
Keypoints
-
1.
Children experience tinnitus and might present similar suffering as observed in adults but they rarely mention the symptom unless directly asked about it.
-
2.
Difficulty on concentration, sleeping, hearing, leisure activities, sports practice, and hyperacusis are the most frequent complaints associated to tinnitus in children.
-
3.
Only a few population studies have been performed and have disclosed prevalence rates from 6% to 59%. Many factors might be implicated in the large inter-study variability of tinnitus prevalence in children.
-
4.
Age, gender, hearing loss, motion sickness, hyperacusis, and noise exposure have been suggested as risk factors to development of tinnitus in children.
-
5.
A proper model to investigate children should be developed for the purpose of obtaining accurate information about the prevalence of tinnitus in children.
-
6.
Preventive measures should aim at hearing education about the risk of hearing loss and tinnitus. Prevention of noise exposure should be promoted as early as possible.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others
Keywords
Introduction
Children rarely mention tinnitus unless they are asked specifically about it. The frequency with which they mention the symptom spontaneously ranges from 1.6% to 6.5% [1–4]. Therefore, the observed proportion of children who seek professional help does not represent all children with tinnitus. Also, investigating tinnitus is seldom a part of routine pediatric otolaryngological practice. For these reasons, the prevalence of the symptom is generally underestimated in childhood [5].
Children who experience tinnitus may suffer in a similar way as adults with tinnitus. Difficulty in concentration, sleeping, hearing, and hyperacusis are the most frequent complaints associated with tinnitus in children [1, 6–8]. The symptoms might affect many kinds of leisure activities such as sports [1] as well as cause a decrease in school performance [9, 10]. The symptoms may significantly interfere with children’s life in general, which will inevitably affect their entire families as well [11].
Terms such as “ringing” [2, 12], “beeping” or “buzzing,” and a “high-pitched noise” or “whistling” [6] have been used by children to describe tinnitus sounds.
Some hypotheses have been presented regarding why children rarely report tinnitus spontaneously. (1) Children rarely refer to symptoms that are not associated with pain [13]; (2) children have a less-developed body image [14]; (3) there are specific differences in the ascending auditory pathways in children [15]; (4) children may perceive tinnitus as a familiar experience [16]; (5) children may be more easily distracted by events of the external environments [17]; (6) do not perceive the medical significance of the symptom [18]; and (7) children’s attention process is different from that in adults, and this might also have an effect on how they perceive tinnitus.
In order to diagnose tinnitus in children, it is therefore important to ask children specifically if they have tinnitus.
Studying Tinnitus in Children
When studying tinnitus in childhood, it must be kept in mind that a child is not a miniature version of the adult. Children obviously do not possess adult brains. The organs of perception linking the child to the external world are still under maturation. The organization of sensory systems in the brain [15] (see also Chap. 8) and perception and attention in a child are different from adult, promoting a different perception and attitude to the world.
Other obstacles in studies of tinnitus in children are related to the fact that children tend to give positive answers to please the interviewer [19] and it is important to minimize and parents preoccupations that children’s their might have after being aware of tinnitus.
In managing tinnitus in children, it is important to distinguish between the perception of the tinnitus and the impact that the tinnitus has on a person (tinnitus suffering) [5]. Lack of information about the prevalence of tinnitus suffering in children makes it difficult to judge the impact of tinnitus on children.
Epidemiological Studies
Although the existence of tinnitus in childhood has been reported since the 1970s there is still great uncertainty regarding the prevalence of tinnitus in children.
Population Studies
The few population studies that have been published were done in only a few countries and have shown widely different values of prevalence (from 6% to 59%) (Table 6.1).
Many different factors may have contributed to the discrepancies between the results of the different studies that have been published: (1) the criteria used for defining tinnitus may have been different; (2) hearing criteria may have been different; (3) age range may have been different; (4) methodological factors – interview or questionnaires most likely were different; (5) studies have used different statistical procedures, with different sample sizes; (6) the effect of confounding variables may also have contributed to the variations, for example, social and economic classes, ethnic, and cultural background may have varied; (7) different behavioral factors may have influenced the results such as emotional problems; (8) the effect of environmental factors such as exposure to noise may have been different.
Two studies of the prevalence of tinnitus in children had many participants recruited from otolaryngological clinics. Aust [20] screened children who sought help for otological complaints and Savastano [4] evaluated a general population of children using a specific protocol to investigate tinnitus (Table 6.2). They found tinnitus in 7% and 34%, respectively.
