
Abstract
MRI is the primary means of diagnosis of brain tumors. It is also used to decide on best treatment options based on possible tumor grade, plan biopsy and surgery, evaluate extent of tumor resection, assess response to treatment, and detect recurrence.
This chapter will provide an overview of when to use imaging for brain tumors, a general overview of follow-up imaging, criteria used to assess treatment response, and recommended protocols. While the use of advanced imaging methods will be mentioned and some aspects of conventional MRI sequences will be discussed, these will be in the context of their utility in general terms. Details regarding specific uses, pearls and pitfalls of conventional sequences, and advanced imaging techniques will be discussed in other chapters of the book.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others

Keywords
1 Introduction
Modern imaging techniques are the primary means of diagnosis of brain tumors [1]. They are also used to decide on best treatment options based on possible tumor grade, plan biopsy and surgery, evaluate extent of tumor resection, assess response to treatment, and detect recurrence.
This chapter will provide an overview of when to use imaging for brain tumors, a general overview of follow-up imaging, criteria used to assess treatment response, and recommended protocols. While the use of advanced imaging methods will be mentioned and some aspects of conventional MRI sequences will be discussed, these will be in the context of their utility in general terms. Details regarding specific uses, pearls and pitfalls of conventional sequences, and advanced imaging techniques will be discussed in other chapters of the book.
2 When to Use Imaging
2.1 Diagnosis
MRI remains the cornerstone of brain tumor imaging, and is considered the standard imaging method for diagnosis [2]. In cases where a brain tumor might be suspected, such as those with chronic headache with new features or increasing frequency, new onset headache with optic disc edema, nontraumatic seizure in patients older than 40 or with focal neurologic deficit, the most appropriate imaging is MRI with and without contrast [3, 4]. CT can be used in the emergency setting, or to look for calcification in selected patients.
While a specific histopathological diagnosis may not be possible based on the images, it is usually not needed. In many cases the distinction of low- and high-grade lesions is more important, and many patients will have biopsies or surgery for histopathologic diagnosis and molecular studies (and in case of surgery, for treatment) in any case.
2.2 Preoperative Planning
Surgery remains the cornerstone of treatment of brain tumors and maximum safe resection is recommended in all patients with newly diagnosed gliomas whenever feasible [2]. While some tumors in eloquent cortex or brainstem have been traditionally considered inoperable, recent advances in neurosurgery and mapping techniques make it possible to operate on at least some of those lesions [5].
In certain cases, biopsy may be preferred before (or instead of) surgery. It is well known that the heterogeneity of gliomas can cause undergrading and misdiagnosis due to sampling errors in biopsy [6]. In such patients, advanced imaging techniques can be used to target specific regions of interest to potentially improve diagnostic accuracy [6, 7].
MRI is also used in preoperative planning for navigational purposes. This is usually done with contrast-enhanced 3D-SPGR sequences that allow for high resolution and easy distinction of the tumor due to contrast enhancement. Coupled with some fiducials placed on the patient’s head before the imaging study, these images can be used for intraoperative navigation. Imaging with head frames can also be performed for the same purpose in stereotactic radiosurgery or frame-based stereotactic biopsy.
Another factor with potential impact on surgery is the relation of the lesion to eloquent brain and critical white matter tracts [8]. Conventional anatomic MR imaging is insufficient to provide this information; for instance, while one can easily tell if a lesion is in the motor cortex provided one knows where the motor cortex is in that patient; brain mapping is not generalizable and must be done in a patient specific manner [9]. Functional MRI can be used to evaluate the location of the lesion with respect to eloquent brain (Fig. 2.1). The relationship of white matter tracts with the tumor can be delineated using diffusion tensor imaging (DTI) [8, 10]; thus DTI can also help improve tumor resection [11] and reduce the risk of new postoperative neurological deficits [12].

fMRI study (a) to determine the location of the Broca area and plan surgery accordingly in a patient with a right temporal mass (b). The Broca region is demonstrated to be on the left side, which would have been impossible to determine with conventional MRI
2.3 Intraoperative Imaging
Intraoperative MRI (iMRI) scans are beginning to get more widespread. The extent of resection is one of the factors improving overall survival in patients with gliomas [13] and use of intraoperative imaging makes it easier to ensure that as much of the lesion as is surgically feasible has been taken out [2]. This allows immediate further resection in the same session [14] and improved overall survival and progression-free survival have been reported by some groups [15, 16]. Despite these apparent benefits, there is a high cost of installation and an increase in the healthcare cost and length of surgery [13]. There are also few studies providing high-quality evidence and evaluating whether the use of iMRI translates to improved progression-free survival or overall survival [14].
