
Abstract
The effectiveness of screening mammography in reducing mortality from breast cancer has been well documented in several randomized clinical trials. Mammographic signs of breast cancer cover a wide spectrum including the commonly encountered irregular spiculated masses, pleomorphic microcalcifications, as well as asymmetry and architectural distortion. There are certain mammographic signs that are subtle, and these account for a significant number of missed cancers. Such subtle signs include small developing densities or findings that are obscured by dense glandular tissue. The mammographic signs of breast cancer and the differential diagnosis are discussed in this chapter.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others



Keywords
- Breast Cancer
- Human Epidermal Growth Factor Receptor
- Inflammatory Breast Cancer
- Architectural Distortion
- Screen Mammogram
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
Introduction
The effectiveness of screening mammography in reducing mortality from breast cancer has been well documented in several randomized clinical trials. Mammographic signs of breast cancer cover a wide spectrum including the commonly encountered irregular spiculated masses, pleomorphic microcalcifications, as well as asymmetry and architectural distortion. There are certain mammographic signs that are subtle, and these account for a significant number of missed cancers. Such subtle signs include small developing densities or findings that are obscured by dense glandular tissue. The mammographic signs of breast cancer and the differential diagnosis are discussed in this chapter.
On a mammogram there are four signs that are commonly associated with breast cancer, and there are additional signs that are less commonly seen and represent subtle signs of breast cancer (Box 5.1). The two most common mammographic appearances of breast cancer on a mammogram are masses and calcifications. Masses have been reported in a higher percentage of cancers in those series that include a larger number of invasive cancers, and microcalcifications are reported in a higher percentage of cancers in series that have a larger proportion of ductal carcinoma in situ [DCIS]. Asymmetry and architectural distortion are other commonly seen signs of breast cancer although less frequently associated with breast cancer than are masses and calcifications. In a series of 1,552 breast cancers of which 1,287 were invasive, 56 % of cancers appeared mostly as masses, 29 % appeared as calcifications, with asymmetry (12 %) and architectural distortion (4 %) accounting for the remainder of the cases [1]. In a series of 543 cases of breast cancer where a larger proportion of cases were made of DCIS (36 %), microcalcifications (47 %) were seen more commonly than masses (41 %) [2]. A majority of breast cancers presenting as masses were invasive cancers [95 %], and a majority of calcifications (68 %) were associated with DCIS. Architectural distortion was seen as a sign of breast cancer in 4 % of cases in this series [2].
Box 5.1 Mammographic Signs of Breast Cancer
Classic signs of breast cancer |
1. Mass |
2. Architectural distortion |
3. Malignant-appearing microcalcifications |
4. Focal asymmetry |
Subtle signs of breast cancer |
1. Developing densities |
2. Subtle asymmetries |
3. Partially visualized abnormalities |
4. One-view-only finding |
The positive predictive value on a screening examination for masses and calcifications is similar and is slightly lower for developing asymmetry and least for focal asymmetry [1]. Although architectural distortion is the least common of the four frequent signs of breast cancer, its reported positive predictive value for breast cancer on a screening examination (10.2 %) is similar to masses (9.7 %) and calcifications (12.7 %) and higher than for developing asymmetry (7.4 %). Focal asymmetry has a relatively low PPV for breast cancer at 3.7 %. A mass with spiculated margins (PPV = 81 %) and linear calcifications (PPV = 81 %) had the highest predictive value among 225 cancers in a series of 492 cases undergoing surgical biopsy. Other mammographic features that also show a high positive predictive value for cancer include masses with an irregular shape (73 %) and calcifications in a segmental (74 %) or linear distribution (68 %) [3].
Mass
A mass is a space-occupying lesion that is seen in two different mammographic projections. It has an outwardly convex border, is seen on two views, and is at least as dense centrally as in the periphery. Summation shadows on the other hand are produced by fortuitous superimposition of fibroglandular tissue and are not visualized in more than one projection [4]. When a mass is identified on a screening mammogram, an analysis of its features is done as follows: The shape of the mass is described as being round, oval, or lobular when a mass has an undulating contour. If a mass cannot be described as one of these, it is described as having an irregular shape (Fig. 5.1a–c). Once the primary features are ascertained, recall for a diagnostic assessment is often initiated. Spot compression views help define the margin characteristics of a mass. A margin that is sharply demarcated and well defined in at least 75 % of its extent and remainder is obscured is considered circumscribed with an abrupt transition from the mass to the surrounding tissue. Small undulations of the border of a mass are defined as a macrolobulated border. A poor definition of the margin is suspicious for infiltration, a finding suggestive of malignancy. When lines radiate from the edge of a mass, the margin is described as being spiculated [5]. A mass with a density higher than of the surrounding fibroglandular parenchyma is more likely to be malignant than a low-density mass (Fig. 5.2a–c). In a retrospective study of 348 breast masses with biopsy confirmation, 70.2 % of the high-density masses were malignant, and 22.3 % of the iso- or low-density masses were malignant [6]. Similar results have been reported using inductive logic programming and conditional probabilities and validating this association in an independent dataset [7].

(a–c) A 47-year-old with a 9 mm mass histologically proven to be a DCIS. (a) Mediolateral oblique view of a screening mammogram demonstrates a dense mass in the axillary tail (arrow). (b) Spot compression view in the mediolateral oblique projection reveals a mass with fine spiculated borders suspicious for a malignant mass. (c) Ultrasound demonstrates a 9 mm irregular mass with malignant features

(a–c) A 31-year-old with a palpable mass histologically proven to be invasive ductal cancer. (a) Mediolateral oblique view demonstrates a hyperdense mass with a circumscribed margin. (b) Craniocaudal projection reveals the mass with obscured borders. (c) Ultrasound shows a hypoechoic lobulated solid mass with ill-defined margins
There is a reported association between morphologic features and tumor stage and prognosis. Masses with spiculated margins are known to be associated with lower-grade tumors and hence have a better prognosis (Fig. 5.3a, b). On the other hand triple-negative breast cancers have been found to be associated with circumscribed masses and masses with microlobulations and with ill-defined borders. Lymphovascular invasion has been reported to be seen more often in breast cancers associated with architectural distortion rather than those with spiculated mass. The reason behind this association is unknown [8]. Lymphovascular invasion is also more common in masses with calcifications. In invasive cancers, the presence of calcifications is often associated with extensive intraductal component and necrosis. In one series breast cancers presenting as architectural distortion were reported to have positive margins in 65 % of cases. These investigators, however, did not find a significant correlate between mammographic features and tumor differentiation or ER (estrogen receptor)/PR (progesterone receptor) status [8].

(a, b) A 48-year-old with a screen-detected small spiculated mass histologically proven to be an invasive ductal cancer. (a) Spot compression magnification mediolateral view demonstrates a spiculated mass with microcalcifications and a second area of pleomorphic microcalcifications superiorly (arrow) that was proven to be DCIS. (b) Spot compression magnification craniocaudal view demonstrates a spiculated mass with microcalcifications
It is known that the proportion of invasive cancers tends to be higher in younger women (Fig. 5.4a–c). The ratio of invasive to noninvasive cancers increased from 1:1 in those younger than 50 years of age to 3:1 in those over 70 years. Breast cancers presenting with calcifications are also decreased from 63 % in women younger than 50 years to 26 % in older than 70 years [2]. Generally calcifications that are malignant are associated with DCIS in 63 % of cases, whereas a spiculated mass is associated with invasive cancer in as high as 95 % of cases [9]. In a small percentage of cases, spiculated masses may represent pure DCIS or DCIS associated with a radial scar, 8 % of a series of 86 lesions with predominant DCIS in one series [10]. The prognosis is best and 8-year survival was the longest for small spiculated masses [95 %] that are 1–9 mm and good for rounded masses [91 %] compared to those presenting with calcifications [77 %]. Patients with casting or pleomorphic calcifications had significantly worst prognosis [11].


