
Abstract
The development of ablation energy sources has allowed for catheter-based therapy of various arrhythmic substrates. Each energy source differs in its physiology of lesion formation as well as its relative advantages and disadvantages when harnessed for reduced-fluoroscopy ablation. Commonly used and alternative ablation energy sources are surveyed here. Specific considerations when these energy sources are utilized in low- and zero-fluoroscopy scenarios are addressed, and potential strategies that may be employed are outlined.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others

Keywords
Introduction
While the advent of the electrophysiology study in the 1960s–1970s provided the clinician with the ability to probe the behavior of intracardiac conduction and thereby elucidate the mechanisms of cardiac arrhythmias, therapeutic interventions were limited to open surgical techniques [1]. It was not until the development of catheter-based ablation modalities that percutaneous therapeutic options for arrhythmia management became widely available. Initial catheter ablation techniques utilized the delivery of direct-current (DC) shocks to the area of interest, which were both limited in efficacy and capable of significant harm, including cardiac perforation and unintended collateral injury [1, 2]. Presently, the primary energy sources used in catheter ablation are radiofrequency energy and cryothermal energy. In this chapter, we review how these energy sources have been harnessed in the ablation of cardiac arrhythmias, along with their use in the setting of fluoroscopic reduction.
Radiofrequency Energy
Radiofrequency (RF) energy has become the most widely used modality for the ablation of cardiac arrhythmias. When alternating current is delivered to an antenna, electromagnetic energy at wavelengths similar to radio waves can be generated. By allowing this energy to conduct through tissue, radiofrequency energy can be harnessed for lesion generation. By utilizing high-frequency stimulation, tissue heating and damage can occur in the absence of cardiac myocyte depolarization; as a result, proarrhythmia due to radiofrequency is avoided [3].
RF energy delivery during catheter ablation is transmitted from the metal electrode of the catheter to the grounding pad, traversing intervening tissue in the process. Every component of this electrical circuit contributes to the impedance of the system, and as the current passes through the tissue, energy is lost proportional to the impedance of the component. The energy expended traversing the impedance is dissipated as heat. While RF energy is expended along the entire course of its journey from the electrode-tissue interface to the grounding pad, due to the small surface area of the electrode compared to the grounding pad, the current density is highest at the electrode, with tissue heating thus occurring predominantly at the ablation site. A large proportion of delivered energy, however, is delivered to the surrounding blood pool, as a result of both the lower impedance of blood and a larger surface area of contact between the electrode and blood compared to the electrode and tissue [3].
Resistive heating occurring by impedance-mediated voltage drop results in a fairly shallow area of effect, limited largely to the first 1–1.5 mm of tissue depth [4]. Deeper tissue heating occurs via conduction of heat, which requires time to allow for sufficient penetration of energy to occur. Delayed results of ablation can thereby be seen even after RF application is halted, in a phenomenon referred to as thermal latency. While lesion depth can be increased by raising RF power, formation of coagulum once tissue temperatures approach 100 °C limits further energy delivery. Excessive heating of the tissue can also produce high-pressure steam vapor beneath the surface, which can then produce a “steam pop”—rupturing either into the endocardium, thus forming a crater, or into the pericardial space [2, 5]. Tissue temperatures between 50 and 90 °C delivered over at least 60 s provide ideal conditions for lesion formation [3, 4]. Convective cooling of the electrode tip by blood moving past the electrode tip reduces local tissue temperature and allows for greater energy delivery to the tissue of interest.
Irrigated tip RF catheters (Fig. 3.1) are designed to overcome limitations in lesion size formation by providing even more cooling of the tissue-electrode interface, allowing for greater energy delivery and even greater lesion depth. When compared to nonirrigated ablation catheters, irrigated catheters produce lesions that are larger in volume and greater in depth, and are less likely to cause rises in impedance, coagulum formation, steam pops, or crater formation [6]. Aside from these advantages, irrigated RF catheters also allow for effective ablation in areas with poor blood flow and convective cooling, such as in myocardial trabeculation or within the coronary sinus.