2.4 Postoperative Imaging
In the immediate postoperative period, unless there are operative complications or clinical concern, imaging is usually performed to determine the extent of tumor resection. In this situation, MRI is the modality of choice, provided the patient is clinically stable and there are no contraindications to an MRI scan.
Post-op imaging is also required to act as a baseline for further follow-up. The most appropriate time for baseline imaging to evaluate residual tumor is considered to be within 24–48 h of surgery and no later than 72 h [2, 17, 18]. Diffusion-weighted imaging (DWI) can also be included in the baseline imaging to determine if any future enhancement would be due to recurrence or ischemia related to surgery [18]. However, it should be noted that RANO criteria for diffuse low-grade gliomas recommend the baseline postoperative images to be preferably acquired 2–3 months after the surgery to minimize the effects of postsurgical changes such as edema, ischemia and enhancement and to better evaluate the extent of resection of non-enhancing tumors [19].
2.5 Follow-Up Imaging
There are two different scenarios where follow-up imaging is performed: To follow up the lesion after treatment for recurrence or progression of any non-resected parts of the mass; and to follow up lesions that did not receive any treatment. While the imaging protocol is similar in both cases, the distinction is important since it changes the differential diagnosis: new enhancement in a lesion that has been treated with chemoradiotherapy might be due to tumor progression as well as pseudoprogression or radiation necrosis in the appropriate timeframe, whereas the same change in a tumor that has not been treated would be very alarming for tumor progression.
Follow-up imaging should be performed using the same imaging modality as the baseline, which would be MRI in almost all cases [20]. Ideally, the same MRI scanner should be used, but if that is not possible or feasible, at least scanners with same magnet strength should be used (Fig. 2.2) [20].

Preoperative and follow-up FLAIR images of a 21-year-old (at time of four year follow-up) male patient with grade II glioma. (a) Preoperative, (b) 3 months post-op, (c) one year post-op, (d) four years post-op. Note the changes in FLAIR intensities surrounding the operation cavity, corresponding to gliosis
Some clinical data can help with the interpretation of follow-up images: Type of treatment the patient received and when the treatment was completed would help determine if increasing or new enhancement could be due to pseudoprogression, radiation necrosis, or tumor progression; antiangiogenic therapy might cause decreased enhancement without true regression; changes in steroid dose can affect the size of T2/FLAIR hyperintense component and enhancement; knowledge of the radiation field could help differentiate progression or new disease outside the field from radiation-induced changes [17].
Edema, treatment-related changes, and postoperative gliosis surrounding the surgical cavity might make it difficult to determine the recurrence of the lesion using T2W or FLAIR images. Outside of the timeframe for treatment-related changes, increases in T2/FLAIR hyperintensity should be suspicious for progression of non-enhancing tumor or increasing edema. Similarly new or increasing contrast enhancement, especially outside the high-dose radiation zone, is also a red flag [17].
2.5.1 Pseudoprogression
Pseudoprogression is a temporary, new, or increased area of contrast enhancement without true tumor progression, caused by treatment-induced changes [21,22,23]. It has been described in 10–30% of GBM patients who receive radiotherapy and temozolomide, in GBM patients receiving immunotherapy, and in LGG patients receiving radiotherapy [21, 22, 24]. It occurs most commonly within 3–6 months following therapy [17, 25]. Pseudoprogression may be more frequent in patients with MGMT promoter hypermethylation [17, 22]. Although most patients are asymptomatic, there may be deterioration in neurologic status or an increased need for steroids [22]. It typically resolves spontaneously [21].
Differentiating pseudoprogression from true tumor progression is challenging [24, 26]. Multifocality, the signal abnormality extending across the corpus callosum and subependymal involvement are suggestive of true progression, but there are no definitive conventional MRI findings to rule out true progression reliably [24]. Higher ADC values and lower perfusion parameters have been observed in pseudoprogression compared to true tumor progression [23, 24]; however, the thresholds reported in the literature should be applied with care [23]. Clinical data can also help with the differential diagnosis: pseudoprogression occurs up to 6 months after treatment, and changes are expected to stabilize or improve in follow-up without any treatment [17, 24].
