
Abstract
Asthma is common in adults and in children. Asthma prevalence, morbidity, and mortality are not experienced equally in the United States. For decades, asthma health disparities have been known and interventions implemented, and yet the disparities continue. In this chapter, we describe the state of asthma health disparities and explanations for why they persist. We then discuss efforts in Chicago to reduce asthma health disparities. Multilevel, collaborative efforts are necessary to reduce asthma morbidity and mortality and provide equal access to care for all with asthma in the United States.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
Jayden
Jayden, a 17-year-old African American male living on the south side of Chicago, presented to the emergency room intubated and in septic shock. The last time he accessed the healthcare system was as an outpatient to a primary care physician at the age of 15. His chart indicated nonadherence to inhaled corticosteroids throughout his childhood, six hospitalizations, and no asthma subspecialist consultation. Spirometry from several years ago revealed severe obstruction that was fixed (unresponsive to albuterol). He had been intubated twice for asthma, at age 9 (when he had influenza) and age 13. He dropped out of high school this year because he missed too many school days. He started smoking cigarettes at 12 years of age and was smoking one pack per day at the time of admission. His nasal swab tested positive for influenza A. His mother revealed that he did not get the influenza vaccine because she had heard that the influenza vaccine makes you sick. He had been using his brother’s albuterol over the last week, but Jayden’s mother thinks the pump is empty now. Upon arrival, Jayden was immediately transferred to the pediatric intensive care unit. Unfortunately, he could not maintain oxygenation despite mechanical ventilation. He was placed on an oscillator, and the intensivists were preparing for extracorporeal membrane oxygenation when he coded and died.
Introduction
Asthma is a common disease of varying severity. When left untreated or inadequately treated, asthma can be fatal. Asthma deaths, in many cases, are considered preventable. In this case presentation, a child on the verge of adulthood died of a communicable disease called influenza that in the setting of asthma has increased risk of secondary bacterial infections and adverse outcomes [1,2,3]. Jayden’s death was preventable. Health disparities contributed to his poor asthma management, lack of medicine, refusal of the influenza vaccine, tobacco addiction, and late presentation for emergency care. This chapter will discuss how asthma health disparities relate to asthma prevalence, risk, outcomes, and management. Ways to mitigate these disparities will also be described, using Chicago as an example.
Existing Health Disparities in Asthma
Asthma is common in both adults and children, and its prevalence, morbidity, and mortality are not experienced equally in the United States. For decades, these asthma health disparities have been known and yet they continue. We will now review the current epidemiologic evidence of asthma health disparities.
Prevalence
Asthma prevalence for both children and adults increased steadily from 1980 to 1996 and then plateaued [4, 5]. The results of the National Health Interview Survey (NHIS) completed in 2016 through the Centers for Disease Control (CDC) reported an overall prevalence of current asthma as 8.3% [6]. The highest prevalence age group was in young adolescents aged 12–14 years (11.2%) [6]. Asthma was overall more common in females (9.7%) compared to males (6.9%), but in school-aged children, boys had more current asthma (9.2%) than girls (7.4%) [6]. Disparities in prevalence by race/ethnicity documented in the 1980s in both adults and children remain today [4, 6]. The highest prevalence of current asthma in 2016 by race was in non-Hispanic black (15.7%) and Puerto Rican (14.3%) children. Current asthma prevalence for non-Hispanic white children was 7.1% [6]. Asthma prevalence also varies by income level with an asthma prevalence of 11.8% in persons 100% below the poverty level, compared to 7.1% in those 450% of the poverty level or higher [6].
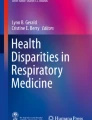
Asthma disparities are even more dramatic in certain urban areas. Data from the Medical Expenditure Panel Survey (MEPS) 2000–2014 database showed that low-income urban children throughout the country had some of the highest rates of asthma attacks and were less likely to use controller medicines. However, NHIS data from 2009 to 2011 suggested that non-Hispanic black race, Puerto Rican ethnicity, and low-income status were more powerful predictors of asthma prevalence than urban status [7]. In a school-based survey conducted in Chicago, asthma prevalence for children in non-Hispanic black neighborhoods was 19.9% compared to 11.4% in non-Hispanic white neighborhoods and 12.1% in Hispanic neighborhoods [8] (Fig. 7.1). While age, gender, family medical history of asthma, and neighborhood socioeconomic status were associated with asthma prevalence, they could not explain the differences seen between neighborhoods [8]. Race did explain a large portion of the variation between neighborhoods [8]. A population-based survey of asthma in Chicago reported that more than a third of Puerto Rican children had likely asthma. Non-Hispanic black children followed closely behind at 25% with likely asthma [9]. This is in comparison to 20% with likely asthma in non-Hispanic white children [9]. Cities like New York and Miami share similar statistics [10, 11].

Child asthma prevalence and race/ethnicity in Chicago. (Gupta et al. J Allergy Clin Immunol 2008)
Disparities also exist in rural areas where access issues are magnified, especially in the setting of poverty [12]. Most published literature and interventions focus on urban populations, leaving a gap in our understanding of asthma in rural populations. Although some studies report a lower prevalence of asthma in rural population [13] (others have shown similar prevalence) [14], there are significant access to care issues including location of clinics and potential problems related to quality of care [14]. In Arkansas, Pesek et al. reported that rural children were more likely to be labeled as having “chronic bronchitis” instead of asthma; this misdiagnosis has implications for their asthma management and surveillance [14]. Rural populations are more likely to have lower income and governmental insurance, compared to urban populations [13] and a higher risk of death [15]. Probst et al. attributed rural asthma disparities to these differences in income, education, and insurance coverage [15]. Limited access to asthma care extends to the school setting, where children spend a lot of time. School nurses in rural communities have been shown to have less access to asthma educational resources and to provide less asthma education to students [16, 17]. They also provide less asthma assessments and management, provide fewer referrals for asthma, and have reduced access to asthma specialists in comparison to urban communities [16, 17].
Environmental exposures are different in rural and urban areas, likely contributing to some of the differences in asthma prevalence. Nonatopic asthma, which has a different presentation and treatment approach than atopic asthma, may be more common in rural areas when certain exposures are present [18]. The hygiene hypothesis speculates a potential protective effect of farm and rural exposures related to the development of atopic asthma [19]. Additionally, rural areas’ reliance on biomass fuels constitutes another potential negative exposure; however, further studies need to be done to better understand these exposures [20].
Outcomes Related to Disparities in Asthma
Asthma health disparities are not limited to prevalence; certain population groups suffer worse asthma morbidity than others. This is demonstrated by differences in hospitalizations, emergency department (ED) visits, health status, asthma severity, and quality of life. National data demonstrated that ED use for non-Hispanic black adults and children was over two times greater than for non-Hispanic white adults and children; separating out for age did not modify these results [21]. These trends apply to a lower likelihood of outpatient asthma management as well, even for those with severe asthma [21]. Urban, minority children have been shown to have more daily asthma symptoms, exacerbations, ED visits, hospitalizations, less asthma action care plans, and less access to specialists [6, 22]. Inpatient asthma management also varies by race/ethnicity. Chandra et al. showed that 37% of Hispanic children compared to 60% of non-Hispanic white children and 63% of non-Hispanic black children received an asthma action plan at discharge [23].
Morbidity
Data from the Centers for Disease Control’s 2015 Behavioral Risk Factor Surveillance System (BRFSS) showed that adults with asthma were more likely to self-describe their health status as fair to poor opposed to the other options of good, very good, or excellent [24]. Specifically, individuals with asthma described their health as fair to poor 33.1% of the time compared to fair to poor health 15.9% of the time in those without asthma [24]. For school-aged children with asthma in Chicago, non-Hispanic white children had better quality of life and less severe asthma attacks compared to non-Hispanic black and Hispanic children; this difference could not be fully attributed to income differences [25]. In Chicago adults with asthma, Hispanic adults described a lower quality of life, and non-Hispanic black and Hispanic adults did worse compared to their non-Hispanic white counterparts in all outcomes related to asthma [26]. While socioeconomic status and health literacy partially explained these findings, nothing other than difference in race explained the higher hospitalization rates in non-Hispanic black adults [26].
Poorly controlled asthma can interfere with school attendance for children, affect academic performance, and cause parents to miss work. The number of reported missed school days among children with asthma from Centers for Disease Control data varies annually, from 12.4 million in 2003 to 13.8 million in 2013 [27]. Since the number of children with asthma has changed over time, another way to consider school attendance is the actual percentage of children with asthma who reported one or more asthma-related missed school days; these rates were 61.4% in 2003, 59.6% in 2008, and 49% in 2013 (49.0%) [27]. The reported missed school days in each year did not differ by age, sex, race or ethnicity, and poverty level [27]. However, data from state insurers and other sources suggest there is a disparity in missed school days for children with asthma and workdays for parents. For example, Lieu et al. reported more missed school days for non-Hispanic black and Hispanic children compared to non-Hispanic white children in their analysis of Medicaid-insured children [28]. Another study showed that urban minority children missed more school, experienced more asthma-related symptoms and healthcare utilization, and caregivers missed more work when compared to non-Hispanic white peers [22].
Mortality
National data shows that non-Hispanic black individuals with asthma are 2.8 times more likely to die from asthma than non-Hispanic white individuals [29]. Urban areas make up a disproportionate number of these deaths. In 1985, Cook County (Chicago area) and New York City accounted for 21.1% of all asthma deaths for 5–34-year-olds with asthma in the United States [30, 31]. The rate of asthma deaths decreased from 15 per million in 2001 (n = 4269) to 10 per million (n = 3518) in 2016 but this improvement is not experienced equally [32]. Non-Hispanic black adults and children remain much more likely to die from asthma [32]. The death rate for non-Hispanic black adults and children from 2016 was 22.3 per million compared to 8.2 per million in non-Hispanic whites [32]. Overall mortality rates for those of Hispanic ethnicity appear lower than non-Hispanic whites but when Hispanic subgroups are examined, Puerto Ricans have a higher mortality rate [33, 34].
Costs
If not swayed by the ethical dilemma surrounding disparate asthma outcomes, society must at least acknowledge the financial costs of asthma health disparities. Medical costs for asthma from 2008 to 2013 totaled $50.3 billion/year, with the average cost per person with asthma estimated to be $3266 per year [35]. The medical costs for those living under the poverty line were higher, at $3581 per person annually. Asthma-related mortality (which is largely preventable) cost another $29 billion/year [35]. Missing school and work also has a cost, reported as $3 billion/year [35]. These estimates do not include the long-term consequences of missed school such as future potential earnings.
Reasons for Asthma Health Disparities
Models for Examining the Etiology of Health Disparities
Before effective treatments can be developed and delivered, we need to understand two main things about asthma: (1) Why do some people develop asthma? and (2) What contributes to asthma morbidity and mortality? When considering health disparities, these questions become modified: Why are some population groups differentially affected in the development of asthma? Why do some population groups suffer worse asthma outcomes than others? Is it genetic? Environmental? Or a mixture of both, such as epigenetics?
We can begin to understand these questions by looking at asthma health disparities from the lens of the socioeconomic model (Fig. 7.2). At the individual level, factors such as genetics, comorbidities, and asthma management behaviors drive development of asthma and its outcomes. Household exposures and family dynamics contribute. At the organizational level, families receive varying degrees of guidelines-based asthma care depending on their healthcare access and quality. Community settings bring challenges of environmental exposures, violence, school factors, and issues such as collective efficacy. Finally, policy influences air quality and access to healthcare resources and medications.

Asthma Disparities Applied to the Socioecological Model
Even though many of the causes and influences of asthma fall outside the individual domain, children experiencing asthma health disparities bear a disproportionate burden. Children live in homes, under the care and influence of families. Modifiable factors such as beliefs, behaviors, and psychological stress come to play in homes. Homes are located in communities that may be prone to environmental factors like outdoor allergens, pollutions, and neighborhood stress. Children then interact with the healthcare system and providers, where operations and practices may not always be supportive of best care for the children. Finally, children also spend a huge portion of their time in schools which have a whole other set of modifiable and environmental factors. These different settings all impact the child and each other, but they do not communicate with each other except through the child/caregiver. For some families with low resources or skills, this burden is intolerable; they cannot bridge the settings (Fig. 7.3) [36, 37]. Primary care providers do not always know about ED visits. Parents sometimes do not get or give medicines.

The current burden of asthma on children and families. (Martin MA, et al. J Allergy Clin Immunol 2016)
Next, we will summarize some of the primary evidence of contributing factors to asthma. This is not an exhaustive review. These factors can have influences on the individual with asthma, as well as effects on offspring, household members, and communities.
Genetics and Epigenetics
Genetics are a known contributor to the development of asthma and also influence early respiratory infection severity which may contribute to future asthma persistence [38,39,40]. Overall, there are several distinct possible genetic predispositions to asthma that are hypothesized or correlated with the future development of asthma [39, 41,42,43,44,45,46,47,48,49,50,51,52], some specific to Hispanic populations [53]. No ethnic-specific asthma susceptibility gene has yet been defined in Hispanic subgroups [33, 54,55,56,57], making the genetic link likely more complex. There have been differences in single nucleotide polymorphisms that differentiate certain individuals with asthma to be more or less steroid responsive [58]. Some variants in the 17q21 locus seem to have the greatest effect on the pathogenesis of asthma in Puerto Ricans, but this still needs to be further validated [39, 55]. A review of genetic variants on the asthma susceptibility 17q21 locus showed possible, but inconsistent, connections to genetic polymorphisms seen in non-Hispanic black individuals [59]. Genetic variants in the Native American population are similar to the overall population in terms of common genetic variants associated with an increased risk of asthma [60]. In a severe asthma cohort, biologic factors seemed to be related to asthma severity, but the nature of these factors was not entirely clear [61].
