
Abstract
Thanks to modern protective equipment and advanced medical solutions, many service members now survive severe limb injuries that in previous wars would have been lethal. Unfortunately, these injuries can be devastating, requiring amputation, reconstruction, and prosthetics to restore function. Military research and development has taken the lead in addressing these challenges, establishing advanced prosthetic solutions as a top priority to meet the needs of injured service members. One such solution is conceived as a manufacturer-agnostic, interoperable lower extremity gait system (LEGS) to restore ambulatory function. As envisioned, the LEGS system would be adaptively responsive and volitionally controlled by the user and configured to maximize component compatibility through the use of open standards. In this chapter, we summarize the primary concerns and considerations that were addressed as objectives through the LEGS initiative, emphasizing essential design features and componentry, including control, sockets, bus, power, algorithms, and the need for open source and open standards to support meaningful and efficient scientific and technical collaboration. Critical knowledge gaps, capability gaps, component limitations, and nontechnical considerations point to the need for additional research and development. These efforts will require significant funding, commitment, and convergence of scientific and engineering resources. We hope that the knowledge and ideas presented here and throughout this volume will stimulate further progress toward the successful realization of advanced solutions such as LEGS.
Access provided by CONRICYT-eBooks. Download chapter PDF
Similar content being viewed by others


Keywords
Introduction
Military conflicts in Iraq and Afghanistan exposed US service members to the widespread use of improvised explosive devices (IEDs) by enemy combatants and thus to potentially devastating blast-related injuries. Thanks to modern protective military equipment and advanced medical solutions and technologies, many service members have survived these and other injuries that in previous wars would have been lethal. Unfortunately, many survivors have sustained significant limb injuries or losses that require reconstruction or amputation (see MacKenzie and Bosse [35] in this volume) and subsequent orthotic or prosthetic intervention to restore function (see also Pasquina et al. [48] in this volume). Dealing with the number, complexity, and long-term sequelae of limb trauma and amputations has become a top priority for military medical researchers and caregivers, whose work ultimate extends to benefit the treatment and recovery of civilians who suffer similar injuries.
To promote advanced military medical solutions for lower limb amputees, the US Army Medical Research and Materiel Command’s (MRMC) Telemedicine and Advanced Technology Research Center (TATRC) sponsored a series of meetings to identify the state of the art and to advance the state of the possible in lower limb prosthetic concept, technology, and design. Participants and contributors were drawn from industry, academe, clinical practice, nonprofit, and government sectors. Government-level subject matter experts were included from the National Aeronautics and Space Administration (NASA), Food and Drug Administration (FDA), Department of Defense (DoD), and Walter Reed National Military Medical Center (WRNMMC). The goal of their collaboration with TATRC was to envision and identify requirements for a manufacturer-agnostic lower extremity gait system (LEGS)Footnote 1 that would consist of customizable, interchangeable, and interoperable components to restore ambulatory function. The envisioned system would exemplify an easy-to-maintain human-centric design that is adaptively responsive and volitionally controlled by the user and configured to maximize component compatibility through the use of open standards.
The insights and findings drawn from the LEGS meeting series inspired development of this book, with chapters developed and organized to capture the broad scope and multiple domains and disciplines of scientific medical inquiry, componentry, and technical development necessary to foster the design and development of advanced prosthetics in general and of LEGS in particular. Through literature search, site visits, and extensive discussion and collaboration, LEGS project workers and participants identified specific challenges, gaps, needs, and barriers that must be overcome to advance numerous involved component capabilities (see also Fite [7] in this volume) and to bridge the divide between current device capabilities and the ideal future system envisioned as LEGS. Their deliberations targeted essential design features and componentry, including control, sockets, bus, power, algorithms, and the need for open source and open standards to support meaningful and efficient scientific and technical collaboration. Critical knowledge gaps, capability gaps, component limitations, and nontechnical considerations (e.g., limited training, lack of standardization) were identified, pointing to the need for additional research and development to achieve the vision of an advanced system such as LEGS. Here, we summarize the primary concerns and considerations that were addressed as research and development objectives through the LEGS initiative.
Sockets and Sensors
Specific gaps identified included the need for more durable socket technologies, advanced materials, and liners to preserve patient health and comfort while maintaining residual limb homeostasis and management of external forces. Although socket design has advanced over more than a century of prosthetic design and development history (see also Gailey et al. [8] in this volume), today’s prosthetic users all too commonly experience residual limb skin problems related to residual limb volume, moisture accumulation, shear force, and external stressors associated with walking and running [4, 29, 39]. Although not yet a viable alternative, researchers are working to develop osseointegration procedures that could eliminate the need for socket-based suspension by allowing direct attachment of a prosthetic limb to the bone (see Webster et al. [61] in this volume). As a near-term requirement for LEGS , project participants identified the need for improved socket and liner materials that enable heat dissipation, user-controlled adjustment, and adaptability to ambulatory function without the need for user input. They considered that these objectives could be addressed initially by determining the minimum biomechanical surface necessary to allow a lighter, more comfortable interface while preserving security and function.