(a–c) A 35-year-old with a palpable lump in left breast histologically proven to be invasive ductal cancer. (a) Mediolateral oblique view reveals no abnormality. (b) Craniocaudal view with spot compression demonstrates dense tissue but no mass. (c) Ultrasound demonstrates a solid hypoechoic mass with ill-defined and microlobulated borders suggestive of malignancy
Architectural Distortion
Architectural distortion refers to a localized disruption of the breast architecture which can include spiculations or thin lines that radiate from a focal point or a localized retraction of the edge of the parenchyma at its interface with fat. It is a normal finding to see lines randomly crossing within the breast parenchyma; what is abnormal is when one sees these lines converging to a focal area. Not uncommonly overlapping crisscrossing tissue lines may simulate architectural distortion on a screening mammogram. Careful inspection alone with use of a magnifying lens may suffice to make this assertion; when unclear, recall for spot compression and rolled views of the breast in the projection where it is best seen will help to exclude an area of true architectural distortion (Fig. 5.5a, b). Architectural distortion when unassociated with other findings such as masses or clustered calcifications can be often subtle and accounts for a significant number of missed breast cancers; a discussion on missed cancers appears later. Architectural distortion is less common than a mass as a mammographic sign of breast cancer but is highly predictive of breast cancer both at screening and diagnostic mammography [1]. Architectural distortion is a sign of invasive ductal and invasive lobular cancer and results from the fibrosis in a scirrhous carcinoma. Ductal carcinoma in situ most commonly manifests as indeterminate or malignant-appearing microcalcifications. However, a small percentage of DCIS can appear as areas of distortion, 2.1 % [4/190] in one series [12]. Architectural distortion in an area of DCIS is often attributed to associated sclerosing adenosis rather than due to the in situ cancer itself. In one series, 5 of 54 cases of DCIS [10.8 %] appeared as an area of architectural distortion. Histopathological correlation in this series showed that the AD in 4 of 5 cases correlated with sclerosis in the interstitium around DCIS, and DCIS in Cooper’s ligament accounted for the appearance of AD on the mammogram [13].

(a, b) An invasive ductal cancer appearing as an area of architectural distortion. (a) Spot compression magnification views in the CC projection demonstrates an area of subtle architectural distortion (between arrow and arrowhead). (b) Spot compression magnification views in the MLO projection demonstrate an area of subtle architectural distortion (arrow)
It is also known that in patients with architectural distortion on mammography, there is more likely to be positive margins than those with masses or calcifications [2]. Breast cancer presenting as AD is also reported to be significantly larger than that seen on mammography compared to other mammographic abnormalities. It is therefore recommended that in those patients with nonpalpable architectural distortions, a wider excision be undertaken to minimize the risk of having positive margins. Although most series of invasive breast cancers have found architectural distortion a less common mammographic presentation, architectural distortion has been reported to be more frequently seen in invasive lobular cancer. Architectural distortion was found to be the second most common appearance after a mass, in some studies ranging from 10 to 34 % of cases of invasive lobular cancer [14]. The differential diagnosis of an area of architectural distortion appears in Box 5.2. A finding of an architectural distortion on a mammogram except for those that can definitively be attributed to prior surgery, biopsy, or trauma is an indication for excisional biopsy in most instances. Known mimics of cancers that can appear as areas of architectural distortion include a radial scar and sclerosing adenosis.
Box 5.2 Differential Diagnosis of Architectural Distortion on a Mammogram
1. Invasive ductal and invasive lobular cancer |
2. Radial scar |
3. Sclerosing adenosis |
4. Postsurgical or post biopsy |
5. Post breast trauma |
Differential Diagnosis of Architectural Distortion
Radial Scars
A radial scar is a known mammographic mimic of breast cancer. When these lesions are smaller than 1 cm, they are referred to as a radial scar and when larger than 1 cm are called complex sclerosing lesions (Fig. 5.6a–d). Mammographic features that are typical of radial scars include the presence of a central lucency from which thin long spicules radiate. The abnormality has a characteristic varying appearance on different projections and radiolucent linear structures parallel the spicules. Such a mammographic appearance has been called the black star in contradistinction to cancer where the central area of architectural distortion is dense and hence is referred as a white star. Radial scars are not typically palpable and not associated with microcalcifications [15, 16]. The mammographically described radial scar is distinct from those that are incidentally reported in histology specimens in about 28 % of cases [17]. These latter radial scars are small lesions, mammographically occult, and do not carry an increased risk of associated cancer.


(a–d) A 35-year-old with a family history of cancer and a palpable lump histologically proven to be a complex sclerosing lesion. (a) Mediolateral oblique view demonstrates a large irregular focal asymmetry with architectural distortion. (b) Craniocaudal view demonstrates a large irregular focal asymmetry with architectural distortion. (c, d) Ultrasound demonstrates an irregular mass that was considered probably malignant
The reported incidence of radial scars on screening mammograms is about 3 per 1,000 [18]. Although benign, when suspected on a mammogram, excisional biopsy is generally recommended due to the known association with invasive cancer and the difficulty in distinguishing tubular cancer from radial scar on core biopsy specimens [19]. Sonography is generally not performed when a radial scar is identified on the mammogram; however, sonographic appearance of radial scars has been described. Ultrasound is useful when the area of distortion is seen on one view only and if seen may then be used for presurgical localization [20–22].
Sclerosing Adenosis
Sclerosing adenosis is a proliferative benign abnormality characterized by proliferation of stromal and myoepithelial cells leading to distortion of the acini. It is often associated with other benign and malignant abnormalities. When sclerosing adenosis exists as a dominant component, it may appear as a localized area of calcifications, mass, focal asymmetry, or an area of architectural distortion [23]. In one series of 69/76 cases of histologically proven sclerosing adenosis that were mammographically detectable, 12 % appeared as areas of localized architectural distortion [24]. In another series of 43 cases, 6.9 % [3/43] of sclerosing adenosis appeared on the mammogram as an area of architectural distortion [25].
Breast Trauma
Trauma to the breast may lead to mammographic findings that mimic cancer; however, appropriate history and evolution of changes in the appearance are helpful in the differential diagnosis (Fig. 5.7a, b). The spectrum of trauma encompasses blunt trauma such as in a seat belt injury, all types of breast biopsy, lumpectomy, as well as mammoplasty. Fat necrosis that can result from any insult to the breast parenchyma may also present diagnostic dilemma particularly when a reliable history is not present. A description of the postoperative breast appears in a separate chapter (Chap. 16).

(a, b) A 44-year-old with a history of a seat belt injury 3 months prior to a screening mammogram. (a) Mediolateral oblique view demonstrates an area of asymmetry and distortion in upper breast. (b) Spot compress view in the craniocaudal projection shows the area of distortion
Fat necrosis is a clinical and imaging mimic of breast cancer. The mammographic spectrum of findings includes a lipid cyst with or without calcification of the wall, clustered microcalcifications, spiculated mass, and nonlucent focal mass. Fat necrosis may result from accidental breast trauma or any of the previously listed causes of iatrogenic breast trauma, surgery, and biopsy [26]. Seat belt injuries cause appearance of areas of fat density necrosis and areas of increased density in a band-shaped distribution. In the short term the increased density may decrease in size, and the line of fibrosis is evident. These changes evolve over a period of time with development of calcifications and resultant architectural distortion [27].
Microcalcifications
Calcifications that are identified on a screening mammogram and that do not exhibit the established criteria of benign calcifications are recalled to undergo a diagnostic mammogram. Spot compression magnification views in the mediolateral and craniocaudal projections are routinely obtained. The rationale for obtaining magnification views is to study the morphology and the distribution pattern of the calcifications. Magnification mammography decreases noise and improves image sharpness allowing for optimal evaluation of the morphology and distribution of calcifications. A description of mammographically identified calcifications should include the morphologic features and the distribution of the calcifications. Macrocalcifications are typically larger than 2 mm and are associated with benign processes; microcalcifications are smaller than 0.5 mm and can be associated with ductal carcinoma in situ or invasive cancer [28]. In DCIS the tumor grows within the duct, distending it but remaining within the basement membrane.
Malignancies presenting as calcifications on mammography are most commonly associated with DCIS and have been reported in up to 68 % of cases of ductal carcinoma in situ [2]. About 29–47 % of breast cancers appear as microcalcifications without a mass [1]. About 24 % of the suspicious calcifications are associated with DCIS. Microcalcifications in DCIS are most commonly linear, linear branching, and fine pleomorphic, in a linear distribution. Other forms described in DCIS include the dot-dash pattern, consisting of round and needle-shaped calcifications.
The histological high-grade carcinoma or comedocarcinoma tends to be associated with linear, branching, and irregular calcifications that are in a linear or segmental distribution, formerly referred to as casting type of calcifications. These cancers may also be associated with pleomorphic or amorphous type of calcifications. In comedocarcinoma there is significant necrosis within the lumen of the duct that is involved with cancer. About 90 % of high-grade DCIS is associated with microcalcifications. The lower-grade or noncomedo DCIS is associated more often with clustered calcifications of amorphous or coarse heterogeneous morphology calcifications. Overall unlike the high-grade DCIS, the low-grade DCIS is less frequently associated with microcalcifications and reported in about 50 % of cases. Sometimes in DCIS one sees clustered fine pleomorphic or coarse heterogeneous calcifications, and these are often associated with necrotic tumors of the cribriform or micropapillary type [28]. The differential diagnosis for linear calcifications includes two important benign causes, secretory calcifications and vascular calcifications. Linear calcifications can be associated with benign secretory disease of the breast; these calcifications are often bilateral, regional, and seen in older women. When confined to a smaller region and unilateral, secretory calcifications are a challenge, these tend to be dense and have smooth margins [29]. Vascular calcifications when patchy and confined to one wall of a vessel may appear as a linear calcification. Magnification views help to identify the true nature of these benign vascular calcifications.
There have been reports attempting to correlate the appearance of microcalcifications with likelihood of invasive cancers [30]. In malignant calcifications without a focal mass, invasive foci are more likely when calcifications were larger than 11 mm and with linear calcifications than with granular calcifications [30]. Invasive cancers presenting as calcifications are often associated with high-grade DCIS and are also more likely to be Her2/Neu [human epidermal growth factor receptor 2]-negative cancers [2]. Invasive ductal cancers may also be associated with fine pleomorphic calcifications (Fig. 5.8). Invasive lobular cancer on the other hand is rarely associated with microcalcifications.