Not everyone with a genetic predisposition for asthma develops asthma, and some have more severe or less severe asthma for reasons we do not understand. This suggests that external factors might alter asthma expression. The best evidence of this to date are the impact of stress and trauma on DNA methylation and ability to respond to steroids [62, 63]. DNA methylation is the change of genetic expression based on exposure to various factors [63, 64]. Even in children with an identical twin with exactly the same DNA, the gene expression can be different based on the DNA methylation patterns [64]. In asthma, one example of this is the demonstrated links between genetic expression changes and airway epithelial cells [65,66,67,68,69,70,71,72], leading to airway cells that are more vulnerable to stress and skew toward a pro-inflammatory cytokine and expression milieu [73,74,75,76,77,78]. Environmental factors have been implicated in DNA methylation patterns in asthma [63, 79]. In a mouse model, these DNA methylation changes to gene expression can also be inherited to offspring [80].
Chronic stressors modulate lung development , airway epithelium, neuroendocrine and autonomic nervous system responses, and the immune system [81,82,83,84,85,86,87]. Stress can change the response to the adrenal axis and potentially create enhanced airway hyperactivity and obstruction to triggers [58, 88]. Even prenatally, cord blood mononuclear cells have been shown to produce a skewed Th2 cytokine milieu with increased IL13 production after dust mite stimulation [88, 89]. Prenatal psychosocial stressors in parents in two birth cohorts found an association with future diagnosis of childhood asthma [90, 91]. Postnatal stress induces both a pro-inflammatory Th1 response and Th2 via increased total IgE at 2 years of age [92, 93]. Stress has been shown to decrease expression of steroid-responsiveness genes, which may contribute toward reduced inhaled corticosteroid and/or oral glucocorticoid effectiveness in treatment of asthma [94, 95]. Additional stressors to the body including particulate matter have also been shown to change expression and lead to pro-inflammation markers increasing regardless of asthma status [96].
Minorities in the USA and those living in poverty are exposed to more stressors, which affect health negatively [97]. These stressors have been linked to both asthma development and worse asthma morbidity [86]. This has been shown in the setting of survivors of physical and sexual abuse in both minority women and children [98, 99]. Exposure to violence in the urban, minority community also affects wheeze in children [91, 100]. The everyday stressors that minority families living in poverty have to deal with can affect asthma control in children [101]. There is some evidence to believe that stressors may be modulated depending on coping mechanisms and resilience that an individual with asthma may have [102], further complicating this relationship between stress and asthma, but also offering a glimmer of hope in perhaps finding a target for potential intervention.
Comorbidities
Allergic Diseases
Allergic disease is a significant and common comorbidity in the setting of asthma. Allergies are often thought to be the precursor to asthma in the theory of the atopic march [103,104,105,106,107,108,109,110,111,112,113,114]. There are significant health disparities seen in other allergic diseases which can directly influence asthma. We will not expand on these in this chapter, as they will be extensively covered in other chapters in this book.
Obesity
Health disparities related to obesity exist, with more non-Hispanic black children being obese than non-Hispanic white children; these disparities are independent of asthma risk [115]. Obesity is a risk factor for asthma. Asthma prevalence is higher in overweight and obese children and adults, and epidemiologic data suggest that obesity precedes asthma development [116,117,118,119,120,121,122,123,124]. The mechanisms proposed to explain this association include reduced lung volume and tidal volume with obesity, low-grade systemic inflammation from obesity, obesity-related changes in adipose-derived hormones such as leptin and adiponectin, common genetics, common in utero conditions, common predisposing dietary factors, and comorbidities of obesity such as dyslipidemia, gastroesophageal reflux, sleep-disordered breathing, type 2 diabetes, and hypertension [121, 122]. Obesity also seems to contribute to greater asthma morbidity. A multicenter study by Belamarich et al. reported that inner-city children with asthma who were obese used more medicine, wheezed more, and had more unscheduled emergency department visits than children with asthma who were not obese [116]. Being overweight has been associated with more severe asthma in a cohort of inner-city non-Hispanic black and Hispanic children in New York [125]. Obese children with asthma exacerbations in an intensive care unit had longer hospital stays and required more medications than nonobese children [126].
Mental Health
Stress and mental health issues are worse in populations where health disparities exist. Depression and anxiety symptoms predict worse asthma outcomes, including increased functional impairment, severity of asthma, rescue medication use, and frequency of emotional triggers [127,128,129,130,131,132,133]. Mothers of children with asthma have been reported to have higher rates of depression and anxiety, and caregiver depression has been repeatedly associated with worse asthma severity [133,134,135,136,137,138,139,140,141]. A large cross-sectional analysis of the National Health and Nutrition Examination Survey (NHANES) demonstrated that adults with asthma who also have depression are two times more likely to have poor asthma outcomes for several indicators [142]. These findings have been shown in other studies as well [143, 144]. Non-Hispanic black women are at greater risk than other groups; this may be linked to the experience of racism [145]. Stress and depression distort perceptions of access and can serve as a barrier to seeking care, especially in urban, low-income communities [146, 147].
Behaviors
Non-Hispanic white populations have been shown to use inhaled corticosteroids, which are proven to help control asthma in most individuals, more frequently than other groups [148,149,150,151,152,153]. Despite the efficacy of inhaled corticosteroids, there is a low adherence to inhaled corticosteroids in all age and race/ethnic minority groups with persistent asthma [154, 155]. This includes never starting the medication at all, only filling the first month of the inhaler, or using the inhaler sub-optimally [154,155,156,157,158,159,160,161]. Studies show that minority groups are less likely to take offered daily controller inhalers prescribed to control asthma across all age groups [28, 136, 162,163,164,165,166,167]. When reviewing interventions to improve adherence in minority populations, many approaches have not been associated with improvements in study participants [168]. This is compounded by the episodic nature of asthma symptoms, perpetuating the beliefs that many have that asthma disappears and there is no need to take medication in periods of wellness [169].
Multiple factors likely contribute to worse adherence to controller medications in disadvantaged, minority populations; however, a primary marker seems to be race/ethnic minority status coupled with low socioeconomic status [162, 163]. Fear of inhaled steroid medications as well as beliefs such as inevitable dependence on the medications contribute to low adherence to inhaled controller medications in asthma [157, 170, 171]. These beliefs have been documented in both non-Hispanic black and Hispanic populations [167, 172,173,174]. Depression in caregivers and in patients with asthma of all ages can affect adherence to controller medications [136, 175,176,177].
Perceived discrimination has been linked with worse asthma outcomes. In the United States, our prior history of misconduct in research fuels this legitimate concern in minority populations [178]. In an analysis that combined two large datasets of predominantly minority youth, perceived discrimination was found to increase the likelihood of having poor asthma control in non-Hispanic black youth [179]. Race and discrimination can affect healthcare outcomes through conscious or unconscious bias, and through social or environmental stressors which can affect chronic disease outcomes, such as asthma [180]. Racial discrimination has been linked to a significant change in bronchodilator response in non-Hispanic black and Hispanic children with asthma which correlated with higher TNF-alpha, a pro-inflammatory cytokine [181].
Tobacco exposure is a risk factor for the development of asthma both in utero and postnatally [182,183,184], and worse asthma-related health outcomes [185]. The National Heart, Lung, and Blood Institute Expert Panel Report 3 guidelines cite B-level evidence for avoidance in pregnant women and in household contacts of children with asthma [186,187,188,189], and a grade A recommendation is made by the US Preventative Task Force [190]. The effects of smoking tobacco for adults and youth are well known, leading to worsened asthma, lung cancer, chronic obstructive pulmonary disease (COPD), and heart disease, among other factors [187, 190,191,192,193,194,195]. Tobacco use is not equal. Overall tobacco smoking rates are highest nationally for Puerto Ricans (28.5%), followed by non-Hispanic white adults (24.9%) [196]. The Centers for Disease Control published slightly lower rates by ethnicity: non-Hispanic white (15.2%), non-Hispanic black (14.9%), Native American (24.0%), and Hispanic (9.9%, without division of Latino subgroups). The CDC classifies a prevalence of 20.6% for “multi-race.” [197]
Exposure to secondhand smoke in the United States has been declining from 1988 to 2014, from 87.5% to 25.2% [198]. Secondhand smoke exposure is likely higher than what is self-reported. A review of the National Health and Nutrition Examination Survey (NHANES) data from 1999 to 2010 reported 6% exposure to tobacco in the home and 14% in the workplace; however, serum cotinine was detected in 40% of these individuals [199]. Those in lower socioeconomic brackets were found to be more likely to have secondhand smoke exposure [199]. Despite these reductions, non-Hispanic black and Hispanic children are disproportionately exposed to secondhand tobacco smoke compared to non-Hispanic white children [200,201,202,203]. Recent data links nicotine aerosols that may be delivered in an alternate device distinct from classic cigarettes with worsened asthma morbidity, so recent trends of these devices also carry significant risk to children [204].
These data indicate that secondhand smoke – despite decreasing smoking prevalence in the population – is common in both adults and children and more common in the same populations that have the worst asthma outcomes.
Influenza vaccination is important for adults and children with asthma. The Centers for Disease Control report that 46.7% of adults over the age of 18 with asthma are vaccinated compared to 39% of adults without asthma [205]. In children, these rates are higher with 63.7% of children with asthma receiving an influenza vaccination [205]. In adults, influenza vaccine rates are significantly different between non-Hispanic black and white adults [206].
Environmental Exposures
Environmental exposures and their control are essential to asthma care [187]. Some hypothesize that a key distinction in health disparities in asthma can be explained in large part by disproportionate amount of environmental exposures that minorities and those with low socioeconomic statuses are exposed to [207], many of which are unavoidable. In this section, we will describe modifiable and nonmodifiable exposures which are disproportionately affecting minorities in the United States.
Allergens
Allergen exposure can affect everyone who has atopic or allergic asthma, and avoidance or mitigation of triggers is a key part of guideline-based asthma care [187]. There is a relationship between exposure of allergens and sensitization to the allergens in children living in the inner-city [208], especially when allergens are present in the bedroom at home. The Childhood Asthma Management Program verified this for both cockroach and dust mite allergen [209]. Indoor allergen sensitization, especially cockroach, has been shown to be higher in non-Hispanic black and Mexican American children compared to non-Hispanic white children [209,210,211]. Further, those with the highest-risk asthma in a predominantly African American inner-city cohort were found to be more sensitized to mouse allergen as well as overuse of albuterol [212]. Other indoor allergens have also been associated with asthma in minority populations [213]. Pest and indoor allergen reduction strategies may be helpful in these cases [214], depending on the approach and the control the individuals have over the home environment. Studies have attributed much of the unavoidable indoor allergen exposure, such as cockroach, to dilapidated housing infrastructure [215, 216]. Some have proposed that interventions would need to be community-wide in order to make a meaningful impact on allergen exposure in asthma [217]. This phenomenon is best understood in children; the relationships between allergen exposure and health disparities are less studied in adults [218, 219].
Allergen exposure is not limited to homes. In the School Inner-City Asthma Study, exposure to mouse allergen in the school building was found to be associated with increased asthma symptom days and decreased Forced Expiratory Volume in one second or FEV1 [220, 221]. What was particularly interesting is that this effect was seen regardless of the allergen sensitization status, suggesting that those without mouse sensitization and that also had asthma were also negatively affected by the exposure [220]. A similar phenomenon is seen in high schools in regard to mouse and cockroach [222]. Newer studies are also suggesting that fungal spore exposure is another possible allergen in schools that can affect asthma morbidity [223, 224].
Allergen exposure and sensitization are important, as they relate to severity of asthma and asthma morbidity [225]. Sensitization is associated with increased risk of atopic diseases such as asthma, especially when skin tests demonstrate sensitization to multiple allergens [226,227,228]. For example, the quantity of airborne mouse allergen levels in inner-city homes has been shown to be directly correlated with asthma symptoms and worse asthma outcomes [229]. Mouse allergen exposure has also been connected to asthma severity in minorities [229,230,231]. Those children who were most atopic with asthma in the inner-city were shown to require greater amounts of medications, severity scores, and worse lung function [225]. In “difficult-to-control” asthma, asthma severity did not improve and remained difficult to control in those inner-city groups who had worse atopy and rhinitis scores [232]. These data demonstrate that allergen exposures in the inner-city directly affect asthma and remain a significant public health concern.
Air Quality and Pollution
Poor air quality and pollution influence asthma in many ways including the development of asthma [213, 233,234,235,236,237,238,239]. In inner-city schools reviewed for air quality, researchers found that fine particulate matter, nitric dioxide, carbon monoxide, and physical dilapidation of school buildings contributed to poor air quality in many inner-city schools [240, 241]. This was not an isolated incident – inner-city children and minority children with asthma across the country are exposed to significant pollution [242, 243]. Pollution increases asthma morbidity and mortality [244, 245], as well as affects lung function [234, 246]. One study in the Bronx reported that children with asthma exposed to higher pollution levels were 66% more likely to be hospitalized for their asthma [247].
