
Abstract
Aging enhances muscle desaturation responses due to reduced O2 supply. Even though aerobic training enhances muscle desaturation responses in young subjects, it is unclear whether the same is true in elderly subjects. Ten elderly women (age: 62 ± 4 years) participated in 12-weeks of cycling exercise training. Training consisted of 30 min cycling exercise at the lactate threshold. The subjects exercised 15 ± 6 sessions during training. Before and after endurance training, the subjects performed ramp cycling exercise. Muscle O2 saturation (SmO2) was measured at the vastus lateralis by near infrared spectroscopy during the exercise. There were no significant differences in SmO2 between before and after training. Nevertheless, changes in peak pulmonary O2 uptake were significantly negatively related to changes in SmO2 (r = −0.67, p < 0.05) after training. Muscle desaturation was not enhanced by low volume aerobic training in this study, possibly because the training volume was too low. However, our findings suggest that aerobic training may potentially enhance muscle desaturation at peak exercise in elderly subjects.
Access provided by Autonomous University of Puebla. Download conference paper PDF
Similar content being viewed by others


Keywords
1 Introduction
Muscle desaturation responses during whole-body exercise can be measured by near infrared spatial resolved spectroscopy (NIRSRS), which has been widely utilized in many previous studies [1, 2]. However, few previous studies have evaluated the effects of exercise training on muscle desaturation responses using NIRSRS during cycling exercise. A previous study found that aerobic exercise training enhances muscle desaturation during incremental cycling exercise in young subjects [1]. In another study, muscle desaturation responses were found to be enhanced in elderly subjects because muscle blood flow (i.e. O2 supply to exercising muscle) was reduced due to aging [2]. In view of that, it is unclear whether aerobic exercise training enhances muscle desaturation responses in elderly subjects. The aim of this study was to examine the effects of aerobic exercise training on muscle O2 dynamics in elderly subjects.
2 Methods
2.1 Subjects
Untrained elderly women (n = 10; age: 65 ± 2 years; height: 158.6 ± 8.0 cm; weight: 62.1 ± 11.9 kg, mean ± SD) participated in the study. This study protocol was approved by the institutional ethics committee, and was conducted in accordance with the Declaration of Helsinki. Two subjects were taking a statin, and one subject was taking an angiotensin II receptor antagonist and a calcium channel blocker. All subjects were informed of the purpose and nature of the study and written informed consent was obtained.
2.2 Experimental Design
The subjects performed 12-weeks of cycling exercise training for 30 min at the individual’s estimated lactate threshold (LT). Estimated LT was determined as previous studies had reported [3, 4]. Training frequency was set at two exercise sessions/week for 12 weeks.
Before and after exercise training, the subjects performed 10 or 15 W/min ramp cycling exercise until exhaustion (Strength Ergo 8, Fukuda-Denshi, Japan). Pulmonary O2 uptake (VO2) was monitored continuously during the experiments to determine peak VO2 by using an automated gas analysis system (AE300S, Minato Medical Science, Japan).
Muscle O2 saturation (SmO2) and relative changes from rest in oxygenated hemoglobin concentration (ΔOxy-Hb), deoxygenated hemoglobin concentration (ΔDeoxy-Hb), and total hemoglobin concentration (ΔTotal-Hb) were measured at vastus lateralis (VL) in the left leg by NIRSRS (Astem Co., Japan). The probe consisted of one light source and two photodiode detectors, and the distances between light source and detector were 20 and 30 mm, respectively. The data sampling rate was 1 Hz. The obtained signals were defined as the values averaged over the last 10 s. Changes in SmO2 were calculated as SmO2 at peak exercise before training subtracted from SmO2 at peak exercise after training. Although fat layer thickness affects NIRSRS data because of light scattering, Niwayama et al. have recently reported that the effects of fat layer thickness can be corrected in relative changes in Hb and SmO2 [5]. The corrected relative changes in Hb were obtained by dividing the measured values by the normalized optical path length for muscle (Smuscle; when the fat layer thickness is zero), and the value of Smuscle can be calculated by only fat layer thickness. For the calculations of SmO2, the measurements using NIRSRS can be corrected by using the appropriate curve plotting the spatial slope of light intensity and absorption coefficient of the muscle for fat layer thickness. In this study, we measured fat layer thickness at each measurement site in VL muscles with an ultrasound device (LogiQ3, GE-Yokokawa Medical Systems, Japan). Then, we calculated the muscle O2 dynamics with correction for light scattering effects. The specifications of correction for the influence of fat layer thickness have been fully described [5]. Even though an upper limit of fat layer thickness was designated as 10 mm to correct for the effects in this study, fat layer thickness was within ~10 mm at each measurement site in all subjects.