Socket liner materials have been widely explored, for example, to include thermoplastic materials such as copolymer (TPE), polyurethane (PUR), and silicone. Some difficulties might be mitigated by the incorporation of newer materials, composites, and designs that can exploit the properties of advanced alternative materials such as nickel titanium, ceramic (porous, thread, matrix for composite), shape memory, and thermo-conductive polymers. Unfortunately, the influence of liner materials on prosthetic user performance is not well understood. Little research has been done to inform prescription practice as to how liner material selection might affect individual residual limb and patient health [28]. As a result, clinicians must rely primarily upon their own professional experience. In addition to improved materials research, development, and testing, there is a need for improved socket measurement and fitting processes. Although measurement and fit have improved greatly through the use of computer-aided design (CAD) and other advanced tools, these techniques are not error-free. Practitioners need evidence-based guidance and training to better meet the specific needs of their individual patients.
Socket design and function would be improved by the incorporation of durable, rugged, miniaturized sensors that can be used to provide device and biological feedback to the system and its user. Sensors can be used to detect changes in temperature, pressure, moisture, volume, shear, impedance, kinetics and kinematics, blood flow, and other biological and environmental variables. For example, movement can be “sensed” by measuring linear acceleration via an accelerometer and angular rate via a gyroscope [17]. Sensors can be embedded in wearable items such as socks, but prosthetic applications present unique challenges with respect to sensor size and durability . To fit comfortably, and to function reliably within a prosthetic device socket, the sensor must be miniaturized, flexible, and ruggedized to perform effectively in hot, humid, or desert-like environments and at close proximity to human tissue. Advanced computer capability is also needed to support the integration of multiple sensors as a functional suite with actuator output.
The ideal LEGS would include a responsive homeostatic device that could dynamically manage force, circulation, moisture, volume, and other socket environment variables without requiring direct user input. By feeding proprioceptive and exteroceptive sensor feedback to prosthetic device control, it may be possible to support more natural motion. To this end, it would be helpful to determine what type and how much feedback is most effective, for example, to improve user gait without requiring unnatural or extraordinary effort by the user. Research is needed to test and compare various types of feedback (e.g., tactile vs. auditory) and evaluate their relative effectiveness and impact on user performance. Relatedly, researchers should consider that it may be helpful to prioritize performance-critical feedback and to filter out potentially distracting feedback that might interrupt or hinder performance. The ultimate objective is to translate meaningful information about prosthetic performance and socket environment into effective user control, via adaptive algorithms and control loops that are as analogous as possible to native motor control and reflexive systems.
In order for an advanced prosthesis to “learn” its user’s intent, the system will require advanced pattern recognition, time series analysis, and learning algorithms to monitor, analyze, and respond to user performance and outcome data (e.g., correct event detections, responses, adjustments, and falls). One candidate approach is a wireless body sensory network (BSN; [13]), which could be used to monitor physical demands that are placed on the user while mobile (e.g., ground reaction forces during heal-toe strike), supply information directly to the user, and ultimately inform researchers working to improve prosthetic design. Autonomous patient control could further be enhanced through the additional use of electroencephalography (EEG), targeted muscle reinnervation (TMR), and implantable myoelectric sensors (IMES). These volitional control technologies are considered in more detail later in this chapter.
Power and Control
Among the challenges to achieving a fully integrated LEGS system is the need for standardized power and data buses that can communicate effectively and reliably with one another. Currently, separate prosthetic devices (e.g., knee and ankle prostheses) are forced by design to operate independently, never communicating with one another concerning their respective operations, power, or performance. Where a prosthetic configuration includes multiple devices, the user should have the option to exploit fully integrated control and linkage, for example, via a personal computer bus that allows each device to draw power from the other as needed, download updated software for each device, or adjust performance of one device to accommodate the known capabilities or limitations of another. This proposal is achievable in principle but is not yet possible in practice. Integrated device control is well within the capabilities of currently available systems and technologies, but linkage requires willingness on the part of prosthetic manufacturers to employ shared standards.
The “muscle” or driver of the prosthetic is its actuator. Historically, actuator technologies have been heavy, bulky, inefficient, difficult to control, and capable of high force but ineffective for fine movements or adjustments. Direct current motor technology improves actuator power density but at torques and speeds that are not well matched to the needs of prosthetic ankle and knee systems. The speed and force of conventional actuators cannot replicate what is achieved by human musculature that supports native lower limb gait and function. Notable advances have occurred in the development and demonstration of back-drivable and series-elastic actuators that can be more precisely controlled [18, 37, 58]. The application of pneumatic muscle actuators (pMAs) to wearable exoskeleton legs also demonstrates the potential for “soft” actuation, at least in the rehabilitative setting ([3]; Rovekamp et al. [52] in this volume). New designs emphasize force and torque control to support more precise user-system interaction. Additional efforts to achieve biomimetic actuation include explorations using electroactive and conducting polymers [17, 26] and artificial and animal-derived muscle [19, Shahinpoor [56] in this volume]. Among the advantages of these solutions would be more quiet and adaptive function of the sort envisioned through the LEGS initiative [18, 20]. “Soft” technologies and conforming biomimetic structures can also serve to reduce system weight and improve portability and efficiency.
