for example, lymphoma cell lines originate from different types of lymphomas) and is derived from a different population (i.e., Caucasian or African populations). Overexpression or silencing of appropriate genes and treatment of cell lines with different reagents do not reflect what happened during disease development or treatment due to the exclusion of many factors and cells that are involved in a given process. The disadvantage of the SNP approach is the necessity to include a large number of subjects in each group and perform an accurate selection of each participant in the analyzed group.
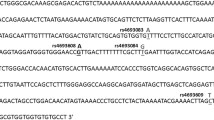
Up today 9746 SNPs were found in the HPSE gene. The frequencies of 1680 SNPs were determined. Five hundred and fifty-three SNPs are located in coding regions, and 71 SNPs have a double hit. The first characterization of the HPSE gene SNPs was performed by us in 2006 in four Israeli Jewish populations [38]. During 12 years 21 SNPs were analyzed in normal and pathological samples. Figure 8.1 shows all SNPs, which were investigated in different studies. The most prominent SNPs are marked in bold. The frequencies of the HPSE gene SNPs differed between Jewish and non-Jewish populations, excluding a partial similarity between Caucasian and Israeli populations [40]. It should be noted that Japanese, Chinese, and Sab-Saharan Africans differ from Caucasians in these SNPs (Table 8.1 according to NCBI SNPs database, http://www.ncbi.nlm.nih.gov/projects/SNP/).

HPSE gene SNPs map. Numbered boxes represent the 12 exons. Filled boxes represent open reading frame, and open boxes represent the 5′- and 3′-untranslated regions. The most prominent SNPs were marked in bold. Arrows show the locations of SNPs. Red brackets represent a block area
Detailed examination of linkage disequilibrium (LD) among all analyzed SNPs showed the presence of two blocks [40] (Fig. 8.1). These data were congruent with the information regarding the HPSE gene in Haploviewer and Ensemble genome browser. The first block includes SNPs from rs4693612 to rs11099592 and the second block starts from SNP rs6856901. The most prominent SNP rs4693608, located in intron 2 and included in the first block, was found in LD with the other SNPs in spite of the presence of two blocks. Analysis of SNPs that form an anchor of the association revealed that the combination of two SNPs rs4693608 and rs4364254 significantly correlates with heparanase mRNA and protein expression. Polymorphism rs4364254 is located in intron 9 between the two LD blocks. In this genotype combination, the rs4693608 SNP is the leading polymorphism. The rs4364254 SNP helps to identify heterozygote AG individuals with low mRNA HPSE expression levels (AG-CC genotype) [40].
Our more recent study [43] shows that a region in intron 2 of the HPSE gene exhibits enhancer activity in both the sense and antisense directions (chr4: 84,241,177-84,242,376). This region includes the most prominent rs4693608 SNP. Additional rs4693609, rs4693084, and rs4693083 SNPs are also located in the enhancer region. These SNPs were found in strong LD with rs11099594 (intron 2), rs6535455 (intron 4), and rs11099592 (intron 7) (Fig. 8.1). We genotyped additional SNP rs10034682, which is located in intron 3 (unpublished data) and found that this SNP is also in strong LD with 6 other SNPs (rs4693609, rs4693084, rs4693083, rs11099594, rs6535455, and rs11099592). According to the UCSC Genome Browser (http://genome.ucsc.edu/), additional putative enhancer is located in intron 3, and it is active in keratinocytes. NCBI SNPs database includes many other SNPs which were mapped in the first block and have the same allele frequencies as the above-mentioned polymorphisms among Caucasians. An association between rs11099592 and the risk of acute lymphoblastic leukemia (ALL) development [39], and poor outcome of gastric cancer [28, 58] was detected previously. Given the strong LD between rs11099592 with SNPs located in the enhancer regions, the observed disease associations may result from modification in the enhancer activity. According to EMSA and luciferase assays, rs4693084 may also affect the intron 2 HPSE gene enhancer activity [43]. The distance between rs4693608 and rs4693084 is only 17 bp, and under appropriate conditions both SNPs may be part of a common DNA/protein complex. Importantly, any of the 7 SNPs mentioned above may be a marker for SNP-associated studies. As a result of strong LD between SNPs in this region, identification of a causative SNP needs additional investigations.
2 Correlation Between the HPSE Gene SNPs and Heparanase Expression Among Healthy Individuals
Up today an association between the HPSE gene SNPs and heparanase expression was performed only among healthy Israeli population [40]. The known similarity in HPSE gene SNPs frequencies between Caucasians and Israeli Jewish populations allows assuming that the correlation between HPSE gene SNPs and heparanase expression also exists in the Caucasian population. Without SNP association analysis it is difficult to predict what happened in Asian and African populations as a result of different selection pressures (resource availability, environmental conditions, and biological factors) on various populations.
Our previous study [40] has demonstrated a significant correlation between at least five HPSE gene SNPs (rs4693608, rs11099594, rs6535455, rs11099592, rs4364254) and the expression level of heparanase, SNP rs4693608 being the most prominent. Haplotype analysis indicated the existence of significant differences between groups with relatively low and high heparanase expression levels. Notably, best results were obtained when the combination of two SNPs (rs4693608 and rs4364254) was assessed. This approach allowed distribution of all possible HPSE genotype combinations into three groups (LR, MR, and HR) correlating with low, intermediate and high heparanase mRNA and protein expression levels. Group LR included four genotype combinations (GG-CC, GG-CT, GG-TT, and GA-CC), while groups MR and HR included two genotype combinations each (GA-CT, GA-TT, and AA-TT, AA-CT, respectively). Genotype combinations were not casually distributed. These combinations were grouped according to the first SNP rs4693608, except the GA-CC genotype. Presumably, the A-C haplotype of the GA-CC genotype originates from single ancestor recombination between this variation and rs4693608 SNP and correlates with low levels of heparanase.
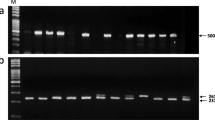
Although HPSE mRNA and plasma protein levels correlated with the same SNPs, an inverse association was observed [40]. For example, the rare genotype GG of rs4693608 SNP was associated with low HPSE mRNA expression level and high plasma heparanase concentration. In contrast, the frequent AA genotype of this SNP was associated with high HPSE mRNA expression and low plasma protein level. In this study mRNA expression was analyzed in total leukocytes of peripheral blood (PB). In another investigation [42] the correlation between rs4693608 and mRNA HPSE expression level was performed in mononuclear cells (MNC) from PB of healthy adults and umbilical cord blood (CB). Analysis of heparanase expression in resting MNC did not reveal differences among individuals with various HPSE gene genotypes in both PB and CB samples. We, therefore, assume that this type of correlation in resting leukocytes is restricted to neutrophils (Fig. 8.2A).

