
Abstract
The family Bunyaviridae is one of the largest and most diverse of all viral families. It is comprised of viruses with negative-sense RNA genomes that produce enveloped spherical virions measuring 80–120 nm in diameter. All bunyavirus genomes consist of three segments (S, M, L), but they differ in their coding strategies to generate structural and nonstructural proteins. Virus replication occurs in the cytoplasm of infected cells, and virus particles mature inside the cell by budding primarily at the membranes of the Golgi apparatus. The family has over 400 member viruses that are classified predominantly into five genera: Hantavirus, Nairovirus, Orthobunyavirus, Phlebovirus, and Tospovirus. Bunyaviruses are distributed worldwide and infect vertebrate and invertebrate animals and plants. Viruses are transmitted by infected vectors, including mosquitoes, ticks, sandflies, thrips, rodents, eulipotyphla, and bats. Infections in humans lead to a variety of illnesses ranging from mild febrile syndromes to severe respiratory illnesses or fatal hemorrhagic fevers and encephalitides. Some bunyaviruses cause disease in domestic animals and plants that result in significant economic losses. In many areas of the world, new disease syndromes caused by bunyaviruses are being characterized. In addition, with the use of new technologies for virus discovery, new bunyaviruses are continuing to be identified in new arthropod vectors and reservoir hosts, and it is likely this trend will continue into the future.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
FormalPara Core MessageThe family Bunyaviridae is one of the largest and most diverse of the established viral families. Viruses within this family infect a wide range of organisms including invertebrates, vertebrates, and plants. Bunyaviruses are transmitted by mammals or arthropods, including ticks, mosquitoes, biting midges, sandflies, and thrips. Some viruses within this family are important pathogens causing encephalitis or hemorrhagic fever in humans, abortions in pregnant animals, or devastating disease in economically important plants.
1 Introduction
The large family Bunyaviridae includes more than 400 distinct members (bunyaviruses) that are grouped into five genera—Hantavirus, Nairovirus, Orthobunyavirus, Phlebovirus, and Tospovirus. Bunyaviruses possess a tripartite, single-stranded RNA genome that encodes four structural and, in some cases, one or two additional nonstructural proteins in a mostly negative-sense (i.e., anti-message) manner. Exemplifying the great diversity of the family Bunyaviridae, viruses in this family are known to infect invertebrates, vertebrates, and plants. Indeed, most viruses of the family are arthropod-borne, and various mosquitoes, ticks, biting flies, and thrips are vectors for transmission of orthobunyaviruses, nairoviruses, phleboviruses, and tospoviruses, respectively. Small mammals serve as amplifying hosts for most bunyaviruses, although some members (hantaviruses) use small mammal reservoirs and are transmitted via aerosolized excreta. Bunyaviruses have a worldwide geographic distribution, and some of these viruses are associated with significant human illnesses, including encephalitides and viral hemorrhagic fevers. Other bunyaviruses cause diseases in domestic animals and plants that are associated with significant economic impact.
2 History and Classification
Undoubtedly, many bunyaviral diseases were known long before viruses were discovered in the late nineteenth century. As far back as 960 A.D., the Chinese described illnesses closely resembling hemorrhagic fever with renal syndrome (HFRS) [1, 2], which is now known to be caused by certain hantaviruses. During the Napoleonic Wars (1803–1815), soldiers suffered from an epidemic of febrile illness, named Mediterranean fever that had symptoms similar to sandfly fever [3] that is caused by a phlebovirus. Sandfly fever was first clinically described by Alois Pick in 1886 in the Balkans region where the disease was prevalent in an endemic form [4].
In 1943, Smithburn and colleagues initially isolated Bunyamwera virus from Aedes mosquitoes during studies of yellow fever in Uganda [5] that is now classified in the genus Orthobunyavirus. Early classification of arboviruses (arthropod-borne viruses) relied mostly on serological relatedness, using methods such as complement fixation and neutralization tests. By 1960, eastern equine encephalitis virus, western equine encephalitis virus, and certain other viruses were known to be related to each other and were referred to as group A arboviruses (which are now classified in the genus Alphavirus in the family Togaviridae). Japanese encephalitis virus, yellow fever virus, St. Louis encephalitis virus, West Nile virus, and certain other viruses were also known to be related to each other and were referred to as group B arboviruses (which are now classified in the family Flaviviridae). Following the isolation of Bunyamwera virus, several other arboviruses were isolated that clearly did not fit into these two antigenic groups. These viruses were subsequently assigned to what became known as the group C arboviruses [6]. The family Bunyaviridae was formally established in 1975 to incorporate this group [7], and its members are now grouped into five genera—Hantavirus, Nairovirus, Orthobunyavirus, Phlebovirus, and Tospovirus. Viruses in all genera infect vertebrates, except for those in the genus Tospovirus, which infect plants [8].
3 Physical Properties
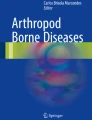
Bunyavirion morphology varies among viruses of each of the five genera; however, virions are generally spherical, 80–120 nm in diameter, and possess surface glycoprotein projections of 5–10 nm. These peplomers are embedded in a lipid bilayered envelope approximately 5 nm thick and are thought to mostly consist of heterodimers of the two viral glycoproteins (Fig. 10.1). The previous designations of these glycoproteins, G1 and G2, were based on their relative migration in polyacrylamide gels. Today, these proteins are referred to as Gn and Gc, referring to the amino-terminal and carboxy-terminal coding of the proteins [9]. Orthobunyavirions have surfaces covered with closely packed, knob-like morphologic units with no detectable order. Similarly, no obvious order is found for the small surface structures with central cavities observed on nairovirions [10]. In contrast, hantavirions have a surface structure that is distinctly ordered in a square grid-like pattern [10]. Phlebovirions have round, closely packed subunits approximately 10–11 nm in diameter with central cavities approximately 5 nm in diameter [10]. The appearances of tospovirions are similar to those of nairovirions in which, other than the presence of glycoprotein spikes, distinctive surface structures have not been observed.

Schematic enveloped, spherical bunyavirion, 80–120 nm diameter. Image courtesy of ViralZone, SIB Swiss Institute of Bioinformatics, with permission
Bunyavirions consist of 2 % RNA, 58 % protein, 33 % lipid, and 7 % carbohydrate (estimated for Uukuniemi virus of the genus Phlebovirus) and are sensitive to heat, lipid solvents, detergents, and formaldehyde [11]. Treatment with lipid solvents or detergents removes the viral envelope, resulting in loss of infectivity in arthropods and mammals [11]. Interestingly, however, the envelope is not required for viral entry or replication in plant cells of the plant-infecting tomato spotted wilt virus [12].
4 Genome Structure
The bunyaviral genome comprises three segments of negative or ambisense single-stranded RNA designated as small (S), medium (M), and large (L). The lengths of the genomic segments vary among the genera, with the total genome lengths of approximately 11–19 kb (Table 10.1). The 3′ and 5′ terminal nucleotides of each genomic segment are highly conserved among viruses of a given genus, but differ among viruses of different genera (Table 10.2). Stretches of the 3′ and 5′ termini are complementary. Thus, the termini of each segment base-pair, forming noncovalently closed, panhandle-like RNAs. Direct support for base-pairing comes from electron microscopy studies of extracted RNA from Uukuniemi virions, in which three sizes of circular RNAs are evident [13].
5 Protein Coding and Viral Replication Strategies
The S, M, and L genome segments of all bunyaviruses encode a nucleocapsid protein (N), two envelope glycoproteins (Gn and Gc), and an RNA-dependent RNA polymerase (L), respectively (Fig. 10.2).

Genome organization of viruses of the five bunyavirus genera. Structural proteins are N (nucleocapsid) and the two viral glycoproteins, Gn and Gc, named according to their proximity to the N or C termini of the precursor polyprotein, respectively. The L protein possesses RNA-dependent RNA polymerase activity. Virus abbreviations: BUNV Bunyamwera virus, CCHFV Crimean-Congo hemorrhagic fever virus, HTNV Hantaan virus, RVFV Rift Valley fever virus, TSWV tomato spotted wilt virus
The S segment is approximately 1.0–3.0 kb and has one open reading frame (ORF) in the negative-sense orientation that codes for N. N is the most abundant component of virions and viral product in infected cells. N plays several important roles in viral replication, including protecting the RNA from degradation. The S segment of the orthobunyaviruses encodes for both the N protein and a nonstructural (NS)s protein in overlapping reading frames. Likewise, some hantavirus genomes have an ORF within the N ORF, and an NSs protein has been detected in cells infected with some hantaviruses [14, 15].