Advanced developments in the field of lower extremity prosthetics are moving increasingly toward actively powered designs that require independent power sources. Here again, the need for open standards and standardization presents a nontechnical but significant challenge. Interoperability among multiple devices is necessary to an integrated system. The ideal power supply/battery would be a single small, centralized, lightweight, rugged, long-duration supply that is quickly and easily rechargeable using standardized connectors and chargers. Additional beneficial capabilities might include central logic data processing, energy harvesting, and stand-by power management.
Prosthetics users desire control that is responsive to their intent. A key design challenge is to provide an effectively balanced combination of conscious and automated control features. The goal is to enable the user to execute behavioral choices (e.g., position, motion, speed, and trajectory) in real time, unburdened by excessive requirements to monitor or adjust variables that are critical to comfort, safety, or device attributes such as power management. To address the latter concern, a number of advanced prosthetic devices have already demonstrated the benefits of microprocessor-supported control, including improved knee flexion, enhanced energy management, better knee resistance, improved smoothness, and symmetry of gait [25, 27, 53, 55]. As to the need for conscious user control, one key objective of the LEGS project was to consider state-of-the-possible solutions for intent-responsive control.
Volitional Control
Researchers have explored and continue to explore various methods of voluntary control via signals recorded from muscular and neural sources (see Hargrove [14] in this volume). Potential applications have been demonstrated using invasive and noninvasive brain machine interfaces (BMIs), myoelectric sensors (MES), electromyography (EMG), and targeted muscle reinnervation (TMR) [6, 15, 16, 47]. In each case, technical challenges concern signal recording quality, transmission, and signal processing algorithms, additional power requirements, human tissue fragility, and the installation of permanent electrode arrays. Noninvasive BMIs avoid the need for surgical implantation but are relatively more vulnerable to recording artifact. Noninvasive BMI users must learn to control specific derivative signal indices such as brain-evoked potentials, specific rhythms, or firing rates.
Brain-Based Control
Intracranial BMIs have been demonstrated using implanted electrode arrays in animal as well as human subjects, to achieve real-time control of robotic devices via the recording of motor commands from ensemble neuronal activity in the motor cortex [2, 21, 45]. Potential applications include restoration of motor behavior in patients who have suffered loss of function due to brain or spinal disease or injury, including amputation. Though certainly promising, there are numerous biomedical engineering challenges associated with the design and implementation of BMI-based prosthetics. For example, because it is difficult to obtain electrically stable recordings with appropriate fidelity from large populations of neurons in multiple brain areas, implantable amplifiers and signal processors must be resistant to electrical noise and artifact [49]. Computationally sophisticated but efficient algorithms are necessary to translate neuronal activity into command signals that can control prosthetic or robotic actuators with multiple degrees of freedom. It remains to be seen how or if the brain’s own plasticity can be exploited effectively to incorporate a prosthetic device into the human body’s full neural representation and if the human brain can adapt and respond to accept, integrate, and directly control an artificial limb. Lebedev and colleagues [33, 34] provide thoughtful discussion of numerous bioengineering problems that have yet to be addressed. In addition, there are questions surrounding the biocompatibility, longevity, and sustainability of chronic brain implants. Brain inflammatory responses can cause recording failure, and, to ensure stable recording, it is necessary to prevent movement or migration of an electrode array relative to the underlying cortex [51, 54].
A number of clinical trials are underway or recently completed to study the use of implanted brain-recording devices to achieve “thought” control of external assistive devices such as computers, robotics, and virtual reality environments by individuals who have suffered spinal cord injuries, stroke, or neurodegenerative disease (see ClinicalTrials.gov identifiers NCT00912041, NCT01393444, NCT01958086, NCT01849822, NCT01964261, NCT01364480). Where the ultimate goal is to control a prosthetic limb, a significant technical question is how best to provide proprioceptive feedback to a user whose ability to control the prosthetic may otherwise depend almost entirely upon constant visual attention to the prosthetic [50, 60].
EEG-based control technologies employ scalp surface electrodes to record spontaneous changes in voltage generated by large populations of underlying neurons. EEG can be used to detect changes that correspond to specific medical conditions (e.g., seizures, coma) and can be derived (averaged) as evoked or event-related potential waveforms to identify responses to specific sensory stimuli, changes in attention, or recognition. EEG signal recording allows high temporal resolution (milliseconds) and has been applied in a variety of settings to support mind-based control of fairly simple tasks such as basic cursor control, with potential application to prosthetic control [11, 31, 32, 36, 41]. However, scalp surface-recorded EEG signals are limited by poor cortical spatial resolution. Recorded signals represent electrical activity coming from large and/or multiple underlying brain regions; signal quality is greatly attenuated by the skull. As a result, EEG signal discrimination and processing tend to be slow and imprecise. EEG recordings are also highly susceptible to contamination by electrical artifact from muscle tissue, body movement, recording instruments, eye blinks, and the environment. EEG electrodes can be uncomfortable and are difficult to position on the scalp with repeatable precision. Thus, EEG-based control is not optimal for applications that involve complex sequences, rapid movements, and multiple degrees of freedom. Other noninvasive methods of recording changes in brain activity associated with magnetic field or blood flow, such as magnetoencephalography (MEG) and functional magnetic resonance imaging (fMRI), can eliminate much of the signal distortion associated with EEG and provide much better signal spatial resolution. However, MEG and fMRI recording equipment is very large, fragile, vulnerable to motion artifact, and not at all portable as would be necessary for use to control ambulation. Limited to research and clinical settings, MEG and fMRI may nonetheless be useful in research that aims to identify, localize, and characterize motor control signal sources and patterns to inform other BMI applications.
