
Abstract
Implementing emerging technologies is a complex task which requires time, precision, and organization. The definition of a logical structure for classifying and organizing complex information during the design process of a technological solution provides flexibility while the process becomes more prescriptive. One of the most used methods in the ICT field is the user-centered design methodology (UCD). UCD methodology situates the final user as the cornerstone of the research and development process since the success or failure of a technological solution will depend on users’ acceptance. The following chapter presents experiences, best practices and lessons learned applying UCD methodology in different European projects from several years of work conducted at LifeSTech group from UPM, in areas such as: chronic diseases management, accessibility, and cognitive rehabilitation. Specifically, the chapter explains how the UCD methodology was applied during the different stages of the design and development process for different domains and use cases.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
1 Introduction
The development of ICT applications for the healthcare domain involves and requires the cooperation and interaction of multidisciplinary stakeholders (e.g., health professionals, end users, engineers, etc.) in order to guarantee the successful and acceptability of the developed applications. Because of the complexity of this interaction, different methodologies and frameworks are used to help ICT teams to include these actors during all the phases of the design and development process.
User-centered design is a design philosophy and process that considers the users and their requirements as the most important factor to improve the quality of designs. This process relies hardly on user’s continuous feedback during all phases of the design and development process of the solution [1]. The term ‘User-Centered Design’ was presented by Donald Norman in the publication of a co-authored book entitled: User-Centered System Design: New Perspectives on Human-Computer Interaction [2]. In this book, Norman et al. adapted and re-defined the participatory design concept into the user-centered design philosophy. Later, according to Abras et al. [3] Norman built further on the UCD and recognizes the needs of the user and the usability of the design, presenting four basic suggestions on how a design should be. These conditions are: (1) make it easy to determine what actions are possible at any moment; (2) make things visible, including the conceptual model of the system, the alternative actions, and the results of actions; (3) make it easy to evaluate the current state of the system; (4) follow natural mappings between intentions and the required actions, between actions and the resulting effect, and between the information that is visible and the interpretation of the system state.
Initially, UCD included several areas of basic and applied research such as: cognitive and social psychology, linguistics, mathematics, computer science, engineering, human factors and ergonomics, socio-technical systems design, scientific management, industrial and occupational psychology, human relations and organizational behavior [4]. Since 1992 UCD has been used also in the healthcare domain, addressing different focus areas such as elderly care, cognitive care, chronic diseases care, etc., [5]. It has been used as a method for the design and development of healthcare delivery systems such as mobile and web care devices and applications, emergency systems, self-management and decision support systems.
The most important phases of UCD when applied in relevant healthcare applications in domains like chronic diseases management [8] and cognitive rehabilitation [6, 7] are:
-
Needs and technical requirements identification: include the collection of users’ needs and their transformation into technological requirements. This could be done using different methods such as: interviews, observations, questionnaires, workshops, and focus groups.
-
Definition of use cases: refers to the description, during the design process, of the user actions and all possible interactions with the system.
-
Validations: is the phase when users test the proposed solution and give their feedback. This process could involve different assessment methods such as: heuristic evaluation, usability tests, end user evaluation, pre- and post-survey, among others.
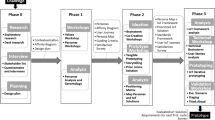
UCD phases can be adapted to the design and the develop process of an ICT solution as shown in Fig. 9.1, where five stages of the development are described as follow:

An example of the user-centered design methodology in health care
-
Needs: Research about the needs of the potential users of the solution.
-
Methods: Analyze the existing technologies in the domain of your solution.
-
Design: Provide a proposal of the solutions, define functionalities based on the user needs.
-
Development: The proposed solution.
-
Evaluation: Perform with potential users and redefine if needed.
In this chapter, we present the UCD methodology applied in different ICT healthcare-related and research-based projects hosted by our research group. Because of the diversity of these projects, we present them divided based on their focus domain. Specifically, we present some important aspects and ways of applying UCD for different use cases, adaptations that should be taken into consideration when applying UCD in certain scenarios, and the outcomes, most important insights, lessons learned, and recommendations gathered from these experiences that could help researchers and developers to deliver better solutions.
2 Applying UCD in Different Domains
In this section, we present our experiences, best practices, and recommendations applying UCD in high impact ICT European projects, form the Life Supporting Technologies group, in areas such as: chronic diseases management, accessibility and cognitive rehabilitation, and training.