A single, continuous ORF in the M RNA segment encodes the polyprotein precursor of the glycoproteins, which is co-translationally cleaved by a cellular protease into mature Gn and Gc. The M segment of nairoviruses is 30–50 % larger than M segments of viruses of the other genera and has the coding potential of up to 240 kDa of protein [16]. The M segment of Crimean-Congo hemorrhagic fever virus (CCHFV) encodes a precursor Gn (preGn) that undergoes posttranslational cleavage to two proteins of unknown functions, a mucin-rich protein, and glycoprotein GP38 [17]. The M segments of some bunyaviruses (but not those of hantaviruses) also encode a NSm protein. NSm is encoded in negative-sense orientation in the case of orthobunyaviruses and phleboviruses, but in positive-sense orientation in the case of tospoviruses. The nairovirus CCHFV also encodes NSm [18]. This integral membrane protein is cleaved off from the C-terminal region of preGn and is detected in cells infected with CCHFV, but not in virion pellets [18]. The function of this protein is currently unknown. In fact, the only M segment NS protein to have a defined role is the NSm of tospoviruses, which aids viral cell-to-cell movement (see below). The L segment uses a conventional negative-sense (i.e., complementary to mRNA) coding strategy.
The bunyaviral L segments encode the RNA-dependent RNA polymerase (L). Hantaviral, orthobunyaviral, and phleboviral L is of similar mass ≈250 kDa, whereas tospoviral and nairoviral L is considerably larger (330 kDa and 450 kDa, respectively) (Table 10.3).
Bunyavirions gain entry into host cells by mechanisms similar to many other enveloped viruses. The viral glycoproteins, Gn and Gc, are primarily responsible for attachment to host cells and fusion with cellular membranes. Attachment to the host cell is followed by virion endocytosis. Most bunyaviruses assemble and bud into the Golgi apparatus (visualized by electron microscopy in the case of Bunyamwera virus) [19]. After budding into the Golgi cisternae, maturing virions are transported to the plasma membrane in small vesicles. By a process that resembles normal exocytosis, virion release occurs after fusion of the vesicles with the plasma membrane [20].
6 Ecology and Epidemiology
6.1 Orthobunyaviruses
The genus Orthobunyavirus includes ≈53 species and contains more than 193 viruses. Most of these viruses are grouped into ≈20 serogroups based on antigenic relationships (Table 10.4) [8, 21]. The vast majority of the viruses are vectored by mosquitoes; however, some orthobunyaviruses have culicoid flies (i.e., biting midges of the genus Culicoides) or ticks as vectors. These viruses are distributed worldwide; however, the majority of these viruses are not well studied. The exceptions are those viruses that have medical (e.g., La Crosse and Oropouche viruses) or veterinary importance (e.g., the newly emerged Schmallenberg virus).
La Crosse virus (LACV) is a member of the California serogroup and one of the most significant bunyaviruses in terms of causing human encephalitis. LACV is transmitted by its primary vector, the forest-dwelling, tree-hole-breeding mosquito Aedes triseriatus [22] (Fig. 10.3). This mosquito is found throughout the northern, midwestern, and northeastern USA. LACV is maintained in these mosquitoes by transovarial transmission, which allows overwintering of the virus in mosquito eggs [23]. Squirrels, chipmunks, foxes, and woodchucks often serve as amplifying reservoir hosts [24]. Most cases of La Crosse encephalitis occur in the summer and early fall when risk of being bitten by infected mosquitoes is highest. The majority of cases occur in the Mississippi and Ohio River basins with over 90 % of cases reported from Wisconsin, Minnesota, Iowa, Indiana, Ohio, and Illinois; however, cases also occur throughout most of the eastern half of the USA (Fig. 10.4).

Aedes triseriatus, commonly known as the “treehole mosquito,” obtaining a blood meal from a human hand (courtesy of James Gathany, obtained from the Centers for Disease Control and Prevention (CDC) Public Health Image Library at http://phil.cdc.gov/phil/home.asp [accessed Feb 25, 2014])

Most reported cases of California serogroup virus neuroinvasive disease (encephalitides, meningoencephalitides, or meningitides) are due to La Crosse virus (LACV). Counties are shaded according to incidence ranging from less than 0.06, 0.06–0.99, and greater than 1.00 per 100,000. Most of the counties with the highest incidence are located along the Appalachian range and the upper Mississippi River basin (Obtained from the CDC website at http://www.cdc.gov/lac/tech/epi.html [accessed Feb 25, 2014])
Oropouche virus (OROV) was first identified from Trinidad in 1955 [25] and was later isolated from the blood of a pale-throated sloth (Bradypus tridactylus) in 1960 [26]. Recently, OROV has become the second most frequent cause of arboviral infection in Brazil, surpassed only by dengue viruses [26]. OROV has been associated with large and explosive outbreaks of febrile disease in South and Central America, especially in the Amazon Basin. More than half a million cases have been reported in the Americas [26]. In addition to outbreaks, OROV can also cause sporadic human infections [27]. OROV is transmitted to sloths, marsupials, primates, and birds by Aedes serratus and Culex quinquefasciatus mosquitoes. Notably, OROV has adapted to an urban cycle involving man, with biting midges (Culicoides paraensis) as the primary vector [28, 29].
In addition to human pathogens, the genus Orthobunyavirus also contains pathogens of significant veterinary importance. One example is the recently emerged Schmallenberg virus (SBV). In late 2011, a nonspecific febrile syndrome occurred in dairy cattle that was characterized by decreased milk production and watery diarrhea [30]. The affected farms were located along the German-Dutch boarder in North Rhine-Westphalia, near the city of Schmallenberg, Germany. Next-generation sequencing and metagenomic analysis was used to identify the novel orthobunyavirus from blood samples of deceased cows from a farm in Schmallenberg [30]. Since the first detection in Germany, SBV has spread rapidly over large parts of northern and western Europe (Fig. 10.5). In addition to the febrile syndrome initially described for the virus, transplacental infection often results in the birth of malformed calves, lambs, and goat kids [31, 32]. Based on similarities to other related viruses affecting livestock, researchers suspected that Schmallenberg virus was transmitted by biting midges (Culicoides). In fact, several studies have detected the virus in field-collected midges [33–36], and viral replication and dissemination in C. sonorensis midges have been observed under laboratory conditions [37]. Interestingly, SBV appears to be a reassortant virus, with the M segment from Sathuperi virus and the S and L segments from Shamonda virus, both members of the Simbu serogroup of orthobunyaviruses [38].

Distribution of Schmallenberg virus by country in Europe as of February 2013 (courtesy of O. Smooth, obtained at http://en.wikipedia.org/wiki/Schmallenberg_virus [accessed Feb 27, 2014])
6.2 Nairoviruses
The genus Nairovirus includes ≈50 predominantly tick-borne viruses in eight established and four proposed species [39, 40] (Table 10.5). The pathogenicity of many of these viruses is not known. However, two nairoviruses are known to be serious pathogens: Crimean-Congo hemorrhagic fever virus (CCHFV) and Nairobi sheep disease virus (NSDV). CCHFV causes severe hemorrhagic fever in humans, and NSDV causes severe gastroenteritis in sheep and goats. Case-fatality rates of infections with either virus can reach 90 % [41, 42]. CCHF is the most widespread tick-borne viral infection of humans, occurring across a vast area including western China through Southern Asia, the Middle East to southeastern Europe, and most of Africa [43]. CCHFV is maintained through vertical and horizontal transmission in ixodid (hard) ticks of several genera, which spread the virus to a variety of wild and domestic mammals. Affected mammals develop transient viremia without signs of illness. Human infections occur through tick bite or exposure to the blood or other body fluids from infected animals or humans. Ticks of the genus Hyalomma (Fig. 10.6) are the principal source of human infection, probably because both the immature and the adult forms of the tick actively seek hosts for their obligate blood meals. Of note, during a recent viral metagenomics study, novel nairovirus sequences were detected in France in bats belonging to two different species [44]. These sequences diverge significantly from all known nairovirus genomes and thus represent a new nairovirus, Ahun virus, which will probably to be assigned to a novel species.

Hyalomma marginatum rufipes tick, a known vector of Crimean-Congo hemorrhagic fever. This specimen was collected from Kenya and has the characteristic banded coloration pattern on the legs, typical of Hyalomma ticks (courtesy of Alan R. Walker, obtained at http://en.wikipedia.org/wiki/Ticks_of_domestic_animals [accessed Feb 26, 2014])
6.3 Hantaviruses
The Hantavirus genus contains 36 viruses classified into 24 species and an additional ≈67 unclassified viruses (Table 10.6). Unlike all other members of the family Bunyaviridae, hantaviruses are not arboviruses, but infect rodents, eulipotyphla (shrews and moles), and bats [45]. Human hantavirus infection is thought to occur following exposure to excretions from infected mammalian hosts. Researchers generally agree that hantaviruses have co-evolved with their hosts over the course of several hundreds of thousands to millions of years [46]. Phylogenetic trees visualize that most hantaviruses clearly group according to their mammalian hosts (Fig. 10.7) [47]. Rodent-borne hantaviruses form two basic lineages, Old World and New World, which primarily reflect the geographic distribution of their rodent hosts. Significant human pathogens among the Old World viruses include Hantaan, Seoul, Puumala, and Dobrava-Belgrade viruses, which cause HFRS. Hantaan virus, named after the Hantaan River in Korea, is the prototype hantavirus and was first isolated from the striped field mouse (Apodemus agrarius) in 1976 [48]. After this discovery, other related viruses were characterized and classified including Puumala virus from the bank vole (Myodes glareolus) [49], Seoul virus from brown and roof rats (Rattus norvegicus and R. rattus) [50], and Dobrava-Belgrade virus from the yellow-necked field mouse (Apodemus flavicollis) [51].