Radiofrequency (RF) ablation catheter tips. Left—nonirrigated 8 mm RF ablation catheter. Right—Irrigated 3.5 mm RF ablation catheter. Note ejection of saline via ports at distal end of catheter tip
At the cellular level, the effects of RF energy are dependent on the achieved tissue temperatures, with reversible loss of excitability seen in the 45–50 °C range, followed by permanent loss once tissue temperatures exceed ~54 °C [3]. Acutely, the local tissue undergoes protein denaturation with formation of a layer of fibrin. If tissue temperatures approach boiling point, char, thrombus, and coagulum may also be found. Surrounding a core of coagulation necrosis is a penumbra of hemorrhagic tissue and inflammation. With maturation, this forms a well-demarcated lesion comprised of fibrosis and chronic inflammatory infiltrates. However, some variability in maturation can occur at the transition zone of the acute lesion, with either progressive inflammatory changes and necrosis resulting in what may be referred to as lesion expansion, or healing of the tissue resulting in recovery of function [3].
Multielectrode RF ablation catheters designed specifically for pulmonary vein isolation (PVI) allow for rapid ablation from multiple electrodes situated on the catheter. These systems utilize phased RF energy, whereby ablation can occur simultaneously in either a unipolar (vs. grounding pad) or a bipolar fashion (vs. another electrode on the catheter). Lesion depth is provided by unipolar ablation, while confluent lesions between electrodes are provided by bipolar ablation [7]. Deflectable, circular multielectrode catheters are designed for ablation at the antrum of pulmonary veins, while multielectrode catheters preformed in specific geometric shapes facilitate mapping and modification of left atrial substrate [8]. A higher rate of silent cerebral ischemic events has been observed with PVI with multielectrode RF catheters [9, 10]. Saline-irrigated systems have been introduced to curtail this increased incidence of silent cerebral microemboli [2].
Cryoablation
Cryoablation utilizes cryothermal energy to produce tissue freezing and subsequent lesion formation. Generation of cryothermal energy is reliant on the Joule-Thomson effect, where precooled liquid refrigerant is delivered to the catheter tip and allowed to rapidly decompress and expand, resulting in a fall in temperature. This allows for catheter tip temperatures to approach −75 °C or lower. With relatively mild tissue cooling (0 to −20 °C), ice crystals form in the extracellular space, resulting in osmotic shift of water out of cells. This produces reversible cellular damage initially, but can become irreversible following prolonged cooling. With deeper cooling (<−40 °C), intracellular crystals form, resulting in direct damage to cardiac myocytes and cell death. Vasoconstriction also occurs with the temperature drop, and may persist for hours after thawing. This leads to ischemia-mediated necrosis [3, 11]. While the freeze is the most obvious means of lesion formation, the thaw and rewarming phase also contributes to tissue injury. Thawing of intracellular ice crystals further damages cellular organelles, while hyperemia leads to edema formation and an inflammatory response [3]. As a result, freezing followed by thawing followed by another freeze (a freeze-thaw-freeze cycle) is usually performed to maximize the results of cryoablation.
Similar to RF ablation, the tissue adjacent to the catheter tip experiences the most effective ablation effect, as intense local cooling results in tissue damage occurring typically within the first 30 s of ablation. More peripheral areas not only receive comparatively less cooling, but the effect is also delayed; thus, these regions are more likely to recover following rewarming. Unlike RF lesions that benefit from high surrounding blood flow and convective cooling to improve power delivery and thus generate larger lesions, cryoablation lesions suffer from convective warming as it may limit tissue freezing. As a result, cryoablation fares better in areas of low blood flow [3]. Compared to lesions produced by RF ablation, cryoablation lesions generally demonstrate less endothelial damage and thrombus formation [3, 11].
Cryoablation provides certain advantages over RF ablation. Formation of ice at the catheter tip during cryothermal energy application results in the catheter becoming firmly attached to the ablation area. This is known as cryoadherence , and allows for catheter stability despite cardiorespiratory motion. As noted above, mild cooling allows for reversible disruption of myocyte function, and this can be harnessed via cryomapping . By cooling the tissue to −30 °C for no more than 60 s, electrophysiologic testing can be performed to assess the effects of tissue disruption, and full cryoablation subsequently applied if the desired effect is observed. If either an undesired effect or a lack of response is seen, cryomapping can be stopped, with full recovery of tissue function. Coupled with more dense and better demarcated lesions, cryoablation allows for an increased margin of safety when ablating areas in close proximity to vital cardiac structures due to its potentially reversible, more compact lesions [3, 11].