A 67-year-old with histologically proven invasive ductal cancer in the right breast. Spot compression magnification view demonstrates linear branching pleomorphic calcifications associated with an irregular mass
The morphologic types of calcifications that are suspicious for malignancy can be categorized as those with intermediate concern for cancer and those that have a higher probability of being associated with breast cancer [5] (Table 5.1).
Intermediate Concern for Malignancy
-
1.
Amorphous or indistinct calcifications are small and hazy in appearance; a specific morphologic classification cannot be given. The distribution of such calcifications determines degree of suspicion, when diffuse and scattered are benign, however when seen on a baseline mammogram magnification views are generally obtained. When these types of calcifications have a regional, linear, or segmental distribution, they are considered suspicious and an indication for biopsy.
-
2.
Coarse heterogeneous calcifications are irregular and larger than 0.5 mm and tend to be clustered. Such calcifications may be associated with malignancy and are also seen in benign lesions such as fibroadenomas, fibrosis, and trauma and in dystrophic calcifications.
Higher Probability of Malignancy
-
1.
Fine pleomorphic: These are calcifications smaller than 0.5 mm and are more clearly defined than the amorphous type and are irregular with varying sizes and shapes.
-
2.
Fine linear or fine-linear branching calcifications: These are thin linear or curvilinear irregular calcifications which may be discontinuous and smaller than 0.5 mm. This is suggestive of filling of the lumen of a duct by cancer cells (Fig. 5.9a, b).
Fig. 5.9 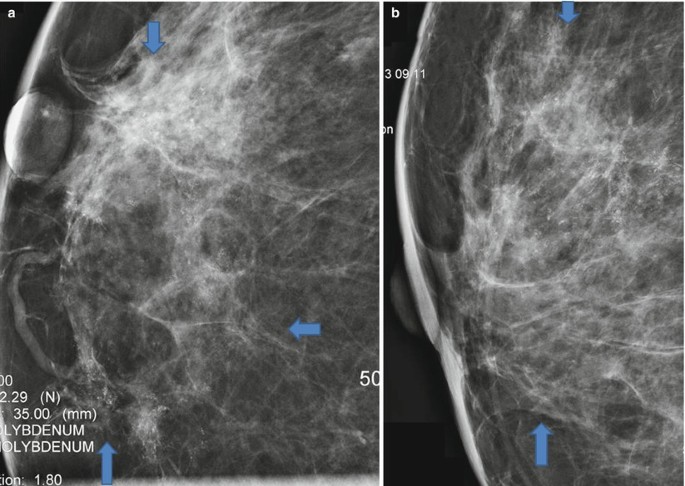
(a, b) A 53-year-old with extensive calcifications identified on a screening mammogram histologically proven to be DCIS. (a) Spot compression magnification views in the craniocaudal projection demonstrate linearly arranged clusters of microcalcifications in a segmental distribution extending to the nipple. (b) Spot compression magnification views in the mediolateral projection demonstrate linearly arranged clusters of microcalcifications in a segmental distribution extending to the nipple. Area of microcalcifications is outlined by arrows

Distribution of Calcifications
The distribution of calcifications is also an additional indicator of the likelihood of calcifications being associated with breast cancers:
-
1.
Diffuse and scattered calcifications are usually benign particularly when bilateral. Such a distribution is often seen with punctuate and amorphous calcifications.
-
2.
Regional calcifications may involve most of a quadrant or more than a single quadrant and do not conform to a duct distribution. Such a distribution is generally indicative of a benign etiology although careful assessment of the morphology may modify final assessment and the need for biopsy. Intermediate and high probability morphology even in such a distribution should prompt biopsy.
-
3.
Grouped or clustered calcifications are when five or more calcifications are seen in a small volume of breast tissue. These are generally considered suspicious.
-
4.
Linear distribution is when calcifications are arrayed in a line; such a distribution is highly suspicious for cancer and suggests that calcifications are intraductal.
-
5.
Segmental distribution of calcifications implies calcifications in ducts and their branches and may imply extensive or multifocal breast cancer in a lobe or segment of the breast. Except in the case of coarse rodlike calcifications in older women associated with secretory calcifications, segmental distribution is worrisome and should prompt a biopsy.
Focal Asymmetry
Focal asymmetry is a localized area of increased density that is visible as a confined asymmetry with similar shape in two views, but does not fit the criteria of a mass and lacks defined borders. In majority of cases it represents an island of normal breast tissue especially when there is interspersed fat. Focal asymmetry that is associated with a palpable finding, architectural distortion, or microcalcifications is worrisome for malignancy [5, 31]. Breast asymmetry is generally a result of localized distribution of fibroglandular parenchyma and unlike a mass tends to have concave borders and is interspersed with fat and not dense centrally like one sees in a mass. To appreciate breast asymmetry views of each breast are inspected side by side as is standard practice of viewing mammograms. There are four types of breast asymmetry described [32]:
-
Asymmetry of the breast is seen in one of two standard mammographic views, formerly referred to as a density. The likelihood of malignancy is slightly less than 2 %; nevertheless, Sickles rightly points out that it is not appropriate to categorize such findings as probably benign since 80 % of these asymmetries can be identified as summation artifact at screening or on additional evaluation and do not require short interval follow-up. The likelihood of malignancy for the remainder lesions is significantly higher [10.3 %], and thereby short interval follow-up is not justified [32, 33].
-
Global asymmetry is when there is substantially more tissue in one breast compared to the other and occupies at least one quadrant of the breast. When not associated with a palpable abnormality, this finding is benign, and when associated with a palpable finding, a small percentage (3 %) may be associated with breast cancer [34].
-
Focal asymmetry lacks convex borders of a mass and occupies less than one quadrant of the breast. The likelihood of malignancy for such a finding that is not associated with a mass, palpable finding, architectural distortion, calcifications, and sonographic correlate and with no prior mammograms to assess stability is less than 1 %.
-
A developing asymmetry is a focal asymmetry that is new or enlarging or denser when compared to prior mammogram (Fig. 5.10a–g). Unlike such developing focal asymmetry, hormone-induced developing asymmetry is bilateral and global. Infection, trauma, and surgery are other nonsuspicious causes of a developing asymmetry that can be excluded by clinical history [31]. Developing asymmetry is an uncommon finding and reported in 0.16 % of 180,801 screening mammograms and 0.11 % of 27,330 diagnostic mammograms. On a screening examination, the incidence of cancer in a developing asymmetry has been reported to be 12.8 %, and in those that are persistent after a diagnostic work-up, irrespective of the presence of a correlative physical finding, the reported cancer rate is as high as 26.7 % [35]. Therefore, an uncomplicated developing asymmetry that is persistent after a diagnostic work-up unless proven to be due to benign finding such as a cyst by ultrasound should be categorized as a BI-RADS 4 with a recommendation for biopsy. A normal ultrasound does not preclude recommendation for a biopsy. In one series of 300 nonpalpable cancers, 6 % were manifest as developing asymmetry [36].
Fig. 5.10 
(a–g) A 55-year-old with a new developing asymmetry that was subsequently proven to be invasive ductal carcinoma. (a) Left breast mediolateral oblique view obtained in August 2011 demonstrates a fat-replaced breast parenchymal pattern with no abnormal findings. (b) Left breast craniocaudal view obtained in August 2011 demonstrates no abnormal findings. (c) Left breast mediolateral oblique view obtained in August 2012 demonstrates a developing asymmetry in the posterior outer central breast. (d) Left breast craniocaudal view obtained in August 2012 demonstrates a developing asymmetry in the posterior outer central breast. (e) Spot compression mediolateral oblique view obtained in February 2013 demonstrates a high-density irregular mass in the posterior outer central breast. Patient had failed to return for a recommended diagnostic mammogram in August 2012. (f) Spot compression craniocaudal view obtained in February 2013 demonstrates a high-density irregular mass in the posterior outer central breast. (g) Ultrasound shows a solid mass with malignant features

Sonography is an appropriate work-up for a focal asymmetry that is persistent mainly to exclude an underlying mass. In one series sonography had a negative predictive value for breast cancer of 89.4 % (7/9 cancers detected). One palpable focal asymmetry without a sonographic correlate proved to be an invasive ductal cancer as did one without a palpable correlate. A negative sonography should not preclude biopsy in those with a palpable focal asymmetry. However, the presence of localized hyperechoic tissue matching an area of focal asymmetry is suggestive of a benign process [37]. See Fig. 5.11a–d.