2.1 Chronic Diseases Self-management
According to the World Health Organization, chronic diseases are responsible for almost 70% of all deaths worldwide. In addition, 82% of the 16 million people who died before reaching age 70 due to chronic diseases take place in low- and middle-income countries. These types of diseases have shown to produce devastating health consequences for individuals, families, and communities [9].
The self-management of chronic diseases is one of the most used techniques nowadays because it gives the patient the tools to manage and improve their condition. The management skills provided by a self-management program include problem solving, decision making, resource utilization, establishing a patient–caregiver partnership, and undertake actions [6].
At the Life Supporting Technologies group, we have applied the UCD methodology specifically in technological projects for patients with chronic diseases such as: cardiovascular diseases, diabetes and Parkinson. All these projects aimed to design and develop an ICT solution that, not only could help patients to manage their disease in the best possible way, allowing them to improve their quality of life, but also provide useful information to healthcare professionals to manage patients’ health conditions.
2.1.1 Experiences Applying UCD in ICT Solutions for Chronic Diseases Management
In this section, we present the experiences and lessons learned during the phases of technical requirements’ definitions, use cases, and validation, in chronic disease management projects for patients with diseases such as diabetes, cardiovascular, and Parkinson.
Technical requirements’ definitions:
The major goal of this phase is to identify the relevant set of medical and technical requirements that will be the starting point for developing the specifications of the overall architecture. Conducting research, indagating and agreeing on requirements during the design phase, can help during the development of the project facilitating the project planning.
To determine the technical requirements of an ICT solution, we first must consider that not only is it necessary to do a theoretical investigation of the specific kind of chronic disease and its treatment, but also to receive useful information from potential stakeholders (e.g., physicians, patients, caregivers, nurses, users, etc.). For example, in a study conducted for the HeartCycle project, in which we developed a personal health system for cardiovascular diseases management, a total of 26 patients were interviewed at the beginning of the design phase. The interviews followed a protocol that included a presentation of the project concept, a conversation on a storyboard that showed some of the potential functionalities, and a final questionnaire with a scoring sheet. The results were analyzed in order to identify patients’ major problems and needs in specific workshops that involve experts and health professionals [10].
Based on our experience, we have been able to detect that, although each chronic disease is different in symptoms, the evolution and treatment to follow, the needs and goals of patients, doctors and caregivers are similar. First, patients seek out to have a tool that helps them to manage their health and at the same time provide educational content, reminders, physical activity monitoring, feeding guide, emergency interventions and allow them to have greater independence and control on the disease leading to an improvement of their well-being. Second, doctors and caregivers seek for a tool in which they can evaluate the evolution of their patients, their treatment adherence and maintain contact with them remotely as well.
Furthermore, other aspects to be considered in the later development phase are: (1) any solution targeted to be used by patients should be easy to use; and (2) there was a clear need to add patient education and motivation strategies into the solutions [10].
Use cases:
The definition of use cases for the management of patients with chronic diseases does not have much difference from what the theory suggests, which consists of the description of the system focused on low-level user actions including system response [11]. However, we can point out that for developments that seek to provide a complete solution that gives the necessary tools to both the patient and the healthcare professionals, different cases such as: intervention in case of emergency, management and intervention for taking medication, exercise management, diet guide, medical patient communication, etc., must be included to ensure better health management of the chronic disease.
We also recommend not ruling out any use case, even if it is considered obvious since we are talking about scenarios in where the health of the patients could be affected or where useful interventions could help them. Based on this assumption, in an initial phase, everything must be considered. For example, in the METABO project, which consisted in the development of a system to assist diabetic patients in controlling their metabolic disorders, a total of 33 use cases were clearly defined to guarantee the complete functionality of the solution and meet the expectations of all the potential users. These definitions include, as an example, a simple task as user login, the possibility to have an error during the login process and how to solve the issue [12]. This sometimes is considered evident for when developing ICT solution, but not consider it from the beginning could produce design and definition problems during the development and validation phases in some cases and in particular with specific type of users (e.g., elderly people).
-
Validations:
The validation process is the key element in every ICT development process as the users are the ones that determine the usability and reliability of the solution and its quality and capacity to meet their needs. Throughout our experience, we have applied different validation methods that we describe below.
In the METABO project [13], we applied the accepted standards DIN EN ISO 9241 and ISO 3407 as the foundation of the validation process. According to these standards, usability can be measured as efficacy, efficiency, and satisfaction. A total of 36 Type 1 diabetes patients tested the solution. The usability problems were reported to the development teams and have been addressed by them following an iterative process of development. As result of this validation 43 usability issues were identified, managed, and solved.