Disadvantages with this energy source , however, are at times an extension of their potential benefits. Procedural duration may be increased due to the time required to provide sufficient cooling of the tissue, as up to 240 s is provided per ablation lesion. Completion of a full freeze-thaw-freeze cycle may then be required, further lengthening procedural time [12]. Recurrences may also be more likely, as permanent lesions require accurate catheter placement such that the region of interest receives sufficient cooling from the catheter tip as opposed to reversible stunning.
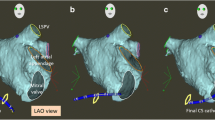
The cryoballoon (Fig. 3.2) is a specialized tool that harnesses cryothermal energy for PVI procedures. Once the balloon is inflated within the left atrium, it can be maneuvered into the antrum of the pulmonary vein. An appropriate seal between the balloon and the pulmonary vein is confirmed, followed by introduction of cryorefrigerant into the balloon, resulting in circumferential ablation of the antrum of the vein.

Cryoballoon ablation catheter . Left—cryoballoon deflated with circular multipolar mapping catheter extruding from distal end. Right—cryoballoon inflated with active cryoablation application. Note the formation of ice cap on the side of the balloon closest to the circular mapping catheter
Other Energy Sources
In clinical practice, RF and cryothermal energy sources serve as the primary modalities harnessed for the ablation of cardiac arrhythmias. However, a handful of other energy sources have been investigated for their potential use in this arena. While these alternative energy sources either have failed to establish clinical utility or serve a very specific niche, they nonetheless deserve mention.
Laser Energy
Laser energy delivers photons to the target tissue which are absorbed by molecules in the tissue known as chromophores, exciting them and thereby creating thermal injury [5]. Balloon-based systems using laser energy are available for PVI. Once deployed within the antrum of the pulmonary vein, direct visualization of the endocardial surface is achieved via endoscopic views from within the balloon. Laser energy can then be delivered from the catheter shaft within the balloon to create a circumferential lesion around the vein [2, 13]. The efficacy of this strategy appears comparable to the use of other energy modalities, with a potentially favorable risk of complications [13, 14].
Microwave Energy
Microwave energy, when applied to cardiac tissue, causes kinetic excitement of water molecules, thereby causing intermolecular friction and generation of heat. Unlike RF ablation, there is no reliance on resistive heating, and thus energy can be delivered at a distance from the delivery source without direct contact [3, 5]. Despite initial attempts to bring microwave ablation into routine clinical practice, difficulties in the incorporation of this technology in catheter designs have limited its utility [3].
Ultrasound Energy
High-frequency sound waves can be focused on the tissue of interest to produce tissue injury at a distance from the delivery source. Ultrasound energy produces thermal heating upon attenuation within cardiac tissue. On top of this, microcavitation results from the generation of microbubbles within the tissue that expand and collapse violently, further causing cellular injury. High-intensity focused ultrasound (HIFU) can produce intramural lesions in the absence of tissue contact or injury to intervening structures [15]. Attempts to introduce HIFU into atrial fibrillation ablation have been limited due to the persistence of gaps within linear lesions produced by the technique, as well as a number of complications including unintended collateral injury to the phrenic nerve and esophagus [5, 16]. In addition, complications may result from cavitation in much the same way as steam pops during RF ablation, including cardiac perforation and tamponade [15]. The narrow therapeutic window with HIFU has thus to-date limited its routine clinical use [14, 16].
Considerations with Fluoroscopic Reduction in Selection of Ablation Energy Sources
Fluoroscopy has been the mainstay for visualization of catheter position during ablation procedures. Attempts at fluoroscopic reduction have employed a number of different strategies, some of which apply more readily to some ablation energy sources than others. We review below some of these strategies and their utility with different energy sources.
Electroanatomical Mapping
The advent of electroanatomical mapping (EAM) has allowed for fluoroscopic reduction by allowing for the accurate determination and portrayal of catheter position in three-dimensional space. By superimposing functional electrical data onto a 3D representation of the heart, both anatomy and electrophysiology can be displayed simultaneously [2]. In order to register on current EAM systems, catheters require either an active electrode (in impedance-based systems) or proprietary location sensors (in electromagnetic sensor-based systems); however, some combination of these two localization systems are currently employed by leading EAM systems. As a result, in the absence of any limitations posed by technical considerations, zero-fluoroscopy ablation can be achieved with comparable efficacy using either RF or cryothermal energy using available EAM systems [17].
