
Abstract
Pelvic inflammatory disease (PID) encompasses infections of the uterus (endometritis or myometritis), fallopian tubes (salpingitis), ovaries (oophoritis), broad ligaments (parametritis), and pelvic peritoneum (peritonitis). PID accounts for up to 2.5 million outpatient visits and 350,000 emergency department visits per year for women. It is the leading cause for hospital admissions among women of reproductive age, though its incidence is decreasing due to more aggressive screening for chlamydial infections. PID is a polymicrobial disorder that results from disruption of the normal bacterial flora of the vagina and cervix, including Streptococcus agalactiae, gram-negative cocci, and anaerobes. The two initiating pathogens are Neisseria gonorrhoeae and Chlamydia trachomatis.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
- Fallopian Tube
- Bacterial Vaginosis
- Chlamydia Trachomatis
- Pelvic Inflammatory Disease
- Neisseria Gonorrhoeae
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
Pathogenesis
Pelvic inflammatory disease (PID) encompasses infections of the uterus (endometritis or myometritis), fallopian tubes (salpingitis), ovaries (oophoritis), broad ligaments (parametritis), and pelvic peritoneum (peritonitis). PID accounts for up to 2.5 million outpatient visits and 350,000 emergency department visits per year for women. It is the leading cause for hospital admissions among women of reproductive age, though its incidence is decreasing due to more aggressive screening for chlamydial infections.
PID is a polymicrobial disorder that results from disruption of the normal bacterial flora of the vagina and cervix, including Streptococcus agalactiae, gram-negative cocci, and anaerobes (Fig. 82.1). The two initiating pathogens are Neisseria gonorrhoeae and Chlamydia trachomatis. PID initiated by N. gonorrhoeae tends to be more acute and severe than that caused by C. trachomatis. By definition, this is a sexually transmitted infection, not one caused by medical procedures or pregnancy. Approximately 50 % of males may be asymptomatic at the time of transmission of infection.

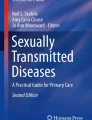
Treatment algorithm for pelvic inflammatory diseases. STDs sexually transmitted diseases, WBCs white blood cells, ESR erythrocyte sedimentation rate, IBD inflammatory bowel disease, IV intravenous, CT computed tomography, MRI magnetic resonance imaging
Risk factors for PID include young age at first sexual intercourse, multiple sexual partners (which represents a 3.4-fold increase in the risk of PID if a woman has had four or more sexual partners within 6 months), and a history of sexually transmitted infections. Barrier contraception is protective against PID. Patients with PID commonly present with acute or subacute lower abdominal pain, especially with coitus, during or after their menses. In the 7 days preceding menses, cervical mucus is thinnest and most susceptible to penetration by pathogens. Additional clinical criteria for PID include cervical motion tenderness, adnexal or uterine tenderness, abnormal uterine bleeding, purulent vaginal discharge, fevers, and chills.
Diagnosis
Minimal criteria for the diagnosis of PID include abdominopelvic pain in a sexually active woman plus cervical, uterine, or adnexal tenderness. Criteria that increase the specificity of the diagnosis include temperature greater than 38.3 °C, white blood cells seen on saline preparation of vaginal secretions, cervical exudates, and cervical friability. Laboratory evaluation that supports the clinical diagnosis of PID includes elevated C-reactive protein or sedimentation rate and positive cervical cultures. If a diagnosis of PID is confirmed, these patients should be offered testing for human immunodeficiency virus (HIV).
Differential Diagnosis
The differential diagnosis includes appendicitis, diverticulitis, inflammatory bowel disease (IBD), nephrolithiasis, cystitis, pyelonephritis, ectopic pregnancy, ovarian torsion, ruptured ovarian cyst, or degenerating fibroids.
Triage
Once the diagnosis is established, it is important to determine whether a patient needs to be admitted for intravenous antibiotic therapy. Generally, patients who require hospitalization included pregnant patients, severely ill patients (with nausea, vomiting, and fever), patients unable to tolerate oral antibiotics, patients who may be noncompliant with oral antibiotics, patients with suspected tubo-ovarian abscess, patients in whom the diagnosis is uncertain, and patients who have not responded to oral antibiotics in the outpatient setting.
