
Abstract
Childhood maltreatment has long-term negative effects on individuals’ physical and mental well-being, and may increase the risk for suicidal ideation. However, how different patterns of childhood maltreatment affect subsequent suicidal ideation and the underlying mediating mechanisms remain unclear, particularly among Chinese adolescents. This study used latent profile analysis to identify patterns of childhood maltreatment among adolescents and explored how these patterns predicted subsequent suicidal ideation via depression, hope, and expressive suppression. This study used a two-wave, 1-year longitudinal design and included 2156 adolescents (Mage = 13.97 years, SDage = 1.61 years; 49.6% females). We identified three patterns of childhood maltreatment: low maltreatment, high psychological neglect, and high maltreatment. Compared with the low maltreatment group, the high maltreatment group indirectly predicted subsequent suicidal ideation 1 year later via depression through hope and expressive suppression, whereas the direct effect on suicidal ideation was not significant. Compared with the low maltreatment group, the high psychological neglect group had a significant direct effect on subsequent suicidal ideation and indirectly predicted suicidal ideation through depression or hope. Identifying patterns of childhood maltreatment among adolescents will assist mental health workers in developing targeted interventions to effectively alleviate suicidal ideation.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Childhood maltreatment includes physical abuse, emotional abuse, sexual abuse, physical neglect, and emotional neglect in childhood. It is prevalent in the Chinese general population [1] and is associated with a range of adverse mental health outcomes [2], particularly increased suicidal ideation [3]. Suicidal ideation, defined as thinking about, considering, or planning suicide [4], is an early stage in the development of suicidal behavior [5]. The interpersonal theory of suicide [6] suggests that childhood maltreatment is a risk factor that hinders the development of positive interpersonal interaction patterns. This can lead to difficulties in social functioning, resulting in low-quality interpersonal relationships [7], increased social isolation [8], and a thwarted sense of belonging. All these factors may result in more negative emotions and feelings of hopelessness and limit individuals’ emotional expression, thereby increasing the likelihood of suicidal ideation [6]. Most previous studies found that childhood maltreatment or specific maltreatment subtypes have enduring effects on suicidal ideation throughout the lifespan [9, 10]. However, these studies were generally conducted from a traditional variable-centered perspective, overlooking the fact that multiple subtypes of maltreatment may co-occur and be interconnected within an individual [11]. This raises important questions that previous studies were unable to resolve, such as what patterns of childhood maltreatment individuals exhibit, how these patterns influence suicidal ideation, and what the underlying psychological mechanisms might be.
Nevertheless, theories and findings from the variable-centered perspective may inspire further exploration of these above-mentioned questions, especially since some research has already accumulated evidence on how the relation between childhood maltreatment and suicidal ideation is influenced separately by depression, hope, or expressive suppression [12, 13]. Here, the cognitive models of depression [14] suggested that depression may be a potential mechanism. In light of this model, individuals exposed to abuse or neglect during childhood are prone to develop dysfunctional schemas about themselves [15]. They may also exhibit cognitive vulnerabilities and adopt a negative cognitive style to interpret negative events in life, thereby further increasing their susceptibility to depression [16]. Individuals with high levels of depressive symptoms tend to perceive themselves as worthless, unlovable, and incompetent [17]. Constant rumination also brings about negative self-perceptions and causes unbearable distress, ultimately increasing the risk for suicidal ideation [18, 19].
Theoretically, hope is another potential mechanism underlying the process of childhood maltreatment predicting suicidal ideation. Hope is defined as the perceived capability that derives pathways to desired goals and motivates oneself via agency thinking to use those pathways [20]. Hopeful individuals find effective strategies to achieve their goals, manage stress easily, and report low daily stress [20, 21]. However, the theory of hope [20] posits that individuals with childhood maltreatment may not have learned to adopt a hopeful perspective when encountering obstacles, resulting in the development of negative pathways and agency thinking, ultimately leading to a lack of hope. Furthermore, this can reduce individuals’ coping abilities [21], making them lack confidence in finding ways to overcome persistent challenges. This potentially causes extreme frustration and leads to giving up on life goals; such individuals may turn towards ending their lives [22].
In addition to depression and hope, expressive suppression was also a theoretical mechanism underlying the relation between childhood maltreatment and suicidal ideation. Expressive suppression, as a form of response modulation, refers to continuous efforts to restrain one’s behavior of expressing emotions [23]. Children who suffer from chronic maltreatment are often emotionally, socially, or economically dependent on their caregivers and may suppress their emotional expressions to avoid conflicts [24]. According to the process model of emotion regulation [23, 25], when these adverse experiences and negative emotions are suppressed for a long time, the inconsistency between the individual’s outward behavior and inner feelings leads to a lack of authenticity [26]. This may amplify feelings of life being meaningless and worthless [27] and ultimately increase the risk for suicidal ideation [28].
Depression, expressive suppression, and hope may mediate the relation between childhood maltreatment and suicidal ideation, but there are temporal relations among the three mediators. On the one hand, certain core depressive symptoms, such as anhedonia and sadness, mean that individuals become negative and passive in their daily lives. They may use suppression as a short-term functional strategy to temporarily reduce their experience of sadness, so the occurrence and persistence of depressive emotions may result in increased use of expressive suppression [29]. On the other hand, depressive symptoms contribute to individuals’ feelings of being trapped in their current stress and difficulties, perceiving a lack of control and an inability to solve problems [30]. Therefore, they may lack the motivation and willingness to seek pathways and strategies to achieve future goals [20], leading to reduced expectations for the future and subsequent decreased hope [31]. This gradually erodes individuals’ motivation for their future, leading them to become cautious and more likely to suppress their emotions [29].
Although extant studies assessed the relation between childhood maltreatment and suicidal ideation, several aspects remain poorly understood. First, most of the previous studies adopted a traditional variable-centered perspective and assumed that the effects of childhood maltreatment on suicidal ideation were uniformly distributed among participants. However, this perspective overlooked individual heterogeneity and neglected the cumulative effects of multiple subtypes of maltreatment that may coexist and interrelate within an individual [11]. To differentiate coexisting subtypes of childhood maltreatment, some researchers adopted latent profile analysis (LPA). This person-centered approach is used to group participants into discrete subgroups based on correlations among continuous variables [32]. In fact, more studies utilized latent class analysis [33, 34] to identify distinct classes of childhood trauma histories. Yet, this method requires a binary measure of childhood maltreatment, overlooks maltreatment severity, and results in information loss compared to LPA. Of note, previous studies often included sexual abuse as a childhood maltreatment subtype, which might directly interfere with the classification outcomes. Compared with other subtypes, the global incidence rate of sexual abuse is relatively low (1.6%) [11]. In addition, under the Chinese cultural context, victims may feel ashamed to disclose their sexual abuse experiences [35]. This makes sexual abuse challenging to detect and accurately measure, thereby biasing the questionnaire survey and classification results. Therefore, our study focused on non-sexual childhood maltreatment (i.e., emotional abuse, physical abuse, emotional neglect, and physical neglect) to explore the effect of these potential childhood maltreatment patterns on suicidal ideation.