Limitations of EAM systems may still exist with certain ablation energy types, however, and may influence the choice of ablation energy if zero-fluoroscopy ablation is desired. Unlike RF ablation, EAM support for cryothermal ablation is somewhat less universal. Certain EAM setups that require proprietary location sensors on its ablation catheter may need to be “tricked” into recognizing cryoablation catheters [17, 18]. On the other hand, the absence of electrodes or proprietary sensors on the inflatable balloon on certain PVI ablation systems may limit the exclusive use of EAM systems in visualizing adequate balloon positioning, unless intracardiac echocardiography is simultaneously used (see below).
Intracardiac Echocardiography
Intracardiac echocardiography (ICE) , when integrated with EAM systems, can facilitate generation of anatomical geometries by translating echocardiographic images into anatomical shells. Moreover, it can be used to confirm catheter tip position when anatomically complex structures that are poorly defined by routine EAM are encountered (e.g., papillary muscles).
As noted earlier, ICE can also be used to visualize catheter components not usually visible with EAM, most notably deployment of the cryoballoon in the pulmonary vein antrum during PVI. Once positioned, the adequacy of balloon seal can also be determined without fluoroscopy by using color flow Doppler imaging to look for leaks. In addition, as phrenic nerve palsy is a known complication of cryoballoon PVI, ICE can also be employed to directly visualize diaphragmatic excursion in place of fluoroscopy [19]. By combining ICE with EAM, zero-fluoroscopy cryoballoon PVI procedures may thus be safely performed [18].
Contact Force
Contact force (CF) determination is yet another technologic innovation that can aid in fluoroscopic reduction. Adequate tissue-electrode contact is highly sought after in order to ensure sufficient ablation energy delivery to the tissue of interest to produce desired lesion depth and durability. While tactile feedback and surrogate markers including local electrogram attenuation and impedance drops provide some indication of this, fluoroscopy is conventionally relied upon to confirm motion of the catheter tip as it is held in contact with the endocardium [20].
By detecting either force transduced by spring-based sensors or changes in interference patterns of reflected light by deformation of the catheter tip, CF can be measured. Studies have confirmed that increased CF correlates with improved tissue contact and results in higher tissue temperatures during ablation, improved catheter stability, and larger lesion size [20]. When used for PVI procedures, this has been shown to translate to lower recurrence rates and shorter procedural times, with a trend towards reduced complications [21].
Fluoroscopy can thereby be avoided when CF is used in conjunction with EAM, as this can be employed to not only determine tissue-electrode contact, but also confirm accuracy of created geometry and warn against potential cardiac perforation [2]. A meta-analysis comparing the use of CF ablation catheters with conventional ablation catheters in PVI showed a significant reduction in fluoroscopic time by ~20% [21]. Currently, contact force technology is available only for radiofrequency ablation catheters.
Conclusions
The advent of numerous safe and efficacious ablation energy sources that may be delivered via a steerable catheter has provided the clinician the tools to effect electrophysiologic change and thereby treat arrhythmias. Cardiac electrophysiologists who wield these tools need to be aware of their unique therapeutic attributes, including both their comparative strengths and limitations. With the promulgation of low- and zero-fluoroscopic ablation procedures, an appreciation must also be developed of how facilely each energy source may be incorporated into these procedures. By recognizing the limitations in the use of a given energy source in fluoroscopic reduction, strategies may be employed to circumvent any barriers or an alternative energy source may be selected. Furthermore, as more novel energy sources are harnessed, fluoroscopic reduction will need to be presciently incorporated.
References
Joseph JP, Rajappan K. Radiofrequency ablation of cardiac arrhythmias: past, present and future. QJM. 2012;105:303–14.
Andrade JG, Rivard L, Macle L. The past, the present, and the future of cardiac arrhythmia ablation. Can J Cardiol. 2014;30:S431–41.
Issa Z. Ablation energy sources. In: Issa ZF, Miller JM, Zipes DP, editors. Clinical arrhythmology and electrophysiology: a companion to Braunwald’s heart disease. 1st ed. Philadelphia, PA: Saunders Elsevier; 2009.
Wittkampf FH, Nakagawa H. RF catheter ablation: lessons on lesions. Pacing Clin Electrophysiol. 2006;29:1285–97.
Cummings JE, Pacifico A, Drago JL, Kilicaslan F, Natale A. Alternative energy sources for the ablation of arrhythmias. Pacing Clin Electrophysiol. 2005;28:434–43.
