
Abstract
The following study expands Dr. Penelope Trickett’s research on the heterogeneity in outcomes related to childhood maltreatment by testing the associations between perception of maltreatment as adolescents’ most upsetting experience and mental health symptoms. We expected adolescents who reported maltreatment (vs. nonmaltreatment) as their most upsetting experience would experience greater internalizing and externalizing behavior problems across adolescence. We also expected emotionally abused/neglected youth compared to sexually/physically abused youth would fare better when reporting a maltreatment (vs. nonmaltreatment) most upsetting experience. Hypotheses were tested with data collected from 303 maltreated (n = 151 girls) adolescents across four waves of measurement. Trajectories of depression and anxiety symptoms differed for girls reporting maltreatment versus nonmaltreatment as their most upsetting experience. Boys reporting maltreatment (vs. nonmaltreatment) as their most upsetting experience had lower levels of aggression and rule breaking behavior at wave 1. Findings from the present study are relevant for clinicians as an indicator of risk for mental health problems and suggest tailored treatment plans for boys versus girls. Findings from the present study should be used to support legislation that prioritizes children and their families, providing resources to limit the traumatic nature of maltreatment in order to reduce the short- and long-term mental health consequences associated with perceptions of maltreatment as upsetting.
Access provided by CONRICYT-eBooks. Download chapter PDF
Similar content being viewed by others


Keywords
- Child maltreatment
- Maltreatment perception
- Internalizing problems
- Externalizing behavior
- Gender differences
Child maltreatment is a serious public health concern and the consequences of maltreatment are pervasive, spanning multiple domains of functioning. Although the experience of child maltreatment has many known developmental consequences that can manifest across the lifespan (Trickett & McBride-Chang, 1995; Trickett, Negriff, Ji, & Peckins, 2011), not all children who experience maltreatment go on to develop mental health problems. Protective factors such as familial support and self-esteem are thought to impact a child’s resilience in the face of adversity (Masten, 2001) yet few studies are able to longitudinally test for lasting positive or negative effects on development. Furthermore, less is known about how the perception of maltreatment experiences are associated with risk and resilience across development. Thus, the purpose of this study was to test whether the perception of maltreatment experiences as upsetting was associated with the development of internalizing and externalizing behavior problems during adolescence, a developmental period when internalizing symptoms and externalizing behaviors may increase in prevalence and severity (Moffitt, 1993; Petersen et al., 1993).
3.1 Perception of Maltreatment
Perception of an experience is a multifaceted construct as it is influenced by numerous psychological and contextual circumstances, such as an individual’s emotional or psychological state at the time of occurrence or recollection as well as all of the individual’s previous experiences and memories (Wilson & Ross, 2003). As the time since the event in question increases, perception of the event may change based on new experiences (Wilson & Ross, 2003), making the assessment of perception of a childhood experience a difficult task. Few studies have considered maltreated children’s perception of maltreatment experiences as a protective or risk factor for mental health processes, yet other studies of children and adults suggest perception of a traumatic event may be an important predictor of resilience (Boals & Schuettler, 2009). For instance, in a retrospective study of adults recalling their most traumatic experience, the perceived feeling of fear or helplessness during the event rather than characteristics of the event itself predicted the presence of PTSD symptoms (Boals & Schuettler, 2009). Similarly, one bereavement study of children and adolescents suggested the perception of loss is important for predicting outcomes, finding that adolescents’ perceived impact of the loss was positively associated with symptoms of depression (Harrison & Harrington, 2001).
Studies of disclosure which capture a component of perception (i.e., maltreatment is wrong and should be reported) also lend support for the role of perception in predicting mental health problems. The decision to disclose and the mental health effects of disclosure for children and adults vary by characteristics of the child (e.g., age), maltreatment (e.g., type), and disclosure experience (e.g., social reaction) (Goodman-Brown, Edelstein, Goodman, Jones, & Gordon, 2003; Graham-Bermann, Kulkarni, & Kanukollu, 2011; Nagel, Putnam, Noll, & Trickett, 1997; Ullman, 2007). For example, in children exposed to physical threat in the home, disclosure was associated with greater improvement in internalizing problems and reductions in pro-violent cognitions (Graham-Bermann et al., 2011). However, studies of adult women survivors of child sexual abuse found voluntary disclosure to be associated with worse mental health outcomes (Nagel et al., 1997) and women who did not disclose and engaged in repressive coping reported fewer internalizing and externalizing behavior problems (Bonanno, Noll, Putnam, O'Neill, & Trickett, 2003). The findings from previous studies on disclosure suggest aspects of the maltreatment or disclosure experience such as threat (e.g., sexual abuse) and deprivation (e.g., lack of social support) may play a role in the emergence and progression of internalizing and externalizing behavior problems across adolescence (McLaughlin, Sheridan, & Lambert, 2014). Despite evidence from studies of perceived impact and disclosure suggesting perception of maltreatment is important for understanding the development of mental health problems, no studies have directly tested this hypothesis in maltreated youth. The present study aims to address this gap in the literature by testing whether adolescents’ perception of maltreatment as their most upsetting experience is associated with the development of internalizing and externalizing behavior problems across adolescence and whether this association is conditional on maltreatment type.