Alternately, in the HeartCycle Project, we have applied questionnaires, combining semantic differentials and Likert scales to evaluate the usability and acceptability of the system. Each interview itself included three main parts: (1) a general introduction of the project and purpose of the test; (2) questions focused on general motivation factors; and (3) the interview with a short introduction and demonstration of the application. In the third part, the patients were asked to use the application performing specific tasks and fill in a questionnaire with their impressions. The outcomes of this validation led to a refinement of the global design and the implementation of an improved application. This upgrade took into consideration all the received suggestions and specifically addressed the aspects that obtained worse acceptance rates during the validations [14].
Finally, in the PD manager Project, which developed an m-health ecosystem for Parkinson’s disease management by using non-intrusive mobile and wearable devices, the acceptability and utility of the PD manager system were assessed by comparing it with traditional practices of using a patient/career diary for the management of the disease. The validation phase was performed following a non-blinded parallel two-group randomized controlled pilot study for a period of two weeks [15]. A total number of 200 patients and 200 caregivers were enrolled and tested the solution. After the test period, interviews were made to collect their opinions to assess the acceptance, ease of use, usefulness of information of the PD manager system and the specific section of the solution related to “Symptoms Diary”.
In the previous examples, several validation procedures were applied, all of them widely used by ICT researchers and development teams. However, it is important to point out that the key element of the validation phase in these kinds of solutions is to select the validation technique that best suits the needs of the different stakeholders involved and the goals of the specific study. Following this, we can objectively detect the weak points that will ultimately determine the success or failure of the solution.
2.2 Accessibility
Accessibility, in terms of human–computer interaction, refers to the computer accessibility and the capability of a computing system to be accessible to everyone, regardless the impairments, age, assistance needed, or disabilities people might have. In this domain, several use cases have been implemented through different projects and UCD has been used extensively. Thus, we present our findings and the insights we consider valuable when we applied UCD to projects dealing with accessibility issues.
2.2.1 Utilizing UCD with Virtual User Modeling to Create Accessible Application Interfaces, the Case Study of VERITAS
VERITAS presented and delivered an adaptation of UCD to serve a large portion of users with different needs such as hearing and/or visual disabilities, cognitive impairments, mobility issues, etc., or elderly people with problems related to their health conditions and the age. The motivation for this adaptation is that the application of UCD with the patient-centric approach [16] has not been explored thoroughly and the end products or services are not well adapted to the final users. The patient-centric approach refers to the way a healthcare system involves the experts together with patients and their families to adjust choices to patients’ needs and inclinations. Furthermore, it incorporates the conveyance of explicit education and bolster patients need to settle on these choices and take an interest in their very own health care.
This intersection between the patient-centric approach and the UCD leads to accessible products that finally could satisfy the end users by meeting their special needs. It is important to address the accessibility issues to bridge the gap between software development methodologies and UCD. While this task is very challenging, VERITAS addressed it with the help of interaction paths. We described the interaction path by defining all the possible states that a user can go through in the system and within its graphical user interface (GUI). The solution implemented by VERITAS is described below. The procedure is to associate the interaction paths and tasks models in order to bring off scenario files [17, 18].
During the modeling and design phase, the goal-oriented design (G-OD) [12] was chosen as an approach to focus mainly on the goals of the users and define detailed the use cases and scenarios. The methodology follows iteration circles within these states: research, modeling, requirements, framework, refinement, and support. At first, we defined the goals in the research phase, then we modeled the goals with the “personas” concept in order to represent them effectively, and later, in the requirements phase, we designed the scenarios able to describe the complete context and the conditions of use. The next phase is the framework phase in which we start to design the GUI. To do so, first, we chose the available interaction devices, designed all the possible screens, and created the key paths that describe the most frequent tasks the user can perform in the system. The key paths are important, and they represent the best-case scenarios that can describe all actions with minimal steps, by means while the system operates normally and with no human errors. In the next phase on refinement, we defined all the possible secondary tasks that can derive from the best-case scenarios.
In the field of medical applications, it is critical for the systems to be able to react in real time. Also, the users should be able to have the ability to choose their preferred way of presentation of the content according to their preferences and their specific technical knowledge. Although the interaction paths can describe effectively all the actions in one system, sometimes they disregard some important fundamentals: they remain static and they cannot react in real time to user inputs (e.g., answers to questionnaires). In order to bypass this, dynamic key paths enable the interaction workflows to meet the needs of the users in real time. Delivering a more personalized solution before the support phase while following the G-OD methodology is achieved by the following steps [17]:
-
Step 1: In the refinement phase, the GUI is initiated and designed to meet the specific needs. In this step, we record the interaction sessions for creating scenarios to be used in the next step.