(a–d) Small palpable invasive ductal cancer with subtle visibility on a screening mammogram. (a) Mediolateral view of left breast shows a questionable area of increased density in a breast with dense fibroglandular parenchyma. (b) Spot compression view in the craniocaudal projection reveals a small focal asymmetry. (c) Spot compression view in the mediolateral projection reveals a small focal asymmetry. (d) Ultrasound reveals a small solid mass with microlobulated borders and malignant features
In summary, most cases of asymmetry are due to a summation artifact and appropriately categorized as benign with a recommendation for routine follow-up. Those that are determined not to be a summation artifact after a diagnostic work-up and if new or enlarging or palpable following either a negative ultrasound examination or an ultrasound finding of an indeterminate mass get a category 4 assessment with a recommendation for a biopsy. Uncomplicated focal asymmetry seen on a baseline screening mammogram or when there are no prior mammograms available for comparison need to be worked up with diagnostic mammography and if persistent assessed by sonography; if there is no benign finding accounting for the focal asymmetry, the finding is considered probably benign with a recommendation for a short interval follow-up in 6 months. Uncomplicated global asymmetry does not require a diagnostic work-up and is assigned a BI-RADS 2 category with a recommendation for routine screening. Uncomplicated developing asymmetry is always recalled and if determined not to be due to summation or a sonographic benign correlate is categorized as a BI-RADS 4, with a recommendation for a biopsy. Asymmetry, global asymmetry, or a focal asymmetry associated with a palpable finding, architectural distortion, or suspicious microcalcifications is always an indication for biopsy.
One-View Density
Density that is visible on one view and defined as asymmetry is often due to summation artifact. Women are recalled for a diagnostic mammogram where supplemental views are obtained to exclude summation artifact as well as to identify a corresponding area on the orthogonal view. Two methods have been described to triangulate a lesion in two projections [38]. First is the arc method where the distance from the nipple to the density is used to form the radius of an arc with the nipple at its center. In the straight line method, the distance from the nipple to a perpendicular line passing through the density is measured. A corresponding density is sought in the orthogonal plane along the arc or the line; if none is found the finding is considered as an asymmetry. One-view asymmetry if not a summation artifact may be caused by an abnormality that is not included on the second view due to technical difficulties in including that area of the breast, such as lesions in the axillary fold, very medial in the chest, very posterior, or in the inframammary fold [38]. When a lesion is apparent only on the mediolateral oblique view, a straight mediolateral view has to be obtained to determine if the finding persists and its location in the breast. Lesions that are in the medial breast will move superiorly and those in the lateral breast will move inferiorly on the straight mediolateral views. Rolled views are obtained for lesions that are seen only in the craniocaudal view, to confirm that it is a real finding or not [39].
A new area of focal asymmetry is sometimes related to initiation of hormone replacement therapy [HRT]. In such cases repeat mammogram after cessation of HRT may demonstrate a resolution of the focal asymmetry. A developing asymmetry that may appear less prominent but persists following cessation of therapy could at least in theory represent an estrogen-sensitive breast cancer [31]. Short-term cessation of hormone replacement prior to performance of screening mammography has been suggested although patient compliance may be an issue; one study reported that a majority of women [54 %] were unwilling to stop HRT for 1–2 months prior to undergoing a screening mammogram [40]. There is no proven benefit in stopping HRT in all patients prior to screening mammography. No significant reduction in recall rate was seen in those in whom HRT was suspended for 1–2 months prior to screening mammography [41].
Subtle Cancers/Missed Cancers
The sensitivity of mammography, i.e., the percentage of cancers with a positive interpretation, was 83.5 % based on 1,960,150 screening examinations performed between 2002 and 2006 [42]. Mammography misses 10–30 % of breast cancers [43]. Some of these cancers are truly occult, while others are missed due to perceptual error, interpretive error, or to limitation of the modality and/or technique such as dense breast parenchyma obscuring a lesion and poor positioning or technique [43]. Known pitfalls cited for missing a potential breast cancer on a screening mammogram include edge of the film findings, findings that are suspicious but stable, slowly developing asymmetry, architectural distortion, a finding seen on one-view only, benign-appearing nodule, presumed intramammary lymph node, shrinking breast, and scar carcinoma [44].
An edge of the image finding may also be due to lack of inclusion of the entire breast and should prompt recall and work-up to identify the lesion in orthogonal plane and if determined to be a true finding will need supplemental imaging with ultrasound. Another reason for failure to diagnose a breast cancer results from equating lesion stability with a benign process. Stable findings do not confirm benignity when morphological features are worrisome such as a mass with ill-defined borders or calcifications that have a suspicious distribution and/or morphology. A biopsy recommendation is appropriate after a diagnostic work-up for such lesions even if stability has been shown for 2–3 years. Architectural distortion when not associated with a mass particularly in a heterogeneously dense breast may be subtle and difficult to perceive or simulate the crisscrossing lines of normal breast parenchyma. Computer-aided detection [CAD] used to assist in lesion detection also tends to have low sensitivity for areas of architectural distortion. Certain cancers such as medullary, mucinous, and papillary cancers may appear as circumscribed masses that may appear benign and hence incorrectly categorized as benign and/or probably benign; such masses often reveal ill-defined borders on supplemental compression and magnification views. Close inspection of margin characteristics on ultrasound will often reveal suspicious morphology.
On occasion a small low-density nodule with a shallow notch may be presumed to be a lymph node and not be worked up. It is important to ensure that a fatty hilum is seen and that this finding is in the upper outer quadrant of the breast; multiplicity and bilaterality of such findings is also suggestive of intramammary lymph nodes. When masses appearing like lymph nodes are seen in locations that are not typical for lymph nodes such as in the inner breast, recall for a mammographic work-up, and identification of the sonographic correlate of a hyperechoic hilum is warranted to confirm the diagnosis of a benign intramammary lymph node. Although quite rare to develop at the site of a benign biopsy, it is not uncommon for recurrence of breast cancer to occur at the site of scar; careful analysis to look for increasing density, size, increasing convexity, or architectural distortion is required [44].
Findings seen in one view can also be problematic and a frequent reason for missing a breast cancer at screening mammography (Fig. 5.12a–c). About 3.3 % of such one-view findings have been reported in a series of 61,273 screening studies. A majority of these [82.7 %] are due to summation artifacts without a need for recall. There were 36 cancers, with a finding that was visible on one view only. An unusually large percentage of such missed cancers [33 %] were invasive lobular cancers; the remainder were DCIS [6 %] and invasive ductal cancers [18 %]. A large majority of these findings were density [84.8 %]; others included architectural distortion [10.7 %], calcifications [4.1 %], and combination [0.3 %]. Most one-view findings are seen on the MLO view since it includes more fibroglandular tissue than the CC view, with the exception of ILC which is often best seen on the CC view [33].

(a–c) Small invasive ductal cancer visible on one view. Ultrasound (not shown) confirmed a 7 mm solid mass in the upper inner left breast. (a) Craniocaudal view shows a small round irregular density in the inner left breast (arrow). (b) Mediolateral view does not show a corresponding finding. (c) Mediolateral oblique view of the upper breast fails to demonstrate the cancer
Poor mammographic technique and/or positioning can be an important cause of missing a breast cancer on a screening study. On occasion cancer may not be included on the mammographic views due to its location; this may happen particularly for those in the far medial breast or along the inframammary fold (Fig. 5.13a–d). Motion blurring, for instance, can mask out calcifications, small densities, and small areas of architectural distortion. Up to 62 % of breast cancers that presented as microcalcifications were not biopsied and were attributed to blurring on magnification views [43]. A detailed description of and the importance of optimal technique and positioning is discussed elsewhere in this textbook.