2.5.2 Radiation Necrosis
Another difficulty is radiation necrosis in patients who underwent radiotherapy. Radiation necrosis most commonly occurs 9–12 months after treatment but can be seen years after radiotherapy [17, 22]. Differentiating radiation necrosis from tumor progression is difficult using conventional MRI [17, 27]. Perfusion MRI might be helpful, but there is significant disparity in published results [17].
2.5.3 Pseudoresponse
Pseudoresponse or pseudoregression is a decrease in enhancement without a true antitumor effect [17, 22]. It is seen in 20–60% of patients receiving antiangiogenic therapy such as bevacizumab or cediranib and thought to be due to a normalization of abnormally permeable blood vessels which can cause marked decrease in contrast enhancement and peritumoral edema as early as day 1 after treatment [21, 24]. To distinguish this from true antitumor effect, patients under antiangiogenic therapy who demonstrate marked reduction in enhancement need to have another scan at least 4 weeks later to confirm the persistence of changes [18, 28]. Antiangiogenic therapies may select for hypoxic and invasive tumor that first grows as a non-enhancing mass before progressing to enhancing disease [24]. Therefore, careful consideration of T2/FLAIR intense non-enhancing parts of the mass is essential in this subset of patients.
3 Evaluating Treatment Response
In patients who underwent treatment, there is an obvious need to report whether the disease is stable, progressing, or regressing in follow-up studies. One way of doing this is simply reporting measurements and/or a subjective assessment by the radiologist. An alternative is creating an objective set of criteria to determine the response to treatment as well as provide a common terminology to be used in radiology reports. This would be beneficial especially for research purposes; however, easy-to-use, consistent, and objective terminology would certainly be useful in daily clinical practice as well. While RECIST criteria are widely used to this end for solid tumors in the body, different sets of rules are used for brain tumors [29].
The first set of such criteria was published by Levin et al. in 1977, followed by WHO oncology response criteria published in 1981 [30, 31]. The more widely used and well-known criteria (commonly referred to as Macdonald criteria) based on CT images, but later extrapolated to MRI, was proposed by Macdonald et al. in 1990. In the paper, the state of the tumor was described as complete response (CR), partial response (PR), stable disease (SD), or progression (progressive disease, PD) (Table 2.1) [32].
However, some limitations of the Macdonald criteria became apparent over time, such as not accounting for pseudoprogression, not evaluating non-enhancing component of the tumor, failing to address pseudoresponse in patients using antiangiogenic treatment, difficulty of measuring irregularly shaped tumors as well as in measuring enhancing lesions located on the walls of cysts or surgical cavities [18, 33]. To address these issues, Response Assessment in Neuro-Oncology (RANO) criteria for high-grade gliomas (RANO-HGG) was proposed in 2010 [18]. These criteria, commonly referred to as the RANO criteria, consider radiologic appearance, corticosteroid use and dose, and clinical status to define CR, PR, SD, or PD (Table 2.1). However, in the following section, only the radiographic criteria will be discussed. Interested readers are referred to the original paper for more information regarding clinical details [18].
3.1 Response Assessment in Neuro-Oncology: High-Grade Glioma (RANO-HGG)
RANO-HGG criteria (commonly referred to as only the “RANO criteria”) define measurable disease as bidimensionally contrast-enhancing lesion(s) with clearly defined margins on CT or MRI, with two largest perpendicular diameters on an axial slice being at least 10 mm (Fig. 2.3). The lesion should be visible on at least two consecutive axial slices, and the slice thickness must preferably be at most 5 mm with 0 mm gap. If the slice thickness is greater than 5 mm, the size of the lesion should be at least two times the slice thickness to be considered measurable. If the lesion is unidimensionally measurable, lacks clearly defined margins, or smaller than 10 mm (or twice the slice thickness) in at least one dimension, it should be considered nonmeasurable. Special note is made of tumors around a cyst or surgical cavity: such lesions are to be considered nonmeasurable unless they have a clear nodular component that satisfies criteria for being measurable (i.e., at least 10 mm in two perpendicular dimensions).

Sample measurement of a high-grade glioma according to RANO criteria. With both dimensions of the enhancing part greater than 10 mm, this constitutes measureable disease
If there is more than one lesion, two to five of the largest lesions should be measured in two dimensions, the area should be calculated as the product of the two diameters and then the areas of the measured lesions should be added to get a single final value. Comparisons in follow-up should be made using this single value. While typically the largest lesions are selected for measurement, care should be taken to ensure that these lesions allow reproducible measurements. In cases where the largest lesions do not lend themselves to reproducible measurements, the next largest lesion that can be measured reproducibly can be selected instead. The lesions picked for measurement and calculation of the final value for comparison are defined to be the “target lesions.”