Muscle-Based Control
Surface-recorded EMG contains signal components from multiple muscle sources. Design features and signal processing strategies are needed to challenge the inherent limitations of surface-recorded EMG and to enhance its utility (e.g., [5, 12, 18,19,24, 44]). To achieve more robust control of lower limb prostheses, researchers are working to develop safe, comfortable implantable myoelectric sensor systems that can provide greater and more precise control via wireless connection to the target device (e.g., [1, 38, 62]). Long-term implantable myoelectric sensors (IMES) allow recording of source EMG signals, which can be transmitted to a controller by wireless telemetry [38, 62]. To date, research in this area has focused primarily on the use of IMES to control prostheses for upper limbs (e.g., [59]).
Targeted muscle reinnervation (TMR) is an advanced surgical procedure involving the transfer of residual nerves to alternative muscle sites. Once the alternative muscle sites are reinnervated, they produce EMG signals that can be recorded and measured at the skin surface and used to control a prosthetic device. In 2012, TMR was applied to enable an above-the-knee, right leg amputee to climb 103 floors of Chicago’s Willis Tower (http://www.npr.org/sections/thetwo-way/2012/11/05/164335844/amputee-climbs-103-floors-of-chicagos-willis-tower-using-bionic-leg). Though TMR-based control is certainly at the leading edge of volitionally controlled (“bionic”) prosthetic system development, additional research is needed to provide sensory feedback to the prosthetic limb or to the reinnervated muscle. Additional degrees of freedom (e.g., via nerve splitting) are also needed to provide more independent signals. These advances are necessary to support systems that are responsive to changing terrain and can avoid obstacles. If TMR can ultimately be combined with advanced tissue replacement/regeneration technologies, it may become possible to develop functional, bio-artificial neuromuscular junctions (e.g., man-made muscle attached to titanium bone).
Biomaterials and Tissue Engineering
Some far-future research and technology development objectives could one day revolutionize or even obviate the need for prosthetics as they are currently defined, designed, and envisioned. Advanced medical scientific pursuits in tissue engineering, limb transplantation, and limb regrowth may eventually allow surgeons to replace lost or damaged original limbs with fully functional, biomaterial substitutes. Various such endeavors are explored in detail elsewhere in this volume (see chapters by Gorantla et al. [9] Shahinpoor [56]; Muneoka et al. [42]).
Explorations in stem cell research are especially relevant to bioengineering objectives. For example, embryonic, induced pluripotent (iPS) and mesenchymal stem cells are under investigation to restore various types lost or diseased tissue , including limb tissues such as the skin, bone, and tendon [40, 42, 46, 63]. Embryonic stem cells are especially flexible for use in bioengineering applications; they are easy to expand in culture and can be differentiated to any cell type [30]. However, it is a challenge to direct and sustain stem cell differentiation, and it can be difficult to predict how stem cells will behave after they are transplanted. Undifferentiated stem cells can give rise to malignant transformation, which must be suppressed. Much additional research is needed to specify signaling proteins, matrix chemicals, and molecules needed to overcome various difficulties. Although similar technical challenges are raised by the use of iPS cells, this approach is less controversial because the cells are derived from adult body tissues rather than human embryos. In principle, iPS cells can be harvested directly from the patient. In an original demonstration that connective tissue cells could be differentiated into other tissue types in three dimensions, Sommar et al. [57] successfully cultured connective tissue cells from human skin in vitro to create cartilage, bone, and vascular endothelium.
Other Requirements
Additional challenges to achieving the envisioned LEGS system do not require new or improved technology itself but rather the pressing need for improved access to existing technology. Chief among these requirements is the need for interchangeable component configurations and platforms that provide open source, innovative, standardized communication with one another via sensors and actuators. Open source innovations are not entirely incompatible with proprietary interests. For example, open application programming interfaces (APIs) can be exposed without revealing their underlying code, to allow programming for component communication without violating proprietary protections. However, a current lack of shared standards in the prosthetics industry slows progress toward the development of fully integrated systems with interchangeable componentry. The Open Prosthetics Project (openprosthetics.org) attempts to overcome this challenge by supporting open source collaboration among users, designers, and research funders. The objective is to accelerate innovation and promote free sharing of new designs.
The need for open source standards was raised repeatedly by LEGS project participants, who recognized generally that progress on this point is limited only by the willingness of the prosthetic development and manufacturing community itself. When proprietary objections are resolved, it will be possible to overcome current barriers to the system-of-systems approach that is crucial to achieve and advance fully integrated and advanced prosthetic systems. Open standards are needed for power, data, physical, and network component connections.