Second, extant studies found that various subtypes of childhood maltreatment exposure had differing impact mechanisms on psychopathology, as they may impair different developmental and emotional processes [24, 36]. This suggested that different childhood maltreatment patterns may have various mechanisms in predicting suicidal ideation; however, these mechanisms remain poorly understood.
Third, based on previous theories and studies, depression, hope, and expressive suppression are potential mechanisms through which childhood maltreatment influences suicidal ideation. However, existing studies mainly explored their unique roles, but the combined mediating role of these factors in the relation of childhood maltreatment to suicidal ideation is not yet well understood. This limited the assessment of the mechanisms underlying the impact childhood maltreatment patterns has on suicidal ideation. Among these potentially mediators, depression is the most common risk factor for suicidal ideation [37, 38] and is also one of the main consequences of childhood maltreatment [39, 40]. Yet, the process through which childhood maltreatment experiences give rise to suicidal ideation after exhibiting depressive symptoms received less attention. Moreover, most previous studies used cross-sectional designs and lacked evidence from longitudinal studies, which restricts our understanding of the temporal relations.
To fill these forementioned gaps, this study uses a longitudinal design and LPA to identify the latent patterns of childhood maltreatment and to explore how these patterns influence suicidal ideation through the mediating roles of depression, hope, and expressive suppression. We considered adolescents as participants, because of their limited protective resources and that they are in a sensitive and vulnerable developmental period [41, 42]. With reference to previous theories and studies, we hypothesized that at least two distinct groups would be identified among Chinese adolescents: one characterized by low maltreatment and another by high maltreatment. Furthermore, we hypothesized that, in contrast to the reference pattern (i.e., low maltreatment pattern), alternative patterns of childhood maltreatment predict suicidal ideation both directly and indirectly via paths mediated by depression, hope, and expressive suppression (see Fig. 1).

Hypothesized model
Note: T1 = the first survey; T2 = 12 months after the first survey. Controlled for gender, age, location, single parent family, only child family, family income, time spent, hope, expressive suppression, and suicidal ideation at T1
Methods
Participants and procedures
We conducted a longitudinal survey with students from two junior and senior high schools in Zhejiang Province, China. The first assessment was conducted in November 2019 (Time [T] 1), and 2156 students participated. At the second assessment 1 year later (T2), 1777 (82.4%) of the original participants completed the survey. Because of attrition (e.g., dropout, graduation, or school transfer), it was challenging to obtain data from all original participants in this longitudinal survey. In order to make full use of all the data, all students (N = 2156) who participated in the first wave were included in the analyses. The final sample in this study is 2156 for T1 and 1777 for T2. Among these participants at T1, 1082 (50.2%) were male and 1070 (49.6%) were female, and 4 (2%) did not report their gender. The mean age at T1 was 13.97 (standard deviation [SD] = 1.61) years. The attrition analysis showed there were significant differences in age (t(573) = 4.71, p < 0.001), gender (χ2(1) = 22.69, p < 0.001), location (χ2(1) = 22.86, p < 0.001), only child family (χ2(1) = 6.90, p = 0.009), physical abuse (t(503) = − 2.52, p = 0.012), and physical neglect at T1 (t(530) = − 2.98, p = 0.003) between the two groups. There were no significant differences in single parent family (χ2(1) = 1.22, p = 0.269), family income (χ2(1) = 0.03, p = 0.858), time spent (χ2(1) = 0.22, p = 0.64), emotional abuse (t(509) = − 1.30, p = 0.195), emotional neglect (t(519) = − 1.71, p = 0.088), depression (t(499) = 0.34, p = 0.735), hope (t(498) = − 1.22, p = 0.221), expressive suppression (t(2108) = 1.26, p = 0.207), or suicidal ideation at T1 (t(2123) = − 0.38, p = 0.704).
This study was approved by the ethics committee at Hangzhou Normal University, local education authorities, and school principals. We adopted a cluster sampling method and randomly selected two junior and senior high schools. After obtaining permission from these schools to survey all students, we invited all students from these schools to participate in this study. All students and their guardians provided written consent. On the day the survey was conducted, all students on campus were willing to participate in this study and completed the study questionnaires. Trained psychology students supervised the survey process, explained the aim of this study, and emphasized that participation was voluntary. Participants were informed that they could leave the survey at any time. No compensation was provided, but counseling services were available as necessary.
Measures
Childhood maltreatment
At T1, we used the revised version of the Childhood Trauma Questionnaire (CTQ), developed by Zhou and Zhen [24] based on the original version by Bernstein et al. [43], to assess the childhood maltreatment experiences that occurred during the growing-up process before the age of 18 years. The questionnaire comprises 15 items on five 3-item subscales: physical neglect, emotional neglect, physical abuse, emotional abuse, and sexual abuse. Participants rated these items on a 5-point Likert scale from 0 (never) to 4 (always). Adolescents who scored ≥ 3 on at least one item in the CTQ subscales were considered to have experienced abuse or neglect [24]. Considering the low prevalence of sexual abuse and the difficulty in detection and measurement under Chinese culture as mentioned in the introduction section, we only assessed non-sexual forms of childhood maltreatment (i.e., emotional abuse, physical abuse, emotional neglect, and physical neglect). In this study, the physical abuse, emotional abuse, and emotional neglect subscales demonstrated good internal reliability (Cronbach’s α = 0.84, 0.75, and 0.80, respectively), but the physical neglect subscale showed low internal reliability (Cronbach’s α = 0.41).