Non-enhancing components of the tumor are evaluated using T2W or FLAIR images, where they have similar appearance to peritumoral edema and radiation-related changes, making exact delineation of its margins quite difficult. Signs of mass effect such as sulcal effacement or compression of the ventricles; infiltration of the cortical ribbon or simply the location being outside of the radiation field suggest infiltrating tumor. Sometimes, there might still be doubt as to whether the changes represent an increase in non-enhancing tumor. In such cases further follow-up usually confirms or refutes the idea. While objective measures of non-enhancing tumor would obviously be helpful, there are no widely accepted methods for this purpose and RANO criteria do not incorporate any such methods yet.
Response is determined in comparison to the baseline imaging to determine CR or PR, and the smallest tumor measurement (in pre-treatment baseline images or in follow-up images after the initiation of treatment) to determine PD. In cases where the changes are equivocal, close follow-up is indicated. Rules to classify response are provided in Table 2.1.
3.2 Other RANO Criteria
Patients receiving immunotherapy and patients with other types of brain tumors should not be evaluated using RANO-HGG criteria. There are different criteria described for brain metastases (RANO-BM), low-grade gliomas (RANO-LGG), and patients undergoing immunotherapy (iRANO) [19, 34, 35]. Major differences of these criteria and how they compare to RANO-HGG are provided in Table 2.1. Response assessment for leptomeningeal metastases (RANO-LM) is handled in a totally different manner and interested readers are referred to the original paper for details on how to score imaging data [36]. Criteria for spine tumors (SPINO), pediatric brain tumors (RAPNO), and meningiomas (RANO-meningioma) are also under development [37,38,39].
4 Imaging Protocol
To standardize neuro-oncologic imaging in clinical trials, Consensus Recommendations for a Standardized Brain Tumor Imaging Protocol (BTIP) have been reported [20]. While this protocol is concerned mostly with standardizing MRI acquisition to facilitate multicenter studies and comparison of different studies, it is also recommended to be used for routine, clinical brain tumor imaging [33]. According to BTIP, MRI imaging of brain tumors should include at least the following sequences (Fig. 2.4) [20]:
-
Pre-contrast and post-contrast isotropic 3D inversion recovery-prepared T1W gradient-recalled echo (IR-GRE) images with matching parameters
-
Axial 2D T2W TSE (dual echo preferred but not required) acquired after contrast injection but before post-contrast T1W images
-
Pre-contrast axial 2D TSE T2W FLAIR
-
Pre-contrast axial 2D three-directional DWI using echoplanar (EPI) or radial acquisition

Sample images for brain tumor imaging according to the recommended protocol: (a) 2D FLAIR, (b) ADC map acquired from DWI using 3 directions and b values 0, 500 and 1000 s/mm2, (c) 2D T2W, (d) post-contrast 3D T1W. It should be noted that T1W images were acquired in the sagittal plane but are here demonstrated in the axial plane (using MPR) to be consistent with other images
The scanner used may be 1.5 T or 3 T [20]. There have been studies reported on 7 T scanners, but whether the use of 7 T scanners would translate into clinical benefit within the context of brain tumors is not clear [40]
Specific acquisition parameters as described by the consensus statements are provided in Table 2.2 [20]
Other sequences such as high-resolution isovolumetric 3D T2W images and advanced imaging techniques can be included in the study based on clinical indications and whether they are needed for differential diagnosis or surgical planning, but are not included in the minimum required study. The protocol also allows for other additional post-contrast T1W imaging, such as 2D fat-saturated T1W TSE images. However, such images should be acquired after the recommended 3D T1W images to ensure consistency of the timing of the contrast injection and 3D T1W image acquisition.
Perfusion-weighted imaging has not yet made its way into standardized imaging protocols or treatment response criteria. Nonetheless, perfusion studies are very helpful during follow-up, to differentiate recurrence from treatment-related changes such as radiation necrosis or pseudo-progression. In the proper clinical setting, these images are invaluable as problem solvers and in our opinion should be included in every follow-up study where it is technically possible to do so. With dynamic susceptibility contrast (DSC) studies, tumor recurrence is expected to have a higher relative cerebral blood volume (rCBV) than radiation necrosis or pseudoprogression; however, there is considerable overlap and the findings can be dependent on the technique used [17]. Therefore, clinical findings and, more importantly, correlation with conventional MRI images are essential for an accurate diagnosis. A more detailed explanation of perfusion imaging is provided in another chapter of this book.