Dorwarth U, Fiek M, Remp T, et al. Radiofrequency catheter ablation: different cooled and noncooled electrode systems induce specific lesion geometries and adverse effects profiles. Pacing Clin Electrophysiol. 2003;26:1438–45.
Kiss A, Sandorfi G, Nagy-Balo E, Martirosyan M, Csanadi Z. Phased RF ablation: results and concerns. J Atr Fibrillation. 2015;8:1240.
Andrade JG, Dubuc M, Rivard L, et al. Efficacy and safety of atrial fibrillation ablation with phased radiofrequency energy and multielectrode catheters. Heart Rhythm. 2012;9:289–96.
Herrera Siklody C, Deneke T, Hocini M, et al. Incidence of asymptomatic intracranial embolic events after pulmonary vein isolation: comparison of different atrial fibrillation ablation technologies in a multicenter study. J Am Coll Cardiol. 2011;58:681–8.
Gaita F, Leclercq JF, Schumacher B, et al. Incidence of silent cerebral thromboembolic lesions after atrial fibrillation ablation may change according to technology used: comparison of irrigated radiofrequency, multipolar nonirrigated catheter and cryoballoon. J Cardiovasc Electrophysiol. 2011;22:961–8.
Skanes AC, Klein G, Krahn A, Yee R. Cryoablation: potentials and pitfalls. J Cardiovasc Electrophysiol. 2004;15:S28–34.
Manusama R, Timmermans C, Limon F, Philippens S, Crijns HJ, Rodriguez LM. Catheter-based cryoablation permanently cures patients with common atrial flutter. Circulation. 2004;109:1636–9.
Schade A, Krug J, Szollosi AG, El Tarahony M, Deneke T. Pulmonary vein isolation with a novel endoscopic ablation system using laser energy. Expert Rev Cardiovasc Ther. 2012;10:995–1000.
Filgueiras-Rama D, Merino JL. The future of pulmonary vein isolation—single-shot devices, remote navigation or improving conventional radiofrequency delivery by contact monitoring and lesion characterisation? Arrhythm Electrophysiol Rev. 2013;2:59–64.
Laughner JI, Sulkin MS, Wu Z, Deng CX, Efimov IR. Three potential mechanisms for failure of high intensity focused ultrasound ablation in cardiac tissue. Circ Arrhythm Electrophysiol. 2012;5:409–16.
Neven K, Schmidt B, Metzner A, et al. Fatal end of a safety algorithm for pulmonary vein isolation with use of high-intensity focused ultrasound. Circ Arrhythm Electrophysiol. 2010;3:260–5.
Scaglione M, Ebrille E, Caponi D, et al. Zero-fluoroscopy ablation of accessory pathways in children and adolescents: CARTO3 electroanatomic mapping combined with RF and cryoenergy. Pacing Clin Electrophysiol. 2015;38:675–81.
Patel N. Experience with arctic front advance cryoablation system for paroxysmal atrial fibrillation in an established fluoroless EP lab. EP Lab Digest. 2016;16(3).
Su W, Kowal R, Kowalski M, et al. Best practice guide for cryoballoon ablation in atrial fibrillation: the compilation experience of more than 3000 procedures. Heart Rhythm. 2015;12:1658–66.
Shah DC, Namdar M. Real-time contact force measurement: a key parameter for controlling lesion creation with radiofrequency energy. Circ Arrhythm Electrophysiol. 2015;8:713–21.
Shurrab M, Di Biase L, Briceno DF, et al. Impact of contact force technology on atrial fibrillation ablation: a meta-analysis. J Am Heart Assoc. 2015;4:e002476.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2019 Springer Nature Switzerland AG
About this chapter

Cite this chapter
Khoo, C. (2019). Ablation Energy Sources: Principles and Utility in Ablation Without Fluoroscopy. In: Proietti, R., Wang, Y., Yao, Y., Zhong, G., Lin Wu, S., Ayala-Paredes, F. (eds) Cardiac Electrophysiology Without Fluoroscopy. Springer, Cham. https://doi.org/10.1007/978-3-030-16992-3_3
Download citation
DOI: https://doi.org/10.1007/978-3-030-16992-3_3
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-16991-6
Online ISBN: 978-3-030-16992-3
eBook Packages: MedicineMedicine (R0)