Depression
To measure depressive symptoms in adolescents at T1, we used the Center for Epidemiologic Studies Depression Scale (CES-DS) developed by Fendrich et al. [44]. The CES-DS comprises 20 items that assess emotional, cognitive, and behavior-related symptoms of depression (e.g., “I felt down and unhappy this week”). Participants rated the frequency of each item within the last week on a 4-point Likert scale ranging from 0 (not at all) to 3 (a lot). Higher scores indicated a higher level of depressive symptoms. Consistent with previous recommendations [45], we used a cutoff score of 28 to identify the prevalence of depression among adolescents. In our study, the CES-DS demonstrated high reliability (Cronbach’s α = 0.91).
Hope
We used the Chinese version of the State Hope Scale [46] to measure hope at T1 and T2, which was originally developed by Snyder et al. [47]. The scale comprises 6 items (e.g., “I can think of many ways to reach my current goals”). In the present study, items were rated on an 8-point Likert scale (1 = definitely false, 8 = definitely true) and showed good internal consistency, with Cronbach’s α coefficients of 0.91 at T1 and 0.93 at T2.
Expressive suppression
The Emotion Regulation Questionnaire [48] was used to assess expressive suppression at T1 and T2. This questionnaire comprises two subscales: cognitive reappraisal and expressive suppression. The expressive suppression subscale contains 4 items (e.g., “I did not disclose my emotions”) which are rated on a 7-point Likert scale from 1 (completely disagree) to 7 (completely agree). The internal reliability of this subscale was good at both T1 (Cronbach’s α = 0.85) and T2 (Cronbach’s α = 0.89).
Suicidal ideation
The suicidal ideation subscale from the Child Behavior Problems Questionnaire developed by Zhou et al. [49] was used to assess suicidal ideation at T1 and T2. This subscale has 3 items: “having suicidal thoughts”, “preparing for suicide”, and “considering attempting suicide”. Responses were on a 5-point Likert scale from 0 (almost never) to 4 (almost always). Higher scores indicated more frequent suicidal ideation. This subscale showed good internal consistency (Cronbach’s α: 0.87 at T1 and 0.88 at T2).
Covariance
We used questionnaire items to measure participants’ demographic information, including their gender (0 = male, 1 = female), age at T1, location (0 = city, 1 = village), single parent family (0 = intact family, 1 = single parent family), only child family (0 = non-only child family, 1 = only child family), the average monthly family income (0 = 10,000 CNY and less, 1 = more than 10,000 CNY), and the average time that parents spend with their children every day (0 = less than four hours, 1 = four hours or more). Gender, age, location, single parent family, only child family, family income, and time spent at T1 were included as covariates in the analyses.
Statistical analysis
We used SPSS version 26.0 for the descriptive statistics and correlation analyses. The main analysis was conducted using three procedures. First, the sum scores of the four CTQ subscales (physical and emotional neglect, physical and emotional abuse) were used as indicators for performing LPA using Mplus version 8.3 [50]. A robust maximum likelihood estimate for LPA was used to identify different patterns of childhood maltreatment. The optimal number of latent classes was determined by evaluating and comparing 1- to 6-class profiles based on fit statistics, interpretability, and theoretical considerations. A good model fit was characterized by lower Bayesian information criterion (BIC), adjusted Bayesian information criterion (aBIC), and Akaike information criterion (AIC) values, as well as higher entropy. In addition, significant tests such as the Lo–Mendell–Rubin likelihood ratio test (LMR-LRT), Lo–Mendell–Rubin adjusted likelihood ratio test (ALMR-LRT), and bootstrap likelihood ratio test (BLRT) further contributed to indicating a good fit. Based on model fit indices, the optimal number of profiles was selected. Moreover, LPA was conducted independently for males and females as the sensitivity analysis, aiming to confirm the stability of profile membership.
Second, to validate the differentiation between the identified groups, analysis of variance (ANOVA) and Bonferroni post hoc comparisons were performed using SPSS version 26.0. The results the mean differences for childhood maltreatment subtypes across the groups. In addition, we investigated the differences in sociodemographic characteristics across the identified profiles. Chi-square tests were used to compare differences in gender, location, single parent family, only child family, family income, and time spent across maltreatment profiles. ANOVA was used to examine the differences in age at T1 across profiles.
Third, a direct effect model was established using Mplus version 8.3 [50] to examine the direct effects of T1 childhood maltreatment profiles on T2 suicidal ideation. Given that the independent variable, i.e., childhood maltreatment profiles, were categorical, they were coded as dummy variables, with the low maltreatment group serving as the reference group. Gender, age, location, single parent family, only child family, family income, and time spent at T1 were included as covariates. Then, we built a structural equation model to examine the mediating roles of T1 depression, T2 hope, and T2 expressive suppression in the relations between T1 childhood maltreatment profiles and T2 suicidal ideation. Furthermore, we performed the bootstrap percentile confidence method with a 95% confidence interval (CI; 5000 bootstraps) to assess the significance of the indirect effects. A significant indirect effect was indicated if the 95% CI did not include zero. Model fit was assessed using χ2, comparative fit index (CFI), Tucker–Lewis index (TLI), root mean square error of approximation (RMSEA), and standardized root mean square residual (SRMR) values. Cutoff values for good model fit were applied (i.e., CFI and TLI ≥ 0.90; SRMR and RMSEA < 0.08) [51]. Besides, we used full information maximum likelihood estimation (FIML) to deal with missing data and maximize information in mediation effect testing, which is a method known for producing less biased and more reliable results compared with traditional approaches [52].
Results
Preliminary analyses
In this study, we assessed the prevalence of childhood maltreatment and found that the prevalence rates of childhood emotional abuse, physical abuse, emotional neglect, and physical neglect in adolescents were 13.7% (n = 295), 13.6% (n = 293), 39.8% (n = 858), and 27.0% (n = 582), respectively. This study also revealed that 29.2% (n = 630) of adolescents reported depression above the cutoff point at T1. Table 1 shows the mean, SD, and correlation for all examined variables. Most of the main variables were significantly associated with each other, but emotional/physical neglect was not significantly related to T1 expressive suppression. In addition, T2 expressive suppression showed no significant associations with physical abuse, emotional neglect, physical neglect, and T2 hope. Demographic variables were significantly associated with most main variables, with some exceptions (see Table 1).
