
Abstract
Paediatric radiology is a subspecialty of radiology that covers all aspects of diagnostic imaging and image-guided treatment for children. The pathologies encountered in children are often different than those found in adults and paediatric radiology therefore differs in its approach and findings. Every imaging modality used in adult radiology is also used in paediatric radiology but with more emphasis on those with either low or no radiation, and on using distraction and pleasant environments to ease the process of acquiring images. After completing this tutorial students should be able to describe some of the reasons for specific modality choices when imaging children, and the important imaging features in a number of key pathologies.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
Aims and Guidance for Tutors
Paediatric radiology is a subspecialty of radiology that covers all aspects of diagnostic imaging and image-guided treatment for children. The pathologies encountered in children are often different than those found in adults and paediatric radiology therefore differs in its approach and findings. Every imaging modality used in adult radiology is also used in paediatric radiology but with more emphasis on those with either low or no radiation, and on using distraction and pleasant environments to ease the process of acquiring images. After completing this tutorial students should be able to describe some of the reasons for specific modality choices when imaging children, and the important imaging features in a number of key pathologies.
Introduction
-
Childhood injury and illnesses differ to the those seen in adults
-
Children are more susceptible to the potential negative effects of medical ionising radiation than adults:
-
Modalities that do not use radiation (ultrasound and MRI) are used more often in paediatric radiology than in adult radiology
-
When using modalities that use radiation, great care is taken to use the lowest dose necessary for diagnosis.
-
-
Congenital and developmental pathologies are key, whereas degenerative pathologies are less frequent than in adult radiology.
Radiologist’s tip: Imaging babies and young children
-
One of the challenges in paediatric imaging is getting the patients to remain still enough to acquire diagnostic images.
-
Child-friendly staff, equipment and environments can help to successfully acquire imaging in an awake child, as well as the help of the parents.
-
A minority of children need to be imaged under sedation or general anaesthesia in order to obtain diagnostic quality imaging.
-
Anaesthesiology, nursing and specialist paediatric radiographers are key team members in a paediatric radiology department.
-
Radiological Modalities Used in Paediatric Radiology
-
Plain radiography:
-
The most commonly used modality in the paediatric radiology department and is often first line for investigation of trauma, pneumonia or suspected bowel obstruction.
-
-
Ultrasound:
-
Ultrasound scanning is a cornerstone of paediatric imaging due to the absence of radiation and due to its portability.
-
Children’s small size and relatively low subcutaneous fat thickness provide excellent acoustic windows into almost the entire abdomen, with the exception of air-filled bowel.
-
The unossified anterior fontanelle of the still-developing skull, especially in the first 6 months of life allows the brain to be imaged with ultrasound in small babies.
-
It can also be used to rule out hip dysplasia and image the spinal cord in the neonate as the adjacent bones have still not fully ossified.
-
-
Magnetic resonance (MR) imaging:
-
Relied heavily upon in paediatric imaging due to the absence of radiation.
-
Shows excellent soft tissue detail.
-
Requires long periods of stillness to produce high quality imaging.
-
Complex to acquire and interpret.
-
Requires a team approach with nursing and anaesthesiology when sedation or general anaesthesia is necessary.
-
MR Simulators can be used to help patients overcome their anxiety and potentially obviate the need for general anesthetic.
-
-
Fluoroscopy:
This modality uses pulsed x-rays to obtain real time imaging of the patient.
-
It is particularly helpful in diagnosing potentially life threatening bowel malrotation as well as assisting in the reduction of intussusception.
-
Computed tomography (CT):
-
This requires a higher radiation dose when compared with plain radiography or fluoroscopy but ongoing technical advances are continuing to allow doses to be reduced.
-
-
Nuclear imaging:
-
Imparts a radiation dose to the patient.
-
Requires patients to lie still, sometimes for prolonged periods of time.
-
Used to find pathology such as osteomyelitis in bones that may not be detectable on xrays.
-
Used for measuring function in kidneys and for evaluation of obstructed kidneys.
-
-
Paediatric interventional radiology:
-
Uses imaging modalities such as ultrasound, fluoroscopy, CT and MRI to perform procedures in the paediatric population.
-
Procedures include vascular catheter placement, tissue biopsy, tumour ablation and angiography.
-
Chest and Airway Imaging in Children
Causes of acute dyspnoea in newborn infants:
-
Transient tachypnoea of the newborn is due to delayed clearance of fluid from the lungs. It is more common in small babies and in babies delivered by C-section owing to reduced mechanical squeeze from the birth canal to clear the fluid in the lungs. The retained fluid appears as interstitial oedema- fine lines-on chest radiograph, often with fluid in fissures. It classically resolves in 24 hours.
-
Meconium aspiration: If a baby aspirates meconium stained liquor during delivery the meconium is very irritant to the bronchi. The meconium or the resulatant airway inflammation may obstruct airways or narrow them. This may appear on a chest x-ray as streaky densities due to atelecatasis and air-trapping. There is a high incidence of pneumothorax and pneumomediastinum in babies with meconium aspiration.
-
Respiratory Distress Syndrome (RDS): Neonates born as prematurely as 23 weeks can survive with modern neonatal ICU care. Surfactant, which keeps the alveoli of the lungs open to exchange gas, begins to be produced in an immature form in the lungs from 24 weeks. The administration of synthetic surfactant to treat Respiratory Distress Syndrome RDS or ‘surfactant deficiency of prematurity’ has led to markedly increased survival of premature infants. The typical appearance is of bilateral symmetrical alveolar densities with air bronchograms and low lung volumes (Fig. 1).
Fig. 1 
Chest radiograph in a premature neonate which shows small lung volumes and a hazy opacification throughout the lungs in keeping with RDS
-
Neonatal pneumonia: This can be caused by maternal systemic infection or acquired bacteria such as Group B Streptococcus. The most characteristic pattern is dense air space opacification with air bronchograms, but patterns may be variable and a high index of suspicion is required if there is a clinical deterioration.
-
Congenital diaphragmatic hernia: The lung development is limited by a herniation of bowel into the thorax. These patients can have severe morbidity if the lung fails to develop due to mass effect from the hernia (Fig. 2).
Fig. 2 
Chest radiograph in a baby which shows bubbly lucencies in the left thorax in keeping with bowel loops (arrowhead). This is a left sided congenital diaphragmatic hernia. The nasogastric tube is in the thorax (arrow) instead of its expected position below the diaphragm