-
Step 2: In this step, we connect the previous scenarios with the simulation models. These models are defined in the processing phase and they describe all the objects in the GUI. Then, the task models are generated, and they map and relate to the user events corresponding to the UI elements. Thus, for every task, different events are associated with the recorded images of the previous step 1. This process is very important as provides the users’ activity on every task and deliver for each event all the interactions involved.
-
Step 3: The task models created in the previous step 2 were exported in order to be reproduced in the GUI with different virtual user models. At this step and having created the virtual user models, we evaluated the GUI with specific groups of people each one represented from one or more virtual user models. In that manner, we evaluated the interactions and addressed all the accessibility issues. Finally, the development team applied the final changes after having implemented all the virtual models to represent all groups of users.
This approach found to be very informative as we discovered at early stages many accessibility problems of the GUI, before the development phase. Hence, the design of accessible and personal healthcare solutions can take advantage of all these insights, on an early phase, in order to deliver more adapted solutions to specific segment of users. The evaluation of all the tools and the processes followed by VERITAS demonstrated that there is a good correlation between the final outcomes of the virtual modeling with UCD approach and the real users. Finally, while tested with real users, more problems occurred but there was enough correspondence to the results of the virtual users so that this approach should be adopted by other developers or actors as well.
2.2.2 Applying Holistic UCD in ICT Health Desktop, Mobile and Web Applications, the Case Study of AEGIS
Aegis examined the third-generation access techniques and the possibility to exploit them in order to build mainstream and accessible applications including desktop and mobile applications and utilizing the rich Internet. Open accessibility framework (OAF) was developed and is open access to everyone in order to provide guidelines regarding the design and development of accessible ICT solutions. Through a holistic UCD adaptation, AEGIS explored user needs and interaction models for several user groups such as users with visual, hearing, and cognitive problems and provided insights for developers as well [19].
Because of the diversity of the applications developed, different use cases implemented on this project. All the use cases are designed to serve people with disabilities and the following groups of people are identified:
-
1.
Cognitive impairment users
-
2.
Hearing impairment users
-
3.
Speech impairment users
-
4.
Blind and low-vision users
-
5.
Motor impairment users.
In those target groups, various health ICT applications have been developed with the UCD applied, on the domain of accessibility and they consist of desktop applications, web applications, and mobile applications. Hence, the results and lessons learned from this project provide valuable contribution to the reader and the scientific community.
The first steps were to initiate the UCD process and involve all the main stakeholders such as experts in the field, developers and users with disabilities at this early stage to have plenty of time for future modifications and adaptations. A consensus was defined and agreed to the following elements: user involvement at very early stages as high priority due to the diversity of the user groups; everything users can see, hear, and touch to be designed together with a multidisciplinary team.
The UCD plan followed four phases: thoroughly analysis of all the users to collect the needs of the users and other relevant insights; definition of requirements and use cases by translating the previous needs to a more meaningful representation; initiation of the development through the conceptual designs utilizing a co-design approach; test and evaluate the prototype with end users.
After the application of this procedure, we present the main outcomes and lessons learned through this feedback gained through a participatory design method.
Summarizing the experiences and lessons learned through holistic UCD methodology in ICT applications for the specific target groups mentioned before [20, 21]:
-
Avoid all in one solution, as the requirements divert on the user groups. For example, blind users had the desire to avoid the screens and the hearing-impaired users could not adapt to this solution.
-
Developers should develop with the help of the users and never release a version without the approval of at least one expert user.
-
Each iteration cycle is done only after the previous iteration solved all the identified issues.
-
Specific features are implemented only if they are asked by the users; developers should avoid thinking possible features without being experts on the field.
-
Full hardware specifications must be given in the testers on each cycle to avoid causing problems with compatibilities.
-
Developers should use or integrate already existing elements and software to gain time while respecting the copyright policy.
-
People with disabilities and elderly usually lack the knowledge of assistive technologies and confuse the outcomes in the piloting phase. To avoid that, experts should be involved and provide their valuable feedback.
Evaluation performed through a framework implemented within the project in order to validate all three markets of the applications developed: rich Internet, mobile and desktop applications. Because of the UCD applicability in all stages as mentioned before, the validation techniques include all the related stakeholders and professionals while they take place in four different countries and six sites feeding with feedback the technical teams on each phase.