The poor air quality that minorities are exposed to, coupled with other environmental exposures, can be directly linked to community housing infrastructure [248]. The National Institutes of Health recognized this threat and recently published a workgroup report on suggested areas of further research to better measure, understand, and intervene on quality concerns throughout the country, especially in the most vulnerable populations [249]. The American Thoracic Society also urges collaboration with public health efforts to combat the concept of “respiratory health equality” [250]. Segregation may play a role in how individuals react to pollution exposures [251]. It is possible that how one responds to air pollution may be dependent on psychosocial and genetic factors [243].
Occupational hazards also lead to poor respiratory health by either worsening asthma control or by contributing to the development of occupational asthma [252]. The risk of occupational hazard exposure is higher in minority populations [253, 254]. A recent review details significant work-related exposure experienced by adult immigrants within the United States, and in some cases, their children that can lead to adverse allergic and respiratory disease effects [255]. In Michigan, workers from minority racial/ethnic backgrounds were overrepresented in lower-paid jobs with greater occupational risks, with an increase in work-related asthma seen in non-Hispanic black adults along with silicosis and pesticide injury in Hispanic adults [256]. Increased efforts to protect minorities in the workplace are necessary to protect from exposures that can affect respiratory health and the overall health and well-being [257].
Healthcare Access and Quality
Insurance-related barriers are significant in minority populations, especially those individuals on public insurance [163, 258, 259]. Many clinics do not accept state insurance plans. In one study that looked at multiple clinics’ willingness to schedule patients with either state or private insurance, there was a 66% denial rate with state insurance compared to 11% for private insurance [258]. Minority status was associated with absence of referrals and chronic disease diagnosis [258]. Improving access and insurance coverage does improve healthcare disparities and should be more aggressively targeted for intervention [260].
Access to care issues directly affects asthma control [261]. In the inner-city, access to care is less and this disproportionately affects minorities. Non-Hispanic black children with asthma use more emergency services, and less use of ambulatory and asthma specialty services than non-Hispanic white children [262]. This is a missed opportunity for prevention. Inner-city minority children also lack asthma care plans, are less likely to be referred to an asthma specialist, and are more likely to utilize emergency services overall [22]. Looking at parental perspectives, these barriers are so prominent that parents believe that seeking emergency services for asthma is usual care [263].
Access to medications is affected by insurance status [264, 265]. The patient costs related to prescriptions create a barrier [266, 267]. Inner-city children with asthma are less likely to be prescribed the medications they require for their asthma [268]. When research assistants looked into the medications available in the home of Puerto Rican youth in Chicago with persistent asthma, 74.9% had a quick reliever and 48.6% had a controller [269]. This means that one in four children was without a potentially life-saving reliever medication available to them in their home. Further, only 35.6% of children were able to properly identify >70% of steps in how to take their inhaler [269]. There is a clear disconnect at every level in the treatment of asthma, which emphasizes the need to target interventions to consider the many facets of health disparities in asthma.
Guideline-based asthma care [187] is often not routinely followed by practitioners in the United States for multiple reasons; some studies suggest that this is worse in minority populations [268, 270,271,272,273]. Despite difficulty in implementing guidelines, their implementation works to improve asthma control and therefore should be the standard of care for all. Care may also be influenced by the homogeneity of providers, racism, and implicit bias toward racial minorities [274,275,276]. Language barriers between providers and patients can also influence adherence to medications and affect asthma management, especially in elderly Hispanic populations [277, 278]. Educating providers on guideline-based asthma care has been shown to increase inhaled corticosteroid prescription rates, but not to address the other barriers to adherence [279]. Coordinated efforts to improve access to care and remove system-level barriers can improve systematic health disparities in asthma and have the potential to improve health in minorities [280].
Lastly, adolescents as a group pose a slightly different challenge to asthma care. Adolescents are less likely to seek healthcare, thus compromising access further [281]. In asthma, there is significant stigma against the use of inhalers, which further complicates this issue [282, 283]. Adherence in adolescents with asthma to controllers is particularly low [283]. Minority teens are more likely to die and have significant morbidity from asthma than other age groups [262]. Beliefs may affect adherence to medications, access to care, and asthma perception [284]. Adolescent perception of asthma symptoms may not be accurate or congruent with parent’s perception [285]. Transition to adult care may also be an area that may be difficult to gauge in adolescents with asthma, with some adolescents demonstrating readiness more than others [286].
Potential Solutions to Asthma Disparities: Community-Driven Intervention Development in Chicago
The multifactorial nature of asthma and asthma disparities require innovative solutions that target problems at multiple levels and engage all stakeholders. Chicago serves as an example of this type of approach. Termed “Asthma’s Ground Zero,” Chicago is an example of how to leverage community organization and data to drive research and policy initiatives aimed at improving asthma outcomes for all and eliminating asthma disparities.
Defining Asthma in Chicago
Chicago’s asthma epidemic was highlighted early, through detailed analyses of mortality data [30]. From 1980 to 2002, non-Hispanic black adults were nearly eight times more likely to die from asthma than non-Hispanic white adults [287]. The Illinois Department of Public Health funded numerous surveillance initiatives to monitor asthma in EDs throughout Chicago and the State. Data from 2011 showed that while 74% of adults in the EDs had moderate/severe asthma, only 46% were taking an inhaled corticosteroid [288]. Thirty-nine percent used more than one canister/month of albuterol and 27% had three or more ED visits in the past 12 months [288]. Data for children were similar. Adults and children were not receiving optimal guideline-based asthma care.
At the same time, several large research studies aimed to better characterize asthma disparities. One study conducted from 2003 to 2005 followed 353 adults and 561 children with asthma recruited from 105 Chicago schools [289]. The diagnosed asthma rate was 21.2% for non-Hispanic black children, compared to 9.7% for non-Hispanic white and 11.8% for Hispanic children [290]. Non-Hispanic black children were more than twice as likely and Hispanic children were 1.57 times more likely than non-Hispanic children to have diagnosed asthma [290]. This persisted at all school district income levels even when controlling for other household members with asthma, type of school, age of the child, gender, and language preference [290]. Non-Hispanic white children and adults had better asthma-specific quality of life and fewer severe asthma exacerbations compared to non-Hispanic black and Hispanic children and adults [25]. While non-Hispanic white children also had fewer days with asthma symptoms, no ethnic differences in the frequency of asthma symptoms were seen among adults [25]. Socioeconomic status was shown to mediate race/ethnic disparities in asthma outcomes [291]. Asthma prevalence was also associated with neighborhood race/ethnicity, demonstrating the importance of neighborhood factors but raising questions about what neighborhood race/ethnicity actually represents [8].
A separate study screened for asthma in six diverse Chicago neighborhoods from 2002 to 2003. Data were gathered from 1699 adults and 811 children (ages 0–12 years). Rates of physician-diagnosed asthma for adults were 18–19% in three of the neighborhoods, compared to 11% nationally [9]. These three neighborhoods were low-income and primary non-Hispanic black and Puerto Rican ethnicity. In two neighborhoods, almost half of adults with asthma reported poor asthma control [9]. Rates were even higher for children. Twenty-one percent of Puerto Rican children and 16% of non-Hispanic black children had physician-diagnosed asthma [9]. When children with probable asthma (due to report of significant asthma symptoms) were added, 33% of Puerto Rican children and 25% of non-Hispanic black children had likely asthma [9]. Over half of children with potential asthma had been to the ED in the past year with asthma-related symptoms. In three neighborhoods, 48–59% of children with diagnosed asthma lived with a smoker [9, 292].
The Chicago Department of Public Health analyzed city-level data from 2011 on asthma. The overall Chicago rate of asthma-related ED visits for children was 147 per 10,000 but the rate for non-Hispanic black children was double [293]. Asthma prevalence was concentrated in certain zip codes, mainly on the west and south side where the majority of residents are non-Hispanic black and Hispanic [293]. The map of child asthma ED visits mirrors almost exactly the map of child “low opportunity index” [293]. Analysts calculated the low opportunity index using measures of relative opportunity that include access to daycare centers, parks, and schools [294]. Nearly one in two children living in a low opportunity index was non-Hispanic black or Hispanic, compared to 1 in 50 non-Hispanic white children [293].
Intervention Development and Testing
One of the main interventions developed to combat the asthma crisis in Chicago involved asthma community health workers (CHWs). CHWs are frontline public health workers who are trusted members of and/or have an unusually close understanding of the community served [295]. The Sinai Urban Health Institute (the research arm of the Sinai Health System) began testing CHW asthma interventions in 2001. They trained laypeople to deliver home and hospital-based asthma education and support services for high-risk families. Their programs for both adults and children showed a reduction in asthma ED visits and hospitalizations by 50–80%, decreased symptom frequency, improved quality of life, and a cost saving of $3–8 for every dollar spent [296]. Other child-focused CHW studies using rigorous designs determined that CHW programs need to be community-wide, not targeted at just one population group [297]. Four home visits were not adequate to achieve improved asthma control [297]. CHWs needed to be formally connected with clinical partners, and mental health issues were impacting asthma control significantly [297, 298].
School-based asthma management programs are also being developed to address the high burden of asthma reported in schools. For over 100 years, the Respiratory Health Association has been educating and advocating in the Chicago area regarding asthma and other lung health issues. They created a program called Fight Asthma Now©, which is an evidence-based curriculum delivered to youth in schools [299]. The Respiratory Health Association also developed the Asthma Management program for adults interacting with children with asthma. This is delivered to parents, school staff, childcare providers, and park district staff.
Collaboration to Challenge Asthma
Chicago has a long history of health advocacy and collaboration. The epidemiologic data from the 1990s were so concerning that leaders in asthma research and advocacy founded the Chicago Asthma Consortium in 1996 to specifically address asthma disparities [300]. In 2003, the Chicago Emergency Department Asthma Collaborative began citywide quality improvement initiatives at 28 local hospitals. This effort expanded statewide into the Illinois Emergency Department Asthma Surveillance Project, monitoring 70 EDs throughout Illinois. Researchers at multiple institutions coordinated asthma interventions to maximize the community and scientific impacts [301]. But disparities persisted. In May of 2012, the Academic Chicago EMED Collaborative to Improve Public Health: Focus on Asthma was convened in Chicago. Attendees represented academic, governmental, and social service institutions from throughout the Chicago area. After reviewing data and discussion, the Collaborative expressed interest in moving forward to seek additional funding. The Coordinated Healthcare Interventions for Childhood Asthma Gaps in Outcomes (CHICAGO) Plan idea was formed.
With funding from a Patient-Centered Outcomes Research Institute (PCORI) award, the CHICAGO Plan moved forward an initiative to develop and test interventions to improve asthma outcomes for high-risk children presenting to EDs. This began in June of 2014 with a public stakeholder meeting on the emergency management of asthma led by the Chicago Asthma Consortium. A formative assessment was then conducted that involved focus groups, interviews, and observations with families and healthcare providers and nurses in EDs, outpatient settings, and homes [302]. In the EDs, patient education was found to be positioned at the weakest moment and the discharge experience was often fragmented. In homes, families had a lot of challenges getting and using medicines properly. They could not get or attend follow-up appointments. Families did not have good ways to coordinate care and share information within the families. Discharge information was stored out of sight. Finally, caregivers had an incomplete understanding of asthma [302]. These data led to the creation of a new ED discharge tool called the CHICAGO Action Plan after ED discharge (CAPE) [303].
The CHICAGO Plan then conducted a three-arm randomized controlled trial. All groups received routine ED care and basic inhaler instruction. Group 1 served as the comparison arm. Group 2 also received the CAPE. Group 3 received the CAPE and five home CHW visits [304]. Despite involvement of six clinical centers, recruitment from the ED was difficult and retention at 6 months was 63%. Of the 373 children enrolled, no difference was seen in asthma outcomes at 6 months. However, families in the arms receiving the CAPE were more likely to receive guideline-based asthma care in the ED [305].
As this trial was being conducted in EDs, investigators and partners explored opportunities to expand asthma care. The CHICAGO Plan II study was funded by an award from the National Institutes of Health (U34HL130787). Led by a team of five principal investigators from two health systems, Respiratory Health Association, and the Chicago Asthma Consortium, the group set out to conduct a community-based needs assessment for childhood asthma. Using a mixed-methods approach, 162 different stakeholders were engaged, 9 citywide project meetings were held, and 31 small meetings were conducted. Stakeholders came not only from individual patients/families and hospital and healthcare systems but also from schools, the Chicago Department of Public Health, the Chicago Housing Authority, the Illinois Institute of Technology Institute of Design, multiple advocacy organizations, and health insurance payers. The results showed the lines of communication and collaboration between stakeholders (hospitals, EDs, clinics, families, and schools) were weak; caregivers were the only consistent force and could not always manage this burden [37]. Recommendations for interventions and how to implement them were generated. The main interventions needed were CHWs that were based outside the healthcare setting, to maintain their skills and support, and to be able to follow families wherever they go. An electronic version of the CAPE was recommended, to allow families to communicate their children’s asthma plan with other family, schools, and healthcare providers. School-based asthma education was also identified as a need [37].