4.1 Contrast Use
0.1 mmol/kg gadolinium-chelated contrast agent should be injected at an injection rate of 3–5 cc/s with a power injector if possible [20]. The same contrast agent must be used for follow-up; in cases where this is not possible, at least contrast agents with the same chemical composition should be used [20]. Images should be acquired 4–8 min after contrast injection [20].
Regarding adverse reactions, complications and contraindications of gadolinium-based contrast agents, and their use in special patient groups such as children, those with renal failure, or pregnant women, relevant national or international guidelines such as ACR Manual on Contrast Media (https://www.acr.org/Clinical-Resources/Contrast-Manual) [41] or ESUR Guidelines on Contrast Agents (http://www.esur-cm.org/index.php/en/) [42] should be followed.
5 Conclusion
MRI is the preferred imaging method to diagnose and follow-up brain tumors. Consensus statements regarding imaging protocols recommend, at a minimum, 3D isotropic T1W parameter matched pre- and post-contrast images, 2D T2W and 2D FLAIR images, DWI using 3 b values (b = 0, 500, and 1000 s/mm2) in at least three directions. Other advanced imaging methods are also useful and may be included in the routine protocol or on a case-by-case basis as needed.
MRI is essential for surgical planning, where advanced imaging modalities such as DTI and fMRI can be very useful. Intraoperative MRI can improve tumor resection, and thus prognosis. Postoperative imaging is necessary to ensure tumor resection and to provide baseline images for follow-up.
Follow-up is mainly concerned with the size of enhancing lesion as well as non-enhancing mass as demonstrated by T2W/FLAIR images. Based on the treatments used and the timeframe, pseudoresponse, pseudoprogression, and radiation necrosis should be taken into consideration where appropriate. DWI and perfusion images are very useful as problem solvers and to increase confidence in diagnosis of recurrence or treatment-related changes. Depending on whether the tumor is primary or metastatic, its histopathological type and grade, and the use of immunotherapy, different criteria to evaluate treatment response have been proposed and their use provide objective methods to assess response as well as a common terminology to use in reporting.
Notes
- 1.
Adapted from [18].
References
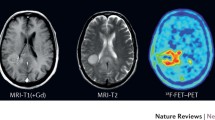
Langen KJ, Galldiks N, Hattingen E, Shah NJ. Advances in neuro-oncology imaging. Nat Rev Neurol. 2017;13(5):279–89. https://doi.org/10.1038/nrneurol.2017.44.
Weller M, van den Bent M, Tonn JC, Stupp R, Preusser M, Cohen-Jonathan-Moyal E, Henriksson R, Le Rhun E, Balana C, Chinot O, Bendszus M, Reijneveld JC, Dhermain F, French P, Marosi C, Watts C, Oberg I, Pilkington G, Baumert BG, Taphoorn MJB, Hegi M, Westphal M, Reifenberger G, Soffietti R, Wick W, European Association for Neuro-Oncology (EANO) Task Force on Gliomas. European Association for Neuro-Oncology (EANO) guideline on the diagnosis and treatment of adult astrocytic and oligodendroglial gliomas. Lancet Oncol. 2017;18(6):e315–29. https://doi.org/10.1016/S1470-2045(17)30194-8.
American College of Radiology. ACR appropriateness criteria: headache. 2019. Available at: https://acsearch.acr.org/docs/69482/Narrative/. Accessed 23 Apr 2019.
American College of Radiology. ACR appropriateness criteria: seizures and epilepsy. 2019. Available at: https://acsearch.acr.org/docs/69479/Narrative/. Accessed 23 Apr 2019.
Southwell DG, Birk HS, Han SJ, Li J, Sall JW, Berger MS. Resection of gliomas deemed inoperable by neurosurgeons based on preoperative imaging studies. J Neurosurg. 2018;129:567–75. https://doi.org/10.3171/2017.5.JNS17166.
McCullough BJ, Ader V, Aguedan B, Feng X, Susanto D, Benkers TL, Henson JW, Mayberg M, Cobbs CS, Gwinn RP, Monteith SJ, Newell DW, Delashaw J Jr, Fouke SJ, Rostad S, Keogh BP. Preoperative relative cerebral blood volume analysis in gliomas predicts survival and mitigates risk of biopsy sampling error. J Neurooncol. 2018;136(1):181–8. https://doi.org/10.1007/s11060-017-2642-2.