A model of the HPSE gene enhancer regulation in normal leukocytes (neutrophils) and LPS treated mononuclear cells. A. Normal cells. Heparanase binds to the enhancer region of intron 2 and regulates HPSE expression by negative feedback in rs4693608 SNP dependent manner. Additional molecules of heparanase bind to the enhancer region in carriers of allele G in comparison to possessors of allele A. As a result, the expression level of the HPSE gene will be higher in persons with genotype AA than in individuals with genotype GG. B. LPS-treated MNCs. LPS treatment leads to a decrease in the ability of heparanase to bind to the enhancer region and modify heparanase expression in rs4693608 SNP dependent manner. Possessors of the AA genotype disclose up-regulation of heparanase with high ratio in MNCs, while individuals with genotype GG showed non-responsiveness or down-regulation of the HPSE gene in response to LPS. C. PB and CB MNC with genotypes AA and GG were exposed to increasing concentrations of LPS for 18 h and relative quantification (RQ) of the HPSE gene expression was determined. MNC with the AA genotype exhibited up-regulation of the HPSE gene, while MNC with the GG genotype disclosed non-responsiveness to increasing amounts of LPS in both PB and CB samples. D. Effect of LPS on the ability of DNA/protein complexes to bind to the enhancer. LPS treatment resulted in disappearance of DNA/protein complexes in normal MNCs and decreased affinity of DNA/protein complexes in monocytic U937 cell line
The level of nuclear heparanase is also correlated with rs4693608 SNP [43]. It was higher in possessors of the GG genotype in comparison to carriers of the AA genotype. EMSA analysis of normal blood samples revealed the binding of a DNA/protein complex to both alleles with higher affinity to allele G (Fig. 8.2A). DNA pull-down assay followed by Western blot verification showed that heparanase binds to the enhancer region of intron 2 and regulates HPSE gene expression via negative feedback in rs4693608 SNP-dependent manner. This may explain an inverse correlation between HPSE gene SNPs and heparanase expression.
Heparanase is normally expressed in PB neutrophils, monocytes, macrophages, NK and activated T-lymphocytes. In cord blood, heparanase (both mRNA and protein) is expressed in neutrophils, monocytes, macrophages and NK cells. Heparanase expression in T and B lymphocytes is very low. The pattern of heparanase expression in cord blood NK cells differs from its expression in other hematopoietic cells. While in NK cells heparanase appears on the cell membrane in clusters and is widely expressed in the nucleus, in neutrophils and monocytes heparanase is more uniformly distributed on the cell membrane and is hardly detected in the cell nucleus [42].
Functional assay for NK cell activity revealed that susceptibility of Hela cells to lysis by fresh NK cells from different healthy persons correlates with rs4693608 and rs4364254 SNPs. Percent of specific lysis in individuals possessing HR genotype was higher (50.4%) in comparison to possessors of the MR (37.6%) and LR (23.3%) genotypes (p = 0.009). Moreover, treatment of NK cells with heparanase led to their increased cytotoxic ability. In contrast, HPSE gene silencing in NK92 cells resulted in low-efficiency killing of their K562 target cells as compared to control NK cells treated with non-specific siRNA (unpublished results).
3 HPSE Gene SNPs and Inflammation
The connection between inflammation and heparanase was first shown more than 20 years ago, prior to cloning of the heparanase gene, when HS-degrading activity was detected in immunocytes (neutrophils, activated T-lymphocytes) and found to contribute to their ability to extravasate and accumulate in target organs [30, 31, 53]. Up-regulation of heparanase in response to inflammatory and autoimmune stimuli was noted in various pathologies including arthritis [29], colitis [21, 27], autoimmune diabetes [61], sepsis [47] and experimental encephalomyelitis [30].
In our previous study [42] we tried to mimic the influence of the recipient pro-inflammatory milieu on heparanase expression in donor cells by stimulation of PB and CB MNC with LPS, revealing a significant increase in HPSE expression, which was mediated by TLR4. We found that heparanase expression is modified differently in MNC in accordance with their rs4693608 SNP genotype. Possessors of the AA genotype disclosed up-regulation of heparanase with high ratio in both PB and CB MNC, while individuals with genotype GG showed little or no responsiveness or down-regulation of the HPSE gene in response to LPS (Fig. 8.2B). PB and CB MNC with genotypes AA and GG were exposed to increasing concentrations of LPS, and relative quantification (RQ) of HPSE gene expression was determined. While MNC with the AA genotype exhibited up-regulation of the HPSE gene, MNC with the GG genotype disclosed non-responsiveness to increasing amounts of LPS in both PB and CB samples (Fig. 8.2C).
In a recent study [43] we analyzed the effect of LPS on the ability of DNA/protein complexes to bind to the strong HPSE gene intron 2 enhancer. LPS treatment resulted in disappearance of DNA/protein complexes in normal MNC and decreased affinity of DNA/protein complexes in U937 monocytic cells (Fig. 8.2D).
Pro-inflammatory genes can be regulated by epigenetic mechanisms such as methylation of gene regulatory regions or post-translational modification of histone proteins in chromatin [18]. Increase of methylated DNA decreases transcription factor-binding activity and affects promoter activity and gene transcription [44, 49]. Post-translational histone modifications alter the open or closed chromatin configurations [20]. The relaxed chromatin exposes DNA for transcription factor binding, leading to increased gene expression [56]. LPS treatment attenuates the ability of heparanase, in normal cells, and of the helicase transcription factor (HLTF), in malignant U937 cells, to bind the enhancer region and modify heparanase expression in rs4693608 SNP dependent manner [43].
Heparanase is involved in several inflammatory/autoimmune processes including leukocyte recruitment, immune cell extravasation and migration, release of HS-bound cytokines and chemokines and activation of innate immune cells [54]. Heparanase modulates inflammatory reactions in neuroinflammation [60], sepsis-associated lung injury [47] and inflammatory bowel disease [27], and is an important player in coupling inflammation and tumorigenesis, particularly in colitis-associated colon carcinoma.