Causes of acute dyspnoea in children: lower respiratory tract.
-
Bronchiolitis is common in children under 1 year and is caused typically by RSV (respiratory syncytial virus). The lungs are hyperinflated with bronchial wall thickening and can have bilateral areas of atelectasis. In severe cases the patient may need to be intubated in ICU.
-
Pneumonia can look different in a child to an adult on a chest radiograph. An entity called round pneumonia is unique to children. If a child has clinical evidence of infection a mass on a chest radiograph can be treated as probable infection. A follow up radiograph must be done to confirm resolution.
Causes of acute dyspnoea in children: upper respiratory tract.
-
Croup (acute laryngotracheobronchitis) which is a viral infection of the airway and the commonest cause of acute upper airway obstruction in children. The radiograph typically shows a “steeple sign” due to narrowing of the subglottic airway (Fig. 3).
Fig. 3 
Radiograph in a 2 year old presenting with stridor showing the ‘steeple sign’ of croup (arrow)
-
Epiglottitis, a potentially life threatening infection of the epiglottis caused by Hemophilus Influenza that should be diagnosed clinically without need for radiographs.
-
Foreign Body Inhalation or ingestion: Children under 3 are most at risk for ingesting foreign bodies such as coins or batteries. These may be radio-opaque and can be seen on chest radiographs when the child presents with wheeze, stridor or respiratory distress. Some foreign bodies for example peanuts are not seen on a radiograph. Instead signs such as hyperinflation or air trapping on the side of the aspiration, collapse of the lung distal to the obstruction are sought on the radiograph. Figure 4 shows a hair clip lodged in the right main bronchus in a child.
Fig. 4 
Chest radiograph in a child who presented with stridor which shows a foreign body, a hair-clip, lodged in the right main bronchus