(a–d) A palpable invasive ductal cancer mammographically occult in a fatty breast with failure to image the cancer due to its location. (a) Mediolateral oblique view does not show the palpable mass. (b) Spot compression view in the mediolateral view of the palpable finding fails to show the mass. (c) Spot compression view of the medial breast in the area of the palpable finding fails to show the mass. (d) Ultrasound demonstrates a large malignant-appearing mass close to the chest wall
Incorrect interpretation of a mammographic finding may be attributed to a lack of experience as in the case of general radiologist who may read a low number of mammograms or may be due to fatigue. Slow growing lesions or the absence of prior mammograms for comparison also increases the likelihood of misinterpreting subtle signs of a breast cancer [43]. Failure to adequately work up findings such as margin evaluation by spot compression views leads to erroneous interpretation of a mass with fine irregular margins as having a circumscribed border. In order to ensure that small cancers or cancers with subtle findings are not missed, careful and methodical inspection of mammograms comparing similar views of the right and left breast, looking for subtle asymmetry and changes from priors, and use of magnifying device to carefully evaluate the entire mammogram are needed. This will minimize the chances of missing subtle potential signs of breast cancer.
Meticulous attention to quality assurance and quality control to ensure proper positioning to include the entire breast, optimizing mammographic technical factors, and above all repeating mammograms that are blurred are also critical to avoid missing cancers with subtle signs.
A multi-institutional retrospective study examined the nonspecific findings on prior mammograms at locations where breast cancer subsequently developed. One unblinded radiologist determined that 286 findings of 493 examinations were deemed to be visible in retrospect at sites where cancer later developed. However, among a group of five blinded radiologists who reviewed these mammograms, none or only one or two of the radiologists recommended recall from screening [45]. The most frequent findings among interpretation factors were benign-appearing tissues, benign-appearing calcifications, or too few calcifications. Among detection errors the most common were findings seen only on one view, overlooked calcifications, or findings at the edge of the glandular tissue. This study showed that a proportion of breast cancers display nonspecific mammographic findings that may not warrant recall and failure to act on such perceptible but nonspecific findings do not constitute interpretation below the standard of care. Berlin points out that during disposition of a malpractice claim, it is the testimony of individual experts that matters and majority votes of groups of expert witnesses are not considered in determining whether a defendant radiologist has or has not breached the standard of care [46]. In a comparison of retrospective versus blinded review of mammograms obtained prior to a diagnosis of impalpable breast cancers, in 30 patients [41 % of cancers] evidence of cancer was shown by blinded reviewers; however, in the remaining 43 patients [59 %] of those with cancers, the prior mammograms were read as negative or benign [47]. However, the retrospective reviewers thought that there was evidence of cancer in 25 of these patients. The majority of these findings that were called abnormal on a retrospective review were focal asymmetries. These authors concluded that impalpable cancers are frequently visible in retrospect on prior mammograms; however, since most are visible as an asymmetric density, these are not true radiologic errors. In a medical malpractice case of missed breast cancer, most experts testifying against a defendant radiologist are in essence performing a retrospective review having the benefit of knowing the diagnosis and location of the missed cancer. Retrospective reviews of this nature do not actually reflect the everyday practice of screening mammography; failure to detect or act upon a retrospectively evident finding should therefore not be considered as necessarily negligent [47].
The use of computer-aided detection (CAD) has been shown to decrease false-negative rate of mammography [48, 49]. In one study CAD decreased the false-negative rate at double reading by more than a third [31–19 %]. CAD system correctly marked 37 of 52 actionable findings that were read as negative in previous screening mammograms [48]. In another study CAD marked 42 % of 172 findings that subsequently developed cancer. Although CAD seemingly finds cancers that are subtle and missed, it can also lead to increased recall and biopsies [49]. A meta-analysis of studies looking at the value of CAD as a supplement to screening mammography showed that CAD yielded an additional 50 cancers in 100,000 women screened, but also led to recalls in 1,190 healthy women and 80 biopsies in healthy women. Ninety-six percent of women recalled based upon CAD and 65.1 % of women biopsied based upon CAD were healthy [50].
Missed cancers can be attributed to reader factors as well as due to subtle signs. The former may be a perceptual difference as in a cancer with subtle signs or interpretive errors. Suboptimal technique such as improper positioning and/or technical factors can also lead to decreased conspicuity of the cancer leading to a missed diagnosis [51]. Cancers in certain locations such as in the axillary tail or in the inframammary fold are often seen only on one view making their diagnosis challenging [52]. Some have reported that a significant number of missed cancers, up to a third, are in the retroglandular region of the breast [53], while others have found no statistically significant t difference in the location of missed cancers [54].
Uncommon Mammographic Signs of Breast Cancer
Solitary Dilated Duct
In the BI-RADS atlas, a solitary duct is described as a special case. Ducts are usually seen as tubular densities in a subareolar location; when prominent and bilateral, it is a benign finding indicative of duct ectasia. Wolfe has described a unilateral dilated duct as a possible sign of breast cancer [55]. One series looked at all cases of asymmetrically dilated ducts in a nonsubareolar location and found cancers in 11 [24 %] of 46 cases. Six [54 %] of these 11 cases had suspicious microcalcifications. They concluded that asymmetrically dilated ducts in a nonsubareolar location when associated with suspicious microcalcifications and/or interval change warrant biopsy [56].
Nevertheless the finding of a solitary dilated duct that is not associated with a mass, calcifications, or architectural distortion is exceedingly rare [57]. Only 21 [0.0079 %] cases were recorded for 264,476 consecutive mammography examinations. Ten were stable on follow-up for 2 years and presumed benign; 11 underwent biopsy. Among these there were two cancers, both DCIS [57]. Since the likelihood of malignancy is greater than 2 %, a BI-RADS 4 assessment may be warranted for this rare finding on mammography [57].
Diffuse Skin Thickening
Breast infection can demonstrate mammographic signs that mimic inflammatory breast cancer, namely, skin thickening, diffuse increase in density, irregular mass, and uncommonly architectural distortion. Mammography shows an abnormality in a significant number of patients with breast infection with sonography depicting an abscess in most cases when present [58]. The presence of diffuse breast thickening and of dense lymph nodes is suggestive of an underlying carcinoma. Diffuse skin thickening is rarely seen in unusual breast infections [58].
Breast skin thickening and edema may be caused by a variety of causes including mastitis, inflammatory breast cancer, lymphatic obstruction, lymphoma, postradiation changes, congestive heart failure, or nephritic syndrome [59] (Box 5.3). Granulomatous mastitis is a rare inflammatory disease of unknown origin that can mimic cancer. There is an association with oral contraceptive use. Pathologically it is characterized by granulomatous inflammation of the lobules with noncaseating granulomas. Mammographically peripheral areas of focal asymmetry are seen. Sonography demonstrated clustered tubular hypoechoic areas. Excisional biopsy with or without steroids may be needed, with local recurrence following excision having been reported [60, 61].
Box 5.3. Differential Diagnosis of Diffuse Skin Thickening of the Breast
1. Mastitis |
2. Lymphatic obstruction |
3. Lymphoma |
4. Postradiation |
5. Inflammatory breast cancer |
6. Nephritic syndrome [bilateral] |
7. Congestive heart failure [bilateral] |
Inflammatory Breast Cancer
Inflammatory breast cancer is a rare but highly aggressive form of breast cancer and accounts for 1–6 % of breast cancer cases [62–64]. Prognosis is often poor due to the fact that micrometastasis is present at the time of diagnosis. Distant metastasis is present in 20 % of cases at the time of diagnosis, and the mean 5-year survival rate with modern multidisciplinary therapy is 20–40 %. Patients present with rapid onset of swelling and enlargement of the breast with skin erythema. A peau d’orange texture of the skin is caused by dermal edema resulting from lymphatic obstruction by tumor emboli. Tenderness, induration, and warmth are clinically apparent, and a palpable mass may or may not be present. IBC usually represents a poorly differentiated invasive ductal cancer.
Mammographic findings are seen in a majority of patients and include diffuse skin thickening, trabecular thickening, increased density, a mass, architectural distortion, and or calcifications [65–73]. Mammographic findings of a mass or calcifications are seen in 80–95 % of cases (Fig. 5.14a–c) [65, 66]. MRI has been reported to be the most accurate technique in detecting a breast parenchymal lesion in IBC patients [65]. The differential diagnosis of IBC is locally advanced breast cancer, primary breast lymphoma, and nonpuerperal mastitis, all of which are characterized by diffuse skin thickening, breast enlargement, and increased breast density [64].