Osterholm et al. [37] showed that heparanase expression was increased in carotid plaques and elevated in symptomatic lesions. They analyzed different combinations of the two SNPs (rs4693608 and rs4364254) and found associations between these polymorphism combinations and HPSE expression in carotid plaque. Heparanase gene expression was higher in carotid endarterectomies with HR genotype (n = 27) in comparison to samples with MR (n = 48) and LR (n = 29) genotypes (p = 0.029 using a linear regression model). The authors concluded that heparanase expression is increased in human atherosclerosis associated with inflammation, coagulation and plaque instability. Additional investigations are needed to clarify if possessors of the AA genotype have a higher risk to develop atherosclerosis-related complications in comparison to carriers of AG and GG genotypes.
Another study performed by Seifert et al. [48] revealed the involvement of heparanase SNPs in development of sinusoidal obstruction syndrome (SOS), previously known as veno-occlusive disease (VOD ; referred to as SOS/VOD). This is a common, potentially life-threatening complication observed after hematopoietic stem cell transplantation (HSCT). SOS/VOD is characterized by ongoing inflammation of terminal hepatic venules and sinusoids in zone 3 of the hepatic sinus, which contributes to occlusion. Histopathologically, the epithelium injury is accompanied by secretion of vasoactive mediators, activation of the coagulation cascade, and subendothelial deposition of clotting factors (i.e., large von Willebrand factor multimers, factor VIII, fibrin) with progressive obstruction. More recent studies indicate that the toxic damage primarily relates to sinusoidal endothelial cells and leads from ischemia and structural destruction, up to hepatocellular necrosis. Furthermore, hepatic stellate perisinusoidal cells are also involved in the pathogenesis of SOS/VOD [7, 23]. This study [48] indicated that patients with genotypes GG and AG of rs4693608 had a significantly reduced incidence of SOS on day 100 after HSCT compared to patients with genotype AA (4.7 vs. 14.3%, p = 0.038). In addition, the incidence of SOS in patients with genotype TT of rs4364254 was significantly higher in comparison to patients with genotype CC and CT (14.7 vs. 2.3%, p = 0.004). The authors concluded that HPSE gene polymorphism (rs4693608 and rs4364254) is a significant independent risk factor (p = 0.03) for development of SOS/VOD.
Pemphigus is a group of potentially fatal autoimmune blistering diseases of the skin and/or mucous membranes caused by IgG autoantibodies, which predominantly target two transmembrane desmosomal cadherins: desmoglein Dsg 1 and Dsg3 [17]. Higher incidence of pemphigus has been described in the Mediterranean population, Ashkenazi Jewish population, and Macedonian Roma population. Both genetic and environmental factors are involved in the development of pemphigus. Analysis of acantholytic lesions in the epidermis (one of them is pemphigus Vulgaris) showed a pronounced loss of syndecan-1 expression, suggesting that loss of syndecan-1 may be a prerequisite for loss of cell adhesion. Syndecan-1 is a transmembrane heparan sulfate proteoglycan (HSPG). One of the enzymes that modulate its function is heparanase [4, 34]. In our pilot study, we analyzed frequencies of rs4693608 and rs4364254 SNPs in 29 patients with pemphigus Vulgaris and compared them to 210 healthy individuals. Frequencies of LR genotype were significantly higher in the group of patients compared to healthy individuals (46.4% vs 23.3%, p = 0.028) (unpublished data). Studies in a large cohort of patients will clarify the significance of the results and involvement of heparanase in the development of pemphigus Vulgaris. As mentioned earlier, according to the UCSC Genome Browser, the additional putative enhancer is located in intron 3 and is active in keratinocytes. Analysis of HPSE SNPs located in this region is therefore needed.
4 Involvement of HPSE Gene SNPs in Cancer Development and Progression
Published data reveal a role of heparanase in dictating tumor progression. It is well supported by in vitro and in vivo studies as well as extensive research focusing on human cancer patients [55]. On the other hand, the significance of heparanase in the early phase of tumor initiation and development was not fully elucidated. Twelve HPSE gene SNPs were analyzed in different malignancies (Table 8.2). Part of them showed significant correlation with the risk of developing hepatocellular carcinoma and hematological malignancies. Additional studies in different populations are needed to further support these results. Analysis of SNPs in correlation with cancer progression and patient survival yielded clear results (Table 8.2). Allele A of rs4693608 and allele G of rs11099592 revealed significant association with poor disease survival and worse prognosis in gastric cancer and multiple myeloma (MM) (Table 8.2). Our recently published article [43] showed that rs11099592 is in strong linkage disequilibrium (LD) with rs4693084, both located close to rs4693608 (17 bp only) in the enhancer region. We assume that common rs4693608 and rs4693084 SNP-dependent enhancer activity affect cancer progression and outcomes.
SNP rs4364254, located in intron 9, revealed a significant correlation with progesterone receptor expression among patients with breast cancer. High expression of progesterone receptor was correlated with allele C, and low expression - with allele T, respectively (p = 0.002) (unpublished data). The progesterone receptor (PR), a member of the nuclear receptor family, is a well-known estrogen receptor (ER)-regulated gene that is expressed in over two-thirds of ER-positive breast cancers. PR is highly expressed in the luminal A breast cancer subtype and is associated with tumor grade, ER expression, Nottingham Prognostic Group and negative HER2 status in early breast cancer. Multiple studies have demonstrated improved prognosis of PR-positive breast cancers [15, 25, 32]. Allele C of rs4364254 is in LD with allele G of rs4693608, allele T of rs4693084 and allele A of rs11099592, which were found in correlation with better prognosis in other types of malignancies. However, the only correlation to rs4364254 was found in breast cancer. We have previously reported that rs4364254 SNP polymorphism helps to identify heterozygote AG individuals for rs4693608 with low heparanase expression [40] and low risk of acute GVHD development [41]. As mentioned above allele C of this SNP was also found in association with low risk of VOD development. This rs4364254 SNP is located between two main blocks of SNPs, and no regulatory elements were found in intron 9. Additional studies are needed to clarify the role of rs4364254 SNP in different processes.
Multiple myeloma is a B cell malignancy characterized by destructive bone lesions, chemoresistance, tumor relapse, and poor patient outcome. Heparanase is an important driver of myeloma progression [34, 46] (Purushothaman and Sanderson, Chap. 12 This book). Our recent results showed that HPSE gene enhancer is highly active in multiple myeloma (MM) cell lines (CAG, RPMI8226, U266). Andersen et al. [1] observed that rs4693608, which modulates the enhancer activity, correlates with bone morbidity and survival in MM patients. The authors found that additional SNP rs6535455, located in intron 4, is associated with the outcome of 348 MM patients in Denmark [1]. According to our previous studies, rs6535455 was found in complete LD with rs11099592. However, the authors did not identify any correlation to rs11099592. Notably, DNA for analysis was purified from PB MNCs by the salting out method or from paraffin-embedded tissue by phenol extraction. We assume that DNA extracted from paraffin-embedded tissues is enriched in myeloma cells. In another study, Huang et al. [26] using a custom SNP microarray demonstrated a high frequency of loss of heterozygosity (LOH) in the HPSE gene of hepatocellular carcinoma. Allele loss in paraffin-embedded tissue samples of MM patients may explain the observation of Andersen et al. [1] that homozygous carriers of the variant T-allele of rs6535455 had better overall survival in comparison to carriers of the C-allele.
