
Abstract
Pelvic inflammatory disease (PID) is an infection of the female reproductive organs (upper genital tract and the surrounding structures including the endometrium, ovaries, and fallopian tubes) [1]. PID occurs when bacteria move from the vagina and cervix upward into the uterus, ovaries, or fallopian tubes. The bacteria can lead to an abscess in a fallopian tube or ovary. Long-term problems can occur if PID is not treated promptly [1, 2].
Access provided by CONRICYT-eBooks. Download chapter PDF
Similar content being viewed by others


Keywords
- Fallopian Tube
- Pelvic Inflammatory Disease
- Uterosacral Ligament
- Lower Uterine Segment
- Female Reproductive Organ
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
Introduction
Pelvic inflammatory disease (PID) is an infection of the female reproductive organs (upper genital tract and the surrounding structures including the endometrium, ovaries, and fallopian tubes) [1]. PID occurs when bacteria move from the vagina and cervix upward into the uterus, ovaries, or fallopian tubes. The bacteria can lead to an abscess in a fallopian tube or ovary. Long-term problems can occur if PID is not treated promptly [1, 2].
Recurrent PID can double a woman’s risk of infertility and quadruple her risk of chronic pelvic pain. PID contributes to approximately 2.5 million office visits and 125,000-150,000 hospitalizations every year. Some women with PID have only mild symptoms or no symptoms at all. Because the symptoms can be vague, women or their gynecologists or other health care professionals do not recognize many cases [3, 4].
Following are the most common signs and symptoms of PID:
-
Abnormal vaginal discharge
-
Pain in the lower abdomen (often a mild ache)
-
Pain in the upper right abdomen
-
Abnormal menstrual bleeding
-
Fever and chills
-
Painful urination
-
Nausea and vomiting
-
Painful sexual intercourse
It is believed that in up to 25% of women with lower abdominal pain admitted to emergency departments, the pain is caused by PID [2, 4, 5].
Ultrasound
Ultrasonography should be the first diagnostic imaging examination to be performed in cases of suspected PID in which there are ambiguous or unexplained clinical findings or an inability to perform an adequate clinical examination. Ultrasonography is also indicated to evaluate for complications of PID, which may impact surgical vs. non-surgical management or the decision to hospitalize a patient [5,6,7]. US is considered to be the first-line imaging modality in the evaluation of suspected salpingitis; however, US may only show subtle abnormalities such as tubal tortuosity, wall hyperemia, and fallopian tube thickening of more than 5 mm. When they are normal in size, the fallopian tubes measure 1–4 mm in diameter and are not regularly depicted on US or CT [8,9,10].

Right adnexal region inflammatory process: ultrasound demonstrating the tortuous and dilated fallopian tube, filled with liquid, and the ovary with increased dimensions, compatible with tube and ovary abscesses. It shows up as an ill-defined adnexal tumor, containing thick liquid
MRI
MRI serves as an excellent imaging modality in cases in which the ultrasonographic findings are equivocal. In a study by Tukeva et al., the authors compared findings from MRI with sonograms and found that MRI was more accurate than ultrasonography in the diagnosis of PID [8].
Findings: The tubular structure is readily identified as cystic, with high signal intensity on T2- weighted images, which is lower than that of a pure cyst and may present a lack of internal enhancement. The signal intensity of T1-weighted images varies, depending on the protein content of the fluid. There is enhancement of the thickened fallopian tube walls and pelvic fat stranding. Although differentiating between pyosalpinx and hydrosalpinx is difficult, the thick hyper-enhancing tubal walls and surrounding inflammation serve as clues to the diagnosis. In cases of tubo-ovarian abscesses, MR imaging findings depend on the hemorrhagic and protein content of the mass. The abscess is usually hypointense at T1-weighted imaging; however, hemorrhagic or proteinaceous material can be hyperintense. A hyperintense rim along the inner wall of the abscess cavity has been described at T1-weighted imaging and is thought to correspond to granulation tissue and hemorrhage. T2-weighted imaging demonstrates a heterogeneous mass with low-signal-intensity septa, as well as hypointense linear stranding in the adjacent pelvic fat.
CT
Occasionally, CT scanning may be used as the initial diagnostic study for the investigation of nonspecific pelvic pain in a female, and PID may be found incidentally. CT scanning is very sensitive for the detection of pelvic pathology; however, it may not be as specific as sonography when an adnexal pathology must be differentiated from a tubal or ovarian one. If the diagnosis of PID is still in question, confirmation with ultrasonography is suggested.
The most common general CT findings of PID described in the literature are thickening of the uterosacral ligaments; obliteration of fascial planes; free fluid in the cul-de-sac; loss of definition of the uterine border; pelvic fat infiltration or haziness and pelvic edema; reactive lymphadenopathy; and signs of peritonitis. The uterosacral ligaments are paired structures that extend from the lower uterine segment to the mid-sacrum and are best seen on axial cross-sectional images. The normal thickness of the uterosacral ligaments is subjective and has not yet been established on CT images [11,12,13,14]. Salpingitis should be suspected at CT when the fallopian tubes are thickened, measuring more than 5 mm in axial dimension, and show enhancing walls. Associated free fluid may be depicted within the cul-de-sac. For the diagnosis of PID, the CT finding of tubal thickening was found to have a high specificity of 95% [14].
PID is often accompanied by reactive lymphadenopathy affecting the para-aortic lymphatic chain at the level of the renal hila. This lymphadenopathy is caused by the course of drainage of the ovarian and salpingian lymphatic vessels along the gonadal veins [14, 15] (Figs. 4.1, 4.2, 4.3, 4.4, 4.5, 4.6, 4.7 and 4.8).