Radiologist’s tip : Inhaled foreign body
-
If a small child presents with stidor and one lung appears larger and more lucent than the other an inhaled foreign body must be considered. The foreign body itself may or may not be visible on a chest radiograph.
Cardiac Anomalies
-
Cardiac anomalies are classified into groups according to whether they cause the child to be cyanotic (the blue infant) or non-cyanotic.
-
In cyanotic congenital heart disease there may be no mechanical route for deoxygenated blood to reach the lungs for oxygenation as in the Tetralogy of Fallot where there is pulmonary stenosis.
-
There may be no pumping ability of the heart to supply blood to the body as in hypoplastic left heart syndrome.
-
In atrial or ventricular septal defects the atrial or ventricular septum are deficient leading to mixing of oxygenated blood and deoxygenated blood. A combined defect, AVSD (atrio-ventricular septal defect), is associated with Trisomy 21 (Down Syndrome).
Gastrointestinal (GI) Imaging in Children
Upper GI obstruction in neonates.
Malrotation and volvulus:
-
Bilious vomiting in a new-born implies there is obstruction below the level of the bile duct opening into the second part of the duodenum.
This presentation should raise concern for malrotation of the bowel with volvulus which is a true paediatric surgical emergency.
-
Neonates born with malrotation are predisposed to volvulus due to a shortened mesentery.
-
The plain radiograph may show a distended stomach and proximal duodenum with little or no gas beyond this.
-
However radiographs are often normal or unhelpful. The best imaging modality to diagnose this is a flouroscopic upper GI contrast study.
-
Volvulus results in compromise of enteric blood supply. The entire bowel can infarct and require resection which carries huge morbidity and mortality (Fig. 5).
Fig. 5 
An upper GI fluoroscopic study demonstrating the duodenal-jejunal flexure in an abnormal position to the right of the midline in keeping with malrotation. The bowel is tortuous distal to this due to volulus

Hypertrophic pyloric stenosis:
-
A cause of non-bilious vomiting typically in a first born, male infant under 3 months of age and can be diagnosed with ultrasound.
-
Ultrasound typically shows a thickened circular muscle of the pylorus with a distended stomach. Treatment is surgical with a pyloromyotomy.
Other causes of upper GI obstruction in a baby include:
-
Oesophageal atresia which is often associated with a tracheoesophageal fistula.
-
Duodenal atresia which is associated with Trisomy 21.
Lower GI obstruction in neonates:
-
This is suspected clinically when vomiting is associated with abdominal distension and failure to pass meconium. The abdominal radiograph shows multiple dilated loops throughout the abdomen.
-
Contrast enema is used for further assessment. The most common cause is Hirschprung disease. Other causes include imperforate anus, meconium ileus, meconium plug, ileal or colonic atresia.
Hirschsprung’s disease:
-
This is aganglionosis of the distal bowel typically involving the rectum and extending over a variable length of bowel.
-
It can present in the newborn with failure to pass meconium or in childhood with chronic constipation. It is diagnosed definitively with rectal biopsy but the transition point may be delineated with a contrast enema.
Imperforate anus:
-
These patients have no anal opening. The condition may be associated with other congenital anomalies such as oesophageal atresia and vertebral anomalies in the VACTERL syndrome (Vertebral, Anorectal, Cardiac, Tracheoesophageal fistula, Renal and Limb abnormalities).
Meconium ileus:
-
This is small bowel obstruction in a newborn due to thick, inspissated meconium lodged in the distal ileum, causing obstruction and sometimes perforation. Meconium ileus occurs almost exclusively in babies with cystic fibrosis which will be diagnosed using a sweat test when the baby is at least one month old (Fig. 6).
Fig. 6 
Contrast enema in a neonate who failed to pass meconium. Thick plugs of meconium are seen obstructing the small bowel (arrows). Note the appendix filled with contrast (arrowhead)