(a–c) Inflammatory breast cancer in a 54-year-old woman. (a) Left mediolateral oblique view shows a large irregular focal asymmetry associated with suspicious-appearing microcalcifications. (b) Left craniocaudal view shows a large irregular focal asymmetry associated with suspicious-appearing microcalcifications and diffuse skin thickening. (c) Ultrasound demonstrates a large irregular malignant-appearing mass
Isolated Enlarged Lymph Nodes
In the BI-RADSTM atlas axillary adenopathy is included under associated findings with a guidance statement that reads “enlarged non fatty replaced axillary lymph nodes can be commented upon, mammographic assessment of these nodes is unreliable” [5]. The criteria to classify a lymph node as abnormal include a rounded shape, size > 2 cm, increased density, and absence of fatty hilum [74]. Unilaterally enlarged lymph nodes may be due to an underlying malignancy most commonly breast cancer, other malignancies, or non-neoplastic causes [74–80]. These may include those patients in whom enlarged lymph nodes are not associated with an underlying mammographic abnormality and represent an isolated finding. The malignancy rate reported in such instances varies from 33.3 to 52.3 %; sonographic evaluation of such abnormal lymph nodes identified at screening mammography has been shown to be useful in reducing false-positive and improving positive predictive value for biopsy [74]. The most common cause would be an occult breast primary; other causes would include lymphoma, metastasis from malignant melanoma, and lung, stomach, or ovarian carcinoma. Benign causes would include systemic inflammatory diseases such as sarcoidosis, infectious diseases such as tuberculosis, collagen vascular diseases, and miscellaneous causes such as silicone granulomas [74–78]. MRI is recommended in patients with isolated enlarged lymph nodes and a mammographically occult primary [81–83].
Triple-Negative Breast Cancers
Triple-negative breast cancers are a subgroup of breast cancers that do not express estrogen receptors (ER), progesterone receptors (PR), or human epidermal growth factor receptor 2 (HER 2). This particular phenotype of breast cancer has aggressive tumor biology and a higher degree of association with suppression of BRCA 1 function and a consequent poor prognosis. Triple-negative breast cancer (estrogen receptor-negative, progesterone receptor-negative, and HER2-negative) is a high-risk breast cancer that cannot be treated with drugs that target these proteins. Triple-negative breast cancers accounts for 11–20 % of all subtypes of breast cancer and accounts for 23–38 % of locally advanced disease [84]. Women with triple-negative tumors tend to be younger, more likely African-American, and overweight. Triple-negative cancers and HER 2+ cancers are less likely to be detected by screening mammography and less likely to be present as TI [46.5 %] or diagnosed as Stage 1 [32.6 %]. TN tumors are often high grade [83 %] and invasive [93 %] [84]. Despite the large size at the time of diagnosis, up to 28.9 % of TNBC may be mammographically occult. The most common presentation on a mammography is as a mass which is circumscribed in 20–24 % of cases and with absence of calcifications in 49–100 % of cases [84–88].
Triple-negative breast cancers may lack the common and typical features on mammography that are encountered with breast cancer such as irregular masses, spiculation, or malignant-appearing calcifications. Mammography may hence be of limited value in screening women who are at risk to develop TNBC. Ultrasound has a higher sensitivity than mammography; however, in a substantial number of cases masses may exhibit benign features (21–41 % of cases). MRI has a higher sensitivity than either mammography or ultrasound and has been proposed as a modality of choice for establishing baseline prior to neoadjuvant chemotherapy [85–87]. In one series ultrasound found all 88 of TN cancers, most frequently as masses [92.5 %]; posterior acoustic enhancement was seen in 41.6 % of TN tumors, and posterior acoustic attenuation was seen in only in 8.7 % of cases. An elasticity score of 4 or 5 was noted on elastography in 87.5 % of tumors [88]. Triple-negative DCIS present mammographically as calcifications less commonly than non-TN DCIS, 22 % in one series. They more commonly appeared as masses or focal asymmetry. Triple-negative DCIS are rare, reported in 3.6 % in one series of 494 cases [89] (Fig. 5.15a, b).

(a, b) A 47-year-old woman with a triple-negative ductal carcinoma in situ with an invasive component. (a) Spot magnification view in the mediolateral projection shows a small irregular mass with clustered pleomorphic calcifications. (b) Spot magnification view in the craniocaudal projection shows a small irregular mass with clustered pleomorphic calcifications
Invasive Lobular Cancer
Invasive lobular cancer accounts for 10–15 % of invasive breast cancers. ILC has a higher rate of multiplicity and bilaterality, despite which tends to have a better prognosis than invasive ductal cancers [14]. These cancers can be difficult to detect at mammography due to the fact that the opacity may be equal to or lower than normal fibroglandular tissue due to lack of incitement of a desmoplastic reaction. Mammographically they are often seen only on one view, often on the craniocaudal projection. These cancers often fail to form discrete palpable masses and hence may also remain occult to clinical examination [14]. Up to 19 % of false-negative rates are reported for ILC at mammography because of difficulty in mammographic detection [90, 91]. Ultrasound is superior to mammography in detecting multifocality and multicentricity of ILC. The size of tumor is more accurately assessed by sonography. The sensitivity of US for detection of ILC ranges from 68 to 98 %. Ultrasound is also a valuable adjunct to mammography to biopsy and preoperatively localizes ILC particularly when seen only on one view [14, 92].
Mammographic Features of ILC
The reported sensitivity of mammography is 57–81 % [14, 90, 93, 94]. ILC is most commonly seen on a mammogram as a mass [44–65 %] usually with spiculated margins. Architectural distortion is the next most common mammographic pattern [10–34 % of cases] followed by focal asymmetry [1–14 % of cases]. Calcifications are less commonly associated with a reported association in 0–24 % of cases [14, 90, 93, 94]. Round and circumscribed masses are uncommon and seen only in 1–3 % of cases [14, 95]. In a series of 49 patients with ILC, masses were seen in 43 % of cases, architectural distortion in 20 %, and asymmetries in 18 %. Surprisingly in 16 % of patients ILC was associated with microcalcifications. Normal or benign findings were seen in 10 % of cases [14]. The most common US manifestation of ILC is solid hypoechoic and heterogeneous mass with irregular or angular or spiculated borders and posterior acoustic shadowing seen in 54–61 % of cases [92, 95–97]. ILC can also appear on ultrasound as a circumscribed mass, an area of focal shadowing without a discreet mass, or be sonographically occult [95] (Fig. 5.16a–i).