Latent profiles of childhood maltreatment
Table 2 presents the goodness-of-fit indices for six LPA model solutions. Comparisons of the models indicated that the LMR-LRT, ALMR-LRT, and BLRT values were significant in the 2-class, 3-class, and 5-class models. However, as one group in both the 4-class and 5-class models only accounted for 3.5% and 2.2% of the total sample, respectively, these solutions were deemed unacceptable. Although the entropy value of the 2-class solution was higher, significant LMR-LRT, ALMR-LRT, and BLRT demonstrated that the entropy value of the 3-class solution was superior. In addition, the 3-class model had smaller AIC, BIC, and aBIC values compared with the 1- and 2-class models. Therefore, we ultimately selected the 3-class model as the best model.
Discriminant analysis confirmed the accuracy of the LPA results with high prediction rates for the three categories (94.1%, 95.4%, and 93.0%, respectively). Table 3; Fig. 2 show the differences in childhood abuse (i.e., physical abuse and emotional abuse) and neglect (i.e., physical neglect and emotional neglect) among the three groups.

Three latent profiles of childhood maltreatment
The groups were named based on ANOVA results (see Table 3; Fig. 2): “low maltreatment” (n = 1482, 68.7%) with lower neglect/abuse scores, “high psychological neglect” (n = 475, 22.0%) with high emotional/physical neglect but low abuse scores, and “high maltreatment” (n = 199, 9.2%) with severe abuse/neglect experiences. The ANOVA results for childhood maltreatment showed that the high maltreatment group had the highest abuse levels, the high psychological neglect group had the highest emotional neglect, and both groups had equally high physical neglect, whereas the low maltreatment group scored lowest in all areas.
Furthermore, the high maltreatment group exhibited the most severe depression at T1 and suicidal ideation at T1 and T2, followed by the high psychological neglect group, whereas the low maltreatment group reported the lowest levels. Compared with other groups, the low maltreatment group had higher hope at T1 and T2, whereas the high maltreatment group had higher T1 expressive suppression. Detailed outcomes are presented in Table 3.
We examined the sociodemographic differences among three groups (see Table 3). The ANOVA results showed that participants in the low maltreatment group was older than the other two groups. Chi-square analysis indicated that there was a lower proportion of females in the high psychological neglect group, a higher proportion of rural residents in the low maltreatment group, and higher proportions of single parent family in the high maltreatment and high psychological neglect groups. Besides, the proportion of adolescents whose parents spend an average of four hours or more with them daily was higher in the low maltreatment group compared to the high maltreatment group. This suggested that there were sociodemographic differences across the three maltreatment profiles.
Mediators between childhood maltreatment profiles and suicidal ideation
Based on the mediation model hypothesis, we examined the association between childhood maltreatment profiles at T1 and suicidal ideation at T2, with T1 depression, T2 hope, and T2 expressive suppression as mediators. Covariates were gender, age, location, single parent family, only child family, family income, and time spent. Initially, we tested the direct effect model, which revealed that compared with the low maltreatment group, the high psychological neglect group exhibited a stronger effect on T2 suicidal ideation (β = 0.09, p = 0.002), whereas the high maltreatment group showed a non-significant direct effect on T2 suicidal ideation (β = 0.05, p = 0.254). Comparison of the high psychological neglect group (reference group) and the high maltreatment group in predicting T2 suicidal ideation showed no significant difference (β = −0.02, p = 0.643). These findings indicated that the high psychological neglect group (vs. the low maltreatment group) demonstrated a significant direct effect on T2 suicidal ideation, whereas the high maltreatment group (vs. other two groups) did not show a direct effect.
Subsequently, we constructed a multiple indirect effect model by incorporating T1 depression, T2 hope, and T2 expressive suppression into the direct effect model of T1 childhood maltreatment profiles predicting T2 suicidal ideation among adolescents. The model demonstrated good fit indices (χ2(1) = 106.49, CFI = 0.96, RMSEA = 0.22, SRMR = 0.02). Path analysis results were shown in Fig. 3 and Table S1 (see the supplementary materials). Compared with the low maltreatment group, the high psychological neglect group showed higher depression at T1, lower hope at T2, and increased suicidal ideation at T2; the high maltreatment group had higher levels of depression at T1. Furthermore, the high maltreatment group had a greater predictive effect on T1 depression (vs. the high psychological neglect group; refer to Fig. 4 and Table S2 in the supplementary materials). Moreover, T1 depression not only directly and positively predicted T2 suicidal ideation but also indirectly affected it by reducing T2 hope and increasing T2 expressive suppression.

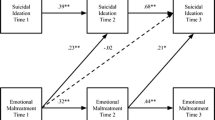
Mediation model (Low maltreatment group as the reference group)
Note: *p < 0.05, **p < 0.01, ***p < 0.001. Controlled for gender, age, location, single parent family, only child family, family income, time spent, hope, expressive suppression, and suicidal ideation at T1. Dotted lines represent non-significant paths; solid lines represent significant paths. Model shows standardized coefficients

Mediation model (High psychological neglect group as the reference group)
Note: *p < 0.05, **p < 0.01, ***p < 0.001. Controlled for gender, age, location, single parent family, only child family, family income, time spent, hope, expressive suppression, and suicidal ideation at T1. Dotted lines represent non-significant paths; solid lines represent significant paths. Model shows standardized coefficients
Furthermore, we used bootstrap percentile confidence interval to test the significance of the relative mediation effects. The results showed that total indirect effect from high psychological neglect group (vs. the low maltreatment group; Table S3 in the supplementary materials) on T2 suicidal ideation was significant. To be specific, this effect was mediated by T1 depression, T2 hope, and the pathway from T1 depression to T2 hope, as indicated by the 95% CIs of the indirect paths not including zero. Besides, the high maltreatment group predicted T2 suicidal ideation either directly through T1 depression, or indirectly through the pathway of T1 depression via T2 hope (vs. the other two groups; Tables S3 and S4 in the supplementary materials) and T2 expressive suppression (vs. the low maltreatment group). Overall, the findings of this study revealed that T1 depression, T2 hope, and T2 expressive suppression played mediating roles in the relations between childhood maltreatment profiles and suicidal ideation.
Sensitivity analysis
To examine the stability of profile membership, LPA was performed separately for males and females, replicating the same three-profile model (low maltreatment, high psychological neglect, high maltreatment) for both subgroups (see Tables S5–S6 and Figs. S1 and S2 in the supplementary materials). This confirmed the robustness of the profile solution.