Because of the close collaboration with the Chicago Department of Public Health on the CHICAGO Plan II, these interventions are now part of Chicago’s strategic plan for asthma. Asthma CHW programs are being implemented and tested in a variety of formats and settings to determine integration protocols, dosing, and reimbursement opportunities. A digital version of the CAPE was created and is ready for testing. Asthma education continues in schools throughout Chicago. Researchers and schools are also working closely together to identify strategies for expanding asthma services [306, 307]. These will include identification of high-risk schools and school-specific asthma needs assessments and supports provided by CHWs. Clinical asthma services continue to be provided in partnership with schools in mobile asthma clinics from Mobile Care Chicago.
Asthma Policy Efforts
While efforts to improve asthma for individuals usually constitute the main discussion of asthma interventions, policy efforts deserve attention as well. Changes on a policy level can have drastic impacts on many. As shown in Fig. 7.4, asthma has been supported by a range of policy efforts over the last two decades. Much of these policies are related to schools. First, school code was modified to allow children to self-administer and carry asthma medication. The asthma emergency response protocol in 2016 gave schools more ability to care for children in emergencies. As of 2018, schools now have a policy allowing the use of stock albuterol which is critical for ensuring non-expired medication is available and used when needed. These policies were supported by expansions in health insurance and Medicaid that provided more access to healthcare coverage and medications for children and their families.

Asthma-related policy achievements in Chicago
Conclusion and Final Remarks
Jayden’s death, like the deaths of many others with asthma, was preventable. Multiple systematic failures contributed to his death. Despite having severe, persistent asthma with fixed obstruction from years of chronic inflammation, he had not successfully been seen by an asthma subspecialist. Perhaps, he had been referred and never went. If that was the reason, he may not have gone because of insurance barriers. Perhaps, the asthma subspecialist was very far away and his family could not take the time off work to bring him or afford the transportation and parking costs. Very likely, he was not referred, which happens frequently in urban minority populations [22, 258]. A primary care provider could have managed his asthma with additional medications according to guideline-based asthma care [187]. Unfortunately, young males are the least likely to seek healthcare [281] and not all primary care providers follow evidence-based asthma guidelines [271, 272]; this is more common in low-income neighborhoods [266, 267]. He might not have been adherent to those medications even if they were prescribed; he did not have his own albuterol inhaler at the time of his admission to the hospital. Asthma medications can be very expensive, confusing to use, and are felt to be socially unacceptable by adolescents [269, 282, 308, 309]. He did not receive an influenza vaccination. Influenza vaccine adherence is low overall and even lower in African American communities [206]. He may have been offered it and refused, but it also may not have been available to him if he did not go to a clinic. He and his family did not fully comprehend his asthma symptoms or the severity of his illness, as they waited too long to seek emergency care. Blame for Jayden’s death cannot be assigned to one person or component of the system. Many factors conspired to create an environment that led to the worst possible outcome.
Models of health disparities in asthma cite multiple factors related to the health disparities that work in parallel to negatively impact asthma management [162]. To combat health disparities, we need to take into consideration these multiple factors and realize that systematic change requires complex partnerships, collaboration, and multilevel interventions. While much remains unknown about why asthma occurs, we do know how to treat asthma and prevent exacerbations. The goal of reducing health disparities is to ensure these treatments are accessed by all.
For individuals with asthma, we need to ensure they have healthy homes, families, and neighborhoods where their exposures to physical and emotional triggers are minimized. Children and adults with asthma need unrestricted access to the right medications and devices. They need education on asthma symptom and trigger recognition, and how to manage medication regimens. All with asthma deserve care from providers that practice guideline-based asthma care and are accessible. At schools and in the workplace, children and adults with asthma need an environmentally healthy environment with appropriate access to medications and communication with families and healthcare providers.
To move this agenda forward, health system reform and partnerships are essential. Partnerships include healthcare systems and families, and also public health departments, housing agencies, and school systems to support sustainable change. Implementation science is a field designed to bring about systematic changes and provides a structure for how to implement and evaluate these efforts.
Support of all with asthma to reach their potential by keeping them safe and healthy is a common goal. It should be our goal for both ethical and financial reasons to overcome asthma health disparities and ensure everyone can breathe and contribute to our society. While novel drug development and mechanistic bench research are important, ensuring equal access to known therapies and comparable outcomes for all should be prioritized at the same level, if not higher. The benefits to society would be many.
References
Nair HD, Brooks WA, Katz M, et al. Global burden of respiratory infections due to seasonal influenza in young children: a systematic review and meta-analysis. Lancet. 2011;378(9807):1917–30.
Wong KK, Jain S, Blanton L, et al. Influenza-associated pediatric deaths in the United States, 2004-2012. Pediatrics. 2013;132(5):796–804.
Centers for Disease Control and Prevention. The Flu Season. 2018; http://www.cdc.gov/flu/about/season/flu-season.htm. Accessed 18 April 2019.
Moorman JE, Rudd RA, Johnson CA, et al. National Surveillance for asthma — United States, 1980–2004. Morb Mortal Wkly Rep Surveill Summ. 2007;56(SS-8):1–54.
Moorman JE, Akinbami LJ, Bailey CM, et al. National surveillance of asthma: United States, 2001-2010. Vital Health Stat 3. 2012;(35):1–58.
Centers for Disease Control and Prevention. National Current Asthma Prevalence 2016. May 2018; https://www.cdc.gov/asthma/most_recent_national_asthma_data.htm. Accessed 18 April 2019.
Keet CA, McCormack MC, Pollack CE, Peng RD, McGowan E, Matsui EC. Neighborhood poverty, urban residence, race/ethnicity, and asthma: rethinking the inner-city asthma epidemic. J Allergy Clin Immunol. 2014;135(3):655–62.
Gupta RS, Zhang X, Sharp LK, Shannon JJ, Weiss KB. Geographic variability in childhood asthma prevalence in Chicago. J Allergy Clin Immunol. 2008;121(3):639–645.e631.
Whitman S, Williams C, Shah A. Sinai health system's community health survey: report 1. Sinai Health System: Chicago; 2004.
New York Health Department. 2017 health care disparities in New York State. New York State, 2017.
Beck-Sague CM, Arrieta A, Pinzon-Iregui MC, et al. Trends in racial and ethnic disparities in childhood asthma in Miami, Florida: 2005–2013. J Immigr Minor Health. 2018;20(6):1429–37.
Perry TTRM, Brown RH, Nick TG, Jones SM. Uncontrolled asthma and factors related to morbidity in an impoverished, rural environment. Ann Allergy Asthma Immunol. 2012;108(4):254–9.
Valet RS, Perry TT, Hartert TV. Rural health disparities in asthma care and outcomes. J Allergy Clin Immunol. 2009;123(6):1220–5.
Pesek RD, Vargas PA, Halterman JS, Jones SM, McCracken A, Perry TT. A comparison of asthma prevalence and morbidity between rural and urban schoolchildren in Arkansas. Ann Allergy Asthma Immunol. 2010;104(2):125–31.
Probst JC, Bellinger JD, Walsemann KM, Hardin J, Glover SH. Higher risk of death in rural blacks and whites than urbanites is related to lower incomes, education, and health coverage. Health Aff (Millwood). 2011;30(10):1872–9.
Huss K, Winkelstein M, Calabrese B, et al. Rural school nurses’ asthma education needs. J Asthma. 2001;38(3):253–60.
Carpenter DMER, Robers CA, Elio A, Prendergast M, Durbin K, Jones GC, North S. Urban-rural differences in school nurses’ asthma training needs and access to asthma resources. J Pediatr Nurs. 2017;36:157–62.
Lawson JA, Chu LM, Rennie DC, et al. Prevalence, risk factors, and clinical outcomes of atopic and nonatopic asthma among rural children. Ann Allergy Asthma Immunol. 2016;118(3):304–10.
Rönmark E, Lundbäck B, Jönsson E, Rönmark E, Lundbäck B, Platts-mills T. Different pattern of risk factors for atopic and nonatopic asthma among children – report from the obstructive lung disease in Northern Sweden Study. Allergy. 1999;54(9):926–35.
Jie Y, Isa ZM, Jie X, Ju ZL, Ismail NH. Urban vs. rural factors that affect adult asthma. Rev Environ Contam Toxicol. 2013;226:33.
Fitzpatrick AM, Gillespie SE, Mauger DT, et al. Racial disparities in asthma-related health care use in the National Heart, Lung, and Blood Institute’s Severe Asthma Research Program. J Allergy Clin Immunol. 2019;143:2052.
Flores G, Snowden-Bridon C, Torres S, et al. Urban minority children with asthma: substantial morbidity, compromised quality and access to specialists, and the importance of poverty and specialty care. J Asthma. 2009;46(4):392–8.
Chandra D, Clark S, Camargo CA. Race/ethnicity differences in the inpatient management of acute asthma in the United States. Chest. 2009;135(6):1527–34.
Centers for Disease Control and Prevention. Asthma and Fair or Poor Health. 2017; https://www.cdc.gov/asthma/asthma_stats/default.htm. Accessed 18 April 2019.
Evans AT, Sadowski LS, VanderWeele TJ, et al. Ethnic disparities in asthma morbidity in Chicago. J Asthma. 2009;46(5):448–54.
Curtis LM, Wolf MS, Weiss KB, Grammer LC. The impact of health literacy and socioeconomic status on asthma disparities. J Asthma. 2012;49(2):178–83.
Centers for Disease Control and Prevention. Asthma-related missed school days among children aged 5–17 Years. 2015; https://www.cdc.gov/asthma/asthma_stats/missing_days.htm. Accessed 18 April 2019.
Lieu TA, Lozano P, Finkelstein JA, et al. Racial/ethnic variation in asthma status and management practices among children in managed Medicaid. Pediatrics. 2002;109(5):857–65.
Centers for Disease Control and Prevention. Current asthma prevalence precents by age, United States: national health interview survey, 2015. 2017; https://www.cdc.gov/asthma/nhis/2015/table4-1.htm. Accessed 18 April 2019.
Weiss KBWD. Changing patterns of asthma mortality. Identifying target populations at high risk. JAMA. 1990;264(13):1683–7.
Weiss KB. Geographic variations in US asthma mortality: small-area analyses of excess mortality, 1981-1985. Am J Epidemiol. 1990;132:S107–15.
Centers for Disease Control and Prevention. Asthma as the underlying cause of death. 2018; https://www.cdc.gov/asthma/asthma_stats/asthma_underlying_death.html. Accessed 18 April 2019.
Rosser FJ, Forno E, Cooper PJ, Celedón JC. Asthma in Hispanics. An 8-year update. Am J Respir Crit Care Med. 2014;189(11):1316–27.
Hunninghake GM, Celedon JC. Asthma in Hispanics. Am J Respir Crit Care Med. 2006;173(2):143–63.
Nurmagambetov T, Kuwahara R, Garbe P. The economic burden of asthma in the United States, 2008-2013. Ann Am Thorac Soc. 2018;15(3):348–56.
Martin MA, Press VG, Nyenhuis SM, et al. Care transition interventions for children with asthma in the emergency department. J Allergy Clin Immunol. 2016;138(6):1518–25.
Martin MA, Kapheim MG, Erwin K, et al. Childhood asthma disparities in Chicago: developing approaches to health inequities. Fam Community Health. 2018;41(3):135–45.
Taussig LM, Wright AL, Holberg CJ, Halonen M, Morgan WJ, Martinez FD. Tucson Children’s respiratory study: 1980 to present. J Allergy Clin Immunol. 2003;111(4):661–75.
Moffatt MF, Kabesch M, Liang L, et al. Genetic variants regulating ORMDL3 expression contribute to the risk of childhood asthma. Nature. 2007;448(7152):470–3.
Matricardi PM, Illi S, Gruber C, et al. Wheezing in childhood: incidence, longitudinal patterns and factors predicting persistence. Eur Respir J. 2008;32(3):585–92.
Ober C. Perspectives on the past decade of asthma genetics. J Allergy Clin Immunol. 2005;116(2):274–8.
Ober C, Thompson EE. Rethinking genetic models of asthma: the role of environmental modifiers. Curr Opin Immunol. 2005;17(6):670–8.
Weiss ST, Raby BA, Rogers A. Asthma genetics and genomics 2009. Curr Opin Genet Dev. 2009;19(3):279–82.
Moffatt MF, Gut IG, Demenais F, et al. A large-scale, consortium-based genomewide association study of asthma. NEJM. 2010;363(13):1211–21.
Aoki T, Hirota T, Tamari M, et al. An association between asthma and TNF-308G/A polymorphism: meta-analysis. J Hum Genet. 2006;51(8):677–85.
Nishimura F, Shibasaki M, Ichikawa K, Arinami T, Noguchi E. Failure to find an association between CD14-159C/T polymorphism and asthma: a family-based association test and meta-analysis. Allergol Int. 2006;55(1):55–8.
Finkelstein Y, Bournissen FG, Hutson JR, Shannon M. Polymorphism of the ADRB2 gene and response to inhaled beta-agonists in children with asthma: a meta-analysis. J Asthma. 2009;46(9):900–5.
Hancock DB, Romieu I, Shi M, et al. Genome-wide association study implicates chromosome 9q21.31 as a susceptibility locus for asthma in mexican children. PLoS Genet. 2009;5(8):e1000623.