(a–i) A 56-year-old woman with a palpable lump in right breast histologically proven to be infiltrating lobular cancer. (a) Mediolateral oblique view demonstrates an area focal asymmetry (arrow) in the upper right breast adjacent to the implant corresponding to the palpable finding. (b) Craniocaudal view of the right breast demonstrates no abnormal finding. (c) Ultrasound shows a large irregular malignant-appearing mass adjacent to the implant. (d) Ultrasound shows a large irregular malignant-appearing mass adjacent to the implant. (e) Mediolateral oblique view obtained at the end of 3 months of chemotherapy reveals near-complete resolution of the focal asymmetry. A post biopsy clip is visible. (f) Ultrasound obtained at the end of 3 months of chemotherapy reveals near-complete resolution of the focal asymmetry. A post biopsy clip is visible. (g) Post gadolinium sagittal T1-weighted fat-suppressed MRI image of the right breast demonstrates an enhancing cancer superior to the implant. (h) Subtracted image reveals the enhancing cancer in right breast. (i) Axial MRI CAD image demonstrates the enhancing tumor in the right breast
References
Venkatesan A, Chu P, Kerlikowske K, Sickles E, Smith-Bindman R. Positive predictive value of specific mammographic findings according to reader and patient variables. Radiology. 2009;250(3):648–57.
Gajdos C, Tartler PI, Bleiweiss IJ. Mammographic appearance of nonpalpable breast cancer reflects pathologic characteristics. Ann Surg. 2002;235(2):246–51.
Liberman L, Abramson AF, Squires FB, Glassman JR, Morris EA, Dershaw DD. The breast imaging reporting and data system: positive predictive value of mammographic features and final assessment categories. AJR Am J Roentgenol. 1998;171(1):35–40.
Sickles EA. Breast masses: mammographic evaluation. Radiology. 1989;173(2):297–303.
American College of Radiology. Breast imaging reporting and data system (BI-RADS). 4th ed. Reston: American College of Radiology; 2003.
Woods RW, Sisney GS, Salkowski LR, Shinki K, Lin Y, Burnside ES. The mammographic density of a mass is a significant predictor of breast cancer. Radiology. 2011;258(2):417–25.
Woods RW, Oliphant L, Shinki K, Page D, Shavlik J, Burnside E. Validation of results from knowledge discovery: mass density as a predictor of breast cancer. J Digit Imaging. 2010;23(5):554–61.
Tamaki K, Ishida T, Miyashita M, Amari M, Ohuchi N, Tamaki N, Sasano H. Correlation between mammographic findings and corresponding histopathology: potential predictors for biological characteristics of breast diseases. Cancer Sci. 2011;102(12):2179–85.
Thurfjell MG, Lindgren A, Thurfjell E. Nonpalpable breast cancer: mammographic appearance as predictor of histologic type. Radiology. 2002;222(1):165–70.
Reiff DB, Cooke J, Griffin M, Given-Wilson R. Ductal carcinoma in situ presenting as a stellate lesion on mammography. Clin Radiol. 1994;49:396–9.
Thurfjell E, Thurfjell MG, Lindgren A. Mammographic finding as predictor of survival in 1–9 mm invasive breast cancers. Worse prognosis for cases presenting as calcifications alone. Breast Cancer Res Treat. 2001;67(2):177–80.
Ikeda DM, Anderson I. Ductal carcinoma in situ: atypical mammographic appearances. Radiology. 1989;172:661–9.
Sekine K, et al. DCIS showing architectural distortion on screening mammogram – comparison of mammographic and pathological findings. Breast Cancer. 2007;14(3):281–4.
Lopez JK, Bassett LW. Invasive lobular carcinoma of the breast: spectrum of mammographic, US, and MR imaging findings. Radiographics. 2009;29:165–76.
Tabar L, Dean PB. Stellate lesions. In: Tabar L, Dean PB, editors. Teaching atlas of mammography. Second revised. New York: Georg Thieme Verlag; 1985. p. 87–136.
Kennedy M, Masterson AV, Kerin M, Flanagan F. Pathology and clinical relevance of radial scars: a review. J Clin Pathol. 2003;56(10):721–4.
Neilsen M, Christensen L, Anderson J. Radial scars in women with breast cancer. Cancer. 1987;59:1019–25.
Ciatto S, Morrone D, Catarzi S, et al. Radial scars of the breast: review of 38 consecutive mammographic diagnoses. Radiology. 1993;187:757–60.
King TA, Scharfenberg JC, Smetherman DH, et al. A better understanding of the term radial scar. Am J Surg. 2000;180(6):428–32.
Cohen MA, Sferlazza SJ. Role of sonography in evaluation of radial scars of the breast. AJR Am J Roentgenol. 2000;174:1075–8.
Shetty MK. Radial scars of the breast: sonographic findings. Ultrasound Q. 2002;18(3):203–7.
Finlay ME, Liston JE, Lunt LG, et al. Assessment of the role of ultrasound in the differentiation of radial scars and stellate carcinomas of the breast. Clin Radiol. 1994;49:52–5.
Shaheen R, Schimmelpenninck CA, Stoddart L, Raymond H, Slanetz PJ. Spectrum of diseases presenting as architectural distortion on mammography: multimodality radiologic imaging with pathologic correlation. Semin Ultrasound CT MR. 2011;32(4):351–62.
Taşkin F, Köseoğlu K, Unsal A, Erkuş M, Ozbaş S, Karaman C. Sclerosing adenosis of the breast: radiologic appearance and efficiency of core needle biopsy. Diagn Interv Radiol. 2011;17(4):311–6.
Günhan-Bilgen I, Memiş A, Ustün EE, Ozdemir N, Erhan Y. Sclerosing adenosis: mammographic and ultrasonographic findings with clinical and histopathological correlation. Eur J Radiol. 2002;44(3):232–8.
Hogge JP, Robinson RE, Magnant CM, Zuurbier RA. The mammographic spectrum of fat necrosis of the breast. Radiographics. 1995;15(6):1347–56.
DiPiro PJ, Meyer JE, Frenna TH, Denison CM. Seat belt injuries of the breast: findings on mammography and sonography. AJR Am J Roentgenol. 1995;164(2):317–20.
Demitri-Lewis A, Slaentz PJ, Eisneberg RL. Breast calcifications: the focal group. AJR Am J Roentgenol. 2012;198:W325–43.
Bird RE. Critical pathways in analyzing breast microcalcifications. Radiographics. 1995;15:928–34.
Stomper PC, Geradts J, Edge SB, Levine EG. Mammographic predictors of the presence and size of invasive carcinomas associated with malignant microcalcifications lesions without a mass. AJR Am J Roentgenol. 2003;181:1679–84.
Samardar P, Shaw de Paredes E, Grimes MM, Wilson JD. Focal asymmetric densities seen at mammography: US and pathologic correlation. Radiographics. 2002;22:19–33.
Sickles EA. The spectrum of breast asymmetries: imaging features, work-up, management. Radiol Clin North Am. 2007;45(5):765–71.
Sickles EA. Findings at mammographic screening on only one standard projection: outcomes analysis. Radiology. 1998;208(2):471–5.
Kopans DB, Swan CA, White G, et al. Asymmetric breast tissue. Radiology. 1989;171(3):639–43.
Leung JWT, Sickles EA. Developing asymmetry identified on mammography: correlation with imaging outcome and pathologic findings. AJR Am J Roentgenol. 2007;188(3):667–75.
Sickles EA. Mammographic features of 300 consecutive nonpalpable breast cancers. AJR Am J Roentgenol. 1986;146:661–3.
Shetty MK, Watson AB. Sonographic evaluation of focal asymmetric density of the breast. Ultrasound Q. 2002;18(2):115–21.
Youk JH, Kim E, Ko KH, et al. Asymmetric mammographic findings based on the fourth edition of BI-RADS: types, evaluation, and management. Radiographics. 2009;29(1):1–48.
Brenner RJ. Strategies in the evaluation of breast asymmetries. Appl Radiol. 1998;27:15–20.
Reed SD, Buist DS, Anderson ML, Bowles EJ, Fitzgibbons D, Seger D, Newton KM. Short-term (1–2 mo) hormone therapy cessation before mammography. Menopause. 2009;16(6):1125–31.
Buist DS, Anderson ML, Reed SD, Aiello Bowles EJ, Fitzgibbons ED, Gandara JC, Seger D, Newton KM. Short-term hormone therapy suspension and mammography recall: a randomized trial. Ann Intern Med. 2009;150(11):752–65.
Performance measures for 1,960,150 screening mammography examinations from 2002 to 2006 by age – based on BCSC data as of 2009 NCI-funded Breast Cancer Surveillance Consortium co-operative agreement (U01CA63740, U01CA86076, U01CA86082, U01CA63736, U01CA70013, U01CA69976, U01CA63731, U01CA70040). Downloaded from the Breast Cancer Surveillance Consortium Web site. http://breastscreening.cancer.gov/data/performance/screening/2009/perf_age.html.
Majid AS, Parades ES, Doherty RD, Sharma NR, Salvador X. Missed breast carcinoma: pitfalls and pearls. Radiographics. 2003;23:881–95.
Roberts-Klein S, Iuanow E, Slaentz PJ. Avoiding pitfalls in mammographic interpretation. Can Assoc Radiol J. 2011;62:50–9.
Ikeda DM, Birdwell RL, O’Shaughnessy KF, Brenner RJ, Sickles EA. Analysis of 172 subtle findings on prior normal mammograms in women with breast cancer detected at follow-up screening. Radiology. 2003;226:494–503.
Berlin L. Missed mammographic abnormalities, malpractice, and expert witnesses: does majority rule in the courtroom? [letter]. Radiology. 2003;229:288–9.
Harvey JA, Fajardo LL, Innis CA. Previous mammograms in patients with impalpable breast carcinoma: retrospective vs blinded interpretation. 1993 ARRS President’s Award. Am J Roentgenol. 1993;161:1167–72.