Other paediatric GI pathologies:
Intussusception:
-
Telescoping of one part of the bowel into the adjacent part through peristalsis which leads to obstruction. In children 90% are idiopathic and the usual age range is between 3 months and 3 years.
-
Crying, pallor, drawing legs up to the abdomen are presenting features. Bloody (red currant jelly) stools, though classic, is a less common presenting feature.
-
A mass may be felt within the right side of the abdomen. Ultrasound shows a donut appearance of the intussusception. An air-enema carried out by the radiologist successfully reduces the intussusception in approximately 85% of babies. The procedure has a 0.5% rate of perforation.
Appendicitis
-
A common cause of abdominal pain presenting to the Paediatric ED. Ultrasound may show a thickened appendix. There may be inflammation of the surrounding mesentery and possibly an appendicolith.
-
Children may form an inflammitory mass around an appendicitis that may be visible as an appendiceal mass on ultrasound.
Necrotising enterocolitis:
-
This is an idiopathic colitis related to infection and ischemia affecting the premature infant in ICU. There may be nonspecific bowel dilatation with intramural air (pneumatosis) or, if the bowel perforates, pneumoperitoneum.
-
Treatment is nil PO and antibiotics. This entity may be complicated by bowel strictures.
Renal Imaging in Children
-
It is important to diagnose and promptly treat kidney and bladder infection in children as, if left untreated, the renal cortex may become scarred and non-functional.
-
Ultrasound, micturating cysto-urethrograms (MCUG) and nuclear medicine studies may help to determine whether an infection is present, may detect any structural abnormality that could predispose to infection and may detect complications of infection, especially scarring.
Dilated renal collecting systems in the neonate:
-
This may be identified on pre-natal ultrasound scanning. Post natal imaging is used to determine the cause of the dilated collecting system:
-
Pelviureteric junction (PUJ) obstruction:
-
Obstruction of the proximal ureter. PUJ obstruction is the commonest cause of congenital hydronephrosis.
-
-
Posterior urethral valves:
-
These are prominent folds in the lumen of the urethra that can block the passage of urine from the posterior urethra leading to bilateral hydronephrosis. Posterior urethral valves are diagnosed on MCUG.
-
Treatment of valves (Fig. 7) involves surgical fulguration.
Fig. 7 
Micturating cystourethrogram in a 2 month old boy who had hydronephrosis noted antenatally. Note the dilated posterior urethra (arrow) and the obstructing valves (arrowhead)

Radiologist’s tips
-
An ultrasound of the kidneys and bladder will diagnose dilated collecting systems (hydronephrosis) and malformed kidneys
A micturating cystourethrogram is a flouroscopic study that will diagnose posterior urethral valves and vesoureteric reflux.
Nuclear medicine studies: MAG3 is used to evaluate obstruction and DMSA scan to show scarring and differential function of each kidney.
Paediatric Neuroimaging
-
It is possible to evaluate the neonatal brain by cranial ultrasound via the open fontanelle or sutures. As well as having no ionising radiation, it has the advantage of being very portable and can be used at the incubator in the neonatal intensive care unit for the sick newborn.
Intraventricular haemorrhage
-
In the premature newborn, cranial ultrasound is used to detect intraventricular haemorrhage, (IVH) post haemmorhagic hydrocephalus and periventricular leukomalacia.
-
IVH is more common in premature infants and tends to occur in the first week of life.
Neonatal encephalopathy:
-
In the term infant this is usually secondary to a hypoxic ischaemic insult.
-
Neonatal encephalopathy results in low APGAR scores, metabolic acidosis and, in severe cases, EEG abnormalities and seizures.
-
This injury to the developing brain can lead to severe neurological deficits in later life.
-
If suspected clinically it may be treated with cooling of the infant.
-
MRI is the most sensitive investigation.
Spinal dysraphism:
-
Also called spina bifida. This is caused by varying degrees of abnormal closure of the embryonic neural tube.
-
It is the most common CNS congenital anomaly and can vary widely in severity from a dimple in the lower back to a myelomeningocele, which is a collection of CSF and spinal nerve roots lying exposed at the base of the spine.
-
Patients may be functionally unaffected by milder forms but may be wheelchair-bound in more severe cases.
Paediatric Skeletal Imaging
-
Children are prone to different types of musculoskeletal injuries than adults due to differences in bone structure and biomechanics.
-
The presence of the growth plates or physis also makes childhood fractures different from those of adults (Fig. 8). The weakest link in the growing skeleton is at the physis. Fractures involving the physis are classified according to the Salter Harris classification system.
Fig. 8 
AP and lateral radiographs of the wrist demonstrating a fracture of the distal radius in a child which appears as a bump in the cortex (arrow) best appreciated on the lateral projection. This is known as a Buckle fracture. It occurs because developing bone falters with longitudinal compression resulting in a spectrum from buckle to greenstick to complete fracture