Phylogenetic tree based on the coding sequence of the S segments of hantavirus genomes showing coevolution with their mammalian reservoir hosts. Image modified from Guo et al. [47]
Hantaviruses were first recognized in the New World in 1982 (Prospect Hill virus) and then again in 1993 when Sin Nombre virus was identified as the causative agent of an outbreak of acute respiratory distress, today called hantavirus (cardio-)pulmonary syndrome (HCPS), in the Four Corners area of the US Southwest [52]. Sin Nombre virus (Fig. 10.8) was ultimately isolated from North American deermice (Peromyscus maniculatus), which were confirmed as the primary rodent reservoirs for this hantavirus [53]. Since the first detection of this Sin Nombre virus in the USA, numerous additional hantaviruses have been discovered throughout the Americas, some of which (e.g., Andes virus) are clearly pathogenic to humans and cause HCPS [54].

Transmission electron micrograph showing the ultrastructure of virions of the hantavirus Sin Nombre virus (courtesy of CDC/Brian W.J. Mahy and Luanne H. Elliott, obtained from CDC’s Public Health Image Library at http://phil.cdc.gov/phil/home.asp [accessed Feb 11, 2014])
Thottapalayam virus was isolated from an Asian house shrew in India in 1964 [55], but was not classified as a hantavirus until 1989 [56]. Since 2006, at least 26 new hantaviruses have been identified from eulipotyphla [8, 57]. In addition, more recently, hantaviruses have been identified in bats from diverse geographic locations, including Africa [58, 59] and Asia [47, 60]. Until now, none of the non-rodent-borne hantaviruses has been associated with disease.
6.4 Phleboviruses
The genus Phlebovirus includes ≈24 species and ≈115 viruses (Table 10.7) that can be classified based on their antigenic similarities, arthropod vectors, and the presence of an open reading frame in M segments coding for a non-structural protein. Phleboviruses are transmitted by arthropod vectors, namely, sandflies, mosquitoes, biting midges of the Culicoides genus, or ticks [8]. Infection of the vector is frequently persistent and lifelong. Within the vectors, the viruses multiply and spread transovarially (i.e., vertical transmission) and venereally (i.e., horizontal transmission) [61–63]. Generally, phleboviruses are specific with regard to arthropod vectors and vertebrate hosts. However, some phleboviruses infect multiple vectors, with several distinct phleboviruses using the same vectors. This multivirus infection provides considerable opportunity for reassortment of the genome segments and therefore results in the evolution of new viruses. The vertebrate hosts or reservoirs of most phleboviruses have not been characterized to date. However, the role of the amplifying hosts might be minimal or secondary in regard to the horizontal amplification of the viruses in vectors [64].
Phleboviruses occupy broad geographic and ecologic niches, defined by the distribution, host competency, and biological behavior of their vectors. Phleboviruses are endemic in Europe, Africa, Central Asia, and the Americas, and have even been found on a subantarctic island [65, 66]. There is considerable evidence that phlebovirus habitats, especially for sandfly-borne viruses and Rift Valley fever virus, are expanding, possibly due to climate change and thereby changing ranges of vectors [64, 67].
Sandfly-borne phleboviruses are transmitted by the sandflies in the family Psychodidae, which are present in the warm zones of Asia, Africa, Australia, Southern Europe, and the Americas [68]. In the Old World (Figs. 10.9 and 10.10), the most important human pathogens are sandfly fever Sicilian virus (SFSV), sandfly fever Naples virus (SFNV), and Toscana virus (TOSV), all of which are transmitted by Phlebotomus sandflies and cause febrile disease [64]. The risk for phlebovirus exposure via sandflies is high in populations residing in regions south and east of the Mediterranean Sea [64]. Little is known about the epidemiology of sandfly-borne phleboviruses of the New World that are transmitted by Lutzomyia sandflies. Several viruses, such as Alenquer, Candiru, Chagres, E(s)charate, Morumbi, Punta Toro, and Serra Norte viruses, were isolated from humans with clinical febrile disease in Brazil, Panama, Columbia, Peru, and regions of northern South America. The phleboviral diseases of tropical America are probably associated with rodents living in forests that may act as amplifying hosts [69, 70].

Phlebotomus papatasi sandfly, a known vector of sandfly fever Naples and sandfly fever Sicilian viruses, taking a blood meal (photo courtesy of CDC/James Gathany, obtained from CDC’s Public Health Image Library at http://phil.cdc.gov/phil/home.asp [accessed March 18, 2014])

Transmission electron micrograph of virions of the phlebovirus sandfly fever Turkey virus (50,000× magnification, courtesy of Dr. Stefan Frey, Bundeswehr Institute of Microbiology, Munich, Germany)
Transmission of sandfly-borne phleboviruses to susceptible humans and animals occurs during the blood meal of female sandflies, which are the primary reservoirs for these viruses [64, 65]. Vertical and horizontal transmissions, demonstrated experimentally and in natural habitats, are contributing mechanisms that assure long-term maintenance of phleboviruses in these vectors [71]; however, the exact role and efficiency of these mechanisms in the transmission cycles of various phleboviruses have not been fully explored. Researchers generally agree that humans or other large vertebrates are dead-end hosts that do not participate in the natural virus transmission cycle. Horizontal transmission among infected vertebrates does not occur. Toscana virus was isolated from a Kuhl’s pipistrelle (Pipistrellus kuhli) in Italy [72], but the role of bats in virus circulation remains clear. Direct aerosol or parenteral transmission of sandfly-borne phleboviruses has not been demonstrated.
Rift Valley fever virus (RVFV) is the best characterized mosquito-borne phlebovirus. RVFV is the causative agent of Rift Valley fever (RVF), an acute disease of domestic ruminants characterized by deaths of newborn animals and abortion in pregnant sheep, goats, and cattle. RVF was initially described in British Kenya in 1931 [73]. The disease is endemic in sub-Saharan Africa and has caused major outbreaks in several African countries including Egypt, Kenya, Madagascar, Mauritania, Tanzania, Senegal, Somalia, South Africa, and Sudan [74, 75]. The largest human epidemic occurred in Egypt in 1977–1978, when there were an estimated 200,000 human infections, with some 18,000 cases of illness and 600 deaths. In 2000, an outbreak occurred in Saudi Arabia and Yemen, the first outbreak occurring outside of Africa. This outbreak raises concern that the disease could spread further into Asia or Europe, or even to the Western Hemisphere where susceptible mosquitoes may be present [76, 77]. In its enzootic regions, RVFV persists in the environment through vertical transmission in mosquitoes and horizontal transmission by mosquitoes among domestic and wild herbivores, including cattle, buffalo, sheep, and goats. The principal hosts for RVFV have not been identified but presumably involve native ungulates and rodents [76, 78]. Bats can also be infected experimentally [79]. RVFV may replicate in a number of potential vectors, including ticks and a variety of flies [80–82]. However, various mosquitoes, including Aedes and Culex mosquitoes, are the main arthropod vectors in the natural environment [77]. RVFV is transmitted to vertebrates by the bites of infected mosquitoes or by direct contact with infected tissues, blood, body fluids, and fomites, particularly if associated with abortions. Aborted materials and placental membranes contain high numbers of virions, which can either contaminate the local environment or infect animals or humans in close contact. In vitro experiments have described the relatively long-term persistence of RVFV in the environment [77, 83]. Because of this persistence and the potential for aerosol transmission, biosafety level 3/4 laboratory conditions are recommended for handling the virus. Due to habitat expansion of competent vectors, increases in live animal trade, and impact of climatic and environmental changes, the risk of an introduction of RVFV into naive zones and preparedness for a probable emergence have been considered by several national and international agencies [77, 84].
Tick-borne phleboviruses [8] are transmitted via competent hematophagous hard (ixodid) or soft (argasid) ticks to various warm-blooded vertebrates [51]. Uukuniemi virus (UUKV) is the prototype tick-borne phlebovirus in the Old World and was originally isolated from a pool of Ixodes ricinus ticks collected in southern Finland [85]. Subsequently, UUKV was detected in Scandinavia and central and Eastern Europe and from Azerbaijan in Central Asia. Vertebrate hosts for UUKV are forest rodents (e.g., bank voles) and ground-feeding passerine birds [86]. Serological surveys suggest that humans have been exposed to UUKV without serious consequences. In fact, other than UUKV, which has been associated with a self-limiting acute febrile disease in individuals from southern Russia, no human illness has been reported with the other Uukuniemi group viruses [86, 87].
Bhanja virus (BHAV) is another tick-borne phlebovirus that was initially isolated from Haemaphysalis intermedia ticks collected from a paralyzed goat in India. BHAV has subsequently been isolated in Europe and Africa from ticks of several other species, domestic animals, and humans, and has been associated with febrile disease in domestic animals (sheep, goats, and cows) and meningoencephalitis in humans [86].