Because of the different applications developed in this project, different evaluation categories have identified: technical validation, human factor assessment, impact assessment, and socio-economic assessment of all the AEGIS applications. The testing sites performed the trials with the end users assessing the human factors while the more technical evaluations performed in the developers’ sites. However, the remaining impact and socio-economic assessment was conducted only with the feedback of the previous technical and human factors’ assessment.
For a better understanding the technical assessment examined the validity of the system, its performance, the quality offered and the accessibility issues including all the involved stakeholders. The human factors assessment considered to examine the acceptance of the system and how is it affecting the users and their lives. The impact assessment was conducted to examine if the users were satisfied and if they improved their quality of life. At the same time, it assessed the new possibilities to enter the market and deliver future business solutions in health care. Only experts were involved in this phase. Finally, the socio-economic assessment considered all the economical possibilities to pay the products performing and strengths and weaknesses analyses.
The pilots on each country performed the evaluation in three phases [22] in order to provide adequate feedback to the developers and deliver a satisfactory project. These three phases consist of: (a) test the initial conceptual design with simulations and mock-ups utilizing the Wizard of Oz technique; (b) creation of interfaces of early prototypes and for the initial testing with specific test cases; (c) perform full trials and tests with the application demonstrators with the final users and with experts involved.
2.3 Cognitive Rehabilitation and Training
People with cognitive impairments face various problems related to their cognition, memory, and learning capabilities. Cognitive rehabilitation refers to programs and applications tailored for individuals able to help them restore their normal cognitive functioning or to compensate deficits [23]. Computer-assisted types of rehabilitation and training have shown evidence that can be effective for individuals who suffered from a stroke, a brain trauma, or have a cognitive decline.
2.3.1 Providing Detailed Use Case Scenarios Based on UCD and Literature Review, the Case Study of InLife
The project focused on elderly with cognitive impairments. The solution adopted by InLife delivered ICT interoperable and personalized applications able to prolong the independent living, promote the socialization, and control the health of the people with cognitive impairments [24].
This project followed a slightly different approach to design the use cases using the UCD methodology [25]. Firstly, a detailed review was done in all previous funding calls and EU projects related to the same target user, seniors with cognitive impairments. Secondly, insights and the state of the art of several projects but for the same target groups were provided, in addition to a review of papers associated with relevant existing technologies. Furthermore, because of the division of the project in different pilots running in different regions, local workshops were held on each region in order to instantiate the findings of the user needs in terms of service functionality and variations in different locations. Finally, the outputs of the workshops combined with the previous literature analysis created a very detailed “personas” scenario that can describe the overall solution and service to potential users with great accuracy. Through this methodology, the main user requirements were exported and used to create the “personas” scenarios before the development.
To evaluate the results of the previous methodology, the project used mainly interviews and questionnaires because of the diversity of the stakeholders involved in the process. Also, to homogenize all the information from all the partners, an ad hoc template was developed and used to gather all the information in quantitative and qualitative categories and to perform various analyses on those data. After the data analysis, it was acknowledged that the extraction of user needs had been focusing on two kinds of primary users, people with cognitive impairments and healthy older people, while people living alone and wanting to maintain their independence was the majority.
Defining use cases found to be more time-consuming but effective and slightly different from the existing approaches due to its mixed elements. Using this ap-approach, we were able to identify specific groups of people at a higher degree of abstraction and classify them better according to their needs and their associated environments.
To conclude, this approach of defining use cases found to be more sluggish but effective and slightly different from the existing approaches due to its mixed elements. The outcome is that this approach can identify specific groups of people at a higher degree of abstract, classify them better according to their needs and associated environments and provide detailed use cases.
2.3.2 Co-creation of a Hybrid UCD with Stakeholders, Products and IoT, the Case Study of ACTIVAGE
It is worth mentioning the application of UCD and relevant insights in large-scale projects with pilots currently running simultaneously in different countries. For this reason, we present you in this section the project ACTIVAGE [26]. The main objective is the implementation of a reference framework for smart living for aging well solutions encompassing the use of Internet of Things.
In the context of UCD methodology, each deployment site (DS) adapted its own UCD method. Nonetheless, we can find common elements that can give insights for future integration of UCD in large pilots. All the pilots followed classical methods to gather the required information about the environment, stakeholders and the needs of users, professionals and caregivers and other involved stakeholders. These methods include documentary analysis, open questionnaires, structure and semi-structure interviews and focus groups.