Discussion
To our knowledge, this is the first longitudinal study to investigate the underlying mechanisms by which different patterns of childhood maltreatment contributed to suicidal ideation 1 year later. The results showed that childhood maltreatment could be classified into three patterns: low maltreatment (68.7%), high psychological neglect (22.0%), and high maltreatment (9.2%); this revealed the heterogeneity of childhood maltreatment in adolescents. Furthermore, we found that the high maltreatment group (vs. other groups) indirectly predicted subsequent suicidal ideation mainly through the mediating roles of depression, hope, and expressive suppression, whereas the high psychological neglect group (vs. the low maltreatment group) predicted subsequent suicidal ideation mainly through direct effect. These findings suggest that various patterns of childhood maltreatment have distinct mechanisms in predicting adolescents’ suicidal ideation; psychological neglect directly activates adolescents’ suicidal ideation, whereas high maltreatment elicits suicidal ideation through promoting dysfunctional psychological processes, such as aggravated depression, followed by reduced hope or increased expressive suppression.
Patterns of childhood maltreatment
We used LPA to identify three distinct patterns of childhood maltreatment in Chinese adolescents. First, most adolescents belonged to the low maltreatment group (68.7%), with minimal abuse or neglect experiences, which was consistent with similar findings and categorizations in previous studies [34, 53]. The second group was high psychological neglect (22.0%), which was characterized by highest emotional and physical neglect scores, indicating neglect was relatively common. This is not consistent with previous studies in western contexts [33] and one possible reason is cultural differences. For example, Western cultures emphasize individualism and agency and encourage the expression of thoughts and emotions [54]. In contrast, the Chinese culture values group harmony and social norms. Caregivers often engage in didactic conversations about behavioral expectations, rather than discussing emotions and thoughts directly with their children [55], leading to low perceived parental warmth. The third group was high maltreatment (9.2%), which had the lowest number of adolescents but the highest abuse accompanied by a high level of neglect. This could be because of the strong correlation (r = 0.71) between emotional and physical abuse in this study. These aspects are often seen together in abuse (e.g., scolding and corporal punishment) and is considered normal in Chinese parenting [24]. Overall, four maltreatment subtypes were investigated jointly and exhibited distinct patterns. The discussion on the ANOVA results regarding sociodemographic differences and T2 suicidal ideation among the identified maltreatment patterns is included in the supplementary materials.
Childhood maltreatment patterns and suicidal ideation
An interesting finding was that compared with the low maltreatment group, the high psychological neglect group showed a positive and direct effect on suicidal ideation one year later. Adolescents that report high psychological neglect may often experience being ignored and rejected by caregivers [39]. As a result, their basic relationship needs are not met, which exacerbates their insecurity [56, 57], leading to difficulties in social interactions [58], challenges in establishing connectedness with others, and resulting in a greater sense of thwarted belongingness, ultimately increasing suicidal ideation [6].
However, the high maltreatment group had a non-significant direct effect on suicidal ideation compared with the other two groups, partially supporting our hypothesis. This may be because adolescents in the high maltreatment group might view abusive behaviors as normal [59]. As mentioned in traditional Chinese sayings, “beating is care and scolding is love”, caregivers perceive these abusive behaviors as expressions of care and love [60], and these adolescents might internalize these views, which may not directly lead to the emergence of suicidal ideation. Another possible reason is that depression, hope, and expressive suppression may completely mediate the relation between the high maltreatment group (vs. the low maltreatment group) and suicidal ideation, resulting in its non-significant direct predictive effect.
Depression, hope, and expressive suppression as mediators
The results of the mediation effect showed that compared with the other two groups, the high maltreatment group primarily predicted subsequent suicidal ideation through the pathway of increased depression, which supported our hypothesis. This finding suggests that depression is a crucial mediator in this process. Of note, average scores for depressive symptoms were the highest in the high maltreatment group and were above the cutoff score of depression [45]. Adolescents in the high maltreatment group were exposed to an environment where various forms of abuse and neglect intertwined. Therefore, they may develop negative inferential styles and high levels of dysfunctional attitudes [16], leading to denial of self, others, and the world, and increasing the occurrence of depressive symptoms [42, 61]. This may further result in a loss of interest and confidence in lives, thereby increasing suicidal ideation [62].
Moreover, we found that the high maltreatment group (vs. other groups) aggravated depression, which reduced subsequent hope and increased the use of expressive suppression strategies, and indirectly exacerbated suicidal ideation one year later. This finding partially supported our hypothesis and was consistent with the theory of hope [20] and the process model of emotion regulation [23, 25]. On the one hand, compared to the other two groups, depressed adolescents in the high maltreatment group may dwell on past experiences [63], overlooking positive possibilities and opportunities, resulting in lower levels of hope after a year. Adolescents without hope may remain immersed in overwhelming psychological pain and myriad negative experiences [64], and perceive suicide as the only way to escape the pain [65], as well as the source of motivation and ultimate goal [20], thereby stimulating the emergence of suicidal ideation. On the other hand, depressed adolescents in the high maltreatment group (vs. the low maltreatment group) may feel exhausted and lack energy during long-term learning and social interactions [66]. To conserve their energy, they may frequently suppress negative emotional expression as a coping mechanism. This use of expressive suppression restricts their access to new relationships and impedes the maintenance of existing relationships, potentially impacting adolescents’ social functioning [67], and exacerbating subsequent suicidal ideation [68, 69].
Furthermore, our mediation analysis revealed that the high psychological neglect group, compared to the low maltreatment group, indirectly exacerbated suicidal ideation by increasing depression and reducing hope, as well as through the pathway of depression via hope, suggesting that depression and hope could act as mediators. This finding partially supported our hypothesis, validated cognitive models of depression [14] and the theory of hope [20], which was consistent with previous studies [70]. Specifically, repeated experiences of psychological neglect can result in negative cognitive schemas about the self (e.g., “I am worthless”), others (e.g., “Nobody cares about me”), and the future (e.g., “Things will get worse”) [14], which increases depressive symptoms [71] and reduces subsequent hope. Moreover, adolescents with higher levels of depression are more likely to become socially withdrawn and increase the feeling of despair, helplessness, and loneliness [72], which in turn results in a pessimistic attitude towards future relationships. Adolescents with low hope often perceive their incapability and insufficient contribution to the society, and gives rise to a long-term feeling of being a burden to others [73, 74], ultimately increasing the risk for suicidal ideation [6, 75].