3.2 Gender Differences
Boys and girls differ in a variety of biological and behavioral domains and in some situations, experience and respond to the environment differently. For example, boys and girls differ in their biological reactivity to different types of challenges (e.g., social stressor vs. cognitive stressor) (Stroud, Salovey, & Epel, 2002) and in response to psychological distress girls are more likely than boys to use emotion-focused coping strategies and seek comfort from a social support network (Brougham, Zail, Mendoza, & Miller, 2009; Eschenbeck, Kohlmann, & Lohaus, 2007). Gender differences in the biopsychosocial response to threat are considered to be adaptive from an evolutionary standpoint (Crick & Zahn–Waxler, 2003; Klein & Corwin, 2002; Taylor et al., 2000). Therefore, although studies suggest boys and girls experience similar rates of maltreatment (Finkelhor, Turner, Shattuck, & Hamby, 2015; Prevoo, Stoltenborgh, Alink, Bakermans-Kranenburg, & van Ijzendoorn, 2017), the mental health consequences of maltreatment are expected to differ. To account for gender differences in the response to maltreatment as well as mental health outcomes, the association between perception of maltreatment, internalizing and externalizing behavior problems, and maltreatment type was examined separately for boys and girls .
3.3 Present Study
The following study tested whether perception of maltreatment as the most upsetting experience was associated with internalizing and externalizing behavior problems in maltreated youth separately for boys and girls, and whether maltreatment type moderated these associations. We were not able to directly measure adolescents’ perceptions of maltreatment. Instead, we asked adolescents to describe their most upsetting experience. The nature of these analyses were primarily exploratory due to the lack of research available on perception of maltreatment experiences in youth. The closest evidence that we can draw from to formulate hypotheses is the disclosure literature that suggests disclosure is associated with greater mental health problems in individuals with sexual abuse experiences (Bonanno et al., 2003; Nagel et al., 1997; Ullman, 2007). Therefore, we hypothesized that maltreated girls who perceived maltreatment as being their most upsetting experience would report experiencing greater internalizing problems than girls who did not perceive maltreatment as their most upsetting experience. Similarly, we hypothesized that maltreated boys who perceived maltreatment as being their most upsetting experience would report greater externalizing behavior problems than boys who did not perceive maltreatment as being their most upsetting experience. We also acknowledge that the association between perception of maltreatment as upsetting and mental health may differ by maltreatment type. Therefore, we also hypothesized maltreatment type would moderate these associations such that boys and girls with a history of emotional abuse and/or neglect (without sexual or physical abuse experiences) would report fewer internalizing and externalizing behavior problems when identifying maltreatment as their most upsetting experience compared to those reporting a nonmaltreatment most upsetting experience.
3.4 Methods
3.4.1 Sample Characteristics
Data were from four waves of an ongoing longitudinal study examining the effects of maltreatment on adolescent development. At Time 1 (T1), the sample was composed of 454 adolescents aged 9–13 years (n = 241 boys, n = 213 girls). Time 2 (T2), Time 3 (T3), and Time 4 (T4) occurred on average 1, 2.7, and 7.2 years after baseline. The present study only used data from the maltreated sample of 303 maltreated (n = 151 girls) youth (T1 M age = 10.87 years, SD = 1.13). The maltreated sample was diverse, consisting of youth identifying as Black or African American (n = 123, 41%), Latino (n = 106, 35%), White/non-Latino (n = 35, 12%), or Biracial (n = 39, 13%). Descriptive characteristics of the sample can be found in Table 3.1. Percentages for ethnicity, maltreatment type, and maltreatment type grouping are calculated by gender and most upsetting experience.
3.4.2 Sample Recruitment
Maltreated youth were recruited from active cases in the Children and Family Services (CFS) of a large west coast city. The inclusion criteria were: (1) a new substantiated referral to CFS in the preceding month for any type of maltreatment (e.g., neglect, physical abuse, sexual abuse, emotional abuse); (2) child age of 9–12 years; (3) child identified as Latino, African-American, or White (non-Latino); and (4) child residing in one of 10 zip codes in a designated county at the time of referral to CFS. With the approval of CFS and the Institutional Review Board (IRB) of the affiliated university, potential participants were contacted via postcard and asked to indicate their willingness to participate. Contact via mail was followed by a phone call. A Certificate of Confidentiality was obtained from the Federal Government to protect each participant’s confidentiality. Disclosures of maltreatment that were not already reported to a CFS agency were not protected under this agreement. Retention strategies (e.g., contact through back-up contact information and social media) were effective as 81%, 64%, and 73% of the maltreated sample was retained at waves 2, 3, and 4, respectively. Information on recruitment and retention for the comparison sample not included in the present study is available in an earlier publication (Negriff, Saxbe, & Trickett, 2015).
3.4.3 Procedure
Assessments were conducted at an urban research university and all procedures were reviewed and approved by the IRB of the affiliated university. Following assent and consent from the adolescent and parent/guardian, the adolescent completed an array of questionnaires and tasks during a four-hour protocol, including hormonal, cognitive, behavioral, and health measures. Only a subset of the measures were used in the following analyses. Child and parent/guardian participants were compensated according to the National Institutes of Health Normal Volunteer Program guidelines.