Factors that may Promote Tinnitus (Risk Factors)
Risk factors refer to an increase in the chance that an event is going to occur; in the present situation, this means the likelihood that a child will get tinnitus. Identification of risk factors plays an important role toward understand the etiology of tinnitus. Identification of risk factors might help understanding the symptoms and develop strategies for prevention of tinnitus (see Chap. 69). They can be identified by logistic regression models where the risk odds is determined while controlling for irrelevant factors. The OR (OR) is the likelihood that an event will occur; in our case, the likelihood of occurrence of tinnitus versus the chance of absence of tinnitus. The OR for a predictor tells the relative amount by which the odds of the outcome increases (OR > 1.0) or decreases (OR < 1.0). Decrease in OR is a sign that a protective factor against the occurrence of an event is present.
To our knowledge, only two studies on tinnitus prevalence in children have so far used such statistical analysis.
The following risk factors have been identified on tinnitus in children.
Age
The risk for tinnitus sensation and tinnitus annoyance increases with age by 1.1 times, for every year among children in the Brazilian study [1] and by a factor of 1.2 according to Nodar [12]. Aksoy et al. [8] reported a progressive increase on tinnitus incidence around the age of 13–14 years from 10 to 18 years and 6 to 16 years have observed.
Gender
Holgers and Svedlund [21] found a higher prevalence of tinnitus among girls, as well as a higher prevalence of depressive and anxiety symptoms. Coelho et al. [1] found that boys had an OR of 0.
To present, tinnitus suffering when compared to girls means that the male gender was a protective factor for the development of tinnitus among children. These findings could be related to: (1) girls present a higher tendency to express symptoms than boys, including those related to affective disorders [22]; (2) spontaneous otoacoustic emissions are more frequent among females [23] and have been described as a possible tinnitus etiology[24]; (3) genetic differences among genders associated with neurotransmitter expressions pursuing an action on auditory pathway, including serotonin [25] and female reproductive hormones affect GABA receptors in the brain [26] (see Chap. 10).
Hearing Loss
Tinnitus is more frequent in children with normal hearing [12, 19] than in hearing impaired children, but children with profound hearing loss have lower prevalence of tinnitus than children with moderate loss [27]. Comparison of children with middle ear disease to those with sensorineural hearing loss showed that 43.9% of children with middle ear disease had tinnitus while 29.5% with sensorineural hearing loss had tinnitus [16].
Children with hearing loss had an OR of 3.3 regarding tinnitus that could not be related to sound exposure according to a Swedish study from Holgers and Svedlund [21].
Similar findings were made by Coelho et al. [1] using a regression model where tinnitus was less prevalent in children with moderate to profound sensorineural hearing loss, than in those children with minimum to mild hearing loss. Minimum to mild hearing loss was a risk factor for tinnitus with an OR of 1.8 for tinnitus sensation and 2.4 for tinnitus suffering. Moderate to profound hearing loss (including deafness) was also considered risk factors with ORs of 0.5 for tinnitus sensation and 1.1 for tinnitus suffering.
The fact that a mild loss on hearing is a risk factor for tinnitus in children may be explained by the finding that even a mild hearing loss (thresholds at 30 dB HL) could promote tonotopic reorganization of the auditory cortex [28].
Temporary Threshold Shifts
Holgers and Petterson [29] have reported that individuals with temporary threshold shift (TTS) from noise exposure had an OR of 1.4 to present spontaneous tinnitus and 2.0 to noise-induced tinnitus. When comparing participants who sometimes experienced TTS to participants who did not have TTS, the OR was 2.8 to present spontaneous tinnitus and 8.4 to noise-induced tinnitus.
Noise Exposure
Holgers and Petterson [29] found that adolescents who attended concerts and discos/clubs had an OR of 1.4 regarding noise-induced tinnitus. Individuals who visited concerts 6–12 times per year had an OR of 4.4, compared to those who never went to concerts. Children who visited discos/clubs had an OR of 3.8.
Coelho et al. [1] reported that history of noise exposure was a risk factor for both tinnitus sensation and tinnitus suffering with ORs of 1.8 and 2.8, respectively. They found that firecrackers were the most frequent kind of noise exposure. Such noise may have peak levels of 145–165 dB HL at a distance of 2 m or less from the explosion site [30]. Risk of exposure to excessive noise from toys has also been mentioned on the literature [31, 32]. Exposure to high levels of noise from toys and firecrackers were reported by 25% of children who sought medical care because of noise trauma [33].
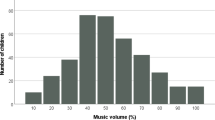
Tinnitus is also often associated with the use of music players such as the walkman and iPOD devices both in the right ear (p = 0.004) and in the left ear (p = 0.000) [34].