Developmental dysplasia of the hip
-
Babies are clinically screened at birth for dislocation of the hip and for developmental dysplasia of the hip (DDH).
-
Females, those born by breech delivery and those with a family history for DDH are more likely to have this condition which can be diagnosed on ultrasound in the first 8 weeks of life and with x-rays thereafter.
-
Ultrasound or x-ray may show a dysplastic (shallow) acetabulum, subluxation or dislocation of the hip. These patients may need bracing or surgery.
Perthes disease
-
This is an idiopathic avascular necrosis of the femoral head, and is most common in the 3–6 year age group.
-
Radiographs may be normal initially and later may show a smaller irregular femoral head which becomes progressively flatter and more deformed as the condition progresses (Fig. 9).
-
Treatment is related to symptom control early in the disease.
Fig. 9 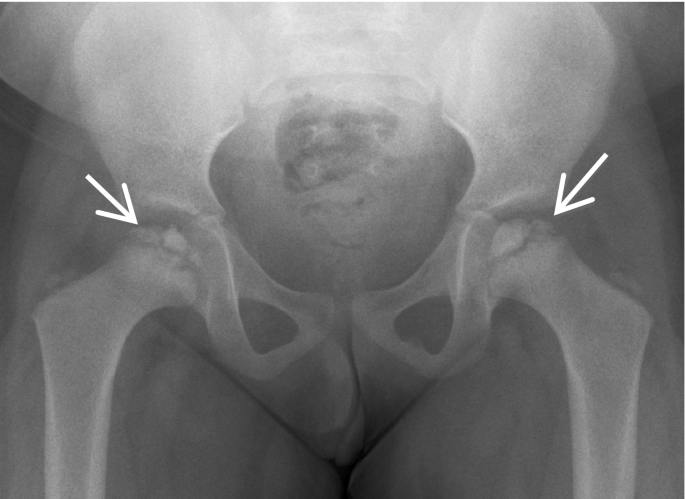
A 4 year child presenting with bilateral hip pain. There is fragmentation and loss of height of the right femoral head and of the lateral aspect of the left femoral head in keeping with avascular necrosis or Perthe’s disease

Slipped upper femoral epiphysis (SUFE):
-
This is a fracture of the physeal plate of the upper femur which needs orthopaedic fixation. This can be best seen on a frog-lateral view of the hips where the proximal femoral physis slips posteromedially.
-
It is more common in overweight peripubertal boys (Fig. 10).
Fig. 10 
Radiograph of the pelvis in an 11 year old with a painful right hip. It shows a right slipped upper femoral epiphysis. Notice the widened physis on the right (arrow) and the downward displacement of the femoral head

Non-accidenal injury
-
Radiologists have important role in identifying cases of potential non-accidental injury.
-
Fractures of different ages on radiographs or that don’t fit with the provided history should raise the suspicion of the radiologist and clinician for non-accidental injury.
-
If this is suspected a full body series of radiographs called a skeletal survey can be carried out to check for other fractures. Certain fractures that are particularly suspicious include corner metaphyseal fractures, fractures of the posterior ribs, long bone fractures in a pre-ambulant child and multiple fractures at different stages of healing (Fig. 11).
Fig. 11 
A 3 month old baby who presented with a cough and fever. CXR showed multiple healing rib fractures. There was no history of trauma to account for these
-
Subdural and intraparenchymal brain haemorrhages can also occur from abusive head trauma in ‘shaken baby’ syndrome. A CT brain is carried out on all suspected cases of NAI in the first year of life.