3.4.4 Measures
Perception of Maltreatment as Most Upsetting Experience
Adolescents completed the Comprehensive Trauma Interview (CTI) (Horowitz, 1999; Noll, Horowitz, Bonanno, Trickett, & Putnam, 2003) at T3 and T4. The CTI includes a screen for 34 potentially traumatic experiences and a follow-up portion to capture relevant information regarding each event (e.g., age at occurrence, identity of perpetrator). During the follow-up, adolescents were asked to describe their most upsetting experience. Responses were coded according to whether or not the experience was a form of child maltreatment as defined by the Centers for Disease Control and Prevention (CDC) (Leeb, Paulozzzi, Melanson, Simon, & Arias, 2008). Examples of nonmaltreatment most upsetting experiences included the death of a relative or friend, witnessing or knowing the victim of neighborhood violence, and having a sick relative or friend. Coded responses were used to categorize adolescents into one of two groups: adolescents who perceived maltreatment to be their most upsetting experience (34% boys, 57% girls) and adolescents who did not perceive maltreatment to be their most upsetting experience (66% boys, 43% girls).
Internalizing Problems
Symptoms of depression were assessed at all four waves of measurement by self-report using the Child Depression Inventory (CDI) (Kovacs, 1981, 1992). Adolescents rated symptoms of depression (k = 27) on a scale of 0–2 with higher scores indicating more severe symptoms (α = .86–.89). Responses were summed to create a composite score of depressive symptoms. Symptoms of anxiety were assessed at all four waves of measurement by self-report with the Multidimensional Anxiety Scale for Children (MASC) (March, Parker, Sullivan, Stallings, & Conners, 1997). The MASC consists of 30 items on a scale from 0 to 3 with higher scores representing greater symptom severity. Only MASC items administered at all four waves (k = 21) were summed to create a composite score of anxiety symptoms (α = .87–.90). MASC items not administered at T4 (k = 9) due to the age appropriateness of the questions were not included in the anxiety sum scores at T1-T3 .
Externalizing Behavior Problems
Subscales from the Youth Self Report (YSR) (Achenbach & Rescorla, 2001) assessed aggressive behavior (k = 14 items) and rule breaking behavior (k = 10 items) at all four waves of measurement by self-report. For each item, adolescents reported whether the statement was “never true,” “sometimes true,” or “always true.” Items that were not administered at T3 and T4 for aggressive behavior (k = 3 items) and rule breaking behavior (k = 1 item) due to the age inappropriateness of the questions, and rule breaking behavior items that improved Cronbach’s α when deleted (k = 1 item) were not included in the aggressive behavior and rule breaking behavior sum scores (aggressive behavior α = .80–.84; rule breaking behavior α = .75–.79).
Maltreatment Type
Records from the CFS agency were carefully reviewed and documented at T1 for each child’s history and type of maltreatment using the Maltreatment Case Record Abstraction Instrument (MCRAI) (Barnett, Manly, & Cicchetti, 1993; Mennen, Kim, Sang, & Trickett, 2010). In this sample, 232 youth (74% girls, 80% boys) experienced neglect, 156 youth (55% girls, 48% boys) experienced emotional abuse, 156 youth (44% girls, 59% boys) experienced physical abuse, and 60 youth (27% girls, 13% boys) experienced sexual abuse. In order to more meaningfully test for effects of maltreatment type, maltreated youth were classified into two mutually exclusive groups according to their sexual and physical abuse history. One group consisted of sexually and/or physically abused adolescents who may have also experienced emotional abuse and/or neglect (61% girls, 67% boys). Sexually and physically abused adolescents were grouped together because victims of sexual and/or physical abuse are more likely to have experienced poly-victimization (U.S. Department of Health and Human Services, 2012) and psychological trauma (Leeb et al., 2008) compared to victims of emotional abuse and neglect. A second group consisted of adolescents who experienced emotional abuse and/or neglect without a history of sexual or physical abuse (39% girls, 33% boys).
Covariates
The time-varying covariate age was included as a covariate to account for the increase in prevalence and severity of internalizing and externalizing behavior problems that occurs during adolescence (Petersen et al., 1993). Age was also considered to be a proxy for pubertal development as the two are highly correlated and the majority of adolescents age out of pubertal staging (i.e., Tanner Stage 5) by age 15 (Slyper, 2006). The time-invariant covariate ethnicity was reported by the adolescent’s parent or guardian at T1 as being Black/African-American (35%, 52%), Latino (42%, 25%), White (non-Latino) (8%, 11%), or Biracial (15%, 12%) for adolescents reporting maltreatment and nonmaltreatment as their most upsetting experience, respectively. Ethnicity was included as a covariate to account for ethnic differences in risk for internalizing and externalizing behavior problems in adolescents (López et al., 2017). In the US, the largest percentage of victimized youth identified as being White/non-Latino (44%) (U.S. Department of Health and Human Services, 2012); therefore, in subsequent analyses adolescents’ ethnicity was regrouped as either being White (non-Latino) or an ethnic minority (Black/African American, Latino, or Biracial) .