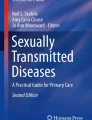
Salpingitis: Pelvic CT, where one can observe anomalous enhancement in the left adnexal region, with a serpiginous aspect, corresponding to the wall of the tube, thickened by inflammation (solid arrows). A small amount of fluid surrounds it. The right ovary appears normal (casting arrows). (a, b) Axial sections in the venous phase of contrast injection. Salpingitis is characterized by the absence of tube dilation, but shows thickening and enhancement by contrast of tubal walls, associated with adjacent inflammatory signs. These signs manifest in the CT as a densification of adnexal fatty plans and free fluid in the pelvic cavity, as well as reactive thickening of adjacent bowels

Salpingitis: MRI of the pelvis, showing the presence of serpiginous formation in the right adnexal region (arrows a, b, d), clearly separated from the uterus (stars in a, b), with intense parietal enhancement, by contrast, featuring its inflammatory nature (arrow c). The aspect in c is highly suggestive of a fallopian tube with thickened walls. (a, b: axial T1 and T2, respectively; c: axial T1 with fat saturation technique, after contrast injection; d: coronal T2)

Tubo-ovarian abcess: CT scan showing nodular formation, with heterogeneous enhancement, located in the right adnexal region, that represents the inflamed ovary (star b). The uterine tube is dilated and has parietal enhancement, indicating pyosalpinx or salpingitis (arrows in a, b). (a, b) Axial sections obtained in the portal phase, after the injection of contrast. Some differential diagnoses must be observed. In hydrosalpinx, unlike in pyosalpinx, tubal parietal enhancement by the contrast agent does not occur. Other diagnoses, such as appendicitis and complex adnexal masses, may make the differential diagnosis difficult

Severe PID shown by CT (a, b) and MR (c, d). Extensive and diffuse thickening of the endometrium can be noted, with air-fluid level in the uterine cavity (arrows a, b). Also heterogeneous collection in front of the uterus, with thick walls, and exhibiting moderate enhancement by contrast is associated (star a). The MRI shows thick material in the uterine cavity (stars c, d) as well as enhancement of adnexal structures (arrows d). (a, b): axial sections obtained in the portal phase; c: MRI in sagittal plan, in T2; d: MRI in axial plan in T1, with fat saturation technique, after contrast injection. The presence of gas within the inflammatory/infectious process is not common, yet it is a very specific finding. The associated signs commonly found are mainly the thickening and enhancement of the peritoneum and uterine ligaments. There may also be involvement of adjacent structures, such as ileus, hidroureteronefrosis, and intraperitoneal abscess secondary to the rupture

Tubo-ovarian abcess. MRI of the pelvis showing collection (white stars), with thickened walls, and that feature enhancement by contrast and thin internal folds (solid arrows in a, c, d) that are compatible with a dilated tube. The wall of the formation presents high-signal intensity on T1 (full arrow b) compatible with small foci of parietal bleeding. There is still a loculated collection in the posterior fornix (black stars a, c) and intense enhancement of the peritoneum (casting arrows in c, d). (a, b) Axial plan T2 and T1 respectively; (c, d) T1 axial plan with fat saturation technique, after injection of contrast. The MRI findings depend on the hematic and protein content, with variable signals on T1-weighted sequences, depending on the amount of these components. A thin inner halo of low-signal intensity on the T1, along the inner wall of the collection, has been recently described, and assigned to the granulation tissue. The T2-weighted images show high signal, with multiple coarse internal septa, exhibiting low signal, as well as a loud signal of peritoneal fat in T2 sequences with fat saturation, corresponding to edema. These septa, along with the collection capsule, exhibit intense enhancement after contrast, associated with the enhancement of fat and abdominal structures involved