Himes BE, Hunninghake GM, Baurley JW, et al. Genome-wide association analysis identifies PDE4D as an asthma-susceptibility gene. Am Hum Genet. 2009;84(5):581–93.
Li X, Howard TD, Zheng SL, et al. Genome-wide association study of asthma identifies RAD50-IL13 and HLA-DR/DQ regions. J Allergy Clin Immunol. 2010;125(2):328–335.e311.
Mathias RA, Grant AV, Rafaels N, et al. A genome-wide association study on African-ancestry populations for asthma. J Allergy Clin Immunol. 2010;125(2):336–346.e334.
Sleiman PM, Flory J, Imielinski M, et al. Variants of DENND1B associated with asthma in children. NEJM. 2010;362(1):36–44.
Pino-Yanes M, Thakur N, Gignoux CR, et al. Genetic ancestry influences asthma susceptibility and lung function among Latinos. J Allergy Clin Immunol. 2014;135(1):228–35.
Gravel S, Zakharia F, Moreno-Estrada A, et al. Reconstructing native American migrations from whole-genome and whole-exome data. PLoS Genet. 2013;9(12):e1004023.
Galanter JM, Torgerson D, Gignoux CR, et al. Cosmopolitan and ethnic-specific replication of genetic risk factors for asthma in 2 Latino populations. J Allergy Clin Immunol. 2011;128(1):37–43.e12.
Yan Q, Brehm J, Pino-Yanes M, et al. A meta-analysis of genome-wide association studies of asthma in Puerto Ricans. Eur Respir J. 2017;49(5).
Szentpetery SE, Forno E, Canino G, Celedon JC. Asthma in Puerto Ricans: lessons from a high-risk population. J Allergy Clin Immunol. 2016;138(6):1556–8.
Chen E, Miller GE. Stress and inflammation in exacerbations of asthma. Brain Behav Immun. 2007;21(8):993–9.
Stein MM, Thompson EE, Schoettler N, et al. A decade of research on the 17q12-21 asthma locus: piecing together the puzzle. J Allergy Clin Immunol. 2018;142(3):749–764.e743.
Best LG, Azure C, Segarra A, et al. Genetic variants and risk of asthma in an American Indian population. Ann Allergy Asthma Immunol. 2017;119(1):31–36.e31.
Gamble CD, Talbott ED, Youk AP, et al. Racial differences in biologic predictors of severe asthma: data from the Severe Asthma Research Program. J Allergy Clin Immunol. 2010;126(6):1149–1156.e1141.
Stefanowicz D, Hackett T-L, Garmaroudi FS, et al. DNA methylation profiles of airway epithelial cells and PBMCs from healthy, atopic and asthmatic children. PLoS One. 2012;7(9):e44213.
Pascoe CD, Obeidat ME, Arsenault BA, et al. Gene expression analysis in asthma using a targeted multiplex array. BMC Pulm Med. 2017;17(1):189–14.
Fraga MF, Ballestar E, Paz MF, et al. Epigenetic differences Arise during the lifetime of monozygotic twins. Proc Natl Acad Sci U S A. 2005;102(30):10604–9.
Dunnill MS. The pathology of asthma, with special reference to changes in the bronchial mucosa. J Clin Pathol. 1960;13(1):27–33.
Amishima M, Munakata M, Nasuhara Y, et al. Expression of epidermal growth factor and epidermal growth factor receptor immunoreactivity in the asthmatic human airway. Am J Respir Crit Care Med. 1998;157(6 Pt 1):1907–12.
Trautmann A, Kruger K, Akdis M, et al. Apoptosis and loss of adhesion of bronchial epithelial cells in asthma. Int Arch Allergy Immunol. 2005;138(2):142–50.
Barbato A, Turato G, Baraldo S, et al. Epithelial damage and angiogenesis in the airways of children with asthma. Am J Respir Crit Care Med. 2006;174(9):975–81.
Fedorov IA, Wilson SJ, Davies DE, Holgate ST. Epithelial stress and structural remodelling in childhood asthma. Thorax. 2005;60(5):389–94.
de Boer WI, Sharma HS, Baelemans SM, Hoogsteden HC, Lambrecht BN, Braunstahl GJ. Altered expression of epithelial junctional proteins in atopic asthma: possible role in inflammation. Can J Physiol Pharmacol. 2008;86(3):105–12.
Hackett TL, Shaheen F, Johnson A, et al. Characterization of side population cells from human airway epithelium. Stem Cells. 2008;26(10):2576–85.
Hackett TL, Warner SM, Stefanowicz D, et al. Induction of epithelial-mesenchymal transition in primary airway epithelial cells from patients with asthma by transforming growth factor-beta1. Am J Respir Crit Care Med. 2009;180(2):122–33.
Hackett T-L, Singhera GK, Shaheen F, et al. Intrinsic phenotypic differences of asthmatic epithelium and its inflammatory responses to respiratory syncytial virus and air pollution. Am J Respir Cell Mol Biol. 2011;45(5):1090–100.
Kicic A, Sutanto EN, Stevens PT, Knight DA, Stick SM. Intrinsic biochemical and functional differences in bronchial epithelial cells of children with asthma. Am J Respir Crit Care Med. 2006;174(10):1110–8.
Mullings RE, Wilson SJ, Puddicombe SM, et al. Signal transducer and activator of transcription 6 (STAT-6) expression and function in asthmatic bronchial epithelium. J Allergy Clin Immunol. 2001;108(5):832–8.
Sampath D, Castro M, Look DC, Holtzman MJ. Constitutive activation of an epithelial signal transducer and activator of transcription (STAT) pathway in asthma. J Clin Investig. 1999;103(9):1353–61.
Holgate ST, Lackie P, Wilson S, Roche W, Davies D. Bronchial epithelium as a key regulator of airway allergen sensitization and remodeling in asthma. Am J Respir Crit Care Med. 2000;162(3 Pt 2):S113–7.
Lopez-Guisa J, Powers C, File D, Cochrane E, Jimenez N, Debley JS. Airway epithelial cells from asthmatic children differentially express proremodeling factors. J Allergy Clin Immunol. 2012;129(4):990–997.e996.
Esteller M. The necessity of a human epigenome project. Carcinogenesis. 2006;27(6):1121–5.
Hollingsworth JW, Maruoka S, Boon K, et al. In utero supplementation with methyl donors enhances allergic airway disease in mice. J Clin Investig. 2008;118(10):3462.
Forno E, Wang T, Qi C, et al. DNA methylation in nasal epithelium, atopy, and atopic asthma in children: a genome-wide study. Lancet Respir Med. 2019;7(4):336–46.
Rosenberg SL, Miller GE, Brehm JM, Celedón JC. Stress and asthma: novel insights on genetic, epigenetic, and immunologic mechanisms. J Allergy Clin Immunol. 2014;134(5):1009–15.
Yang IV, Pedersen BS, Liu A, et al. DNA methylation and childhood asthma in the inner city. J Allergy Clin Immunol. 2015;136(1):69–80.
Yang IV, Pedersen BS, Liu AH, et al. The nasal methylome and childhood atopic asthma. J Allergy Clin Immunol. 2017;139(5):1478–88.
Kang DH, Weaver MT. Airway cytokine responses to acute and repeated stress in a murine model of allergic asthma. Biol Psychol. 2010;84(1):66–73.
Yonas MA, Lange NE, Celedón JC. Psychosocial stress and asthma morbidity. Curr Opin Allergy Clin Immunol. 2012;12(2):202–10.
Bahreinian S, Ball GDC, Vander Leek TK, et al. Allostatic load biomarkers and asthma in adolescents. Am J Respir Crit Care Med. 2013;187(2):144–52.
Wright RJ, Cohen RT, Cohen S. The impact of stress on the development and expression of atopy. Curr Opin Allergy Clin Immunol. 2005;5(1):23–9.
Peters JL, Cohen S, Staudenmayer J, Hosen J, Platts-Mills TAE, Wright RJ. Prenatal negative life events increases cord blood IgE: interactions with dust mite allergen and maternal atopy. Allergy. 2012;67(4):545–51.
Klinnert MD, Nelson HS, Price MR, Adinoff AD, Leung DYM, Mrazek DA. Onset and persistence of childhood asthma: predictors from infancy. Pediatrics. 2001;108(4):e69.
Chiu Y-H, Coull BAP, Sternthal MJ, et al. Effects of prenatal community violence and ambient air pollution on childhood wheeze in an urban population. J Allergy Clin Immunol. 2013;133(3):713–722.e714.
Wright RO, Wright RJ, Finn P, et al. Chronic caregiver stress and IgE expression, allergen-induced proliferation, and cytokine profiles in a birth cohort predisposed to atopy. J Allergy Clin Immunol. 2004;113(6):1051–7.
Sternthal MJ, Coull BA, Chiu YH, Cohen S, Wright RJ. Associations among maternal childhood socioeconomic status, cord blood IgE levels, and repeated wheeze in urban children. J Allergy Clin Immunol. 2011;128(2):337–345.e331.
Miller GE, Chen E. Life stress and diminished expression of genes encoding glucocorticoid receptor and beta2-adrenergic receptor in children with asthma. Proc Natl Acad Sci U S A. 2006;103(14):5496–501.
Miller GE, Gaudin A, Zysk E, Chen E. Parental support and cytokine activity in childhood asthma: the role of glucocorticoid sensitivity. J Allergy Clin Immunol. 2009;123(4):824–30.
Iwanaga K, Elliott MS, Vedal S, Debley JS. Urban particulate matter induces pro-remodeling factors by airway epithelial cells from healthy and asthmatic children. Inhal Toxicol. 2013;25(12):653–60.
Matthews KA, Gallo LC. Psychological perspectives on pathways linking socioeconomic status and physical health. Annu Rev Psychol. 2011;62(1):501–30.
Cohen RT, Canino GJ, Bird HR, Celedon JC. Violence, abuse, and asthma in Puerto Rican children. Am J Respir Crit Care Med. 2008;178(5):453–9.
Coogan PF, Wise LA, O'Connor GT, Brown TA, Palmer JR, Rosenberg L. Abuse during childhood and adolescence and risk of adult-onset asthma in African American women. J Allergy Clin Immunol. 2013;131(4):1058–63.
Eldeirawi K, Kunzweiler C, Rosenberg N, et al. Association of neighborhood crime with asthma and asthma morbidity among Mexican American children in Chicago, Illinois. Ann Allergy Asthma Immunol. 2016;117(5):502–507.e501.
Bellin MH, Collins KS, Osteen P, et al. Characterization of stress in low-income, inner-city mothers of children with poorly controlled asthma. J Urban Health. 2017;94(6):814–23.
Chen EP, Strunk RC, Trethewey A, Schreier H, Maharaj N, Miller GE. Resilience in low-socioeconomic-status children with asthma: adaptations to stress. J Allergy Clin Immunol. 2011;128(5):970–6.
Guilbert TW, Morgan WJ, Zeiger RS, et al. Atopic characteristics of children with recurrent wheezing at high risk for the development of childhood asthma. J Allergy Clin Immunol. 2004;114(6):1282–7.
Gustafsson D, Sjoberg O, Foucard T. Development of allergies and asthma in infants and young children with atopic dermatitis a prospective follow-up to 7 years of age. Allergy. 2000;55(3):240–5.
Kapoor R, Menon CP, Hoffstad O, Bilker WP, Leclerc P, Margolis DJ. The prevalence of atopic triad in children with physician-confirmed atopic dermatitis. J Am Acad Dermatol. 2008;58(1):68–73.
Kulig M, Bergmann R, Klettke U, Wahn V, Wahn U, Tacke U. Natural course of sensitization to food and inhalant allergens during the first 6 years of life. J Allergy Clin Immunol. 1999;103(6):1173–9.
Martinez FD, Wright AL, Taussig LM, et al. Asthma and wheezing in the first six years of life. NEJM. 1995;332(3):133–8.
Novembre E, Cianferoni A, Lombardi E, Bernardini R, Pucci N, Vierucci A. Natural history of “intrinsic” atopic dermatitis. Allergy. 2001;56(5):452–3.
Ohshima Y, Yamada A, Hiraoka M, et al. Early sensitization to house dust mite is a major risk factor for subsequent development of bronchial asthma in Japanese infants with atopic dermatitis: results of a 4-year followup study. Ann Allergy Asthma Immunol. 2002;89(3):265–70.
Ricci G, Patrizi A, Baldi E, Menna G, Tabanelli M, Masi M. Long-term follow-up of atopic dermatitis: retrospective analysis of related risk factors and association with concomitant allergic diseases. J Am Acad Dermatol. 2006;55(5):765–71.
van der Hulst AE, Klip H, Brand PL. Risk of developing asthma in young children with atopic eczema: a systematic review. J Allergy Clin Immunol. 2007;120(3):565–9.
Wüthrich B, Schmid-Grendelmeier P. The atopic eczema/dermatitis syndrome: epidemiology, natural course, and immunology of the IgE-associated ("extrinsic") and the nonallergic ("intrinsic") AEDS. J Investig Allergol Clin Immunol. 2003;13(1):1–5.
Spergel JM, Paller AS. Atopic dermatitis and the atopic march. J Allergy Clin Immunol. 2003;112(6):S118–27.