3.4.5 Analytic Plan
Descriptive analyses were performed for all continuous variables by gender. Hypotheses were tested using linear and quadratic growth models in a multilevel model framework using SAS ® (Version 9.4) Proc Mixed. Missing data were accounted for with restricted maximum likelihood (REML) estimation. Growth models were fit separately for depressive symptoms, anxiety symptoms, rule breaking behaviors, and aggressive behaviors, stratified by gender. All model predictors were grand mean centered so that the intercept represents the average mental health outcome for the prototypical adolescent at T1. Models were built by fitting an unconditional (i.e., no growth) model, a linear growth model with intercept at T1, a quadratic growth model with intercept at T1, a linear or quadratic growth model with most upsetting experience as a time-invariant covariate, and then testing the moderating effect of maltreatment type on the association between the mental health outcome and most upsetting experience. For each of the outcomes, the best fitting model for depressive symptoms, aggressive behavior, and rule breaking behavior in boys and girls, and anxiety symptoms in boys included the linear term and covariates. The best fitting model for symptoms of anxiety in girls included the quadratic term and covariates. The results did not differ when covariates were removed from models.
3.5 Results
3.5.1 Descriptive Analyses
Descriptive statistics of study measures are presented in Table 3.2. Results from independent t-tests show mean differences in internalizing and externalizing behavior problems between boys and girls. On average, compared to boys, girls: reported more symptoms of depression at T4 (t222 = −2.59, p < .05); reported more symptoms of anxiety at T1 (t299 = −2.03, p < .05), T3(t191 = −2.88, p < .01), and T4 (t219 = −3.98, p < .01); reported fewer aggressive behaviors at T1 (t299 = 2.59, p < .05); and reported fewer rule breaking behaviors at T1 (t299 = 3.04, p < .01).
In girls, those reporting maltreatment (vs. nonmaltreatment) as their most upsetting experience were older at T3 (t102 = −2.30, p < .05). In boys, those reporting maltreatment (vs. nonmaltreatment) as their most upsetting experience: were younger at T4 (t101 = 2.19, p < .05); reported fewer aggressive behaviors at T1 (t108.36 = 2.07, p < .05) and T2 (t100 = 2.19, p < .05); and reported fewer rule breaking behaviors at T1 (t114.63 = 3.22, p < .01).
3.5.2 Hypothesis Tests
Intraclass Correlation Coefficients (ICC)
Unconditional, no-growth models (i.e., intercept only) were fit for both boys and girls for symptoms of depression, symptoms of anxiety, aggressive behavior, and rule breaking behavior. The ICC for boys and girls was .48 and .43 (symptoms of depression), .29 and .23 (symptoms of anxiety), .35 and .42 (aggressive behavior), and .30 and .24 (rule breaking behavior), respectively.
Internalizing and Externalizing Behavior Problems in Girls
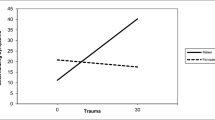
Model estimates for girls are presented in Table 3.3. In girls, the trajectory of depressive symptoms differed according to most upsetting experience; girls reporting maltreatment as their most upsetting experience increased in symptoms of depression across adolescence whereas girls reporting nonmaltreatment as their most upsetting experience decreased in symptoms of depression across adolescence (Fig. 3.1). Most upsetting experience was also associated with change in anxiety symptoms over time. Girls reporting a nonmaltreatment most upsetting experience decreased in symptoms of anxiety at a steeper rate from T1 to T2, and increased in anxiety symptoms at a steeper rate from T3 to T4 compared to girls reporting a maltreatment most upsetting experience (Fig. 3.2). Maltreatment type did not moderate the association between most upsetting experience and depressive or anxiety symptoms, or in the change in depressive or anxiety symptoms over time.

Depression symptom trajectories differ according to most upsetting experience in girls

Anxiety symptom trajectories differ according to most upsetting experience in girls
In girls, most upsetting experience was not associated with the trajectory of aggressive behavior. However, most upsetting experience was associated with rule breaking behavior at T1 of the study and this association was conditional on maltreatment type. Of girls who experienced emotional abuse and/or neglect (without sexual and/or physical abuse experiences), those reporting maltreatment as their most upsetting experience reported lower levels of rule breaking behavior than girls with a nonmaltreatment most upsetting experience (Fig. 3.3).

Rule breaking behavior at Time 1 differs according to most upsetting experience and maltreatment type in girls
Internalizing and Externalizing Behavior Problems in Boys
Model estimates for boys are presented in Table 3.4. In boys , most upsetting experience was not associated with the trajectories of depressive or anxiety symptoms, nor was there a moderating effect of maltreatment type on any of the associations. However, in boys, those reporting maltreatment as their most upsetting experience had lower levels of aggressive behavior and rule breaking behavior at T1 than boys reporting nonmaltreatment as their most upsetting experience.
3.6 Discussion
Our study found that girls’ and boys’ reports of most upsetting experience were associated with internalizing and externalizing behavior problems during adolescence. Regardless of maltreatment type, reporting maltreatment as their most upsetting experience was associated with increased depressive symptoms and less steep change in anxiety symptoms over time in girls, and lower levels of aggressive and rule breaking behavior in boys. Further, in girls with a history of emotional abuse and/or neglect, rule breaking behavior was lower at study onset in girls reporting a maltreatment most upsetting experience. Our results for depression and rule breaking behavior in girls are consistent with the disclosure literature (Bonanno et al., 2003; Graham-Bermann et al., 2011; Nagel et al., 1997). For boys, the results are consistent with disclosure of non-sexual forms of maltreatment (Graham-Bermann et al., 2011) however the association was present for both emotionally abused/neglected and physically/sexually abused boys. Our finding of gender differences may be attributed to differences in coping responses to adversity between boys and girls (for example, see Eschenbeck et al., 2007) and the effectiveness of those coping strategies (Littleton, Horsley, John, & Nelson, 2007; Schnider, Elhai, & Gray, 2007), contributing to differences in what type of experience boys and girls find most upsetting and how this perception relates to mental health. However, we are not able to test these important questions with data from the current study but these are avenues of research future studies can explore.