2.3 Statistics
All data are given as means ± standard deviation (SD). To compare changes in NIRS variables during exercise between groups, a 2-way repeated-measures analysis of variance was used with training and power output as factors. Where appropriate, the Bonferroni post hoc test was conducted. Because one subject could not exercise at more than 59 W before training, repeated measures between groups were limited to rest, 20, 30, 40, and 50 W compared as a function of power output. Differences in NIRSRS and cardiorespiratory variables at peak exercise were compared between groups using paired t tests. Pearson’s correlation coefficient was employed to determine the relationship between variables. For all statistical analyses, significance was accepted at p < 0.05.
3 Results
Even though training frequency was set at two exercise sessions/week for 12 weeks, unfortunately, the subjects exercised 15 ± 6 sessions during 12 weeks training as their schedules permitted. Estimated LT was significantly increased after training (before: 12.8 ± 3.1 ml/kg/min, after: 14.0 ± 2.1 ml/kg/min, p < 0.05), while peak VO2 was not significantly increased (before: 20.1 ± 6.0 ml/kg/min, after: 21.1 ± 4.1 ml/kg/min, p = 0.28). Similarly, workload at estimated LT was significantly improved after training than before (before: 54 ± 15 W, after: 62 ± 16 W, p < 0.05), even though peak workload was not significantly increased (before: 98 ± 30 W, after: 101 ± 30 W, p = 0.44). Fat layer thickness was not significantly altered after training than before (7.41 ± 2.67 vs. 7.14 ± 2.67 mm, p = 0.29).
During submaximal exercise, there were no significant training × power output interactions for SmO2 (p = 0.82), ΔOxy-Hb (p = 0.46), ΔDeoxy-Hb (p = 0.23), or ΔTotal-Hb (p = 0.29) between before and after training in all subjects. Moreover, no significant main effect for training was observed in SmO2 (p = 0.75), ΔOxy-Hb (p = 0.61), ΔDeoxy-Hb (p = 0.48), or ΔTotal-Hb (p = 0.50). Also at peak exercise, no significant difference was found in SmO2 (p = 0.90), ΔOxy-Hb (p = 0.26), ΔDeoxy-Hb (p = 0.20), or ΔTotal-Hb (p = 0.17) (Fig. 8.1).


Change in muscle O2 saturation (SmO2: a), oxygenated hemoglobin (oxy-Hb: b), deoxygenated hemoglobin (deoxy-Hb: c), and total hemoglobin (total-Hb: d) responses in vastus lateralis muscles during ramp cycling exercise before (closed circles) and after (open circles) exercise training
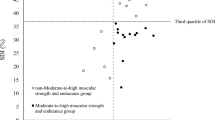
Improvement of peak VO2 by exercise training was significantly positively related to the number of sessions of training (r = 0.66, p < 0.05) and negatively related to changes in SmO2 (r = −0.67, p < 0.05) (Fig. 8.2). In addition, changes in ΔOxy-Hb (r = −0.76, p < 0.05) and ΔTotal-Hb (r = −0.66, p < 0.05) were significantly negatively associated with improvement of peak VO2. Similarly, changes in ΔOxy-Hb (r = −0.84, p < 0.01) and ΔTotal-Hb (r = −0.73, p < 0.05) were significantly negatively associated with the number of sessions of training. However, ΔDeoxy-Hb was not significantly related to peak VO2 (r = 0.05, p = 0.88) or training frequency (r = 0.09, p = 0.80).


Relationship between change in muscle O2 saturation at peak exercise (values at after training minus values at before training) and improvement of peak VO2 after aerobic exercise training
4 Discussion
In the present study, muscle desaturation during submaximal and peak exercise was not significantly changed by aerobic training. One possible interpretation may be that training volume was too low when compared to previous studies [1, 6]. Some previous studies demonstrated that peak VO2 was significantly related to muscle desaturation responses in cross-sectional observation [7, 8]. In fact, in this study, peak VO2 was not significantly increased by exercise training, and the number of training sessions was positively related to changes in peak VO2 after training. These results suggest that no significant difference in muscle desaturation were observed in this study due to low volume exercise training. Another possibility to explain the lack of significant difference in muscle desaturation after aerobic training may be the subjects’ characteristics. Previous studies reported that aerobic training enhanced muscle desaturation in healthy young subjects [1] and heart disease patients [6]. However, to our knowledge, there have been no published reports on effects of aerobic training on muscle deoxygenation responses in elderly subjects. This area warrants further investigation.