Novel tick-borne phleboviruses causing disease in humans have recently emerged in China and the USA. These include severe fever with thrombocytopenia syndrome virus (SFTSV; also known as Huaiyangshan virus or Henan fever virus) and Heartland virus [88–91]. SFTSV causes a severe and potentially fatal febrile illness with thrombocytopenia and hemorrhagic manifestations. SFTSV mainly occurs in the rural areas of eastern, central, and northeastern China, but SFTSV has also been reported from South Korea and Japan [92]. SFTSV has been detected in Haemaphysalis longicornis and Rhipicephalus microplus ticks collected in the endemic region of China [93]. A wide range of animals, including sheep, goats, cattle, pigs, dogs, chickens, and rodents have tested positive for antibodies against SFTSV [94]. Incidence of livestock infection was significantly higher than the incidence in poultry, humans, and rats, suggesting livestock might serve as amplifying hosts in human transmission. Heartland virus (HRTV) has been associated with human cases of severe febrile illness with thrombocytopenia after tick exposure in the central USA [88]. Ticks are implicated as potential vectors, as the virus was recently detected in field-collected Amblyomma americanum ticks [95]. Preliminary investigations also suggest exposure to HRTV or an antigenically similar virus in cattle, sheep, goats, deer, and elk [96]. Genetically, Bhanja group virus and its close relatives form a clade distinct from those of SFTSV/HRTV and UUKV.
7 Clinical Features of Human and Animal Bunyaviridae Infections
7.1 Orthobunyaviruses
At least 36 orthobunyaviruses have been associated with human disease (Table 10.4), causing a range of syndromes such as febrile illnesses, encephalitides, or hemorrhagic fevers. California serogroup viruses are important causes of disease among humans in the USA. For example, La Crosse virus (LACV) is a common cause of arboviral encephalitis in children in the midwestern USA, whereas Jamestown Canyon virus commonly causes encephalitis in adults [97]. The onset of illness is usually sudden and characterized by fever, headache, malaise, nausea, and vomiting. Within a few days, these signs and symptoms are accompanied by meningeal signs and lethargy. In severe forms, the disease may progress to seizures (approximately 50 %) and coma (about 10 %) [97]. The case-fatality rate is approximately 1 % or less, and the total duration of the illness rarely exceeds 2 weeks [97]. Most infected individuals do not experience neurologic sequelae. Other orthobunyaviruses (e.g., Cache Valley virus) cause abortion or teratogenic effects in pregnant livestock.
7.2 Nairoviruses
Crimean-Congo hemorrhagic fever virus (CCHFV) is the most important of the nairoviruses in terms of human disease [42, 43]. CCHFV infection can result in a severe hemorrhagic syndrome with a 5–30 % case-fatality rate. The course of the disease is divided into four phases: incubation period, prehemorrhagic phase, hemorrhagic phase, and convalescent phase. The length of the incubation period appears to depend in part on the mode of acquisition of virus. Following a tick bite, the incubation period ranges from 1 to 5 days, whereas it is usually 5–7 days (maximum 13 days) following contact with infected blood or tissues [98]. The prehemorrhagic phase begins as a sudden and nonspecific prodrome that is characterized by fever, myalgia, arthralgia, and lower back and abdominal pain [98]. In patients who progress to hemorrhagic signs, the start of the hemorrhagic phase is abrupt and begins approximately 3–6 days following the onset of signs and symptoms. Bleeding occurs at various sites, including the brain and respiratory, gastrointestinal, and urogenital tracts. At this phase, the most common manifestation is a petechial rash of the skin, conjunctivae, and other mucous membranes, which progresses to large cutaneous ecchymoses. In those patients who succumb to infection, death occurs approximately 6–10 days after the first signs and symptoms from irreversible shock (e.g., loss of blood pressure, elevated levels of proinflammatory cytokines, and disseminated intravascular coagulation) [98, 99]. In patients who survive CCHF, full recovery may take up to a year [98].
7.3 Hantaviruses
Hantavirus infections are associated with two clinical disorders in humans: HFRS and HCPS. HFRS is associated with Old World viruses (e.g., Hantaan, Seoul, Dobrava, and Puumala viruses), whereas, HCPS is associated with New World viruses (e.g., Sin Nombre and Andes viruses) (Table 10.6). In general, the severity of HFRS varies with the causative agent. HFRS caused by Hantaan and Dobrava viruses are more severe, while disease caused by Seoul virus is more moderate and disease caused by Puumala virus is mild (“nephropathia epidemica”). Hantaan virus-associated HFRS, which first came to the attention of western physicians during the Korean War, is among the most severe forms of HFRS, resulting in a case-fatality rate of 5–15 % [100]. Classically, the clinical course of HFRS occurs in five distinct phases. First, a febrile phase consists of headache, high fever, and chills. A hypotensive phase then follows during which blood platelet numbers drop and petechial hemorrhage can be observed. Abdominal pain and tachycardia are also observed during this stage. An oliguric phase may occur next in which decreased urine production, proteinuria and may progress to kidney failure. Urine production is then increased in the diuretic phase, which can last for months before the patient enters the convalescent phase and recovery [101].
In contrast, HCPS is a severe acute disease associated with a rapid onset of respiratory failure and cardiogenic shock [102]. HCPS bears some resemblance to HFRS except that the lungs are targeted for capillary leakage, instead of the kidneys [101]. As with HFRS, the clinical presentation and case-fatality rate depends on the etiological hantavirus [101]. The onset of HCPS in the Americas is generally characterized by nonspecific symptoms such as fever, myalgia, cough, gastrointestinal symptoms, chills, and headache. HCPS evolves rapidly (1–3 days) to a lung capillary leak syndrome, resulting in respiratory distress, followed by respiratory failure and then cardiogenic shock. These clinical signs are responsible for the majority of deaths (case-fatality rate up to 50 %) [100].
Although in general the Old World hantaviruses target the kidneys (resulting in HFRS) and New World hantaviruses target the lungs and heart (resulting in HCPS), this distinction is far from absolute. Indeed, controversy exists among hantavirologists whether the terms HFRS and HCPS should be abandoned in favor of the more generic single designation, “hantavirus fever” [103]. In the last few years, cases of hantavirus infection with divergent symptomatology have been reported. For example, cases of Puumala virus infection with pulmonary involvement were observed in Europe, and acute renal failure has been recognized in patients infected with New World hantaviruses [104, 105]. Similarly, in a recent study in China, investigators examined the clinical characteristics and outcome of 48 patients with HFRS who also had acute respiratory distress syndrome [106]. Patients in this study were in critical condition, with 21 succumbing to the disease (43.8 % case-fatality rate).
7.4 Phleboviruses
The best-known clinical condition associated with phleboviruses is a febrile illness known as sandfly fever (also known as phlebotomus, papatacci, or 3-day fever in the Old World). Sandfly fever is prevalent in the countries in the Mediterranean Basin, Northern Africa, and parts of Central, Western, and Southern Asia [65]. Cases and outbreaks of sandfly fever still occur in non-immune individuals in endemic regions [107, 108]. Sandfly fever has also been described as an important travel-related infection, and several cases of imported sandfly fever have been reported in patients following visits to endemic regions [107, 109]. Sandfly fever is characterized by high fever, headache, retroorbital pain, photophobia, generalized aches, malaise, and chills. Abdominal pain, discomfort, diarrhea, or constipation may also occur. The duration of fever is usually 2–4 days, but may be extended in some cases. Following the febrile stage, the affected patients frequently suffer from fatigue and weakness. Convalescence may require a few days to several weeks and can be incapacitating. The prognosis is favorable without any complications, sequelae, or lethality. In infected individuals, viral replication is controlled by the immune response. The immunity to sandfly fever phleboviruses is specific to the virus, and neutralizing antibodies produced during exposure are sufficient to suppress the occurence of symptoms upon rechallenge with homotypic agent [110, 111]. In the Old World, phleboviruses responsible for sandfly fever are sandfly fever Sicilian virus (SFSV) and sandfly fever Naples Virus (SFNV) [64, 110]. Regional SFSV variants, sandfly fever Cyprus virus (SFCV) and sandfly fever Turkey virus (SFTV), are also associated with the clinical picture of sandfly fever similar to that caused by SFSV and SFNV, but induce more prominent gastrointestinal symptoms, including elevation of hepatic enzymes and thrombocytopenia, with a more emphasized post-infectious asthenic syndrome [112–114]. In the New World, primarily Alenquer, Chagres, Candiru, and Punta Toro viruses have been detected in individuals with febrile diseases [61, 70]. Tick-borne Uukuniemi virus has also been identified in a limited number of cases of acute illness characterized by fever, headache, muscle and joint pain, facial hyperemia, and body rash [86, 87].Toscana virus (TOSV), another sandfly-borne phlebovirus, transmitted by the bites of Phlebotomus perniciosus and P. perfiliewi sandflies, is a significant human pathogen due to its distinct neurotropism, causing central nervous system infections in endemic regions around the Mediterranean Sea [115]. TOSV has been pinpointed as a major agent of seasonal aseptic meningitis or meningoencephalitis, especially occurring during spring-summer months when the activity of vectors increase. TOSV infection is also a travel-associated infection in individuals leaving endemic regions [115]. Similar to the other phleboviral infections, the majority of the TOSV exposures result in an asymptomatic seroconversion or subclinical infection. Clinical manifestations in symptomatic TOSV infections are frequently characterized by high fever, severe headache, myalgia, and neurological symptoms of cortical and/or meningeal involvement from which patients generally recover within 7–10 days [64, 110, 115]. Central nervous system involvement in most cases is associated with a favorable outcome, but severe and lethal infections have also been reported [116]. Moreover, a variety of clinical signs and symptoms including hydrocephalus, impaired speech, paresis, hearing loss, diffuse intravascular coagulation, myositis-fasciitis, and testicular manifestations have also been reported [116–120].