Inpatient Care
Those admitted for intravenous antibiotic therapy can be treated with one of the following regimens:
-
(a)
Cefotetan 2 g IV q 12 h or cefoxitin 2 g IC q 6 h plus doxycycline 100 mg IV q I2h
-
(b)
Clindamycin 900 mg IV q 8 h plus either gentamicin IV/IM load of 2 mg/kg body weight then 1.5 mg/kg q 8 h or gentamicin 3–5 mg/kg IV/IM once daily
-
(c)
Ampicillin/sulbactam 3 g IV q 6 h plus doxycycline 100 mg IV q 12 h
Only regimen (b) can be used in pregnant patients. All other regimens contain antibiotics that are contraindicated in pregnancy.
Patients are continued on parenteral antibiotics for 24 h after the improvement of symptoms. If these criteria are met, patients can be discharged on one of the following regimens of oral antibiotic therapy:
-
(a)
Doxycycline 100 mg twice a day
-
(b)
Clindamycin 450 mg four times a day
Regimen (b) is preferable for patients in whom a tubo-ovarian abscess is suspected. Patients must be treated for a total of 14 days. Treatment of the sexual partner and use of barrier contraception should be encouraged.
These patients should be reevaluated within a week. If they continue to show improvement, they should complete their antibiotic course. Upon completion they can be followed-up routinely.
Outpatient Care
Patients who met criteria for outpatient therapy upon initial evaluation can be treated with one of the following regimens:
-
(a)
Ceftriaxone 250 mg IM once plus doxycycline 100 mg PO twice a day for 14 days with or without metronidazole 500 mg PO twice a day for 14 days
-
(b)
Cefoxitin 2 g IM once plus probenecid 1 g PO concurrently plus doxycycline 100 mg PO twice a day for 14 days with or without metronidazole 500 mg PO twice a day for 14 days
-
(c)
Other 3rd-generation cephalosporin (ceftizoxime, cefotaxime) plus doxycycline 100 mg PO twice a day for 14 days with or without metronidazole 500 mg PO twice a day for 14 days
Cefoxitin provides better anaerobic coverage; ceftriaxone provides better coverage for N. gonorrhoeae. Metronidazole provides better coverage for bacterial vaginosis, which is frequently associated with PID. Treatment of the sexual partner and use of barrier contraception should be encouraged. For patients who do not improve, further studies should be done to rule out an abscess.
Further Studies
If the patient is not improving on IV antibiotics, if an adnexal mass is palpable, or if the patient is too tender for a proper pelvic exam, further studies are warranted. Endometrial biopsy may lend histopathologic proof of endometritis. Imaging studies include transvaginal ultrasound (TVUS) with or without Doppler, MRI, and abdominal CT. A TVUS may show thickened or filled fallopian tubes with or without free pelvic fluid. A CT or MRI may show evidence of a pelvic or tubo-ovarian abscess.
Abscess
When imaging studies reveal the presence of an abscess, one of the following management protocols can be pursued:
-
(a)
If the patient becomes hypotensive, tachycardic, and acidotic or manifests peritoneal signs, or if there is evidence of sepsis or abscess while on antibiotics, a laparoscopy or laparotomy is warranted to remove the abscess. These patients should be counseled preoperatively about the possibility of a hysterectomy and/or possible removal of the fallopian tubes and ovaries.
-
(b)
If the patient is not worsening nor improving on antibiotics, image-guided drainage of the abscess is warranted. The patient should continue IV antibiotics with additional anaerobic coverage.
-
(c)
If the patient is hemodynamically stable, the abscess is less than 9 cm, the patient has had adequate response to antibiotics, and the patient is premenopausal, then the patient should receive broad-spectrum antibiotics. If there is no significant improvement in 24–48 h, these patients should undergo surgical assessment.
Once the diagnosis of PID is made, patients should be counseled about the following sequelae of the disease:
-
Women with PID have an increased infertility rate. The degree of infertility appears to be directly proportional to the number of episodes of PID. Women with three or more episodes have infertility rates up to 60 %.
Author information
Authors and Affiliations
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2015 Springer New York
About this chapter
Cite this chapter
Blank, J. (2015). Pelvic Inflammatory Diseases. In: Saclarides, T., Myers, J., Millikan, K. (eds) Common Surgical Diseases. Springer, New York, NY. https://doi.org/10.1007/978-1-4939-1565-1_82
Download citation
DOI: https://doi.org/10.1007/978-1-4939-1565-1_82
Published:
Publisher Name: Springer, New York, NY
Print ISBN: 978-1-4939-1564-4
Online ISBN: 978-1-4939-1565-1
eBook Packages: MedicineMedicine (R0)