Tham EH, Leung DY. Mechanisms by which atopic dermatitis predisposes to food allergy and the Atopic March. Allergy, Asthma Immunol Res. 2019;11(1):4–15.
Ogden CL, Carroll MD, Lawman HG, et al. Trends in obesity prevalence among children and adolescents in the United States, 1988-1994 through 2013-2014. JAMA. 2016;315(21):2292–9.
Belamarich PF, Luder E, Kattan M, et al. Do obese inner-city children with asthma have more symptoms than nonobese children with asthma? Pediatrics. 2000;106(6):1436–41.
Beuther DA, Weiss ST, Sutherland ER. Obesity and asthma. Am J Respir Crit Care Med. 2006;174(2):112–9.
Halfon N, Larson K, Slusser W. Associations between obesity and comorbid mental health, developmental, and physical health conditions in a nationally representative sample of US children aged 10 to 17. Acad Pediatr. 2013;13(1):6–13.
Dixon AE, Holguin F, Sood A, et al. An official American Thoracic Society workshop report: obesity and asthma. Proc Am Thorac Soc. 2010;7(5):325–35.
Chen YC, Dong GH, Lin KC, Lee YL. Gender difference of childhood overweight and obesity in predicting the risk of incident asthma: a systematic review and meta-analysis. Obes Rev. 2013;14(3):222–31.
Shore SA. Obesity and asthma: possible mechanisms. J Allergy Clin Immunol. 2008;121(5):1087–93; quiz 1094-1085.
Matricardi PM, Gruber C, Wahn U, Lau S. The asthma-obesity link in childhood: open questions, complex evidence, a few answers only. Clin Exp Allergy. 2007;37(4):476–84.
Castro-Rodriguez JA, Holberg CJ, Morgan WJ, Wright AL, Martinez FD. Increased incidence of asthmalike symptoms in girls who become overweight or obese during the school years. Am J Respir Crit Care Med. 2001;163(6):1344–9.
Gilliland FD, Berhane K, Islam T, et al. Obesity and the risk of newly diagnosed asthma in school-age children. Am J Epidemiol. 2003;158(5):406–15.
Luder E, Melnik TA, DiMaio M. Association of being overweight with greater asthma symptoms in inner city black and Hispanic children. J Pediatr. 1998;132(4):699–703.
Carroll CL, Bhandari A, Zucker AR, Schramm CM. Childhood obesity increases duration of therapy during severe asthma exacerbations. Pediatr Crit Care Med. 2006;7(6):527–31.
Kean EM, Kelsay K, Wamboldt F, Wamboldt MZ. Posttraumatic stress in adolescents with asthma and their parents. J Am Acad Child Adolesc Psychiatry. 2006;45(1):78–86.
McCauley E, Katon W, Russo J, Richardson L, Lozano P. Impact of anxiety and depression on functional impairment in adolescents with asthma. Gen Hosp Psychiatry. 2007;29(3):214–22.
Richardson LP, Lozano P, Russo J, McCauley E, Bush T, Katon W. Asthma symptom burden: relationship to asthma severity and anxiety and depression symptoms. Pediatrics. 2006;118(3):1042–51.
Weil CM, Wade SL, Bauman LJ, Lynn H, Mitchell H, Lavigne J. The relationship between psychosocial factors and asthma morbidity in inner-city children with asthma. Pediatrics. 1999;104(6):1274–80.
Wood BL, Lim J, Miller BD, et al. Family emotional climate, depression, emotional triggering of asthma, and disease severity in pediatric asthma: examination of pathways of effect. J Pediatr Psychol. 2007;32(5):542–51.
Feldman JM, Siddique MI, Morales E, Kaminski B, Lu SE, Lehrer PM. Psychiatric disorders and asthma outcomes among high-risk inner-city patients. Psychosom Med. 2005;67(6):989–96.
Feldman JM, Steinberg D, Kutner H, et al. Perception of pulmonary function and asthma control: the differential role of child versus caregiver anxiety and depression. J Pediatr Psychol. 2013;38(10):1091–100.
Easter G, Sharpe L, Hunt CJ. Systematic review and meta-analysis of anxious and depressive symptoms in caregivers of children with asthma. J Pediatr Psychol. 2015;40(7):623–32.
Ortega AN, Goodwin RD, McQuaid EL, Canino G. Parental mental health, childhood psychiatric disorders, and asthma attacks in island Puerto Rican youth. Ambul Pediatr. 2004;4(4):308–15.
Bartlett SJ, Krishnan JA, Riekert KA, Butz AM, Malveaux FJ, Rand CS. Maternal depressive symptoms and adherence to therapy in inner-city children with asthma. Pediatrics. 2004;113(2):229–37.
Kozyrskyj AL, Mai XM, McGrath P, Hayglass KT, Becker AB, Macneil B. Continued exposure to maternal distress in early life is associated with an increased risk of childhood asthma. Am J Respir Crit Care Med. 2008;177(2):142–7.
Cookson H, Granell R, Joinson C, Ben-Shlomo Y, Henderson AJ. Mothers' anxiety during pregnancy is associated with asthma in their children. J Allergy Clin Immunol. 2009;123(4):847–853.e811.
Lefevre F, Moreau D, Semon E, Kalaboka S, Annesi-Maesano I, Just J. Maternal depression related to infant's wheezing. Pediatr Allergy Immunol. 2011;22(6):608–13.
Wright RJ, Cohen S, Carey V, Weiss ST, Gold DR. Parental stress as a predictor of wheezing in infancy: a prospective birth-cohort study. Am J Respir Crit Care Med. 2002;165(3):358–65.
Bartlett SJ, Kolodner K, Butz AM, Eggleston P, Malveaux FJ, Rand CS. Maternal depressive symptoms and emergency department use among inner-city children with asthma. Arch Pediatr Adolesc Med. 2001;155(3):347–53.
Patel PO, Patel MR, Baptist AP. Depression and asthma outcomes in older adults: results from the national health and nutrition examination survey. J Allergy Clin Immunol Pract. 2017;5(6):1691–1697.e1691.
Choi HG, Kim J-H, Park J-Y, Hwang YI, Jang SH, Jung K-S. Association between asthma and depression: a National Cohort Study. J Allergy Clin Immunol Pract. 2019;7(4):1239–1245.e1231.
Trojan TDMD, Khan DAMD, DeFina LFMD, Akpotaire OBS, Goodwin RDP, Brown ESMDP. Asthma and depression: the Cooper Center longitudinal study. Ann Allergy Asthma Immunol. 2014;112(5):432–6.
Coogan PFS, Yu JMPH, O'Connor GTMD, Brown TAP, Palmer JRS, Rosenberg LS. Depressive symptoms and the incidence of adult-onset asthma in African American women. Ann Allergy Asthma Immunol. 2014;112(4):333–338.e331.
Laster N, Holsey CN, Shendell DG, McCarty FA, Celano M. Barriers to asthma management among urban families: caregiver and child perspectives. J Asthma. 2009;46(7):731–9.
Welkom JS, Hilliard ME, Rand CS, Eakin MN, Riekert KA. Caregiver depression and perceptions of primary care predict clinic attendance in head start children with asthma. J Asthma. 2015;52(2):176–82.
Davidson AE, Klein DE, Settipane GA, Alario AJ. Access to care among children visiting the emergency room with acute exacerbations of asthma. Ann Allergy. 1994;72(5):469–73.
Rand CS, Butz AM, Kolodner K, Huss K, Eggleston P, Malveaux F. Emergency department visits by urban African American children with asthma. J Allergy Clin Immunol. 2000;105(1):83–90.
Warman KL, Silver EJ, McCourt MP, Stein RE. How does home management of asthma exacerbations by parents of inner-city children differ from NHLBI guideline recommendations? National Heart, Lung, and Blood Institute. Pediatrics. 1999;103(2):422–7.
Ortega AN, Gergen PJ, Paltiel AD, Bauchner H, Belanger KD, Leaderer BP. Impact of site of care, race, and Hispanic ethnicity on medication use for childhood asthma. Pediatrics. 2002;109(1):E1.
Diaz T, Sturm T, Matte T, et al. Medication use among children with asthma in East Harlem. Pediatrics. 2000;105(6):1188–93.
Halterman JS, Yoos HL, Kaczorowski JM, et al. Providers underestimate symptom severity among urban children with asthma. Arch Pediatr Adolesc Med. 2002;156(2):141–6.
Rust G, Zhang S, Reynolds J. Inhaled corticosteroid adherence and emergency department utilization among Medicaid-enrolled children with asthma. J Asthma. 2013;50(7):769–75.
Bender BG, Pedan A, Varasteh LT. Adherence and persistence with fluticasone propionate/salmeterol combination therapy. J Allergy Clin Immunol. 2006;118(4):899–904.
Corrao G, Arfe A, Nicotra F, et al. Persistence with inhaled corticosteroids reduces the risk of exacerbation among adults with asthma: a real-world investigation. Respirology. 2016;21(6):1034–40.
Apter AJ, Boston RC, George M, et al. Modifiable barriers to adherence to inhaled steroids among adults with asthma: It’s not just black and white. J Allergy Clin Immunol. 2003;111(6):1219–26.
Morton RW, Everard ML, Elphick HE. Adherence in childhood asthma: the elephant in the room. Arch Dis Child. 2014;99(10):949–53.
Bollinger ME, Mudd KE, Boldt A, Hsu VD, Tsoukleris MG, Butz AM. Prescription fill patterns in underserved children with asthma receiving subspecialty care. Ann Allergy Asthma Immunol. 2013;111(3):185–9.
Wu AC, Butler MG, Li L, et al. Primary adherence to controller medications for asthma is poor. Ann Am Thorac Soc. 2015;12(2):161–6.
McNally KA, Rohan J, Schluchter M, et al. Adherence to combined montelukast and fluticasone treatment in economically disadvantaged african american youth with asthma. J Asthma. 2009;46(9):921–7.
Canino G, McQuaid EL, Rand CS. Addressing asthma health disparities: a multilevel challenge. J Allergy Clin Immunol. 2009;123(6):1209–17; quiz 1218-1209.
McQuaid EL. Barriers to medication adherence in asthma the importance of culture and context. Ann Allergy Asthma Immunol. 2018;121(1):37–42.
Kharat AA, Borrego ME, Raisch DW, Roberts MH, Blanchette CM, Petersen H. Assessing disparities in the receipt of inhaled corticosteroid prescriptions for asthma by Hispanic and non-Hispanic white patients. Ann Am Thorac Soc. 2015;12(2):174–83.
Lintzenich A, Teufel RJ, Basco WT Jr. Under-utilization of controller medications and poor follow-up rates among hospitalized asthma patients. Hosp Pediatr. 2011;1(1):8–14.
Mosnaim G, Li H, Martin M, et al. Factors associated with levels of adherence to inhaled corticosteroids in minority adolescents with asthma. Ann Allergy Asthma Immunol. 2014;112(2):116–20.
McQuaid EL, Vasquez J, Canino G, et al. Beliefs and barriers to medication use in parents of Latino children with asthma. Pediatr Pulmonol. 2009;44(9):892–8.
Riley WT, Pilkonis P, Cella D. Application of the National Institutes of Health Patient-reported Outcome Measurement Information System (PROMIS) to mental health research. J Ment Health Policy Econ. 2011;14(4):201–8.
Halm EA, Mora P, Leventhal H. No symptoms, no asthma - the acute episodic disease belief is associated with poor self-management among inner-city adults with persistent asthma. Chest. 2006;129(3):573–80.
Conn KM, Halterman JS, Lynch K, Cabana MD. The impact of Parents’ medication beliefs on asthma management. Pediatrics. 2007;120(3):e521–6.
Peterson-Sweeney K, McMullen A, Yoos HL, Kitzman H. Parental perceptions of their child's asthma: management and medication use. J Pediatr Health Care. 2003;17(3):118–25.
Koinis-Mitchell D, McQuaid EL, Friedman D, et al. Latino Caregivers' beliefs about asthma: causes, symptoms, and practices. J Asthma. 2008;45(3):205–10.
Sidora-Arcoleo K, Yoos HL, McMullen A, Kitzman H. Complementary and alternative medicine use in children with asthma: prevalence and sociodemographic profile of users. J Asthma. 2007;44(3):169–75.
George M, Birck K, Hufford DJ, Jemmott LS, Weaver TE. Beliefs about asthma and complementary and alternative medicine in low-income inner-city African-American adults. J Gen Intern Med. 2006;21(12):1317–24.
Bender B, Zhang L. Negative affect, medication adherence, and asthma control in children. J Allergy Clin Immunol. 2008;122(3):490–5.
Smith A, Krishnan JA, Bilderback A, Riekert KA, Rand CS, Bartlett SJ. Depressive symptoms and adherence to asthma therapy after hospital discharge. Chest. 2006;130(4):1034–8.
Krauskopf KA, Sofianou A, Goel MS, et al. Depressive symptoms, low adherence, and poor asthma outcomes in the elderly. J Asthma. 2013;50(3):260–6.
Shavers VL, Lynch CF, Burmeister LF. Racial differences in factors that influence the willingness to participate in medical research studies. Ann Epidemiol. 2002;12(4):248–56.
Thakur N, Barcelo NE, Borrell LN, et al. Perceived discrimination associated with asthma and related outcomes in minority youth the GALA II and SAGE II studies. Chest. 2017;151(4):804–12.