Malignant cells escape immune-mediated cell death by deploying epigenetic mechanisms to evade host immune recognition and immunogenicity. This acquired immune evasive phenotype is achieved by epigenetic down-regulation of many critical molecules required for efficient cancer and immune cell interactions, such as suppression of tumor-associated antigens (TAAs), reduced expression of many antigen processing and presentation machinery (APM) components, and low cell surface levels of accessory/co-stimulatory molecules, death receptors, and stress-induced ligands [5, 50]. Malignant cells use chromatin remodeling for their purpose and alter gene transcription by post-translational modification of histone proteins, which include acetylation, methylation, phosphorylation, deimination, and ubiquitination. Also, the 3D nuclear architecture in normal and malignant cells contributes to transcriptional regulation and malignant cells escape. Chromatin domains containing transcriptionally active genes can form chromatin loops that extend away from compact chromosome territories to reposition near transcriptional factors at the center of the nucleus. Organization of the nuclear architecture is thought to mediate gene transcription by controlling the accessibility of regulatory DNA elements to transcription factors and RNA polymerases through subnuclear gene positioning and intra−/inter-chromosomal interactions [18].
Strong enhancer recently identified in intron 2 of the HPSE gene [43] may be involved in epigenetically regulated malignant cells escape. Applying electromobility shift assay (EMSA) , we analyzed the binding of nuclear proteins, extracted from normal leukocytes, malignant cell lines (12 hematological cancer cell lines and 14 solid tumor cell lines) and primary leukemia samples, to DNA probes that contained the rs4693608 SNP. We observed SNP-dependent and SNP independent binding. Analysis of healthy control samples demonstrated gel shift bands for both allelic probes (Fig. 8.3C). In all 26 analyzed cancer cell lines and primary leukemia samples, the band of DNA-protein complex was shifted significantly in comparison to normal samples. The affinity of the complex to the G allele probe was slightly higher in comparison to the A allele probe (Fig. 8.3C). At least 5 extra shifted bands were incorporated to allele A probe while allele G probe was bound to only one main DNA/protein complex (Fig. 8.3C).

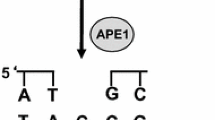
A model of the HPSE gene enhancer regulation in normal and malignant cells. (A). Normal cells. Heparanase binds to intron 2 enhancer region and regulates HPSE expression by negative feedback in rs4693608 SNP dependent manner. (B). Malignant cells. In malignant cells, heparanase is not recruited to the enhancer region, and hence its negative self-regulation is discontinued. Instead, the helicase-like transcription factor (HLTF) binds to the regulatory enhancer region. Two different consensus sequences that are recognized by HLTF were identified in the enhancer region: (C/A)C(T/A)TN(T/G) for allele A and (A/G)G(T/C) (G/T)G for allele G. While in carriers of allele A, HLTF binds to the enhancer region together with other proteins, possessors of allele G bind the HLTF alone. (C). Electromobility Shift Assay (EMSA) using DNA probes containing rs4693608 in normal leukocytes and PANC-1 cells. Rs4693608 SNP-dependent and SNP-independent binding were observed. Healthy control samples demonstrated gel shift bands for both allelic probes. In malignant cells, the band of DNA-protein complex was shifted significantly in comparison to normal samples. Additional shifted bands were incorporated to allele A probe while allele G probe was bound to only one main DNA/protein complex. We speculate that discontinuation of heparanase normal self-regulation and binding of the HLTF to the HPSE gene enhancer region results in translocation of heparanase from the cell nucleus to the cytoplasm and extracellular matrix. This may function in malignant cell escape from immune-mediated cell death and contribute to the process of cancerogenesis and tumor progression
DNA pull-down assay followed by Western blot verification showed that in normal leukocytes heparanase binds to the enhancer region and regulates HPSE gene expression via negative feedback in rs4693608 SNP-dependent manner (Fig. 8.3A). In all analyzed malignant cell lines and primary leukemia samples, heparanase halted self-regulation of the enhancer region. Instead of heparanase, the Helicase-like transcription factor (HLTF) binds to the regulatory region (Fig. 8.3B) [43]. HLTF is a member of the yeast mating SWItch/Sucrose Non-Fermenting (SWI/SNF) family of proteins involved in chromatin remodeling. HLTF plays a significant role in gene transcription, DNA repair, ubiquitination, and genome stability (Hishiki et al. 2015, Cheng et al. 2016). Two different consensus sequences recognized by HLTF were proposed: (C/A)C(T/A)TN(T/G) and (A/G)G(T/C)(G/T)G [14]. Analysis of the HPSE enhancer region included in rs4693608 SNP indicated that in the case of allele A, HLTF recognizes the first sequence CCATTG. A to G alteration does not result in loss of the transcription site but rather a change to the second variant of the HLTF recognition site (CGTTG), except the first nucleotide. Our EMSA results disclosed that not only HLTF binds to the HPSE enhancer region in allele A, but other proteins may form a common DNA-protein complex. In contrast, in the case of allele G, only HLTF binds to the HPSE gene enhancer region (Fig. 8.3B). These results may explain worse prognosis and poor survival of patients with genotypes AA/AG in comparison to possessors of genotype GG [43].
HLTF is thought to be a tumor suppressor supported by the detection of HLTF promoter hypermethylation in various types of cancer tissues and cell lines [14]. However, recent observations of increased expression of HLTF in transformed cells and cancer tissues suggest that in some cases HLTF could be associated with cancerogenesis and may act as an oncogene. Investigation of HLTF expression in a hamster model of kidney tumors revealed that HLTF gene activation is linked to initial steps of cancerogenesis and should be analyzed in an early stage of other neoplasms [13]. Taken together we speculate that cessation of heparanase normal self-regulation and binding of HLTF to the HPSE gene enhancer region results in translocation of heparanase from the nucleus to the cytoplasm and ECM and may function in malignant cell escape from immune-mediated cell death, thereby contributing to the process of cancerogenesis and tumor progression. Our hypothesis is supported by Cohen et al. [12] showing that cytoplasmic staining of heparanase is associated with a poor prognosis whereas nuclear heparanase predicts a favorable outcome of patients with lung cancer.