3.6.1 Clinical Implications
Findings from the present study offer a broader understanding of how perceptions of maltreatment as an adolescent’s most upsetting experience relate to mental health outcomes across adolescence for clinicians, social workers, and other advocates for the health and wellbeing of children. Our findings suggest clinicians can gauge maltreated children’s risk for depression, anxiety, aggression, and rule breaking behavior by asking children to reflect on their most upsetting experience. Treatment plans can then be tailored to address each child’s individual risk. Tools for discussing most upsetting experiences have already been developed and shown to be feasible in treatment and intervention settings. For example, clinicians administering PTSD assessments prompt children to describe their most significant trauma and clinicians administering Trauma-Focused Cognitive Behavioral Therapy (Cohen, Mannarino, & Deblinger, 2016) ask children to create their trauma narrative based on their most upsetting or scary experience. However, care should be taken when asking a child to describe their most upsetting experience as this line of questioning could cause emotional distress to the child or clinician, require a report to be made to CFS agencies, or influence an ongoing investigation (Kuehnle & Connell, 2010).
Findings from the present study also highlight the importance of developing interventions and treatment plans that account for gender differences in risk for mental health problems. While maltreatment as a most upsetting experience has not been widely studied across genders, our findings are consistent with other studies showing gender differences in risk factors for psychopathology. For example, previous research has found gender differences in the psychological response to adversity (Eschenbeck et al., 2007) and in the developmental pathway that links child maltreatment to risk for internalizing and externalizing behavior problems (Maschi, Morgen, Bradley, & Hatcher, 2008). Thus, our findings suggest that both a child’s gender and most upsetting experience are critically important for clinicians and child advocates when determining risk for and treatment plans to prevent mental health problems following maltreatment experiences.
3.6.2 Program Evaluation Implications
Our findings have important implications for evaluating interventions and treatments that target depressive disorders in adolescent girls with a history of child maltreatment. Specifically, we suggest that evaluators test short- and long-term intervention and treatment effectiveness for depressive symptoms in girls according to their most upsetting experience. Given that girls reporting a maltreatment most upsetting experience reported increased depressive symptoms over time, the effectiveness of an intervention may not be apparent in girls until years following the maltreatment experience. While most upsetting experience was not associated with change in aggressive or rule breaking behavior over time, most upsetting experience may be a useful metric for evaluating baseline differences in boys and girls following assignment to an intervention, standard care, or no treatment group.
3.6.3 Policy Implications
Our study demonstrated that adolescents’ most upsetting experience was associated with risk for mental health problems. While many aspects of the maltreatment experience (e.g., relationship to the perpetrator) likely contribute to the traumatic nature of maltreatment and whether or not it is perceived as most upsetting, the aftermath of reporting maltreatment can also be traumatizing for youth. For example, the child’s experience with CFS agencies and the judicial process and familial support following a report have been shown to increase the traumatizing effects of child maltreatment (Goodman et al., 1992). Thus, while legislative efforts to prevent child maltreatment should continue to be supported, it is also crucial to support legislation that protects children during and after the initial report of child maltreatment.
One way legislators can reduce the traumatic aftereffects of maltreatment is through increased financial support of children’s advocacy centers (CAC). CAC’s are community-based centers that allow children to report child maltreatment to representatives from the criminal justice system, health care system, and other professionals involved in investigating maltreatment allegations and providing treatment (Boeskin, Edwards, Laird, & Lounsbury, 2016). The implementation of CAC’s and enacting laws to protect child witnesses has likely improved mental health outcomes for maltreated children (Smith, Witte, & Fricker-Elhai, 2006) by reducing the psychological harm associated with reporting maltreatment. Currently, the majority of funding for CAC’s comes from the government, primarily through the Victims of Child Abuse Act (VOCAA). However, public and private funds gained through VOCAA have not been able to keep up with the rapid development and utilization of CAC’s across the US (Boeskin et al., 2016). Given CAC’s reduce the traumatic nature of maltreatment which can contribute to children’s perception of maltreatment, it is imperative that VOCAA and other laws that provide support for CAC’s (e.g., Victims of Crime Act) continue to be reauthorized with annual increases in funding (for review, see Boeskin et al., 2016).
3.6.4 Limitations
The findings from the present study contribute to our understanding of how perception of maltreatment as the most upsetting experience is associated with internalizing and externalizing behavior problems in boys and girls, and how our findings can be used to inform clinical risk, program evaluation, and support for policies that prioritize children and their families. However, the findings and their implications should be considered within the context of the study’s limitations. First, perception of maltreatment was indirectly assessed by asking adolescents to describe their most upsetting experience and not by directly asking adolescents about their feelings toward maltreatment. Therefore, we were unable to ascertain whether adolescents reporting maltreatment as their most upsetting experience was a proxy for psychological adjustment to maltreatment (e.g., the ability to describe a maltreatment experience to a stranger) or willingness to voluntarily disclose maltreatment. We were also unable to establish whether adolescents reporting nonmaltreatment as their most upsetting experience was reflective of something comparatively more traumatic happening (e.g., death of a loved one) rather than poor psychological adjustment, or the refusal to voluntarily disclose maltreatment. Although we were unable to directly test these questions, the latter scenario (i.e., something more traumatic happening) is less methodologically problematic as it would have a suppressive effect on our findings.