The pilot of Madrid DS is focusing on the early detection and prevention of cognitive decline and the falling risk of elderly people in their living environment. The hybrid solution adopted by Madrid DS combines UCD with technological development approaches while exploiting the IoT and the Smart Cities paradigms. The initial results of this adaptation of the co-creation framework revealed us already on the first iterations’ detailed needs and scenarios of the users and guided us to design improved technologically interventions incorporating the IoT paradigm.
The co-creation framework [26, 27] is being used specifically in the Madrid DS. Figure 9.2 presents the framework which is a combined UCD and IoT paradigm in order to identify the user needs, contextualize them to requirements, and deliver them as a service solution (provided by the demand side) combined with technology (provided by the supplier side) to the stakeholders.

Co-creation framework [27]
For a comprehensive understanding in the framework (Fig. 9.2): The number of the iterations is dependent on the discovery of new services and implementation, thus the desirable satisfaction of the stakeholders. In the first iteration, the previous project inputs are used to extract the user needs and couple them with the existing literature in order to design proper use case scenarios. Then, these use case scenarios are contrasted with end users and different stakeholders (e.g., elderly, caregivers). Continuing, the solution is proposed by combining the service and technology and delivered to the appropriate stakeholder for the next phase. In the second iteration, we repass all the elements but viewing it from a different angle. At this phase, we examine the values that we can extract based on a technological perspective and on the IoT paradigm incorporated in our proposed solution. We define and construct all the services consolidating the results on each iteration, and we utilize a waterfall generic model to assist us on the technical development with these phases: analysis, adaptation, and assessment. Finally, after each iteration, the solution is tested with the users and given the feedback we iterate until we reach a satisfactory service for the users.
This method has been useful up now to define the services on our pilot. The defined solutions have been tested in our living laboratory technically. However, because this is an on-going task, the evaluation will occur at a later phase. One of the key requirements to achieve this satisfaction and keep improving our services is the interoperability. Exploiting and expanding interoperability on all levels offers flexibility, enhances the solution, and allows reusability and scalability of the solutions.
To conclude, this methodology has been used as our core framework to design interventions on large scale projects. This enabled us possibilities to adapt it to the new emerging paradigms such as IoT and smart cities. Deriving values from these paradigms within UCD pushes the technological boundaries, optimizes the solutions and their acceptability.
2.3.3 Utilizing UCD in All Phases to Implement a Satisfactory Product, the Case Study of Smart4MD
The SMART4MD project develops and tests a health application specifically tailored to people with mild dementia. The SMART4MD application that is currently being tested by users was developed for tablets. The trials will last two years [28]. In the Smart4MD project, the principles for Agile software development and inclusion of the user are influencing the whole design and adaptation process. A systematic review of earlier studies in the field has showed that user involvement in the design process has improved the usefulness and acceptability of the applications.
In this case, the UCD is applied before the development and the project initiation. The first step included semi-structured interviews and focus groups (first phase) with the end users, people with mild dementia, their careers and the associated professionals. The purpose of this was to get the most important insights at first, in order to understand in depth, the needs of these people and at a later stage to define properly the requirements for the solution. Based on this information, the first prototype was designed and exposed to the second stage of interviews. At that stage, the target was to explore extra undiscovered problems related to usability, user experience, and personalization to this group of people. The steps followed are typical and can be seen below:
-
1.
Preparation to identify and address important tasks and questions, ethical issues, information sheet, informed consent, guide for the moderator, etc.
-
2.
Focus groups/interviews/observations with patients and careers (inclusion, why, how, when, whom, how many, structure.)
-
3.
Interviews with healthcare professionals (why, how, when, whom, how many, structure.)
Finding of both phases showed important outcomes as they revealed information about the familiarity of technology with those people, past experiences with technology, content preferable for them, potential usage/agreement of the solution’s features, requirements and usage motivation and ethics related issues. UCD played an important role in revealing all this information and making the solution adapted and adopted by people with mild dementia.
More specifically, the processed followed can be summarized in the following Fig. 9.3. This UCD process can be used as a guide for future implementation when working with specific people such as people with mild cognitive impairments and mild dementia.

UCD method applied in Smart4MD
3 Highlights and Conclusion
Through this chapter, we have shown our experiences and lessons learned over the years dedicated to research and development of ICT solutions applied in multiple domains, using user-centered design methodology. This methodology puts the end user in the center of attention since the success of innovation depends on them. So, considering their experience, needs and expectations are fundamental during the whole process.