Activation of neural plasticity by overexposure or reduced impact to the auditory nervous system caused by hearing loss may cause tinnitus (see Chaps. 12 and 13). The reorganization on the tonotopic map of the primary auditory cortex following noise trauma is one sign of activation of neural plasticity that has been documented in several studies [35, 36] and it has been suggested that tinnitus may be related to such reorganization [37–39].
Motion Sickness
Motion sickness was found to be a risk factor for tinnitus sensation with an OR of 1.8 [1]. Motion sickness has been highly associated to migraine and vestibular symptoms in children [40].
Hyperacusis
Hyperacusis and tinnitus are related symptoms [41] (see Chap. 3). Coelho et al. [1] showed that hyperacusis was the highest risk factor for tinnitus in children, with an OR of 4.2, but tinnitus was not a risk factor for hyperacusis [1, 42].
Conclusions
The remedy from some of the shortcomings of present studies is as follows.
The available data regarding the epidemiology of tinnitus have a high degree of variations among different studies. There is therefore a need of more studies to bring down the variability. This chapter has pointed to some factors that have contributed to the variations in the results among different studies. Cross over or cohort studies with randomized samples representative of the whole population should be considered. Participants for such studies could be recruited from schools where stratification and randomization of the participants can be achieved. Participants from a school environment have fewer dropouts; consents from parents can easily be obtained. Multivariate regression models should be used to describe risk factors.
Some of the problems with present studies are related to the definition of tinnitus. Standardized interviews such as: “Do you hear a noise (sound) in your ears or in your head that last more than 5 min?” should be used in evaluation of the tinnitus, and evaluation of the impact on everyday life is important. Questions such as “Does this noise (sound) bother you?” should be included in the questionnaires.
Audiological testing is important for evaluating tinnitus etiology and standardized methodology, and classification of results should be used.
An epidemiological surveillance system would be the basic action to prevent tinnitus. Efficient preventive measures should aim at hearing education and prevention of noise exposure as early as possible (see Chap. 69).
Abbreviations
- OR:
-
OR
- TTS:
-
Temporary threshold shift
- HL:
-
Hearing Level
References
Coelho, CB, TG Sanchez, and RS Tyler, Tinnitus in children and assciated risk factors. Prog Brain Res, 2007 166:179–91
Mills, RP, DM Albert, and CE Brain, Tinnitus in childhood. Clin Otolaryngol Allied Sci, 1986 11(6):431–4
Nodar, R and M Lezak, Paediatric tinnitus: a thesis revisited. J Laryng Otol, 1984 9:234–5
Savastano, M, Characteristics of tinnitus in childhood. Eur J Pediatr, 2006 166(8):797–801
Coelho, CB and RS Tyler, Management of tinnitus in children, in Paediatric Audiological Medicine, V Newton, Editor 2009, Wiley & Sons: West Sussex, 418–27
Martin, K and S Snashall, Children presenting with tinnitus: a retrospective study. Br J Audiol, 1994 28(2):111–5
Gabriels, Children with tinnitus in 5th International Tinnitus Seminar.1996 Portland: USA American Tinnitus Association
Aksoy, S, et al, The extent and levels of tinnitus in children of central Ankara. Int J Pediatr Otorhinolaryngol, 2007 71(2):263–8
Drukier, GS, The prevalence and characteristics of tinnitus with profound sensori-neural hearing impairment. Am Ann Deaf, 1989 134(4):260–4
Kentish, RC, SR Crocker, and L McKenna, Children’s experience of tinnitus: a preliminary survey of children presenting to a psychology department. Br J Audiol, 2000 34(6):335–40
Kentish, RC and SR Crocker, Scary monsters and waterfalls: tinnitus narrative therapy for children, in Tinnitus Treatment Clinacal Protocols, R Tyler, Editor 2006, Thieme: New York
Nodar, RH, Tinnitus aurium in scholl age children: a survey. J Aud Res, 1972 12:133
Graham, J, Tinnitus aurium. Acta Otolaryng, 1965 Suppl(202):24–6
Leonard, G, F Black, and J Schramm, Tinnitus in Children, in Pediatric Otolaryngology, CD Bluestone, S Stool, and S Arjona, Editors 1983, W Saunders: Philadelphia, 271–277
Møller AR and P Rollins, The non-classical auditory system is active in children but not in adults. Neurosci Lett, 2002 319:41–4.