Williams DR. Race, socioeconomic status, and health the added effects of racism and discrimination. Ann N Y Acad Sci. 1999;896(1):173–88.
Carlson S, Borrell LN, Eng C, et al. Self-reported racial/ethnic discrimination and bronchodilator response in African American youth with asthma. PLoS One. 2017;12(6):e0179091.
Agabiti N, Mallone S, Forastiere F, et al. The impact of parental smoking on asthma and wheezing. SIDRIA Collaborative Group. Studi Italiani sui Disturbi Respiratori nell'Infanzia e l'Ambiente. Epidimiology. 1999;10(6):692.
Gergen PJ, Fowler JA, Maurer KR, Davis WW, Overpeck MD. The burden of environmental tobacco smoke exposure on the respiratory health of children 2 months through 5 years of age in the United States: third national health and nutrition examination survey, 1988 to 1994. Pediatrics. 1998;101(2):E81–6.
Gilliland FD, Li YF, Peters JM. Effects of maternal smoking during pregnancy and environmental tobacco smoke on asthma and wheezing in children. Am J Respir Crit Care Med. 2001;163(2):429–36.
Mannino DM, Moorman JE, Kingsley B, Rose D, Repace J. Health effects related to environmental tobacco smoke exposure in children in the United States: data from the third national health and nutrition examination survey. Arch Pediatr Adolesc Med. 2001;155(1):36–41.
McEvoy CT, Spindel ER. Pulmonary effects of maternal smoking on the fetus and child: effects on lung development, respiratory morbidities, and life long lung health. Paediatr Respir Rev. 2016;21:27–33.
National Asthma Education and Prevention Program, Third expert panel on the diagnosis and management of asthma. Expert panel report 3: guidelines for the diagnosis and management of asthma. In: National Heart L, and Blood Institute ed. Bethesda, 2007.
Hayatbakhsh MR, Sadasivam S, Mamun AA, Najman JM, Williams GM, O'Callaghan MJ. Maternal smoking during and after pregnancy and lung function in early adulthood: a prospective study. Thorax. 2009;64(9):810–4.
Stocks J, Hislop A, Sonnappa S. Early lung development: lifelong effect on respiratory health and disease. Lancet Respir Med. 2013;1(9):728–42.
Force USPST. Final recommendation statement: tobacco smoking cessation in adults, including pregnant women: behavioral and pharmacotherapy interventions 2017.
Khokhawalla SA, Rosenthal SR, Pearlman DN, Triche EW. Cigarette smoking and emergency care utilization among asthmatic adults in the 2011 asthma call-back survey. J Asthma. 2015;52(7):732–9.
Thomson NC, Chaudhuri R. Asthma in smokers: challenges and opportunities. Curr Opin Pulm Med. 2009;15(1):39–45.
Dockery DW, Speizer FE, Ferris BG Jr, Ware JH, Louis TA, Spiro A. Cumulative and reversible effects of lifetime smoking on simple tests of lung function in adults. Am Rev Respir Dis. 1988;137(2):286–92.
Troisi RJ, Speizer FE, Rosner B, Trichopoulos D, Willett WC. Cigarette smoking and incidence of chronic bronchitis and asthma in women. Chest. 1995;108(6):1557–61.
Strachan DP, Cook DG. Health effects of passive smoking. 6. Parental smoking and childhood asthma: longitudinal and case-control studies. Thorax. 1998;53(3):204–12.
Martell BN, Garrett BE, Caraballo RS. Disparities in adult cigarette smoking — United States, 2002-2005 and 2010-2013. Morb Mortal Wkly Rep. 2016;65(30):753–8.
Centers for Disease Control and Prevention. Current cigarette smoking among Adults in the United States. National Center for Chronic Disease Prevention and Health Promotion; 2019.
Tsai J, Homa DM, Gentzke AS, et al. Exposure to secondhand smoke among nonsmokers - United States, 1988-2014. MMWR Morb Mortal Wkly Rep. 2018;67(48):1342–6.
Gan WQ, Mannino DM, Jemal A. Socioeconomic disparities in secondhand smoke exposure among US never-smoking adults: the national health and nutrition examination survey 1988-2010. Tob Control. 2015;24(6):568–73.
Neophytou AM, Oh SS, White MJ, et al. Secondhand smoke exposure and asthma outcomes among African-American and Latino children with asthma. Thorax. 2018;73(11):1041–8.
Zhang X, Johnson N, Carrillo G, Xu X. Decreasing trend in passive tobacco smoke exposure and association with asthma in U.S. children. Environ Res. 2018;166:35–41.
Ciaccio CE, DiDonna A, Kennedy K, Barnes CS, Portnoy JM, Rosenwasser LJ. Secondhand tobacco smoke exposure in low-income children and its association with asthma. Allergy Asthma Proc. 2014;35(6):462–6.
Fedele DA, Tooley E, Busch A, McQuaid EL, Hammond SK, Borrelli B. Comparison of secondhand smoke exposure in minority and nonminority children with asthma. Health Psychol. 2016;35(2):115–22.
Bayly JE, Bernat D, Porter L, Choi K. Secondhand exposure to aerosols from electronic nicotine delivery systems and asthma exacerbations among youth with asthma. Chest. 2019;155(1):88–93.
Centers for Disesae Control and Prevention. Flu vaccination among children with current asthma. 2017; https://www.cdc.gov/asthma/asthma_stats/flu_vaccination_child.html. Accessed 18 April 2019.
Quinn SC, Jamison A, Freimuth VS, An J, Hancock GR, Musa D. Exploring racial influences on flu vaccine attitudes and behavior: results of a national survey of White and African American adults. Vaccine. 2017;35(8):1167–74.
Forno E, Celedón JC. Asthma and ethnic minorities: socioeconomic status and beyond. Curr Opin Allergy Clin Immunol. 2009;9(2):154–60.
Eggleston PA, Rosenstreich D, Lynn H, et al. Relationship of indoor allergen exposure to skin test sensitivity in inner-city children with asthma. J Allergy Clin Immunol. 1998;102(4):563–70.
Huss K, Adkinson NF, Eggleston PA, Dawson C, Van Natta ML, Hamilton RG. House dust mite and cockroach exposure are strong risk factors for positive allergy skin test responses in the childhood asthma management program. J Allergy Clin Immunol. 2001;107(1):48–54.
Pacheco CM, Ciaccio CE, Nazir N, et al. Homes of low-income minority families with asthmatic children have increased condition issues. Allergy Asthma Proc. 2014;35(6):467–74.
Kattan M, Mitchell H, Eggleston P, et al. Characteristics of inner-city children with asthma: the National Cooperative Inner-City Asthma Study. Pediatr Pulmonol. 1997;24(4):253–62.
Bollinger ME, Butz AS, Lewis-Land C, DiPaula F, Mudd S. Characteristics of inner city children with life-threatening asthma. J Allergy Clin Immunol. 2015;135(2):AB80.
Sharma HP, Hansel NN, Matsui E, Diette GB, Eggleston P, Breysse P. Indoor environmental influences on Children’s asthma. Pediatr Clin N Am. 2007;54(1):103–20.
Ahluwalia SK, Matsui EC. Indoor environmental interventions for furry pet allergens, pest allergens, and mold: looking to the future. J Allergy Clin Immunol Pract. 2018;6(1):9–19.
Rauh VA, Chew GL, Garfinkel RS. Deteriorated housing contributes to high cockroach allergen levels in inner-city households. Environ Health Perspect. 2002;110(2):323–7.
Arruda LK, Ferriani VPL, Vailes LD, Pomés A, Chapman MD. Cockroach allergens: environmental distribution and relationship to disease. Curr Allergy Asthma Rep. 2001;1(5):466–73.
Peters JL, Levy JI, Rogers CA, Burge HA, Spengler JD. Determinants of allergen concentrations in apartments of asthmatic children living in public housing. J Urban Health. 2007;84(2):185–97.
Wisnivesky JP, Sampson H, Berns S, Kattan M, Halm EA. Lack of association between indoor allergen sensitization and asthma morbidity in inner-city adults. J Allergy Clin Immunol. 2007;120(1):113–20.
Busse PJ, Lurslurchachai L, Sampson HA, Halm EA, Wisnivesky J. Perennial allergen-specific immunoglobulin E levels among inner-city elderly asthmatics. J Asthma. 2010;47(7):781–5.
Sheehan WJ, Permaul P, Petty CR, et al. Association between allergen exposure in inner-city schools and asthma morbidity among students. JAMA Pediatr. 2017;171(1):31–8.
Permaul P, Hoffman E, Fu C, et al. Allergens in urban schools and homes of children with asthma. Pediatr Allergy Immunol. 2012;23(6):543–9.
Chew GL, Correa JC, Perzanowski MS. Mouse and cockroach allergens in the dust and air in northeastern United States inner-city public high schools. Indoor Air. 2005;15(4):228–34.
Baxi SN, Sheehan WJ, Sordillo JE, et al. Association between fungal spore exposure in inner-city schools and asthma morbidity. Ann Allergy Asthma Immunol. 2019;122:610.
Baxi SN, Muilenberg ML, Rogers CA, et al. Exposures to molds in school classrooms of children with asthma. Pediatr Allergy Immunol. 2013;24(7):697–703.
Lu KD, Phipatanakul W, Perzanowski MS, Balcer-Whaley S, Matsui EC. Atopy, but not obesity is associated with asthma severity among children with persistent asthma. J Asthma. 2016;53(10):1033–44.
Arshad SH, Tariq SM, Matthews S, Hakim E. Sensitization to common allergens and its association with allergic disorders at age 4 years: a whole population birth cohort study. Pediatrics. 2001;108(2):e33.
Sheehan WJ, Rangsithienchai PA, Wood RA, et al. Pest and allergen exposure and abatement in inner-city asthma: a work group report of the American Academy of Allergy, Asthma & Immunology indoor allergy/air pollution committee. J Allergy Clin Immunol. 2010;125(3):575–81.
Lynch SV, Wood RA, Boushey H, et al. Effects of early-life exposure to allergens and bacteria on recurrent wheeze and atopy in urban children. J Allergy Clin Immunol. 2014;134(3):593–601.e512.
Matsui EC, Simons E, Rand C, et al. Airborne mouse allergen in the homes of inner-city children with asthma. J Allergy Clin Immunol. 2005;115(2):358–63.
Grant T, Aloe C, Perzanowski M, et al. Mouse sensitization and exposure are associated with asthma severity in urban children. J Allergy Clin Immunol Pract. 2016;5(4):1008–1014.e1001.
Ahluwalia SK, Peng RD, Breysse PN, et al. Mouse allergen is the major allergen of public health relevance in Baltimore City. J Allergy Clin Immunol. 2013;132(4):830–835.e832.
Pongracic JA, Krouse RZ, Babineau DC, et al. Distinguishing characteristics of difficult-to-control asthma in inner-city children and adolescents. J Allergy Clin Immunol. 2016;138(4):1030–41.
Dockery DW, Pope Iii CA. Acute respiratory effects of particulate air pollution. Annu Rev Public Health. 1994;15(1):107–32.
Nishimura KK, Galanter JM, Roth LA, et al. Early-life air pollution and asthma risk in minority children the GALA II and SAGE II studies. Am J Respir Crit Care Med. 2013;188(3):309–18.
Dockery DW. Health effects of particulate air pollution. Ann Epidemiol. 2009;19(4):257–63.
Guarnieri M, Balmes JR. Outdoor air pollution and asthma. Lancet. 2014;383(9928):1581–92.
Liu L, Poon R, Chen L, et al. Acute effects of air pollution on pulmonary function, airway inflammation, and oxidative stress in asthmatic children. Environ Health Perspect. 2009;117(4):668–74.
Barraza-Villarreal A, Sunyer J, Hernandez-Cadena L, et al. Air pollution, airway inflammation, and lung function in a cohort study of Mexico City schoolchildren. Environ Health Perspect. 2008;116(6):832–8.
Khreis H, Kelly C, Tate J, Parslow R, Lucas K, Nieuwenhuijsen M. Exposure to traffic-related air pollution and risk of development of childhood asthma: a systematic review and meta-analysis. Environ Int. 2017;100:1–31.
Majd E, McCormack M, Davis M, et al. Indoor air quality in inner-city schools and its associations with building characteristics and environmental factors. Environ Res. 2019;170:83–91.
Kravitz-Wirtz N, Teixeira S, Hajat A, Woo B, Crowder K, Takeuchi D. Early-life air pollution exposure, neighborhood poverty, and childhood asthma in the United States, 1990-2014. Int J Environ Res Public Health. 2018;15(6):1114.
Kanchongkittiphon W, Gaffin JM, Phipatanakul W. The indoor environment and inner-city childhood asthma. Asian Pac J Allergy Immunol. 2014;32(2):103–10.
Nardone A, Neophytou AM, Balmes J, Thakur N. Ambient air pollution and asthma-related outcomes in children of color of the USA: a scoping review of literature published between 2013 and 2017. Curr Allergy Asthma Rep. 2018;18(5):1–12.
Eggleston PA. The environment and asthma in US inner cities. Chest. 2007;132(5):782S–8S.
Bryant-Stephens T. Asthma disparities in urban environments. J Allergy Clin Immunol. 2009;123(6):1199–206.