In the research stage, referring to the published literature is an excellent way to understand the context in which the development is focused. Scientific articles, patents, even commercial products, are basic sources to accomplish this stage. However, it is also worth-knowing first-hand, so doing interviews or consultations with potential users will help to have clearer the goals in terms of usability of the solution.
There are several methods of approaching users to know their needs and expectations, in terms of their health condition and the use of new technologies, which allow to establish the use cases. These methods can be, for example: focus groups, online or telephone surveys, individual interviews, etc. The selection of the method to use will depend on the type of users, considering age, characteristics of a disease, intellectual and physical capacity, and affinity with new technologies.
On the other hand, during the development phase of the solution, it is advisable to carry out validations with potential users, so that any problem that may affect the final solution can be detected on time. For this validation, there is no single rule. Standards such as DIN EN ISO 9241 and ISO 3407 can be applied as well as other usability tests applying Likert scales. The key is to select the best validation technique that really allows to detect both the strengths and weaknesses of the development and that contributes to improve the final solution.
Table 9.1, we provide a summary of all the recommendations for the different phases of the UCD based on the experiences and lessons learned.
References
Li Y, Oladimeji P, Monroy C, Cauchi A, Thimbleby H, Furniss D, Vincent C, Blandford A (2011, December) Design of interactive medical devices: feedback and its improvement. In: 2011 IEEE international symposium on IT in medicine and education, vol 2. IEEE, pp 204–208
Norman DA, Draper SW (1986) User centered system design: new perspectives on human-computer interaction. CRC Press, Boca Raton
Abras C, Maloney-Krichmar D, Preece J (2004) User-centered design. In: Bainbridge W (eds) Encyclopedia of human-computer interaction, vol 37(4). Sage Publications, Thousand Oaks, pp 445–456
Ritter FE, Baxter GD, Churchill EF (2014) Foundations for designing user-centered systems. Springer, London, pp 978–981
Ghazali M, Ariffin NAM, Omar R (2014, September) User centered design practices in healthcare: a systematic review. In: 2014 3rd international conference on user science and engineering (i-USEr). IEEE, pp 91–96
Teriús-Padrón JG, Kapidis G, Fallmann S, Merdivan E, Hanke S, García-Betances RI, Cabrera-Umpiérrez MF (2018, March) Towards self-management of chronic diseases in smart homes: physical exercise monitoring for chronic obstruction pulmonary disease patients. In: 2018 IEEE international conference on pervasive computing and communications workshops (PerCom workshops). IEEE, pp 776–781
Liappas N, Cabrera-Umpiérrez MF (2018, March) Enabling adaptive interactions to leverage interventions for people with mild cognitive impairments. In: 2018 IEEE international conference on pervasive computing and communications workshops (PerCom workshops). IEEE, pp 454–455
Liappas N, García-Betances RI, Teriús-Padrón JG, Cabrera-Umpiérrez MF (2018, March) Studying the technological barriers and needs of people with dementia: a quantitative study. In: 2018 IEEE international conference on pervasive computing and communications workshops (PerCom workshops). IEEE, pp 884–889
World Health Organization (2018) Noncommunicable diseases [Online]. Available https://www.who.int/en/news-room/fact-sheets/detail/noncommunicable-diseases. Accessed 05 Apr 2019
Vera-Muñoz C, Arredondo MT, Ottaviano M, Salvi D, Stut W (2013, July) HeartCycle: user interaction and patient education. In: 2013 35th annual international conference of the IEEE engineering in medicine and biology society (EMBC). IEEE, pp 6988–6991
Cooper A, Reimann R, Cronin D, Noessel C (2014) About face: the essentials of interaction design. Wiley, Hoboken
Fioravanti A (2016) A technological framework based on automatic messaging for improving adherence of diabetic patients. Doctoral dissertation, Telecomunicacion
Fico G, Fioravanti A, Arredondo MT, Leuteritz JP, Guillén A, Fernandez D (2011, August) A user centered design approach for patient interfaces to a diabetes IT platform. In: 2011 annual international conference of the IEEE engineering in medicine and biology society. IEEE, pp 1169–1172