Destounis SV, DiNitto P, Logan-Young W, Bonaccio E, Zuley ML, Willison KM. Can computer-aided detection with double reading of screening mammograms help decrease the false-negative rate? Initial experience. Radiology. 2004;232(2):578–84.
Ikeda DM, Birdwell RL, O’Shaughnessy KF, Sickles EA, Brenner RJ. Computer-aided detection output on 172 subtle findings on normal mammograms previously obtained in women with breast cancer detected at follow-up screening mammography. Radiology. 2004;230(3):811–9.
Noble M, Bruening W, Uhl S, Schoelles K. Computer aided detection mammography for breast cancer screening: systematic review and meta-analysis. Arch Gynecol Obstet. 2009;279(6):881–90.
Giess CS, Frost EP, Birdwell RL. Difficulties and errors in diagnosis of breast neoplasms. Semin Ultrasound CT MR. 2012;33:288–99.
Brenner RJ. False-negative mammograms: medical, legal, and risk management implications. Radiol Clin North Am. 2000;38:741–57.
Bird RE, Wallace TW, Yankaskas BC. Analysis of cancers missed at screening mammography. Radiology. 1992;184:613–7.
Goergen SK, Evans J, Cohen GP, et al. Characteristics of breast carcinomas missed by screening radiologists. Radiology. 1997;204:131–5.
Wolfe JN. Mammography: ducts as a sole indicator of breast carcinoma. Radiology. 1967;89:206–10.
Huynh PT, Parellada JA, de Paredes ES, et al. Dilated duct pattern at mammography. Radiology. 1997;204:137–41.
Chang CB, Lvoff NM, Leung JW, et al. Solitary dilated duct identified at mammography: outcomes analysis. AJR Am J Roentgenol. 2010;194:378–82.
Crowe DJ, Helvie MA, Wilson TE, Crowe DJ. Breast infection. Mammographic and sonographic findings with clinical correlation. Invest Radiol. 1995;30(10):582–7.
Kwak JY, Kim EK, Chung SY, You JK, Oh KK, Lee YH, et al. Unilateral breast edema: spectrum of etiologies and imaging appearances. Yonsei Med J. 2005;46:1–7.
An YY, Kim SH, Cha ES, et al. Diffuse infiltrative lesion of the breast: clinical and radiologic features. Korean J Radiol. 2011;12(1):113–21.
Han BK, Choe YH, Park JM, Moon WK, Ko YH, Yang JH, et al. Granulomatous mastitis: mammographic and sonographic appearances. AJR Am J Roentgenol. 1999;173:317–20.
Levine PH, Steinhorn SC, Ries LG, Aron JL. Inflammatory breast cancer: the experience of the surveillance, epidemiology, and end results (SEER) program. J Natl Cancer Inst. 1985;74:291–7.
Chang S, Parker SL, Pham T, Buzdar AU, Hursting SD. Inflammatory breast carcinoma incidence and survival: the surveillance, epidemiology, and end results program of the National Cancer Institute, 1975–1992. Cancer. 1998;82:2366–72.
Hance KW, Anderson WF, Devesa SS, Young HA, Levine PH. Trends in inflammatory breast carcinoma incidence and survival: the surveillance, epidemiology, and end results program at the National Cancer Institute. J Natl Cancer Inst. 2005;97:966–75.
Yang WT, Le-Petross HT, Macapinlac H, et al. Inflammatory breast cancer: PET/CT, MRI, mammography, and sonography findings. Breast Cancer Res Treat. 2008;109(3):417–26.
Dershaw DD, Moore MP, Liberman L, et al. Inflammatory breast carcinoma: mammographic findings. Radiology. 1994;190:831–4.
Lee B, Tannenbaum N. Inflammatory carcinoma of the breast: a report of twenty-eight cases from the breast clinic of memorial hospital. Surg Gynecol Obstet. 1924;39:580–5.
Droulias CA, Sewell CW, McSweeney MB, et al. Inflammatory carcinoma of the breast: a correlation of clinical, radiologic and pathologic findings. Ann Surg. 1976;184:217–22.
Gunhan-Bilgen I, Ustun EE, Memis A. Inflammatory breast carcinoma: mammographic, ultrasonographic, clinical, and pathologic findings in 142 cases. Radiology. 2002;223:829–38.
Kushwaha AC, Whitman GJ, Stelling CB, et al. Primary inflammatory carcinoma of the breast: retrospective review of mammographic findings. AJR Am J Roentgenol. 2000;174:535–8.
Caumo F, Gaioni MB, Bonetti F, et al. Occult inflammatory breast cancer: review of clinical, mammographic, US and pathologic signs. Radiol Med (Torino). 2005;109:308–20.
Tardivon AA, Viala J, CorvellecRudelli A, et al. Mammographic patterns of inflammatory breast carcinoma: a retrospective study of 92 cases. Eur J Radiol. 1997;24:124–30.
Lee KW, Chung SY, Yang I, et al. Inflammatory breast cancer: imaging findings. Clin Imaging. 2005;29(22–250):1014–24.
Shetty MK, Carpenter WS. Sonographic evaluation of isolated abnormal axillary lymph nodes identified on mammograms. J Ultrasound Med. 2004;23(1):63–71.
Given-Wilson RM, Murray ME. The clinical importance of axillary lymphadenopathy detected on screening mammography. Clin Radiol. 1997;52:458–61.
Bergvist L, Frodis E, Hedborg-Mellander C, Hansen J. Management of accidentally found pathological lymph nodes on routine screening mammography. Eur J Surg Oncol. 1996;22:250–3.
Lee LH, Giurescu ME, Philpotts LE, Horvath LJ, Tocino I. Clinical importance of unilaterally enlarging lymph nodes on otherwise normal mammograms. Radiology. 1997;203:329–34.
Görkem SB, O’Connell AM. Abnormal axillary lymph nodes on negative mammograms: causes other than breast cancer. Diagn Interv Radiol. 2012;18(5):473–9.
Walsh R, Kornuguth PJ, Soo MS, Bentley R, Delong DM. Axillary lymph nodes: mammographic, pathologic and clinical correlation. AJR Am J Roentgenol. 1997;168:33–8.
Rahbar H, Partridge SC, Javid SH, Lehman CD. Imaging axillary lymph nodes in patients with newly diagnosed breast cancer. Curr Probl Diagn Radiol. 2012;41(5):149–58.
Morris EA, Schwartz LH, Dershaw DD, Van Zee KJ, Abramson AF, Liberman L. MR imaging of the breast in patients with occult primary breast carcinoma. Radiology. 1997;205:437–40.
Tilanus-Linthorst MM, Obdeijn AI, Bontenbal M, Oudkerk M. MRI in patients with axillary metastases of occult breast carcinoma. Breast Cancer Res Treat. 1997;44:179–82.
Obdeijn IM, Brouwers-Kuyper EM, Tilanus-Linthorst MM, Wiggers T, Oudkerk M. MR imaging-guided sonography followed by fine-needle aspiration cytology in occult carcinoma of the breast. AJR Am J Roentgenol. 2000;174:1079–84.
Lin NU, Vanderplas A, Hughes ME, et al. Clinicopathological features and sites of recurrence according to breast cancer subtype in the National Comprehensive Cancer Network (NCCN). J Clin Oncol. 2009;27(15s):Abstr 543.
Yang WT, Dryden M, Broglio K, et al. Mammographic features of triple receptor negative primary breast cancers in young premenopausal women. Breast Cancer Res Treat. 2008;111:405–10.
Wang Y, Ikeda DM, Narasimhan B, et al. Estrogen receptor-negative invasive breast cancer: imaging features of tumors with and without human epidermal growth factor receptor type 2 over expression. Radiology. 2008;246:367–75.
Dogan BE, Gonzalez-Angulo AM, Gilcrease M, et al. Multimodality imaging of triple receptor-negative tumors with mammography, ultrasound, and MRI. AJR Am J Roentgenol. 2010;194:1160–6.
Kojima Y, Tsunoda H. Mammography and ultrasound feature of triple-negative breast cancer. Breast Cancer. 2011;18:146–51.
Kojima Y, Tsunoda H, Honda S, Kikuchi M, Kawauchi N, Yoshida A, Yagata H, Yamauchi H, Suzuki K. Radiographic features for triple negative ductal carcinoma in situ of the breast. Breast Cancer. 2011;18(3):213–20.
Krecke KN, Gisvold JJ. Invasive lobular carcinoma of the breast: mammographic findings and extent of disease at diagnosis in 184 patients. AJR Am J Roentgenol. 1993;161(5):957–60.
Berg WA, Gutierrez L, NessAiver MS, et al. Diagnostic accuracy of mammography, clinical examination, US, and MR imaging in preoperative assessment of breast cancer. Radiology. 2004;233(3):830–49.
Selinko VL, Middleton LP, Dempsey PJ. Role of sonography in diagnosing and staging invasive lobular carcinoma. J Clin Ultrasound. 2004;32(7):323–32.
Hilleren DJ, Andersson IT, Lindholm K, Linnell FS. Invasive lobular carcinoma: mammographic findings in a 10-year experience. Radiology. 1991;178(1):149–54.
Le Gal M, Ollivier L, Asselain B, et al. Mammographic features of 455 invasive lobular carcinomas. Radiology. 1992;185(3):705–8.
Butler RS, Venta LA, Wiley EL, Ellis RL, Dempsey PJ, Rubin E. Sonographic evaluation of infiltrating lobular carcinoma. AJR Am J Roentgenol. 1999;172(2):325–30.
Paramagul CP, Helvie MA, Adler DD. Invasive lobular carcinoma: sonographic appearance and role of sonography in improving diagnostic sensitivity. Radiology. 1995;195(1):231–4.
Evans WP, Warren Burhenne LJ, Laurie L, O’Shaughnessy KF, Castellino RA. Invasive lobular carcinoma of the breast: mammographic characteristics and computer- computer-aided detection. Radiology. 2002;225(1):182–9.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2015 Springer Science+Business Media New York
About this chapter
Cite this chapter
Shetty, M.K. (2015). Mammographic Signs of Breast Cancer. In: Shetty, M. (eds) Breast Cancer Screening and Diagnosis. Springer, New York, NY. https://doi.org/10.1007/978-1-4939-1267-4_5
Download citation
DOI: https://doi.org/10.1007/978-1-4939-1267-4_5
Published:
Publisher Name: Springer, New York, NY
Print ISBN: 978-1-4939-1266-7
Online ISBN: 978-1-4939-1267-4
eBook Packages: MedicineMedicine (R0)