As a starting point, the prosthetic device community could develop and demonstrate an open source system simply for the purpose of gathering aggregate outcome data (e.g., usage, event detection, long-term monitoring) from various individual prosthetic systems, sensors, and component technologies. A centralized data repository would also be needed to provide access to the collected data and to enable outcome-based research aimed at improving system safety, reliability, and faster regulatory review to the benefit of all concerned. This would also help meet the need for data and information exchange between experts in medicine, industry, academe, and the military.
Participants in the LEGS project meetings also identified the need for more and improved training and awareness to benefit practitioners as well as their patients. As advanced solutions and capabilities develop rapidly, even those who work and are served in dedicated facilities may be unaware of emerging technologies. More proactive efforts are needed to provide continuing education and outreach to those who provide prosthetic services and to patients who need the best available, most advanced and emerging solutions. LEGS project participants suggested holding annual training events, for example, to align with annual professional meetings (e.g., American Academy of Orthotists and Prosthetists/AAOP), as well as centralized training at major military medical centers (e.g., Walter Reed National Military Medical Center/WRNNMC).
Although regulatory processes are certainly necessary to ensure safety, liability, and fiscal responsibility, they sometimes have unintended, unanticipated, and discouraging effects on research and development. Participants in the LEGS meetings considered that best outcomes are rarely driven by policies and practices defined in isolation by a single organization or interest. Rather, policy better supports and represents all relevant objectives, concerns, and perspectives when it is developed as a coordinated effort involving all relevant stakeholders. Where the goal is to create an affordable, capable, safe, and effective prosthetic system such as that envisioned by LEGS, policy development should allow participation of relevant government entities, researchers, industry representatives, clinicians, insurers, and – arguably most important – prosthetics users who can by their own experience speak directly to the health concerns, practical needs, and functional priorities of those who rely on advanced prosthetic technologies.
One regulatory response to these concerns has been the FDA’s recent revision of its Investigational Device Exemptions (IDE) guidance (http://www.fda.gov/MedicalDevices/DeviceRegulationandGuidance/HowtoMarketYourDevice/Investi-gationalDeviceExemptionIDE/ucm162453.htm). The provisions of the FDA’s IDE regulation assign responsibilities to all participants in clinical investigation and exempt consumer preference testing of a modification or of a combination of devices. When combined with Early Feasibility Studies (usually involving 15 or fewer subjects) and the FDA’s Expedited Access Pathway (EAP) program (FDA involvement through the collaborative creation of a “Data Development Plan”), the FDA hopes to “facilitate timely access to medical devices by expediting their development, assessment, and review, while preserving our statutory standards for safety and effectiveness and protecting patients” (http://www.fda.gov/downloads/medicaldevices/deviceregulationandguidance/guidancedocuments/ucm393978.pdf).
Conclusion
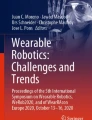
In May of 2016, two veterans wounded by roadside bombs in Iraq and Afghanistan made history and inspired fellow wounded warriors as they made their way into thin air toward the 29,029-ft summit of Mount Everest. Former Marine Staff Sergeant Thomas Charles “Charlie” Linville and former Army reservist Chad Jukes (Fig. 1.1) both wore lower limb prostheses and took the route less traveled, along the northern, Chinese side of the mountain. Although the two combat amputees belonged to different expedition teams sponsored by different veterans’ organizations, they met during the climb. Linville and Jukes had to avoid all of the same dangers that threaten other climbers, while taking care to mitigate potentially more severe consequences. For example, reduced blood flow to an amputee’s stump introduces an increased risk for frostbite. But for wounded warriors Linville and Jukes, it is not enough to overcome the challenges of daily life as an amputee. They challenged themselves to extreme adverse conditions, including raging winds and the “death zone” above 26,000 ft.

Chad Jukes is pictured climbing ice at advanced basecamp (6,400 m) on Mount Everest. Photograph courtesy of Dr. David Ohlson (daveohlson.com)
The many ordinary and extraordinary accomplishments of wounded warriors bring into sharp focus the original vision of the LEGS project as part of TATRC’s commitment to “cultivate great ideas” and the exploration of new concepts [10]. This volume was developed not simply to capture the current state of the art but to inspire continued development toward the state of the possible as envisioned by LEGS. For those who will engage prosthetic technology challenges yet to be overcome, this book provides a benchmark for today’s state of the science and identifies current gaps in knowledge, materials, technology, and access. The “great idea” envisioned by LEGS was and is a human-centric adaptive and assistive powered system design that is customizable and interchangeable, with interoperable components to restore volitionally controlled ambulatory function. Driven by great ideas, science, engineering, and development of advanced technology are, by necessity, iterative processes that require investment, intellectual freedom, and dogged determination to continue climbing, sometimes against all odds through the thin air of institutional and proprietary barriers.
Originally wounded in 2011, Charlie Linville reached the summit of Mount Everest just 5 years later on May 19, 2016. Chad Jukes, wounded in 2005, arrived at the Mount Everest summit on May 24, 2016. Both climbers have expressed that they want their efforts to benefit veterans and promote physical and psychological healing of the wounds of war. Though humbled by their achievements, we share their desire. We imagine, for example, how future mountain climbers might benefit by the development of LEGS-inspired prosthetics with assistive power, better agility, just-in-time on-the-spot adjustment and correction, and unlimited volitional control. We hope this book provides essential knowledge, perspective, and a creative blueprint that will inspire medical scientists and bioengineers to progress toward such a vision and toward ever more advanced prosthetic solutions.