Ragel BT, Ryken TC, Kalkanis SN, Ziu M, Cahill D, Olson JJ. The role of biopsy in the management of patients with presumed diffuse low grade glioma: a systematic review and evidence-based clinical practice guideline. J Neurooncol. 2015;125(3):481–501. https://doi.org/10.1007/s11060-015-1866-2.
Mohammadzadeh A, Mohammadzadeh V, Kooraki S, Sotoudeh H, Kadivar S, Shakiba M, Rasuli B, Borhani A, Mohammadzadeh M. Pretreatment evaluation of glioma. Neuroimaging Clin N Am. 2016;26(4):567–80. https://doi.org/10.1016/j.nic.2016.06.006.
Silva MA, See AP, Essayed WI, Golby AJ, Tie Y. Challenges and techniques for presurgical brain mapping with functional MRI. Neuroimage Clin. 2017;17:794–803. https://doi.org/10.1016/j.nicl.2017.12.008.
Pope WB, Brandal G. Conventional and advanced magnetic resonance imaging in patients with high grade glioma. Q J Nucl Med Mol Imaging. 2018;62:239–53. https://doi.org/10.23736/S1824-4785.18.03086-8.
Yan JL, van der Hoorn A, Larkin TJ, Boonzaier NR, Matys T, Price SJ. Extent of resection of peritumoral diffusion tensor imaging-detected abnormality as a predictor of survival in adult glioblastoma patients. J Neurosurg. 2017;126(1):234–41. https://doi.org/10.3171/2016.1.JNS152153.
Mert A, Kiesel B, Wöhrer A, Martínez-Moreno M, Minchev G, Furtner J, Knosp E, Wolfsberger S, Widhalm G. Introduction of a standardized multimodality image protocol for navigation-guided surgery of suspected low-grade gliomas. Neurosurg Focus. 2015;38(1):E4. https://doi.org/10.3171/2014.10.FOCUS14597.
Rao G. Intraoperative MRI and maximizing extent of resection. Neurosurg Clin N Am. 2017;28(4):477–85. https://doi.org/10.1016/j.nec.2017.05.003.
Jenkinson MD, Barone DG, Bryant A, Vale L, Bulbeck H, Lawri TA, Hart MG, Watts C. Intraoperative imaging technology to maximise extent of resection for glioma. Cochrane Database Syst Rev. 2018;1:CD012788. https://doi.org/10.1002/14651858.CD012788.pub2.
Senft C, Bink A, Franz K, Vatter H, Gasser T, Seifert V. Intraoperative MRI guidance and extent of resection in glioma surgery: a randomised, controlled trial. Lancet Oncol. 2011;12(11):997–1003. https://doi.org/10.1016/S1470-2045(11)70196-6.
Wu JS, Gong X, Song YY, Zhuang DX, Yao CJ, Qiu TM, Lu JF, Zhang J, Zhu W, Mao Y, Zhou LF. 3.0-T intraoperative magnetic resonance imaging-guided resection in cerebral glioma surgery: interim analysis of a prospective, randomized, triple-blind, parallel-controlled trial. Neurosurgery. 2014;61(Suppl 1):145–54. https://doi.org/10.1227/NEU.0000000000000372.
Dalesandro MF, Andre JB. Posttreatment evaluation of brain gliomas. Neuroimaging Clin N Am. 2016;26(4):581–99. https://doi.org/10.1016/j.nic.2016.06.007.
Wen PY, Macdonald DR, Reardon DA, Cloughesy TF, Sorensen AG, Galanis E, Degroot J, Wick W, Gilbert MR, Lassman AB, Tsien C, Mikkelsen T, Wong ET, Chamberlain MC, Stupp R, Lamborn KR, Vogelbaum MA, van den Bent MJ, Chang SM. Updated response assessment criteria for high-grade gliomas: response assessment in neuro-oncology working group. J Clin Oncol. 2010;28(11):1963–72. https://doi.org/10.1200/JCO.2009.26.3541.
van den Bent MJ, Wefel JS, Schiff D, Taphoorn MJ, Jaeckle K, Junck L, Armstrong T, Choucair A, Waldman AD, Gorlia T, Chamberlain M, Baumert BG, Vogelbaum MA, Macdonald DR, Reardon DA, Wen PY, Chang SM, Jacobs AH. Response assessment in neuro-oncology (a report of the RANO group): assessment of outcome in trials of diffuse low-grade gliomas. Lancet Oncol. 2011;12(6):583–93. https://doi.org/10.1016/S1470-2045(11)70057-2.
