
Abstract
This chapter presents a modified levator advancement technique in which the orbicularis, levator aponeurosis complex is reflected from its insertion on the underlying inferior one third of tarsus. This allows for advancement of the aponeurosis while ensuring clear anatomic visualization as the aponeurosis is dissected from underlying Mueller’s muscle in a bloodless, surgical plane.
You have full access to this open access chapter, Download chapter PDF
Similar content being viewed by others


Keywords
A preferred technique for the repair of ptosis is a modification of a levator advancement technique.
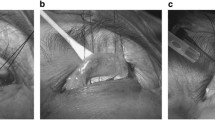
In this modified technique, 1–2 cc of a 50:50 mixture of 2 % xylocaine with 1:100:000 epinephrine and 0.25 % Marcaine with 1:200:000 epinephrine, sodium bicarbonate, and hyaluronidase is injected into the area of the lateral aspect of the upper eyelid. A “digital diffusion” technique is used to wipe the local solution across the eyelid. The patient is then prepped, draped, and marked in the usual sterile fashion. A blepharoplasty is performed if needed, after which the levator aponeurosis is reflected from its insertion from underlying tarsus and Müller’s muscle. The aponeurosis is elevated by incising the orbicularis directly over the inferior one third of tarsus. The orbicularis, levator complex is elevated from its insertion onto tarsus as the surgical space is entered. The aponeurosis orbicularis complex is then dissected from underlying Müller’s muscle. The aponeurosis can be swept off Müller’s in this natural anatomic space. Müller’s muscle can be identified by its vascularity. The peripheral vascular arcade can often be identified superior to the superior tarsal margin. Two or three double-armed 5-0 or 6-0 Vicryl sutures on an S-14, S-24, or SS-2 spatulated semicircle needle are then placed in a lamellar fashion through tarsus. These sutures are placed in the midline as well as medially and occasionally laterally. There is a “sweet spot” just medial to the midline that provides for an optimal eyelid configuration. Once positioned, the sutures are placed in a mattress fashion through the levator aponeurosis superior to the area of relative thinning. Place the central suture first. If the height and contour of the eyelid is appropriate, additional sutures may not be needed. All the double-armed sutures are then held with a snap and tied and cut. The orbital septum may be incised to avoid lagophthalmos as needed. Often, weakening of the septum just superior to the sutures placed may be sufficient. The advanced aponeurosis may or may not be trimmed. The skin is then closed in the usual fashion.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2015 Springer Science+Business Media New York
About this chapter
Cite this chapter
Silkiss, R.Z. (2015). Modified Levator Advancement Ptosis Technique. In: Hartstein, MD, FACS, M., Massry, MD, FACS, G., Holds, MD, FACS, J. (eds) Pearls and Pitfalls in Cosmetic Oculoplastic Surgery. Springer, New York, NY. https://doi.org/10.1007/978-1-4939-1544-6_185
Download citation
DOI: https://doi.org/10.1007/978-1-4939-1544-6_185
Published:
Publisher Name: Springer, New York, NY
Print ISBN: 978-1-4939-1543-9
Online ISBN: 978-1-4939-1544-6
eBook Packages: MedicineMedicine (R0)