5 HPSE Gene SNPs and the Risk of Acute Graft Vs. Host Disease (aGVHD)
Allogeneic hematopoietic stem cell transplantation (HSCT) is a potentially effective curative therapy for a variety of malignant and non-malignant hematological diseases [3, 6, 11, 35]. However, transplant-related complications remain a major obstacle [2, 19, 51]. The outcome of HSCT is affected by several variables including disease and disease status, general condition, patient and donor age, and patient and donor HLA matching [22, 33]. Disease relapse and transplant-related complications including graft-versus-host disease (GVHD), major infection, and organ toxicities such as interstitial pneumonitis and hepatic veno-occlusive disease (sinusoidal obstruction) are the major causes for transplant failure [22, 33]. Long-term causes of morbidity include chronic GVHD and infection [36]. In addition to HLA matching, genetic diversity among patients and donors contribute to differences in individual responses to tissue injury, inflammation, and severity of acute and/or chronic GVHD.
We have demonstrated a highly significant association between rs4693608 and rs4364254 combinations and the risk of acute GVHD. The genotype combination HR, associated with increased heparanase mRNA expression [41], correlates with a high risk of acute GVHD. Conversely, the genotype combination LR, associated with decreased level of heparanase mRNA, correlates with a low risk of GVHD. Moreover, disparities between recipient and donor pairs in HPSE gene SNPs combinations significantly increased the probability of developing acute GVHD post-HSCT (Fig. 8.4C).

Status of the HPSE gene enhancer following allogeneic hematopoietic stem cell transplantation (HSCT) in various patient and donor cells. (A). Electromobility Shift Assay (EMSA) using DNA probes containing rs4693608 in patient cells after conditioning and exposure to pro-inflammatory environment, and malignant patient cells. Three types of cells with different states of the enhancer region interact with donor cells following graft intake. Conditioning led to an increase in affinity of DNA/protein binding to the enhancer region. Pro-inflammatory environment results in obstruction of transcription factor accessibility to the enhancer region. In patient-derived tumor cells, heparanase discontinues its normal self-regulation, and the HLTF binds to the enhancer region resulting in overexpression of cytoplasmatic and extracellular matrix heparanase. (B). Electromobility Shift Assay (EMSA) using DNA probes containing rs4693608 in donor cells after 5 days of exposure to G-CSF. G-CSF treatment leads to high-affinity binding of heparanase to the enhancer region with elevation of heparanase level in donor cells. (C). Cumulative incidence of acute GVHD grade II-IV after HSCT according to the discrepancy of HPSE gene SNPs rs4693608 and rs4364254 combinations between recipients and donors. The D1 group contains HR-MR and HR-LR recipient-donor genotype combination pairs. The D2 group contains MR-MR, MR-HR, MR-LR, and HR-HR recipient-donor pairs, and the D3 group contains LR-LR, LR-MR, and LR-HR recipient-donor pairs. The incidence was higher in group D1 compared to the D2 and D3 groups (P < .00001). (D). Apoptotic effect of constructs containing the G allele of rs4693608 SNP in the antisense direction in H1229 cells. Six HPSE enhancer constructs were designed and inserted upstream of the luciferase gene in pGL4.26 vector with minimal promoter. The constructs were transfected using the Ingenio Electroporation Kit (Mirus Bio, Madison, WI) and Nucleofector™ (AMAXA Biosystems, Lonza, Germany). The effect was observed 24 h after transfection
Association between increased risk of extensive chronic GVHD and either the recipient genotype combination HR or the D1 group was found. Moreover, a significant correlation between rs4693608 and rs4364254 combinations and both transplant-related mortality (TRM) and overall survival (OS) post HSCT were revealed [41].
We investigated the effect of pre-transplant conditioning regimens on heparanase expression levels in transplant recipients, as well as the predictive value of rs4693608 polymorphism for post-transplant engraftment and GVHD occurrence [42]. Pre-transplant conditioning led to a significant over-expression of the HPSE gene, followed by a gradual decrease thereafter. Notably, the increase in HPSE gene expression postconditioning was higher in patients harboring the AA genotype vs. the GG genotype.
Successful immune reconstitution post-transplant is important for decreasing infection incidence and relapse rate without increasing GVHD. The first recovered cells are neutrophils. Differences in rs4693608 between recipient and donor affect the time of neutrophils recovery. It is conceivable that high heparanase expression level in the bone marrow microenvironment of AA recipients promotes faster recovery of AG/GG donor neutrophils (AA-AG, AA-GG, and AG-GG recipient-donor pairs) [42].
Allogeneic hematopoietic stem cell transplantation (HSCT) is a well-accepted treatment modality for several malignant and non-malignant diseases. The aim of treatment is to replace the damaged hematopoietic cells with normal stem cells. Like other medical treatments, HSCT has clear risks and benefits. The primary benefit is to replace the abnormal hematopoiesis with normal cells in a way that the new immune system will elicit a graft-versus-tumor/leukemia effect. On the other hand, GVHD is also based on the recognition of foreign antigens by T-cells. Prevention of GVHD while preserving graft versus leukemia (GVL) is an elusive goal of allogeneic hematopoietic stem cell transplantation. The holy of HSCT is the ability to induce sufficient GVL to cure the patient without the induction of GVHD. A T-cell therapeutic window between achieving GVL without GVHD is highly desirable [59].
If we focus only on the enhancer region of the HPSE gene after HSCT, at least three types of cells with different states of the enhancer region may interact following graft intake: (i) without bold formatting normal patient cells after conditioning and exposure to pro-inflammatory environment (enhancer obstruction to transcription factors and heparanase overexpression in carriers of AA genotype and low elevation, unresponsiveness or downregulation in possessors of the GG genotype); (ii) tumor patient cells (discontinuation of heparanase normal self-regulation and binding of HLTF to the HPSE gene enhancer region, followed by overexpression of heparanase and involvement in tumor progression) (Fig. 8.4A); and (iii) donor cells after 5 days exposure to G-CSF (high affinity of heparanase to the enhancer, associating with elevation of heparanase level in donor cells) (Fig. 8.4B). We have previously demonstrated that discrepancy of HPSE gene SNPs between recipients and donors was the most prominent factor for risk of acute GVHD, especially in the group receiving reduced toxicity conditioning regimens [41]. We speculate that heparanase-related differences in the level of signals between recipients and donors may lead to activation and subsequent proliferation and differentiation of donor T-cells and NK cells. Since the strongest association was observed in the D1 group, it is conceivable that in D1, as opposed to the D2 and D3 groups, the recipient signal threshold, affected by heparanase, is higher compared to that of their donors. This delicate balance may be further modulated by the recipient and donor inflammatory cytokine polymorphism, leading to hyperactivation of donor T cells and thereby elevate the risk of acute GVHD.