Ellingson BM, Bendszus M, Boxerman J, Barboriak D, Erickson BJ, Smits M, Nelson SJ, Gerstner E, Alexander B, Goldmacher G, Wick W, Vogelbaum M, Weller M, Galanis E, Kalpathy-Cramer J, Shankar L, Jacobs P, Pope WB, Yang D, Chung C, Knopp MV, Cha S, van den Bent MJ, Chang S, Yung WK, Cloughesy TF, Wen PY, Gilbert MR, Jumpstarting Brain Tumor Drug Development Coalition Imaging Standardization Steering Committee. Consensus recommendations for a standardized brain tumor imaging protocol in clinical trials. Neuro-Oncology. 2015;17(9):1188–98. https://doi.org/10.1093/neuonc/nov095.
Nowosielski M, Wen PY. Imaging criteria in neuro-oncology. Semin Neurol. 2018;38(1):24–31. https://doi.org/10.1055/s-0038-1627468.
Shiroishi MS, Booker MT, Agarwal M, Jain N, Naghi I, Lerner A, Law M. Posttreatment evaluation of central nervous system gliomas. Magn Reson Imaging Clin N Am. 2013;21(2):241–68. https://doi.org/10.1016/j.mric.2013.02.004.
Thust SC, van den Bent MJ, Smits M. Pseudoprogression of brain tumors. J Magn Reson Imaging. 2018;48:571–89. https://doi.org/10.1002/jmri.26171.
Villanueva-Meyer JE, Mabray MC, Cha S. Current clinical brain tumor imaging. Neurosurgery. 2017;81(3):397–415. https://doi.org/10.1093/neuros/nyx103.
Ellingson BM, Chung C, Pope WB, Boxerman JL, Kaufmann TJ. Pseudoprogression, radionecrosis, inflammation or true tumor progression? Challenges associated with glioblastoma response assessment in an evolving therapeutic landscape. J Neurooncol. 2017;134(3):495–504. https://doi.org/10.1007/s11060-017-2375-2.
Yun TJ, Park CK, Kim TM, Lee SH, Kim JH, Sohn CH, Park SH, Kim IH, Choi SH. Glioblastoma treated with concurrent radiation therapy and temozolomide chemotherapy: differentiation of true progression from pseudoprogression with quantitative dynamic contrast-enhanced MR imaging. Radiology. 2015;274(3):830–40. https://doi.org/10.1148/radiol.14132632.
Delgado-López PD, Riñones-Mena E, Corrales-García EM. Treatment-related changes in glioblastoma: a review on the controversies in response assessment criteria and the concepts of true progression, pseudoprogression, pseudoresponse and radionecrosis. Clin Transl Oncol. 2018;20:939–53. https://doi.org/10.1007/s12094-017-1816-x.
Wen PY, Chang SM, Van den Bent MJ, Vogelbaum MA, Macdonald DR, Lee EQ. Response assessment in neuro-oncology clinical trials. J Clin Oncol. 2017;35(21):2439–49. https://doi.org/10.1200/JCO.2017.72.7511.
Eisenhauer EA, Therasse P, Bogaerts J, Schwartz LH, Sargent D, Ford R, Dancey J, Arbuck S, Gwyther S, Mooney M, Rubinstein L, Shankar L, Dodd L, Kaplan R, Lacombe D, Verweij J. New response evaluation criteria in solid tumours: revised RECIST guideline (version 1.1). Eur J Cancer. 2009;45(2):228–47. https://doi.org/10.1016/j.ejca.2008.10.026.
Levin VA, Crafts DC, Norman DM, Hoffer PB, Spire JP, Wilson CB. Criteria for evaluating patients undergoing chemotherapy for malignant brain tumors. J Neurosurg. 1977;47(3):329–35.
Miller AB, Hoogstraten B, Staquet M, Winkler A. Reporting results of cancer treatment. Cancer. 1981;47(1):207–14.
Macdonald DR, Cascino TL, Schold SC Jr, Cairncross JG. Response criteria for phase II studies of supratentorial malignant glioma. J Clin Oncol. 1990;8(7):1277–80.
Huang RY, Wen PY. Response assessment in neuro-oncology criteria and clinical endpoints. Magn Reson Imaging Clin N Am. 2016;24(4):705–18. https://doi.org/10.1016/j.mric.2016.06.003.