Notes
- 1.
Although it is arguably more common to describe the lost leg as a lost “limb” (vs. “extremity”) – the term “limb” distinguishes the leg in whole or part from its extreme appendages (toes) – prosthetic devices designed to replace the lost lower limb are often described as “lower extremity prostheses” (e.g., see http://www.aopanet.org/legislative-regulatory/study-higher-standard-of-care-for-patients-with-limb-loss-or-spinal-injuries-saves-medicare-money-in-most-cases/). Thus, when we refer to the “lower extremity gait system” described by the LEGS project, we use the term “extremity” to describe the envisioned prosthetic system, rather than the limb it supposes to replace.
References
Alcaide-Aguirre RE, Morgenroth DC, Ferris DP. Motor control and learning with lower-limb myoelectric control in amputees. JRRD. 2013;50(5):687–98.
Chapin JK, Moxon KA, Markowitz RS, Nicolelis MA. Real-time control of a robot arm using simultaneously recorded neurons in the motor cortex. Nat Neurosci. 1999;2(7):664–70.
Costa N, Caldwell DG. Control of a biomimetic “soft-actuated” 10DoF lower body exoskeleton. BioRob. 2006:495–501.
Dudek NL, Marks MB, Marshall SC, Chardon JP. Dermatologic conditions associated with use of a lower-extremity prosthesis. Arch Phys Med Rehabil. 2005;86(4):659–63.
Ferris DP, Gordon KE, Sawicki GS, Peethambaran A. An improved powered ankle-foot orthosis using proportional myelectric control. Gait Posture. 2006;23(4):425–8.
Fetz EE. Volitional control of neural activity: implications for brain-computer interfaces. J Physiol. 2007;579(3):571–9.
Fite KB. Overview of the components used in active and passive lower limb prosthetic devices. In: Tepe V, Peterson CM, editors. Full stride: advancing the State of the art in lower extremity gait systems. New York: Springer; 2017. p. xx.
Gailey RS, Clemens SM. Sacrifice, science, and support: a history of modern prosthetics. In: Tepe V, Peterson CM, editors. Full stride: advancing the State of the art in lower extremity gait systems. New York: Springer; 2017. p. xx.
Gorantla VS, Serdar Nasir FZ, Breidenbach WC, Davis MR. Lower extremity transplantation: concepts, challenges, controversies. In: Tepe V, Peterson CM, editors. Full stride: advancing the State of the art in lower extremity gait systems. New York: Springer; 2017. p. xx.
Grundfest WS, Lai E, Peterson CM, Friedl KE. Promoting innovation and convergence in military medicine: technology-inspired problem solving. IEEE Circ Syst Mag. 2012;12:14–29.
Guger C, Harkam W, Hertnaes C, Pfurtscheller G. Prosthetic control by an EEG-based brain-computer interface (BCI). In: Proc. AAATE 5th European Conference for the Advancement of Assistive Technology. 1999. Nov 3. pp. 3–6.
Ha KH, Varol HA, Goldfarb M. Volitional control of a prosthetic knee using surface electromyography. IEEE Trans Biomed Eng. 2011;58(1):144–51.
Hao Y, Foster R. Wireless body sensor networks for health-monitoring applications. Physiol Meas. 2008;29(11):R27–56.
Hargrove L. Volitional control research. In: Tepe V, Peterson CM, editors. Full stride: advancing the State of the art in lower extremity gait systems. New York: Springer; 2017. p. xx.
Hargrove LJ, Simon AM, Young AJ, Lipschutz RD, Finucane SB, Smith DG, Kuiken TA. Robotic leg control with EMG decoding in an amputee with nerve transfers. N Engl J Med. 2013;369:1237–42.
Hatsopoulos NG, Donoghue JP. The science of neural interface systems. Annu Rev Neurosci. 2009;32:249–66.
Herr H. Exoskeletons and orthoses: classification, design challenges and future directions. J Neuro Eng Rehabil. 2009;6(1):21.
Herr H, Whiteley GP, Childress D. Cyborg technology – biomimetic orthotic and prosthetic technology. In: Bar-Cohen Y, Breazeal CL, editors. Biologically inspired intelligent robots. SPIE Publications: WA; 2003.
Herr H, Dennis RG. A swimming robot actuated by living muscle tissue. J Neuro Eng Rehabil. 2004;1:6.
Herr HM, Kornbluh RD. New horizons for orthotic and prosthetic technology: artificial muscle for ambulation. Proc SPIE 5385. 2004.
Hochberg LR, Bacher D, Jarosiewicz B, Masse NY, Simeral JD, Vogel J, Haddadin S, Liu J, Cash SS, van der Smagt P, Donoghue JP. Reach and grasp by people with tetraplegia using a neutrally controlled robotic arm. Nature. 2012;485:372–5.