Mills, RP and JR Cherry, Subjective tinnitus in children with otological disorders. Int J Pediatr Otorhinolaryngol, 1984 7(1):21–7
Viani, LG, Tinnitus in children with hearing loss. J Laryngol Otol, 1989 103(12):1142–5
Savastano, M, A protocol of study for tinnitus in childhood. Int J Pediatr Otorhinolaryngol, 2002 64(1):23–7
Stouffer, J, et al, Tinnitus in normal-hearing and hearing-impaired children. In IV International Tinnitus Seminar 1991 Kugler Publications: Bordeaux
Aust, G, Tinnitus in childhood. Int Tinnitus J, 2002 8(1):20–6
Holgers, K and Svedlund C, Tinnitus in childhood. J Psychosomat Res, 2003 55(2):135
Eley, TC, P Lichtenstein, and J Stevenson, Sex differences in the etiology of aggressive and nonaggressive antisocial behavior: results from two twin studies. Child Dev, 1999 70(1):155–68
Penner, MJ, Linking spontaneous otoacoustic emissions and tinnitus. Br J Audiol, 1992 26(2):115–23
Burns, EM, KH Arehart, and SL Campbell, Prevalence of spontaneous otoacoustic emissions in neonates. J Acoust Soc Am, 1992 91(3):1571–5
Weiss, LA, et al, Sex-specific genetic architecture of whole blood serotonin levels. Am J Hum Genet, 2005 76(1):33–41
Tremere, LA, JK Jeong and R Pinaud, Estradiol shapes auditory processing in the adult brain by regulating inhibitory transmission and plasticity-associated gene expression. J Neurosci, 2009 29(18):5949–63
Graham, JM, Tinnitus in children with hearing loss. Ciba Found Symp, 1981 85:172–92
Norena, AJ and JJ Eggermont, Enriched acoustic environment after noise trauma reduces hearing loss and prevents cortical map reorganization. J Neurosci, 2005 25(3): 699–705
Holgers, KM and B Pettersson, Noise exposure and subjective hearing symptoms among school children in Sweden. Noise Health, 2005 7(27):27–37
Smoorenburg, GF, Risk of noise-induced hearing loss following exposure to Chinese firecrackers. Audiology, 1993 32(6):333–43
Axelsson, A, et al, Noisy toys – a risk of hearing injuries? Lakartidningen, 1984 81(45):4162–6
Rytzner, B and C Rytzner. Schoolchildren and noise. The 4 kHz dip-tone screening in 14391 schoolchildren. Scand Audiol, 1981 10(4):213–6
Segal, S, et al, Inner ear damage in children due to noise exposure from toy cap pistols and firecrackers: a retrospective review of 53 cases. Noise Health, 2003 5(18):13–8.
Bulbul, SF, et al, Subjective tinnitus and hearing problems in adolescents. Int J Pediatr Otorhinolaryngol, 2009 73(8):1124–31
Robertson, D and DR Irvine, Plasticity of frequency organization in auditory cortex of guinea pigs with partial unilateral deafness. J Comp Neurol, 1989 282(3):456–71
Komiya, H and JJ Eggermont, Spontaneous firing activity of cortical neurons in adult cats with reorganized tonotopic map following pure-tone trauma. Acta Otolaryngol, 2000 120(6):750–6
Rauschecker, JP, Auditory cortical plasticity: a comparison with other sensory systems. Trends Neurosci, 1999 22(2):74–80
Norena, A, et al, Psychoacoustic characterization of the tinnitus spectrum: implications for the underlying mechanisms of tinnitus. Audiol Neurootol, 2002 7(6):358–69
Norena, AJ and JJ Eggermont, Changes in spontaneous neural activity immediately after an acoustic trauma: implications for neural correlates of tinnitus. Hear Res, 2003 183(1–2):137–53
Uneri, A and D Turkdogan, Evaluation of vestibular functions in children with vertigo attacks. Arch Dis Child, 2003 88(6):510–1
Tyler, RS and LJ Baker, Difficulties experienced by tinnitus sufferers. J Speech Hear Disord, 1983 48(2):150–4
Coelho, CB, TG Sanchez, and RS Tyler, Hyperacusis, sound annoyance and loudness hypersensitivity in children. Prog Brain Res, 2007 166:169–78
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2011 Springer Science+Business Media, LLC
About this chapter
Cite this chapter
Coelho, C.B. (2011). Epidemiology of Tinnitus in Children. In: Møller, A.R., Langguth, B., De Ridder, D., Kleinjung, T. (eds) Textbook of Tinnitus. Springer, New York, NY. https://doi.org/10.1007/978-1-60761-145-5_6
Download citation
DOI: https://doi.org/10.1007/978-1-60761-145-5_6
Publisher Name: Springer, New York, NY
Print ISBN: 978-1-60761-144-8
Online ISBN: 978-1-60761-145-5
eBook Packages: MedicineMedicine (R0)