Lin NU, Lee EQ, Aoyama H, Barani IJ, Barboriak DP, Baumert BG, Bendszus M, Brown PD, Camidge DR, Chang SM, Dancey J, de Vries EG, Gaspar LE, Harris GJ, Hodi FS, Kalkanis SN, Linskey ME, Macdonald DR, Margolin K, Mehta MP, Schiff D, Soffietti R, Suh JH, van den Bent MJ, Vogelbaum MA, Wen PY, Response Assessment in Neuro-Oncology (RANO) Group. Response assessment criteria for brain metastases: proposal from the RANO group. Lancet Oncol. 2015;16(6):e270–8. https://doi.org/10.1016/S1470-2045(15)70057-4.
Okada H, Weller M, Huang R, Finocchiaro G, Gilbert MR, Wick W, Ellingson BM, Hashimoto N, Pollack IF, Brandes AA, Franceschi E, Herold-Mende C, Nayak L, Panigrahy A, Pope WB, Prins R, Sampson JH, Wen PY, Reardon DA. Immunotherapy response assessment in neuro-oncology: a report of the RANO working group. Lancet Oncol. 2015;16(15):e534–42. https://doi.org/10.1016/S1470-2045(15)00088-1.
Chamberlain M, Junck L, Brandsma D, Soffietti R, Rudà R, Raizer J, Boogerd W, Taillibert S, Groves MD, Le Rhun E, Walker J, van den Bent M, Wen PY, Jaeckle KA. Leptomeningeal metastases: a RANO proposal for response criteria. Neuro-Oncology. 2017;19(4):484–92. https://doi.org/10.1093/neuonc/now183.
Rogers L, Barani I, Chamberlain M, Kaley TJ, McDermott M, Raizer J, Schiff D, Weber DC, Wen PY, Vogelbaum MA. Meningiomas: knowledge base, treatment outcomes, and uncertainties. A RANO review. J Neurosurg. 2015;122(1):4–23. https://doi.org/10.3171/2014.7.JNS131644.
Thibault I, Chang EL, Sheehan J, Ahluwalia MS, Guckenberger M, Sohn MJ, Ryu S, Foote M, Lo SS, Muacevic A, Soltys SG, Chao S, Gerszten P, Lis E, Yu E, Bilsky M, Fisher C, Schiff D, Fehlings MG, Ma L, Chang S, Chow E, Parelukar WR, Vogelbaum MA, Sahgal A. Response assessment after stereotactic body radiotherapy for spinal metastasis: a report from the SPIne response assessment in Neuro-Oncology (SPINO) group. Lancet Oncol. 2015;16(16):e595–603. https://doi.org/10.1016/S1470-2045(15)00166-7.
Warren KE, Poussaint TY, Vezina G, Hargrave D, Packer RJ, Goldman S, Wen PY, Pollack IF, Zurakowski D, Kun LE, Prados MD, Rutkowski S, Kieran MW. Challenges with defining response to antitumor agents in pediatric neuro-oncology: a report from the response assessment in pediatric neuro-oncology (RAPNO) working group. Pediatr Blood Cancer. 2013;60(9):1397–401. https://doi.org/10.1002/pbc.24562.
Barrett TF, Sarkiss CA, Dyvorne HA, Lee J, Balchandani P, Shrivastava RK. Application of ultrahigh field magnetic resonance imaging in the treatment of brain tumors: a meta-analysis. World Neurosurg. 2016;86:450–65. https://doi.org/10.1016/j.wneu.2015.09.048.
ACR Committee on Drugs and Contrast Media. ACR manual on contrast media version 10.3. Published Jun 2017. https://www.acr.org/Clinical-Resources/Contrast-Manual. Accessed 25 Jun 2018.
The Contrast Media Safety Committee of the European Society of Urogenital Radiology (ESUR). ESUR Guidelines on Contrast Agents, version 10.0. Published Mar 2018. Available at: http://www.esur-cm.org/index.php/en/. Accessed 25 Jun 2018.
Author information
Authors and Affiliations
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2020 Springer Nature Switzerland AG
About this chapter

Cite this chapter
Öztek, M.A. (2020). When and How to Use Imaging in Brain Tumors, Protocols. In: Özsunar, Y., Şenol, U. (eds) Atlas of Clinical Cases on Brain Tumor Imaging. Springer, Cham. https://doi.org/10.1007/978-3-030-23273-3_2
Download citation
DOI: https://doi.org/10.1007/978-3-030-23273-3_2
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-23272-6
Online ISBN: 978-3-030-23273-3
eBook Packages: MedicineMedicine (R0)