Second, perception of maltreatment was assessed retrospectively under the assumption that adolescents’ most upsetting experience at T3 or T4 would be indicative of adolescents’ psychological adjustment or willingness to disclose to the interviewer at earlier time points, regardless of traumatic or disturbing experiences occurring from T1-T3. Perception of maltreatment was not assessed at earlier time points due to ethical and methodological concerns. The CTI assesses a wide variety of traumatic experiences (e.g., rape) and was not administered at T1 and T2 to prevent young adolescents from experiencing emotional distress. Although perception of maltreatment was assessed retrospectively, the elapsed time between the maltreatment and T3 is still less than the elapsed time between childhood and adulthood, when most studies of perception and disclosure take place.
Despite these limitations, this study has many strengths. The present study is valuable in that data were collected longitudinally from a high-risk population of maltreated youth, with high retention rates at each wave of measurement. Similarly, few studies are able to test developmental hypotheses about maltreated youth while considering differences between boys and girls. As such, the findings from the present study contribute to the literature on how perception of maltreatment as upsetting is associated with the development of mental health problems for adolescent boys and girls.
3.6.5 Conclusions and Future Directions
In summary, the findings from the present study have clinical, program evaluation, and policy implications. In the clinical setting, most upsetting experience can be used by clinicians and social workers to assess risk for internalizing and externalizing behavior problems in boys and girls, which are consistently associated with poor developmental outcomes across the lifespan (Fergusson & Woodward, 2002; Lewinsohn, Rohde, Seeley, Klein, & Gotlib, 2003; Whiteford et al., 2013). Most upsetting experience can be used as a metric to test for baseline differences in intervention groups and short- and long-term intervention effectiveness. Further, both child maltreatment and the events that follow can contribute to the traumatic nature of maltreatment (Goodman et al., 1992). Legislators can minimize the trauma associated with the aftermath of reporting maltreatment by supporting programs that provide resources to maltreated children and their families, such as CAC’s (Smith et al., 2006).
Future studies on perception of maltreatment and the development of internalizing and externalizing behavior problems should consider ethically and methodologically sound ways to measure perception of maltreatment during childhood and early adolescence when the maltreatment experience is more proximal. For example, researchers can consult with caseworkers, psychologists, and other licensed professionals on how to ask children about their thoughts and feelings toward their maltreatment experiences in a valid way without causing psychological distress. Future studies should also consider the role programs and services resulting from legislation and intervention by CFS agencies play in shaping children’s perceptions of maltreatment, and their association with internalizing and externalizing behavior problems from childhood into adulthood.
References
Achenbach, T., & Rescorla, L. (2001). Manual for the Achenbach system of empirically based assessment school-age forms profiles. Burlington, VT: Aseba.
Barnett, D., Manly, J. T., & Cicchetti, D. (1993). Defining child maltreatment: The interface between policy and research. In D. Chicchetti & S. L. Toth (Eds.), Child abuse, child development, and social policy (pp. 7–73). Norwood, NJ: Ablex.
Boals, A., & Schuettler, D. (2009). PTSD symptoms in response to traumatic and non-traumatic events: The role of respondent perception and A2 criterion. Journal of Anxiety Disorders, 23, 458–462. https://doi.org/10.1016/j.janxdis.2008.09.003
Boeskin, B., Edwards, D., Laird, W., & Lounsbury, K. (2016). Snapshot 2017: Advocacy, efficacy, and funding in CACs. Washington, DC: National Children's Alliance.
Bonanno, G. A., Noll, J. G., Putnam, F. W., O'Neill, M., & Trickett, P. K. (2003). Predicting the willingness to disclose childhood sexual abuse from measures of repressive coping and dissociative tendencies. Child Maltreatment, 8, 302–318. https://doi.org/10.1177/1077559503257066
Brougham, R. R., Zail, C. M., Mendoza, C. M., & Miller, J. R. (2009). Stress, sex differences, and coping strategies among college students. Current Psychology, 28, 85–97. https://doi.org/10.1007/s12144-009-9047-0
Cohen, J. A., Mannarino, A. P., & Deblinger, E. (2016). Treating trauma and traumatic grief in children and adolescents. New York, NY: The Guilford Press.