RVF is the clinical manifestation of infection with the mosquito-borne RVFV, affecting ruminant animals and humans. Outbreaks of RVF in ruminants are often recognized initially as an abortion storm in herds of pregnant animals. Sheep are the most susceptible mammals, while cattle, goats, and camels demonstrate variations in susceptibility. Forty to 100 % of pregnant RVFV-infected sheep abort, and the fetuses often have malformations [76]. Newborn lambs suffer from an acute disease, characterized by necrotic hepatitis with 95–100 % lethality. Some breeds of adult sheep also exhibit hemorrhagic signs, similar to those seen in humans. In humans, exposure to RVFV frequently remains asymptomatic. In those with clinical signs, the disease presents with an influenza-like febrile disease without complications. However, severe manifestations such as hepatitis, retinitis, encephalitis, and hemorrhagic disease have been observed in a small number of cases with RVF, with the overall case-fatality rate estimated to be between 0.5 and 2 % [77, 121].
Severe fever with thrombocytopenia syndrome (SFTS) is a recently described human clinical disease caused by the emerging tick-borne phlebovirus SFTSV [90]. The disease is characterized by high fever, fatigue, anorexia, vomiting, and diarrhea, as well as laboratory findings of thrombocytopenia, leukocytopenia, and elevation of certain serum enzymes, including alanine aminotransferase, aspartate aminotransferase, lactate dehydrogenase, creatine phosphokinase, and creatine kinase. The symptoms of SFTS frequently resolve after a week. However, in some cases, the patient’s condition progresses to multiorgan dysfunction, disseminated intravascular coagulation, shock, and/or acute respiratory distress syndrome, with neurologic and hemorrhagic manifestations [122, 123]. Case-fatality rates as high as 30 % have been reported [124]. HRTV infections present similar to SFTS. However, the prognosis is favorable, with no respiratory or kidney involvement or coagulation abnormalities [88].
8 General Features of Plant-Infecting Tospoviruses
Currently, 11 species are included in the genus Tospovirus, each of which has one member virus. Many other tospoviruses have yet to be classified into species (Table 10.8) [8]. Thrips of numerous species (Fig. 10.11) of the genera Frankliniella, Thrips, Scirtothrips, and Ceratothripoides have been reported to transmit tospoviruses to a wide variety of plant species [8]. Transmission can also occur by mechanical means via infected plant sap. Tomato spotted wilt virus (TSWV) is the prototype tospovirus, and, contrary to its name, has a broad host range with susceptible plants belonging to more than 925 species of 70 botanical families [8]. Spotted wilt disease of tomato was first described in 1915 in Australia. The disease was later shown to be transmitted by thrips and caused by TSWV in 1930 [125]. The worldwide dispersal in the 1980s of the western flower thrip (Frankliniella occidentalis), a major vector of TSWV, led to a reemergence of the disease. By 1994, worldwide losses of tomato were estimated to be in excess of US $1 billion annually [126]. In addition to tomatoes, other economically important plants affected by TSWV include peppers, lettuce, peanuts, and chrysanthemums [127]. Tospoviruses cause variable signs, including necrotic or chlorotic rings and flecking on leaves, stems and fruits, with early infections leading to one-sided growth, drooping or deformed leaves, wilting, stunting, and death [127] (Fig. 10.12). Late in TSWV infection, tomatoes produce unmarketable fruit with necrotic ringspots that often appear only when the fruit reaches full color (Fig. 10.13).

A thrip on a person’s finger. Thrips are small insects with a distinctive cigar-shaped body. They are the primary vectors of plant diseases caused by tospoviruses (courtesy of OpenCage, obtained at http://en.wikipedia.org/wiki/Thrips [accessed March 18, 2014])

Pepper plant infected with tomato spotted wilt virus showing the initial development of necrotic spots on the leaves (courtesy of Carlos Gonzalez, obtained at http://en.wikipedia.org/wiki/Tospovirus [accessed March 18, 2014])

Tomato infected with tomato spotted wilt virus showing the development of necrotic ringspots on the fruit (obtained at http://en.wikipedia.org/wiki/Tospovirus [accessed March 18, 2014])
Molecular and structural studies, mostly performed on TSWV, have shown many similarities with animal-infecting bunyaviruses, including particle morphology, genomic organization, and replication and transcription cycles [128]. The presence of an envelope membrane is relatively unique among plant viruses, and is only found on tospovirions and plant-adapted rhabdovirions [128]. In contrast to the many similarities tospoviruses have with animal-infecting bunyaviruses, some interesting differences reflect tospovirus adaptation to plants. Unlike all other bunyaviruses, the NSm protein of tospoviruses is translated using a genomic ambisense strategy [129] (Fig. 10.2). Also, the NSm protein of tospoviruses is the only NSm in the family for which a well-defined function is known. Unlike the animal-infecting bunyaviruses, tospovirus particles accumulate in large vesicles within the cell and are not secreted from plant cells. Spread of the viruses to neighboring plants only occurs after larval-stage thrips have acquired the virus after feeding on infected plants [130]. After a latency period, thrips can transmit the tospovirus during the adult stage. Furthermore, due to the presence of a rigid cell wall in plants, plant viruses can only spread to neighboring cells through channels connecting the plant cells called plasmodesmata. As TSWV and most other plant viruses have a diameter of 80–120 nm, these virus cannot pass through the plasmodesmata that have a diameter in the range of only 5 nm. Thus, to facilitate movement, many plant viruses have adapted and encode cell-to-cell movement proteins (MPs) that modify plasmodesmata to allow passage of macromolecules, including virions [131]. The NSm protein of TSWV has been identified as the cell-to-cell MP that allows virus to move between plant cells [132–134].
9 Unclassified Bunyaviruses
At least 28 viruses, mostly isolated from mosquitoes or ticks and with unknown pathogenic potential for humans, are possible bunyaviruses, but currently remain unclassified (Table 10.9).
References
Lee HW. Hemorrhagic fever with renal syndrome (HFRS). Scand J Infect Dis Suppl. 1982;36:82–5.
Lee HW. Korean hemorrhagic fever. Prog Med Virol. 1982;28:96–113.
Verani P, Nicoletti L. Phlebovirus infections. In: Porterfield JS, editor. Exotic viral infections. London, UK: Chapman & Hall; 1995. p. 295–318.
Pick A. Zur Pathologie und Therapie einer eigenthümlichen endemischen Krankheitsform. Wiener Klin Wochenschr. 1886;36(1141–1145):1168–71.
Smithburn KC, Haddow AJ, Mahaffy AF. A neurotropic virus isolated from Aedes mosquitoes caught in the Semliki forest. Am J Trop Med Hyg. 1946;26:189–208.
Casals J, Whitman L. Group C, a new serological group of hitherto undescribed arthropod-borne viruses. Immunological studies. Am J Trop Med Hyg. 1961;10:250–8.
Fenner F. Classification and nomenclature of viruses—second report of the International Committee on Taxonomy of Viruses. Intervirology. 1976;7:1–115.
Plyusnin A, Beaty BJ, Elliott RM, Goldbach R, Kormelink R, et al. Bunyaviridae. In: King AMQ, Adams MJ, Carstens EB, Lefkowitz EJ, editors. Ninth report of the International Committee on Taxonomy of Viruses. San Diego, CA: Elsevier Academic; 2012. p. 725–41.
Elliott RM, Schmaljohn CS. Bunyaviridae. In: Knipe DM, Howley PM, editors. Fields virology. Philadelphia, PA: Lippincott Williams & Wilkins; 2013. p. 1244–82.
Martin ML, Lindsey-Regnery H, Sasso DR, McCormick JB, Palmer E. Distinction between Bunyaviridae genera by surface structure and comparison with Hantaan virus using negative stain electron microscopy. Arch Virol. 1985;86:17–28.
Obijeski JF, Murphy FA. Bunyaviridae: recent biochemical developments. J Gen Virol. 1977;37:1–14.
Resende Rde O, de Haan P, de Avila AC, Kitajima EW, Kormelink R, et al. Generation of envelope and defective interfering RNA mutants of tomato spotted wilt virus by mechanical passage. J Gen Virol. 1991;72(Pt 10):2375–83.
Hewlett MJ, Pettersson RF, Baltimore D. Circular forms of Uukuniemi virion RNA: an electron microscopic study. J Virol. 1977;21:1085–93.
Vera-Otarola J, Solis L, Soto-Rifo R, Ricci EP, Pino K, et al. The Andes hantavirus NSs protein is expressed from the viral small mRNA by a leaky scanning mechanism. J Virol. 2012;86:2176–87.