Hoover CD, Fulk GD, Fite KB. Stair ascent with a powered transfemoral prosthesis under direct myoelectric control. IEEE/ASME Trans Mechatron. 2013;18(3):1191–200.
Huang H, Zhang F, Hargrove LJ, Dou Z, Rogers DR, Englehart KB. Continuous locomotion-mode identification for prosthetic legs based on neuromuscular-mechanical fusion. IEEE Trans Biomed Eng. 2011;58(1):2867–75.
Jiang N, Englehart KB, Parker PA. Extracting simultaneous and proportional neural control information for multiple-DOF prostheses from the surface electromyographic signal. IEEE Trans Biomed Eng. 2009;56(4):1070–80.
Johansson JL, Sherrill DM, Riley PO, Bonato P, Herr H. A clinical comparison of variable-damping and mechanically passive prosthetic knee devices. Am J Phys Med Rehabil. 2005;84:563–75.
Jung K, Ryew S, Jeon JW, Kim H, Choi H. Experimental investigations on behavior of IPMC polymer actuator and artificial muscle-like linear actuator, smart structures and materials 2001: electroactive polymers actuators and devices. Proc SPIE. 2001;4329:449–57.
Kaufman KR, Levine JA, Brey RH, Iverson BK, McCrady SK, Padgett DJ, Joyner MJ. Gait and balance of transfemoral amputees using passive mechanical and microprocessor-controlled prosthetic knees. Gait Posture. 2007;26(4):489–93.
Klute GK, Glaister BC, Berge JS. Prosthetic liners for lower limb amputees: a review of the literature. Prosthetics Orthot Int. 2010;34(2):146–53.
Koc E, Tunca M, Akar A, Erbil AH, Demiralp B, Arca E. Skin problems in amputees: a descriptive study. Int J Dermatol. 2008;47(5):463–6.
Korin N, Levenberg S. Engineering human embryonic stem cell differentiation. Biotechnol Genet Eng Rev. 2007;24(1):243–62.
Lauer RT, Peckham PH, Kilgore KL. EEG-based control of hand grasp neuroprosthesis. Neuroreport. 1999;10(8):1767–71.
Lauer RT, Peckham PH, Kilgore KL, Heetderks WJ. Applications of cortical signals to neuroprosthetic control: a critical review. IEEE Trans Rehabil Eng. 2000;8(2):205–8.
Lebedev MA, Nicolelis MA. Brain-machine interfaces: past, present and future. Trends Neurosci. 2006;29:536–46.
Lebedev MA, Tate AJ, Hanson TL, Li Z, O’Doherty JE, Winans JA, Ifft PJ, Zhuang KZ, Fitzsimmons NA, Schwartz DA, Fuller AM, An JH, Miguel AL, Nicolelis MA. Future developments in brain-machine interface research. Clinics. 2011;66(S1):25–32.
MacKenzie EJ, Bosse MJ. Limb amputation vs. limb salvage. In: Tepe V, Peterson CM, editors. Full Stride: advancing the State of the art in lower extremity gait systems. New York: Springer; 2017. p. xx.
Mahmoudi B, Erfanian A. Single-channel EEG-based prosthetic hand grasp control for amputee subjects. In: Engineering in Medicine and Biology, 2002. 24th Annual Conference and the Annual Fall Meeting of the Biomedical Engineering Society EMBS/BMES Conference, 2002. Proceedings of the Second Joint 2002 Oct 23 (Vol. 3, pp. 2406–2407). IEEE.
Mathijssen G, Cherelle P, Lefeber D, Vanderborght B. Concept of a series-parallel elastic actuator for a powered transtibial prosthesis. Actuators. 2013;2:59–73.
Merrill DR, Lockhart J, Troyk PR, Weir RF, Hankin DL. Development of an implantable myoelectric sensor for advanced prosthesis control. Artif Organs. 2011;35(3):249–52.
Meulenbelt HE, Geertzen JH, Jonkman MF, Dijkstra PU. Skin problems of the stump in lower limb amputees: 1. A clinical study. Acta Derm Venereol. 2011;91(2):173–7.
Metcalfe AD, Ferguson MWJ. Tissue engineering of replacement skin: the crossroads of biomaterials, wound healing, embryonic development, stem cells and regeneration. JR Soc Interface. 2007;4:413–37.
Müller-Putz GR, Pfurtscheller G. Control of an electrical prosthesis with an SSVEP-based BCI. Biomed Eng IEEE Trans. 2008 Jan;55(1):361–4.
Muneoka K, Lai E, Christy RJ, Mogford JE. Limb regrowth and tissue engineering alternatives. In: Tepe V, Peterson CM, editors. Full stride: advancing the State of the art in lower extremity gait systems. New York: Springer; 2017. p. xx.
Murphy MB, Moncivais K, Caplan AI. Mesenchymal stem cells: environmentally responsive therapeutics for regenerative medicine. Exp Mol Med. 2013;45:e54.
Myers DR, Moskowitz GD. Myoelectric pattern recognition for use in the volitional control of above-knee prostheses. IEEE Trans Syst Man Cybern. 1981;11(4):296–302.