Neophytou AM, White MJ, Oh SS, et al. Air pollution and lung function in minority youth with asthma in the GALA II (Genesenvironments and admixture in Latino Americans) and SAGE II (study of African Americans, asthma, genes, and environments) studies. Am J Respir Crit Care Med. 2016;193(11):1271–80.
Maantay J. Asthma and air pollution in the Bronx: methodological and data considerations in using GIS for environmental justice and health research. Health Place. 2007;13(1):32–56.
Servadio JL, Lawal AS, Davis T, et al. Demographic inequities in health outcomes and air pollution exposure in the Atlanta area and its relationship to urban infrastructure. J Urban Health. 2019;96(2):219–34.
Gold DR, Adamkiewicz G, Arshad SH, et al. NIAID, NIEHS, NHLBI, and MCAN workshop report: the indoor environment and childhood asthma-implications for home environmental intervention in asthma prevention and management. J Allergy Clin Immunol. 2017;140(4):933–49.
Celedón JC, Roman J, Schraufnagel DE, Thomas A, Samet J. Respiratory health equality in the United States: the American thoracic society perspective. Ann Am Thorac Soc. 2014;11(4):473–9.
Levy JI, Quiros-Alcala L, Fabian MP, Basra K, Hansel NN. Established and emerging environmental contributors to disparities in asthma and chronic obstructive pulmonary disease. Curr Epidemiol Rep. 2018;5(2):114–24.
Tarlo SM, Lemiere C. Occupational asthma. NEJM. 2014;370(7):640–9.
Steege AL, Baron SL, Marsh SM, Menéndez CC, Myers JR. Examining occupational health and safety disparities using national data: a cause for continuing concern. Am J Ind Med. 2014;57(5):527–38.
Gany F, Novo P, Dobslaw R, Leng J. Urban occupational health in the Mexican and Latino/Latina immigrant population: a literature review. J Immigr Minor Health. 2014;16(5):846–55.
Pappalardo AA, Mosnaim G. Immigrant respiratory health: a diverse perspective in environmental influences on respiratory health. Curr Allergy Asthma Rep. 2018;18(4):1–10.
Stanbury M, Rosenman KD. Occupational health disparities: a state public health-based approach: occupational health disparities. Am J Ind Med. 2014;57(5):596–604.
Smith CK, Bonauto DK. Improving occupational health disparity research: testing a method to estimate race and ethnicity in a working population. Am J Ind Med. 2018;61(8):640–8.
Bellinger JD, Hassan RM, Rivers PA, Cheng Q, Williams E, Glover SH. Specialty care use in US patients with chronic diseases. Int J Environ Res Public Health. 2010;7(3):975–90.
Shone LP, Dick AW, Brach C, et al. The role of race and ethnicity in the State Children’s Health Insurance Program (SCHIP) in four states: are there baseline disparities, and what do they mean for SCHIP? Pediatrics. 2003;112(6):e521–E532.
Shone LP, Dick AW, Klein JD, Zwanziger J, Szilagyi PG. Reduction in racial and ethnic disparities after enrollment in the state Children’s health insurance program. Pediatrics. 2005;115(6):e697–705.
Mansour ME, Lanphear BP, DeWitt TG. Barriers to asthma care in urban children: parent perspectives. Pediatrics. 2000;106(3):512–9.
Akinbami LJ, Moorman JE, Garbe PL, Sondik EJ. Status of childhood asthma in the United States, 1980-2007. Pediatrics. 2009;123(Supplement):S131–45.
Dinkevich EI, Cunningham SJ, Crain EF. Parental perceptions of access to care and quality of care for inner-city children with asthma. J Asthma. 1998;35(1):63–71.
Merrick NJ, Houchens R, Tillisch S, Berlow B, Landon C, Group M. Quality of hospital care of children with asthma: medicaid versus privately insured patients. J Health Care Poor Underserved. 2001;12(2):192–207.
Lantner R, Brennan RA, Gray L, McElroy D. Research, outcomes Committee of the Suburban Asthma C. Inpatient management of asthma in the Chicago suburbs: the Suburban Asthma Management Initiative (SAMI). J Asthma. 2005;42(1):55–63.
Frankenfield DL, Wei II, Anderson KK, Howell BL, Waldo DR, Sekscenski E. Prescription medication cost-related non-adherence among medicare CAHPS respondents: disparity by Hispanic ethnicity. J Health Care Poor Underserved. 2010;21(2):518–43.
Briesacher BA, Gurwitz JH, Soumerai SB. Patients at-risk for cost-related medication nonadherence: a review of the literature. J Gen Intern Med. 2007;22(6):864–71.
Riekert KA, Butz AM, Eggleston PA, Huss K, Winkelstein M, Rand CS. Caregiver-physician medication concordance and undertreatment of asthma among inner-city children. Pediatrics. 2003;111(3):e214–20.
Pappalardo AA, Karavolos K, Martin MA. What really happens in the home: the medication environment of urban, minority youth. J Allergy Clin Immunol Pract. 2017;5(3):764–70.
Hasegawa K, Stoll SJ, Ahn J, Kysia RF, Sullivan AF, Camargo CA. Association of insurance status with severity and management in ED patients with asthma exacerbation. West J Emerg Med. 2016;17(1):22–7.
Lingner H, Burger B, Kardos P, Criee CP, Worth H, Hummers-Pradier E. What patients really think about asthma guidelines: barriers to guideline implementation from the patients' perspective. BMC Pulm Med. 2017;17(1):13.
Fischer F, Lange K, Klose K, Greiner W, Kraemer A. Barriers and strategies in guideline implementation-a scoping review. Healthcare (Basel). 2016;4(3).
Finkelstein JA, Barton MB, Donahue JG, Algatt-Bergstrom P, Markson LE, Platt R. Comparing asthma care for Medicaid and non-Medicaid children in a health maintenance organization. Arch Pediatr Adolesc Med. 2000;154(6):563–8.
Paradies Y, Truong M, Priest N. A systematic review of the extent and measurement of healthcare provider racism. J Gen Intern Med. 2014;29(2):364–87.
Greenwald AG, McGhee DE, Schwartz JLK. Measuring individual differences in implicit cognition: the implicit association test. J Pers Soc Psychol. 1998;74(6):1464–80.
Sabin JA, Greenwald AG. The influence of implicit bias on treatment recommendations for 4 common pediatric conditions: pain, urinary tract infection, attention deficit hyperactivity disorder, and asthma. Am J Public Health. 2012;102(5):988–95.
Inkelas MP, Garro NMPH, McQuaid ELP, Ortega ANP. Race/ethnicity, language, and asthma care: findings from a 4-state survey. Ann Allergy Asthma Immunol. 2008;100(2):120–7.
Wisnivesky JP, Krauskopf KM, Wolf MS, et al. The association between language proficiency and outcomes of elderly patients with asthma. Ann Allergy Asthma Immunol. 2012;109(3):179–84.
Cloutier MM, Hall CB, Wakefield DB, Bailit H. Use of asthma guidelines by primary care providers to reduce hospitalizations and emergency department visits in poor, minority, urban children. J Pediatr. 2005;146(5):591–7.
Kercsmar CM, Beck AF, Sauers-Ford H, et al. Association of an asthma improvement collaborative with health care utilization in medicaid-insured pediatric patients in an urban community. JAMA Pediatr. 2017;171(11):1072–80.
Klein JD, McNulty M, Flatau CN. Adolescents’ access to care: Teenagers’ self-reported use of services and perceived access to confidential care. Arch Pediatr Adolesc Med. 1998;152(7):676–82.
Naman J, Press VG, Vaughn D, Hull A, Erwin K, Volerman A. Student perspectives on asthma management in schools: a mixed-methods study examining experiences, facilitators, and barriers to care. J Asthma. 2018:1–12.
KyngÄs HA, Kroll T, Duffy ME. Compliance in adolescents with chronic diseases: a review. J Adolesc Health. 2000;26(6):379–88.
Ahmad A, Sorensen K. Enabling and hindering factors influencing adherence to asthma treatment among adolescents: a systematic literature review. J Asthma. 2016;53(8):862–78.
Heyduck K, Bengel J, Farin-Glattacker E, Glattacker M. Adolescent and parental perceptions about asthma and asthma management: a dyadic qualitative analysis: adolescent and parental perceptions about asthma. Child Care Health Dev. 2015;41(6):1227–37.
Jones MR, Frey SM, Riekert K, Fagnano M, Halterman JS. Transition readiness for talking with providers in urban youth with asthma: associations with medication management. J Adolesc Health. 2019;64(2):265–71.
Naureckas E. Are we closing the disparities gap? Small-area analysis of asthma in Chicago. Chest. 2007;132(5 suppl):858S.
Health IDoP. Asthma burden update. 2013.
Weiss KB, Shannon JJ, Sadowski LS, et al. The burden of asthma in the Chicago community fifteen years after the availability of national asthma guidelines: the design and initial results from the CHIRAH study. Contemp Clin Trials. 2009;30(3):246–55.
Shalowitz MU, Sadowski LM, Kumar R, Weiss KB, Shannon JJ. Asthma burden in a citywide, diverse sample of elementary schoolchildren in Chicago. Ambul Pediatr. 2007;7(4):271–7.
Washington DM, Curtis LM, Waite K, Wolf MS, Paasche-Orlow MK. Sociodemographic factors mediate race and ethnicity-associated childhood asthma health disparities: a longitudinal analysis. J Racial Ethn Health Disparities. 2018;5(5):928–38.
Dell JL, Whitman S, Shah AM, Silva A, Ansell D. Smoking in 6 diverse Chicago communities--a population study. Am J Public Health. 2005;95(6):1036–42.
Dircksen JCPN, et al. Healthy Chicago 2.0: partnering to improve health equity. City of Chicago. In: Health CDoP, editor. . Chicago; 2016.
Management THSfSPa. Diversity Data kids. In. Waltham, MA: Brandeis University.
American Public Health Association Community Health Worker Section. http://www.dph.illinois.gov/sites/default/files/publications/healthy-smiles-09-050216.pdf. Accessed 15 April 2019.
Gutierrez Kapheim MCJ. Best practice guidelines for implementing and evaluating community health worker programs in health care settings: Sinai Urban Health Institute; 2014.
Martin MA, Mosnaim GS, Olson D, Swider S, Karavolos K, Rothschild S. Results from a community-based trial testing a community health worker asthma intervention in Puerto Rican youth in Chicago. J Asthma. 2015;52(1):59–70.
Martin MA, Floyd EC, Nixon SK, Villalpando S, Shalowitz M, Lynch E. Asthma in children with comorbid obesity: intervention development in a high-risk urban community. Health Promot Pract. 2016;17(6):880–90.
Mosnaim GS, Li H, Damitz M, et al. Evaluation of the Fight Asthma Now (FAN) program to improve asthma knowledge in urban youth and teenagers. Ann Allergy Asthma Immunol. 2011;107(4):310–6.
Naureckas ET, Wolf RL, Trubitt MJ, et al. The Chicago asthma consortium: a community coalition targeting reductions in asthma morbidity. Chest. 1999;116(4 Suppl 1):190s–3s.
Whitman S, Shah AM, Benjamins M. Urban health : combating disparities with local data. New York: Oxford University Press; 2011.
Martin MA, Press VG, Erwin K, et al. Engaging end-users in intervention research study design. J Asthma. 2017:1–9.
Erwin K, Martin MA, Flippin T, et al. Engaging stakeholders to design a comparative effectiveness trial in children with uncontrolled asthma. J Comp Eff Res. 2016;5(1):17–30.
Krishnan JA, Martin MA, Lohff C, et al. Design of a pragmatic trial in minority children presenting to the emergency department with uncontrolled asthma: the CHICAGO plan. Contemp Clin Trials. 2017;57:10–22.
Institute P-COR. Comparing three ways to prepare children and caregivers to manage asthma after an emergency room visit – the CHICAGO Trial. 2018; https://www.pcori.org/research-results/2013/comparing-three-ways-prepare-children-and-caregivers-manage-asthma-after. Accessed 18 April 2019.
Minier MHL, Ramahi R, Glassgow AE, Fox K, Martin M. An essential partnership for the effective care of children with chronic conditions. J School Health. 2017;88:699.
Pappalardo AA, Paulson A, Bruscato R, Thomas L, Minier M, Martin MA. Chicago public school nurses examine barriers to school asthma care coordination. Public Health Nurs. 2019;36(1):36–44.
Mahon J, Fitzgerald A, Glanville J, et al. Misuse and/or treatment delivery failure of inhalers among patients with asthma or COPD: a review and recommendations for the conduct of future research. Respir Med. 2017;129:98–116.
Volerman A, Toups MM, Hull A, Press VG. A feasibility study of a patient-centered educational strategy for rampant inhaler misuse among minority children with asthma. J Allergy Clin Immunol Pract. 2019;7:2028.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2020 Springer Nature Switzerland AG
About this chapter

Cite this chapter
Pappalardo, A.A., Martin, M.A. (2020). Asthma Health Disparities. In: Mahdavinia, M. (eds) Health Disparities in Allergic Diseases. Springer, Cham. https://doi.org/10.1007/978-3-030-31222-0_7
Download citation
DOI: https://doi.org/10.1007/978-3-030-31222-0_7
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-31221-3
Online ISBN: 978-3-030-31222-0
eBook Packages: MedicineMedicine (R0)