Limitations and implications
This study has several limitations that further research should address. First, this study used cluster sampling and relied on adolescent self-report, which might increase sampling errors and introduce subjective reporting biases. Future studies could collect data from multiple sources for a more objective assessment. Second, this study focused on suicidal ideation because of its prevalence in suicide research. However, suicide behavior has serious implications for individuals, families, and society, which should be explored in further studies. Third, this study was conducted in Chinese cultural context, and these findings may have certain cultural characteristics, so caution is needed when applying the findings in other contexts. Further studies should examine the generalizability of the findings across different cultural backgrounds.
Despite these limitations, this study has important theoretical and clinical implications. Regarding its theoretical contribution, this study revealed that depression, hope, and expressive suppression mediated the relations between childhood maltreatment patterns and suicidal ideation. Importantly, the mechanisms by which different childhood maltreatment patterns predicted suicidal ideation varied. The high psychological neglect group (vs. the low maltreatment group) had positive effects on suicidal ideation one year later, either directly or indirectly through early depression and subsequent diminished hope. Surprisingly, compared with other groups, the high maltreatment group did not directly predict suicidal ideation but indirectly affected this factor via depression or through a path from depression to hope or expressive suppression, indicating that depression played a key role in this process. In addition, from the perspective of dysfunctional psychological processes, this study integrated cognitive models of depression [14], the theory of hope [20], and the process model of emotion regulation [23, 25], expanding the understanding of the relation between childhood maltreatment and suicidal ideation.
As for clinical implications, these findings highlight the need for tailored and evidence-based psychological interventions among adolescents with different childhood maltreatment patterns. It is suggested that mental health workers should focus on identifying maltreatment patterns to offer targeted interventions, with particular attention to high maltreatment and psychological neglect groups. The negative impact of psychological neglect, especially its direct effects on suicidal ideation, depression, and hope, needs to be recognized and prioritized by mental health workers. To prevent and reduce the occurrence of suicidal ideation in adolescents with a high maltreatment pattern, it is crucial to promptly screen, identify, and assess their depressive symptoms, and implement appropriate interventions. Besides, it is essential to encourage adolescents to express their emotions and thoughts, learn adaptive emotion regulation strategies, set achievable goals, and find effective pathways to enhance their hope.
Data availability
The data and analysis code that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions collection for this study.
References
Fang X, Fry DA, Ji K et al (2015) The burden of child maltreatment in China: a systematic review. Bull World Health Organ 93:176–185. https://doi.org/10.2471/BLT.14.140970.
Jaffee SR (2017) Child maltreatment and risk for psychopathology in childhood and adulthood. Annu Rev Clin Psychol 13:525–551. https://doi.org/10.1146/annurev-clinpsy-032816-045005
Lippard ETC, Nemeroff CB (2020) The devastating clinical consequences of child abuse and neglect: increased disease vulnerability and poor treatment response in mood disorders. Am J Psychiatry 177:20–36. https://doi.org/10.1176/appi.ajp.2019.19010020
National Institute of Mental Health (2021) Suicide. https://www.nimh.nih.gov/health/statistics/suicide. Accessed 19 Feb 2024
Nock MK, Green JG, Hwang I et al (2013) Prevalence, correlates, and treatment of lifetime suicidal behavior among adolescents: results from the national comorbidity survey replication adolescent supplement. JAMA Psychiatry 70:300–310. https://doi.org/10.1001/2013.jamapsychiatry.55
Van Orden KA, Witte TK, Cukrowicz KC et al (2010) The interpersonal theory of suicide. Psychol Rev 117:575–600. https://doi.org/10.1037/a0018697
Miller AB, Adams LM, Esposito-Smythers C et al (2014) Parents and friendships: a longitudinal examination of interpersonal mediators of the relationship between child maltreatment and suicidal ideation. Psychiatry Res 220:998–1006. https://doi.org/10.1016/j.psychres.2014.10.009
McCrory E, Foulkes L, Viding E (2022) Social thinning and stress generation after childhood maltreatment: a neurocognitive social transactional model of psychiatric vulnerability. Lancet Psychiatry 9:828–837. https://doi.org/10.1016/S2215-0366(22)00202-4
Angelakis I, Gillespie EL, Panagioti M (2019) Childhood maltreatment and adult suicidality: a comprehensive systematic review with meta-analysis. Psychol Med 49:1057–1078. https://doi.org/10.1017/S0033291718003823
Miller AB, Esposito-Smythers C, Weismoore JT, Renshaw KD (2013) The relation between child maltreatment and adolescent suicidal behavior: a systematic review and critical examination of the literature. Clin Child Fam Psychol Rev 16:146–172. https://doi.org/10.1007/s10567-013-0131-5
Vachon DD, Krueger RF, Rogosch FA, Cicchetti D (2015) Assessment of the harmful psychiatric and behavioral effects of different forms of child maltreatment. JAMA Psychiatry 72:1135–1142. https://doi.org/10.1001/jamapsychiatry.2015.1792
Kwok SYCL, Gu M (2019) Childhood neglect and adolescent suicidal ideation: a moderated mediation model of hope and depression. Prev Sci 20:632–642. https://doi.org/10.1007/s11121-018-0962-x
Valencia PD, de la Rosa-Gómez A (2024) Emotion regulation mediates the association between child abuse and adult suicidal ideation: an exploratory study. Rev Colomb Psiquiatr. https://doi.org/10.1016/j.rcp.2024.01.003
Beck AT (1987) Cognitive models of depression. J Cogn Psychother 1:5–37