O’Doherty JE, Lebedev MA, Ifft PJ, Zhuang KZ, Shokur S, Bleuler H, Nicolelis MA. Active tactile exploration using a brain-machine-brain interface. Nature. 2011;479:228–31.
Oreffo ROC, Triffitt JT. Future potentials for using osteogenic stem cells and biomaterials in orthopedics. Bone. 1999;25(2):5S–9S.
Parker P, Engelhart K, Hudgins B. Myoelectric signal processing for control of powered limb prostheses. J Electromyogr Kinesiol. 2006;16(6):541–8.
Pasquina PF, Emba CG, Corcoran M, Miller ME, Cooper RA. Lower limb disability: present military and civilian needs. In: Tepe V, Peterson CM, editors. Full stride: advancing the State of the art in lower extremity gait systems. New York: Springer; 2017. p. xx.
Patil PG, Turner DA. The development of brain-machine interface neuroprosthetics devices. Neurotherapeutics. 2008;5(1):137–46.
Pistohl T, Joshi D, Ganesh G, Jackson A, Nazarpour K. Artificial proprioceptive feedback for myoelectric control. IEEE Trans Neural Syst Rehabil Eng. 2015;23(3):498–507.
Rousche PJ, Normann RA. Chronic recording capability of the Utah intracortical electrode array in cats sensory cortex. J Neurosci Methods. 1998;82(1):1–15.
Rovekamp RN Jr, Francisco GE, Chang S-H, Beck CE. Wearable robotic approaches to lower extremity gait systems. Osseointegration research. In: Tepe V, Peterson CM, editors. Full stride: advancing the State of the art in lower extremity gait systems. New York: Springer; 2017. p. xx.
Schmalz T, Blumentritt S, Jarasch R. Energy expenditure and biomechanical characteristics of lower limb gait: the influence of prosthetic alignment and different prosthetic components. Gait Posture. 2002;16:255–63.
Schwartz AB, Cui XT, Weber DJ, Moran DW. Brain-controlled interfaces: movement restoration with neural prosthetics. Neuron. 2006;52:205–20.
Segal AD, Orendurff MS, Klute GK, McDowell ML, Pecoraro JA, Shofer J, Czerniecki JM. Kinematic and kinetic comparisons of transfemoral amputee gait using C-leg and Mauch SNS prosthetic knees. J Rehabil Res Dev. 2006;43(7):857–70.
Shahinpoor M. Synthetic and biological multi-functional smart materials applications to lower extremity gait systems. In: Tepe V, Peterson CM, editors. Full stride: advancing the State of the art in lower extremity gait systems. New York: Springer; 2017. p. xx.
Sommar P, Pettersson S, Ness C, Johnson H, Kratz G, Junker JPE. Engineering three-dimensional cartilage- and bone-like tissues using human dermal fibroblasts and microporous gelatin microcarriers. J Plast Reconstr Aesthet Surg. 2010;63(6):1036–46.
Sulzer JS, Roiz RA, fishin MA, Patton JL. A highly backdrivable, lightweight knee actuator for investigating gait in stroke. IEEE Trans Robot: Publ IEEE Robot Autom Soc. 2009;25(3):539–48.
Troyk PR, DeMichele G, Kuiken T. Implantable myoelectric sensors (IMES) for upper-extremity prosthesis control-preliminary work. In: Engineering in Medicine and Biology Society, 2003. Proceedings of the 25th Annual International Conference of the IEEE 2003 Sep 17 (Vol. 2, pp. 1562–1565). IEEE.
Tucker MR, Olivier J, Pagel A, et al. Control strategies for active lower extremity prosthetics and orthotics: a review. J Neuroeng Rehabil. 2015;12(1):1.
Webster JB, Bachus KN, Beck JP, Jeyapalina S, Drew AJ, Bloebaum RD. Osseointegration research. In: Tepe V, Peterson CM, editors. Full stride: advancing the State of the art in lower extremity gait systems. New York: Springer; 2017. p. xx.
Weir RF, Troyk PR, DeMichele GA, Kerns DA, Schorsch JF, Maas H. Implantable myoelectric sensors (IMESs) for intramuscular electromyogram recording. IEEE Trans Biomed Eng. 2009;56(1):159–71.
Young RG, Butler DL, Weber W, Caplan AI, Gorden SL, Fink DJ. Use of mesenchymal stem cells in a collagen matrix for Achilles tendon repair. J Orthop Res. 1998;16(4):406–13.
Disclaimer
The views expressed here are the authors’ own and do not necessarily reflect the views, policies, or positions of the Department of Defense, the US Government, or employers.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2017 Springer Science+Business Media LLC
About this chapter
Cite this chapter
Tepe, V., Salas-Snyder, S., Peterson, C.M. (2017). The History and Future of LEGS. In: Tepe, V., Peterson, C. (eds) Full Stride. Springer, New York, NY. https://doi.org/10.1007/978-1-4939-7247-0_1
Download citation
DOI: https://doi.org/10.1007/978-1-4939-7247-0_1
Published:
Publisher Name: Springer, New York, NY
Print ISBN: 978-1-4939-7245-6
Online ISBN: 978-1-4939-7247-0
eBook Packages: MedicineMedicine (R0)