Jaaskelainen KM, Kaukinen P, Minskaya ES, Plyusnina A, Vapalahti O, et al. Tula and Puumala hantavirus NSs ORFs are functional and the products inhibit activation of the interferon-beta promoter. J Med Virol. 2007;79:1527–36.
Elliott RM. Molecular biology of the Bunyaviridae. J Gen Virol. 1990;71(Pt 3):501–22.
Sanchez AJ, Vincent MJ, Erickson BR, Nichol ST. Crimean-Congo hemorrhagic fever virus glycoprotein precursor is cleaved by Furin-like and SKI-1 proteases to generate a novel 38-kilodalton glycoprotein. J Virol. 2006;80:514–25.
Altamura LA, Bertolotti-Ciarlet A, Teigler J, Paragas J, Schmaljohn CS, et al. Identification of a novel C-terminal cleavage of Crimean-Congo hemorrhagic fever virus PreGN that leads to generation of an NSM protein. J Virol. 2007;81:6632–42.
Novoa RR, Calderita G, Cabezas P, Elliott RM, Risco C. Key Golgi factors for structural and functional maturation of bunyamwera virus. J Virol. 2005;79:10852–63.
Taylor SL, Altamura LA, Schmaljohn CS. Bunyaviridae. Encyclopedia of life sciences. Chichester, UK: Wiley; 2009.
Elliott RM, Blakqori G. Molecular biology of orthobunyaviruses. In: Plyusnin A, Elliott RM, editors. Bunyaviridae: molecular and cellular biology. Norfolk, UK: Caister Academic; 2011. p. 1–39.
Pantuwatana S, Thompson WH, Watts DM, Yuill TM, Hanson RP. Isolation of La Crosse virus from field collected Aedes triseriatus larvae. Am J Trop Med Hyg. 1974;23:246–50.
Watts DM, Pantuwatana S, DeFoliart GR, Yuill TM, Thompson WH. Transovarial transmission of LaCrosse virus (California encephalitis group) in the mosquito, Aedes triseriatus. Science. 1973;182:1140–1.
Yuill TM. The role of mammals in the maintenance and dissemination of La Crosse virus. In: Calisher CH, Thompson WH, editors. California serogroup viruses. New York, NY: Alan R. Liss; 1983. p. 77–88.
Anderson CR, Spence L, Downs WG, Aitken TH. Oropouche virus: a new human disease agent from Trinidad, West Indies. Am J Trop Med Hyg. 1961;10:574–8.
Azevedo RS, Nunes MR, Chiang JO, Bensabath G, Vasconcelos HB, et al. Reemergence of Oropouche fever, northern Brazil. Emerg Infect Dis. 2007;13:912–5.
Bernardes-Terzian AC, de-Moraes-Bronzoni RV, Drumond BP, DaSilva-Nunes M, da-Silva NS, et al. Sporadic oropouche virus infection, acre, Brazil. Emerg Infect Dis. 2009;15:348–50.
Pinheiro FP, Hoch AL, Gomes ML, Roberts DR. Oropouche virus. IV. Laboratory transmission by Culicoides paraensis. Am J Trop Med Hyg. 1981;30:172–6.
Pinheiro FP, Travassos da Rosa AP, Gomes ML, LeDuc JW, Hoch AL. Transmission of Oropouche virus from man to hamster by the midge Culicoides paraensis. Science. 1982;215:1251–3.
Hoffmann B, Scheuch M, Hoper D, Jungblut R, Holsteg M, et al. Novel orthobunyavirus in cattle, Europe, 2011. Emerg Infect Dis. 2012;18:469–72.
Beer M, Conraths FJ, van der Poel WH. ‘Schmallenberg virus’—a novel orthobunyavirus emerging in Europe. Epidemiol Infect. 2013;141:1–8.
Garigliany MM, Bayrou C, Kleijnen D, Cassart D, Jolly S, et al. Schmallenberg virus: a new Shamonda/Sathuperi-like virus on the rise in Europe. Antiviral Res. 2012;95:82–7.
De Regge N, Deblauwe I, De Deken R, Vantieghem P, Madder M, et al. Detection of Schmallenberg virus in different Culicoides spp. by real-time RT-PCR. Transbound Emerg Dis. 2012;59:471–5.
Elbers AR, Meiswinkel R, van Weezep E, Sloet van Oldruitenborgh-Oosterbaan MM, Kooi EA. Schmallenberg virus in Culicoides spp. biting midges, the Netherlands, 2011. Emerg Infect Dis. 2013;19:106–9.
Larska M, Polak MP, Grochowska M, Lechowski L, Zwiazek JS, et al. First report of Schmallenberg virus infection in cattle and midges in Poland. Transbound Emerg Dis. 2013;60:97–101.
Rasmussen LD, Kristensen B, Kirkeby C, Rasmussen TB, Belsham GJ, et al. Culicoids as vectors of Schmallenberg virus. Emerg Infect Dis. 2012;18:1204–6.
Veronesi E, Henstock M, Gubbins S, Batten C, Manley R, et al. Implicating Culicoides biting midges as vectors of Schmallenberg virus using semi-quantitative RT-PCR. PLoS One. 2013;8:e57747.
Yanase T, Kato T, Aizawa M, Shuto Y, Shirafuji H, et al. Genetic reassortment between Sathuperi and Shamonda viruses of the genus Orthobunyavirus in nature: implications for their genetic relationship to Schmallenberg virus. Arch Virol. 2012;157:1611–6.
Frias-Staheli N, Medina RA, Bridgen A. Nairovirus molecular biology and interaction with host cells. In: Plyusnin A, Elliott RM, editors. Bunyaviridae: molecular and cellular biology. Norfolk, UK: Caister Academic; 2011. p. 129–61.
Whitehouse CA. Crimean-Congo hemorrhagic fever virus and other nairoviruses. In: Mahy BW, van Regenmortel MHV, editors. Encyclopedia of virology. 3rd ed. Amsterdam, Netherlands: Academic; 2008. p. 596–603.
Marczinke BI, Nichol ST. Nairobi sheep disease virus, an important tick-borne pathogen of sheep and goats in Africa, is also present in Asia. Virology. 2002;303:146–51.
Whitehouse CA. Crimean-Congo hemorrhagic fever. Antiviral Res. 2004;64:145–60.
Bente DA, Forrester NL, Watts DM, McAuley AJ, Whitehouse CA, et al. Crimean-Congo hemorrhagic fever: history, epidemiology, pathogenesis, clinical syndrome and genetic diversity. Antiviral Res. 2013;100:159–89.
Dacheux L, Cervantes-Gonzalez M, Guigon G, Thiberge JM, Vandenbogaert M, et al. A preliminary study of viral metagenomics of French bat species in contact with humans: identification of new mammalian viruses. PLoS One. 2014;9:e87194.
Sironen T, Plyusnin A. Genetics and evolution of hantaviruses. In: Plyusnin A, Elliott RM, editors. Bunyaviridae: molecular and cellular biology. Norfolk, UK: Caister Academic; 2011. p. 61–94.
Plyusnin A, Morzunov SP. Virus evolution and genetic diversity of hantaviruses and their rodent hosts. Curr Top Microbiol Immunol. 2001;256:47–75.
Guo WP, Lin XD, Wang W, Tian JH, Cong ML, et al. Phylogeny and origins of hantaviruses harbored by bats, insectivores, and rodents. PLoS Pathog. 2013;9:e1003159.
Lee HW, Lee PW, Johnson KM. Isolation of the etiologic agent of Korean Hemorrhagic fever. J Infect Dis. 1978;137:298–308.
Brummer-Korvenkontio M, Vaheri A, Hovi T, von Bonsdorff CH, Vuorimies J, et al. Nephropathia epidemica: detection of antigen in bank voles and serologic diagnosis of human infection. J Infect Dis. 1980;141:131–4.
Elwell MR, Ward GS, Tingpalapong M, LeDuc JW. Serologic evidence of Hantaan-like virus in rodents and man in Thailand. Southeast Asian J Trop Med Public Health. 1985;16:349–54.
Avsic-Zupanc T, Xiao SY, Stojanovic R, Gligic A, van der Groen G, et al. Characterization of Dobrava virus: a Hantavirus from Slovenia, Yugoslavia. J Med Virol. 1992;38:132–7.
Nichol ST, Spiropoulou CF, Morzunov S, Rollin PE, Ksiazek TG, et al. Genetic identification of a hantavirus associated with an outbreak of acute respiratory illness. Science. 1993;262:914–7.
Childs JE, Ksiazek TG, Spiropoulou CF, Krebs JW, Morzunov S, et al. Serologic and genetic identification of Peromyscus maniculatus as the primary rodent reservoir for a new hantavirus in the southwestern United States. J Infect Dis. 1994;169:1271–80.
Hjelle B, Torres-Perez F. Hantaviruses in the Americas and their role as emerging pathogens. Viruses. 2010;2:2559–86.
Carey DE, Reuben R, Panicker KN, Shope RE, Myers RM. Thottapalayam virus: a presumptive arbovirus isolated from a shrew in India. Indian J Med Res. 1971;59:1758–60.