Lumley MN, Harkness KL (2007) Specificity in the relations among childhood adversity, early maladaptive schemas, and symptom profiles in adolescent depression. Cognit Ther Res 31:639–657. https://doi.org/10.1007/s10608-006-9100-3
Gibb BE (2002) Childhood maltreatment and negative cognitive styles: a quantitative and qualitative review. Clin Psychol Rev 22:223–246. https://doi.org/10.1016/S0272-7358(01)00088-5
Beck AT (1967) Depression: clinical, experimental, and theoretical aspects. Harper and Row, New York
Hawton K, Saunders KEA, O’Connor RC (2012) Self-harm and suicide in adolescents. Lancet 379:2373–2382. https://doi.org/10.1016/s0140-6736(12)60322-5
Vidal-Arenas V, Bravo AJ, Ortet-Walker J et al (2022) Neuroticism, rumination, depression and suicidal ideation: a moderated serial mediation model across four countries. Int J Clin Health Psychol 22:100325. https://doi.org/10.1016/j.ijchp.2022.100325
Snyder CR (2002) Hope theory: rainbows in the mind. Psychol Inq 13:249–275. https://doi.org/10.1207/S15327965PLI1304_01
Ong AD, Edwards LM, Bergeman CS (2006) Hope as a source of resilience in later adulthood. Pers Individ Dif 41:1263–1273. https://doi.org/10.1016/j.paid.2006.03.028
Snyder CR (1994) The psychology of hope: you can get there from here. Free Press, New York
Gross JJ (2015) Emotion regulation: current status and future prospects. Psychol Inq 26:1–26. https://doi.org/10.1080/1047840X.2014.940781
Zhou X, Zhen R (2022) How do physical and emotional abuse affect depression and problematic behaviors in adolescents? The roles of emotional regulation and anger. Child Abuse Negl 129:105641. https://doi.org/10.1016/j.chiabu.2022.105641
Gross JJ (1998) The emerging field of emotion regulation: an integrative review. Rev Gen Psychol 2:271–299. https://doi.org/10.1037/1089-2680.2.3.271
Gross JJ, John OP (2003) Individual differences in two emotion regulation processes: implications for affect, relationships, and well-being. J Pers Soc Psychol 85:348–362. https://doi.org/10.1037/0022-3514.85.2.348
Allan BA, Bott EM, Suh H (2015) Connecting mindfulness and meaning in life: exploring the role of authenticity. Mindfulness 6:996–1003. https://doi.org/10.1007/s12671-014-0341-z
Marco JH, Pérez S, García-Alandete J (2016) Meaning in life buffers the association between risk factors for suicide and hopelessness in participants with mental disorders. J Clin Psychol 72:689–700. https://doi.org/10.1002/jclp.22285
Larsen JK, Vermulst AA, Geenen R et al (2012) Emotion regulation in adolescence: a prospective study of expressive suppression and depressive symptoms. J Early Adolesc 33:184–200. https://doi.org/10.1177/0272431611432712
Wenzel A, Beck AT (2008) A cognitive model of suicidal behavior: theory and treatment. Appl Prev Psychol 12:189–201. https://doi.org/10.1016/j.appsy.2008.05.001
Li Z, Wang Y, Mao X, Yin X (2018) Relationship between hope and depression in college students: a cross-lagged regression analysis. Personal Ment Health 12:170–176. https://doi.org/10.1002/pmh.1412
Lubke G, Muthén BO (2007) Performance of factor mixture models as a function of model size, covariate effects, and class-specific parameters. Struct Equ Model 14:26–47. https://doi.org/10.1207/s15328007sem1401_2
Keane C, Magee C, Kelly P (2016) Is there complex trauma experience typology for australians experiencing extreme social disadvantage and low housing stability? Child Abuse Negl 61:43–54. https://doi.org/10.1016/j.chiabu.2016.10.001
Warmingham JM, Handley ED, Rogosch FA et al (2019) Identifying maltreatment subgroups with patterns of maltreatment subtype and chronicity: a latent class analysis approach. Child Abuse Negl 87:28–39. https://doi.org/10.1016/j.chiabu.2018.08.013
Ji K, Finkelhor D, Dunne M (2013) Child sexual abuse in China: a meta-analysis of 27 studies. Child Abuse Negl 37:613–622. https://doi.org/10.1016/j.chiabu.2013.03.008
Egeland B, Sroufe LA, Erickson M (1983) The developmental consequence of different patterns of maltreatment. Child Abuse Negl 7:459–469. https://doi.org/10.1016/0145-2134(83)90053-4
El-Hourani M, Zadra A, Castellanos-Ryan N et al (2022) Longitudinal associations throughout adolescence: suicidal ideation, disturbing dreams, and internalizing symptoms. Sleep Med 98:89–97. https://doi.org/10.1016/j.sleep.2022.06.012
Ribeiro JD, Huang X, Fox KR, Franklin JC (2018) Depression and hopelessness as risk factors for suicide ideation, attempts and death: meta-analysis of longitudinal studies. Br J Psychiatry 212:279–286. https://doi.org/10.1192/bjp.2018.27
Brassard MR, Hart SN, Baker AAL, Chiel Z (2019) The APSAC monograph on psychological maltreatment (PM). The American Professional Society on the Abuse of Children (APSAC). https://www.apsac.org. Accessed 26 Dec 2022
Nelson J, Klumparendt A, Doebler P, Ehring T (2017) Childhood maltreatment and characteristics of adult depression: meta-analysis. Br J Psychiatry 210:96–104. https://doi.org/10.1192/bjp.bp.115.180752
Brown J, Cohen P, Johnson JG, Smailes EM (1999) Childhood abuse and neglect: specificity of effects on adolescent and young adult depression and suicidality. J Am Acad Child Adolesc Psychiatry 38:1490–1496. https://doi.org/10.1097/00004583-199912000-00009
Infurna MR, Reichl C, Parzer P et al (2016) Associations between depression and specific childhood experiences of abuse and neglect: a meta-analysis. J Affect Disord 190:47–55. https://doi.org/10.1016/j.jad.2015.09.006
Bernstein DP, Ahluvalia T, Pogge D, Handelsman L (1997) Validity of the childhood trauma questionnaire in an adolescent psychiatric population. J Am Acad Child Adolesc Psychiatry 36:340–348. https://doi.org/10.1097/00004583-199703000-00012
Fendrich M, Weissman MM, Warner V (1990) Screening for depressive disorder in children and adolescents: validating the center for epidemiologic studies depression scale for children. Am J Epidemiol 131:538–551. https://doi.org/10.1093/oxfordjournals.aje.a115529
Radloff LS (1991) The use of the center for epidemiologic studies depression scale in adolescents and young adults. J Youth Adolesc 20:149–166. https://doi.org/10.1007/BF01537606
Zhou X, Wu X, Wang W, Tian Y (2017) The relationship between social support and posttraumatic growth: the mediated role of state hope and positive reappraisal. Psychol Dev Educ 33:587–594