Vera-Muñoz C, Arredondo MT, Peinado I, Ottaviano M, Páez JM, de Barrionuevo AD (2011, July) Results of the usability and acceptance evaluation of a cardiac rehabilitation system. In: International conference on human-computer interaction. Springer, Berlin, Heidelberg, pp 219–225
Antonini A, Gentile G, Giglio M, Marcante A, Gage H, Touray MM, Fotiadis DI, Gatsios D, Konitsiotis S, Timotijevic L, Egan B (2018) Acceptability to patients, carers and clinicians of an mHealth platform for the management of Parkinson’s disease (PD_Manager): study protocol for a pilot randomised controlled trial. Trials 19(1):492
Brand CS (2012) Management of retinal vascular diseases: a patient-centric approach. Eye 26(S2):S1
Scott MJ, Spyridonis F, Ghinea G (2015) Designing for designers: towards the development of accessible ICT products and services using the VERITAS framework. Comput Stand Interf 42:113–124
García-Betances R, Cabrera-Umpiérrez M, Ottaviano M, Pastorino M, Arredondo M (2016) Parametric cognitive modeling of information and computer technology usage by people with aging-and disability-derived functional impairments. Sensors 16(2):266
Korn P, Bekiaris E, Gemou M (2009, July) Towards open access accessibility everywhere: the ÆGIS concept. In: International conference on universal access in human-computer interaction. Springer, Berlin, Heidelberg, pp 535–543
Ignacio Madrid R, Carmona I, Montalvá Colomer JB (2015) Managing the participation of people with disabilities in large-scale R&D technology projects: best practices from AEGIS and CLOUD4ALL. J Accessib Des All 5(2):77–99
Van Isacker K, Slegers K, Gemou M, Bekiaris E, (2009, July) A UCD approach towards the design, development and assessment of accessible applications in a large scale European integrated project. In: International conference on universal access in human-computer interaction. Springer, Berlin, Heidelberg, pp 184–192
Gemou M, Bekiaris E (2009, July) Evaluation framework towards all inclusive mainstream ICT. In: International conference on universal access in human-computer interaction. Springer, Berlin, Heidelberg, pp 480–488
Koehler R, Wilhelm E, Shoulson I (eds) (2012) Cognitive rehabilitation therapy for traumatic brain injury: evaluating the evidence. National Academies Press, Washington DC
Panou M, Cabrera MF, Bekiaris E, Touliou K (2015) ICT services for prolonging independent living of the elderly with cognitive impairments-IN LIFE concept. Stud Health Technol Inform 217:659–663
Panou M, Garcia A, Bekiaris E, Touliou K (2016) From user needs and requirements to use cases for ICT services addressed to elderly with cognitive impairments. In: The international eHealth, Telemedicine and Health ICT Forum for Education, Networking and Business—MEDETEL, Luxembourg, 6–8 Apr 2016
Medrano-Gil AM, de los Ríos Pérez S, Fico G, Montalvá Colomer JB, Cea Sáncez G, Cabrera-Umpierrez MF, Arredondo Waldmeyer MT (2018) Definition of technological solutions based on the internet of things and smart cities paradigms for active and healthy ageing through Cocreation. Wireless Communications and Mobile Computing, 2018
Fico G, Montalva JB, Medrano A, Liappas N, Mata-Díaz A, Cea G, Arredondo MT (2017) Co-creating with consumers and stakeholders to understand the benefit of internet of things in smart living environments for ageing well: the approach adopted in the Madrid Deployment Site of the ACTIVAGE Large Scale Pilot. In: EMBEC & NBC 2017. Springer, Singapore, pp 1089–1092
Frögren J, Quitana M, Anderberg P, Sanmartin Berglund J (2018) Designing a model app for older persons with cognitive impairment: insights from a usability perspective. Gerontechnology 17:80
Acknowledgements
This work has received funding from the European Union’s Horizon 2020 research and innovation program under the Marie Skłodowska-Curie grant agreement ACROSSING No676157.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2020 Springer Nature Switzerland AG
About this chapter

Cite this chapter
Liappas, N., Teriús-Padrón, J.G., García-Betances, R.I., Cabrera-Umpiérrez, M.F., Arredondo, M.T. (2020). User-Centered Design in Defining and Developing Health and Well-Being ICT Solutions. In: Chen, F., García-Betances, R., Chen, L., Cabrera-Umpiérrez, M., Nugent, C. (eds) Smart Assisted Living. Computer Communications and Networks. Springer, Cham. https://doi.org/10.1007/978-3-030-25590-9_9
Download citation
DOI: https://doi.org/10.1007/978-3-030-25590-9_9
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-25589-3
Online ISBN: 978-3-030-25590-9
eBook Packages: Computer ScienceComputer Science (R0)