While analyzing the enhancer activity in hematological and non-hematological malignancies, we observed apoptotic effect of constructs that included the G allele of rs4693608 SNP in antisense direction in H229, Panc-1 and SK_N_SH cell lines (Fig. 8.4D) (unpublished data). We suspect that the normal enhancer region with allele G leads to normal eRNA synthesis in malignant cells with subsequent cancer cells apoptosis. Taken together, we hypothesize that the identified effect of discrepancy in HPSE gene SNPs between recipient and donor may lead not only to risk of aGVHD but also improve the potential GVL effect on donor cells. Subsequent studies are needed to clarify how modification in HPSE enhancer activity may decrease the risk of aGVHD and improve the GVL effect of HSCT.
6 Summary
Functional SNPs are an excellent tool not only for disease-associated research but also for investigation of actual normal and pathological biological processes, which are difficult to study by other approaches. Research focusing on the HPSE gene rs4693608 SNP, located in the active enhancer, allows us to investigate the complex multiple levels of heparanase regulation, study heparanase-related mechanisms of cancer cell escape from immune-mediated cell death, improve the acute GVHD/GVL balance following HSCT, and elucidate how modification in the HPSE enhancer region may help to develop new approaches for cancer treatment.
References
Andersen, N. F., Vogel, U., Klausen, T. W., Gimsing, P., Gregersen, H., Abildgaard, N., & Vangsted, A. J. (2014). Polymorphisms in the heparanase gene in multiple myeloma association with bone morbidity and survival. European Journal of Haematology, 94, 60–66.
Ball, L. M., & Egeler, R. M. (2008). Acute GVHD: Pathogenesis and classification. Bone Marrow Transplantation, 41, S58–S64.
Baron, F., & Storb, R. (2004). Allogeneic hematopoietic cell transplantation as treatment for hematological malignancies: A review. Springer Seminars in Immunopathology, 26, 71–94.
Bayer-Garner, I. B., Dilday, B. R., Sanderson, R. D., & Smoller, B. R. (2001). Acantholysis and spongiosis are associated with loss of syndecan-1 expression. Journal of Cutaneous Pathology, 23, 135–139.
Bhatia, A., & Kumar, Y. (2014). Cellular and molecular mechanisms in cancer immune escape: A comprehensive review. Expert Review of Clinical Immunology, 10, 41–62.
Castillo, J. J., Winer, E. S., & Olszewski, A. J. (2014). Sites of extranodal involvent are prognostic in patients with diffuse large B-cell lymphoma in the rituximab era: An analysis of the surveillance, epidemiology and end results database. American Journal of Hematology, 89, 310–314.
Chalandon, Y., Roosnek, E., Mermillod, B., Newton, A., Ozsahin, H., Wacker, P., Helg, C., & Chapuis, B. (2004). Prevention of veno-occlusive disease with defibrotide after allogeneic stem cell transplantation. Biology of Blood and Marrow Transplantation, 10, 347–354.
Chanock, S. (2001). Candidate genes and single nucleotide polymorphisms (SNPs) in the study of human disease. Disease Markers, 17, 89–98.
Chanock, S. (2003). Genetic variation and hematology: Single-nucleotide polymorphisms, haplotypes, and complex disease. Seminars in Hematology, 40, 321–328.
Cheng, C. K., Chan, N. P. H., Wan, T. S. K., Lam, L. Y., Cheung, C. H. Y., Wong, T. H. Y., Ip, R. K. L., Wong, R. S. M., & Ng, M. H. L. (2015). Helicase-like transcription factor is a RUNX1 target whose downregulation promotes genomic instability and correlates with complex cytogenetic features in acute myeloid leukemia. Haematologica, 101, 448–457.
Chisholm, K. M., Ohgami, R. S., Tan, B., Hasserjian, R. P., & Weinberg, O. K. (2017). Primary lymphoma of bone in the pediatric and young adult population. Human Pathology, 60, 1–10.
Cohen, E., Doweck, I., Narodittsky, I., Ben-Izhak, O., Kremer, R., Best, L. A., Vlodavsky, I., & Ilan, N. (2008). Heparanase is overexpressed in lung cancer and correlates inversely with patient survival. Cancer, 113, 1004–1011.
Debauve, G., Nonclercq, D., Ribaucour, F., Wiedig, M., Gerbaux, C., Leo, O., Laurent, G., Journe, F., Belayew, A., & Toubeau, G. (2006). Early expression of the helicase-like transcription factor (HLTF/SMARCA3) in an experimental model of estrogen-induced renal carcinogenesis. Molecular Cancer, 5, 23–38.
Debauve, G., Capouillez, A., Belayew, A., & Saussez, S. (2008). The helicase-like transcription factor and its implication in cancer progression. Cellular and Molecular Life Sciences, 65, 591–604.
Daniel, A. R., Hagan, C. R., & Lange, C. A. (2011). Progesterone receptor action: Defining a role in breast cancer. Expert Review of Endocrinology and Metabolism, 6, 359–369.
Deng, N., Zhou, H., Fan, H., & Yuan, Y. (2017). Single nucleotide polymorphisms and cancer susceptibility. Oncotarget, 8, 110635–110649.
Di Zenzo, G., Amber, K. T., Sayar, B. S., Muller, E. J., & Borradori, L. (2016). Immune response in pemphigus and beyond: Progresses and emerging concepts. Seminars in immunopathology, 38, 57–74.
Dunn, J., & Rao, S. (2017). Epigenetics and immunotherapy: The current state of play. Molecular Immunology, 87, 227–239.
Ferrara, J. L., & Reddy, P. (2006). Pathophysiology of graft-versus-host disease. Seminars in Hematology, 43, 3–10.
Gibney, E. R., & Nolan, C. M. (2010). Epigenetics and gene expression. Heredity, 105, 7–13.