Zeller HG, Karabatsos N, Calisher CH, Digoutte JP, Cropp CB, et al. Electron microscopic and antigenic studies of uncharacterized viruses. II. Evidence suggesting the placement of viruses in the family Bunyaviridae. Arch Virol. 1989;108:211–27.
Yanagihara R, Gu SH, Arai S, Kang HJ, Song JW. Hantaviruses: rediscovery and new beginnings. Virus Res. 2014;187:6–14.
Sumibcay L, Kadjo B, Gu SH, Kang HJ, Lim BK, et al. Divergent lineage of a novel hantavirus in the banana pipistrelle (Neoromicia nanus) in Cote d’Ivoire. Virol J. 2012;9:34.
Weiss S, Witkowski PT, Auste B, Nowak K, Weber N, et al. Hantavirus in bat, Sierra Leone. Emerg Infect Dis. 2012;18:159–61.
Arai S, Nguyen ST, Boldgiv B, Fukui D, Araki K, et al. Novel bat-borne hantavirus, Vietnam. Emerg Infect Dis. 2013;19:1159–61.
Tesh RB. Phlebotomus fevers. In: Monath TP, editor. The arboviruses: epidemiology and ecology. Boca Raton, FL: CRC Press; 1988. p. 15–27.
Tesh RB, Lubroth J, Guzman H. Simulation of arbovirus overwintering: survival of Toscana virus (Bunyaviridae: Phlebovirus) in its natural sand fly vector Phlebotomus perniciosus. Am J Trop Med Hyg. 1992;47:574–81.
Tesh RB, Modi GB. Maintenance of Toscana virus in Phlebotomus perniciosus by vertical transmission. Am J Trop Med Hyg. 1987;36:189–93.
Alkan C, Bichaud L, de Lamballerie X, Alten B, Gould EA, et al. Sandfly-borne phleboviruses of Eurasia and Africa: epidemiology, genetic diversity, geographic range, control measures. Antiviral Res. 2013;100:54–74.
Depaquit J, Grandadam M, Fouque F, Andry PE, Peyrefitte C. Arthropod-borne viruses transmitted by Phlebotomine sandflies in Europe: a review. Euro Surveill. 2010;15:19507.
Major L, Linn ML, Slade RW, Schroder WA, Hyatt AD, et al. Ticks associated with macquarie island penguins carry arboviruses from four genera. PLoS One. 2009;4:e4375.
Elliott RM. Bunyaviruses and climate change. Clin Microbiol Infect. 2009;15:510–7.
Killick-Kendrick R. The biology and control of phlebotomine sand flies. Clin Dermatol. 1999;17:279–89.
Tesh R. Sandfly fever, Oropouche fever, and other bunyavirus infections. In: Guerrant RL, Walker DH, Weller PF, editors. Tropical infectious diseases: principles, pathogens, and practice. Philadelphia, PA: Elsevier Churchill Livingstone; 2006. p. 781–3.
Travassos da Rosa JF, Travassos da Rosa AP, Vasconcelos PF, Pinheiro FP, Rodrigues SG, et al. Arboviruses isolated in Evandro Chagas Institute, including some described for the first time in the Brazilian Amazon Region, their known host, and their pathology for man. In: Travassos da Rosa AP, Vasconcelos PF, Travassos da Rosa JF, editors. An overview of arbovirology in Brazil and neighboring countries. Belem, Brazil: Grafica e Editora Santo Antonia; 1998. p. 19–31.
Maroli M, Feliciangeli MD, Bichaud L, Charrel RN, Gradoni L. Phlebotomine sandflies and the spreading of leishmaniases and other diseases of public health concern. Med Vet Entomol. 2013;27:123–47.
Verani P, Nicoletti L, Ciufolini MG. Antigenic and biological characterization of Toscana virus, a new Phlebotomus fever group virus isolated in Italy. Acta Virol. 1984;28:39–47.
Daubney R, Hudson JR, Garnham PC. Enzootic hepatitis or Rift Valley fever—an undescribed virus disease of sheep cattle and man from East Africa. J Pathol Bacteriol. 1931;XXXIV:545–79.
Balkhy HH, Memish ZA. Rift Valley fever: an uninvited zoonosis in the Arabian peninsula. Int J Antimicrob Agents. 2003;21:153–7.
Sissoko D, Giry C, Gabrie P, Tarantola A, Pettinelli F, et al. Rift Valley fever, Mayotte, 2007–2008. Emerg Infect Dis. 2009;15:568–70.
Ikegami T. Molecular biology and genetic diversity of Rift Valley fever virus. Antiviral Res. 2012;95:293–310.
Pepin M, Bouloy M, Bird BH, Kemp A, Paweska J. Rift Valley fever virus (Bunyaviridae: Phlebovirus): an update on pathogenesis, molecular epidemiology, vectors, diagnostics and prevention. Vet Res. 2010;41:61.
Olive MM, Goodman SM, Reynes JM. The role of wild mammals in the maintenance of Rift Valley fever virus. J Wildl Dis. 2012;48:241–66.
Oelofsen MJ, Van der Ryst E. Could bats act as reservoir hosts for Rift Valley fever virus? Onderstepoort J Vet Res. 1999;66:51–4.
Davies FG, Highton RB. Possible vectors of Rift Valley fever in Kenya. Trans R Soc Trop Med Hyg. 1980;74:815–6.
Fontenille D, Traore-Lamizana M, Diallo M, Thonnon J, Digoutte JP, et al. New vectors of Rift Valley fever in West Africa. Emerg Infect Dis. 1998;4:289–93.
Turell MJ, Presley SM, Gad AM, Cope SE, Dohm DJ, et al. Vector competence of Egyptian mosquitoes for Rift Valley fever virus. Am J Trop Med Hyg. 1996;54:136–9.
Chambers PG, Swanepoel R. Rift valley fever in abattoir workers. Cent Afr J Med. 1980;26:122–6.
Ahmed J, Bouloy M, Ergonul O, Fooks A, Paweska J, et al. International network for capacity building for the control of emerging viral vector-borne zoonotic diseases: ARBO-ZOONET. Euro Surveill 2009;14: pii: 19160.
Saikku P, Brummer-Korvenkontio M. Arboviruses in Finland. II. Isolation and characterization of Uukuniemi virus, a virus associated with ticks and birds. Am J Trop Med Hyg. 1973;22:390–9.
Hubalek Z, Rudolf I. Tick-borne viruses in Europe. Parasitol Res. 2012;111:9–36.
Palacios G, Savji N, Travassos da Rosa A, Guzman H, Yu X, et al. Characterization of the Uukuniemi virus group (Phlebovirus: Bunyaviridae): evidence for seven distinct species. J Virol. 2013;87:3187–95.
McMullan LK, Folk SM, Kelly AJ, MacNeil A, Goldsmith CS, et al. A new phlebovirus associated with severe febrile illness in Missouri. N Engl J Med. 2012;367:834–41.
Xu B, Liu L, Huang X, Ma H, Zhang Y, et al. Metagenomic analysis of fever, thrombocytopenia and leukopenia syndrome (FTLS) in Henan Province, China: discovery of a new bunyavirus. PLoS Pathog. 2011;7:e1002369.
Yu XJ, Liang MF, Zhang SY, Liu Y, Li JD, et al. Fever with thrombocytopenia associated with a novel bunyavirus in China. N Engl J Med. 2011;364:1523–32.
Zhang YZ, Zhou DJ, Xiong Y, Chen XP, He YW, et al. Hemorrhagic fever caused by a novel tick-borne Bunyavirus in Huaiyangshan, China. Zhonghua Liu Xing Bing Xue Za Zhi. 2011;32:209–20.
Kim KH, Yi J, Kim G, Choi SJ, Jun KI, et al. Severe fever with thrombocytopenia syndrome, South Korea, 2012. Emerg Infect Dis. 2013;19:1892–4.
Liu S, Chai C, Wang C, Amer S, Lv H, et al. Systematic review of severe fever with thrombocytopenia syndrome: virology, epidemiology, and clinical characteristics. Rev Med Virol. 2014;24:90–102.
Niu G, Li J, Liang M, Jiang X, Jiang M, et al. Severe fever with thrombocytopenia syndrome virus among domesticated animals, China. Emerg Infect Dis. 2013;19:756–63.
Savage HM, Godsey Jr MS, Lambert A, Panella NA, Burkhalter KL, et al. First detection of heartland virus (Bunyaviridae: Phlebovirus) from field collected arthropods. Am J Trop Med Hyg. 2013;89:445–52.
Xing Z, Schefers J, Schwabenlander M, Jiao Y, Liang M, et al. Novel bunyavirus in domestic and captive farmed animals, Minnesota, USA. Emerg Infect Dis. 2013;19:1487–9.
Mertz GJ. Bunyaviridae: Bunyaviruses, Phleboviruses, Nairoviruses, and Hantaviruses. In: Richman DD, Whitley RJ, Haydem FG, editors. Clinical virology. 2nd ed. Washington, DC: ASM Press; 2002. p. 921–47.
Ergonul O. Crimean-Congo haemorrhagic fever. Lancet Infect Dis. 2006;6:203–14.