Snyder CR, Sympson SC, Ybasco FC et al (1996) Development and validation of the state hope scale. J Pers Soc Psychol 70:321–335. https://doi.org/10.1037//0022-3514.70.2.321
Wang L, Liu H, Li Z, Du W (2007) Reliability and validity of emotion regulation questionnaire Chinese revised version. China J Health Psychol 15:503–505
Zhou X, Wu X, An Y, Fu F (2014) Longitudinal relationships between posttraumatic stress symptoms and sleep problems in adolescent survivors following the Wenchuan earthquake in China. PLoS ONE 9:e104470. https://doi.org/10.1371/journal.pone.0104470
Muthén LK, Muthén BO (1998–2017) Mplus user’s guide. Muthén & Muthén, Los Angeles
Wen Z, Hau K, Herbert WM (2004) Structural equation model testing: cutoff criteria for goodness of fit indices and Chi-square test. Acta Psychol Sinica 36:186–194
Widaman KF (2006) Missing data: what to do with or without them. Monogr Soc Res Child Dev 71:42–64
Liu S, Ahemaitijiang N, Xu J et al (2023) Patterns of childhood maltreatment influence sleep quality: the role of emotion regulation. Dev Psychopathol 1–11. https://doi.org/10.1017/S0954579423000597
Doan SN, Wang Q (2010) Maternal discussions of mental states and behaviors: relations to emotion situation knowledge in European American and immigrant Chinese children. Child Dev 81:1490–1503. https://doi.org/10.1111/j.1467-8624.2010.01487.x
Luo R, Tamis-LeMonda CS, Song L (2013) Chinese parents’ goals and practices in early childhood. Early Child Res Q 28:843–857. https://doi.org/10.1016/j.ecresq.2013.08.001
Bowlby J (1969) Attachment and loss: vol. 1. Attachment. Basic Books, New York
Bowlby J (1973) Attachment and loss: vol. 2. Separation: anxiety and anger. Basic Books, New York
Kobulsky JM, Dubowitz H (2022) The nature of neglect and its consequences. In: Geffner R, White JW, Hamberger LK et al (eds) Handbook of interpersonal violence and abuse across the lifespan. Springer, Cham, pp 678–694
Qiao DP, Chan YC (2005) Child abuse in China: a yet-to-be-acknowledged ‘social problem’ in the Chinese mainland. Child Fam Soc Work 10:21–27. https://doi.org/10.1111/j.1365-2206.2005.00347.x
Yang C, Liu X, Yang Y et al (2020) Violent disciplinary behaviors towards left-behind children in 20 counties of rural China. Child Youth Serv Rev 114:105016. https://doi.org/10.1016/j.childyouth.2020.105016
Li M, Gao T, Su Y et al (2022) The timing effect of childhood maltreatment in depression: a systematic review and meta-analysis. Trauma Violence Abuse 24:2560–2580. https://doi.org/10.1177/15248380221102558
Batterham PJ, Christensen H, Calear AL (2013) Anxiety symptoms as precursors of major depression and suicidal ideation. Depress Anxiety 30:908–916. https://doi.org/10.1002/da.22066
Habermas T, Ott L-M, Schubert M et al (2008) Stuck in the past: negative bias, explanatory style, temporal order, and evaluative perspectives in life narratives of clinically depressed individuals. Depress Anxiety 25:E121–E132. https://doi.org/10.1002/da.20389
Klonsky ED, May A (2015) The three-step theory (3ST): a new theory of suicide rooted in the ideation-to-action framework. Int J Cogn Ther 8:114–129. https://doi.org/10.1521/ijct.2015.8.2.114
An J, Sun Q, Guo L et al (2012) Suicide ideation and its relationship with depression and hope trait in college freshmen. Chin Ment Health J 26:616–619
Porr C, Olson K, Hegadoren K (2010) Tiredness, fatigue, and exhaustion in the context of a major depressive disorder. Qual Health Res 20:1315–1326. https://doi.org/10.1177/1049732310370841
Butler EA, Egloff B, Wilhelm FH et al (2003) The social consequences of expressive suppression. Emotion 3:48–67. https://doi.org/10.1037/1528-3542.3.1.48
Forkmann T, Scherer A, Böcker M et al (2014) The relation of cognitive reappraisal and expressive suppression to suicidal ideation and suicidal desire. Suicide Life Threat Behav 44:524–536. https://doi.org/10.1111/sltb.12076
Ortiz S, Knauft K, Smith A, Kalia V (2019) Expressive suppression mediates the relation between disordered eating and suicidal ideation. J Clin Psychol 75:1943–1958. https://doi.org/10.1002/jclp.22830
Sekowski M, Gambin M, Cudo A et al (2020) The relations between childhood maltreatment, shame, guilt, depression and suicidal ideation in inpatient adolescents. J Affect Disord 276:667–677. https://doi.org/10.1016/j.jad.2020.07.056
Spruit A, Goos L, Weenink N et al (2020) The relation between attachment and depression in children and adolescents: a multilevel meta-analysis. Clin Child Fam Psychol Rev 23:54–69. https://doi.org/10.1007/s10567-019-00299-9
Huang J, Zhang M, Cai Y et al (2024) Association between social withdrawal and suicidal ideation in patients with major depressive disorder: the mediational role of emotional symptoms. J Affect Disord 347:69–76. https://doi.org/10.1016/j.jad.2023.11.051
Davidson CL, Wingate LR, Rasmussen KA, Slish ML (2009) Hope as a predictor of interpersonal suicide risk. Suicide Life Threat Behav 39:499–507. https://doi.org/10.1521/suli.2009.39.5.499
Joiner TE Jr, Brown JS, Wingate LR (2005) The psychology and neurobiology of suicidal behavior. Annu Rev Psychol 56:287–314. https://doi.org/10.1146/annurev.psych.56.091103.070320
Tucker RP, Wingate LR, O’Keefe VM et al (2013) Rumination and suicidal ideation: the moderating roles of hope and optimism. Pers Individ Dif 55:606–611. https://doi.org/10.1016/j.paid.2013.05.013
Funding
This study was supported by the Research Project of Shanghai Science and Technology Commission (20dz2260300).
Author information
Authors and Affiliations
Contributions
YY and XZ developed the study concept and design. YY, BC, RZ and XZ carried out testing and data collection. YY, BC, YL and ZL performed the data analysis and completed the manuscript with supervision from XZ and RZ. All authors approved the final version of the paper for submission.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Ye, Y., Chen, B., Zhen, R. et al. Childhood maltreatment patterns and suicidal ideation: mediating roles of depression, hope, and expressive suppression. Eur Child Adolesc Psychiatry (2024). https://doi.org/10.1007/s00787-024-02442-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s00787-024-02442-6