Gooley, T. A., Leisenring, W., Crowley, J., & Storer, B. E. (1999). Estimation of failure probabilities in the presence of competing risk: New representations of old estimators. Statistics in Medicine, 18, 695–706.
Gratwohl, A., Brand, R., Frassoni, F., Rocha, V., Niederwieser, D., Reusser, P., Einsele, H., & Cordonnier, C. (2005). Cause of death after allogeneic hematopoietic stem cell transplantation (HSCT) in early leukemias: An EBMT analysis of lethal infectious complications and changes over calendar time. Bone Marrow Transplantation, 36, 757–769.
Guglielmelli, T., Bringhen, S., & Palumbo, A. (2012). Update on the use of defibrotide. Expert Opinion on Biological Therapy, 12, 353–361.
Hishiki, A., Hara, K., Ikegaya, Y., Yokoyama, H., Shimizu, T., Sato, M., & Hashimoto, H. (2015). Structure of a novel DNA-binding domain of helicase-like transcription factor (HLTF) and its functional implication in DNA damage tolerance. The Journal of Biological Chemistry, 290, 13215–13223.
Hsieh, S. M., & Lintell, H. K. W. (2007). Germline polymorphisms are potential metastasis risk and prognosis markers in breast cancer. Breast Disease, 26, 157–162.
Huang, G.-L., Li, B.-K., Zhang, M.-Y., Wei, R.-R., Yuan, Y.-F., Shi, M., Chen, X.-Q., Huang, L., Zhang, H.-Z., Liu, W., Huang, B.-J., Li, H., Zheng, X.-F., Luo, X.-R., & Wang, H.-Y. (2012). Allele loss and down-regulation of heparanase gene are associated with the progression and poor prognosis of hepatocellular carcinoma. PLoS One, 7, e44061.
Lerner, I., Hermano, E., Zcharia, E., Rodkin, D., Bulvik, R., Doviner, V., Rubinstein, A. M., Ishai-Michaeli, R., Atzmon, R., Sherman, Y., Meirovitz, A., Peretz, T., Vlodavsky, I., & Elkin, M. (2011). Heparanase powers a chronic inflammatory circuit that promotes colitis-associated tumorigenesis in mice. The Journal of Clinical Investigation, 121, 1709–1721.
Li, A.-L., Song, Y.-X., Wang, Z.-N., Gao, P., Miao, Y., Zhu, J.-L., Yue, Z.-Y., & Xu, H.-M. (2012). Polymorphisms and a haplotype in heparanase gene associations with the progression and prognosis of gastric cancer in a northern chinese population. PLoS One, 7, e30277.
Li, R. W., Freeman, C., Yu, D., Hindmarsh, E. J., Tymms, K. E., Parish, C. R., & Smith, P. N. (2008). Dramatic regulation of heparanase activity and angiogenesis gene extression in synovium from patients with rheumatoid arthritis. Arthritis and Rheumatism, 58, 1590–1600.
Lider, O., Baharav, E., Mekori, Y. A., Miller, T., Naparstek, Y., Vlodavsky, I., & Cohen, I. R. (1989). Suppression of experimental autoimmune disease and prolongation of allograft survival by treatment of animals with low doses of heparins. The Journal of Clinical Investigation, 83, 752–756.
Lider, O., Mekori, Y. A., Miller, T., Bar-Tana, R., Vlodavsky, I., Baharav, E., Cohen, I. R., & Naparstek, Y. (1990). Inhibition of T lymphocyte heparanase by heparin prevents T cell migration and T cell-mediated immunity. European Journal of Immunology, 20, 493–499.
Lim, E., Palmieri, C., & Tilley, W. D. (2016). Renewed interest in the progesterone receptor in breast cancer. British Journal of Cancer, 115, 909–911.
Loberiza F (2003) The 2003 BMT summary slides with guide. IB-MTR/ABMTR Newslett 7–10.
Mahtouk, K., Hose, D., Raynaud, P., Hundemer, M., Jourdan, M., Jourdan, E., Pantesco, V., Baudard, M., De Vos, J., Larroque, M., Moehler, T., Rossi, J.-F., Reme, T., Goldshmidt, H., & Klein, B. (2007). Heparanase influences expression and shedding of syndecan-1, and its expression by the bone marrow environment is a bad prognostic factor in multiple myeloma. Blood, 109, 4914–4923.
Martelli, M., Ferreri, A. J. M., Agostinelli, C., Di Rocco, A., Pfeundschuh, M., & Pileri, S. (2013). Diffuse large B-cell lymphoma. Critical Reviews in Hematology, 87, 146–171.
Mielcarek, M., Martin, P. J., Leisenring, W., Flowers, M. E., Maloney, D. G., Sandmaier, B. M., Maris, M. B., & Storb, R. (2003). Graft-versus-host disease after nonmyeloablative versus conventional hematopoietic stem cell transplantation. Blood, 102, 756–762.
Osterholm, C., Folkersen, L., Lengquist, M., Ponten, F., Renne, T., Li, J. P., & Hedin, U. (2013). Increased expression of heparanasee in symptomatic carotid atherosclerosis. Atherosclerosis, 226, 67–73.
Ostrovsky, O., Korostishevsky, M., Levite, I., Leiba, M., Galski, H., Gazit, E., Vlodavsky, I., & Nagler, A. (2007). Characterization of HPSE gene single nucleotide polymorphisms in Jewish populations of Israel. Acta Haematologica, 117, 57–64.
Ostrovsky, O., Korostishevsky, M., Levite, I., Leiba, M., Galski, H., Vlodavsky, I., & Nagler, A. (2007). Association of heparanase gene (HPSE) singlr nucleotide polymorphisms with hematological malignancies. Leukemia, 21, 2296–2303.
Ostrovsky, O., Korostishevsky, M., Shafat, I., Mayorov, M., Ilan, N., Vlodavsky, I., & Nagler, A. (2009). Inverse correlation between HPSE gene single nucleotide polymorphisms and heparanase expression: Possibility of multiple levels of heparanase regulation. Journal of Leukocyte Biology, 86, 445–455.
Ostrovsky, O., Shimoni, A., Rand, A., Vlodavsky, I., & Nagler, A. (2010). Genetic variations in the heparanase gene (HPSE) associate with increased risk of GVHD following allogeneic stem cell transplantation: Effect of discrepancy between recipients and donors. Blood, 115, 2319–2328.
Ostrovsky, O., Shimoni, A., Baryakh, P., Margulis, Y., Mayorov, M., Beider, K., Shteingauz, A., Ilan, N., Vlodavsky, I., & Nagler, A. (2014). Modification of heparanase gene expression in response to conditioning and LPS treatment: Strong correlation to rs4693608 SNP. Journal of Leukocyte Biology, 95, 677–688.