Crick, N. R., & Zahn–Waxler, C. (2003). The development of psychopathology in females and males: Current progress and future challenges. Development and Psychopathology, 15, 719–742. https://doi.org/10.1017/S095457940300035X
Eschenbeck, H., Kohlmann, C.-W., & Lohaus, A. (2007). Gender differences in coping strategies in children and adolescents. Journal of Individual Differences, 28, 18–26. https://doi.org/10.1027/1614-0001.28.1.18
Fergusson, D. M., & Woodward, L. J. (2002). Mental health, educational, and social role outcomes of adolescents with depression. Archives of General Psychiatry, 59, 225–231. https://doi.org/10.1001/archpsyc.59.3.225
Finkelhor, D., Turner, H. A., Shattuck, A., & Hamby, S. L. (2015). Prevalence of childhood exposure to violence, crime, and abuse: Results from the national survey of children’s exposure to violence. JAMA Pediatrics, 169, 746–754. https://doi.org/10.1001/jamapediatrics.2015.0676
Goodman, G. S., Taub, E. P., Jones, D. P., England, P., Port, L. K., Rudy, L., … Melton, G. B. (1992). Testifying in criminal court: Emotional effects on child sexual assault victims. Monographs of the Society for Research in Child Development, 57, i–159. https://doi.org/10.2307/1166127
Goodman-Brown, T. B., Edelstein, R. S., Goodman, G. S., Jones, D. P. H., & Gordon, D. S. (2003). Why children tell: A model of children’s disclosure of sexual abuse. Child Abuse & Neglect, 27, 525–540. https://doi.org/10.1016/S0145-2134(03)00037-1
Graham-Bermann, S. A., Kulkarni, M. R., & Kanukollu, S. (2011). Is disclosure therapeutic for children following exposure to traumatic violence? Journal of Interpersonal Violence, 26, 1056–1076. https://doi.org/10.1177/0886260510365855
Harrison, L., & Harrington, R. (2001). Adolescents' bereavement experiences. Prevalence, association with depressive symptoms, and use of services. Journal of Adolescence, 24, 159–169. https://doi.org/10.1006/jado.2001.0379
Horowitz, L. A. (1999). The relationship of childhood sexual abuse to revictimization: Mediating variables and developmental processes. Unpublished doctoral dissertation, The Catholic University of America, Washington, DC.
Klein, L. C., & Corwin, E. J. (2002). Seeing the unexpected: How sex differences in stress responses may provide a new perspective on the manifestation of psychiatric disorders. Current Psychiatry Reports, 4, 441–448. https://doi.org/10.1007/s11920-002-0072-z
Kovacs, M. (1981). Rating scales to assess depression in school-aged children. Acta Paedopsychiatrica: International Journal of Child & Adolescent Psychiatry, 46, 305–315.
Kovacs, M. (1992). Children's depression inventory manual. North Tonawanda, NY: Multi-Health Systems.
Kuehnle, K., & Connell, M. (2010). Child sexual abuse suspicions: Treatment considerations during investigation. Journal of Child Sexual Abuse, 19, 554–571. https://doi.org/10.1080/10538712.2010.512554
Leeb, R., Paulozzzi, L., Melanson, C., Simon, T., & Arias, I. (2008). Child maltreatment surveillance: Uniform definitions for public health and recommended data elements. Atlanta, GA: Centers for Disease Control and Prevention.
Lewinsohn, P. M., Rohde, P., Seeley, J. R., Klein, D. N., & Gotlib, I. H. (2003). Psychosocial functioning of young adults who have experienced and recovered from major depressive disorder during adolescence. Journal of Abnormal Psychology, 112, 353–363. https://doi.org/10.1037/0021-843X.112.3.353
Littleton, H., Horsley, S., John, S., & Nelson, D. V. (2007). Trauma coping strategies and psychological distress: A meta-analysis. Journal of Traumatic Stress, 20, 977–988. https://doi.org/10.1002/jts.20276
López, C. M., Andrews, A. R., III, Chisolm, A. M., de Arellano, M. A., Saunders, B., & Kilpatrick, D. (2017). Racial/ethnic differences in trauma exposure and mental health disorders in adolescents. Cultural Diversity and Ethnic Minority Psychology, 23, 382–387. https://doi.org/10.1037/cdp0000126
March, J. S., Parker, J. D. A., Sullivan, K., Stallings, P. M. A., & Conners, C. K. (1997). The multidimensional anxiety scale for children (MASC): Factor structure, reliability, and validity. Journal of the American Academy of Child & Adolescent Psychiatry, 36, 554–565. https://doi.org/10.1097/00004583-199704000-00019
Maschi, T., Morgen, K., Bradley, C., & Hatcher, S. S. (2008). Exploring gender differences on internalizing and externalizing behavior among maltreated youth: Implications for social work action. Child and Adolescent Social Work Journal, 25, 531–547. https://doi.org/10.1007/s10560-008-0139-8
Masten, A. S. (2001). Ordinary magic: Resilience processes in development. American Psychologist, 56, 227–238. https://doi.org/10.1037/0003-066X.56.3.227
McLaughlin, K. A., Sheridan, M. A., & Lambert, H. K. (2014). Childhood adversity and neural development: Deprivation and threat as distinct dimensions of early experience. Neuroscience & Biobehavioral Reviews, 47, 578–591. https://doi.org/10.1016/j.neubiorev.2014.10.012
Mennen, F. E., Kim, K., Sang, J., & Trickett, P. K. (2010). Child neglect: Definition and identification of youth's experiences in official reports of maltreatment. Child Abuse & Neglect, 34, 647–658. https://doi.org/10.1016/j.chiabu.2010.02.007
Moffitt, T. E. (1993). Adolescence-limited and life-course-persistent antisocial behavior: A developmental taxonomy. Psychological Review, 100, 674–701. https://doi.org/10.1037/0033-295X.100.4.674