Ergonul O, Celikbas A, Baykam N, Eren S, Dokuzoguz B. Analysis of risk-factors among patients with Crimean-Congo haemorrhagic fever virus infection: severity criteria revisited. Clin Microbiol Infect. 2006;12:551–4.
Krautkramer E, Zeier M, Plyusnin A. Hantavirus infection: an emerging infectious disease causing acute renal failure. Kidney Int. 2013;83:23–7.
Jonsson CB, Figueiredo LT, Vapalahti O. A global perspective on hantavirus ecology, epidemiology, and disease. Clin Microbiol Rev. 2010;23:412–41.
Peters CJ, Simpson GL, Levy H. Spectrum of hantavirus infection: hemorrhagic fever with renal syndrome and hantavirus pulmonary syndrome. Annu Rev Med. 1999;50:531–45.
Lee HW, Vaheri A, Schmaljohn CS. Discovery of hantaviruses and of the Hantavirus genus: personal and historical perspectives of the Presidents of the International Society of Hantaviruses. Virus Res. 2014;187:2–5.
MacNeil A, Ksiazek TG, Rollin PE. Hantavirus pulmonary syndrome, United States, 1993–2009. Emerg Infect Dis. 2011;17:1195–201.
Rasmuson J, Andersson C, Norrman E, Haney M, Evander M, et al. Time to revise the paradigm of hantavirus syndromes? Hantavirus pulmonary syndrome caused by European hantavirus. Eur J Clin Microbiol Infect Dis. 2011;30:685–90.
Du H, Li J, Jiang W, Yu H, Zhang Y, et al. Clinical study of critical patients with hemorrhagic fever with renal syndrome complicated by acute respiratory distress syndrome. PLoS One. 2014;9:e89740.
Eitrem R, Niklasson B, Weiland O. Sandfly fever among Swedish tourists. Scand J Infect Dis. 1991;23:451–7.
Ellis SB, Appenzeller G, Lee H, Mullen K, Swenness R, et al. Outbreak of sandfly fever in central Iraq, September 2007. Mil Med. 2008;173:949–53.
Schultze D, Korte W, Rafeiner P, Niedrig M. First report of sandfly fever virus infection imported from Malta into Switzerland, October 2011. Euro Surveill. 2012;17: pii: 20209.
Dionisio D, Esperti F, Vivarelli A, Valassina M. Epidemiological, clinical and laboratory aspects of sandfly fever. Curr Opin Infect Dis. 2003;16:383–8.
Bartelloni PJ, Tesh RB. Clinical and serologic responses of volunteers infected with phlebotomus fever virus (Sicilian type). Am J Trop Med Hyg. 1976;25:456–62.
Carhan A, Uyar Y, Ozkaya E, Ertek M, Dobler G, et al. Characterization of a sandfly fever Sicilian virus isolated during a sandfly fever epidemic in Turkey. J Clin Virol. 2010;48:264–9.
Kocak Tufan Z, Weidmann M, Bulut C, Kinikli S, Hufert FT, et al. Clinical and laboratory findings of a sandfly fever Turkey Virus outbreak in Ankara. J Infect. 2011;63:375–81.
Papa A, Konstantinou G, Pavlidou V, Antoniadis A. Sandfly fever virus outbreak in Cyprus. Clin Microbiol Infect. 2006;12:192–4.
Charrel RN, Bichaud L, de Lamballerie X. Emergence of Toscana virus in the Mediterranean area. World J Virol. 2012;1:135–41.
Baldelli F, Ciufolini MG, Francisci D, Marchi A, Venturi G, et al. Unusual presentation of life-threatening Toscana virus meningoencephalitis. Clin Infect Dis. 2004;38:515–20.
Mosnier E, Charrel R, Vidal B, Ninove L, Schleinitz N, et al. Toscana virus myositis and fasciitis. Med Mal Infect. 2013;43:208–10.
Oechtering J, Petzold GC. Acute hydrocephalus due to impaired CSF resorption in Toscana virus meningoencephalitis. Neurology. 2012;79:829–31.
Sanbonmatsu-Gamez S, Perez-Ruiz M, Palop-Borras B, Navarro-Mari JM. Unusual manifestation of Toscana virus infection, Spain. Emerg Infect Dis. 2009;15:347–8.
Zanelli G, Bianco C, Cusi MG. Testicular involvement during Toscana virus infection: an unusual manifestation? Infection. 2013;41:735–6.
Madani TA, Al-Mazrou YY, Al-Jeffri MH, Mishkhas AA, Al-Rabeah AM, et al. Rift Valley fever epidemic in Saudi Arabia: epidemiological, clinical, and laboratory characteristics. Clin Infect Dis. 2003;37:1084–92.
Deng B, Zhou B, Zhang S, Zhu Y, Han L, et al. Clinical features and factors associated with severity and fatality among patients with severe fever with thrombocytopenia syndrome Bunyavirus infection in Northeast China. PLoS One. 2013;8:e80802.
Gai ZT, Zhang Y, Liang MF, Jin C, Zhang S, et al. Clinical progress and risk factors for death in severe fever with thrombocytopenia syndrome patients. J Infect Dis. 2012;206:1095–102.
Liu Y, Wu B, Paessler S, Walker DH, Tesh RB, et al. The pathogenesis of severe fever with thrombocytopenia syndrome virus infection in alpha/beta interferon knockout mice: insights into the pathologic mechanisms of a new viral hemorrhagic fever. J Virol. 2014;88:1781–6.
Samuel G, Bald JG, Pittman HA. Investigations on “spotted wilt” of tomatoes. Aust Council Sci Ind Res Bull. 1930;44:8–11.
Goldbach R, Peters D. Possible causes of the emergence of tospovirus diseases. Semin Virol. 1994;5:113–20.
Scholthof KB, Adkins S, Czosnek H, Palukaitis P, Jacquot E, et al. Top 10 plant viruses in molecular plant pathology. Mol Plant Pathol. 2011;12:938–54.
Kormelink R, Garcia ML, Goodin M, Sasaya T, Haenni AL. Negative-strand RNA viruses: the plant-infecting counterparts. Virus Res. 2011;162:184–202.
Kormelink R, de Haan P, Peters D, Goldbach R. Viral RNA synthesis in tomato spotted wilt virus-infected Nicotiana rustica plants. J Gen Virol. 1992;73(Pt 3):687–93.
van de Wetering F, Goldbach R, Peters D. Tomato spotted wilt tospovirus ingestion by first instar larvae of Frankliniella occidentalis is a prerequisite for transmission. Phytopathology. 1996;86:900–5.
Benitez-Alfonso Y, Faulkner C, Ritzenthaler C, Maule AJ. Plasmodesmata: gateways to local and systemic virus infection. Mol Plant Microbe Interact. 2010;23:1403–12.
Kormelink R, Storms M, Van Lent J, Peters D, Goldbach R. Expression and subcellular location of the NSM protein of tomato spotted wilt virus (TSWV), a putative viral movement protein. Virology. 1994;200:56–65.
Storms MM, Kormelink R, Peters D, Van Lent JW, Goldbach RW. The nonstructural NSm protein of tomato spotted wilt virus induces tubular structures in plant and insect cells. Virology. 1995;214:485–93.
Lewandowski DJ, Adkins S. The tubule-forming NSm protein from tomato spotted wilt virus complements cell-to-cell and long-distance movement of tobacco mosaic virus hybrids. Virology. 2005;342:26–37.
Yanagihara R, Daum CA, Lee PW, Baek LJ, Amyx HL, et al. Serological survey of Prospect Hill virus infection in indigenous wild rodents in the USA. Trans R Soc Trop Med Hyg. 1987;81:42–5.
Lin XD, Guo WP, Wang W, Zou Y, Hao ZY, et al. Migration of Norway rats resulted in the worldwide distribution of Seoul hantavirus today. J Virol. 2012;86:972–81.
Song JW, Baek LJ, Schmaljohn CS, Yanagihara R. Thottapalayam virus, a prototype shrewborne hantavirus. Emerg Infect Dis. 2007;13:980–5.
Acknowledgments
The authors have no conflict of interests. We thank Laura Bollinger (IRF-Frederick) for technical writing services. The content of this publication does not necessarily reflect the views or policies of the US Department of Defense, the US Department of the Army, the US Department of Health and Human Services, or of the institutions and companies affiliated with the authors. J.H.K. performed this work as an employee of Tunnell Government Services, Inc., a subcontractor to Battelle Memorial Institute, and J.W. as an employee of Battelle Memorial Institute, both under Battelle’s prime contract with NIAID, under Contract No. HHSN272200700016I.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2015 Springer Science+Business Media New York
About this chapter
Cite this chapter
Whitehouse, C.A., Kuhn, J.H., Wada, J., Ergunay, K. (2015). Family Bunyaviridae . In: Shapshak, P., Sinnott, J., Somboonwit, C., Kuhn, J. (eds) Global Virology I - Identifying and Investigating Viral Diseases. Springer, New York, NY. https://doi.org/10.1007/978-1-4939-2410-3_10
Download citation
DOI: https://doi.org/10.1007/978-1-4939-2410-3_10
Publisher Name: Springer, New York, NY
Print ISBN: 978-1-4939-2409-7
Online ISBN: 978-1-4939-2410-3
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)