Ostrovsky, O., Grushchenko-Polaq, A. H., Beider, K., Mayorov, M., Canaani, J., Shimoni, A., Vlodavsky, I., & Nagler, A. (2018). Identification of strong intron enhancer in the heparanase gene: Effect of functional rs4693608 variant on HPSE enhancer activity in hematological and solid malignancies. Oncogene, 7, 51–65.
Qiang, M. D. A., Chen, J., Ticku, M. K., Yan, B., & Henderson, G. (2010). The site specific demethylation in the 5-regulatory area of NMDA receptor 2B subunit gene associated with CIE-induced up-regulation of transcription. PLoS One, 5, e8798.
Ralph, S., Brenchley, P. E. C., Summers, A., Rosa, D. D., Swindell, R., & Jayson, G. C. (2007). Heparanase gene haplotype (CGC) is associated with stage of disease in patients with ovarian carcinoma. Cancer Science, 98, 844–849.
Ramami, V. C., Zhan, F., He, J., Barbier, P., Noseda, A., Tricot, G., & Sanderson, R. D. (2015). Targeting heparanase overcomes chemoresistance and diminishes relapse in myeloma. Oncotarget, 7, 1598–1607.
Schmidt, E. P., Yang, Y., Janssen, W. J., Gandjeva, A., Perez, M. J., Barthel, L., Zemans, R. L., Bowman, J. C., Koyanagi, D. E., Yunt, Z. X., Smith, L. P., Cheng, S. S., Overdier, K. H., Thompson, K. R., Geraci, M. W., Douglas, I. S., Pearse, D. B., & Tuder, R. M. (2012). The pulmonary endothelial glycocalyx regulates neutrophil adhesion and lung injury during experimental sepsis. Nature Medicine, 18, 1217–1223.
Seifert, C., Wittig, S., Arndt, C., & Gruhn, B. (2015). Heparanase polymorphisms: Influence on incidence of hepatic sinusoidal obstruction syndrome in children undergoing allogeneic hematopoietic stem cell transplantation. Journal of Cancer Research and Clinical Oncology, 141, 877–885.
Shen, J., Liu, Y., Ren, X., Gao, K., Li, Y., Yao, J., & Yang, X. (2016). Changes in DNA methylation and chromatin structure of pro-inflammatory cytokines stimulated by LPS in broiler peripheral blood mononuclear cells. Poultry Science, 95, 1636–1645.
Spranger, S. (2016). Mechanisms of tumor escape in the context of the T-cell-inflamed and the non-T-cell-inflamed tumor microenvironment. International Immunology, 28, 383–391.
Sun, Y., Tawara, I., Toubai, T., & Reddy, P. (2007). Pathophysiology of graft-versus-host disease: Recent advances. Translational research : the journal of laboratory and clinical medicine, 150, 197–214.
Tan, P. (2008). Germline polymorphisms as modulators of cancer phenotypes. BioMed Central Medicine, 6, 27–31.
Vlodavsky, I., Eldor, A., Haimovitz-Friedman, A., Matzner, Y., Ishai-Michaeli, R., Lider, O., Naparstek, Y., Cohen, I. R., & Fuks, Z. (1992). Experimental of heparanase by platelets and circulating cells of the immune system: Possible involvement in diapedesis and extravasation. Invasion & Metastasis, 12, 112–127.
Vlodavsky, I., Iozzo, R. V., & Sanderson, R. D. (2013). Heparanase: Multiple functions in inflammation, diabetes and atherosclerosis. Matrix Biology, 32, 220–222.
Vlodavsky, I., Singh, P., Boyango, I., Gutter-Kapon, L., Elkin, M., Sanderson, R., & Ilan, N. (2016). Heparanase: From basiv research to therapeutic applications in cancer and inflammation. Drug Resistance Updates, 29, 54–75.
Wang, G. G., Allis, C. D., & Chi, P. (2007). Chromatin remodeling and cancer. Part I: Covalent histone modifications. Trends in Molecular Medicine, 13, 363–372.
Yu, L., Zhang, X., Zhai, Y., Zhang, H., Yue, W., Zhang, X., Wang, Z., Zhou, H., Zhou, G., & Gong, F. (2017). Association of polymorphisms in the heparanase gene (HPSE) with hepatocellular carcinoma in Chinese populations. Genetics and Molecular Biology, 40, 743–750.
Yue, Z., Song, Y., Wang, Z., Luo, Y., Jiang, L., Xing, L., Xu, H., & Zhang, X. (2010). Association of heparanase gene (HPSE-1) single nucleotide polymorphisms with gastric cancer. Journal of Surgical Oncology, 102, 68–72.
Zhang, P., Chen, B. J., & Chao, N. J. (2011). Prevention of GVHD without losing GVL effect: Windows of opportunity. Immunologic Research, 49, 49–55.
Zhang, X., Wang, B., & Li, J. P. (2014). Implications of heparin sulfate and heparanase in neuroinflammation. Matrix Biology, 35, 174–181.
Ziolkowski, A. F., Popp, S. K., Freeman, C., Parish, C. R., & Simeonovic, C. J. (2012). Heparan sulfate and heparanase play key roles in mouse beta cell survival and autoimmune diabetes. The Journal of Clinical Investigation, 122, 132–141.
Acknowledgments
We wish to thank all people who took part in the following projects: Prof. Ephraim Gazit (Chaim Sheba Medical Center, Israel) – Pemphigus Vulgaris project; Prof. Eitan Friedman and Dr. Yael Laitman (Chaim Sheba Medical Center, Israel) – Breast cancer project; Dr. Hanan Galski and Dr. Tamar Oved (Chaim Sheba Medical Center, Israel) – NK cells project.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2020 Springer Nature Switzerland AG
About this chapter

Cite this chapter
Ostrovsky, O., Vlodavsky, I., Nagler, A. (2020). Mechanism of HPSE Gene SNPs Function: From Normal Processes to Inflammation, Cancerogenesis and Tumor Progression. In: Vlodavsky, I., Sanderson, R., Ilan, N. (eds) Heparanase. Advances in Experimental Medicine and Biology, vol 1221. Springer, Cham. https://doi.org/10.1007/978-3-030-34521-1_8
Download citation
DOI: https://doi.org/10.1007/978-3-030-34521-1_8
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-34520-4
Online ISBN: 978-3-030-34521-1
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)