Radiologist’s tip : Non accidental injury
-
Certain fractures are particularly suspicious for non accidental injury:
-
corner metaphyseal fractures
-
fractures of the posterior ribs
-
long bone fractures in a pre-ambulant child
-
multiple fractures at different stages of healing.
-
Paediatric Oncological Imaging
-
Paediatric oncology is a specialist branch of paediatrics which is treated in specialist centres. A multidiciplinary approach with oncologists, radiation oncologists, radiologists, pathologists and surgeons amongst others is key. Cases are often discussed on a global platform with experts from around the world to share knowledge and experience to improve outcomes.
-
Lukaemia:
-
The most common childhood cancer accounting for approximately 30%. Abnormal leucocytes are produced in the bone marrow which supress the production of normal blood cells.
-
Imaging appearances of leukaemia are subtle and the diagnosis is usually made with blood tests and bone marrow biopsy.
-
-
Lymphoma:
-
Accounts for 6% of childhood cancers and is a group of cancers characterised by reed Sternberg cells. 95% of cases are Hodgkin’s Lymphoma.
-
Patients often present with lymphadenopathy, night sweats or weight loss (Fig. 12).
Fig. 12 
Chest radiograph (a) in a teenager who presented with weight loss and night sweats. The left mediastinal border is markedly abnormal with mass-like enlargement. A PET CT scan (b) shows intense uptake of FDG in the tumour. This is a non-Hodgkin’s lymphoma treated with radiotherapy and chemotherapy
-
-
Wilms tumour
-
The most common abdominal cancer in children.
-
It may present as abdominal mass in a child usually between the ages of 3–6 years. Cure rates are high with prompt recognition (Fig. 13).
Fig. 13 
A coronal image from a CT chest and abdomen with contrast which shows a large mass (arrow) arising from the left kidney. Histology confirmed a Wilms tumour
-


-
Osteosarcoma
-
The most common malignant tumour of the bone in children. These are aggressive appearing tumours with periosteal reaction, tumour bone formation and soft tissue swelling (Fig. 14).
Fig. 14 
Radiograph of the left femur in a 10 year old in a child who presented with pain and swelling. There is an aggressive osteosarcoma in the mid femur with a “sunburst” perisoteal reaction
-

Suggested Further Reading
-
Carty H, et al. Imaging children, 2nd ed. Churchill Livingstone;2005. ISBN-13: 978-0443070396.
-
Donnelly LF. Paediatric imaging: the fundamentals. Saunders;2009. ISBN: 978-1-4160-5907-3.
-
Applegate K, Anderson J, Klatte E, et al. Intestinal malrotation in children: a problem-solving approach to the upper gastrointestinal series. Radiographics. 2006;26 (5):1485–1500.
-
Darras E, Roston A, Yewchuk L, et al. Imaging acute airway obstruction in infants and children. Radiographics. 2015;35 (7):2064–79.
-
Fink K, Thapa M, Ishak G, et al. Neuroimaging of pediatric central nervous system cytomegalovirus infection. Radiographics. 2010;30 (7):1779–96
-
Gordon I, et al. Guidelines for standard and diuretic renal imaging in Children. Eur J Nucl Med Mol Imaging. https://doi.org/10.1007/s00259-011-1811-3.
-
Chao C, Zaleski C, Patton A, et al. Neonatal hypoxic-ischemic encephalopathy: multimodality imaging findings. Radiographics. 2006;26 (suppl_1):S159–S172
-
Offiah A, van Rijn RR, Perez-Rossello JM, et al. Skeletal imaging of child abuse (non-accidental injury). Pediatr Radiol. 2009;39:461. https://doi.org/10.1007/s00247-009-1157-1.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2020 Springer Nature Switzerland AG
About this chapter

Cite this chapter
Logan, C., Byrne, A., Ryan, S. (2020). Tutorial 13: Introduction to Paediatric Radiology. In: Redmond, C., Lee, M. (eds) Tutorials in Diagnostic Radiology for Medical Students. Springer, Cham. https://doi.org/10.1007/978-3-030-31893-2_13
Download citation
DOI: https://doi.org/10.1007/978-3-030-31893-2_13
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-31892-5
Online ISBN: 978-3-030-31893-2
eBook Packages: MedicineMedicine (R0)