Nagel, D. E., Putnam, F. W., Noll, J. G., & Trickett, P. K. (1997). Disclosure patterns of sexual abuse and psychological functioning at a 1-year follow-up. Child Abuse & Neglect, 21, 137–147. https://doi.org/10.1016/S0145-2134(96)00139-1
Negriff, S., Saxbe, D. E., & Trickett, P. K. (2015). Childhood maltreatment, pubertal development, HPA axis functioning, and psychosocial outcomes: An integrative biopsychosocial model. Developmental Psychobiology, 57, 984–993. https://doi.org/10.1002/dev.21340
Noll, J. G., Horowitz, L. A., Bonanno, G. A., Trickett, P. K., & Putnam, F. W. (2003). Revictimization and self-harm in females who experienced childhood sexual abuse: Results from a prospective study. Journal of Interpersonal Violence, 18, 1452–1471. https://doi.org/10.1177/0886260503258035
Petersen, A. C., Compas, B. E., Brooks-Gunn, J., Stemmler, M., Ey, S., & Grant, K. E. (1993). Depression in adolescence. American Psychologist, 48, 155–168. https://doi.org/10.1037/0003-066X.48.2.155
Prevoo, M. J. L., Stoltenborgh, M., Alink, L. R. A., Bakermans-Kranenburg, M. J., & van Ijzendoorn, M. H. (2017). Methodological moderators in prevalence studies on child maltreatment: Review of a series of meta-analyses. Child Abuse Review, 26, 141–157. https://doi.org/10.1002/car.2433
Schnider, K. R., Elhai, J. D., & Gray, M. J. (2007). Coping style use predicts posttraumatic stress and complicated grief symptom severity among college students reporting a traumatic loss. Journal of Counseling Psychology, 54, 344–350. https://doi.org/10.1037/0022-0167.54.3.344
Slyper, A. H. (2006). The pubertal timing controversy in the USA, and a review of possible causative factors for the advance in timing of onset of puberty. Clinical Endocrinology, 65, 1–8. https://doi.org/10.1111/j.1365-2265.2006.02539.x
Smith, D. W., Witte, T. H., & Fricker-Elhai, A. E. (2006). Service outcomes in physical and sexual abuse cases: A comparison of child advocacy center-based and standard services. Child Maltreatment, 11, 354–360. https://doi.org/10.1177/1077559506292277
Stroud, L. R., Salovey, P., & Epel, E. S. (2002). Sex differences in stress responses: Social rejection versus achievement stress. Biological Psychiatry, 52, 318–327. https://doi.org/10.1016/S0006-3223(02)01333-1
Taylor, S. E., Klein, L. C., Lewis, B. P., Gruenewald, T. L., Gurung, R. A. R., & Updegraff, J. A. (2000). Biobehavioral responses to stress in females: Tend-and-befriend, not fight-or-flight. Psychological Review, 107, 411–429. https://doi.org/10.1037/0033-295X.107.3.411
Trickett, P. K., & McBride-Chang, C. (1995). The developmental impact of different forms of child abuse and neglect. Developmental Review, 15, 311–337. https://doi.org/10.1006/drev.1995.1012
Trickett, P. K., Negriff, S., Ji, J., & Peckins, M. (2011). Child maltreatment and adolescent development. Journal of Research on Adolescence, 21, 3–20. https://doi.org/10.1111/j.1532-7795.2010.00711.x
U.S. Department of Health and Human Services, Administration for Children and Families, Administration on Children, Youth and Families, Children’s Bureau. (2013). Child maltreatment 2012. Available from http://www.acf.hhs.gov/programs/cb/research-data-technology/statistics-research/child-maltreatment.
Ullman, S. E. (2007). Relationship to perpetrator, disclosure, social reactions, and PTSD symptoms in child sexual abuse survivors. Journal of Child Sexual Abuse, 16, 19–36. https://doi.org/10.1300/J070v16n01_02
Whiteford, H. A., Degenhardt, L., Rehm, J., Baxter, A. J., Ferrari, A. J., Erskine, H. E., … Vos, T. (2013). Global burden of disease attributable to mental and substance use disorders: Findings from the global burden of disease study 2010. The Lancet, 382, 1575–1586. https://doi.org/10.1016/S0140-6376(13)61611-6
Wilson, A., & Ross, M. (2003). The identity function of autobiographical memory: Time is on our side. Memory, 11, 137–149. https://doi.org/10.1080/741938210
Acknowledgments
We thank Penelope K. Trickett for her mentorship during the preparation of this manuscript and for making this research possible. We also thank the children and their families who participated in this research. Support for this research was provided by the NICHD (R01 HD 039129) and NIDA (R01 Da24569-01A2). The first author was supported by a NICHD T32 Fellowship in Developmental Psychology, Department of Psychology, University of Michigan (2T32 HD007109-36). The third author was supported by DHHS NIH grants through the Prevention Research Center, The Pennsylvania State University (P50 DA039838 and T32 DA017629).
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2018 The Editor(s) and The Author(s), under exclusive license to Springer Nature Switzerland AG
About this chapter

Cite this chapter
Peckins, M.K., Negriff, S., Reader, J.M., Susman, E.J. (2018). Perception of Maltreatment: Gender-Specific Mental Health Outcomes Associated with Maltreatment as Most Upsetting Experience. In: Negriff, S. (eds) Child Maltreatment Research, Policy, and Practice. SpringerBriefs in Psychology(). Springer, Cham. https://doi.org/10.1007/978-3-030-04561-6_3
Download citation
DOI: https://doi.org/10.1007/978-3-030-04561-6_3
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-04560-9
Online ISBN: 978-3-030-04561-6
eBook Packages: Behavioral Science and PsychologyBehavioral Science and Psychology (R0)