We also observed a significant negative relationship between improvement of peak VO2 and changes in SmO2 at peak exercise after exercise training, even though muscle desaturation was not largely enhanced after training in all elderly subjects. In addition, the number of training sessions was significantly positively related to improvement of peak VO2 and negatively related to changes in SmO2 at peak exercise. These findings lead us to speculate that aerobic training may potentially enhance muscle desaturation responses at peak exercise in elderly subjects.
Remarkably, there were significant relationships between enhancement of peak VO2 and decreases in ΔOxy-Hb or ΔTotal-Hb after exercise training, while changes in ΔDeoxy-Hb were not significantly associated with improvement of peak VO2. ΔOxy-Hb is an indicator of the balance between O2 supply and O2 utilization, and ΔTotal-Hb is indicator of blood volume. Additionally, muscle O2 supply is also affected by mechanical stress [9]. In fact, in this study, increased peak workload by training was also significantly negatively related to changes in ΔOxy-Hb (r = −0.63, p < 0.05) or ΔTotal-Hb (r = −0.64, p < 0.05) by training. These data suggest that the change in muscle desaturation at peak exercise after low volume exercise training may have been mainly due to reduced O2 supply, secondary to increased mechanical stress, such as intramuscular pressure.
In summary, muscle desaturation was not enhanced by low volume aerobic training in this study, possibly because the training volume was too low. However, there were significant relationships between change in SmO2, improvement of peak VO2 and the number of sessions. These results suggest that aerobic training may potentially enhance muscle desaturation responses at peak exercise in elderly subjects. However, in this study, the change in muscle desaturation at peak exercise may have been mainly due to reduced O2 supply, secondary to increased mechanical stress, such as intramuscular pressure.
References
Kime R, Niwayama M, Fujioka M et al (2010) Unchanged muscle deoxygenation heterogeneity during bicycle exercise after 6 weeks of endurance training. Adv Exp Med Biol 662:353–358
Takagi S, Kime R, Murase N et al (2013) Aging affects spatial distribution of leg muscle oxygen saturation during ramp cycling exercise. Adv Exp Med Biol 789:157–162
Beaver WL, Wasserman K, Whipp BJ (1986) A new method for detecting anaerobic threshold by gas exchange. J Appl Physiol 60(6):2020–2027
Wasserman K, Whipp BJ, Koyl SN (1973) Anaerobic threshold and respiratory gas exchange during exercise. J Appl Physiol 35(2):236–243
Niwayama M, Suzuki H, Yamashita T et al (2012) Error factors in oxygenation measurement using continuous wave and spatially resolved near-infrared spectroscopy. J Jpn Coll Angiol 52:211–215
Mezzani A, Grassi B, Jones AM et al (2013) Speeding of pulmonary VO2 on-kinetics by light-to-moderate-intensity aerobic exercise training in chronic heart failure: clinical and pathophysiological correlates. Int J Cardiol 167(5):2189–2195
Kime R, Osada T, Shiroishi K et al (2006) Muscle oxygenation heterogeneity in a single muscle at rest and during bicycle exercise. Jpn J Phys Fit Sports Med 55(Suppl):S19–S22
Takagi S, Murase N, Kime R et al (2014) Skeletal muscle deoxygenation abnormalities in early post myocardial infarction. Med Sci Sports Exerc 46(11):2062–2069 doi:10.1249/MSS.0000000000000334
Saltin B, Radegran G, Koskolou MD et al (1998) Skeletal muscle blood flow in humans and its regulation during exercise. Acta Physiol Scand 162:421–436
Acknowledgments
The authors are grateful for revision of this manuscript by Andrea Hope. This study was supported in part by Grant-in-Aid for scientific research from Japan Society for the Promotion of Science (246298) to S.T. and Waseda University Grant for Special Research Projects (2014S-148) to S.T.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2016 Springer Science+Business Media, New York
About this paper
Cite this paper
Takagi, S., Kime, R., Murase, N., Niwayama, M., Osada, T., Katsumura, T. (2016). Effects of Low Volume Aerobic Training on Muscle Desaturation During Exercise in Elderly Subjects. In: Elwell, C.E., Leung, T.S., Harrison, D.K. (eds) Oxygen Transport to Tissue XXXVII. Advances in Experimental Medicine and Biology, vol 876. Springer, New York, NY. https://doi.org/10.1007/978-1-4939-3023-4_8
Download citation
DOI: https://doi.org/10.1007/978-1-4939-3023-4_8
Publisher Name: Springer, New York, NY
Print ISBN: 978-1-4939-3022-7
Online ISBN: 978-1-4939-3023-4
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)