Salpingitis to the left: (a) Endovaginal ultrasound, showing left tube (yellow arrows) as a tubular structure with thick liquid content, adjacent to the left ovary (red arrow). In (b) we can note the irregularity and thickening of the tubal wall, subsequent to inflammation (arrowheads)

Endometritis: Endovaginal ultrasound, in a patient with abdominal pain, vaginal bleeding and fever for 2 days. The image shows the thickened and hyperechoic endometrium, with undefined limits for the most part (between the arrows). The diagnosis of endometritis is often a challenging task, as signs and symptoms are non-specific and the sonographic findings are variableI; these include thickening and irregularity of the endometrium, and fluid or debris accumulated within the endometrial cavity
References
US National Library of Medicine, National Institutes of Health. Pelvic inflammatory disease (PID). Updated 11/29/2011. MedlinePlus. Available at http://www.nlm.nih.gov/medlineplus/ency/article/000888.htm. Accessed 9 Sept 2015.
Ross J. Pelvic inflammatory disease. BMJ. 2001;322(7287):658–9.
Beigi RH, Wiesenfeld HC. Pelvic inflammatory disease: new diagnostic criteria and treatment. Obstet Gynecol Clin North Am. 2003;30(4):777–93.
World Health Organization. Sexually transmitted infections. Available at http://www.who.int/mediacentre/factsheets/fs110/en/. Accessed 4 Oct 2015.
Golden N, Cohen H, Gennari G, Neuhoff S. The use of pelvic ultrasonography in the evaluation of adolescents with pelvic inflammatory disease. Am J Dis Child. 1987;141(11):1235–8.
Ozbay K, Deveci S. Relationships between transvaginal colour Doppler findings, infectious parameters and visual analogue scale scores in patients with mild acute pelvic inflammatory disease. Eur J Obstet Gynecol Reprod Biol. 2011;156(1):105–8.
Thomassin-Naggara I, Darai E, Bazot M. Gynecological pelvic infection: what is the role of imaging? Diagn Interv Imaging. 2012;93(6):491–9.
Tukeva TA, Aronen HJ, Karjalainen PT, Molander P, Paavonen T, Paavonen J. MR imaging in pelvic inflammatory disease: comparison with laparoscopy and US. Radiology. 1999;210(1):209–16.
Lee MH, Moon MH, Sung CK, Woo H, Oh S. CT findings of acute pelvic inflammatory disease. Abdom Imaging. 2014;39(6):1350–5.
Potter AW, Chandrasekhar CA. US and CT evaluation of acute pelvic pain of gynecologic origin in nonpregnant premenopausal patients. RadioGraphics. 2008;28(6):1645–59.
Bennett G, Slywotzky C. Gynecologic causes of acute pelvic pain: spectrum of CT findings. RadioGraphics. 2002;22:785–0.
FebroniocEM,Rosas GQ, D’Ippolito G. Doença inflamatória pélvica aguda: ensaio iconográfico com enfoque em achados de tomografia computadorizada e ressonância magnética. Radiol Bras. 2012;45:345–50.
Agrawal A. Imaging in pelvic inflammatory disease and tubo-ovarian abscess. Available at http://emedicine.medscape.com/article/404537-overview#showall. Accessed 25 Nov 2015.
Revzin MV, Mathur M, Dave HB, Macer ML, Spektor M. Pelvic inflammatory disease: multimodality imaging approach with clinical-pathologic correlation. RadioGraphics. 2016;36(5):1579–96.
Langer JE, Dinsmore BJ. Computed tomographic evaluation of benign and inflammatory disorders of the female pelvis. Radiol Clin North Am. 1992;30(4):831–42.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2017 Springer International Publishing Switzerland
About this chapter
Cite this chapter
de Camargo Penteado, C.A., Alves, G.S.P., De Nicola, H. (2017). Pelvic Inflammatory Disease. In: de Souza, L., De Nicola, A., De Nicola, H. (eds) Atlas of Imaging in Infertility. Springer, Cham. https://doi.org/10.1007/978-3-319-13893-0_4
Download citation
DOI: https://doi.org/10.1007/978-3-319-13893-0_4
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-13892-3
Online ISBN: 978-3-319-13893-0
eBook Packages: MedicineMedicine (R0)